pregnancy rhinitis: pathophysiological effects of oestrogen and
TRANSCRIPT
Thesis for doctoral degree (Ph.D.)2007
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Karin Toll
Thesis for doctoral degree (Ph.D.) 2007
Karin Toll
Pregn
ancy rhin
itis: pathophysiological effects of oestrogen an
d treatmen
t with oral decon
gestants
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Stockholm 2007
Department of Clinical Sciences, Intervention and TechnologyDivision of Otorhinolaryngology
Karolinska InstitutetStockholm, Sweden
Pregnancy rhinitis: pathophysiological effects ofoestrogen and treatment with oral decongestants
Karin Toll

Karin Toll
2007
Gårdsvägen 4, 169 70 Solna
Published and printed by

Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
ABSTRACT
Pregnancy rhinitis, a common condition, is thought to affect about 20 % of pregnant women. Thistype of rhinitis may develop at any time during pregnancy and the nasal stuffiness usually disappearsshortly after delivery. This condition is troublesome and can interfere with sleep, induce tirednessand dryness of the mouth. It is difficult to treat and no specific treatment seems to be entirelysatisfactory. The aetiology of pregnancy rhinitis and the effect of oestrogen on the nasal mucosaremain to be clarified.
For purposes of research, it is essential to evaluate subjective complaints of nasal obstruction.Several methods can be used to rate sensory intensities. The ”telephone scoring system” combinedwith a numerical rating scale (NRS) uses a computer to check the time when the estimate is made.Comparison of the symptoms estimated with two methods, a visual analogue scale (VAS) and”telephone scoring system” combined with a NRS show a strong correlation and symptom scoresare similar. However, the patients find the latter system easier to use.Phenylpropanolamine (PPA), a nasal decongestant given orally in sustained-release preparations, iscommonly prescribed to relieve nasal blockage in viral infections of the upper airways and in allergicrhinitis. PPA in double the recommended dose has an excellent decongestive effect on the nasalmucosa of healthy subjects, and it has the same decongestive effect as oxymetazoline nasal spray,but the systolic and diastolic blood pressures also increase temporarily. When PPA is given in therecommended dose, as assessed by the ”telephone scoring system”, it relieves nasal stuffiness inwomen with pregnancy rhinitis and has no effect on blood pressure.The increase in oestrogen levels in blood during in vitro fertilization (IVF) in a group of healthywomen causes hyperreactivity of the nasal mucosa after histamine challenge. However, no increasein nasal mucosal swelling is noted with low and high oestrogen levels before histamine challengealthough perfusion and velocity tend to increase at high oestrogen levels as measured with laserDoppler flowmetry. The increase in perfusion and velocity after histamine challenge is lower athigh than low oestrogen levels.In the human nasal mucosa of healthy subjects, immunocytochemistry showed distinct oestrogenreceptor (ER) ß positive cells in all sections. These cells, located subepithelially and close to thebasal membrane, had no relation to the vascular or glandular structures or to the epithelium. Theywere comparatively large with a centrally-located nucleus. Immunoreactive signals for ER ß proteinswere seen in their nuclei. Weak signals of ER ß immunostaining in the cytoplasm were also detected,which may indicate the presence of ER ß proteins in the cytoplasm. However, subglandular,endothelial and epithelial cells showed no immunoreactivity for ER ß in the nasal mucosa. Doubleimmunostaining showed co-expression of ER ß with the specific mast cell marker, anti-humanmast cell tryptase, in the vast majority of ER ß positive cells.
In conclusion, PPA in double the recommended dose has an excellent decongestive effect on thenasal mucosa of healthy subjects, and it has the same decongestive effect as oxymetazoline nasalspray. PPA given in the recommended dose relieves nasal stuffiness in women with pregnancyrhinitis and has no effect on blood pressure. These data indicate that PPA may be useful in thetreatment of pregnancy rhinitis. In the human nasal mucosa of healthy subjects, we found ER ßpositive cells. The increase in oestrogen levels in blood during IVF in a group of healthy womencauses hyperreactivity of the nasal mucosa after histamine challenge. These findings indicate thatoestrogen may play a role in the development of pregnancy rhinitis.
ISBN 978-91-7357-358-0

Karin Toll
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
CONTENTS
List of publication ----------------------------------------------------------------- 6.List of abbrevations --------------------------------------------------------------- 7.Introduktion ------------------------------------------------------------------------ 9.
Pregnancy rhinitis ------------------------------------------------------------ 9.Treatment of pregnancy rhinitis ------------------------------------------- 10.Methods of measuring changes in the human nasal mucosa --------- 10.Symptom scoring ------------------------------------------------------------ 11.Phenylpropanolamine ------------------------------------------------------- 12.Oestrogen receptors --------------------------------------------------------- 12.Mast cells --------------------------------------------------------------------- 13.
Aims of the present study ------------------------------------------------------- 13.Subjects and methods ------------------------------------------------------------ 14.
Study populations------------------------------------------------------------ 14.Rhinostereometry ------------------------------------------------------------ 14.Laser-Doppler flowmetry -------------------------------------------------- 15.Laser-Doppler flowmetry in combination with rhinostereometry ---- 15.Acoustic rhinometry -------------------------------------------------------- 17.Telephone method ----------------------------------------------------------- 18.In vitro fertilization --------------------------------------------------------- 18.Histamine challenge--------------------------------------------------------- 18.Immunocytochemistry ------------------------------------------------------ 18.
Results ------------------------------------------------------------------------------- 20.Paper I ------------------------------------------------------------------------- 20.Paper II ------------------------------------------------------------------------ 21.Paper III ----------------------------------------------------------------------- 22.Paper IV ----------------------------------------------------------------------- 23.Paper V ------------------------------------------------------------------------ 24.
Discussion -------------------------------------------------------------------------- 26.Summary --------------------------------------------------------------------------- 29.Acknowledegement --------------------------------------------------------------- 30.References -------------------------------------------------------------------------- 31.

6
Karin Toll
LIST OF PUBLICATIONS
Paper I Graf P, Toll K, Palm J, Hallén H. Effects ofsustained-release oral phenylpropanolamine onthe nasal mucosa of healthy subjects. ActaOtolaryngol (Stockh) 1999; 119: 837-42.
Paper II Hallén H, Djupesland P, Kramer J, Toll K, Graf P.Evaluation of new method for assessing nasalsymptoms. ORL 2001; 63: 92-5.
Paper III Toll K, Graf P. Phenylpropanolamine´sdecongestive effect on the nasal mucosa ofpregnant women with nasal stuffiness. Rhinology2006; 44(4): 274-8.
Paper IV Toll K, Graf P, Backheden M, Stjärne P. Evidencethat nasal mucosal hyperreactivity in healthywomen is induced by high levels of estrogen.Submitted for publication
Paper V Toll K, Canlon B, Dahlén B, Graf P, Henriksson E,Stjärne P. Oestrogen receptor ß in mast cells in thehuman nasal mucosa. Submitted for publication.
7
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
LIST OF ABBREVATIONS
ENT = Ear, nose and throat
ER = Oestrogen receptor
FSH = Follicle-stimulating hormone
GrH = Gonadotropin-releasing hormone
HE = High concentration of s-estrogen
IVF = In vitro fertilisation
LDF = Laser-Doppler flowmetry
LE = Low concentration of s-estrogen
NARES = Persistent non-allergic rhinitis with or without
eosinophilia
NRS = Numerical rating scale
PGH = Placental growth hormone
PPA = Phenylpropanolamine
PNEF = Nasal expiratory peak flow
PNIF = Nasal inspiratory peak flow
s-estrogen = Concentration of estrogen in blood serum
VAS = Visual analogue scale
VIP = Vasoactive intestinal polypeptide

8
Karin Toll

9
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Introduction
Rhinitis affects nearly 25% of the world´s population. It is not a single disease but a hetero-geneous group of disorders with diverse pathophysiologic mechanisms that are not alwaysinflammatory 1. The symptoms consist of one or more of the following: rhinorrhoea, sneezing,itching and/or nasal obstruction as well as a reduced sense of smell. They may have more thanone cause –e.g., anatomic obstruction, infection, underlying systemic disease, allergy or non-allergic inflammation 2. Although the symptoms of allergic and non-allergic rhinitis may besimilar, these subtypes can be distinguished clinically. Examples of non-allergic causes of rhinitisinclude infectious rhinitis, rhinitis medicamentosa, persistent non-allergic rhinitis with or withouteosinophilia (NARES), atrophic rhinitis, drug-induced rhinitis and rhinitis caused by conditionsinvolving hormones. Hormonal rhinitis is frequently associated with hypothyroidism, acromegalyand pregnancy, but it has also been noted in postmenopausal women and older men 3,4. Althoughthe precise mechanisms underlying hormonal rhinitis are disputed, some studies of sex hormonessuggest that these may cause nasal inflammation.
Far fewer recommendations concerning specific diagnostic criteria and treatment for non-allergicrhinitis are available than those for allergic rhinitis 5.
The diagnosis of rhinitis begins with a careful history and physical examination. As regards thehistory, one should focus on the characteristics of the patient´s symptoms, their frequency, andseverity. The examination should include general inspection of the ears, nose and throat, togetherwith rigid or flexible nasoendoscopy.
Both allergic and non-allergic rhinitis are important risk factors for asthma and bronchial hyper-reactivity. The pathophysiological processes that occur in the nasal mucosa with rhinitis and inthe lower airways with asthma are believed to reflect common manifestations of a generalizedinflammatory respiratory disorder 6,7. The presence of rhinitis can predict the degree of bronchialhyperreactivity, even in patients who have not yet been diagnosed as having asthma 8.
The disease is sometimes ignored because it is not life-threatening, but it seriously affects thepatient´s quality of life, productivity and health care costs. One of the commonest complaintscaused by rhinitis is disturbance of sleep. Poor-quality sleep leads to daytime drowsiness, fatigue,indecision, and significant impairments in learning9,10,11.
Pregnancy rhinitis
Pregnancy rhinitis, a common condition, is thought to affect 9-42 % of pregnant women 12,13,14.This type of rhinitis may develop at any time during pregnancy and the nasal stuffiness usuallydisappears shortly after delivery. Some defined pregnancy rhinitis: ”as nasal congestion in thelast 6 or more weeks of pregnancy without other signs of respiratory tract infection and with noknown allergic cause that disappear completely within 2 weeks after delivery”. With thisdefinition, the incidence is 22% 12. The condition is troublesome and can interfere with sleep,induce tiredness and dryness of the mouth. Comparisons of health-related quality of life scores inpatients with pregnancy rhinitis or other types of rhinitis and healthy controls show significantdifferences in these parameters 15.
10
Karin Toll
The possible effects on the foetus have also been discussed. Difficulty in breathing through thenose increases mouth breathing and snoring. Snorers have higher frequencies of hypertension,preeclampsia and of infants with intrauterine growth retardation 16,17.
The aetiology of pregnancy rhinitis remains to be clarified. Many authors have studied therelationship between hormones and pregnancy rhinitis and the effects of numerous hormones andsubstances. For example, progesterone, which has a vasodilating effect, was thought to causepregnancy rhinitis but some studies have shown that the serum levels of progesterone are similarin women with or without this condition 18.
Vasoactive intestinal polypeptide (VIP) and prolactin have also been implicated, but recentstudies do not support these theories 19.
One author reported that serum levels of placental growth hormone (PGH) were significantlyhigher in women with pregnancy rhinitis. However, that study included only five women withpregnancy rhinitis 18.
Oestrogen as a cause of nasal stuffiness is supported by the observation that patients withatrophic rhinitis who are treated with topical oestrogen develop congestion of the nasal mucosa 4.It has also been noted that contraceptive pills with high levels of oestrogen can induce congestionof the nasal mucosa as a side-effect 20. Ultrastructural and histochemical examinations showsquamous metaplasia of the nasal mucosa in these patients 21. Skin test reactivity in the menstrualcycle indicates that the wheal-flare reaction is significantly greater in the mid-cycle whenoestrogen levels reach their peak 22. Moreover, the nasal mucosa becomes hyperreactive tohistamine during ovulation, when the blood levels of oestrogen peak, which may explain whynasal stuffiness occurs in pregnancy 23.
Treatment of pregnancy rhinitis
Pregnancy rhinitis is difficult to treat and no specific treatment seems to be entirely satisfactory.Topical decongestants relieve the symptoms temporarily, but regular over-use of topicaldecongestants may result in nasal hyperreactivity and hypertrophy of the nasal mucosa, leading toa condition called rhinitis medicamentosa 24,25. The influence of topical decongestants on thefoetus has also been discussed 26. Topical steroids are effective in the treatment of many kinds ofrhinitis, such as allergic rhinitis, persistent non-allergic rhinitis, rhinitis medicamentosa and nasalpolyps 27,28,29,30,31. Although they are also widely used to treat pregnancy rhinitis, the onlycontrolled clinical study showed no effect of nasal steroids compared with placebo 32. This wouldsuggest that pregnancy rhinitis is not due to an inflammation and this should be studied further.Systemically-administered steroids have been given to patient with various types of rhinitis, butno clinical data are available on the safety or efficacy of these treatments during pregnancy 33,34.
Methods of measuring changes in the human nasal mucosa
To understand the pathogenesis of nasal mucosal inflammation and distinguish normal mucosalreactions from pathological, ones objective methods must be used to measure the state of themucosa 35. These should be non-invasive to minimize artefacts, and suitable for the human nasalmucosa. However, some methods are more appropriate for certain purposes 36,37.

11
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Nasal mucosal congestion can be assessed directly or indirectly. The commonest indirectmethods are rhinomanometry and nasal inspiratory and expiratory peak flow (PNIF and PNEF).They measure the effects of congestion of the nasal mucosa on nasal airway flow and resistance.Rhinomanometry is the most widely used method for indirect measurement of nasal mucosalcongestion 38. Active anterior rhinomanometry, the most common rhinomanometric method,records nasal airflow and air-pressure differences during quiet breathing in one cavity at a time.It permits an objective evaluation of surgery on cartilage and bone if the mucosa is decongested.It is also of value in the selection of patients who, after functional septoplasty, can expect a goodsurgical result, but less satisfactory for measurements of nasal hyperreactivity 39,40.
Both PNIF and PNEF are inexpensive, quick and easy for patients to use, can be done repeatedlyand the findings compare well with rhinomanometry. In most instances the nasal inspiratory peakflow technique is better than the expiratory peak flow one, because the PNEF measurements areaffected by mucus in the flow meter. They are useful in clinical studies in which the patients cancheck their airflow at home 41.
Another indirect method, acoustic rhinometry, measures the cross-sectional areas at variousdistances from the nostril. Rhinostereometry is a direct method in which the nasal cavity isviewed through an operating microscope. The latter two methods are described on page 14 and17.
An important methodological difference, as regards rhinomanometry, acoustic rhinometry andrhinostereometry, is that in the latter, the external nose is held open by a self-retaining nasalspeculum and the anterior part of the nasal cavity is viewed under magnification by means of anoperating microscope. Therefore measuring instruments, such as probes in the nose, can beintroduced and their position monitored under direct visual control and without touching thenasal mucosa.
Symptom scoring
Many studies are based on symptom scores 42. The most popular method is one in which thepatients record their symptoms in a diary at a certain time. Several methods can be used to ratesensory intensities. The visual analogue scale (VAS) is frequently used in clinical works 43,44.Usually it consists of a 10 cm line on a paper which is shown to the patients, who are asked toindicate the severity of their symptoms by putting a mark along the line with a pencil. Anothermethod for assessing symptoms is to use a numerical rating scale (NRS) with several manynumbers 45. With both methods the patients are usually asked to fill in a diary at certain times,for example, in the morning and evening46. However, it is well-known that some patients forgetto do this and they make entries in the whole diary on the last day of the trial.
A third method, the telephone scoring system, uses a computer to check the time when theestimates are made. The patients phone the computer and receive stepwise instructions. In ourstudy we used a NRS with ten alternatives (0-9) to estimate the severity of symptoms 47. Theresults and the times of the call were registered by the computer. The great advantage of themethod is that the computer records the time when the estimate is made. In this study, we wantedthe patients to score their symptoms in the morning and evening. Some of them went to bed inthe middle of the night and woke up in the middle of the day. With this method, we could seethese variations afterwards and exclude them.

12
Karin Toll
Phenylpropanolamine
Phenylpropanolamine (PPA), a widely used nasal decongestant given orally in sustained-releasepreparations, is commonly prescribed to relieve nasal blockage in viral infections of the upperairways and in allergic rhinitis 48,49,50. PPA, which is known in Sweden as Rinexin® (Recip,www.recip.se) has been available on the market for more than 50 years. In many countries, it isavailable over-the-counter, but in Sweden a prescription is necessary and the recommended doseis 50 mg twice daily.
Unfortunately, only a few controlled clinical studies have been done using objectivemeasurements to assess its decongestive effects.
The action of PPA is not understood, but it may be mediated directly by activation of post-junctional adrenoreceptors, indirectly by affecting the release and/or re-uptake of noradrenalin orby both mechanisms51.
In the USA, PPA has been withdrawn from the market because of a few cases of cerebralhaemorrhage 52. However, those patients took more than the recommended dose to lose weight.Some clinical studies show that when the recommended dose is exceeded, the blood pressureincreases but if the recommended dose is used, PPA has no clinically significant cardiovasculareffects 53,54.
Hardly any data are available that suggest a negative effect of PPA on foetal development. Anassociation between the maternal use of PPA and gastroschisis or small-bowel atresia has beendiscussed in retrospective case-control studies of maternal drug exposure and congenitalmalformations. A relation between the use of PPA and gastroschisis or small-bowel atresia wasfound in one study, but not in another 55,56,57. In a recent large study no teratogenic effect of oraldecongestants was found. They evaluated delivery outcome and included the presence ofcongenital malformations after maternal use of oral decongestants during pregnancy, as well asinformation about drug use that had been collected before pregnancy outcome was known 58.
Oestrogen receptors
Oestrogens are steroid hormones that have profound effects on both the male and femalereproductive systems. They also play important roles in the cardiovascular system and in themaintenance of bone tissue. These effects are all mediated by oestrogen receptors (ER) 59,60.The first ER was cloned in 1986. This receptor was regarded as the only ER until a second ERwas reported ten years later 61. Today they are known as ER-alfa and ER ß. Both receptors arevery similar at the amino acid level but their effects when activating these receptors differ greatly.ER-alfa and ER ß can be detected in many tissues. In some organs, both receptor subtypes areexpressed at about the same level, but in others, one or the other subtype predominates.Moreover, both receptor subtypes may be present in the same tissue, but in different cell types.For example, ER-alfa is mainly expressed in the uterus, prostate, ovary, testes, bone, breast, liverand white adipose tissue while ER-ß is expressed in the colon, lungs, brain, vascular endotheliumand salivary glands 62.
The role of oestrogen in the airways is still not fully understood and the findings are disputed 63.In the lungs, ER ß is highly expressed in pneumocytes and bronchiolar epithelial cells. It plays an
13
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
important role in the development of the lungs and its loss leads to abnormal lung structure andsystemic hypoxia in mice 64,65. Only a few studies have assessed the expression of ER-alfa andER ß in the upper airways and their function remains to be clarified 66,67.
Mast cells
Mast cells are key effector cells in a variety of allergic disorders and chronic inflammatorydiseases including nasal polyposis and asthma 68,69,70. It is well known that degranulation of mastcells leads to both microvascular and cellular responses, causing contractions and rapid oedemaof smooth muscles and mobilising other inflammatory cells to enter the inflammatory site. Themore recent discovery that mast cells are sources of cytokines which play key roles in signaltransduction and communication between immune cells suggests that mast cell activation mayaffect the development of T and B cell responses 71. Mast cells in nasal polyps express oestrogenreceptors and progesterone receptors 67. These findings indicate that mast cells may be theprimary target responsible for the effects of sex hormones in the airways.
Aims of the present study
1. To compare the onset and duration of the decongestive effects of 50 and 100 mgphenylpropanolamine (PPA) in healthy subjects for 8 hours, using rhinostereometry andacoustic rhinometry. An additional aim was to study the possible effects on the systolicand diastolic blood pressures.
2. To evaluate a new method of scoring symptoms with which we could check the timewhen estimates were made and to compare this method with use of a visual analoguescale (VAS) and a diary.
3. To evaluate the decongestive effect of phenylpropanolamine (PPA) 50 mg twice daily forseven days in women with pregnancy rhinitis by using rhinostereometry and thesubjective assessment of symptoms of nasal stuffiness. An additional aim was to studythe possible effects of PPA on the systolic and diastolic blood pressures.
4. To determine whether changes in oestrogen levels in the blood affect nasal mucosalreactivity and the microcirculation when the concentrations of other hormones remainconstant.
5. To investigate the expression and location of oestrogen receptor ß (ER ß) in the humannasal mucosa

14
Karin Toll
Subjects and methods
Study populationsIn Paper I, we studied 15 healthy volunteers (7 women, 8 men) who were students at theUniversity of Stockholm. They were all clinically healthy and had no history of allergy or otherrhinological disease.
In Paper II, we assessed 60 patients with allergic rhinitis, all of whom were allergic to birch.30 were from Ullevål University Hospital, Oslo, Norway and 30 from Soder Hospital,Stockholm, Sweden.
In Paper III, we evaluated 40 pregnant women with pregnancy rhinitis who had complained ofpersistent nasal obstruction for at least two weeks and were patients at Munkbron´s AntenatalClinic in Stockholm. Apart from pregnancy rhinitis, they were in good health and had no historyof allergy or other rhinological disease, high blood pressure or toxaemia in a previous pregnancy.
In Paper IV, we studied 15 healthy women who were undergoing in vitro fertilization (IVF) fortreatment of unexplained infertility. They had no history of allergy or other rhinological disease.
In Paper V, we examined the nasal mucosa of the medial turbinate from 8 patients (4 women,4 men; age 21-43) who underwent nasal septal surgery. They were all healthy patients and had nohistory of allergy or other rhinological disease.
All the studies were approved by the local ethics committee.
Rhinostereometry
This very accurate optical, direct, non-invasive method was designed to measure nasal mucosalswelling. Topographic measurements can therefore be made in the nose, without manipulation ofthe nasal structures. In rhinostereometry, the origin of a three-dimensional coordinate system isused as the fixed point. The apparatus consists of a surgical microscope placed on a micrometertable fixed to a frame. The microscope can be moved in three angular directions, thusestablishing the coordinate system. To permit measurements, the nasal cavity must be placed inthe coordinate system in such a way that it resumes the same position with a high degree ofprecision during repeated measurements. This is achieved by immobilising the subject´s headexactly to the frame by an individually-formed tooth splint 72,73.
The nasal cavity is viewed through the eyepiece of the microscope. Since the microscope has asmall depth of focus, a sharply delineated area of the surface is examined in the plane focus. Asthe ocular is equipped with a horizontal mm scale, the sharply delineated area, verticallydirected, crosses the mm scale and its position can be recorded. With this method, the area ofmeasurement can be re-identified with a high degree of accuracy in the same individual atvarious times with the subject as his own control 74,75.
Rhinostereometry permits measurements of all visible parts of the nasal mucosa. However, inthis study, we chose the mucosal surface of the medial side of the inferior concha. This region ispart of the valve area, which is considered to play a major role in the pathogenesis of nasalobstruction. Moreover, it consists of erectile tissue with high reactivity. These measurementswere made in Papers I, III and IV. In Paper I, we also used acoustic rhinometry becauserhinostereometry was not well known then. Today, rhinostereometry has been used in severalstudies 76,77,78.
15
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Laser-Doppler flowmetry
Laser-Doppler flowmetry (LDF), the only non-invasive method for studying the microcirculation,permits continuous and instantaneous measurements of nasal mucosal blood flow. Non-invasiveness is of great importance because it avoids artefacts. Several multiple microcirculatoryparameters, can be determined -i.e., the concentration of moving blood cells (CMBC), thevelocity of the blood flow (V) and the product of these two, perfusion or flow (P) 79. Someauthors have used laser-Doppler recordings from the nasal mucosa to make quantitativemeasurements -i.e., in mL/100 g tissue/min 4.
Laser-Doppler flowmetry in combination with rhinostereometry
Since no comparisons with other methods that measure blood flow in specific tissue areavailable, we express the data in arbitrary units, perfusion units (PU), concentration units (CU),and velocity units (VU). In our study we used a Periflux 4001 (Perimed, Sweden). The wave-length of the laser beam was 780 nm. We also used specially-designed probe and a micro-manipulator to position the probe tip under microscopic visual control at a well-defined distancefrom the mucosa 80. The measuring distance should be 0.3 mm. At this distance it is easy to avoidtouching the mucosa with the probe. LDF measures blood flow in the superficial parts of thenasal mucosa. In Paper IV, the nasal mucosa was studied with rhinostereometry and laser-Doppler flowmetry during challenge with histamine. The combination of these methods hasmany advantages. This combination permits the use of two non-invasive methods for direct and
Rhinostereometry
16
Karin Toll
simultaneous measurements of congestion and the microcirculation because rhinostereometryallows the laser probe to be in place in the nose during the measurements of congestion. Withrhinostereometry, one can study changes in the position of a small area of the nasal mucosalsurface during various conditions. The degree of congestion can be compared in the samesubjects at different times. However, rhinostereometry alone shows only the position of thesurface, and the degree of congestion. It gives no information about the conditions of the mucosa.Since the inflammatory reactions in the nose consist mainly of changes in the vascular state indifferent layers of vessels, it seems wise to combine the assessment of congestion with a methodfor measuring changes in microcirculation. Laser-Doppler flowmetry seems to be the bestmethod because like rhinostereometry, it is a non-invasive optical method that permitscontinuous recordings of microcirculatory parameters.
Laser Doppler flowmetry; probe in its position in the rhinostereometer.
17
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Acoustic rhinometry
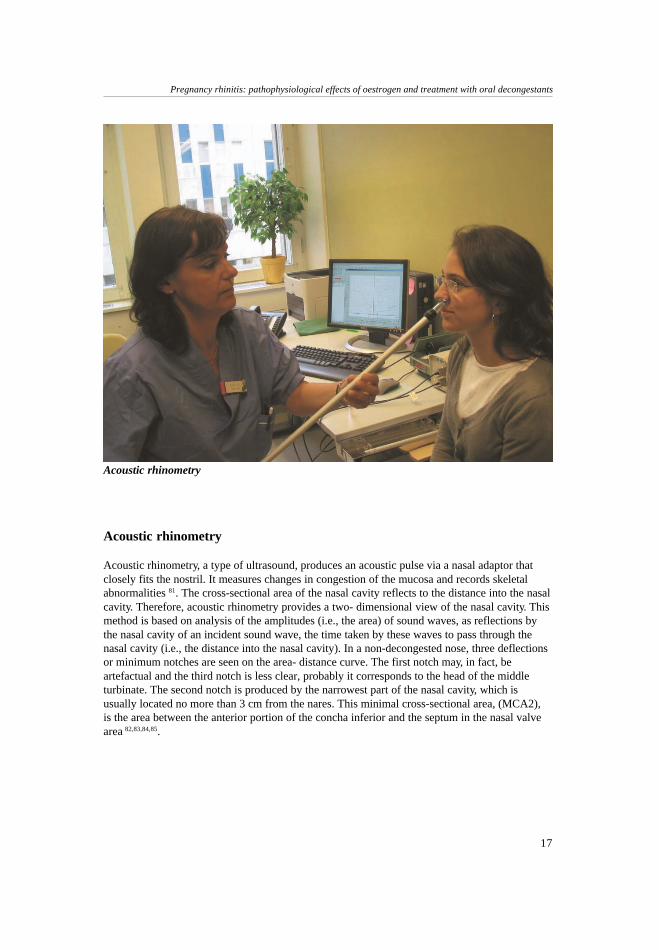
Acoustic rhinometry, a type of ultrasound, produces an acoustic pulse via a nasal adaptor thatclosely fits the nostril. It measures changes in congestion of the mucosa and records skeletalabnormalities 81. The cross-sectional area of the nasal cavity reflects to the distance into the nasalcavity. Therefore, acoustic rhinometry provides a two- dimensional view of the nasal cavity. Thismethod is based on analysis of the amplitudes (i.e., the area) of sound waves, as reflections bythe nasal cavity of an incident sound wave, the time taken by these waves to pass through thenasal cavity (i.e., the distance into the nasal cavity). In a non-decongested nose, three deflectionsor minimum notches are seen on the area- distance curve. The first notch may, in fact, beartefactual and the third notch is less clear, probably it corresponds to the head of the middleturbinate. The second notch is produced by the narrowest part of the nasal cavity, which isusually located no more than 3 cm from the nares. This minimal cross-sectional area, (MCA2),is the area between the anterior portion of the concha inferior and the septum in the nasal valvearea 82,83,84,85.
Acoustic rhinometry

18
Karin Toll
Telephone method
The severity of the symptoms can be assessed with the telephone scoring system, which recordsthe time when the estimates are made with a computer. The patients phone the computer andreceive stepwise instructions. In our study, we used a numerical rating scale (NRS) with tenalternatives (0-9) to estimate the severity of symptoms. The results and the times of the calls areregistered by the computer. The great advantage of this method is that the computer records thetime when the estimate is made. In Paper II, the patients were asked to score their symptoms inthe morning and evening. Some of them went to bed in the middle of the night and woke up inthe middle of the day. These variations could therefore be excluded afterwards 47.
In vitro fertilization
This part describes only the first part of in vitro fertilization (IVF) –i.e., ovarian stimulation, usedin Paper IV.
Various methods are used for IVF, but at Karolinska University Hospital it is common to controlthe development of eggs, and start IVF when the concentrations of oestrogens in blood have beenreduced to about zero. A nasal spray containing gonadotropin-releasing hormone, GrH(Suprecur®, Aventis Pharma AB; www.aventispharma.se) with benzalkonium chloride 0.1 mg/gas preservative, 1 puff (0.15mg) is sprayed into each nostril three times daily for about two tothree weeks until the concentration of oestrogens in blood is < 200 pmol/l. This is followed bystimulation with subcutaneous injections of follicle-stimulating hormone, FSH (GONAL-f®,Serono Nordic AB; www.serono.com), 1 injection (150-300 E) daily for about 12-14 days. Thelevels of oestrogens in blood increase, which stimulate the ovaries and the development of eggs.To reduce the adverse effects such as the ovarian hyperstimulation syndrome, the patientscontinue to take GrH nasal spray, 1 puff daily (alternating between the rihgt and left nostril). Thedevelopment of eggs is followed with ultrasound 86.
Histamine challenge
Nasal challenge has been used to study physiological and pathophysiological mechanisms in thenasal mucosa. Histamine affects irritant receptors, and thereby stimulates the nerves and vesselswhich in turn cause mucosal swelling. Histamine was dissolved in 0.5 % phenol and NaCl and0.14 ml of the solution was applied to the nasal mucosa in a concentration of 2.0 mg/ml.Previous studies have shown that provocation with this concentration seemed to be the criticaldose. A syringe was used to place this solution on the mucosal surface of the medial side of theinferior concha on one side of the nose during visual inspection 87,88,89. The histamine challenge isused in Paper IV.
Immunocytochemistry
In Paper V biopsies were taken during nasal septal surgery from the inferior turbinate in one ofthe nasal cavities. The biopsied tissue was fixed using 4% paraformaldehyde in phosphatebuffered saline (PBS). After fixation (1 hour), it was placed in 0.5% paraformaldehyde in PBSat 4oC, pending use. The tissue was then rinsed in PBS and placed in 20 % sucrose for 48 h for
19
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
cryoprotection. The specimens were embedded in cryomount, quickly frozen in isopentane withdry ice, and stored at -20?C. Serial sections (10 µm thickness) were cut on a cryostat (HM 500M,Zeiss, Germany) at –24?C.
The sections were taken from the freezer, allowed to dry and subsequently washed with TBS for5 min. Endogen peroxidase was removed by using 3 % H2O2 in TBS for 10 min.
After rinsing with TBS three times, they were incubated with background sniper for 10 min toreduce the non-specific background (Biocare Medical BS966G, LLC, 4040 Pike Lane, Concord,CA, USA) and then rinsed again three times with TBS.
The antibodies used were: monoclonal mouse anti-human mast cell tryptase (DAKO Cytomation,Denmark, M 7052 Clone AA1) 0.1ug /ml and polyclonal rabbit oestrogen receptor ß (catalogueno. ab 3577, Abcam, Cambridge, UK) 5 ug/ml. 60 min RT.
After rinsing with TBS, the slides were incubated with mouse probe (Biocare Medical MP530G).They were rinsed again with rabbit probe (Biocare Medical RP531G). To visualize themonoclonal antibody mouse anti-human mast cell tryptase, the slides were incubated withalkalinephosphatase mouse-polymer (Biocare Medical MAP532G). The alkalinephosphatase wasdeveloped with the Vulcan fast Red Chromogen Kit (Biocare Medical FR804). To visualize thepolyclonal oestrogen receptor ß antibody, the slides were incubated with horseradish rabbit-polymer (Biocare Medical RH531G). The HRP was developed with DAB+Ni (Vector SK4100).The slides, counterstained with Mayer HTX, were mounted with crystal mount (Biomeda) andthen with DPX mounting (VWR England).
Monoclonal mouse anti-human mast cells tryptase from Dako Cytomation, Denmark, code no.M7052 Clone AA1. Biocare Medical (www.biocare.net), Biocare Medical LLC,4040 Pike Lane,Concord, CA 94520, USA. Vector (www.vectorlabs.com), Vector Laboratories Inc., 30 IngoldRoad, Burlingame, CA 9410, USA. Biomeda, Novakemi (www.novakemi.se), VWRInternational (www.vwr.com).
The specificity of the antibody was tested by pre-incubation of the antibody with ER â blockingpeptide (catalogue no. ab3564, Abcam, Cambridge, UK) applied to sections, and as a negativecontrol we used sections from mutant mice lacking the ER ß (BERKO mice). We also tested theeffect of various fixatives on the staining pattern of ER ß. These fixatives (4% paraformaldehyde/1% acetic acid or 4% paraformaldehyde/1% acetic acid/0.1% glutaraldehyde) in PBS werecompared to our standard fixation with 4% paraformaldehyde in PBS. The specificity of theantibody was further confirmed by Western blot with positive controls (data not shown) (ER ß530, Panvera, Madison, WI, USA).
20
Karin Toll
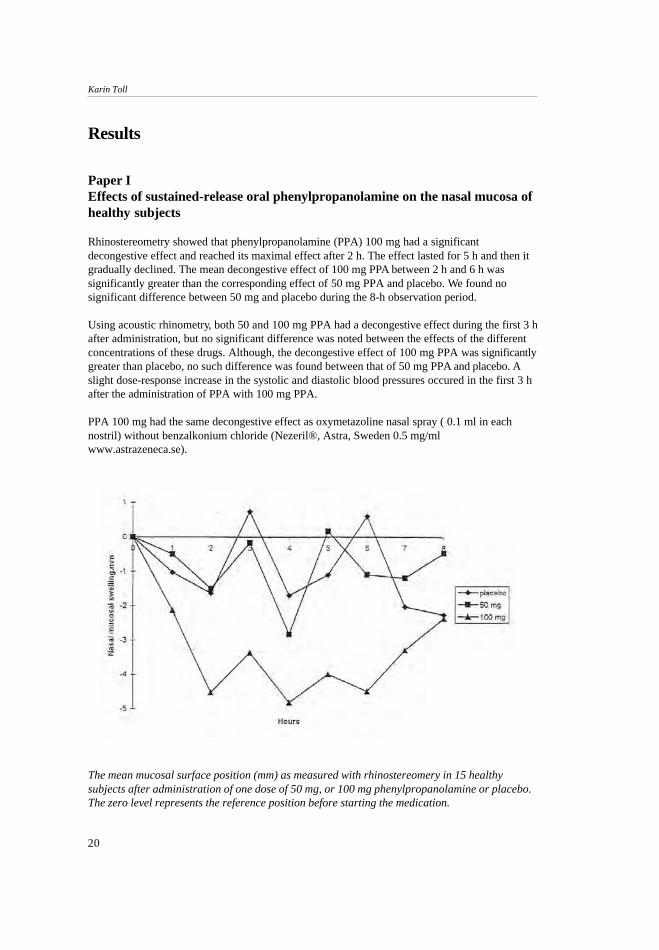
The mean mucosal surface position (mm) as measured with rhinostereomery in 15 healthysubjects after administration of one dose of 50 mg, or 100 mg phenylpropanolamine or placebo.The zero level represents the reference position before starting the medication.
Results
Paper IEffects of sustained-release oral phenylpropanolamine on the nasal mucosa ofhealthy subjects
Rhinostereometry showed that phenylpropanolamine (PPA) 100 mg had a significantdecongestive effect and reached its maximal effect after 2 h. The effect lasted for 5 h and then itgradually declined. The mean decongestive effect of 100 mg PPA between 2 h and 6 h wassignificantly greater than the corresponding effect of 50 mg PPA and placebo. We found nosignificant difference between 50 mg and placebo during the 8-h observation period.
Using acoustic rhinometry, both 50 and 100 mg PPA had a decongestive effect during the first 3 hafter administration, but no significant difference was noted between the effects of the differentconcentrations of these drugs. Although, the decongestive effect of 100 mg PPA was significantlygreater than placebo, no such difference was found between that of 50 mg PPA and placebo. Aslight dose-response increase in the systolic and diastolic blood pressures occured in the first 3 hafter the administration of PPA with 100 mg PPA.
PPA 100 mg had the same decongestive effect as oxymetazoline nasal spray ( 0.1 ml in eachnostril) without benzalkonium chloride (Nezeril®, Astra, Sweden 0.5 mg/mlwww.astrazeneca.se).
21
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
Paper IIEvaluation of a new method for assessing symptoms
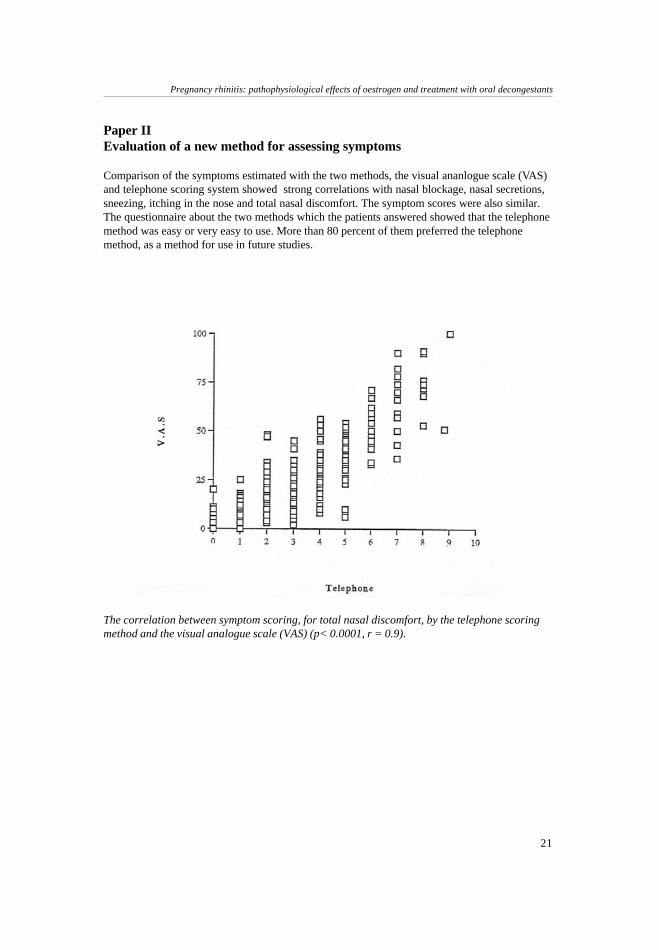
Comparison of the symptoms estimated with the two methods, the visual ananlogue scale (VAS)and telephone scoring system showed strong correlations with nasal blockage, nasal secretions,sneezing, itching in the nose and total nasal discomfort. The symptom scores were also similar.The questionnaire about the two methods which the patients answered showed that the telephonemethod was easy or very easy to use. More than 80 percent of them preferred the telephonemethod, as a method for use in future studies.
The correlation between symptom scoring, for total nasal discomfort, by the telephone scoringmethod and the visual analogue scale (VAS) (p< 0.0001, r = 0.9).
22
Karin Toll
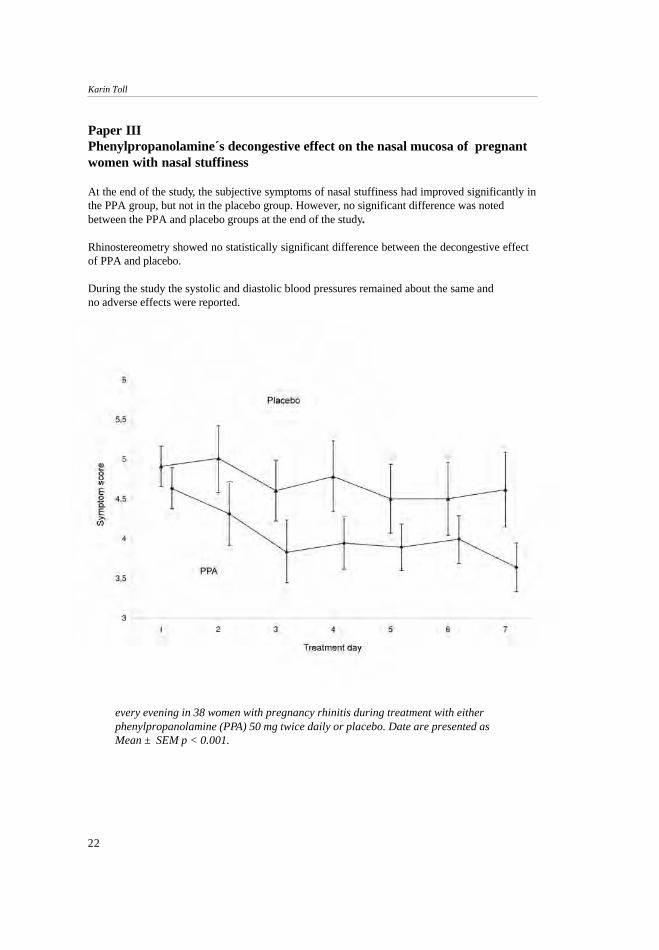
Paper IIIPhenylpropanolamine´s decongestive effect on the nasal mucosa of pregnantwomen with nasal stuffiness
At the end of the study, the subjective symptoms of nasal stuffiness had improved significantly inthe PPA group, but not in the placebo group. However, no significant difference was notedbetween the PPA and placebo groups at the end of the study.
Rhinostereometry showed no statistically significant difference between the decongestive effectof PPA and placebo.
During the study the systolic and diastolic blood pressures remained about the same andno adverse effects were reported.
every evening in 38 women with pregnancy rhinitis during treatment with eitherphenylpropanolamine (PPA) 50 mg twice daily or placebo. Date are presented asMean ± SEM p < 0.001.
23
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
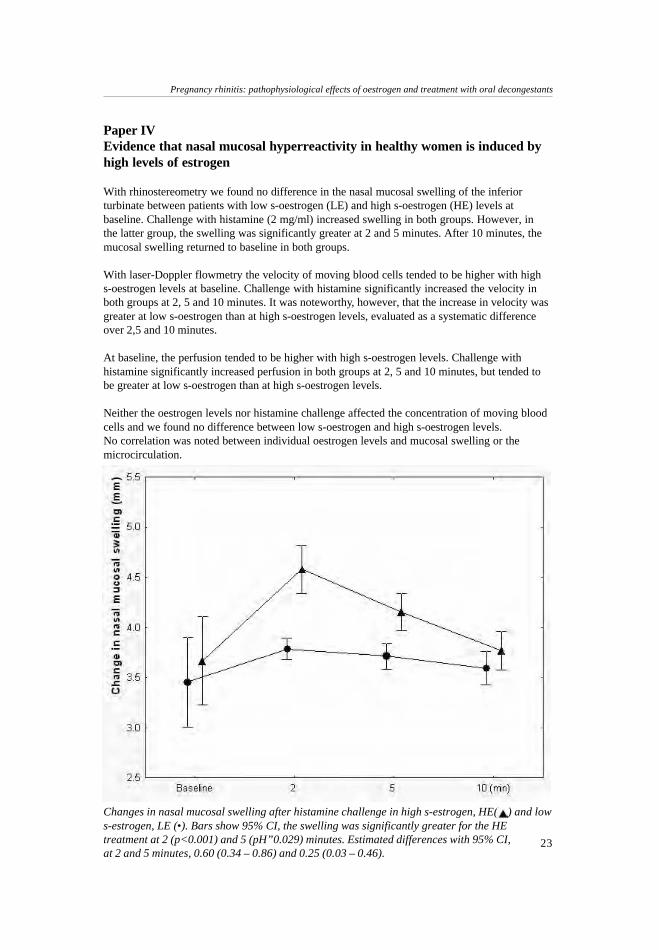
Changes in nasal mucosal swelling after histamine challenge in high s-estrogen, HE( ) and lows-estrogen, LE (•). Bars show 95% CI, the swelling was significantly greater for the HEtreatment at 2 (p<0.001) and 5 (pH”0.029) minutes. Estimated differences with 95% CI,at 2 and 5 minutes, 0.60 (0.34 – 0.86) and 0.25 (0.03 – 0.46).
Paper IVEvidence that nasal mucosal hyperreactivity in healthy women is induced byhigh levels of estrogen
With rhinostereometry we found no difference in the nasal mucosal swelling of the inferiorturbinate between patients with low s-oestrogen (LE) and high s-oestrogen (HE) levels atbaseline. Challenge with histamine (2 mg/ml) increased swelling in both groups. However, inthe latter group, the swelling was significantly greater at 2 and 5 minutes. After 10 minutes, themucosal swelling returned to baseline in both groups.
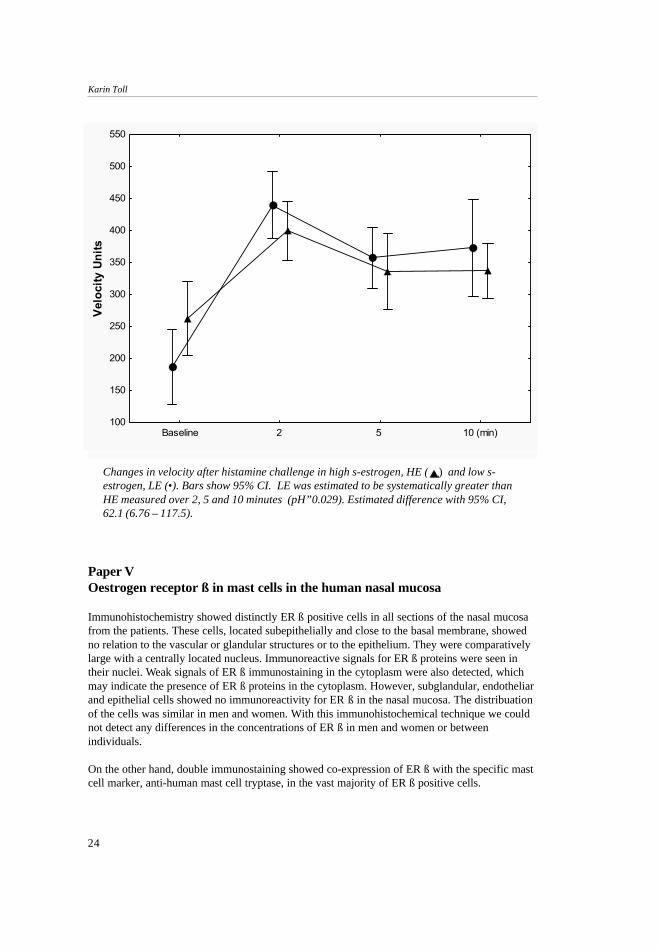
With laser-Doppler flowmetry the velocity of moving blood cells tended to be higher with highs-oestrogen levels at baseline. Challenge with histamine significantly increased the velocity inboth groups at 2, 5 and 10 minutes. It was noteworthy, however, that the increase in velocity wasgreater at low s-oestrogen than at high s-oestrogen levels, evaluated as a systematic differenceover 2,5 and 10 minutes.
At baseline, the perfusion tended to be higher with high s-oestrogen levels. Challenge withhistamine significantly increased perfusion in both groups at 2, 5 and 10 minutes, but tended tobe greater at low s-oestrogen than at high s-oestrogen levels.
Neither the oestrogen levels nor histamine challenge affected the concentration of moving bloodcells and we found no difference between low s-oestrogen and high s-oestrogen levels.No correlation was noted between individual oestrogen levels and mucosal swelling or themicrocirculation.
24
Karin Toll
Changes in velocity after histamine challenge in high s-estrogen, HE ( ) and low s-estrogen, LE (•). Bars show 95% CI. LE was estimated to be systematically greater thanHE measured over 2, 5 and 10 minutes (pH”0.029). Estimated difference with 95% CI,62.1 (6.76 – 117.5).
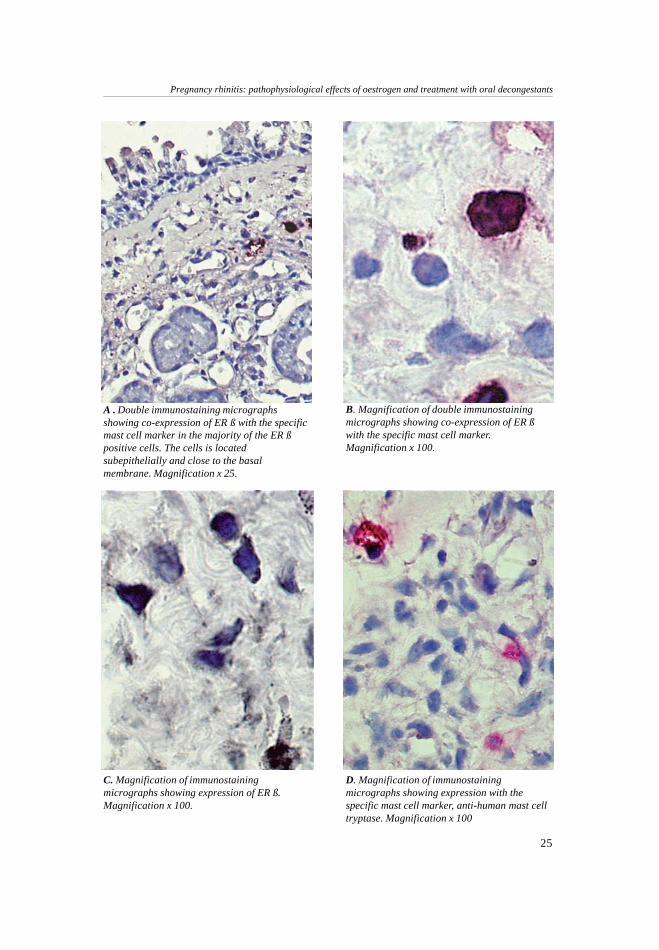
Paper VOestrogen receptor ß in mast cells in the human nasal mucosa
Immunohistochemistry showed distinctly ER ß positive cells in all sections of the nasal mucosafrom the patients. These cells, located subepithelially and close to the basal membrane, showedno relation to the vascular or glandular structures or to the epithelium. They were comparativelylarge with a centrally located nucleus. Immunoreactive signals for ER ß proteins were seen intheir nuclei. Weak signals of ER ß immunostaining in the cytoplasm were also detected, whichmay indicate the presence of ER ß proteins in the cytoplasm. However, subglandular, endotheliarand epithelial cells showed no immunoreactivity for ER ß in the nasal mucosa. The distribuationof the cells was similar in men and women. With this immunohistochemical technique we couldnot detect any differences in the concentrations of ER ß in men and women or betweenindividuals.
On the other hand, double immunostaining showed co-expression of ER ß with the specific mastcell marker, anti-human mast cell tryptase, in the vast majority of ER ß positive cells.
Baseline 2 5 10 (min)100
150
200
250
300
350
400
450
500
550
Velo
city
Uni
ts
Figure 3
25
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
A . Double immunostaining micrographsshowing co-expression of ER ß with the specificmast cell marker in the majority of the ER ßpositive cells. The cells is locatedsubepithelially and close to the basalmembrane. Magnification x 25.
B. Magnification of double immunostainingmicrographs showing co-expression of ER ßwith the specific mast cell marker.Magnification x 100.
C. Magnification of immunostainingmicrographs showing expression of ER ß.Magnification x 100.
D. Magnification of immunostainingmicrographs showing expression with thespecific mast cell marker, anti-human mast celltryptase. Magnification x 100

26
Karin Toll
Discussion
In Papers I and III, we found that the decongestive effect of phenylpropanolamine (PPA) 100mg is excellent in healthy volunteers, as measured with rhinostereometry and acoustic rhino-metry, and that of PPA 50 mg has a decongestive effect on nasal stuffiness in patients withpregnancy rhinitis, as measured by symptom scores 54,90. PPA is widely used as a nasaldecongestant in patients with viral infections and sinusitis and many prefer it to topicaldecongestants. The patients usually obtain their prescriptions from general practitioners. ManyENT specialists do not believe that PPA is effective because of the lack of controlled clinicalstudies using objective measurements for assessment of the decongestive effects of the drug.Since no satisfactory therapy is available pregnancy rhinitis, our results must be regarded asinteresting and useful. No agreement exists, especially in the USA, as regards the possibledeleterious effect of PPA on health. It was therefore PPA removed from the market, but thenshown to have no significant clinical cardiovascular, euphoric or CNS reinforcing effects whengiven in recommended doses. No correlation was found between cough and cold mixturescontaining PPA and haemorrhagic stroke. Some diet preparations contain PPA and a correlationbetween PPA and haemorrhagic stroke was reported in patients who were using those thatsuppress appetite 91. However, overweight is a known risk factor for haemorrhagic stroke. In ourstudies, we found no significant changes in blood pressure in women with pregnancy rhinitiswho were given recommended doses 90. 100 mg PPA had an excellent decongestive effect inhealthy subjects but they showed a slight increase in their blood pressure 54. Pregnancy isaccompanied by an increase in blood volume and frequently by a decrease in blood pressure. Itremains uncertain whether the decongestive effect of 100 mg PPA on the nasal mucosa occurswithout influencing the blood pressure. Since no satisfactory treatment of pregnancy rhinitis isavailable, more studies are needed to elucidate the effects of this dose in women with pregnancyrhinitis.
Concern has been expressed that PPA may have a negative effect on foetal development becausea few authors reported an association between the maternal use of PPA and gastroschisis andsmall-bowel atresia. Others found no significant association between the use of PPA andgastroschisis and small-bowel atresia, but in a later paper, they noted an interaction betweenvasoconstrictive drugs and maternal smoking, which they regarded as a risk for gastroschisis andsmall-bowel atresia. These were all retrospective case-control studies, and the possibility ofrecall bias exists 55,56,57.
In another report which included over 2000 women, PPA had no statistically significant effect onthe total malformation rate of any specific malformation.This study was undertaken to assess delivery outcome -i.e., the presence of congenitalmalformations after maternal use of oral decongestants during pregnancy, and information ondrug use that had been collected before the pregnancy outcome was known 58.
For purposes of research, it is essential to evaluate subjective complaints of nasal obstructionThis is usually done by using a symptom severity score rating or a visual analogue scale (VAS).In Paper II, we evaluated a new method for assessing symptoms with which the patients usedtheir telephone to call a computer 47. Its great advantage is that the computer records the timewhen the estimate is made. In this study, we wanted the patient to score their symptoms in themorning and evening. Those who went to bed in the middle of the night and then woke up in themiddle of the day could therefore be excluded afterwards. Today, most people have a cell phoneand they use it frequently -e.g., for bank transactions, purchase of bus tickets, etc. In our opinionthis is a good method for assessing symptoms in future studies. Since we found that telephone

27
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
scoring of symptoms was reliable and adequate when symptom scoring is used as hard, weevaluated it in Paper III 90.
Nasal congestion is difficult to quantify by clinical examination. Therefore objective assessmentof the nasal airway is essential for rhinologic research. The fact that there are many methodsavailable indicates that no method has proved good enough to replace all the others, but it alsoshows that several are suitable on different occasions.
Moreover, subjective complaints about nasal obstruction are not necessarily confirmed by objec-tive measurements. For example, an increase in nasal stuffiness is not always accompanied by anobjective increase in nasal airway resistance, a decrease in nasal peak flow or a reduction in theacoustic rhinometry value. Because sensations in humans are complex and not entirely linear,small changes in nasal shape, cause large shifts in the symptom severity score or VAS 35,36,92.
In Paper III, we showed that in a group of women with pregnancy rhinitis, PPA 50 mg twicedaily had a decongestive effect on nasal stuffiness, as measured by the symptom score.However, the findings with rhinostereometry were inconclusive. It would have been useful tocombine rhinostereometry with laser-Doppler flowmetry as we did in Paper IV, but theequipment was not available then 90.
In Paper I, we made measurements with rhinostereometry and acoustic rhinometry, both ofwhich are sensitive methods for studying nasal mucosal swelling. This was done becauserhinostereometry had hardly been used outside Sweden at that time. Acoustic rhinometry is well-known and has been evaluated by others 82,83,84,85. However, some differences between thefindings were noted, which accords with those in another study that showed a poor butsignificant correlation between these methods 93. This is not surprising because rhinostereometryrecords swelling, in mm, from a defined point on the inferior concha, but acoustic rhinometrymeasures the minimal cross-sectional area in a defined plane, or volume, in a given region of thenose. Rhinostereometry has now been used in several studies and is well-established. Its greatadvantage is that even minor changes are easily seen and accurately measured. Moreover it canbe combined with laser-Doppler flowmetry (LDF), which is the only non-invasive method forstudying the microcirculation. This combination permits the use of two non-invasive methods fordirect and simultaneous measurements of congestion and the microcirculation because rhino-stereometry allows the laser probe to be in place in the nose during the measurements ofcongestion (Paper IV). A disadvantage is that the investigator must be experienced in its use 73.In Paper III, PPA 50 mg twice daily and placebo had a decongestive effect on the nasal mucosa,as measured by rhinostereometry. This may seem surprising. However, the method is verysensitive and the measurements require an acclimatization period of about 30 minutes before thenasal mucosa reaches a baseline position, which is not affected by physical stress, temperature,etc 74. In this study, the acclimatization periods may have been less than 30 minutes because thesepregnant women were in a hurry. It seems possible that higher concentrations of adrenalin andnoradrenalin have a decongestive effect on the nasal mucosa 74.
The exact cause and pathophysiology of pregnancy rhinitis remain to be elucidated 3. Hormonallevels, especially those of oestrogen may induce nasal congestion. Some data support the viewthat the rhinitis is due to higher levels of oestrogen, e.g., wheal-flare reactions in the skin testincrease at the mid-menstrual cycle when oestrogen levels peak, and women on contraceptivesthat contain high levels of oestrogen frequently have nasal complaints 20,21,22,23. However,pregnancy rhinitis, has few distinct rhinoscopic signs and the possibility exists that the nose isnot congested but hyperreactive 13.
28
Karin Toll
In Paper IV, we showed that the increase in oestrogen levels during in vitro fertilization (IVF) inhealthy women causes nasal mucosa hyperreactivity after histamine challenge. However, noincrease in nasal mucosal swelling was noted with low and high oestrogen levels beforehistamine challenge although perfusion and velocity tended to increase at high oestrogen levels.We also found that the LDF measurements of increases in perfusion and velocity after histaminechallenge were lower at high than low oestrogen levels. Similar results were seen in patients withallergy as compared to those without. The increases in perfusion and velocity were lower in theformer group.
To study the role of oestrogen in pregnant women is difficult because of the effects and variationsin the concentrations of other hormones. We therefore recruited healthy women who wereundergoing in vitro fertilization (IVF). In our model, we increased their levels of oestrogenmarkedly for only 12-14 days and noted no measurable nasal swelling at baseline. In contrast,patients with pregnancy rhinitis develop nasal congestion, but they have high oestrogen levelsover a long period with resultant hyperreactivity, which may also cause this symptom. Althoughseveral mechanisms can explain pregnancy rhinitis, it seems likely that oestrogen is involved.
In Paper V, we found that immunoreactivity for monoclonal antibodies to ER ß is present in thesubepithelium of the nasal mucosa. Moreover, it may be located in mast cells, but not in theglands or vascular structures.
Mast cells are best known for their potent effector functions in allergic disorders 68,69,70. In recentyears, however, mast cells have been shown to be involved in a surprisingly complex range ofimmune functions that extend far beyond allergies and include the development of autoimmunedisorders and the initiation and maintenance of adaptive and innate host responses 71,94. In normalpregnancy, the histamine levels in blood may be highest during the first trimester, but are usuallylower during the second and third trimesters than in healthy subjects who are not pregnant.Many of the complications of pregnancy are associated with increases in the levels of histaminein blood 95. More data are needed on the possible roles of histamine in normal and complicatedpregnancies, but at present it seems likely that treatment to correct high histamine levels may beof value in pregnancy. The role of oestrogen in mast cells and the release of histamine are notclear.
Antihistamines are effective in allergy, a disease mediated by the release of histamine from mastcells 27. Very few studies have been done on the treatment of pregnancy rhinitis with anti-histamines. The second generation antihistamines have not been associated with an increase incongenital malformations in humans; however, most of them lack large safety studies inpregnancy.Intranasal sodium cromoglycate is a mast cell stabiliser used in allergic rhinitis, but no data areavailable on the treatment of pregnancy rhinitis with this drug either. In view of the above, therelations between oestrogen, mast cells, histamine and pregnancy rhinitis need to be clarified.
In conclusion, PPA in double the recommended dose has an excellent decongestive effect on thenasal mucosa of healthy subjects, and it has the same decongestive effect as oxymetazoline nasalspray. PPA given in the recommended dose relieves nasal stuffiness in women with pregnancyrhinitis and has no effect on blood pressure. These data indicate that PPA may be useful in thetreatment of pregnancy rhinitis. In the human nasal mucosa of healthy subjects, we foundoestrogen receptor(ER) ß positive cells. The increase in oestrogen levels in blood during in vitrofertilization (IVF) in a group of healthy women causes hyperreactivity of the nasal mucosa afterhistamine challenge. These findings indicate that oestrogen may play a role in the developmentof pregnancy rhinitis.
29
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
SUMMARY
Phenylpropanolamine (PPA) in double the recommended dose -i.e., 100 mg has an excellentdecongestive effect on the nasal mucosa of healthy subjects, but the systolic and diastolic bloodpressures also increase temporarily.
The effect of PPA on the nasal mucosa of healthy subjects is about the same as that ofoxymetazoline nasal spray ( 0.5 mg/ml; 0.1 ml in each nostril) without benzalkonium chloride.
When PPA is given in the recommended dose -i.e., 50 mg twice daily -it relieves nasal stuffinessin pregnancy rhinitis and has no effect on blood pressure.
The telephone scoring of symptoms is a reliable and adequate method for recording symptomsscoring as hard data.
Rhinostereometry shows that swelling of the nasal mucosa increases after histamine challenge inwomen with high levels of oestrogen in their blood during in vitro fertilization.
Laser-Doppler flowmetry shows that the microcirculatory parameters –i.e., velocity of movingblood cells and perfusion increase less when the oestrogen levels in blood are high.
With immunocytotochemistry, we present evidence for the presence of estrogen receptor ß in thenasal mucosa of healthy men and women. In addition, using double staining we show that theimmunoreactivity is mainly located in subepithelial mast cells.
30
Karin Toll
ACKNOWLEDGEMENTS
Thanks are due to all my dear colleagues and friends who helped me to complete this thesis. Inparticular, I wish to express my sincere gratitude and appreciation to:
Peter Graf, my friend, mentor and former chief, who introduced me to this field, for friendshipand his never-failing enthusiasm.
Pär Stjärne, my friend, other mentor and Head of the ENT department. I am grateful for hisconstant support and his special ability to make science interesting and fun.
Hans Hallén, my former mentor and co-author, for his support at the beginning of my research
Jan-Erik Juto and Hans Grudemo, my colleagues, for introducing me to the”rhinostereometry- and laser Doppler- world”.
Agneta Viberg, at the Dept. of Physiology and Pharmacology, and Elisabeth Henriksson at theDepartment of Medicine for guiding me in the field of immunocytochemistry.
Ingegerd Lundqvist and coworkers, at the Dept. of Obstetrics and Gynaecology, for helping meto encourage my IVF patients to take part in my research studies.
Anna Granath, my next-door friend and colleague for her support and for exciting discussions,not only about research.
Agneta Wittlock, for excellent secreterial assistance.
Zoe Walsh, for checking the English
Christoffer, my husband, for his love, loyalty and support and helping me to think aboutsomething else.
Gustaf, Maria and Annika, our beloved children for joy and happiness
Finally, our cats Misse and Maja, for their company on lonely days when I sat at home andwrote.
31
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
References1. Bachert C. Persistent rhinitis – allergic or
nonallergic?. Allergy 2004; 59(76): 11-5.
2. Lund V. Allergic rhinitis- making the correctdiagnosis. Clin Exp All 1998; 28(6): 25-8.
3. Ellegård EK. Pregnancy rhinitis. ImmunolAllergy Clin N Am 2006; 26: 119-35.
4. Nappi C, Di Spezio Sardo A, Guerra G, Di CarloC, Bifulco G, Acunzo G, Sammartino A, GalliV. Comparison of intranasal and transdermalestradiol on nasal mucosa in postmenopausalwomen. Menopause 2004 Jul-Aug; 11(4): 466-73.
5. Nassef M, Shapiro G, Casale T.B. Identifyingand managing rhinitis and its subtypes: allergicand nonallergic components- a consensusreport and materials from the Respiratory &Allergic Disease Foundation. Curr Med ResOpin 2006 Dec; 22(12): 2541-8.
6. Krouse JH, Veling MC, Ryan MW, PillsburyHC, Krouse JH, Joe S, Heller AJ, Han JK,Fineman SM, Brown RW. Executive summary:asthma and the unified airway. Otolaryngol.Head Neck Surg 2007 May; 136(5): 699-706.
7. Pawankar R. Allergic rhinitis and asthma: arethey manifestations of one syndrome?. ClinExp All 2006 jan; 36(1): 1-4
8. Chrystal-Peters J, Neslusan C, Crown WH,Torres A. Treating allergic rhinitis in patientswith combined asthma: the risk of asthma-related hospitalizations and emergencydepartments visits. J Allergy Clin Immunol2002 Jan; 109(1): 57-62.
9. Nathan RA. The burden of allergic rhinitis.Allergy Asthma Proc 2007 Jan-Feb; 28(1):3-9.
10. Schoenwetter WF, Dupclay L, Appajosyula S,Botteman MF, Pashos CL. Economic impactand quality-of-life burden of allergic rhinitis.Curr Med Res and Opin 2004; 20(3): 305-17.
11. Pratt EL, Craig TJ. Assessing outcomes fromthe sleep disturbance associated with rhinitis.Curr Opin Allergy Clin Immunol. 2007 Jun;7(3):249-56.
12. Ellegård E, Hellgren M, Torén K, Karlsson G.The incidence of pregnancy rhinitis. GynecolObstet Invest 2000; 49: 98-101.
13. Shushan S, Sadan O, Lurie S, Evron S, GolanA, Roth Y. Pregnancy-associated rhinitis. AmJ Perinatol 2006; 23: 431-4.
14. Bende M, Gredmark T. Nasal stuffiness duringpregnancy. Laryngoscope 1999 July; 109:1108-10.
15. Juniper EF. Measuring health-related qualityof life in rhinitis. J Allergy Clin Immunol 1997;99: 742-9.
16. Franklin KA, Holmgren PA, Jonsson F,Poromaa N, Stenlund H, Svanborg E. Snoring,pregnancy-induced hypertension and growthretardation of the fetus. Chest 2000; 117: 137-41.
17. Edwards N, Blyton DM, Kirjavainen TT,Sullivan CE. Hemodynamic responses toobstructive respiratory events during sleep areaugmented in women with preeclampsia. AmJ Hypertens 2001 Nov; 14: 1090-5.
18. Ellegård E, Oscarsson J, Bougoussa M. et al.Serum level of placental growth hormone israised in pregnancy rhinitis. Arch OtolaryngolHead Neck Surg 1998; 124: 439-43.
19. Bende M, Hallgårde U, Sjögren C. Nasalcongestion during pregnancy. Clin Otolaryngol1989; 14: 385-7.
20. Wolstenholme CR, Philpott, Oloto EJ, MurtyGE. Does the use of the combined oralcontraceptive pill cause changes in the nasalphysiology in young women?. Am J Rhinol2006 mars-april; 20: 238-40.
21. Toppozada H, Toppozada M, El-Ghazzawi I,Elwani S. The human respiratory nasal mucosain females using contraceptive pills: Anultramicroscopic and histochemical study. JLaryngol Otol 1984; 98: 43-51.
32
Karin Toll
22. Kalogeromitros D, Katsarou A, Armenaka M,Rigopoulos D, Zapanti M, Stratigos I. Influenceof the menstrual cycle on skin-prick testreactions to histamine, morphine andallergen.Clin Exp Allergy 1995 May; 25(5):461-6.
23. Haeggström A, Östberg B, Stierna P, Graf P,Hallén H. Nasal mucosal swelling andreactivity during a menstrual cycle. ORL 2000;62: 39-42.
24. Graf P. Overuse of oxy- and xylometazolinenasal sprays. Changes in nasal mucosalswelling and histamine sensitivity in healthysubjects and in patients with rhinitismedicamentosa. Thesis, Karolinska Institutet,1994.
25. Lekas M. Rhinitis during pregnancy andrhinitis medicamentosa. Otolaryngol Head andNeck Surg 1992; 107: 845-9.
26. Baxi LV, Gindoff PR, Pregenzer GJ, ParrasMK. Fetal heart rate changes followingmaternal administration of nasal decongestant.Am J Obstet Gynecol 1985; 153(7): 799-800.
27. Van Cauwenberge P, Bachert C, PassalacquaG, Bousquet J et al. Consensus statement onthe treatment of allergic rhinitis. Allergy 2000;55: 116-34.
28. Lundblad L, Sipilä P, Farstad T, DrozdziewiczD. Mometasone furoate nasal spray in thetreatment of perennial non-allergic rhinitis: aNordic, multicenter, randomized, double-blind,placebo-controlled study. Acta Otolaryngol2001; 121: 505-9.
29. Bachert C, Hörmann K, Mösges R, Rasp G,Riechelmann H, Muller R, Luckhaupt H, StuckBA, Rudack C. An update on the diagnosis andtreatment of sinusitis and nasal polyposis.Allergy 2003; 58: 176-91.
30. Hallén H, Enerdal J, Graf P. Fluticasonepropionate nasal spray is more effective andhas a faster onset of action than placebo intreatment of rhinitis medicamentosa. Clin ExpAllergy 1997; 27: 552-8.
31. Holmström M, Holmberg K, Lundblad L,Norlander T, Stierna P. Current perspectives onthe treatment of nasal polyposis: a Swedishopinion report. Acta Otolaryngol 2002 Oct;122(7): 736-44.
32. Ellegård EK, Hellgren M, Karlsson NG.Fluticasone propionate aqueous nasal spray inpregnancy rhinitis. Clin Otolaryngol 2001; 26:394-400.
33. Piette V, Daures JP, Demoly P. Treating allergicrhinitis in pregnancy. Curr Allergy Asthma Rep2006 May; 6(3): 232-8.
34. Mygind N, Andersson M. Topicalglucocorticoids in rhinitis: clinical aspects.Acta Otolaryngol 2006; 126: 1022-9.
35. Wang D-Y, Raza T, Gordon BR. Control ofnasal obstruction in perennial allergic rhinitis.Curr Opin Allergy Clin Immunol 2004; 4: 165-70.
36. Malm L. Measurement of nasal patency.Allergy 1997; 52(40): 19-23.
37. Numminen J, Ahtinen M, Huhtala H,Rautiainen M. Comparison of rhinometricmeasurements methods in intranasal pathology.Rhinology 2003; 41: 65-8.
38. Hirschberg A. Rhinomanometry: An update.ORL 2002; 64: 263-7.
39. Malm L, van Wijk G, Bachert C. Guidlines fornasal provocations with aspects on nasalpatency, airflow, and airflow resistance.Rhinology 2000; 38: 1-6
40. Wilson A, Sims E, Robb F, Cockburn W,Lipworh B. Peak inspiratory flow rate is moresensitive than acoustic rhinometry orrhinomanometry in detecting corticosteroidresponse with nasal histamine challenge.Rhinology 2003; 41: 16-20
41. Ottaviano G, Scadding GK, Coles S, Lund VJ.Peak nasal inspiratory flow; normal range inadult population. Rhinology 2006 Mar; 44(1):32-5.
33
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
42. Mandle M, Nolop K, Lutsky BN. Comparisonof once daily mometasone furoate (Nasonex)and fluticasone propionate aqueous nasalsprays for the treatment of perennial rhinitis:the 194079 Study Group. Ann Allergy AsthamImmunol 1997; 79: 237-45.
43. Linder A. Symptom scores as measures of theseverity of rhinitis. Clin Allergy 1988; 18: 29-37.
44. Aun C, Lam YM, Collett B. Evaluation of theuse of visual analogue scale in Chinese patients.Pain 1986; 25: 215-21.
45. De Conno F, Caraceni A, Gamba A, MarianiL, Abbattista A, Brunelli C, La Mura A,Ventafridda V. Pain measurement in cancerpatients: A comparison of six methods. Pain1994; 57: 161-6.
46. Hallén H, Graf P. Benzalkonium chloride innasal decongestive sprays has a long-lastingadverse effect on the nasal mucosa of healthyvolunteers. Clin Exp Allergy 1995; 25: 401-5.
47. Hallén H, Djupesland P, Kramer J, Toll K, GrafP. Evaluation of new method for assessing nasalsymptoms. ORL 2001; 63: 92-5.
48. Broms P, Malm L. Oral vasoconstrictors inperennial non-allergic rhinitis. Allergy 1982;37: 67-74.
49. Änggård A, Malm L. Orally administereddecongestant drugs in disorders of the upperrespiratory passages: a survey of clinicalresults. Clin Otolaryngol 1983; 9: 43-9.
50. Aschan G. Decongestion of nasal mucousmembranes by oral medication in acute rhinitis.Acta Otolaryngol 1974; 77: 433-8.
51. Johnson D. Pharmacology and safety ofphenylpropanolamine. Drug DevelopmentResearch 1991; 22: 197-207.
52. Kernan WN, Viscoli CM, Brass LM, BroderickJP, Brott T, Feldmann E, Morgenstern LB,Wilterdink JL, Horwitz RI.Phenylpropanolamine and the risk ofhemorrhagic stroke. N Engl J Med 2000; 343:1826-32.
53. Lake CG, Gallant S, Masson E, Miller P.Adverse drug effects attriuted tophenylpropanolamine: a review of 142 casereports. 1990 Aug; 89(2): 195-208.
54. Graf P, Toll K, Palm J, Hallén H. Effects ofsustained-release oral phenylpropanolamine onthe nasal mucosa of healthy subjects. ActaOtolaryngol (Stockh) 1999; 119: 837-42.
55. Torfs CP, Katz EA, Bateson TF, Lam PK, CurryCJ. Maternal medications and environmentalexposure as risk factors for gastroschisis.Teratology 1996 Aug; 54(2): 84-92.
56. Werler MM, Shehan JE, Mitchell AA. Maternalmedication use and risks of gastroschisis andsmall intestinal atresia. Am J Epidemiol 2002Jan 1; 155(1): 26-31.
57. Werler MM, Shehan JE, Mitchell AA.Association of vasoconstrictive exposures withrisks of gastroschisis and small intestinalatresia. Epidemiology 2003 May; 14(3): 349-54.
58. Källen BA, Olausson PO. Use of oraldecongestants during pregnancy and deliveryoutcome. Am J Obset Gynecol 2006; 194: 480-5.
59. Enmark E, Pelto-Huikko M, Grandien K,Lagercrantz S, Lagercrantz J, Fried G,Nordenskjöld M, Gustafsson J-Å. Humanestrogen receptor beta-gene structure,chromosomal localization, and expressionpattern. J Clin Endocrin and Metabol 1997 Dec;82(12): 4258-65.
60. Dahlman-Wright K, Cavailles V, Fuqua S. A,Jordan V.C, Katzenellenbogen J.A, KorachK.S, Maggi A, Muramatsu M, Parker M.G,Gustafsson J-Å. International Union ofPharmacology LXIV. Estrogen receptors.Pharmacol Rev 2006; 58: 773-81.
61. Kuiper G, Enmark E, Pelto-Huikko M, NilssonS, Gustafsson J-Å. Cloning of a novel estrogenreceptor expressed in rat prostate and ovary.Proc Natl Acad Sci USA 1996; 93: 5925-30.
62. Harris H A. Estrogen Receptor-Beta: Recentlessons from in vivo studies. Mol Endocrinol2007 Jan; 21(1): 1-13.
34
Karin Toll
63. Haggerty CL, Ness RB, Kelsey S, Waterer GW.The impact of estrogen and progesterone onasthma. Ann Allergy Asthma Immunol 2003Mar; 90(3): 284-91.
64. Patrone C, Cassel T.N, Pettersson K, Piao Y-S,Cheng G, Ciana P, Maggi A, Warner M,Gustafsson J-Å, Nord M. Regulation ofpostnatal lung development and homeostasisby estrogen receptor beta. Mol Cell. Biol 2003Dec; 23(23): 8542-52.
65. Morani A. Barros R, Imanov O, Hultenby K,Arner a, Warner M, Gustafsson J-Å. Lungdysfunction causes systemic hypoxia inestrogen receptor beta knockout (ER B -/-)mice. Proc Natl Aced Sci USA 2006; 103(18):7165-9.
66. Shirasaki H, Watanabe K, Kanaizumi E, KonnoN, Sato J, Narita S, Himi T. Expression andlocalisation of steroid receptors in human nasalmucosa. Acta Otolaryngol 2004; 124: 958-63.
67. Zhao XJ, McKerr G, Dong Z, Higgins CA,Carson J, Yang ZQ, Hannigan BM. Expressionof oestrogen and progesterone receptors bymast cells alone, but not lymphocytes,macrophages or other immune cells in humanupper airways. Thorax 2001; 56: 205-11.
68. Bradding P, Walls AF, Holgate ST. The role ofmast cell in the pathophysiology of asthma. JAllergy Clin Immunol 2006 Jun; 117(6): 1277-84.
69. Wardlaw Aj, Bradding P, Pavord ID, BrightlingCE. Mastcell localization within the airwaysmooth muscle: relationship to airwayhyperresponsiveness and other asthmaphenotypes. Clin Exp All Rev 2004; 4: 111-7.
70. Gavreau GM, Lee JM, Watson RM, Irani A-M, Schwartz LB, O´byrne PM. Increasednumbers of both airway basophils and mastcells in sputum after allergen inhalationchallenge of atopic asthmatics. Am J RespirCrit Care Med 2000; 161: 1473-8.
71. Metz M, Maurer M. Mastcells- key effectorcells in immune responses. Trend immunol.2007 Jun; 217: 304-28.
72. Juto JE, Lundberg An optical method todetermine changes in mucosal congestion inthe nose in man. Acta Otolaryngol (Stockh)1982; 94: 149-56.
73. Ellegård E. Practical aspects onrhinostereometry. Rhinology 2002 Sep; 40(3):115-7.
74. Juto JE, Lundberg C. Nasal mucosa reaction,catecholamines and lactate during physicalexercise. Acta Otolaryngol (Stockholm) 1984;98: 533-42.
75. Juto JE, Lundberg C. Variation in nasal mucosacongestion during rest. Acta Otolaryngol(Stockh) 1984; 98: 136-9.
76. Rudblad S, Andersson K, Bodin L, Stridh G,Juto JE. Nasal mucosal histamine reactivityamong teachers six years after working in anmoisture-damage school. Scand J WorkEnviron Health 2005; 31(1): 52-8.
77. Ellegård E, Karlsson G. IgE-mediated reactionsand hyperreactivity in pregnancy rhinitis. ArchOtolaryngol Head Neck Surg 1999; 125: 1121-5.
78. Grudemo H, Juto JE. Intranasal histminechallenge in normal subjects and allergicrhinitis before and after intranasal budesonidestudied with rhinostereometry andmicromanipulator-guided laser Dopplerflowmetry. ORL 2000; 62: 33-8.
79. Grudemo H, Juto JE. Rhinostereometry andlaser-Doppler flowmetry in human nasalmucosa: changes in congestion andmicrocirculation during intranasal histaminechallenge. ORL J Otorhinolaryngol Relat Spec1997 Jan-Feb; 59(1): 50-6.
80. Grudemo H, Juto JE. The impact of themeasuring distance on laser-Dopplermeasurements of the microcirculation in humannasal mucosa. A study of rhinostereometry andmicromanipulator-guided laser-Dopplerflowmetry. ORL J Otorhinolaryngol Relat Spec1997 Sep-Oct; 59(5): 280-5.
81. Clement PAR, Gordts F. Consensus report onacoustic rhinometry and rhinomanometry.Rhinology 2005; 43: 169-79.

35
Pregnancy rhinitis: pathophysiological effects of oestrogen and treatment with oral decongestants
82. Hilberg O, Pedersen OF. Acoustic rhinometry:recommendations for technical specificationsand standard operating procedures.Rhinology2000; 16: 3-17.
83. Cole P. Acoustic rhinometry andrhinomanometry. Rhinol Suppl 2000; 16: 29-34.
84. Grymer LF, Hilberg O, Pedersen OF,Rasmussen TR. Acoustic rhinometry: valuesfrom adults with subjective normal nasalpatency. Rhinology 1991; 29: 35-47.
85. Lenders H, Pirsig W. Diagnostic value ofacoustic rhinometry: patients with allergic andvasomotor rhinitis compared with normalcontrols. Rhinology 1990; 28: 5-16.
86. Speroff, Leon. Clinical gynaecologicendocrinology and infertility. Textbook 2005;7ed.
87. Hallén H, Juto J-E. Nasal mucosal reaction. Amodel for mucosal reaction during challenge.Rhinology 1992; 30: 129-33.
88. Hallén H, Juto J-E. Correlation betweensubjective and objective assessment of nasalhyperreactivity. ORL. 1995; 56: 51-4.
89. Hellgren J, Jarlstedt J, Dimberg L, Toren K,Karlsson G. A study of some current methodsfor assessment of nasal histamine reactivity.Clin Otolaryngol 1997 Dec; 22(6): 536-41.
90. Toll K, Graf P. Phenylpropanolamine´sdecongestive effect on the nasal mucosa ofpregnant women with nasal stuffiness.Rhinology 2006; 44(4): 274-8.
91. Morgan JP, Funderburk FR.Phenylpropanolamine and blood pressure: areview of prospective studies. Am J Clin Nutr1992 Jan; 55(1): 206-10.
92. Kim CS, Moon BK, Jung DH, Min Y-G.Correlation between nasal obstructionsymptoms and objective parameters of acousticrhinometry and rhinomanometry. Auris NasusLarynx 1998; 25: 45-8.
93. Hallén H, Graf P. Evaluation of rhinostereo-metry compared with acoustic rhinometry. ActaOtolaryngol (Stockh) 1999; 119(8): 921-4.
94. Cutolo M, Sulli A, Capellino S, Villaggio B,Montagna P, Seriolo B, Straub RH. Sexhormones influence on the immune system:basic and clinical aspects in autoimmunity.Lupus 2004; 13: 635-8.
95. Brew O. Sullivan MH. The links betweenmaternal histamine levels and complicationsof human pregnancy. J Reprod Immunol 2006Dec; 72(1-2): 94-107.
