powerpoint presentationdental2.anamai.moph.go.th/download/article/differential_diagnosis...likely...
TRANSCRIPT
11/27/2016
1
DIFFERENTIAL DIAGNOSIS AND CLINICAL MANAGEMENT EPISODE I:
ORAL LESIONS
ASSOCIATED PROFESSOR SIRIBANG-ON PIBOONNIYOM KHOVIDHUNKIT
ADVANCED GENERAL DENTISTRY DEPARTMENT
FACULTY OF DENTISTRY, MAHIDOL UNIVERSITY
Tissue dessication
Altered cell permeability
Decreased elasticity
Deminished reparative capacity
• The demographic of older adults (i.e., 65 years of age and older) is growing and
likely will be an increasingly large part of dental practice in the coming years.
• Although better than in years past, the typical aging patient’s baseline health state
can be complicated by comorbid conditions (e.g., hypertension, diabetes mellitus)
and physiologic changes associated with aging.
• Older adults may regularly use several prescription and/or over-the-counter
medications, making them vulnerable to medication errors, drug interactions or
adverse drug reactions.
• Potential physical, sensory, and cognitive impairments associated with aging may
make oral health self-care and patient education/communications challenging.
• Dental conditions associated with aging include dry mouth (xerostomia), root
and coronal caries, and periodontitis; patients may show increased sensitivity to
drugs used in dentistry, including local anesthetics and analgesics.
Chaichalermsak S. J Dent Assoc Thai 2010; 60: 11-21.
1787 dental chart records were selected
22.3% (398 patients had systemic diseases)
Most common systemic diseases were
Cardiovascular disease (8.9%)
GI/liver disease (6.4%)
Disease of endocrine system (3.9%)
Most common drugs were
Antihypertensive drug (5.8%)
Analgesic/anti-inflammatory/
antibiotics drugs (5.3%)
Vitamins/supplements (4.5%)
11/27/2016
2
Shinkai RS. Spec Care Dentist 2006; 26: 116-20.
COMMON ORAL LESIONS IN ELDERLY PATIENTS
• Xerostomia/hyposalivation
• Infections in the oral cavity
• Candidiasis
• Viral infection
• Oral lichen planus / lichenoid reactions
• Burning mouth syndrome
• MRONJ
COMMON ORAL LESIONS IN ELDERLY PATIENTS
• Xerostomia/hyposalivation
• Infections in the oral cavity
• Candidiasis
• Viral infection
• Oral lichen planus / lichenoid reactions
• Burning mouth syndrome
• MRONJ
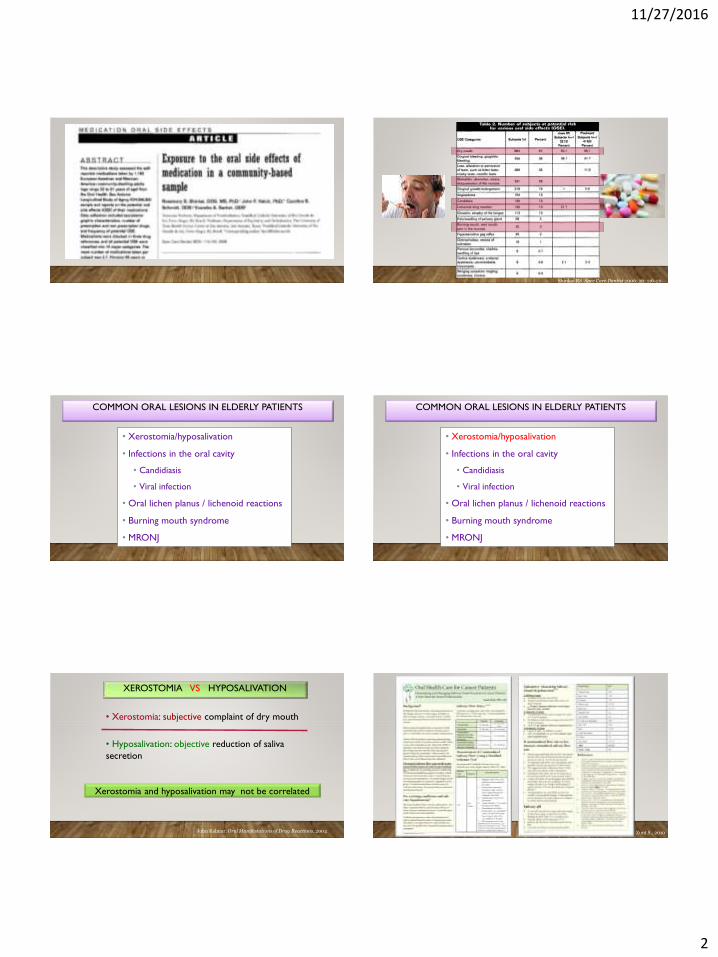
XEROSTOMIA VS HYPOSALIVATION
• Xerostomia: subjective complaint of dry mouth
• Hyposalivation: objective reduction of saliva
secretion
Xerostomia and hyposalivation may not be correlated
John Kalmar. Oral Manifestations of Drug Reactions. 2004 Zunt S., 2010

11/27/2016
3
Zunt S., 2010
Spit test
Modified Schirmer’s test

11/27/2016
4
Frothy saliva
Glassy appearance
No saliva pooling
Fissured tongue
Especially smooth surface caries and root caries
Hyposalivation induced caries
1)Medication
2)Radiation-induced dysfunction
3)Other systemic diseases
4)Sjögren’s syndrome
Common causes of hyposalivation
1)Medication
2)Radiation-induced dysfunction
3)Other systemic diseases
4)Sjögren’s syndrome
Common causes of hyposalivation
• Diuretics ยาขบัปัสสาวะ
• Hypertensive drugs ยารักษาโรคความดนัโลหิตสงู
• Statin drugs ยารักษาโรคไขมนัในโลหิตสงู
• Antihistamine ยาแก้แพ้
• Antireflux ยารักษาโรคกระเพาะ กรดไหลย้อน
• Sedatives ยาคลายเครียด
• Antipsychotics ยารักษาโรคจิตเวช
• Antidepressants ยารักษาโรคซมึเศร้า
11/27/2016
5
Treatment:
1) Hydration: small and frequent sip of water
2) Artificial lubricants
3) Stimulating agents
Sugar free candy or chewing gum: Xylitol, Trident
Pharmacological agents: pilocarpine hydrochloride (10mg qid)
: cevimeline (30mg tid)
4) Drug modification
5) Abstain from caffeinated drinks
5) Dental caries: fluoride application
6) Oral infection: candidiasis
Management of hyposalivation
• Xerostomia/hyposalivation
• Infections in the oral cavity
• Candidiasis
• Viral infection
• Oral lichen planus / lichenoid reactions
• Burning mouth syndrome
• MRONJ
COMMON ORAL LESIONS IN ELDERLY PATIENTS
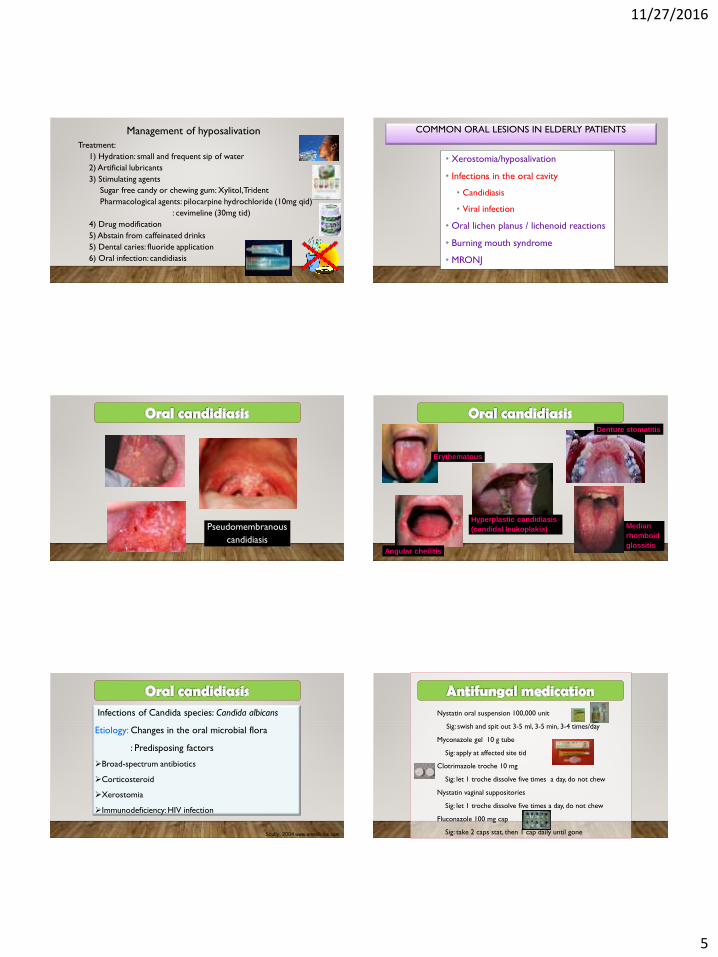
Pseudomembranous
candidiasis
Denture stomatitis
Angular cheilitis
Median
rhomboid
glossitis
Erythematous
Hyperplastic candidiasis
(candidal leukoplakia)
Infections of Candida species: Candida albicans
Etiology: Changes in the oral microbial flora
: Predisposing factors
Broad-spectrum antibiotics
Corticosteroid
Xerostomia
Immunodeficiency: HIV infection
Scully, 2004 www.emedicine.com
Nystatin oral suspension 100,000 unit
Sig: swish and spit out 3-5 ml, 3-5 min, 3-4 times/day
Myconazole gel 10 g tube
Sig: apply at affected site tid
Clotrimazole troche 10 mg
Sig: let 1 troche dissolve five times a day, do not chew
Nystatin vaginal suppositories
Sig: let 1 troche dissolve five times a day, do not chew
Fluconazole 100 mg cap
Sig: take 2 caps stat, then 1 cap daily until gone

11/27/2016
6
Herpes simplex virus infection
Recurrent HSV infection
Herpes labialis
Intra-oral recurrent HSV infection
Keys: Keratinized mucosa
Non-movable mucosa
Attached gingiva
Palate
Multiple small vesicles
or ulcers
Herpes simplex virus infectionSystemic antiviral drugs
CDC recommended regimens
Acyclovir(Zovirax®)
Famciclovir(Famvir®)
Valacyclovir(Valtrex®)
Primary episode 400 mg tid, or200 mg 5 times a day (7-10 days)
250 mg tid(7-10 days)
1 g bid(7-10 days)
Recurrences 400 mg tid, or200 mg 5 times a day, or800 mg bid (5 days)
125 mg bid(5 days)
500 mg bid(5 days)
Suppression(prophylaxis)
400 mg bid(Daily)
250 mg bid(Daily)
500 mg, or 1000mg qd(Daily)
(CDC: sexually transmitted diseases guidelines 2002)

11/27/2016
7
Topical antiviral drugs
Acyclovir cream 5% (1 g or 5 g tube)
Sig: Apply at affected site 5 times a day
วา่นพญายอ ครมี
Sig: Apply at affected site 5 times a day
วา่นพญายอ ใน กลเีซอรนี
Sig: Apply at affected site 5 times a day
• Xerostomia/hyposalivation
• Infections in the oral cavity
• Candidiasis
• Viral infection
• Oral lichen planus/ lichenoid reactions
• Burning mouth syndrome
• MRONJ
COMMON ORAL LESIONS IN ELDERLY PATIENTS
Lace-like white lesions
1) Oral lichen planus
2) Oral lichenoid contact reaction
3) Oral lichenoid drug reaction
4) Chronic GVHD
5) Hepatitis C virus infection
T cells medicated disease which induced the destruction of basal cells
Etiology
Lichen planusLichenoid drug
reactionLichenoid contact
reaction
No history of fillings, medication
History of medication:
HTNDM
DyslipidemiaAntibioticsAllopurinol
Adjacent to amalgam filling, full
metal crown, PFM crown,
Implant
History Lichen planus
11/27/2016
8
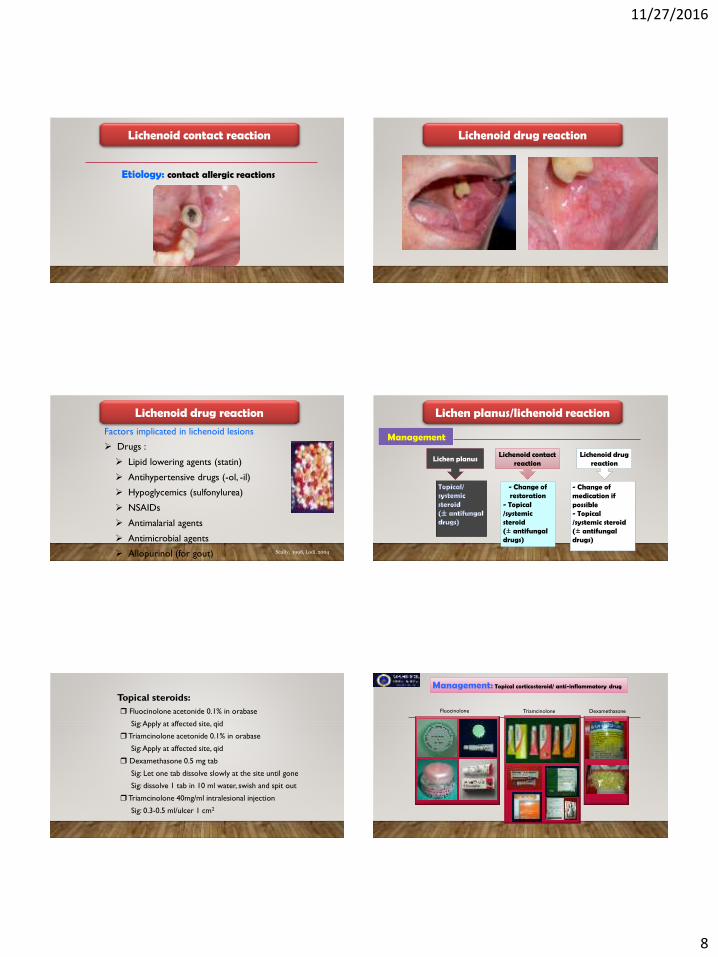
Etiology: contact allergic reactions
Lichenoid contact reaction Lichenoid drug reaction
Factors implicated in lichenoid lesions
Drugs :
Lipid lowering agents (statin)
Antihypertensive drugs (-ol, -il)
Hypoglycemics (sulfonylurea)
NSAIDs
Antimalarial agents
Antimicrobial agents
Allopurinol (for gout) Scully, 1998, Lodi, 2004
Lichenoid drug reaction
Management
Lichen planus/lichenoid reaction
Lichen planusLichenoid drug
reactionLichenoid contact
reaction
- Change of medication if possible- Topical/systemic steroid (± antifungal drugs)
- Change of restoration
- Topical/systemic steroid(± antifungal drugs)
Topical steroids:
Fluocinolone acetonide 0.1% in orabase
Sig: Apply at affected site, qid
Triamcinolone acetonide 0.1% in orabase
Sig: Apply at affected site, qid
Dexamethasone 0.5 mg tab
Sig: Let one tab dissolve slowly at the site until gone
Sig: dissolve 1 tab in 10 ml water, swish and spit out
Triamcinolone 40mg/ml intralesional injection
Sig: 0.3-0.5 ml/ulcer 1 cm2
Management: Topical corticosteroid/ anti-inflammatory drug
Fluocinolone Triamcinolone Dexamethasone
11/27/2016
9
• Xerostomia/hyposalivation
• Infections in the oral cavity
• Candidiasis
• Viral infection
• Oral lichen planus/ lichenoid reactions
• Burning mouth syndrome
• MRONJ
COMMON ORAL LESIONS IN ELDERLY PATIENTS
“Burning pain in the tongue or other oral
mucous membranes with the absence of
pathologic lesions or abnormal laboratory
findings”
Grushka M, et al., 2003
Definition
Primary burning mouth syndrome
Burning sensation without abnormal
clinical findings
Secondary burning mouth syndrome
Burning sensation with systemic or
local abnormalities
Lamey PJ and Lamb AB, 1988
Female, postmenopausal women with mean age of 50-60
years
Feeling discomfort without any clinical abnormal findings
Feeling discomfort after delivery of dental prosthesis
Mostly presented with metal placement: full metal crown,
RPD
Grushka M, et al., 2003
Etiologic factorsLOCAL• Dry mouth (salivary gland hypofunction)• Candidal infection• Denture related oral lesion• Parafunctional habits: clenching, bruxism
SYSTEMIC• Hematologic deficiencies• Endocrine: hormonal change (menopause), diabetes• Medications
PSYCHOLOGIC• Anxiety• Depression• Compulsive disorders• Cancerophobia
Lauren L, et al., 2007

11/27/2016
10
Lauren L, et al., 2007
Pharmacological therapy
Anxiolytics, antidepressant, anticonvulsants, antipsychotics
Non-pharmacological therapy
Psychological therapy, LASER, herbs, acupuncture
Combined pharmacological therapy and psychological therapy
Type Drug Dose Evidence based for use
Anxiolytic Clonazepam 0.25-2.5mg/day- Double-blind, RCT- Open-label, pilot study- Retrospective, pilot study
Tricyclic antidepressants
Amitriptyline 10-150 mg/day - Single-blind, RCT
Nortriptyline 10-75 mg/day- No published evidence for it in BMS but it is used generally for neuropathic pain
Selective serotonin
reuptake inhibitors
(SSRIs)
Paroxetine 10-20 mg/day
- Single-blind, RCT - Single-blind, RCT (no placebo)- Open-label, non-comparative,
prospective study
Sertraline 50-100 mg/day - Single-blind, RCT (no placebo)
Pharmacological therapy
Dentist’s concern:
If the patient has burning
sensation or discomfort without
concomitant clinical findings
BMS should be considered
Referral to oral medicine specialist may be necessary
11/27/2016
11
• Xerostomia/hyposalivation
• Infections in the oral cavity
• Candidiasis
• Viral infection
• Oral lichen planus/ lichenoid reactions
• Burning mouth syndrome
• MRONJ
COMMON ORAL LESIONS IN ELDERLY PATIENTS
History of osteoporosis, long term systemic steroid, solid
organ malignancies with the use of bisphosphonate or
denosumab
Management: debridement, long-term antibiotics, surgery
Symptoms: chronic non-healing ulcer with bone exposure
may be associated with pain and swelling
Signs: bone sequestrum, infection, often found on palatal
area especially on torus palatinus
Current or previous treatment with
a bisphosphonate or denosumab
Exposed bone in the maxillofacial
region that has persisted for more
than 8 weeks
American Association of Oral and Maxillofacial Surgeons, 2014
No history of radiation therapy to
the jaws.
Extensively used in medicine via 2 routes
Oral
bisphosphonates
Intravenous
bisphosphonates
Non-nitrogen containing
• Etidronate (Didronel) 1-10
• Clodronate (Bonefos) 1-10*
• Tiludronate (Skelid) 50
Nitrogen containing (aminobisphosphonates)
• Pamidronate (Aredia) 100-1000
• Alendronate (Fosamax) 500-1000
• Ibandronate (Boniva) 100-1000
• Risedronate (Actonel) 100-2000
• Zoledronic acid 1000-10000
(Zometa 4 mg, Reclast 5 mg)
Half life is approximately 10 years

11/27/2016
12
Non-nitrogen containing
• Etidronate (Didronel) 1-10
• Clodronate (Bonefos) 1-10*
• Tiludronate (Skelid) 50
Nitrogen containing (aminobisphosphonates)
• Pamidronate (Aredia) 100-1000
• Alendronate (Fosamax) 500-1000
• Ibandronate (Boniva) 100-1000
• Risedronate (Actonel) 100-2000
• Zoledronic acid 1000-10000
(Zometa 4 mg, Reclast 5 mg)
Half life is approximately 10 years
Fosamax, Boniva, Actonel, Zometa, Reclast
American Association of Oral and Maxillofacial Surgeons, 2014
I. Drug-related risk factors
• Bisphosphonate potencyIV bisphosphonates > oral bisphosphonates
Nitrogen-containing bisphosphonates > non
nitrogen-containing bisphosphonates
• Duration of therapylonger duration appears to be associated
with increased risk. (>4 years)
II. Local risk factors• Dentoalveolar surgery
Extractions, dental implant placement, periapical surgery,
periodontal surgery involving osseous injury
• Local anatomyTorus palatinus, torus mandibularis, exostosis, sharp
mylohyoid ridges
Can be trauma-induced or spontaneous eruption
Marx RE, 2005
II. Local risk factors• Concomitant oral disease
IV bisphosphonates with a history of
inflammatory dental disease: periodontal and
dental abscesses
Hoff AO, 2006
Badros A, 2006
III. demographic factors• Age
Increasing age
• Race
Caucasians have an increased risk for MRONJ
compared with blacks
Corticosteroid therapy, diabetes, smoking,
alcohol use, poor oral hygiene
IV. Other factors
Badros A, 2006
Thickening of lamina dura Narrowing of inferior alveolar canal
Unremodeled bone in socket
11/27/2016
13
Dentist’s concern:• If the patient has bone
exposure, MRONJ should be considered
• Patient’s medical history is important
• Surgical removal of bone necrosis may be done with caution.
• Referral to oral surgeon may be necessary
ACKNOWLEDGEMENT
•Ministry of Public Health
•Anandamahidol Foundation
• Faculty of Dentistry, Mahidol University