preeclampsia: predicción actualización en obstetricia …10... · la búsqueda de casos debe ser...
TRANSCRIPT

Actualización en
Obstetricia La FE
Formación Continuada
10º Curso de Obstetricia “La FE”
Preeclampsia: Predicción

Early Prediction of Preeclampsia Estimated detection rates of (PE) requiring delivery before 34, 37, and 42 weeks’ gestation, at false positive rates (FPR) of 5% and 10%.
Screening test Detection rate (%)FPR (%) PE < 34 weeks PE < 37 weeks PE < 42 weeks
Maternal characteristics 5.0 36 33 2910.0 51 43 40
Poon LC. Nicolaides K. Early Prediction of Preeclampsia. Obstetrics and Gynecology International. 2014
Ut-PI 5.0 59 40 3110.0 75 55 42
MAP 5.0 58 44 3710.0 73 59 54
PAPP-A 5.0 44 37 3210.0 55 48 42
PlGF 5.0 59 41 2910.0 72 54 40
MAP and Ut-PI 5.0 80 55 3510.0 90 72 57
PAPP-A and PlGF 5.0 60 43 3010.0 74 56 41
Ut-PI, MAP, and PAPP-A 5.0 82 53 3610.0 93 75 60
Ut-PI, MAP, and PlGF 5.0 87 61 3810.0 96 77 53
Ut-PI, MAP, PAPP-A, and PlGF 5.0 93 61 3810.0 96 77 54


Example of nomogram for the estimation of the EOPE riskat 24 w
Perales A, Delgado JL, De La Calle M, García-Hernández JA, Escudero AI, Campillos JM, Sarabia MD, Laíz B, Duque M,
Navarro M, Calmarza P, Hund M, Álvarez FV; STEPS investigators.. sFlt-1/PlGF for early-onset pre-eclampsia prediction:
STEPS (Study of Early Pre-eclampsia in Spain). Ultrasound Obstet Gynecol. 2016 Nov 24. doi: 10.1002/uog.17373.

ACOG (2015). "Committee Opinion No. 638: First-Trimester Risk
Assessment for Early-Onset Preeclampsia." Obstet Gynecol 126(3):
e25-27.
Primiparity
Previous PE
Chr Hypertension, Chr renal disease or both
History of thrombophilia
Multiffetal pregnancy
IVF
Family history of PE
Type I or II Diabetes mellitus
Obesity
SLE
Advanced maternal age (>40 years)
Cribado de la PE: Opinión de sociedades
científicas

Low-dose aspirin use for the prevention :
U.S. Preventive Services Task Force
Risk Level Risk Factors RecommendationHigh History of preeclampsia Aspirin if has ≥ 1
Chronic hypertensionType 1 or 2 diabetesRenal diseaseAutoimmune disease (ie, SLE, APs)Multifetal gestation
Moderate Nulliparity Aspirin if several
Obesity (body mass index 30 kg/m2)Family history of preeclampsia (mother or sister)Sociodemographic characteristics (African American, low socioeconomic status)Age > 35 yPersonal history factors (e.g., low birthweight or small for gestational age, previousadverse pregnancy outcome, 10-y pregnancy interval)
Low Previous uncomplicated full-term delivery No Aspirin
LeFevre ML; U.S. Preventive Services Task Force.. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014 Dec 2;161(11):819-26.

1. La condición debe considerarse un problema sanitario.
2. Debe conocerse la historia natural de la enfermedad.
3. Debe identificarse la enfermedad en etapas de latencia o sintomáticas precoces.
4. Debe haber un test de cribado capaz de detectar la enfermedad etapas de latencia osintomáticas precoces, y debe ser aceptado y validado en la población.
5. Debe haber un tratamiento aceptable para cuando se detecta la enfermedad.
6. Tratar la enfermedad cuando se detecta en estadios latentes o sintomáticos precocesdebe mejorar su curso.
7. Debe disponerse de medios y condiciones para diagnosticar y tratar la enfermedad.
8. Debe haber un acuerdo sobre a que pacientes tratar para prevenir la enfermedad.
9. El coste económico del cribado y del tratamiento debería ser razonable en relación alcoste económico de la enfermedad.
10. La búsqueda de casos debe ser un proceso continuo.
Criterios que debe cumplir un test cribado
(OMS)
Wilson, J.M.G., and Jungner, G. Principles and Practice of Screening for Disease. WHO Public Paper 34. Geneva: World Health
Bibliography Organization, 1968. Whitby, L.G. Screening for disease: Definitions and criteria. Lancet 2:819–822, 1974.

Health Mother.- Pulmonary edema, cerebral hemorrhage, hepatic failure, renal failure, seizures (eclampsia), disseminated intravascular coagulation (primarily with abruption), and maternal death.
Fetus /neonate .- Preterm birth, stillbirth, growth restriction, admission to a neonatal intensive care unit, neurological sequelae, death
IncidenceVaries between countries, believed that worldwide, 3–5 % of pregnant women are affected
Spain 2.23% for pregnancy hypertension status (PHS), of which 1.1% corresponded to PE
(Comino-Delgado, Clin Exp Hypertens B 1986;5:217–30)
1. La condición debe considerarse un problema
sanitario

2.- Debe conocerse la historia natural de la
enfermedad
ETIOLOGÍA es desconocida
Factores inmunológicos, estrés oxidativo,
factores genéticos.
Enfermedad de las múltiples teorías
FISIOPATOLOGÍA Anómala implantación placentaria
PREECLAMPSIA.
Las células trofoblásticas (solo invade la decidua).
Arterias espirales estrechas y con resistencias elevadas que dificultan el
flujo uteroplacentario → Hipoxia → Favorece la liberación de factores
antiangiogénicos.
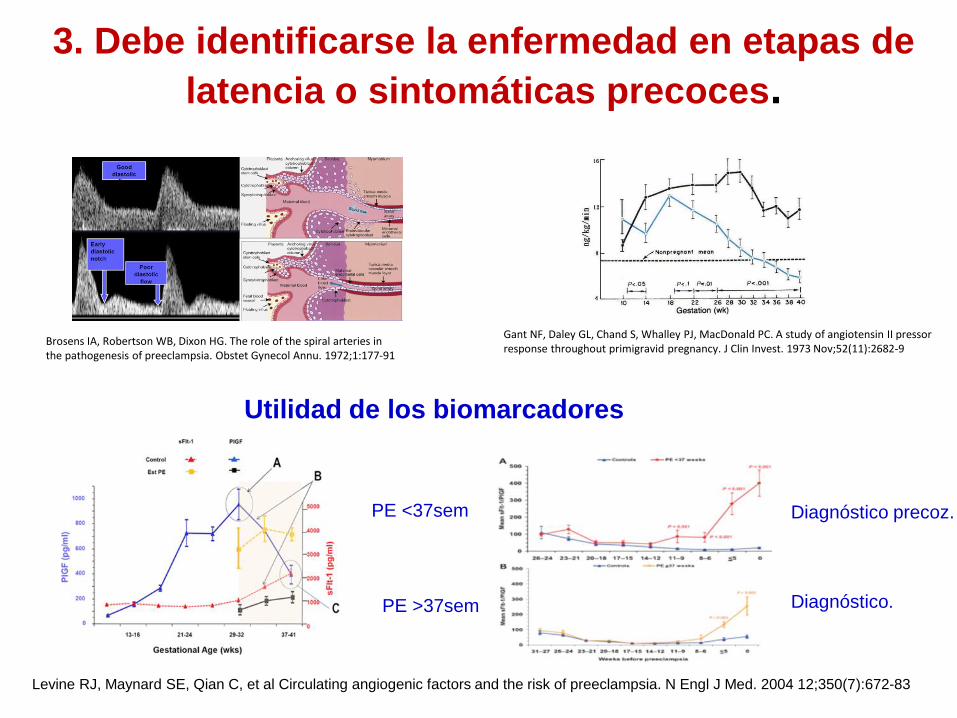
Brosens IA, Robertson WB, Dixon HG. The role of the spiral arteries in the pathogenesis of preeclampsia. Obstet Gynecol Annu. 1972;1:177-91
Gant NF, Daley GL, Chand S, Whalley PJ, MacDonald PC. A study of angiotensin II pressorresponse throughout primigravid pregnancy. J Clin Invest. 1973 Nov;52(11):2682-9
3. Debe identificarse la enfermedad en etapas de
latencia o sintomáticas precoces.
Diagnóstico precoz.
Diagnóstico.
PE <37sem
PE >37sem
Utilidad de los biomarcadores
Levine RJ, Maynard SE, Qian C, et al Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004 12;350(7):672-83

Norwitz ER. Prediction of preecclampsia UpToDate 2016Peter Wein Universal screening for pre-eclampsia and treatment with aspirin – the negative. Australasian Diabetes in Pregnancy Society Annual Scientific Meeting 27 – 28 august 2016
A good test for predicting women who will develop preeclampsia should be simple, rapid, noninvasive, inexpensive, easy to perform, and should not expose the patient to discomfort or risk
The technology should be widely available and the results reproducible and reliable, with a high likelihood ratio for a positive test (>15) and a low likelihood ratio for a negative result (<0.1) and good sensitivity and specificity.
Ideally, it should provide an opportunity for intervention to prevent development of the disease, or at least result in better maternal and/or fetal outcomes.
Currently, there are no clinically available tests that perform well according to these guidelines in distinguishing women who will develop preeclampsia from those who will not
4. Debe haber un test de cribado capaz de detectar
la enfermedad etapas de latencia o sintomáticas
precoces, y debe ser aceptado y validado en la
población.
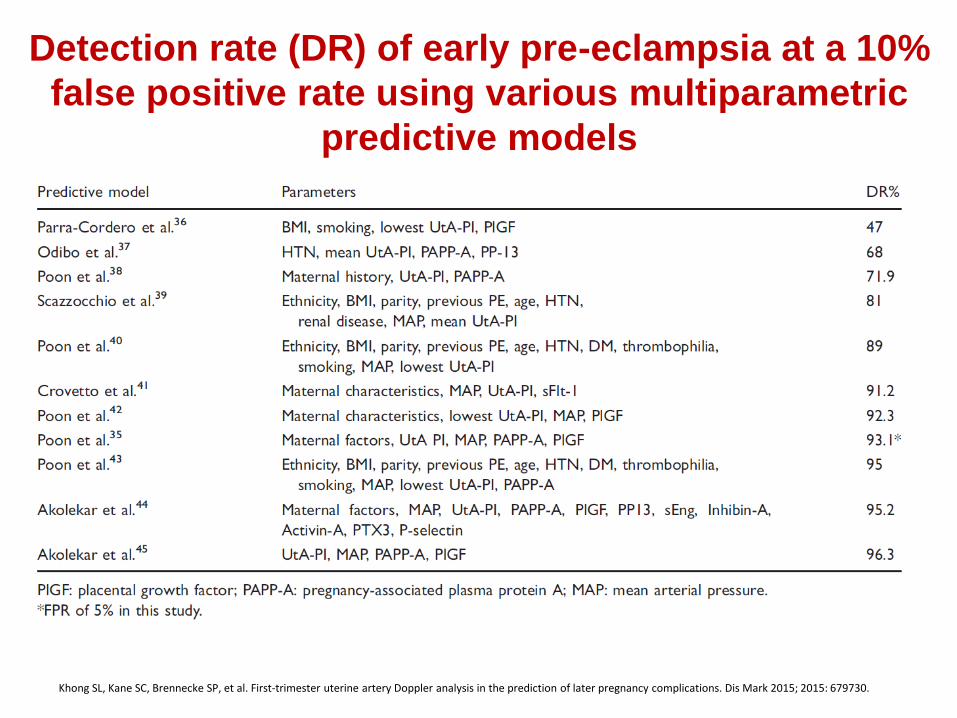
Detection rate (DR) of early pre-eclampsia at a 10%
false positive rate using various multiparametric
predictive models
Khong SL, Kane SC, Brennecke SP, et al. First-trimester uterine artery Doppler analysis in the prediction of later pregnancy complications. Dis Mark 2015; 2015: 679730.

Oliveira N, Magder LS, Blitzer MG, et al. First-trimester prediction of pre-eclampsia: external validity of algorithms in a prospectively enrolled cohort. Ultrasound Obstet Gynecol 2014; 279–285.
External validation of multiparametric models for
the prediction of EOPE and LOPE

Validation of a first-trimester screening model for pre-eclampsia
Scazzocchio, E., F. Crovetto, et al. (2016). "Validation of a first-trimester screening model for pre-eclampsia in an unselected population." Ultrasound Obstet Gynecol. In press
4621 women EOPE 28 (0,7%, LOPE 141 (3,4%), EOPE A priori risk, UtA‐PI, MAP LOPE A priori risk, PAPP‐A
Construction cohort
Validation cohort
Prev
2,1
0,5
Prev
3,4
0,7

5. Debe haber un tratamiento aceptable para
cuando se desarrolla la enfermedad
TRATAMIENTO
CURATIVO PARTO
Paliativo (↓) morbimortalidad
Antihipertensivos
Sulfato de Magnesio

Bazzano, A. N., E. Green, et al., "Assessment of the quality and content of national and international guidelines on hypertensive disorders of pregnancy using the AGREE II instrument." BMJ Open. 2016 6(1): e009189.
Preventions modalities for pre-eclampsia by CPGs
6. Tratar la enfermedad cuando se detecta en
estadíos latentes o sintomáticos precoces debe
mejorar su curso
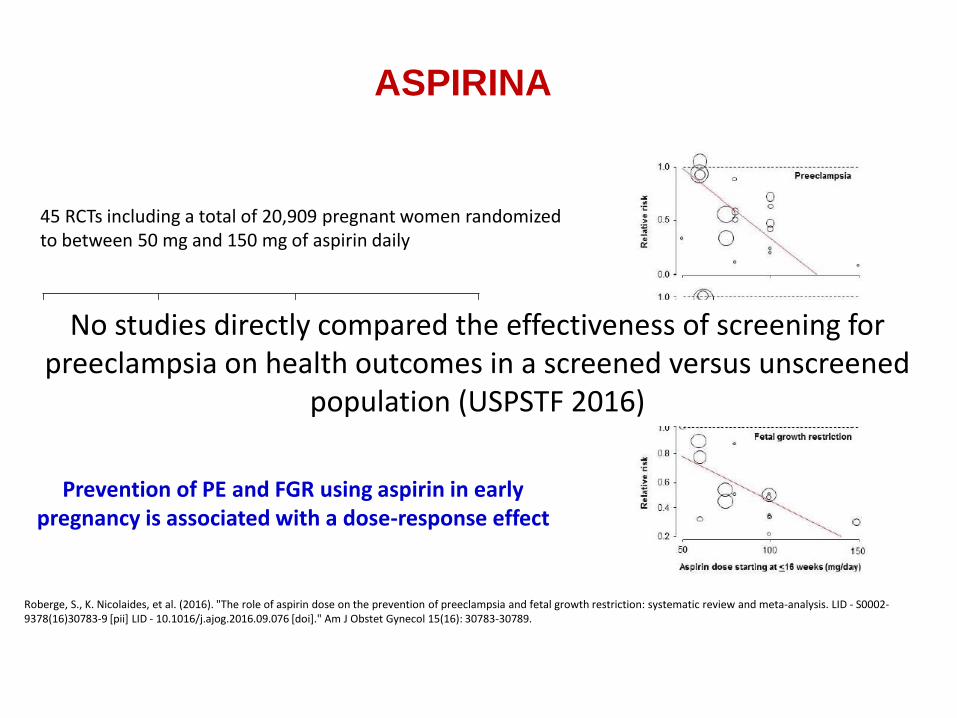
ASPIRINA
Roberge, S., K. Nicolaides, et al. (2016). "The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: systematic review and meta-analysis. LID - S0002-9378(16)30783-9 [pii] LID - 10.1016/j.ajog.2016.09.076 [doi]." Am J Obstet Gynecol 15(16): 30783-30789.
45 RCTs including a total of 20,909 pregnant women randomized to between 50 mg and 150 mg of aspirin daily
RR 95% CIPE 0,57 0.43-0.75Severe PE 0,47 0.26-0.83FGR 0,56 0.44-0.70
Prevention of PE and FGR using aspirin in early pregnancy is associated with a dose-response effect
No studies directly compared the effectiveness of screening for preeclampsia on health outcomes in a screened versus unscreened
population (USPSTF 2016)

7. Deben disponerse de medios y condiciones para diagnosticar y tratar la enfermedad
El Doppler y los biomarcadores serológicos y no siempre están
disponibles y no suelen emplearse en las visitas rutinarias del primer
trimestre.
Se necesita formación especializada en técnicas de ultrasonografía
para que exista uniformidad en los resultados y sea operador-
independiente.

8. Debe haber acuerdo sobre a quiénes hay que
tratar para prevenir.
Revisión sistemática en la que se incluyeron modelos predictivos quepredijeran PE en el primer trimestre.
4 definiciones diferentes de preeclampsia.
Número de eventos por variable: 6.5 en PE y de 5 en el caso
solo de EOPE.
• Cuando es menor de 10 se considera que el resultado
no es lo suficientemente robusto.
Sobreajuste: solo 3 tuvieron en cuenta pocos predictores
para disminuirlo.
Validación: en el momento del estudio, sólo se había
validado dos
Por tanto…
MODELOS
PREDICTIVOS DE
PE EN EL 1ER
TRIMESTRE
DEFICIENTES Y
POCO FIABLES
38 MODELOS PREDICTIVOS (PE 10, EOPE 18, LOPE 9, PE SEVERA 1).
Brunelli VB, Prefumo F. Quality of first trimester risk prediction models for pre-eclampsia: a systematic review. BJOG 2015; 122:904–
914

9. El coste económico del cribado y del tratamiento
debería ser razonable en relacion al coste
económico de la propia enfermedad
cribado + o ↑ riesgo
Bajas dosis de aspirina
y calcio
efectos a 30 años (AVAC)
P 1.7% = 18.919$
P >3% = <10000$
Rentabilidad del cribado ente cuando la prevalencia de la PE > 3% (coste<10000$).Shmueli A, Meiri H, Gonen R. Economic assessment of screening for pre-eclampsia. Prenat Diagn. 2012;32(1):29–38
ESTRATEGIA MUJERES CON PE MUJERES SIN PE COSTE (£)
1. No test-Tratar todas 20.25 980 185.12
2. Test-Tratar todas 20.25 980 215.12
3. Test- Tratar si cribado + 21.11 979 220.32
4. No test-No tratar 25 975 225.23
5. Test-No tratar 25 975 255.23
Económicamente A CORTO PLAZO lo más rentable ”No test - tratar a todas” NO JUSTIFICA EL CRIBADO PRIMER TRIMESTRE
Hyde C, Thornton S. Does screening for pre-eclampsia make sense? BJOG 2013;120:1168–1170

Si un factor de riesgo por sí solo tiene un NNPT < 250, con una reducción
del RR del 10%, se podría de iniciar la profilaxis con aspirina
Bartsch E, Medcalf KE, Park AL, Ray JG; High Risk of Pre-eclampsia Identification Group.. Clinical risk factors for pre-
eclampsia determined in early pregnancy: systematic review and meta-analysis of large cohort studies. BMJ. 2016 Apr
19;353:i1753.
25,356,688 gestaciones en 92 estudios
aPL
PE previa
Hta Cr
Diabetes pregestacional
IMC > 30
TRA
10. La búsqueda de casos debe ser un proceso
contínuo

Giguere, Y., S. Masse J Fau - Theriault, et al. Screening for pre-eclampsia early in pregnancy: performance of a multivariable model combining clinical characteristics and biochemicalmarkers. BJOG. 2015 122: 402-410.
Screening for pre-eclampsia early in pregnancy:
performance of a multivariable model combining clinical
characteristics and biochemical markers
7929 pregnant women between 10 and 18 weeks.
139 had PE, comprising 68 with severe PE and 47 with preterm PE

Conclusiones
Los test que predicen la preeclampsia son heterogéneos (diferentes
parámetros)
Los modelos multivariantes tienen un bajo VPP y su validación es
cuestionable.
La capacidad de predecir la preeclampsia tardía (LOPE) es pobre.
Los modelos multivariantes (biomarcadores serológicos y Doppler) no
siempre están disponibles.
Económicamente no está justificado el cribado.
Actualmente utilizar un modelo clínico, es lo razonable

A pesar de todo lo dicho hay que continuar
investigando nuevos modelos predictivos

New onset of elevated blood pressureAggravation of pre-existing hypertensionNew onset of protein in urineAggravation of pre-existing proteinuriaOther reason(s) for clinical suspicion of preeclampsiaPreeclampsiarelated symptoms
Epigastric painHeadacheExcessive edemaVisual disturbancesSevere swelling (face, hands, feet)Sudden weight gain
Preeclampsiarelated findingsLow plateletsElevated liver transaminasesIUGRAbnormal uterine perfusion
Reasons for suspicion of preeclampsia
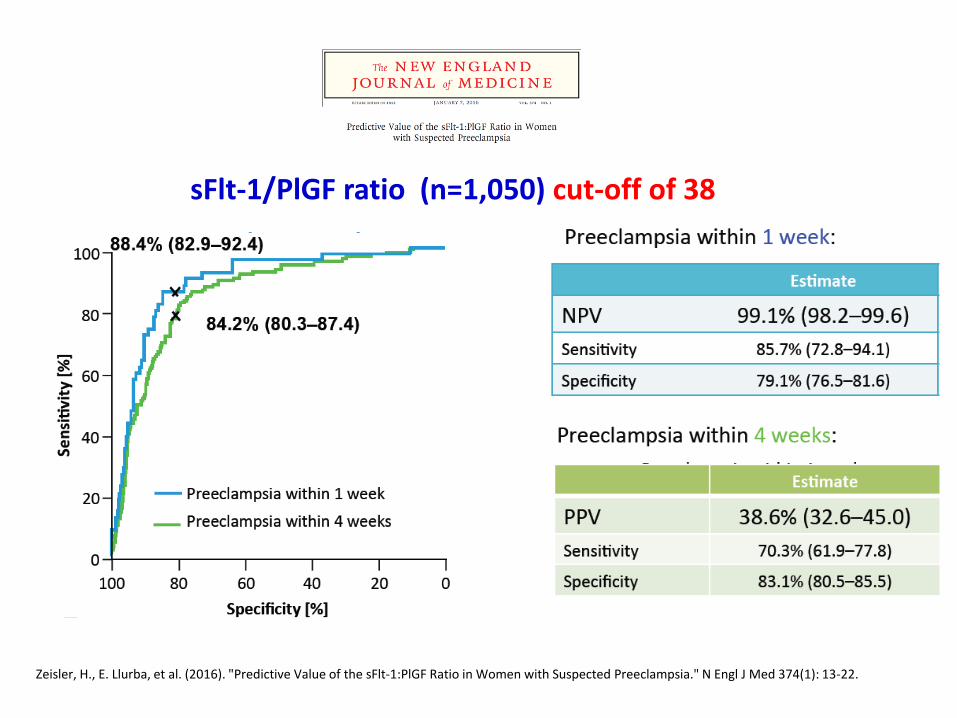
Zeisler, H., E. Llurba, et al. (2016). "Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia." N Engl J Med 374(1): 13-22.
Zeisler, H., E. Llurba, et al. (2016). "Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia." N Engl J Med 374(1): 13-22.
sFlt-1/PlGF ratio (n=1,050) cut-off of 38

% (95% CI) Rule out
within
1 week
Rule out
within
2 weeks
Rule out
within
3 weeks
Rule out
within
4 weeks
NPV 99.3
(97.9–99.9)
97.9
(96.0–99.0)
95.7
(93.3–97.5)
94.3
(91.7–96.3)
Sensitivity 80.0
(51.9–95.7)
78.0
(62.4–89.4)
70.0
(56.8–81.2)
66.2
(54.0–77.0)
Specificity 78.3
(74.6–81.7)
81.1
(77.5–84.4)
82.4
(78.8–85.7)
83.1
(79.4–86.3)
CI, confidence interval; HELLP, hemolysis, elevated liver enzymes, low platelets;
NPV, negative predictive value; PlGF, placental growth factor; sFlt-1, soluble fms-like tyrosine kinase-1
NPV using the sFlt-1/PlGF ratio cut-off value of 38 to rule out preeclampsia/HELLP syndrome
• Of 550 women, 98 (18%) developed preeclampsia/HELLP
syndrome at some point during their pregnancy:
− 5 (1%) within 1 week
− 41 (7%) within 2 weeks
− 60 (11%) within 3 weeks
− 71 (13%) within 4 weeks