pre-access redesign 2015 -...
TRANSCRIPT
Pre-Access Redesign 2015
September 17th , 2015
John Zaharis
System Director Pre-Access
Presence Health
2
Pre-Access Redesign 2015
2015 Reason for Action: Our Burning Platform
The front end must adapt to current marketplace changes which make it critical to secure every dollar in an environment of decreasing reimbursement. The identification of
sponsorship, increased POS collections, and implementing the Pre-Access 2014 redesign supports net revenue enhancement and reduced cost to collect.

3
Pre-Access Redesign 2015
Reason for Action:
Our 2015 Front End VSA determined that
– All orders whether faxed, electronic or held by patient must be scrubbed for
validity, medical necessity, and clinical clearance
– All required authorizations and referrals should be secured before the patient is
contacted
– Patients need reminder calls to decrease “no-show” rates
– Contact to patients should be kept to a minimum to have a truly “one stop”
shop
– Patients desire an online solution for Central Scheduling
– Currently most denials for outpatient services occur in areas where insurance
verification is not performed by a centralized unit
– Unique challenges due to 5 hospitals using EPIC and 6 using Meditech

4
Pre-Access Redesign 2015
Our 2014 Pre-Access EVSA determined via Voice of the Customer Surveys that
included Patients, Physicians, and Hospital Departments that experiences with the
Pre-Access department were varied in regards to process glitches and customer
service. After root cause analysis, many of these inconsistencies were attributable to
Pre-Access functions operating in silos and having inconsistent technologies.

5
Pre-Access Redesign 2015
2014 Voice of the Customer Survey Results
Technology Gaps:
“They need a better process [at Central Scheduling] for tracking faxes that come in.
I faxed an order over, they said they never received it even though I’m holding the
confirmation in my hand. I sent it a second time and got the person’s name. They
call back later and say they never received it and that this person never talked to
me.”
Certain “glitches” reported with some frequency:
– Lost paperwork is not uncommon, with scheduling and the physician office
blaming each other
– Difficulty handling situations that don’t conform to a standard pathway, e.g.
workers’ compensation, treatment for injuries where a lawsuit is involved
– Insurance approvals not secured and patient is threatened with a
cancellation
– Constant repetition of information, even for patients who are already in
EPIC
6
Pre-Access Redesign 2015
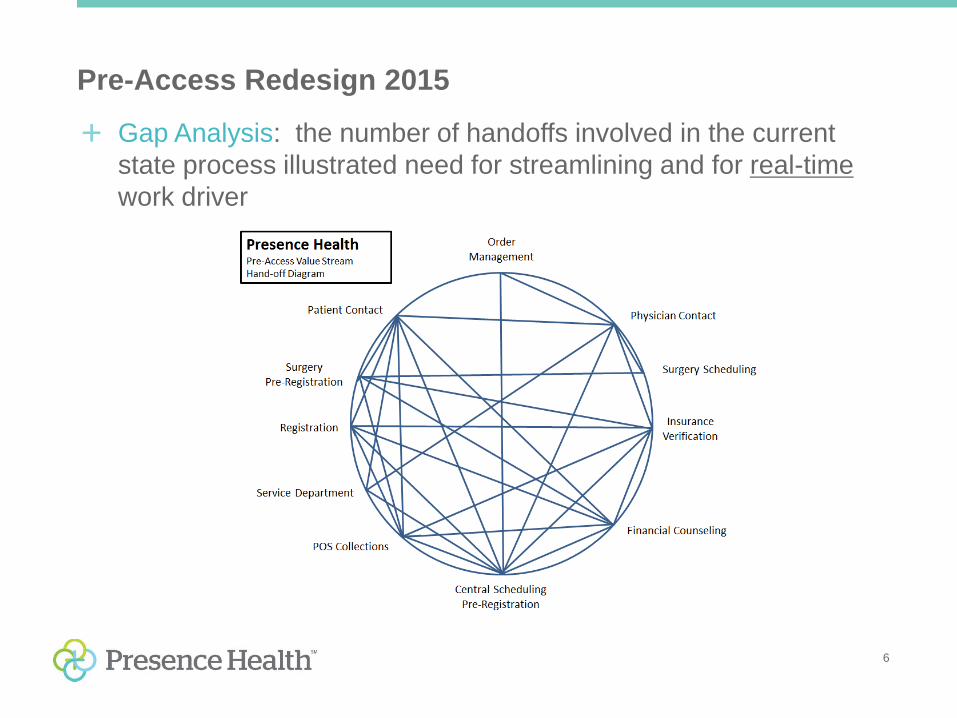
Gap Analysis: the number of handoffs involved in the current
state process illustrated need for streamlining and for real-time
work driver

7
Pre-Access Redesign 2015
Denial Risks Due to No Authorization
Every step in Process
is a potential denial risk

8
Pre-Access Redesign 2015
Voice of the Customer: Creating an Exceptional Experience
2014 2015
Current State Dimension Ideal State
Inconsistent experience between hospitals regarding scheduling process and customer satisfaction
Patient Satisfaction Single interaction with patient that minimizes handoffs including communication of full financial responsibility; provide a single point of contact for patient; allow patient to report directly to service area
Inconsistent experience for physicians regarding scheduling and authorization process
Physician Satisfaction Process that minimizes disruption to physicians and physician offices
High number of defects, lots of time spent searching for information (motion waste)
Process Improvement Standardize processes and integrate current functions and across Presence, defect-free process
Non-standard, inconsistent process for Meditech and EPIC, Downtimes, Numerous Software systems
Technology Coordination of care, navigation, communication, education
Inconsistent reporting structure leads to differences in site practices & standards
Reporting Structure System-based leadership structure that ensures a consistent experience with consistent expectations across Presence

9
Pre-Access Redesign 2015
How do we fix it?

10
Pre-Access Redesign 2015
Creating the Ideal Pre-Access Experience Patient-defined service expectations through Voice of the Customer:
− Greater control over initiating the scheduling process: phone, online
− Urgent tests scheduled for same day/within 24 hours
− Routine tests scheduled for 5 days from physician order
− Reminder call contact customized by mode and patient’s time frame
− Use of demographic information from EMR to solve problems, minimize
repetition
− All calls answered by a live person
− Want written documentation describing test, what/how to prepare, where to
park and enter the facility—not just verbal instructions
− Bypass onsite check in on day of test so that patient goes straight to
department, which is prepped and ready for their arrival

11
Pre-Access Redesign 2015
Future State Themes/Characteristics
ONE TOUCH CONCIERGE SERVICE
12
Pre-Access Redesign 2015
Patients value ease of access to
services, One Touch (or call) before
the scheduled service and want ease
of access to services
Tasks that patients deem
“administrative” such as Order
Management, Insurance Verification
and authorization process should
occur in the background and not
involve patients
How do we get there?
Ideal State for Pre-Access

13
Pre-Access Redesign 2015
Future State Themes/Characteristics
Beyond the 2015 Redesign Implementation
Patient Calls One Unified Call Center for all services inclusive of
Presence Medical Group (PMG), Presence Info Line and Acute
Care Needs
Patient Navigator to help coordinate visits in multiple
departments
Integration with PMG in Scheduling, Authorization, Referrals
Billing and Collections

14
Pre-Access Redesign 2015
Future State Themes/Characteristics
Beyond the 2015 Redesign Implementation
How will we get there:
– Real Time work-driver eliminating defects in process
– Implementation of payment estimation software
– Implementation of call recording software for quality
– Online scheduling with System approach for surgical and outpatient
Services
– Appointment reminders
– Centralized unit with consistent policies and procedures

15
Pre-Access Redesign 2015
Best Practices: HFMA Central Scheduling
– Use single scheduling software enterprise wide
– Have unit dedicated to Central Scheduling
– The Central Scheduling unit answers to the Chief Revenue Officer
– Scheduling System interfaces with Registration System
– Processes and information systems are integrated between scheduling and
pre-registration
– Medical Necessity is screened before the service is provided
– Services are postponed if not pre-authorized in advance
– Financial Counseling is part of the scheduling process
– Patient balances and payment obligations are discussed with the patients
– The hospital’s policy for POS collections is explained to the patient

16
Pre-Access Redesign 2015
Best Practices: HBI Healthcare Business Insights
– Major advantage of centralized model is the opportunity to standardize
policies and procedures
– This standardization further enhances productivity and performance by
allowing the following:
• Consistent performance expectations for staff
• Improved visibility through individual and department-level reporting
– In addition, Centralized Scheduling offers providers the ability to monitor
quality in a standardized manner through staff evaluations on skills that
impact patient satisfaction
17
Pre-Access Redesign 2015
Best Practices: HBI Healthcare Business Insights (Cont.)
– Additional Benefits of Centralized Central Scheduling
• Patients can schedule multiple procedures through one scheduler
• Patients are not as often put on hold, transferred or dropped
• Interaction with fewer staff members can reduce the number of times that
patients are asked to repeat demographic/insurance information
– Foundation for further consolidation and innovation
• Optimized productivity through automation (e.g. work
optimization software, automated workqueues, autodialers, etc.
• Increased pre-service collection due to standardized policies and
protocols
• Earlier detection of patients eligible for financial
assistance/charity care
• Improved hand-offs to authorizations or staff can be cross-trained
to handle authorizations for certain departments
• Is a pre-cursor to a “schedgistration” model

18
Pre-Access Redesign 2015
Solution Approach
– We determined the best solution for a real-time work driver after an
RFP went out to multiple vendors. A decision to move forward was
made with participation of IS
– Reduce and Eliminate Vendors to enable staff to be cross-trained
– Develop Flow Cells for the Front End to mitigate defects
– Integration with PMG referral management department
– Expansion of financial clearance process to departments outside of
current scope including PET Scan at the PCAC building
– Scheduling for ambulatory MRI clinics such as Park Ridge and
Healing Arts Center in Joliet
– Coordination and standardization of exam preps across Presence
Health

19
Pre-Access Redesign 2015
The Pre-Access Redesign occurred in 2014 where the needs of the voice
of the customer were addressed. Our process was redesigned to have
Order Management and Insurance Verification occur before the patient
was contacted for scheduling and Pre-Registration to have a one-touch
process

20
Pre-Access Redesign 2015
2015 Pre-Access Redesign Efforts for Central Scheduling
– Phase I: Central Scheduling Call Center Virtualization due to VOIP (Cisco)
upgrade
– Phase II: One Integrated Leadership Team for Pre-Access
• Benefits include:
– A consistent patient experience at each ministry
– Decreased Call Abandonment Rates
– Increased Average Speed of Answer
– Increase in Scheduled/Booked Appointments
– Leveraging cross-trained staff for absences
– Consistent financial clearance practices
– Elimination of defects at the beginning of Revenue Cycle Process
– Integration with PMG Centralized Referral Department
– Phase III: Real-Time Work driver Installation
– Real-time work driver for all staff with enhanced Order Management
capabilities
– Phase IV: Centralization of Pre-Access Staff
– Consistent experience and cross-training to mitigate absences

21
Pre-Access Redesign 2015
Phase I: VOIP Phone Upgrade
– Allows for greater call clarity and virtualization of call center
– Greater call quality than traditional analog lines
– Sets the foundation for unified reporting and centralization of staff
– We also have installed recording software at the EPIC call center
and plan to expand to the Meditech ministries in 2016
– This allows supervisors to monitor call quality and also provide
training opportunities
22
Pre-Access Redesign 2015
Phase II: Leadership Restructuring:
In order to support the vision of the 2014 and 2015 Pre-Access redesign
it was determined that a leadership restructuring would take place in
Pre-Access
This restructuring is budget neutral and allows for one Director to be
responsible for both EPIC and Meditech Scheduling
Each of the Meditech and EPIC Central scheduling units will report to
one Pre-Access manager to ensure that consistent practices are
followed across the continuum
Order Management will be expanded to include both EPIC and Meditech

23
Pre-Access Redesign 2015
Phase II: Leadership Restructuring: completed 7/20/15

24
Pre-Access Redesign 2015
Phase III: Real-Time work driver Installation – In process
Phase: Description: Begin Date: End Date:
Phase I: Foundational/Pre-Pilot Phase 6/22/15 9/10/15
Phase II: Pilot Sites PSJH/PSFH 9/14/15 11/06/15
Phase III: PRMC/PHFMC 11/09/15 12/11/15
Phase IV: PSMEMC 1/04/16 2/05/16
Phase V: PSJMC/PSMH 2/08/16 3/11/16
Phase VI: PMMC/PSJHE 3/14/16 4/15/16
Phase VII: PUSMC/PCMC 4/18/16 5/20/16
Current State as
of 9/17/14

25
Real-time Work Driver Implementation Update
Customers
– Patients
– Physicians
– Hospital Administration
– Revenue Cycle System
Leader
– Account Resolution
System Director
– Patient Access Regional
Leads
– Case Management
Directors
– Hospital Departments
– HIM
Core Team
– Patient Access System
Director
– Pre-Access System Director
– Financial Counseling Sys. Dir.
– Pre-Access Manager
– Central Scheduling Director
– Project Manager
– HIM Director
– Surgery Director(s)
– Radiology Director(s)
Suppliers
– Healthlink
– Meditech IS
– HWS
– Miramed
– Avadyne
– GLS
– MIDAS
– ONTRAC
– Passport
– emmi
Project Stakeholder High Level Overview:

26
Pre-Access Redesign 2015
Gantt Chart created
encompassing
duration of Project
Key events and
deliverables have
been outlined
including workshops
to outline key
workflows
Synced Gantt chart
to HWS project plan
and vVSM events
Revenue Cycle Project Management Tools: Gantt Chart
27
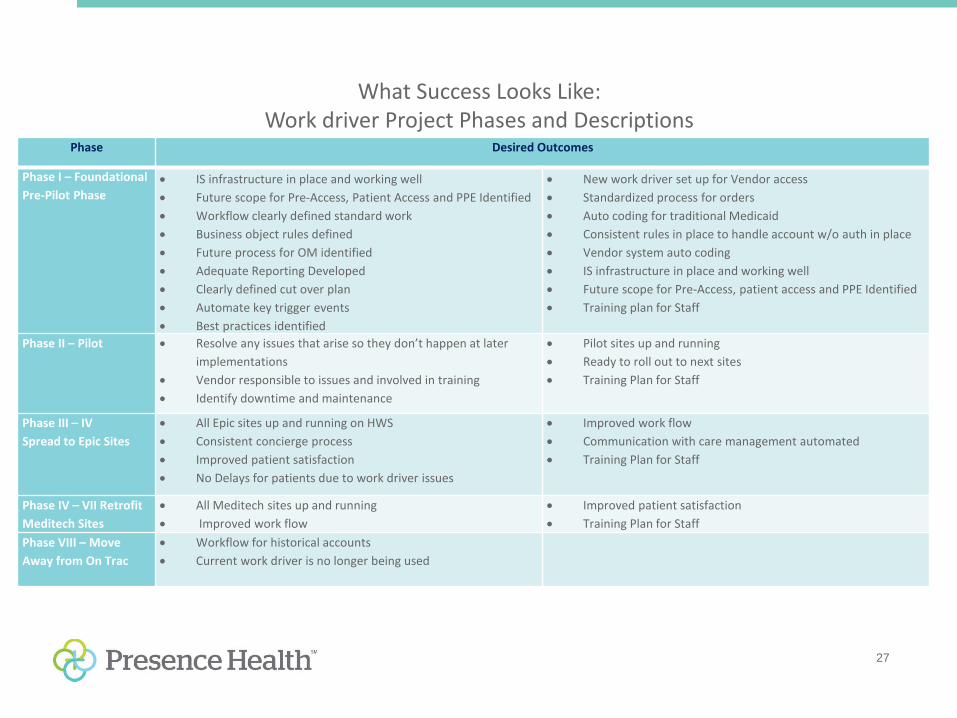
Phase Desired Outcomes
Phase I – Foundational
Pre-Pilot Phase IS infrastructure in place and working well
Future scope for Pre-Access, Patient Access and PPE Identified
Workflow clearly defined standard work
Business object rules defined
Future process for OM identified
Adequate Reporting Developed
Clearly defined cut over plan
Automate key trigger events
Best practices identified
New work driver set up for Vendor access
Standardized process for orders
Auto coding for traditional Medicaid
Consistent rules in place to handle account w/o auth in place
Vendor system auto coding
IS infrastructure in place and working well
Future scope for Pre-Access, patient access and PPE Identified
Training plan for Staff
Phase II – Pilot Resolve any issues that arise so they don’t happen at later
implementations
Vendor responsible to issues and involved in training
Identify downtime and maintenance
Pilot sites up and running
Ready to roll out to next sites
Training Plan for Staff
Phase III – IV
Spread to Epic Sites
All Epic sites up and running on HWS
Consistent concierge process
Improved patient satisfaction
No Delays for patients due to work driver issues
Improved work flow
Communication with care management automated
Training Plan for Staff
Phase IV – VII Retrofit
Meditech Sites
All Meditech sites up and running
Improved work flow
Improved patient satisfaction
Training Plan for Staff
Phase VIII – Move
Away from On Trac
Workflow for historical accounts
Current work driver is no longer being used
What Success Looks Like: Work driver Project Phases and Descriptions

28
Pre-Access Redesign 2015
KPI Source Current metric (baseline)
Future Metric Goal Date:
Reduction of 835 denials attributable to front end
Revenue Cycle KPI metrics
$0
$880,000 reduction
12 months after full implementation at all ministries
Increase net revenue attributable to Pre-Access redesign
Revenue Cycle KPI metrics
$0 $800,000 net revenue enhancement
12 months after full implementation at all ministries
Elimination of Current Work-driver, no PRE-Cert inpatient denials due to late status changes (occur because of limitations in work driver)
Revenue Cycle KPI Metrics
$314,000 per year due to work-driver errors, accounts not scoping in, late status changes, accounts left on FC worklist after status change
50% decrease 12 months after full implementation at all ministries
What Success Looks Like: Project Key Metrics

29
Pre-Access Redesign 2015
Important IS Project Milestones
Achieved to date:
– HWS Server build complete
– HWS Fax Server racked and configured
7/28/15
– EPIC outbound ADT feed complete
7/1/15
– Desktop Faxing workflow developed for
CDA/CBO 7/29/15
– Workflows Developed for Central
Scheduling, Pre-Registration and
Insurance Verification
– Workflows in Process for Financial
Counseling
30
Pre-Access Redesign 2015
Phase IV: Revenue Services Centralization Plan - In Process
Will result in the creation of an integrated EPIC Pre-Service Unit at SMEMC
and an integrated Meditech Pre-Service Unit at PSJMC Blackhawk Building
• Central Scheduling
• Order Management
• Pre-Registration
– Multi-faceted move involving:
• Central Scheduling
• Order Management
• Pre-Registration
• Billing and Follow-up
• Customer Service
• Vendor Management
• Financial Counseling
• Customer Service Staff

31
Pre-Access Redesign 2015
Preliminary Results of Centralization Efforts at PSJHE

32
Pre-Access Redesign 2015
Conclusion
– Future State for Pre-Access includes integration at a System level
with Presence Info line and Presence Medical Group to create a
truly one-stop shop for Presence Health
– The 2014 Pre-Access Redesign has been implemented in 2015
with progress made towards
• Cisco phone integration for call center virtualization
• Leadership Restructuring for consistent experiences
• Healthware real-time work driver implementation
• Centralization of both EPIC and Meditech Pre-Access Units to achieve
a scalable work force

33
Pre-Access Redesign 2015
Questions?
Contact Information:
630.914.2433 (office)