pmdc forensic
TRANSCRIPT

SECTION 6: FORENSIC MEDICINE
================================================
Written by:
Dr. Rana Faizan Ali
M.B.B.S (Dali University, Yunnan, P.R China)
PM&DC (I,II,III)
Javairia Zulfiqar
M.B.B.S (Dali University, Yunnan, P.R China)
Interne
Revised by:
Dr. Muhammad Shoaib
M.D (Kyrgyz-Russian Slavic University, Bishkek, Kyrgyzstan)
PM&DC (I,II,III)
=====================================
Forensic Medicine Curriculum given by PMDC for Step 1:
1. Medical Law
2.Traumatology
3. Poisoning
Division of Marks:
2 SEQ = 10 Marks (5 marks for each SEQ)
10 MCQs = 10 Marks (1 mark for each MCQ)
Forensic Medicine SEQs asked in Last 4 PMDC Papers:
Q1: Define Bruises? What is chemical Antidote?
Q2: What is the function of PMDC? What are the privileges of registered Medical
Practitioner?
-----------------------------
Q1: Bomb explosion cause what kind of injury to one's body?
Q2: What kind of duties of doctor while handling poisoning case?
----------------------------
Q1: What information can be inferred from the Fire Arm Injury [5]
Q2: Medical Negligence:
a. Define Medical Negligence? [1]
b. Mention the Types of Medical Negligence? [2.5]
c. Difference between the Civil and Criminal Negligence? [1.5]

-------------------------------
Q1: What is Stab wound?
Q2: What is Professional Misconduct?
MEDICAL LAWS
Adult: A person who has reached age of 18 years (for males) or 16 years (for
females) or who has attained puberty, whichever is earlier.
Authorized Medical Officer: A medical officer or Medical board constituted by
provincial government is called authorized medical officer or board.
Qisas: means punishment by causing similar hurt at the same part of the body of
convict as he has caused to victim.
Diyat: means compensation specified in section 323 payable to heirs of victim by
the offender.
Arsh: means compensation specified in Qisas and Diyat Ordinance paid by the
offender to the victim or his heirs.
Daman: means compensation determined by the court to be paid by the offender
to victim for causing hurt liable to Arsh.
Wali: is legal heir of victim or deceased or victim himself, in case of qatl; wali is
heir of victim or if the victim is unknown then government.
Medical Practitioner: it is the one who possesses a recognized medical
qualification, as defined in Medical council Act.

Laws Relating to Death:
Qatl-i-Amad: to cause death of a person with full intention and with the
knowledge of causing death with full intention of a specific person.
Qatl-i-shibh-i-Amad: Intention is to cause harm but death has occurred, death of
same or any other person by means of a weapon or an act which usually is not
likely to cause death.
Example: Person "A" gives blow on abdomen of "B" and "B" goes into shock and
death occurs. In ordinary course of nature blow is not likely to cause death.
Qatl-i-khata: to cause death or harm, this leads to death without intention by
mistake of act.
Example: Hunter shoots a bird but a man is killed.
Qatl-i-Sabab: to cause death of a person or harm, this leads to death without any
intention by an unlawful act.
Example: "A" digs a pit for some purpose and "B" falls into it while passing over it
and is killed.
Laws Relating to Hurt:
Definition: whosoever causes pain, harm, disease, injury to any person or impairs,
disables, dismembers any organ of body or part of body of a person; without
causing death is said to cause hurt.
Types of Hurt:

1. Itlaf-i-Udw: whosoever dismembers, amputee, severs any limb or organ of
body of another person.
2. Itlaf-i-Salahiyat-i-Udw: whosoever destroys or permanently impairs the
functioning power of an organ of body of another person or causes permanent
disfigurement.
3. Shajjah: causes hurt/injury on head or face of any person which does not
amount to itlaf-i-udw and itlaf-i-salahyiat-i-udw.
Types of shajjah:
a) Shajjah-i-Khafifah: bone is not exposed by injury.
b) Shajjah-i-Mudiah: bone is exposed without fracture.
c) Shajjah-i-Hashimah: bone is exposed and also fractured but its end is not
displaced.
d) Shajjah-i-munaqqilah: underlying bone is exposed, it is fractured and its end is
displaced.
e) shajjah-i-ammah: underlying bone is fractured and membranes are exposed
but no damage to brain.
f) shajjah-i-damighah: there is fracture of bone of skull, membranes are exposed
and damage to brain.
4. Jurh: whosoever causes hurt on any part of a person other than head and face,
which leaves mark of wound either temporary or permanent.
Allopathic System Ordinance 1962:
Prevention of Misuse:
1. Prohibition of use of word doctor and its abbreviation unless he/she is an RMP
or a person whom a doctor's degree other than a medical degree has been
confirmed.
2. Prohibition of use of medical degree or diploma unless issued by institution
recognized by PMDC.
3. Prohibition of surgical operations by an unqualified person (circumcisions and
injections and abscess drainage can be done)
4. Prohibition of prescription of some drugs (antibiotics) unnecessarily.
5. Restriction on the sale of medicines unless labeled and formula is written on
packing or within packing.
Functions OF PMDC:
1. Supervision of standards of proficiency for registration:
a. Recognition of basic register able medical and dental qualification in and
outside Pakistan.
b. Recognition of additional postgraduate qualification granted in and out of
Pakistan.
c. Power of having detailed information of courses of study and methods of
examination of all those institutes whose qualification is recognized.
d. Power of appointing inspectors to check the standards of teaching and
examination.
2. Maintenance of official register of medical and dental practitioners:
There are 3 parts of PMDC register:
Part 1: Provisional registration for one year. it continues till the members goes on
paying fee.
Part 2: Registration after completing MBBS.
Part 3: Registration for higher Post graduates degree this is open for public for
their interest.
3. To take disciplinary measures
There are 3 punishments:
-Warning
-Temporary removal of name from PMDC registers.
- Permanent removal of name from PMDC registers.
Appeal against PMDC decisions are made only in High Courts.
Privileges of an R.M.P (Registered Medical Practitioner):
Employment: no one other than RMP should be competent to hold dental or
medical appointment in civil or military.
Medical Certificate: no medical certificate should be valid unless signed by RMP
giving his registration number.
Fee for attendance: no person other than RMP should be entitled to charge fee
for professional services.
Dangerous Drug Prescription: only RMP can prescribe drugs of addiction.

Obligations of an RMP:
1. RMP must notify the change of his or her address to PMDC in 30 days.
2. RMP must not use any
-Name
-Title
-Symbol
-Any other qualification that is not in notice of PMDC.
Medical Ethics: It means the normal principles which should guide the
members of Medical profession in course of their practice & their dealing with
their patients and other members of profession.
The Geneva Declaration (1948):
The world medical association at its 3rd general assembly at Geneva in September
1948 adopted certain codes of ethics in the form of Oath to be taken by all
Members of medical profession, at the time of entering into medical profession.
Hippocratic code:
1. I solemnly pledge myself to devote my life to service of humanity
2. I will give my teachers due respect and gratitude.
3. I will serve my profession with devotion and dignity.
4. Health of my patient will be my first priority.

5. I will respect secrets which are confined in me.
6. I will maintain the honor and noble traditions of medical profession.
7. My colleagues will be my brothers except.
8. I will not permit consideration of religion, nationality to intervene between my
duty and my patients.
9. I will maintain utmost respect for human life from time of conception till birth.
10. Even under threat i will not use my medical knowledge contrary to the laws of
humanity.
Duties of a Doctor:
-what a doctor must do?
-what a doctor must not do?
Duties in General: a doctor must have always maintained the highest standards of
professional conduct. Doctor should not practice by motives of profit. Following
practices are unethical:
1. Self advertisement.
2. Connection with non-qualified person.
3. Receiving any money from patient other than fee.
4. Any abuse of his skills etc.
Doctor-Patient Relationship:
1. A doctor must be decent and co-operative with patient.
2. Complete loyalty to patient.
3. Preservation of absolute secrecy.
4. Emergency care as a humanitarian duty.
Doctor-Doctor Relationship:
Basis of Doctor-Doctor relationship is
1. Cooperation
2. Understanding
3. Avoiding of Professional Jealousy.
Professional Secrecy: It is an implied term of contract between the doctor
& his patient. The doctor is obliged to keep secret; all that he comes to know
regarding the patient during treatment.
Following Points May Be Noted:
Should not disclose illness of his patient with or without consent of the patient.
In divorce cases, no information should be given without the consent of client.
In case of reporting medical journals, patients identity should not be disclose.
In case of examining dead body, certain facts found, the disclosure of which may affect the reputation of the decreased or may cause mental suffering to relatives in such cases doctors should maintain secrecy.
Professional/Medical Negligence: Absence of reasonable care and skill,
or willful negligence of a medical practitioner in the treatment of a patient, which causes injury or death of the patient.
Types:
1. Civil Negligence. 2. Criminal Negligence. 3. Contributory Negligence
4. 3rd Party Negligence
1. Civil Negligence: It is a failure to apply reasonable degree of skill and care by
medical practitioner while treating his patient, and responsibility or burden lies on
the Patient. Cases are dealt with civil courts.
Examples are: -Failure to give ALTS in injury cases.
-Failure to give X-rays to doctor in cases of injury to bones or joints in which there
is doubt about diagnosis.
-Excessive exposure of patient to radiation.
-Insufficient care while using dangerous drugs.
2. Criminal Negligence: When a doctor while treating the patient behaves in a
wicked manner showing complete disgrace and disregard for safety of patient's
life resulting into death of patient. He has committed criminal negligence. Such
cases are dealt with criminal courts.
Examples are: -Injecting anesthetic in fatal dose or in wrong tissue.
-Amputation of wrong finger, wrong limb or removal of wrong organ.
-Leaving sponges or instruments in abdomen.
-Giving wrong blood.

-Gangrene after tight plasters.
3. Contributory Negligence: It is defined as concurrent negligence by both patient
and doctor.
4. 3rd Party Negligence: This is done by paramedical staff, nurses, and medical
students, here doctor shares the responsibility, as he is respondent superior.
Cases dealt with civil courts.
Precautions against Negligence:
-Diagnosis where possible confirmed by laboratory tests including biopsy.
-X-rays should be routinely advised in case of injury of bones or joints or where
diagnosis is doubtful.
-Consultation with a specialist should be suggested in obscure cases.
-Immunization should be considered a necessity where there is danger of
infection.
- Sensitivity should be done before injecting preparations likely to cause
anaphylactic shock.
-No experimental procedure should be done without prior consent.
-No procedure should be undertaken beyond one's skills.
Res Ipsa Loquitur: The professional negligence of a doctor must be proved in
court by the expert, evidence of another doctor.
Examples:
1. Fail to give anti-titanic serum in case of injury causing tetanus. 2. Burn by x ray therapy. 3. Prescribing over dose of medicine causing ill effect.

4. Failure to remove swab from abdominal cavity during operation which may leads to complication or even death. SWAB– Cotton or piece of cloth used to clean the abdomen.
Euthansia (Mercy Killing): “Producing painful death of a person suffering
from hopeless, incurable & painful disease.”
Types of Euthansia:
1. Active: Act of commission; means giving large dose of drugs. 2. Passive: Act of omission; means discontinuing or not using life sustaining
measures like removal of ventilator, resuscitation. 3. Voluntary: At the will of patient. 4. Involuntary: Against the will of the patient, when person is incapable of
making decision, like irreversible coma. 5.
Consent: Means voluntary agreement, compliance or permission.
Types of Consent:
1. Expression:
a- verbal, b- written
2. Implied/ Informed:
Put his arm in front of you so you can inject etc.
Rules of Consent:
1- Consent is necessary for every medical examination.
2-Oral consent should be in presence of 3rd party, like nurse.
3-Expressed consent required, if any procedure done beyond routine physical
examination, like blood transfusion, operation.
TRAUMATOLOGY

Traumatology: it is knowledge of trauma or injury.
Trauma: it is illegal harm to any person in body, mind, repute or property.
In Body: Physical Trauma
In Mind: Psychological Trauma
Wound: it is discontinuation or disruption of any tissue of body, every wound is
trauma but every trauma is not wound as trauma can be to mind, repute or
property.
Hurt: is bodily pain, disease or infirmity caused to any Person!
Assault: is to threat or attempt to apply force.
Battery: actual application of force.
Homicide: Killing of a human by conduct of another.
Suicide: is self-murder. It is an unlawful act.
Accident: event neither expected nor desired or designed.
Classification of Injuries:
1. Mechanical injuries by physical violence.
2. Thermal injuries by heat or cold.
3. Chemical injuries
4. Electrical injuries
5. Firearm injuries

1. MECHANICAL INJURIES:
The injuries inflicted by mechanical force are generally divided into those caused
by blunt force and those due to sharp force. Injuries may be single or multiple.
There may be more than one type of skin injury to the body and they may be
localized or widespread. The effects of the injury on the body may be local (e.g. a
bruise on the breast), systemic (e.g. shock following a stabbed blood vessel in the
leg) or as a result of complications (e.g. kidney failure due to shock and infection).
It should be noted however, that the absence of external injury to the skin or
genitalia does not exclude the possibility of serious injury to the internal organs.
Bruises or Contusions: A bruise is an area of skin discoloration. A bruise occurs
when small blood vessels break and leak their contents into the soft tissue
beneath the skin. In bruise external surface may remain intact, only subcutaneous
surface is involved.
Factor modifying appearances of bruises are:
1. Vascularity: greater the vascularity greater will be the size of bruise.
2. Force: greater the striking force greater will be the bruise.
3. Age: old age people bruise easily.
4. Sex: females especially obese one bruises easily
5. Area: bony sites and lax skin bruise easily, while abdominal wall and scalp
does not bruise easily. Scalp of newborn bruise easily.
6. Texture: thin and delicate skin bruise easily.
7. Physical condition: Obese and unhealthy persons bruise easily.
8. Diseases: persons with coagulation disorders, liver and renal failure bruises
easily.
9. Complexion: bruises are well marked on persons with fair complexion.

10. Blisters: due to oblique blow or fractures of underlying bone blisters are
formed over bruise.
Age of Bruise:
Color changes:
1st day: red
2nd day: violet
3rd day: bluish black
4th day: livid red
5-6th day: greenish
8-12th day: yellowish
13-15th day: normal
There are no bluish or greenish stages in subconjunctival hemorrhage.
Medico legal Aspects:
1. identification of objects causing injury
2. degree of violence
3. time of injury
4. Purpose of injury: around neck=throttling, around nose and
mouth=smothering, on arms and face=sign of struggle, on
inner aspects of thighs and genitalia=sexual offence.
5. Is bruise true or false
6. is injury suicidal, homicidal or accidental

Antemortem Bruise Postmortem Bruise
1. Swelling is also seen No swelling
2. Color changes are seen No color changes
3. Epithelium abraded Not so
4. Margins-not shard and well define Sharp and well defined
5. It can be anywhere Occur only 2 hours after death.
True Bruise False Bruise
1. Color changes are seen No color changes
2. Margins are well defined Not defined
3. Swelling is seen No swelling
4. Extravasation of Blood Not present
5. Blood Coagulation No coagulation
6. Occur on any part Only at accessible is seen
7. No itching Itching is present
8. Area is not corroded Irritation corrosion present
9. Chemical tests are negative Positive
10. Blood is present in true bruise Serum is present in false bruise
Abrasion: An abrasion is a superficial injury to the skin in which the outer layer of
the skin is scraped off.

Examples include a scratch from a fingernail, imprint caused by a belt buckle,
grazing of the skin caused by dragging the body over a rough surface and the
impression around the neck caused by a cord or rope used in strangulation.
Abrasions allow inferences to be drawn about the nature and shape of the object
(e.g. a belt buckle); the time of the injury (e.g. recent or healed); the type of the
assault (e.g. abrasions on the neck and genitalia in rape strangulation); and the
cause and mechanism of death (e.g. strangulation)
Lacerations: A laceration is a wound with irregular edges which results from the
application of blunt force which causes tearing or splitting of the skin. Lacerations
also allow inferences to be drawn about the nature and shape of the object; the
time of the injury (e.g. recent, healing or healed); and the cause and mechanism
of death (e.g. head injury caused by beating with a stick)
Incised wounds (cuts): An incised wound is a superficial wound in which the size
of the wound on the surface is larger than the depth of the wound (e.g. wound
caused by a razor blade).
Hesitation or Tentative Cuts: These refer to preliminary cuts made by a person
intending to commit suicide by a cutting instrument- before gathering courage to
make a final incision.
There are: Small, multiple, superficial, merge with main incision, if wound tails
towards right person is right handed, if wound tails towards left person is left
handed.
Medico legal Aspect:
Homicidal are deep and on any part of the body but suicidal are many and on
accessible parts of the body.

Stab/Penetrating incised wounds: In a penetrating incised wound the depth of
the wound is greater than the surface length of the wound (e.g. stab wound
caused by a dagger).
Characteristics:
Wound of entry: It is bigger than the exit wound, margins of the entry wound are
clear cut and inverted.
Wound of exit: it is smaller than the entry wound, margins are averted, it is seen
in perforating not penetrating stab wounds.
Fabricated/Self inflicted/Self suffered Wound: Wound produced by a person on
his own body or caused by another person in agreement with him (self suffered)
Objectives:
2. To support false charge
3. To escape military service
4. To destroy evidence of certain injury
5. To show self defense
It is revealed by careful examination. Examination of clothes is very important.
These injuries are on assessable parts of body, half heatedly inflicted and not on
vital parts.
Defense Wounds: Wounds sustained by a person as a result of his spontaneous
reaction to protect himself, when attacked.
Causes of Death from wounds:
Primary or intermediate causes: Secondary or indirect causes:
Excessive bleeding Infection

Injury to vital organs Thrombosis
Neurogenic shock Secondary shock Embolism Supervention of new disease
Crush syndrome Acceleration of preexisting disease Operational disorders
Neglect of patient
Indirect effect
Age of wound:
Naked eye examination:
6. Abrasion
7. Bruise
8. Aseptic wound
- Edges are red and swollen 12 hours
- Scab formation 12-24 hours
- Epithelium begins to grow 24-36 hours
- Complete epithelial growth 4-7days
- Scab goes off 8-10days
9. Septic wound
-Edges red and swollen 12-24 hours
-Pus is formed 36 hours
-Granulation tissue is seen 7 days
Antemortem wounds: Postmortem wounds:
Free hemorrhage (mainly arterial) Slight hemorrhage (venous)
Blood clot is firm, yellow, can be pealed in layers, composed of fibrin and anti platelets
Blood clots after 4-5 hours and is dark, cannot b pealed, composed of fibrin and RBCs
Washing cannot remove staining Staining is removed by washing
Vital reactions are seen Not seen
Increased histamine and serotonin secretion
Not seen
Leukocytes and RBCs infiltrate in between muscle fibers.
No infiltrates.
2. THERMAL INJURIES:
Tissue injury resulting from the application of excessive heat and cold is called
thermal injury.
Cold: Exposure to cold produces hypothermia which is defined as temperature
less than 35 degree C. The body can tolerate dry cold much better than wet cold,
as wetness increases heat loss considerably.
The localized effects of cold are frost bite, trench foot and immersion foot.
Trench foot and immersion foot are result of prolonged exposure to severe cold
(5-8 degree C), typically seen in soldiers during winter warfare, especially in
trenches and in person exposure to prolonged immersion.
Frost bite occurs due to exposure to greater extremes of cold (-2.5 degree C),
develops more rapidly.
Heat:
Heat cramps: Caused by rapid dehydration of body through the loss of water and
salt in the sweat.
It is seen in workers in high temperature when sweating has been profuse. Severe
and painful paroxysmal cramps affecting the muscles of arms, legs and abdomen
occurs.
Heat stroke: It is a condition when rectal temperature greater than 41 degree C,
occurs when there has been direct exposure to the sun.

Heat Exhaustion: It is a condition of collapse without increase in body
temperature, which follows exposure to excessive heat.
It is precipitated by muscular work and unsuitable clothing. There is extreme
exhaustion and peripheral vascular collapse.
The patient feels suddenly weak, giddy and sick.
Burns: A burn is an injury which is caused by application of heat or chemical
substances to the surfaces of the body, which causes destruction of the tissues.
Causes of burn:
Dry heat: Flame and heated solids
Radiant heat
Friction
Corrosive chemicals: Solid and liquid
Lightning
Electric current
X-rays
Ultra-violet or infra-red light rays
Varieties of burns:
-Most chemicals that can cause moderate to severe chemical burns are strong
acids or bases (such as sulfuric acid and Nitric acid). Hydro sulfuric acid can cause
damage down to the bone and its burns are sometimes not immediately evident.
-Electrical burns: electric shock such injuries may lead to cardiac arrhythmias,
cardiac arrest, and unexpected falls with resultant fractures.

-Burns produced by flame may or may not produce vesiculation, but singeing of
the hair and blackening of the skin are always present.
-Radiation burns may be caused by over-exposure to UV light and X-rays. Burns
due to X-ray and radium vary from redness of the skin to dermatitis, with
shedding of hair and epidermis and pigmentation of the surrounding skin. Severe
exposure may produce burns with erythema, blistering with delayed healing and
ill-formed scars.
-Burns from corrosive substances show ulcerated patches and are usually free
from blisters, and hair is not singed
Classification of Burns:
Burns are often categorized as first-, second-, or third-degree burns, depending
on how badly the skin is damaged.
First-degree burns: burns affect only the outer layer of the skin.
They cause pain, redness, and swelling. The skin is dry without blisters.
Healing time: Healing time is about 3 to 6 days; the superficial skin layer over the
burn may peel off in 1 or 2 days.
Second-degree burns: (partial thickness) burns affect both the outer and
underlying layer of skin. They cause pain, redness, swelling, and blistering.
Healing time: Healing time varies depending on the severity of the burn.
Third-degree burns: (full thickness) burns extend into deeper tissues. They cause
white or blackened, charred skin.
There may be little or no pain or the area may feel numb at first because of nerve
damage.
Healing time: Healing time depends on the severity of the burn. Deep second- and
third-degree burns (called full-thickness burns) will likely need to be treated with
skin grafts, in which healthy skin is taken from another part of the body and
surgically placed over the burn wound to help the area heal.
Wilson classification of Burns:
1st degree: Reddening and blistering of skin only
2nd degree: Charring and destruction of full thickness of skin
3rd degree: Charring of the tissues beneath the skin e.g. fats, muscle and
bones.
Dupuytren classification of Burns (Old surgical):
1st degree: Reddening of skin
2nd degree: Blistering
3rd degree: Skin partly destroyed
4th degree: Skin completely destroyed
5th degree: Subcutaneous tissues burnt
6th degree: Muscles and bones charred.
Estimation of the surface area of the body:
Can be estimated by “RULES OF NINE”
According to ‘Rules of Nine’, percentage of area attributed to different
parts of the body is as follows:
-Head and Neck: 9% of the whole body area
-Front of chest: 9% of the whole body area
-Back of chest: 9% of the whole body area
-Front of abdomen: 9% of the whole body area
-Back of abdomen: 9% of the whole body area
-Right upper limb: 9% of the whole body area
-Left upper limb: 9% of the whole body area
-Front of left lower limb: 9% of the whole body area
-Back of left lower limb: 9% of the whole body area
-Front of right lower limb: 9% of the whole body area
-Back of right lower limb: 9% of the whole body area

-Genitalia: 1% of the whole body area
TOTAL: 100%
Involvement of more than 30% of the body surface area is dangerous. But
50% involvement of body surface area is fatal
Causes of death in burns:
Shock: due to pain and fright (Neurogenic/Hypo-volemic) (death within 24-48hrs)
Suffocation: due to inhalation of smoke of gases(death within1-2days)
Toxemia: due to absorption of various metabolites from burnt tissue
Infection and Sepsis: tetanus, also (pseudomonas & streptococci are usual), death
within 4-5 days.
Renal failure and Mechanical injuries.
GI disturbances, such as acute peptic ulceration, dilation of stomach,
hemorrhages into intestines.
Edema of glottis and pulmonary edema due to inhalation of smoke containing CO
and carbon dioxide
Post mortem appearances:
A. External: Examination of clothing for the evidence of kerosene, petrol or any
other substance.
The appearance of the skin could vary as
i. white: Burns due to radiant heat
ii. Blackening of skin and singeing of hairs: Burns due to flame
iii. Blisters and reddening: Depending upon the size of highly heated
objects
iv. Blackening and tattooing: Due to coal mine explosions and gun powder
v. Pugilistic attitude: if the body is exposed to great heat for long durations

vi. Black spots: Kerosene burn.
vii. Heat ruptures: In some cases extreme heat may result in cracks and
fissures resembling incised wound.
In case of inhalation: Discharge of blood mixed secretion due to rupture of
capillaries.
B. Internal: Heat hematoma occurs when the head has been exposed to intense
heat and skull bones are charred. It is soft clot of light chocolate color and
resembles honey comb appearance.
Fracture of skull bones if death occurs from burns.
The brain is usually shrunken, firm and yellow to brown.
Coal particles can be traced in the respiratory tract, if death occurs from
suffocation. (Carbon soot)
Stomach and duodenum show inflammatory reaction with ulcers. (curling ulcers)
Blood shows cherry red in color.
Spleen and adrenal gland are congested.
Rupture of fatty cells may cause fat emboli.
Various visceral organs may be burnt with fractures of bones.
Burns activates coagulation mechanism and produces thrombosis especially in
coronary arteries.
Age of burns:
Redness: Immediate
Vesication: 2-3 hours
Pus formation: within weeks
Appearance of red granulating surface without any slough: 2 weeks
Medico-legal aspects of burn:

Accident: Large numbers of deaths are accidental.
Suicide: Occasionally, women commit suicide by pouring kerosene on their cloths
before setting fire to themselves due to domestic worries. Extensive burns are
seen over the whole of the body.
Homicide: It is rare; a drunken man may push or throw his wife or child on the
fire.
Scalds: A scald is a type of burn injury caused by hot liquids or vapors or
steams. In scalds singeing of hair, charring of skin, Burning of clothes does-not
occurs. Healing of small scalds is complete by 7-10 days with formation of
temporary scars.
Mostly are accidental in nature and sometimes are homicidal.
Degrees of scalds
-Erythema of skin.
-Blisters formation due to increased permeability of the capillaries.(within
2-3 minutes) .
-Necrosis of the dermis.
Occurrence: Scalds are usually accidental due to bursting of hot water bottles,
bursting of boilers, splashing of fluid from cooking utensils, or pulling over
saucepans or kettles by children.
Post mortem appearance of scalds:
Externally the body will show extensive blisters or ruptured blisters with ante
mortem reaction, in long standing cases, there may be ulcer formation due to
infection
If death has occurred due to swallowing of hot liquid or inhalation of hot vapor,
signs of gross irritation, edema and blister formation will be present inside the
mouth and near the larynx.
Grievous hurt: Grievous hurt is one which endangers life or which causes the
victim to be in severe bodily pain or unable to follow an ordinary pursuits for a
period of twenty days. The following injuries are grievous hurt.
i. Emasculation (loss of masculine power of a male. This includes excision,
injury of vertebral column leading to failure of erection)
ii. Permanent privation of sight of either eye
iii. Permanent privation of hearing of either ear.
iv. Privation of any member or joint: It includes eyes, ears, nose, mouth,
hands, feet etc.
v. Destruction or permanent impairing of the power of any member or
joint: The use of limbs and joints of the body are very essential for the
normal functions of the body, their deprivation causes lifelong crippling and
makes the person defense-less and miserable.
vi. Permanent disfiguration of the head or face: such as permanent scars
amount to disfigurement.
vii. Fracture or dislocation of a bone or tooth.
viii. Any hurt which endangers life or which causes the victim to be severe
bodily pain, or unable to follow his ordinary pursuits for a period of 20 days.
3. CHEMICAL INJURIES:
Injuries produced by the action of chemicals on body like acids and alkalis. These
also include vitriolage (throwing of acids on face). There is damage at the site of
application and below (as fluid flows down).
Chemicals may cause ulceration, may eat up the tissue and form cavities, color of
the affected part may tell us about the used chemical.
Black= H2SO4
Yellow= HNO3
White to Yellow= HCl
By the action of acids or alkalis tissues may be coagulated, dried, shrunken hard,
shriveled necrosed etc. Alkalis mostly cause liquefaction of tissues. Other
chemicals like castor oil seeds are vesicants they cause vesications, if contact
duration is deeper tissues are also involved.
Chemical Burns:
Superficial burns: only superficial tissues are involved and contact is short.
Deep burns: contact time is prolonged and deeper tissues are involved.
Death in Burns:
-Shock: Pain-Neurogenic shock
Fear-Psychogenic shock
Complications- Hypovolemic shock
-Suffocation by gases like carbon mono oxide, carbon di oxide and fumes of
the chemicals
-Inflammation
-Toxemia
Objectives to be obtained:
a. Identification of person.
b. Burns are either antemortem or postmortem, in
case of antemortem vital reaction is seen, red line
at the base of blister, repair signs, scar, scab,
granulations etc.
c. Determine cause of death is it burns or something
else.
d. Mode of death
e. Look at the clothes and identify the smell.
f. Look for the levels of co, co2, in the blood.

g. Have a look at the state of heart.
h. Look at the color of hypostasis.
i. Types of burns
j. Age of burn: immediate=red, 1hr=vesications, 2-
3days=pus, 4-6days=scab
4. ELECTRICAL INJURIES:
Includes death from electricity, lightening and radiation.
Electricity: Electricity is a form of energy produced by the movement of electrons.
Under certain circumstances can injure the body and cause death.
Sources of electrocution:
Domestic sources
Industrial, commercial centers and transport system
Electricity distribution system
Lightening
Electrical injuries: An electrical injury occurs when a current passes through the
body, interfering with the function of an internal organ or sometimes burning
tissue.
Electrical injury may result from contact with faulty electrical appliances or
machinery or inadvertent contact with household wiring or electrical power lines.
Electrical injury can also occur from lightning.
The maximum amount of current passes through the blood vessels.
The current flow adopts the shortest route to the earth, to be neutralized in the
earth.

Features of electrocution:
-Lesion at the site of entrance in the body:
There will be crater formation (due to resistance offered by the skin), which is
tough on palpation and the margin is raised with the depressed floor.
There will be cracking of the skin.
The site of entrance has a metallic luster (due to atomization of metallic electric
wires) If it is high voltage current then burning of tissues, blackening and charring
may be seen.
-Lesion at the site of exit from the body:
Common at the bare soles, The tissues may be rupture giving deep laceration like
appearance. Due to heat production, burning may be seen.
-General features:
Moment of electrocution is painless.
Tingling and numbness is felt.
Severe involuntary muscular contractions, seizures, ventricular fibrillation, or
respiratory arrest due to CNS damage or muscle paralysis may occur.
Cardiac arrest may occur without burns in bathtub accidents (when a wet person
contacts a 110-V circuit—e.g. from a hairdryer or radio).
Suspended animation like state may be observed for a short period.
Unconsciousness, mental confusion, partial deafness, defective vision,
incontinence of urine may be seen.
Cause of death due to electrocution:

Ventricular fibrillation, if the current is of low voltage
Inhibition of the respiratory centers in the medulla, if the current is of high
voltage
May cause both fibrillation and respiratory failure, if the current is of high voltage
(220-1000V)
Death from asphyxia due to paralysis of the respiratory muscles.
Secondary causes: Sustaining mechanical injuries, burning effects.
Medico legal aspects:
Death by electric currents is usually accidental from defective electric appliances
or negligence in the use of equipment.
Rarely death may occur during convulsive therapy to mental patients.
Cases of suicide and even homicide may occur.
Lightening Deaths:
A flash of lightning is due to an electric current discharge from thundercloud to
the earth. The electric current is direct with a potential of 100-1000 million volts
or more.
Mode of death in lightening:
-Due to giant spark of high voltage, person falls un-consciously and dies due to
paralyzing effects either on the nervous system or heart or due to effects of burns
and lacerations after some days.
-Instantaneous death is as a result of electrical discharge passing to earth.

-Injuries may occur due to forceful tossing the body with the ground (blast effect)
-Dry skin and dry clothes are bad conductors, whereas wet skin and wet clothes
are good conductors.
-Common cutaneous findings associated with lightning strike include punctuate
full-thickness burns, linear burns, and contact burns from overlying metal objects
(if worn).
-Branching or ferning marks (zig zag) are an uncommon and unusual cutaneous
manifestation. These ferning patterns are called Lichtenberg figures.
These are due to dilatation and rupture of the smaller blood vessels at several
places giving rise to ecchymoses with an arborescent pattern.
Also called filigree marks.
-Some pericardial and sub-endocardial hemorrhages.
-Subserosal and mucosal hemorrhages of the respiratory and GI tracts.
-Fractured bones may be seen.
-If the electric discharge finds its way through the feet, the skin may be
ruptured at the point of exit and the shoes may be torn.
-Involvement of the central nervous system with paralysis of the heart or
the paralysis of the respiratory centre causes death.
Medico legal importance:
-Death is always due to accident. Sometimes, the appearances left on the human
body closely resemble those produced by criminal violence. Thus a person may be
found dead in an open field or on the highway and body may show contusions,
lacerations and fractures.
-In such cases the diagnosis should be based on the history of a thunderstorm in
the locality, evidence of effects of lightning in the vicinity of the body, and fusion
or magnetization of metallic substance.
Precautionary steps to avoid Lightning stroke
Not to go to an open place during lightning.
Not to go on the open roof during lightning.
Not to take shelter under a solitary tree during lightning.
Not to touch a metallic fencing during lightning.
Not to be near an un-arrested telephone wire or antenna during lightning.
Not to handle any inflammable fuel during lightning.
Not to go for a swimming in open space during lightening.
Radiation Injuries: The term radiation includes both electro-magnetic waves of
energy (e.g. radio-waves, visible light and x-rays) and particles emitted from
atoms under certain conditions.
Sources of Radiation exposure:
Natural:
-Cosmic rays.
-Environmental: (a) Terrestrial – Thorium
- Uranium
- Radium
- K 40
(b) Atmospheric – Radon
- Thoron
-Internal- Potassium-40
- Carbon-14
Man Made:

-Medical and dental x-rays, radioisotopes.
-Occupational exposure.
-Nuclear.
-Miscellaneous: Television sets, watch etc.
Nuclear Radiation:
Types of ionizing radiation:
-The term ‘ionizing radiation’ is applied to radiation which has the ability to
penetrate tissues and deposit its energy within them.
-Ionizing radiation may be classified as follows:
1. Electro-magnetic radiations: x-rays, Gamma rays.
2. Corpuscular radiations: Alpha-particles, Beta particles, Protons.
Effects of Radiation:
1. Biologic effects:
I. Somatic:
Immediate: Radiation sickness.
-Acute radiation syndrome.
Delayed: Leukemia.
- Carcinogenesis.
- Fetal developmental abnormalities.
- Shortening of life.
II. Genetic – Chromosome mutation
- Point mutations

2. Acute general effects:
(a)Central nervous system syndrome (Exposure to 10,000 rads or above)
-Intra-ocular pressure.
-Headache.
-Nausea.
-Vomiting.
-Papillo-edema
(b) Gastro-intestinal syndrome (Exposure to above 400 rads)
-Anorexia, Nausea, Vomiting, Loose motion, mucoid stool, Malena (sometime)
(C) Long term or late effects:
(i) High dose, Long term exposure (x-rays, g-rays, UV):
- Cataract.
- Sterility.
(ii) Low dose, Long term exposure exposure (x-rays, g-rays, UV rays):
- Aplastic anemia.
(iii) Long term exposure to beta rays:
- Chronic radio-dermitis.
- Hyper-pigmentation.
- De-pigmentation.
- Atrophy.
- Squamous cell carcinoma.
- Basal cell carcinoma.

(iv) Cancers due to radiation exposure:
- Skin- squamous cell carcinoma and basal cell carcinoma.
- Bone tumour.
- Leukemia.
- Lymphoma.
- Lung cancer.
- Thyroid carcinoma.
(V) Pre-natal radiation effect:
- Various types of congenital deformities.
Acute Radiation Syndrome: A single exposure of a large dose of over 100 rads
penetrating radiation on the whole body within 1 to 2 days, results in a
progressive series of signs and symptoms known as acute radiation syndrome.
The sign and symptoms are as follows:
- Vomiting and Nausea with diarrhea and abdominal pain.
- Headache, erythema of skin and conjunctivitis.
- Loss of hair and fine desquamation of skin.
- Severe hematological damage-aplasia of bone marrow, agranulocytosis,
thrombocytopenia resulting in hematological disturbances.
SPECIAL TRAUMA:
1. FIREARM INJURIES:
Mechanism of firearms:
I. The firearm is actually fired when the trigger is pulled.
II. The trigger has a firing pin or hammer who strikes the percussion cap at
base of the cartridge.
III. The priming of percussion cap is detonated by the striker or firing pin.
IV. The explosion of primer ignites the propellant powder in the cartridge case.
V. This result in evolution of relatively large volume of gases which is under
high pressure.
VI. This volume of gas expands and causes the cartridge case to swell.
VII. Consequently the hold of bullet is released.
VIII. Bullet is forced out of the muzzle with certain of velocity.
IX. The bullet is accompanied by the blast of highly compressed gases, smoke,
flames, particle of partially burnt or unburnt grains of powder, fragments of
metal, grease, wad etc.
Firearm wounds: Every firearm is a punctured wound, with a wound of entrance,
progressing deep inside, presenting the track of bullet and some time making the
wound of exit.
Case of short guns: Up to some distance the pellets make a single path then due
to dispersion of pellets, multiple small wound of entrance are produced around
the main wound of entrance.
-The margin of main wound is very irregular, ragged and inverted.
-Some of the peripheral pellets may just strike the skin without entering the
depth of the tissue.
-Beside this affects of firearm hot gases, smoke, unburnt powder, semi burnt
powder may be found around the wound of entrance.
-Beside this the wad may trailed to a certain distance and makes the abrasions
around the wound of entrance in case of shot from a near distance.
Injuries due to riffled firearms: There is a single punctured wound of entrance. It
travels deep inside the body injuring organs in its tract and sometimes makes a
wound of exit.

Wound of Entrance: The wound of entrance is circular when the bullet strikes the
surface perpendicular. It is oval when the bullet strikes the body at an angle.
-The wound is smaller when the firing is from close range except in contact shots.
It is slightly larger when firing is from long distance.
-There may be some abrasions and contusions of the friction area around wound
of entrance by the bullet, is called as abraded or contused collar.
-Around the abraded or contused collar there is a dirt or grease collar made by a
metallic dust and grease from the surface of the bullet.
-Grease collar should not be confused with corona, which is blackish circular zone
around the wound caused by smoke in case of short from a near distance.
-The wound of entrance is inverted and no protrusion of fat through the wound.
Depth and track of wound:
-After entering the body the bullet may run in a straight course or it may get
reflected and takes a different course due obstruction by the tissue and mostly by
bone splinter from the fractured bone may show different track and separates the
wound of exit.
-The bullet may be lodged inside the bone or organ; some bullets may be
reflected from the bone and may come out from the same wound of entrance.
-If the body covered by cloths, the fabrics torn out may be pushed inside wound
by the bullet.
-If the body covered by cloths, the fabrics torn out may be pushed inside wound
by the bullet.
-In bullet injury there may be less hemorrhage around the wound of entrance
Wound of Exit:
-Exit wounds are larger than the corresponding entrance wounds the skin edge
averted with protrusion of fat through the wound.
-The margin is irregular.
-Hemorrhage is more near the wound of exit.
-When the site of exit wound is in contact with the hard surface like wall then the
margins are abraded, so called as shored exit wounds.
-There may be multiple exit wounds due fragmentation of bullet or emergence of
fractured bone pieces.
Case of skull:
Punched in: wound of entrance.
Punched out: wound of exit.
Special features of bullet wounds:
I. Ricochet Bullet: It is the bullet which by striking the body strikes some hard
surfaces like wall where it get bunched or reflected to take a different track
and then strikes the body of the person.
-Such a deform ricochet bullet causes more extensive wound of the
entrance, but its power of penetration is reduced.
II. Tandem Bullet (Piggy tail Bullet): First bullet which has been stuck inside
the barrel may be fired out when firing the second bullet and both the
bullets will enter the body at the same wound of entrance. When
postmortem is done there may be two bullets with only one wound of
entrance.
III. Dum Dum Bullet: The bullet splits when it strikes the body is called dum
dum bullet.
IV. Presence of more than one bullet in body: It may be tandem bullet. Two
bullets of two rapidly successive firing.
V. Single wound of entrance with more than one wound of exit:
VI. With more than may one wound of entrance there may be one bullet
present in the body: Bullets getting into the arm and exiting from the
medial aspects of arm and again entering the chest with another wound of
entrance.
VII. Multiple wound of entrance with multiple wounds of exit with no bullet
found inside the body: Entering from outer aspects of chest and exiting
from other aspects of chest then entering from medial aspects of arm and
exiting from the lateral aspects of the arm.
VIII. Kennedy Phenomena: When during autopsy it is difficult to distinguish
between firearms entry wound and exit wound.
American president PJK Kennedy sustained injury on neck, bullet entered
from back of neck and exit was from the front through trachea. The exit
wound was of small size difficult to say that was it entry or exit or another
entry from front. In fact the exit wound was small as the tight collar
supported the neck tissue. As he was taken to hospital, attempts were
made to save his life and during surgical manipulation it further became
difficult to distinguish between entry and exit wound.
Medico legal Aspects of Firearm Injuries:
1: Nature of death due to firearm injury:
A= Suicidal:
i. Located more approachable parts of the body.
ii. Usually use of hand rest weapon.
iii. Often the entrance wounds are contact wounds with presence of muzzle
mark around the wound of entrance.

Iv. The gun may be hold in a tight grip( state of cadaveric spasm).
v. Finger prints of a suicidal person may be in the trigger of the firearms.
B= Homicidal:
i. May be at anywhere in the body with contact, near shot or distant shot of
the wound.
ii. May be both short barreled or long barreled guns are used.
iii. The weapons are usually absent at the spot.
iv. Spot may be approachable to others. May be fingerprints of the
assailants (if weapon present at the spot).
C= Accidental:
i. May be due to wrong aiming or missing the target.
ii. May be due to playing with loaded guns or cleaning the loaded guns.
2: The direction of firing:
The direction from where the firearm has been used can be easily
understood from:
i. Finding at the margin of wound of entrance: circular or oval.
ii. From the direction of track of the wound inside the body.
3: Distance of firing:
A= In case of shot gun firing:
i. Presence of fire, smoke, partially burnt or un burnt gun powder.
ii. The disc and wad causing abrasions at the wound of entrance.
iii. the diameter of the area of dispersion of pellets over the body.
iv. Impression of the muzzle in case of contact wounds.
B= In case of bullet injury (rifled guns):
i. Effects of fire, smoke, burnt and un burnt gun powder , when firing is
from short distance.

ii. Wound of entrance smaller, short distance.
iii. Wound of entrance slight bigger, long distance.
iv. Impression of muzzle, contact firing.
4: Identification of firearm weapon used:
This can be done from following;
A- Comparative study of the bullet recovered from the dead body and the
test bullet fired from the suspected guns, two types of markings are usually
available in used bullets.
Primary markings:
They are the marks engraved on the surface of the bullet due to lands and
grooves present on the inner surface of the barrel of the riffled firearms.
Secondary markings:
These marks on the surface of bullets caused due to certain individual
features of the inner surface of the barrel like minor projections or
elevations or depressions which are specific of a particular gun and not
common to all guns even the same make.
B= Examination of the suspected gun:
Evidence of the recent use of the guns can be established by physical and
chemical exam of the swab from the chamber and bore of the guns.
5: Identification of the assailants:
i- Dermal nitrate or paraffin test:
It is a lab test. If nitrogenous material is present when swab of the accused
person’s fingers is taken (diphenylanine)
ii. Harrison and Gilroy’s test:
It is done for lead, antimony or barium if present from the swab of accused
fingers.

Done by spectro-photometery, atomic absorption spectroscopy.
Also by Neutron activation Analysis.
Causes of death in case of firearm injury:
-Hemorrhages.
-Shock injuring vital organs.
-Fats and air embolism.
-Asphyxia.
-Infections.
-Lead poisoning
Souvenir Bullet: A bullet accommodated in the body with healing of injured
tissues around it and in the track of bullet is called as souvenir bullet.
Difference between the wound of entrance and wound of exit:
Entrance Wound Exit Wound
1- Size: smaller 2- Margin: inverted 3- Blackening, burning: present. 4- Abraded or confused and greeze color: present. 5- Foreign fabrics: enters the wound. 6- Hemorrhages: less. 7- Dispersion of pellets in short gun cases: present. 8- Protrusion of fats: absent. 9- Bright redness due to the formation of COHb: present.
1- Larger. 2- Averted. 3- Absent. 4- Absent. 5- Nothing such seen. 6- More. 7- Absent. 8- Present. 9- Absent.
10- Metallic ring shadow on x ray: present. 11- Impression of muzzle: present in contact shot. 12- Bursting effects: present.
10- Absent. 11- Absent. 12- Absent.
2. Blast/Explosion injuries:
These are due to house made bombs, explosions of shells, torpedoes, and mines
etc in wars and as well as in peace and also in cases of terrorism.
Explosion is mainly accompanied by blast waves, flame, fragments, secondary
missiles, fragments of vehicles, and falling buildings.
There definite waves are recognized:
a. Wave of positive pressure.
b. Wave of air displacement.
c. Wave of negative pressure.
Common types of explosives:
Nitroglycerine (40% dynamite)
PETN
TNT (2:4:6 Trinitrotoluene)
RDX (rapid detonating explosives)
Effects on Victims:
-Bodies are blown into pieces and instantaneous death occurs.
-Flame causes 1st, 2nd and 3rd degree burns.
-Sound effect may cause the rupture of the tympanic membrane.

-Blast waves causes rupture of abdominal organs, pneumothorax, ruptured
stomach and bowl may be the other effects from explosions.
-Embolism in circulation.
Medico-Legal Aspects:
Try to count number of victims and try to put pieces of same person together.
Perform precipitin test to distinguish between the pieces of human and animal
bodies.
3. Communication and Transportation Injuries:
These injuries include:
a. Vehicular Injuries (Road Traffic Accidents)
b. Railway Injuries
c. Aircraft Injuries
Road Traffic Accidents (RTA):
Causes of RTA:
1. Fault of the victim.
2. Fault of the driver.
3. Fault of the Vehicle.
4. Fault of another vehicle, not involved in the accident.
5. Bad road condition.
6. Wrong signaling.

Investigation of RTA:
The investigation of RTA involves the following purposes:
1. To identify the cause of death.
2. To allow adequate compensation to the victim, if he/she is alive or dead.
3. To punish the offender, if offence is involved.
4. To search guidelines towards prevention of such future accidents.
Thus the investigating team should involve Investigating Police officer,
automobile expert and Medico-legal expert.
Thus, the investigating team should investigate the following:
1. Collection of history.
2. Examination of the deceased or the injured.
3. Examination of the vehicles involved in the accident.
4. Examination of the spot or place of occurrence of the accident.
Injuries and their Interpretations in Road traffic accidents.
RTA injuries are blunt force injuries with force-full impact.
According to their mode of production, they have 3 distinct types:
1. Primary impact Injuries.
2. Secondary Injuries.
3. Secondary Impact Injuries.
1. Primary Impact Injuries:
-It is caused by vehicle.
-Caused when the vehicle hits the victim e.g. pedestrian, for the first time, to
knock him down. Thus the injuries may bear the design of the part of vehicle
causing the injuries in the form of Imprint abrasion or patterned bruises.
-The marks on the body of the victim by the part of vehicle may give an idea
about the height of the vehicle.
2. Secondary Injuries:
-It is caused by the roadway, pavement or other objects like trees etc.
-These injuries are sustained by the victim after being knocked down by the
vehicle, due to fall and friction or impact with the ground.
-So, on examination, sand, soil, or gravel on the injuries area helps to link the
place of occurrence.
-Grazed abrasion and Stretched laceration are most common due to friction with
the ground.
3. Secondary Impact Injuries:
-It is due to running over or dragging by the vehicle.
-These injuries are as a result of impact between the body and the vehicle for the
second time.
-When after primary impact, the victim thrown forward and falls on the ground
and if the vehicle is still in motion, then the wheels of the vehicle will run over the
victim. Hence secondary impact injuries bear the tyre marks of the wheels.
-Avulsion laceration is the most frequent injury caused due to run over by the
vehicle.
Post-Mortem Examination:
It includes examination of dead victims for:
1. The body should be examined carefully for abrasions, bruises and
lacerations with their size, numbers and placement.

2. The clothes if available should be examined for tears, grease marks,
blood stains, soil or mud stains etc.
3. Internal injuries should be noted with presence of any glass fragment or
metals, paint flakes to compare with the vehicles.
4. Tyre marks, if presents should be noted.
5. Blood should be taken for estimation of alcohol, or any sedative drugs if
taken during driving.
Railway Accidents:
Railway injuries may be accidental or suicidal.
Fatal railway injuries may be sustained in the following ways:
-While walking along the rail or track.
-While crossing the rail or track.
-When a person is pushed suddenly in-front of a running train.
-When a person lies down on the railway track for a suicidal purposes, when the
train is coming.
-When a person accidently falls or intentionally jumps or is pushed from a running
train.
-When the head or some part of the body is extended out of the door or window
of a running train.
-When two train coming from the opposite direction collides.
-When the train is de-railed.
-When there is an outbreak of fire in a running train.
-When the passengers standing on the roof of train are electrocuted or struck
against and overhead structure or a over-bridge.

-Identification of a victim may become very difficult due to gross mutilation of the
body.
Aviation Accidents:
-Most challenging problem for identification of the victims.
-The bodies are often with gross mutilation or burnt that identification is nearly
impossible.
-Sometimes, the pocket articles, passports, letters, photographs, tattoo marks,
dentition, if un-burnt, may help for identification of victim.
-Now a days, DNA test is the mode of identification is such aviation accidents.
TOXICOLOGY/POISONING
Toxicology is a science dealing with properties, action, toxicity, fatal
dose, detection, estimation and treatment of poisons.
Forensic toxicology deals with the medical and legal aspect of the
harmful effects of chemicals on human being.
Toxicology refers to toxins produced by living organism which are
dangerous to man. Like poisonous plant, venom of snake, spider,
scorpion.
Poison is a substance, which if introduced in living body, or brought in
contact with any part through, will produce ill health or death, by its
constitutional or local effects or both.

Some poisons are harmless in small quantity but produce death if large
quantity is used.
Property of ideal homicidal poisons:
1. Cheap
2. Easily available
3. Colorless, odorless, tasteless.
4. Highly toxic and very small fatal dose.
5. Sign and symptoms should resemble of natural disease.
6. There should not be any antidote.
7. There should be no postmortem changes.
e.g. arsenic, aconite are commonly used homicidal poison.
Property of ideal suicidal poisons:
1. Cheap
2. Easily available
3. Tasteless or pleasant taste.
4. Highly toxic.
5. Can be taken with food or drinks.
6. Capable of producing painless death.
e.g. Organ phosphorus compound (OPC), endrine are commonly used in
rural area. Barbiturates, potassium cyanide and diazepam in urban area
are used as suicidal poison.
Classification of poison according to symptoms they produces (mode
of action):
A. Corrosive:-
1. Strong acids: sulphuric acid, nitric acid, hydrochloric acid, acetic
acid, carbolic acid, oxalic acid, salicylic acid.
2. Strong alkalis: sodium hydroxide or caustic soda, potassium
hydrochloride, ammonium hydrochloride.
3. Metallic salts: zinc chloride, potassium cyanide, ferric chloride,
chromates of alkalis, bichromates of alkalis , Mercuric chloride etc
B. Irritants:-
1. Inorganic:-
a. Non-metallic:- phosphorus, halogen.
b. Metallic:- arsenic, antimony, mercury, copper, lead, zinc, silver.
2. Organic:-
a. Vegetables:- castor oil, cotton oil.
b. Animals:- snake venom, insect bites.
c. Mechanical:- glass powdered, diamond dust.

C. Systemic:-
1. Cerebral:
a. CNS depressants:- alcohols, general anesthetics, opioid analgesic,
hypnotics, sedatives.
b. CNS stimulants: cyclic antidepressants, amphetamine.
c. Deliriant: Dhatura, belladonna, cannabis, cocaine.
2. Spinal: nux vomica (strychnine), gelsemium.
3. Peripheral: conium, curare.
4. Cardiovascular: aconite, quinine, tobacco, HCN, oleander, nicotine.
5. Nephrotoxic: Oxalic acid, mercury, cantharides.
6. Hepatotoxic: Phosphorous, carbon, tetrachloride, chloroform
D. Miscellaneous:-
1. Insecticides:-
a. Organ phosphorus compounds:-
i. Alkyl phosphates:
Hexaethyl tetra phosphate (HETP),
Tetraethyl pyrophosphate (TEPP),
Octamethyl pyro-phosphoramide (OMPA)
ii. Aryl phosphates:- parathion, diazinon.
b. Chlorinated hydrocarbons:- endrine, D.D.T. and gamaxin.
2. Antihistamines
3. Food poisons:- Clostridium Botulism, Mushroom poisoning.
Classification according to motive of use (medico legal aspects):
1. Homicidal Poison: Arsenic, Aconite, Digitalis, Strychnos nux
vomica, opium, mercury, antimony etc.
2. Suicidal Poison: Opium, Barbiturates, OPC, Carbolic acids, Copper
sulphate, Endrine, KCN etc.
3. Accidental Poisons: Aspirin, OPC, Copper sulphate, snake bite,
Ergot, CO, CO2, H2S, kerosene etc
4. Abortifacient: Ergot, Calotropis, Plumbago, Oleander seeds, Lead etc.
5. Stupefying: Dhatura, Cannabis, Chloral hydrate.
6. Causing bodily injury: Corrosives acids and alkalis.
7. Cattle poisons: Abrus precatorius, Calotropis, plumbago, OPC etc
8. Malingering purposes: Semicarpus anacardium
9. Infanticides: Opium, mader, tobacco

Route of administration of poison:-
1. Inhalation in gaseous or vapor form.
2. Injection into blood vessels(IV)
3. Intramuscular, subcutaneous and intradermal injection.
4. Application to a wound(Ulcer)
5. Introduction like oral, nasal, rectal, urethral, vaginal.
Route of elimination of poison:-
1. Kidney
2. Skin
3. Bile, milk, saliva, mucous and serous secretion.
4. Unabsorbed portion by vomit and faeces.
Action of poison:
1. Local: Result from direct action. (acids and alkalis)
a. Corrosion:- lesion by strong mineral acids.
b. Irritants:- gastritis by arsenic.
c. Nervous effects:- dilatation of pupil by Dhatura.
2. Remote:-Opium, barbiturates, tranquilizers, digitalis etc

a. Non specific:-corrosive are capable of producing remote non
specific action such as shock.
b. Specific:-nux vomica acting on spinal cord and produces tetanic
convulsion.
3. Combined local and remote:- OPC, Meruric chloride, phosphorous,
arsenic, snake venom etc
Carbolic acid acts locally as a corrosive and remotely as a narcotic
poison.
Factors modifying the action of poison:
1. Quantity: Greater the quantity more severe would be symptoms of
poison and usually rapid would be fatal.
2. Form of poison:- The action of poison is influences by the form in
which it is administered.
a. Physical state:- gas, liquid or solid.
b. Chemical combination:- for e.g. arsenic is not poisonous but its
salt arsenious oxide is poisonous.
c. Mechanical combination:- for e.g. small dose of concentrated
mineral acid produces corrosive action but same dose largely
diluted with water is harmless.
3. Mode of administration:- The rapidity of action of a poison depends
upon the route of administration, rate of absorption and the mode in
which it is introduce into the system. The route of administration may
be enumerated as follows in order of rapidity of action:-

a. Inhalation
b. Intravenous
c. Intramuscular, subcutaneous, intradermal,rectal
d. Oral
4. Condition of body:-
a. Age:
b. Habit:- action of certain poison decrease with habituate. An addict
can tolerate larger dose than a non addict. Like alcohol, morphine.
Antidotes: These are the substances which prevent or neutralize or
counteract the action of poison.
Reasons of use of antidotes:-
1. The poison may not be completely removed by gastric lavage or
the procedure is contraindicated.
2. The poison is already absorbed.
3. The poison has been administered other than ingestion.
Classification of antidotes:-
1. Mechanical antidotes or physical antidote.
2. Chemical antidotes
3. Physiological or pharmacological antidotes

4. Serological antidote
1. Mechanical antidotes: acts by preventing absorption of poisons.
a. Activated charcoal
b. Demulcents: egg albumin, fats, oil.
2. Chemical antidotes: they counteract the action of poison by forming
harmless compound, when brought in contact with them.
a. Sodium sulphate for lead poisoning
b. Copper sulphate for phosphorus poisoning.
c. Ferric oxide for arsenic poisoning.
d. KMNO4 for Opium and OPC
3. Physiological antidotes: these are the agents which act on the tissue
of the body and produce symptoms exactly opposite to those caused by
poisons. E.g.: a) Atropine, Pralidoxime for OPC
b) Paracetamol poisoning: N-acetyl cystine
c) Opioids poisoning: Naloxone
d) Dhatura Poisoning: Neostigmine.
e) Strychnine Poisoning: Barbiturates.
4. Serological antidote: Anti-snake venom
Universal Antidotes: it is an antidotes that is used in those cases where
the nature of the ingested poison in not known.
It has following composition:-
Activated powder charcoal or burnt toast---2 parts (absorbent)
Magnesium oxide---1 part 9neutralises if poison is acid)
Tannic acid or strong tea----1 part(precipitates alkalis)
Stomach wash/gastric lavage by Boas or Ewald’s tube
Chelating Agent: These are soluble organic compound which fix
metallic ions into their molecular form and make them inactivate. They
form chelate with metallic poisons those are freely available in the
circulation and their early excretion from the body through kidney.
e.g.:-
1. EDTA(ethylene diamine tetra acetic acid):-for lead.
2. Desferrioxamine:-for acute and chronic iron poisoning.
3. Bemigride:- barbiturate poisoning
4. Nalorphine:- morphine, heroine poisoning.
5. Penicillamine (Cuprimine): Free metals
6. Dimercaprol: For arsenic, mercury, copper, bismuth, gold.
Principle of management of poisoning:

The following principle should be followed in case of poisoning:-
1. Removal of unabsorbed poison from the body:-
a. If inhaled:-take pt. to fresh air. Give oxygen and artificial
respiration if necessary.
b. If bitten or injected:- immediately apply tight band above the
wound. Release in every 10 minutes for 20-30 second to prevent
gangrene.
c. If local application:- it should be washing with water.
d. If ingested:- stomach wash/ gastric lavage within 3 hr.
2. Administration of antidotes
3. Prevention of absorption into the system:- by
a. Renal excretion can be improved by plenty of fluid, diuretics.
b. Increasing diaphoresis ( Perspiration) using neostigmine,
pilocarpine
c. By dialysis.
d. By chelating agents
4. Treatment of general symptoms:-
Pain, shock, peripheral circulatory collapse, electrolyte imbalance.
Contraindication of Gastric Lavage:
1. Very old patients with esophageal varices.
2. Poisoning with corrosives: danger of perforation of stomach.
3. Convulsant poisons: attempt of using tube may lead to
convulsions.
4. Comatose patients: risk for aspiration.
Contraindication of Emesis:
-Corrosives and volatile poisons.
-Comatose patients.
-Heart disease patients.
-Pregnant women.
-Kerosene : may cause aspiration pneumonia.
Datura (thorn apple):
Varieties of Datura:-
1. Datura alba, a white flowered plant.
2. Datura niger, a purple flowered plant.
-It grows in waste places.
-The fruits are spherical with sharp spines.
-The seeds are kidney shaped.
-The flowers are bell shaped.
-All parts of plants are poisonous, especially seeds and fruit.

Active principle of Datura:-
1. Hyoscine 0.2 to 1.4 %
2. Hyoscyamine
3. Trace of atropine.
Major medico legal use of Datura:
-Used as stupefy travelers in railway station, bus terminals.
-Religious use.
Mode of use:-
Crushed or powdered seeds or an extract are usually mixed with
cigarette, pans, drinks or sweet.
Fatal dose:- 0.6 – 1 gm. (100-125 seeds)
Fatal period:- 24 hours.
Onset of action:- within half an hour of
swallowing the poison.
Action:-
-The alkaloids atropine, hyoscyamine and hyoscine first stimulate the
higher centre of the brain, then motor centre, and finally causes
depression and paralysis of medulla.
-The respiration is first stimulated, then depression, and the heart
centre is stimulated.
Signs and symptoms:

1. Bitter taste, dryness of mouth and throat.
2. Difficulty in talking, dysphagia.
3. Burning pain in stomach and vomiting are first noticed.
4. Face become flushed, conjunctival congestion, pupils widely
dilated, temporary blindness, photophobia and diplopia.
5. Giddiness, confused, staggering gait.
6. Urinary retention.
7. Skin is dry and hot.
8. Bounding pulse 120-140 bpm, later become weak & irregular.
9. Respiration and temperature increases.
10. In fatal cases, drowsiness passes into stupor, convulsion and
coma.
Treatments:
1. Emetics can be used.
2. Stomach wash with weak solution of tannic acid.
3. Washout lower bowel frequently.
4. Physostigmine 0.5 mg i.v. or i.m. at hourly intervals to counter act
the effect of datura.
5. Pilocarpine nitrate, 5 mg s.c. at 2 hrly interval, but it does not
counteract the effect of Datura in brain.

6. Morphine in contraindicated as it causes respiratory muscle
depression.
7. Delirium can be control by bromide or short acting barbiturates.
8. Light diet, free purgatives for 4-5 days to remove seed.
9. Symptomatic treatments.
Post-mortem appearances:
External :-
1. They are not characteristics.
2. Pupil are dilated.
Internal :-
1. Mucous membrane of stomach, intestine congested.
2. Seed or fragments of may be found in stomach or intestine.
3. Brain and its membrane are congested.
Chlorinated Hydrocarbons:
Many chloro compounds have been synthesized as insecticides from
dichloropropene to very complex modern synthetics. Commonly used
as pesticides.
Common chlorinated hydrocarbons are :-

DDT
Endrine
Gammexane
Dieldrin
DDT (Dichloro-Diphenyl Trichloroethane):
Acute poisoning: It may follow ingestion, extensive contamination of
skin or prolonged inhalation.
Sign and symptoms:-
-Following ingestion within an hour:-
-Salivation, nausea , vomiting, abdominal pain.
-After absorption by inhalation or through the skin:-
-Irritation of eyes, nose and throat.
-Dilated pupil, blurring of vision.
-Cough, pulmonary oedema.
-Dermatitis.
-Nervous system in both ingested or inhaled cases:-
-Tremor, restlessness, incoordination, muscle spasm.

-Convulsion, depression, collapse.
Fatal dose:- 5-6 gm.
Fatal period:-1-7 hours.
Treatment:-
1. Emetics and stomach wash with water.
2. Inj. Atropine.
3. Calcium gluconate i.v.
4. Artificial respiration if necessary.
5. Barbiturates can be given if muscle twitching or tremor persist.
Post-mortem findings:-
The findings are those of asphyxia.
Internal:-
1. Gastric mucosa is congested.
2. Stomach gives smell of kerosene.
3. Pulmonary oedema is common.
4. Lungs, spleen and brain is congested.
5. Liver is damaged.
Kerosene oil poisoning:

Kerosene is refined oil obtain from petroleum or rock oil.
Fatal dose:- 15-50 ml.
Fatal period:-1 day.
Sign and symptoms:-
1. Nausea, vomiting, abdominal pain and diarrhea with risk of
aspiration pneumonitis.
2. Breath, vomit and urine gives peculiar smell of kerosene.
3. Pupil first contracted then dilated as coma proceeds.
4. Aspiration produces coughing, choking, gasping, bronchospasm,
hypoxia and CNS depression.
5. Hemorrhagic pulmonary edema with pink, frothy sputum and
progresses to shock and cardio respiratory arrest.
Treatment:
1. Stomach wash is contraindicated due to danger of aspiration into
lungs.
2. Artificial respiration if necessary.
3. Glucose i.v.
4. Inj. Penicillin to prevent pulmonary infection.
5. High carbohydrate diet and vit. B complex to prevent liver
damage.
6. Steroids for penumonitis.

7. Oils and fats are contraindicated but liquid paraffin may be given.
Post-mortem appearance:
1. Usual sign of asphyxia.
2. Smell of kerosene may be noticed from lungs and stomach.
3. Mucous membrane of stomach and intestine acutely inflamed
with sub mucous hemorrhage.
Organo phosphorus compounds (OPC):
These are derivatives of phosphoric acid. They form 2 series of
compounds:-
i. Alkyl phosphates:-
Hexaethyl tetra phosphate (HETP),
Tetraethyl pyrophosphate (TEPP),
Octamethyl pyro-phosphoramide (OMPA)
ii. Aryl phosphates:- chlorothion, parathion, diazinon.
Mechanism of action:
-Acetylcholine are produced at myoneural junction, which is hydrolyzed
into choline and acetic acid spontaneously by the action of acetyl
cholinesterase.
-OPC inhibits acetyl cholinesterase, as a result it can not hydrolyzed
acetylcholine. So acetylcholine is accumulated at parasympathetic,

sympathetic and somatic sites as a result nerve impulse blocked at
myoneural junction and produces toxic actions.
Sign and symptoms:-
Muscarnic like effect:-
Remember SLUDGE: Salivation, Lacrimation, Urinary incontinence,
Diarrhea, Gastrointestinal distress and Emesis.
1. Bronchial tree:- bronchospasm, increase bronchial secretion,
dyspnoea, pulmonary oedema, cyanosis.
2. GIT:- excessive salivation, anorexia, nausea, vomiting, abdominal
cramps and diarrhoea.
3. Sweat gland:- increase sweating.
4. Lacrimal gland:-increase lacrimation.
5. CVS:- bradycardia, hypotension.
6. Pupil:- miosis, pin point pupil.
7. Ciliary body:- blurred vision,
8. Bladder:- urinary incontinence.
Nicotine like effect:-
1. Striated muscle:- muscle fasciculation, cramps, weakness, muscle
paralysis.

2. Sympathetic ganglia:- hypertension, tachycardia, pallor, mydriasis.
CNS manifestation:-
Restlessness, headache, tremor, drowsiness, confusion, slurred speech,
ataxia, coma, convulsion, depression of respiratory and cardiovascular
system.
Treatment:-
-The patient is removed from source of exposure, the contaminated
cloth is removed, and exposed area are washed with soap and water.
-Atropine sulphate 2 mg iv is given and repeated at 5-10 minute
intervals until symptoms of atropinization appears, and this is
maintained for 2-3 days.
-Gastric lavage with 2% potassium permanganate.
-Pralidoxime should be given in addition to atropine in a dose of
30mg/kg I.V. at a rate not exceeding 500 mg per minute and repeated
every 30 minute as necessary. Alternative obidoxime 3 mg/kg by I.M.
can be used.
-Oxygen inhalation and artificial respiration.
-Aspiration or tracheostomy, if secretion in the respiratory tract causes
obstruction.
-Adequate treatment for dehydration, electrolyte imbalance and shock.
-Exchange transfusion may be needed.
Post-mortem appearances:

The changes are those of asphyxia.
External:-
1. Face is congested, cyanosis of lips, finger and nose.
2. Blood stained froth is seen at mouth and nose.
3. Kerosene like smell may be felt.
Internal:-
1. Stomach:- mucosa is congested, sub mucous petechial hemorrhages
are seen.
2. Respiratory passage:- congested, contains frothy hemorrhagic
exudates.
3. Lungs:- congestion, excessive edema and sub pleural petechiae.
4. Heart:- soft and flabby.
5. Brain:- congested and petechial hemorrhages.
Atropinization: Administration of atropine sulphate in poisoning,
especially in Organo phosphorus poisoning in order to counteract the
effects of the poison and thereby obtaining of the therapeutic effects
slowly is known as atropinization.
Signs of atropinization include dry, flushed skin, pupillary size of at least
4 mm, & heart rate of 120/min.

Opium:
Geographical distribution of opium:
-It is cultivated in India, china, turkey, Egypt, Russia, Yugoslavia and
England.
-Poppy seeds are white, harmless, nutritive and used as food.
-The oil from seeds are use for cooking purpose.
-It is dry juice obtained by incision from unripe capsule of white poppy
(papaver somniferum).
-By multiple longitudinal incision to the unripe poppy capsule, a milky
white juice is obtained, which on drying under atmospheric condition,
gives crude opium. It is reddish brown, characteristic odor and bitter
taste in fresh condition but hard, brittle, dark brown or even black on
keeping.
Opium alkaloids:
Crude opium contains a large number of alkaloids, about 25. these form
2 chemically different groups.
1. Phenanthrenes:-
morphine 10% of opium
codeine 0.5% of opium
Thebaine 0.3% of opium
2. Isoquinoline:-
Papaverine 1% of opium
Narcotine 6% of opium
Morphine:
-Morphine is a white shining crystals, has bitter taste and alkaline
reaction.
-The narcotic symptoms of opium poisoning are practically those of
morphine poisoning.
Classifications of narcotics:-
1. Natural:- morphine, codeine.
2. Semi-synthetic:-heroin, hydromorphine, oxymorphine.
3. Synthetis:-mepridine, methadone, levarphanol,fentanyl.
Action:-
Opiates exert their effects because of their chemical similarity to
natural substances called endorphins.
Fatal dose:- opium—2 gm

codeine—0.5 gm
morphine--0.2gm
Fatal period:- 6-12 hours.
Mode of death in opium poisoning:-
Opium depresses cortex, the respiratory and cough centers in medulla.
Reduces the responsiveness of the respiratory centers to co2 thus
cessation of respiration and causes death.
Sign and symptoms:-
A. Stage of excitement:-
This stage is of short duration, may absent if large dose is taken.
1. Increased sense of well being
2. Mental activity.
3. Free from anxiety.
4. Talkativeness
5. Restlessness
6. Flushing of face.
B. Stage of stupor:-

The nervous centers are depressed during this stage, which sometimes
comes on quite suddenly.
1. Headache and giddiness.
2. Nausea and vomiting.
3. Lethargy, drowsiness.
4. An uncontrollable desire to sleep from which the patient may be
roused by external stimuli but soon passes to stupor and coma.
5. Pupils are constricted.
6. Face and lips are cyanosed.
C. Stage of coma:-
Recovery takes place at this stage under prompt and proper treatment.
1. Patient passes into deep coma and can not roused.
2. Muscle are relaxed and reflexes are lost.
3. All secretion suspended except sweat.
4. Face is pale.
5. Pupil pin point and insensible to light.
6. Temperature subnormal.
7. Blood pressure falls.
8. Pulse and respiration are slow.

Treatment:
1. Stomach wash with a solution of 1:5000 potassium
permanganate.
2. A tablespoonful suspension of charcoal may be introduced into
the stomach.
3. Emetics usually fails due to depression of vomiting centers.
4. The intestine should be cleared out by enema twice daily for 2
days to prevent reabsorption.
5. Naloxone hydrochloride is a specific opoid antagonist.
6. Atropine is contraindicated, as it can cause death by paralyzing
the motor and sensory nerve.
Post-mortem appearances:
1. Face and nail cyanosed.
2. When chest is open smell of opium can found.
3. Tracheas and bronchus:- mucous membrane is congested and
covered with bloody secretion.
4. Lungs:- congested, edematous and frothy exudates.
5. Heart:- right side full and left side empty.
6. Stomach:- lump of opium can be found, and smell of opium can
found.

7. Brain and other abdominal organs are congested.
Cannabis indica:
Active principle
1. Cannabinol
2. Cannabidiol
3. Tetrahydrocannabinol isomer
Fatal dose:-
Bhang:-10 gm/kg.bd.wt.
Ganja:- 8 gm/kg.bd.wt.
Charas:- 2 gm/kg.bd.wt.
Fatal period:- several days.
Onset of action:-
Smoking:- Soon after smoking and last for 1-2 hours.
Swallowing:- 30 minute after swallowing & last for 2-3 hrs.
Forms of cannabis indica:-

-Bhang (Patti):-It is prepared from dried leaves and fruits. It is mildest
form and contains 15 % of active principle. Fresh bhang is highly
intoxicating and narcotics.
-Majoon:- it is sweet prepared from bhang.
-Ganja/ marijuana:-it is prepared from flowering top of female plant. It
has a rusty green color and characteristic odour. It contains 15-25 % of
active principle. It is mixed with little tobacco and smoke in pipe.
-Charas /hashish:-it is the resin exudates from the leaves and stems of
plant. It is dark green or brown in color. It contains25-40 % of active
principle.
Sign and symptoms:
Small dose: Euphoria, heightening of subjective experiences and
disorientation.
Moderate dose: Impaired immediate memory, disturb thought
patterns, lapses of attention.
High dose: Changes of body image, depersonalization and marked
sensory distortion.
Stage of intoxication:-
1. There is giddiness and ataxia.

2. Speech become confused.
3. Tingling and numbness of the skin and drowsiness.
4. The patient passes into deep sleep and wakes with lassitude and
impaired mental function.
5. Death may rarely occur from respiratory failure.
Treatment:-
1. Stomach wash.
2. 100ml. of 50% glucose, 2 mg naloxone and 100mg. Thiamine i.v.
3. 5-10 mg diazepam, if patient is aggressive.
4. Anti anxiety and antipsychotic drugs can be given if necessary.
5. Oxygen inhalation and artificial respiration.
6. Symptomatic management.
Post-mortem finding:-
No characteristic finding.
-Ganja psychosis
-Prolonged over indulgence of any form of cannabis indica leads to a
condition known as Ganja psychosis.
Features are:-

1. Marked congestion of conjunctiva.
2. Anorexia, lethargy, weakness and emaciation.
3. Tremor
4. Impotence
5. Insanity.
Snake poisoning:
There are more than 3500species of snakes, only about 250 are
poisonous.
SNAKE
POISONING
COLUBRIDAE OR COBRA
ELAPIDAE OR LAND SNAKES ( COBRA,
KING COBRA, KRAIT ETC)
HYDROPHINAE OR SEA SNAKES
VIPERIDAE OR VIPERS ( RUSSEL
VIPERS, PIT VIPERS, ECHIS VIPERS ETC
NONPOISONING
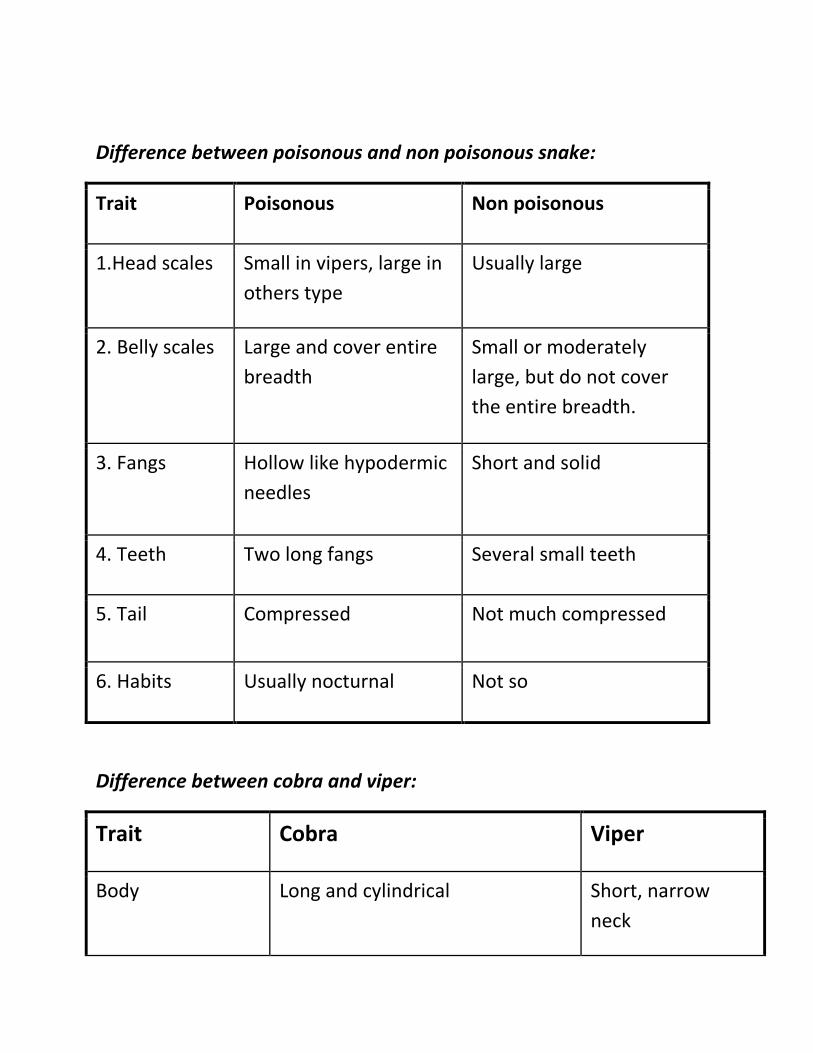
Difference between poisonous and non poisonous snake:
Trait Poisonous Non poisonous
1.Head scales Small in vipers, large in
others type
Usually large
2. Belly scales Large and cover entire
breadth
Small or moderately
large, but do not cover
the entire breadth.
3. Fangs Hollow like hypodermic
needles
Short and solid
4. Teeth Two long fangs Several small teeth
5. Tail Compressed Not much compressed
6. Habits Usually nocturnal Not so
Difference between cobra and viper:
Trait Cobra Viper
Body Long and cylindrical Short, narrow
neck

Head Small, seldom broader than body,
covered by large scales or shields
of special forms.
Large, broader
than body,
triangular and
covered by
numerous small
scales.
Pupil It is round vertical
Maxillary bone Carries poison fangs and other
teeth
Carries only
poison fangs
Fangs Grooved, fixed, short and
fine
Canalised and long
Tail Round Tapering
Eggs Lay eggs Give birth to young one
Venom Neurotoxic Haemotoxic
Snake venom:
Venom is the saliva of the snake. Cobra venom is the faint transparent
yellow and is slightly viscous.

When exposed to sun, it becomes slightly turbid. Russell’s viper venom
is white or yellow.
Composition: Snake venom are complex mixture, chiefly proteins,
many which have enzymatic activities. They include coagulant,
fibrinolytic, proteolytic and neurotoxic proteins.
The enzyme are Neurotoxins, haemolysin, proteolysis, Fibrinolysin,
Cholinesterase(in cobra only), Coagulase, Cardiotoxins, Necleaotidase,
Hyaluronidase(in viper only), phospholipase A.
Action of venom:
Elapidae venom is mainly neurotoxic. Viper venom mainly vasculotoxic
and hydrophinae venom is myotoxic.
1. A Neurotoxic venom causes muscular weakness of the legs and
paralysis involving the muscles of the face, throat and respiration. Local
symptoms and signs at the site of the bite are minimum. General
symptoms are due to local histamine release.
2. A Vasculotoxic venom produces enzymatic destruction of cell walls
and coagulation disorders.
3. A Myotoxic venom produces generalized muscular pain with
respiratory failure.
Symptoms and signs:
In cobra or krait bite:

-Immediate local effects are burning or tingling pain, irritation, redness,
swelling and inflammation at the site of bite.
-Giddiness, lethargy, muscular weakness and a feeling of intoxication.
-Sometimes nausea and vomiting are early symptoms.
-Increasing muscle weakness leading to paralysis of lower limbs,
spreading to trunk and head.
-Difficulty in swallowing and speech due to paralysis of the muscles of
lips, tongue and throat.
-Breathing becomes slow
In viper bite:
-Locally, pain, swelling, discoloration and ecchymosis at the site of bite
and oozing of a bloody serum from the apertures caused by the bite.
-Abdominal pain, nausea, vomiting and signs of collapse such as cold
and clammy skin, feeble pulse.
-Complete unconsciousness follows.
-In case of recovery from these effects, haemorrhages occur from the
mucous membrane of the rectum and other orifices of the body.
Extensive local suppuration, sloughing and gangrene and malignant
oedema or tetanus or death may occur from septicemia.
Treatment:
Local treatment: If the bite is on extremity, a ligature should be applied at
once, at some distance above the site of wound, and should not be
kept more than half hour.
-The part should be immobilized.
-Free and deep incision should be made into puncture without injuring
any large vessels.
-The poisons should be neutralized by washing the wound with a weak
aqueous solution of potassium permanganate.
-In case of cobra or krait bite, local infiltration with a 5% solution of
carbolic soap round the site of bite, when anti venom is not available.
Specific treatment: 20 ml of the polyvalent antisnake venom serum
should be injected I/V as soon as possible after the bite and the dose
should be repeated 2 hours later or even earlier if symptoms of collapse
appear.
-In case of viper bite, some serum should be injected round about the
site of bite to prevent sloughing and gangrene.
-40-60ml of anti-snake venom serum may be injected sub-cutaneously
or I/M, but is not effective as I/V injections.
Symptomatic treatment: Morphine or aspirin should be administered to
relieve pain and nervousness
-Adrenaline injection

-Calcium chloride 0.9gm in 20 minims of water to be injected I/M.
-Steroids given for allergy
-Body heat is to be maintained by hot water bottles.
-Normal saline with or without noradrenalin is to be given I/V.
-Artificial respiration to be given, if necessary
Post mortem appearance:
External:
-In cases of colubrine bites: 2 lacerated punctures about 1.5” deep.
-In cases of viperine bites: 2 lacerated punctures about 1”. These
lacerated punctures may be so minute that they may not be visible to
naked eye, but may be seen with a hand lens.
-Swelling and cellulitis is found about the bitten part.
-Aerolar tissue round the punctures is purple and infiltrated.
Internal:
-Hemorrhages from the mucous membrane of the body orifices.
-Blood extremely fluid and purple in color.
-In case of viperine bites, some clots may occur in the veins due to
fibrin ferment.
============================================================================

Section 6 (Forensic Medicine) of “ALL in ONE for the PMDC Step 1 Preparation by
Faizan Ali & Ghulam Mohiudin”
============================================================================