platelet function: its clinical significance
TRANSCRIPT
P l a t e l e t ~ unc~zo'n :
Its Clinical Significance A. D. GINSBURG
R. H. ASTER

T A B L E O F C O N T E N T S
I. PRELIMINARY CONSIDERATIONS . . . . . . . . . . 4
Plate le t F u n c t i o n . . . . . . . . . . . . . 4
Tests of Pla te le t F u n c t i o n . . . . . . . . . . 9
II. DISORDERS OF PLATELET FUNCTION (QUALITATIVE
PLATELET DEFECTS) . . . . . . . . . . . 15
Defec t ive A d h e s i o n to Col lagen . . . . . . . . 1 6
Defec ts of Seconda ry Aggrega t ion (Defec t ive
" R e l e a s e " R e a c t i o n ) . . . . . . . . . . . 17
Defects of P r i m a r y Pla te le t Aggrega t ion . . . . . . 24
Defects of Pla te le t F a c t o r 3 Act iv i ty
( " T h e T h r o m b o c y t o p a t h i e s " ) . . . . . . . . 25
Defect ive Clo t Re t r ac t ion . . . . . . . . . . 26
Deficiencies of P l a sma Cofac to r s Requ i red
for Plate le t F u n c t i o n . . . . . . . . . . . 26
Defec t ive Pla te le t Phagocy tos i s . . . . . . . . 27
III. TX~ROMBOCYTOPENIA . . . . . . . . . . . . . 27
Bleeding in T h r o m b o c y t o p e n i a States . . . . . . 27
Fac to r s T h a t M a y Affect the T e n d e n c y of
T h r o m b o c y t o p e n i c Pa t ien ts T o Bleed . . . . . . 29
A p p r o a c h to the Pa t i en t wi th T h r o m b o c y t o p e n i a . . 31
IV. THROMBOCYTHEMIA AND THROMBOCY'fOSIS . . . . . . 36
CONCLUSION . . . . . . . . . . . . . . . 39
has recently taken up an appointment as Assistant Professor of Medicine at Queen's University Faculty of Medicine, Kingston, Ontario, Canada. Prior to accepting this appointment, Doctor Ginsburg was a research lellow in hematology at the Thorndike Memorial Laboratory, Boston City Hospital, and Harvard Medical School. He received his M.D. degree trom the University of Cape Town and served as medical registrar at Groote Schuur Hospital from 1964 to 1967. His special interest is in the physiology and pathology of blood platelets.
is Executive Director of the Milwaukee Blood Center, Milwaukee, Wis- consin, and Professor of Medicine at Marquette School of Medicine. tte formerly was Assistant Professor of Medicine at Harvard Medical School and Research Associate, Thorndike Memorial Laboratory, Boston City llospital. Doctor Aster's research has included basic and clinical studies of platelet function, blood coagulation, platelet and leukocyte immunology and blood transfusion therapy.
T H E IMPORTANCE OF P L A T E L E T S in the physiology of organisms sufficiently complex to require a circulatory system is perhaps best illustrated by the fact that cells analogous to mammalian platelets arose very early in the course of evolution, probably even before leukocytes and erythrocytes. A prime example is the horseshoe crab (limulus), a species in existence for some 300 million years, in which platelet-like cells (amebo- cytes) are the only cellular elements present in the blood stream (1) .
Since the 1840s, when descriptions of mammalian platelets were first recorded, the role of platclets in a number of physio- logic processes has been recognized and their mechanism of action clarified.
NOTE: This work was supported by Training Grant No. 2-TOl- AMO5391, National Institute of Arthritis and Metabolic Diseases; Re- search Grant No. HE-12860 (National Heart Institute); and Career Development Award No. 5-K3-HE-18183 (National Heart Institute [Doctor Aster]).
It is the purpose of this report to analyze for the nonhematol- ogist the pathophysiology of the bleeding and thrombotic distur- bances due to quantitative and qualitative abnormalities of platelets, and to discuss briefly their diagnosis and therapy.
The initial section deals with current concepts and methods used for the study of platelet function. Subsequent sections discuss, in turn, qualitative disorders of platelets, thrombocyto- penias and thrombocythemia.
I. Preliminary Considerations PLATELET FUNCTION
PRIMARY HEMOSTASIS.IWhen small blood vessels are injured, bleeding ceases within a few minutes due to the formation of platelet plugs that seal gaps in the damaged vasculature. Forma- tion of these "white thrombi" or "primary hemostatic plugs" is the result of a sequence of reactions about which much has been learned during the past few years. Because of its great impor- tance as the first line of defense against blood loss, and its possible relevance in the pathogenesis of thrombocmbolic dis- ease, white thrombus formation will be considered in detail.
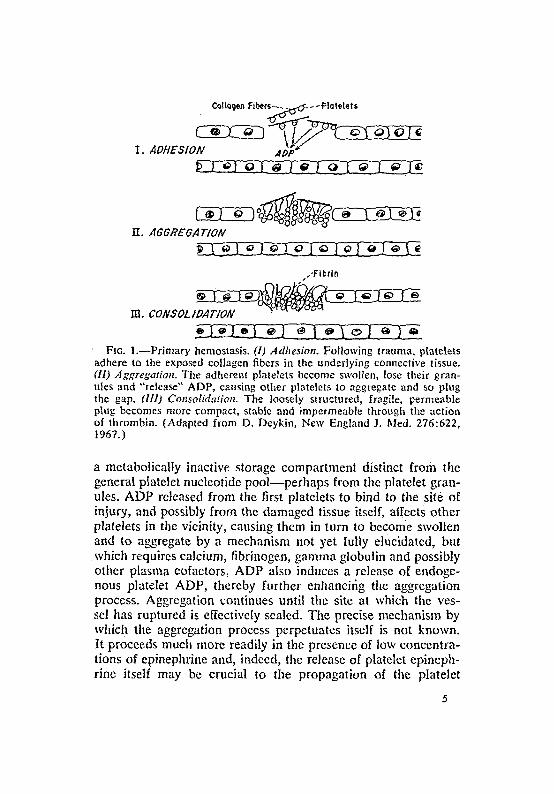
Formation of a primary hemostatic plug may be conveniently divided into three stages (Fig. 1 ) :
Adhesion.--Following trauma to a vessel, circulating human platelets become adherent to the damaged vessel wall and, specifically, to the exposed collagen fibers o f the connective tissue. Why platelets are selectively attracted to collagen is not known with certainty, but it seems clear that the "triple helical structure of native collagen is essential for this 'process and that free amino groups, particularly those of lysine, are necessary constituents of the binding sites. Interaction between platelets and collagen occurs in a purified system and apparently requires no cofactors. i
Aggregation.--As a consequence of their adhesion to colla- gen, platelets become swollen, extend pseudopodia, lose some of their granular constituents and selectively release adenosine diphosphate (ADP), serotonin, catecholamines (notably epi- nephrine) and platelet factor 4 (a highly basic protein with antiheparin activity) into the surrounding medium. It is of con- siderable interest that the ADP that is released is derived from
CQItQgen Fibers - ~ : ~ : - - ~Pla tele t s
I . ADHESION A~;D"
IT. AGGREGATION
.-Fibrin
m co vsoL/oAr o v
FIG. l.--Primary hemostasis. (1) Adhesion. Following trauma, platelets adhere to the exposed collagen fibers in the underlying connective tissue. (11) Aggregation. The adherent platelets become swollen, lose their gran- ules and "release" ADP, causing other platelels to aggregate and so plug the gap. (111) Consolidation. The loosely structured, fragile, permeable plug becomes more compact, stable and impermeable through the action of thrombin. (Adapted from D. Deykin, New England J. Med. 276:622, 1967.)
a metabolically inactive storage compartment distinct from the general platelet nueleotide pool--perhaps from the platelet gran- ules. ADP released from the first platelets to bind to the site of injury, and possibly from the damaged tissue itself, affects other platelets in the vicinity, causing them in turn to become swollen and to aggregate by a mechanism not yet [ully elucidated, but which requires calcium, fibrinogen, gamma globulin and possibly other plasma cofactors, ADP also induces a release of endoge- nous platelet ADP, thereby further enhancifig the aggregation process. Aggregation continues until the site at which the ves- sel has ruptured is effectively sealed. The precise mechanism by which the aggregation process perpetuates itself is not known. It proceeds much more readily in the presence of low concentra- tions of epinephrine and, indccd, the release of platelet epineph- rine itself may be crucial to the propagation of the platelet

plug. The interaction of platelet factor 4 with fibrinogen com- plexes that results in formation of fibrin-like precipitate ("para- coagulation") may also be of importance (2).
A very recent report by S. M. Wolfe, J. Muenzer and N. R. Shulman (J. Clin. Invest. 49: 104a, 1970) has'suggested that cyclic adenosine-3'-5'-monophosphate may be the key to the regulation of platelet aggregation and that prostaglandin E1 may have an important role in this regard through its effects on adenyl cyclase.
Consolidation.--Whereas the first two stages of primary hemostasis are independent of blood coagulation, consolidation of the platelet plug requires the formation and action of throm- bin. Although the probable source of such thrombin is plasma trapped within and about the platelet plug, it may be derived from clotting factors adsorbed to the platelets themselves as well. The role of thrombin may be threefold: to produce further platelet aggregation, to cause the platelet aggregates to shrink into solidly fused masses--possibly through the action of their contractile protein (thrombosthenin)--and to cause fibrin for- mation at the periphery of the plug and within the channels traversing the plug.
CLOT RETRACTION.--C1ot retraction may, in a sense, be con- sidered an extension of the process of primary hemostasis. It requires active platelet metabolism and is almost certainly mediated by contraction of platelet protein,, thrombosthenin, which closely resembles actomyosin found in skeletal muscle. Although the physiologic role of clot retraction is not co{npletely understood, it is generally assumed that its effectiveness in hemostasis is due to the formation of. a more dense, and therefore less permeable, thrombus.
COAGULATION.--In Figure 2 is shown the current "cascade" theory of blood coagulation, in which coagulation factors act sequentially on one another with the eventual evolution of a fibrin clot. The role of platelets in this system may be manifold:
Platelet Jactor 3 (PF:~).--As shown in Figure 2, platelets participate in at least two of the reactions leading to thrombo- plastin generation. Their activity at these points is due to phospholipid "exposed" or "released" as the result of changes in platelet structure. Of particular significance may be the demon- stration that aggregation of platelets increases the availability of
6

" • "INTRINSIC" pATHWAY 0 "EXTRINSIC" PATHWAY
CONTACT PLAT ELETS ~ + FACTOR 3rli
I 'X~ A / "TISSUE'FACTOR
"z" .Z A �9 r I,,-"- ~ P F .
p ffOTHRO§ ~a:~THRCHulBI N 3
FIBRINOGEN J - ~ FIBRIN
FIG. 2.---Cascade theory of coagulation. A, platelet factor 3 enhances (i) the activation of factor VIII and (ii) the formation of "intrinsic" thromboplastin. B, platelet-factor XII interaction produces a "tissue- factor" effect capable of activating factor X via the extrinsic pathway of coagulation.
PF.~. Recent studies suggest, in fact, that aggregatioo may be an essential prerequisite for PF3 activation.
"Tissue-Iactor" activity.--A separate activity, perhaps vestig- ial, but possibly of significance where the intrinsic pathway of coagulation is defective, as in hemophil ia , is the ability of platelets to promote clotting via the extrinsic pathway of coagu- lation, serving in the process as a substitute for tissue thrombo- plastin (Fig. 2) (3).
Other platelet [actors.--Platelet factor 2 (PF2) and platelet factor 4 (PF4) are low molecular weight proteins that have been obtained in highly purified states. PF2 shortens the time required for thrombin to clot fibrinogen. Its physiologic role is obscure. PF4 neutralizes heparin and inhibits the anticoagulant activity of fibrinogen breakdown products. As noted above, it may play a role in white thrombus formation.
The platelet "atmosphere."--Platelets are capable of adsorb- ingvarious materials from the plasma onto their surface--so much so that they have been compared to a sponge (4). All of

the known clotting factors are among the substances found ad- herent to the platelet surface. Plasma factor V is so closely asso- ciated with structural components of the platelet that it was at one stage regarded as a specific platelet factor--platelet factor 1. Fibrinogen is even more tightly bound and, in fact, appears to form an integral part of the platelet structure. Factors VIII, XI, XII and XIII are also tightly bound; factors II, VII, IX and X are present but are easily dissociated by washing. It seems high- ly probable that coagulation factors carried to a site of vessel injury by platelets act in the conventional coagulation se- quence (Fig. 2) to speed fibrin formation.
ENDOTtlELIAL suvPoRx.--Platelets and endothelial cells ap- pear to have a number of biochemical and, possibly, structural similarities. Recent studies have even suggested that platelets may be crucial for the maintenance of a normal vascular endo- thelial lining (5). Thus, in thrombocytopenia, petechial hemor- rhages, indicative of the escape of red cells from an intact vas- culature, may be due to a "weakening" of the vessel wall even though such vessels appear normal on electron microscopic study (6).
The nature of platelet-endothelial interaction (if it exists) is poorly understood. One possibility is that platelets are incorpo- rated bodily into endothelial cells (6). Alternatively, platelets may simply fill gaps between endothelial cells, thus preventing leakage of other blood constituents, or they may "sweep" the cndothelium clean of some toxic material. Since this hemostatic, but "nonthrombotic," function that platelets may possess is of great potential significan.ce for long-term organ preservation and studies of organ function in vitro, additional studies concerning platelet-endothelial interactions may.pi 'ovide information of great practical value.
PIIA~OCVXOSlS.--Platelets appear to be able to "ingest" inert materials such as latex particles. This is associated with a marked increase in aerobic glycolysis and citric acid cycle activity (7). It is not yet clear, however, whether in the case of platelets the process is one of trfie phagocytosis or whether particles merely slip into some of the many canal-like structures within the platelet that communicate with its surface. Antigen- antibody complexes, viruses and bacteria are similarly engulfed by platelets under appropriate conditions. The physiologic signifi-

~ance of platelet phagocytosis is obscure but deserving of further
iin vestigation.
TESTS OF PLATELET FUNCTION
PLATELET r every patient with a blecding or thrombotic tendency, a platelet deficiency, excess or defect should be considered. The first procedure should be the exam- ination of a properly prepared blood smear, since platelet lev- els may be approximated by inspection. At the same time, plate- let morphology and size should be assessed. If thrombocyto- penia or thrombocytosis is suggested from the smear, a platele't count should be performed.
The most satisfactory methods of determining platelet concen- trations are those that employ direct counting technics using a phase microscope. Electronic methods are being used more and more frequently and are useful when a large number of samples must be counted.
PLATELET FUNCTION TESTS.--In patients who have a bleeding defect despite normal levels of platelets and other coagulation parameters, a qualitative platelet abnormality must be consid- ered. A number of tests are available whereby this possibility may be investigated. These are grouped in Table 1 according to the aspects and phases of platelet function to which they are most specifically related.
The primary bleeding time.--Two basic technics, the Ivy (done on the forearm with a blood pressure cuff inflated t o 4 0 mm. Hg on the upper arm) and the Duke (ear lobe), have been described. Both tests are liable to difficulties of standardization
�9 but, with either, a persistently prolonged bleeding time in the presence of adequate platelet numbers is extremely suggestive of
impai red platelet hemostatic ability. The Ivy test is the more sensitive and the more easily standardized. Its theoretical basis is sound, since (a) if there are no platelets to plug the gaps, (b) if platelets are unable to adhere to collagen or (c) if they are unable to aggregate normally, prolongation of bleeding from a wound is to be expected. Thus, a prolonged bleeding time is found in most patients who have a defect of primary hemostasis due either to thrombocytopenia or to defective platelet function. A prolonged bleeding time may also result from a defect of the

T A B L E 1.----TESTS UTILIZED FOR TttE STUDY OF PLATELET FUNCTION
I. Tests relating to primary henzostasis
(a) General--nonspecific (i) Bleeding time (ii) In vivo platelet adhesiveness (Borchgrevink test)
(b) Platelet adhesiveness to collagen (c) Platelet aggregation (d) In vitro platelet adhesiveness
2. Clot retraction 3. Tests measuring platelet coagulation ]actors
Platelet factor III activity 4. Tests o~ endothelial supporting ]unction
Capillary fragility (?) 5. 31iscellaneous tests
(a) Platelet "phagocytosis" (b) Platelet electrophoretic migration
vessel wall, however, as in scurvy and, possibly, from congenital deficiency of a plasma factor necessary for primary hemostasis, as may be the case in von Willebrand's disease.
In classic hemophilia (factor VIII deficiency), the prhnary bleeding time is normal. If, however, the crust covering the wound is gently removed 24 hours later (secondary bleeding time), the bleeding that results may persist much longer than in a normal subject, apparently because there is little tissue damage under these conditions and hence less Stimulhs for platelet aggregation or for activation of the extrinsic pathway of blood coagulation. Hemostasis under such circumstafices depends largely on the intrinsic pathway of thromboplastin generation (Fig. 2) , which is, of course, defective in classic hemophilia.
The in vivo adhesiveness test o f Borchgrevhlk.----This proce- dure is performed by making a standardized cut in the patient's skin and performing serial platelet counts on the drops of blood that appear through the cut. The test has the same theoretical attractions and practical disadvantages as do standard bleeding time tests. If platelets cannot adhere to collagen, or do not aggregate normally, fewer platelets will be selectively removed from blood flowing from the damaged vessels--and hence the percentage of platelets remaining in blood flowing from the wound will be increased.
10
Test o] platelet adhesiveness to connective tissue.--Hirsh and co-workers (8) have described an interesting technic in which platelets are exposed to connective tissue strands in vitro. The extent and mode of their adhesion is studied under the phase microscope. This would seem to be a particularly useful, and informative, yet simple test. Theoretically, it could be of value in differentiating a defect of platelet adhesiveness from one of aggregation.
Platelet aggregation.---Studies of platelet aggregation have shed considerable light on many aspects of platelet physiology and function and provide a new and highly promising approach to the classification and diagnosis of platelet functional defects.
The basis of such studies is the measurement of changes in light transmittcd through platelet-rich plasma as platelets aggre- gate and disaggregate in response to various stimuli. Formation of platelet aggregates can be assessed crudely by eye, or more exactly by the use of a spectrophotometer. Several "aggre- gometers" now commercially available permit a continuous recording to be made of the aggregation process (a most complicated one) at constant temperature, and at a constant rate of agitation, both of which factors should be strictly controlled. In such a system, the effects of various stimuli on platelet aggregation may be assessed. The response of platelets to ADP (in various concentrations), epinephrine, collagen and thrombin have been of particular interest.
Figure 3 illustrates normal patterns of platelet aggregation observed on adding these compounds to platelet-rich plasma,
The response to ADP is strongly dependent on the tempera- ture, 37 ~ C. being optimal, and on the final concentration of ADP achieved. At low concentrations, lesser degrees of aggregation occur and are followed by disaggregation. At a Slightly higher concentration of ADP, the important phenomenon of secondary aggregation may be observed--there is an initial phase of aggre- gation followed by a more profound fall in optical density as maximal aggregation occurs. It is believed that the initial phase is due to platetet aggregation in response to the added ADP, whereas the secondary, more pronounced change follows release of additional ADP from the platelets themselves..The latter process may be thought of as an amplification step by which the concentration of ADP in the medium is increased, thus perpetu-
11

IOO
~ 6o
�9 ~ 40
2 0
I NORMAL PATTERNS
ADP or
Aggregotion
- ~ Secondory
- A I I l i i
o 2 4
\ ,,i" \ ' , ,
I=I I I I l I
o 2 4
DEFECT OF SECONDARY AGGREGATION
,,.Collagen
\ADP
C I I I I I I I
6 0 2 4 6
TIME (mini
FIG. 3 . - - In vitro patterns of platelet aggregation (schematic) . The pat- terns of aggregation following addition of (A) ADP or epinephrine and (B) thrombin or collagen are shown. When there is a defect of secondary aggregation, these patterns are markedly altered (C).
ating the aggregation process. The two phases o/ aggregation can be discerned only if the test is performed at 37 ~ C. The effect of epinephrhle is very similar; two phases of aggregation may also be observed--the first moderate, and probably due to the direct action of epinephrine itself, and the second maximal, and due to the release of platelet ADP. Smallquantities of thrombhz also cause platelet aggregation. A delay of about 10 seconds precedes the response, which is similar to that of ADP and may, in fact, be partially mediated by release of platelet ADP. Aggregation by collagen is preceded by an even longer delay, and is perhaps entirely dependent on the release of endog- enous platelet ADP.
In studying platelet aggregation, it is crueial to remember that aggregation curves may be affected by such drugs as aspirin (Section II, p. 19) for as long as 1 week after their ingestion.
In vitro tests o] platelet adhesiveness.--Several tests have been described (9). In most of these, the number of platelets in whole blood or platelet-rich plasma is counted before and after
12

exposure to a glass bead column, and the percentage of platelets sticking to the glass is determined. Plasma cofactors, hematocrit and an effect of ADP all seem to be important. ADP released from red cells increases the tendency of platelets to adhere to glass. The test is, therefore, dependent to some extent on the mechanical fragility of red cells.
Although platelet adhesiveness is clearly diminished in certain congenital disorders such as yon Willebrand's disease and in acquired conditions such as renal failure, the pathophysiologic significance of this change is not entirely clear and in no instance is it of specific diagnostic value.
Clot retraction.--When blood clots in a test tube, the clot retracts and serum is expressed. Clot retraction does not occur in the absence of platclets or in certain functional platelet disorders. Many other factors, such as temperature, concentra- tion of fibrinogen and possibly other plasma factors, numbers of red and white cells and the degree Of fibrinolysis, may all influence the retraction process and, ideally, should be con- trolled. Defective clot retraction in the face of a normal platelet count occurs, for practical purposes, only in the rare congenital disorder "Glanzmann's disease" (Section II, p. 24).
Assays o/platelet factor 3 activity (PF.~).--PFa activity en- hances the action of factors X and V in converting prothrombin to thrombin (Fig. 2). A reduced rate of prothrombin conversion (easily detected by measuring the residual prothrombin activity of serum) is, therefore, a readily available means for assessing PF~ activity. Provided that there is strict attention to detail,, and if the possibility of reduced plasma coagulant activity can be excluded, this is a useful screeningtest. However, normal values may be obtained in platelets shown to have PF:~ deficiency by other tests (12).
Other tests of PF.~ activity include the thromboplastin genera- tion test (TGT) and determination of the kaolin clotting time or the Stypven time of platelet-rich plasma. All depend on the measurement of the time required for plasma to clot on recalcifi- cation, or on the addition of Stypven (Russell's viper venom). The effectiveness of platelets in shortening the clotting time is due to their action at several points in the coagulation sequence (Fig. 2).
In order for the factor 3 activity of platelets to be fully
13

expressed, they must be "activated" in some way. Addition of kaolin or connective tissue fragments to the platelet-rich plasma, or aggregation of platelets by ADP, are capable of providing the necessary stimulus. More drastic measures (such as distilled water lysis, ultrasonication or repeated freezing and thawing) re- sult in a fourfold greater degree of PF z activity than occurs with "physiologic" activation. It has been suggested that the 20-25 % of maximal activity that is released by kaolin may be equivalent to that made available during blood coagulation.
Although tests of platelet factor 3 activity may be useful under some circumstances, they are difficult to standardize, and the range of normal is quite wide. As noted in Section II, some patients described in the literature as having PF:~ deficiency may have defective aggregation as their primary abnormality.
Tourniquet test o[ capillary [ragility.--Many variations have been used in the performance of this test. Essentially, intravascu- lar pressure in the forearm is increased by applying a cuff to the upper arm inflated to 80-100 ram. Hg. The forearm is then inspected for the development of petechial lesions. Theoretically, the tourniquet test is a measure of endothelial integrity rather than of hemostasis and may, therefore, provide a means of detecting defects specific to this aspect of platelet function. It is conceivable (although still speculative) that an isolated finding of an abnormal tourniquet test may indicate impairment of the endothelial-supporting function of platelets only, whereas the bleeding time, prolonged in the face of a normal tourniquet test, may reflect a defect of primary hemostasis only. This could explain, for example, why patients with von Willebrand's disease sometimes have a long bleeding time but a normal tourniquet test. No platelet disorder character ized 'by the converse--a positive tourniquet test and a normalbleeding t ime--has yet bccn recognized, however.
Platelet electrophoresis.---The effects of aggregating agents such as ADP on the rate at which platelets migrate in an electric field have been studied----especially by Hampton and Mitchell ( I 0 ) . These workers have observed an altered response in subjects with vascular disease and in conditions predisposing to the development of vascular disease that appears to be due to alteration in the concentrations of at least two plasma proteins. While such studies are still investigative, their potential signifi-
14
cance is obvious and further developments will be watched with great interest.
II. Disorders of Platelet Function (Qualitative Platelet Defects)
Classically, disorders of platelet function have been subdi- vided into those manifesting absent or poor clot retraction (thrombasthenia), those showing defective PF:~ activity (throm- bocytopathy) and those having defects of platelet aggregation (athrombia). The literature is extremely confusing on this point, however, for the terms have been interchanged by many work- ers. Moreover, in many reports of patients described as having isolated platelet defects, only one test of platelet function was available to the investigator, or only certain aspects of platelet function were studied. Where more than one function has been investigated," more than one defect often has been discovered, and a combined terminology has been employed in the descrip- tion of the patients studied. Thus, the term "athrombia throm- bocytopathica" has been used to describe the disorder in a subject whose platelets manifested both defective platelet aggre- gation and reduced PF s activity. A combination of deficient PF z activity and absent clot retraction has been labeled "throm- bopathy-thrombasthenia."
It would seem from recent studies that such "combinations" of platelet functional defects may well prove to be the rule rather than the exception, since many of the tests of platelet function may measure interdependent or sequential parameters. Thus, several studies have suggested that PF:~ activity is dependent on prior ADP release and aggregation of platelets. Additionally, pa- tients have been reported in whom platelet aggregation by col- lagen was defective and in whom there was also defective PFz activity. With the development of more satisfactory methods of studying platelet function, it may be anticipated that "thrombo- cytopathy" and "thrombasthenia" will be replaced by terms that more precisely specify the basic defect.
Table 2 illustrates diagrammatically the sequence through which platelets participate in hemostasis. Laboratory tests al- ready available may, as noted in the preceding section, be utilized in some instances to determine the level at which a defect exists.
15

TABLE 2.- -PARTICIPATION OF PLATELETS IN HEMOSTASIS
Trauma
Vascular lesion
Adhesion to collagen
Release of ADP
Platelet aggregation
Activation of PF3 ,L
Enhancement of coagulation mechanism and hemostasis
Clot retraction
In theory, defects might occur at many levels:
1. There might be deJective adhesion of platelets to collagen. 2. There might be deJective release of ADP from tile platelets. 3. There might be an absohtte inability o/ the platelets to
aggregate in response to ADP. 4. Platelet ]actor 3 activation might not occur. 5. There might be a total deficit o[ PF.~. 6. Clot retraction might be defective.
In addition, deficiencies of plasma cofactors prob,'ibly necessary for normal platelet function might conceivably affect any of the above stages.
DEFECTIVE ADHESION TO COLLAGEN
Hirsh and co-workers (8) have described a patient in whom the only abnormality appeared to be a striking defect in platelet adhesion to collagen associated with impaired platelet aggrega- tion by collagen. The bleeding time was prolonged and the tourniquet test positive. Other tests of platelet function, including platelet aggregation by ADP and PF 3 activity, were normal. Surprisingly, ADP release by collagen was normal. However, the
16

latter study was performed on platelets that had been washed, which may well have altered their behavior.
Similar observations were made by Vigliano and Horowitz (11) in their study of a patient with IgA myeloma in whom the bleeding time was prolonged and in vivo platelet adhesive-
ness greatly diminished. Connective tissue exposed to the pa- tient's plasma apparently became coated with the abnormal protein and failed to cause aggregation of either the patient's or normal platelets. In the absence of the myeloma protein, the patient's platelets were aggregated normally by connective tissue.
DEFECTS OF SECONDARY AGGREGATION
(Defective "Release" Reaction)
Attention recently has been focused on an increasing number of patients in whom a bleeding disorder appears to result from the failure of platelets to release ADP (12-14). Whereas exogenous ADP at high concentrations causes platelets from these patients to aggregate, secondary aggregation by low con- ccntrations of ADP, by epinephrine and by connective tissue is defective. In other words, amplification of the aggregating stimu- lus (see above) fails to occur. As noted in Table 3, this type of platelet defect occurs in a variety of clinical contexts.
CONGENITAL DEFECTS.----In many patients, the disorder ap-
TABLE 3.--DEFECTS OF SECONDARY PLATELET AGGREGATION
1. Congenital (usually familial) 2. Acquired
(a) Following drug ingestion: aspirin dipyridamole glyeeryl guaiacolate Persantine Robitussin etc.
(b) In renal failure (c) In liver disease (d) In fibrinolytic states
17

pears to be an inborn error of platelet function. Subjects have ranged in age from 11 months to 45 years but, in many of the adults, a bleeding tendency had been noted since childhood. Both sexes have been affected, with a slight female preponder- ance. In many instances, a definite familial incidence has been demonstrated. It is almost certain that a variety of inheritance patterns will emerge.
For the most part, the bleeding tendency has been mild. Curiously, bruising is more common than petechial hemorrhage. Prolonged bleeding from superficial cuts, epistaxis, menorrhagia and excessive bleeding following tooth extraction have been frequent findings. In some patients, childbirth, tonsillectomy, appendectomy and other operations have occurred without inci- dent, whereas severe postoperative hemorrhage has complicated the course of others. Hemarthrosis has not been reported. In some instances, bleeding has occurred only after the ingestion of drugs, such as aspirin, that are known to inhibit platelet aggrega- tion (see below).
The bleeding time has been moderately prolonged in the majority of patients reported, although Hardisty and Hutton (14) found it to be normal in nearly half of their cases. The tourniquet test has been positive in many instances. Platelet adhesiveness, as measured either in vivo or in vitro, may be diminished or normal. There have been no abnormalities of platelet number or morphology.
A variety of aggregation tests have been performed. The most striking and constant defect has been a failure of aggregation (as opposed to adhesion, which is normal) in response to collagen or connective tissue extract. ADP, when used in low concentra- tions, reveals a failure of secondary aggregation. At high concen- trations, aggregation occurs but the rate of disaggregation is more rapid than normal. Aggregation by thrombin has been defective in some patients but not in others.
Many patients of this type manifest deficient platelet factor 3 activity (12-14). That defective release of endogenous platelet ADP and other substances is, however, the primary abnormality in most, if not all, such patients is suggested by the finding that release was abnormal in all of 7 patients so investigated (12- 14).
Now that tests of platelet aggregation are being performed
18

more commonly, patients whose platelets demonstrate defects of secondary aggregation and "release" are being detected with increasing frequency. I tdoes not seem unwarranted to predict that this disorder (or group of disorders) ultimately will prove to be the most common single cause of a congenital bleeding diathesis. The majority of persons who suffer from "easy bruising" may well fall into this category.
IMPAIRMENT OF PLATELET FUNCTION BY DRUGS.--Interac- tion between platelets and a variety of drugs, a phenomenon recognized only recently, may have great clinical significance. Among these drugs, aspirh~ has been most extensively studied. Its main action appears to be the inhibition of the platelet release reaction. Following its ingestion (or in the presence of aspirin in vitro), release of intrinsic ADP does not occur. As a result, the second wave of aggregation in response to epinephrine or low concentrations of ADP is abolished and aggregation by connec- tive tissue is inhibited (Fig. 3). Release of epinephrine, PF4 and serotonin does not occur either and, as might be anticipated, PF 3 availability is subnormal. Platelet response to large amounts of exogenous ADP is unaffected, as are aggregation by thrombin (except at very low concentrations) and adhesiveness to glass beads.
It is of considerable interest that as little as 150 mg. of aspirin ingested as a single dose will induce these changes, and that they may persist for as long as 1 week. The effect of aspirin appears to be mediated by a chemical interaction between the drug and the platelet membrane in which the acetyl group is incorporated into the platelet. Sodium salicylate, lacking the acetyl group, is ineffective,
The bleeding times of normal subjects are slightly increased following aspirin ingestion (15). In subjects with von Wille- brand's disease, or with severe hemophilia, or in patients receiv- ing anticoagulants, however, a much more striking prolongation may occur (15, 16). In such persons, aspirin ingestion may precipitate severe hemorrhage. In vivo experiments in animals have demonstrated that aspirin markedly inhibits primary hemo- stasis. Other anti-inflammatory drugs have also been found to affect this aspect of platelet function. Phenylbutazone (100 mg.) taken orally usually produced an effect similar to that of aspirin. In a few instances, indomethacin (100 mg.) caused a striking
]9
but transient (4 hours) effect. Ibuprofen (300 mg.) produced minor, transient changes. Acetaminophen (Tylenol) and dextro- propoxyphene (Darvon) have recently been demonstrated to be without effect on platelet aggregation and may be presumed to be relatively safe in hemorrhagic states.
Phenylbutazone and sulfinpyrazone have been shown not on ly to inhibit platelet aggregation but also to prolong the bleeding time of transected mesenteric vessels. It has also been main- tained that these compounds, and aspirin as well, prolong the survival time of circulating platelets, but the significance of the latter finding is presently controversial.
Glyceryl guaiacolate, a compound included in a number of remedies used to treat diseases of the respiratory tract, has been shown to inhibit ADP-induced platelet aggregation when taken either as a single dose of 100 or 200 mg. orally, or at a dosage schedule of 100-200 mg. every 6 hours for 1 week (17). Several authors have noted that adhesiveness of platelets to glass in the presence of added ADP is diminished following administration of this drug.
Dipyridamole (Persantine), a coronary vasodilator, has been shown to inhibit ADP-induced aggregation of human platelets and to prevent thrombus formation in experimental animals (18). The frequency of thromboembolic complications following the implantation of cardiac valve prostheses may be significantly reduced by prolonged treatment with this drug (19). In a single controlled trial of its effects in acute myocardial infarction, dipyridamole appeared to be without benefit/in preventing complications or death (20). A recent study has indicated an advantageous effect of this drug in the modification of the vascular lesions of rejection in cadaveric renal allografts.
Adrenergic blockels such as phentolamine, which are specific for alpha receptors, inhibit secondary platelet aggregation but not the release reaction per se. They are presumed to act by preventing catecholamines released from the platelets them- selves from potentiating the aggregation reaction. Relatively few studies on the effects of alpha adrenergic blockers on human platelets in vivo have been carried out.
Dextran of intermediate molecular weight when given intra- venously causes a significant prolongation of the bleeding time, decreases platelet adhesiveness and diminishes the sensitivity of
20

platelets to ADP and other aggregating stimuli (21). Presum- ably, dextran acts by interacting with the platelet membrane, but the mechanism must be different from that of other agents mentioned in this section, for the compound is ineffective in vitro and requires about 6 hours to achieve its maximal effect during in vivo administration.
Other drugs. The effects of a very large number of com- pounds when incubated with platelets in vitro have been studied, and various sites and modes of action have been demonstrated and postulated. A great deal of information pertaining to platelet function and behavior has been obtained, and this has been reviewed in considerable detail by Michal and Firkin (22). Compounds that inhibit platelet function at very low concentra- t ions-s imi lar to those that may be attained in vivo---and that, therefore, deserve further study of their usefulness as inhibi tors of platelet function include tranquilizers (chlorpromazine), anti- histaminics (diphenhydramine) and antidepressants (amitripty- line).
CLINICAL SIGNIFICANCE OF DRUG-PLATELET INTERACTIONS. --Considerable attention has been paid to this new and rapidly expanding field because of its potentially very great significance in a number of clinical areas. These may be briefly summarized as follows:
a) Use o/ drugs ]or the prevention o] thromboembolic dis- ease.--Many studies indicate that formation of a "white," or platelet, thrombus almost invariably is the initiating event in the formation of an arterial thrombus. The potential value of drugs that inhibit platelet aggregation for the prevention of arterial thrombosis is self-evident. The few clinical studies thus far performed appear promising. Many more trials using a variety of drugs are currently under way and additional clinical informa- tion should be forthcoming.
b) Potentiation o] a bleedh~g diathesis by antiplatelet drugs. - - F r o m quite another aspect, consideration must be given to the possibility that certain drugs that are ordinarily innocuous may be highly dangerous if administered to patients with a pre- existing bleeding tendency. The potentially lethal effect of aspirin in patients with severe hemophilia has been referred to earlier. It is probable that drugs that inhibit the platelet release reaction
21

should also be withheld from patients receiving coumadin or heparin, from those with liver failure sufficiently severe to affect coagulation parameters, from patients with thrombocytopenia and from patients who have gastrointestinal bleeding or who are candidates for any type of surgery. Accordingly, it is of great importance that the full spectrum of drugs capable of affecting platelet function be identified and that their clinical effects in the above conditions be more fully defined.
c) Potentiation o] thrombosis by drugs that enhance platelet aggregation.--Epinephrine, even in physiologic concentrations, is known to increase the sensitivity of platelets to ADP. The possible relationship of this mechanism to the occurrence of coronary thrombosis under conditions of stress requires further study. Of drugs commonly used for pharmacologic purposes, only estrogens have been implicated as enhancing the sensitivity of platelets to ADP (10). It is apparent that further studies in this area are warranted.
PLATELET DEFECTS IN RENAL FA1LURE . - -A b o u t a third of patients with advanced renal failure--whether acute or chronic --have a bleeding tendency, usually manifested by purpura and" ecchymoses, easy bruisability and epistaxis. In a small number of the patients there may be gastrointestinal or genitourinary tract bleeding.
There is now a large body of evidence which suggests that a qualitative platelet defect underlies this bleeding state. The Ivy bleeding time frequently is prolonged, although often only mini- mally so. Platelet aggregation by an "optimal" concentration of ADP was found to be markedly impaired in all 0 f 7 uremic patients studied by Castaldi, Rozenberg and Stewart (23), indicating that the platelet release reaction isimpaired. Dimin- ished platelet adhesiveness has also been a str!king feature (24), and clot retraction has been found to be impaired in a number of instances. PFa activity often is reduced, and was, in fact, the first qualitative platelet defect to be described in patients with renal failure.
Impairment of these various function tests has correlated fairly well with clinical manifestations of bleeding in uremic patients, and it has been suggested that the Ivy bleeding time, platelet adhesiveness tests and prothrombin consumption tests should precede renal biopsy or other operative procedures in
22

these patients. Tests of secondary aggregation may well prove to be the most sensitive parameters of platelet dysfunction in such individuals.
Platelet dysfunction in patients with uremia may be due to some metabolite of urea metabolism, as the observed abnormali- ties can be reproduced in normal subjects by the ingestion of large quantities of urea (25) but cannot be produced by in vitro incubation of platelets with urea. Guanidinosuccinic acid, a metabolite of urea, has been implicated in one study. Regardless of its cause, abnormal platelet function can be corrected, or at least improved, in many cases by either peritoneal dialysis or hemodialysis. Complete, permanent correction, however, can be �9 achieved only by successful transplantation.
PLATELET DYSFUNCTION IN LIVER DISEASE.--Bleeding is common in liver disease and, as is well recognized, may result from local gastrointestinal lesions, depletion of coagulation fac- tors synthesized by the liver, enhanced fibrinolytic activity or thrombocytopenia. A few reports have stressed, in addition, the occurrence of functional disorders of the platelet in both acute and chronic liver disease. The frequency with which such defects have been detected has varied in different laboratories, and has ranged from 15 to 70%.Earlystudies record a deficiency of PFa activity. More recently, Thomas, Ream and Stuart (26) have described impaired platelet aggregation in response to ADP and thrombin. It is probable that in the patients having reduced PF:~ activity the underlying mechanism is one of impaired ADP release and an impairment of secondary aggregation. It is of interest that diminished platelet aggregation was observed only in patients with excessive fibrinolysis, and it seems possible that fibrin and fibdnogen breakdown products released by fibrinolysis are the cause of the impaired platelet function.
EFFECT OF FIBR1NOGEN (AND FIBRIN) DEGRADATION PROD- UCTS (FDP) ON PLATELET FUNCTION.--In a variety of pri- mary or secondary fibrinolytic states, fibrin and fibrinogen are digested by the proteolytic enzyme plasmin. As a result, a number of degradation products (FDP) are formed that differ in molecular weight, in electrophoretic mobility and in their bio- logic effects. Apart from their powerful anticoagulant activity, they also exert a significant influence on platelet function. It is particularly the earlier degradation products that are effective in
93

this regard and, as the fragments become smaller with continued digestion, they lose this action.
"Early" FDP are capable of inhibiting the release of ADP and serotonin by platelets exposed to thrombin or connective tissue. Not unexpectedly, therefore, aggregation by thrombin, by con- nective tissue and by ADP is also impaired. Platelet adhesion to connective tissue, and to glass, is diminished as well.
It is believed that FDP may act to impair platelet function by competitive inhibition of fibrinogen, a compound accepted by most as a necessary factor for the aggregation process.
Excessive fibrinolytic activity may occur in a number of clinical circumstances. It usually is secondary to some other disease process---e.g., cirrhosis of the liver. Hence, the conclu- sion that it may be the presence of FDP that is responsible for the abnormal platelet function noted in liver disease. Dissemi- nated intravascular coagulation is also accompanied by secon- dary fibrinolysis, and inhibition of platelet function by FDP may be a major cause of the bleeding that characterizes this disorder.
DEFECTS OF PRIMARY PLATELET AGGREGATION
In 1918, Glanzmann recorded the occurrence of purpura in subjects with normal platelet counts but manifesting the in vitro phenomenon of defective clot retraction. This he intuitively ascribed to a platelet disorder, which he termed "thrombasthe- nia." It has since been established that the outstanding character- istic of the disease is a total failure of platelets to aggregate in response to any concentration of ADP or any other stimulus.
The clinical manifestations of this extremely rare disorder and its laboratory diagnosis have been well documented. The nature of the platelet defect has not been completely elucidated.
The disease is familial and appears to be inherited as an autosomal recessive trait. Bleeding symptoms appear at an early age and are characterized by bleeding from skin and mucous membranes. Extensive bruising, purpura, prolonged bleeding from cuts, and following tooth extraction, epistaxis and menor- rhagia may all be prominent manifestations.
The bleeding time, especially when performed by the Ivy method, is almost always prolonged. The platelet count usually is
24
normal. Examination of a peripheral blood smear will reveal platelets of normal size and appearance, and in normal num- bers, but will, if examined carefully, provide the important clue that the platelets are isolated and do not form aggregates. The clotting time is normal, but clot retraction usually is totally lacking. Impaired clot retraction may be the only abnormality in the heterozygous state. Platelets from patients with Glanzmann's disease will adhere to connective tissue and collagen, and will manifest the release reaction on exposure to these materials or thrombin. None of these compounds, however, is capable of inducing aggregation. Activation of platelet factor 3 is also defec- tive, emphasizing again the requirement of prior aggregation for PF 3 release.
A large number of electron microscopic and biochemical abnormalities have been described, but none is pathognomonic. A reduced platelet fibrinogen content has been a frequent finding, and the distribution of the fibrinogen among the various platelet components is said to be altered. Other abnormalities of platelet protein composition have been detected by immunologic methods.
DEFECTS OF PLATELET FACTOR 3 ACTIVITY ("The Thrombocytopathies")
As noted above, PF:~ activity is derived from a phospholipid component of the platelet, probably in the membranous portion of the cell, where it exists in a relatively inert state. As p!atelets undergo the release reaction, some change in platelet configura- tion unmasks or activates PFa activity, making it available to participate at two points in the coagulation cascade (Fig. 2).
Numerous reports in the literature describe patients with apparent deficiencies of PF:,. In some, the deficiency could be corrected if platelets were artificially disrupted by hypotonic lysis or by repeated freezing and thawing before being used in coagulation tests.
With the recognition that platelet "release" and activation of PF 3 go hand in hand, a re-evaluation of patients originally reported as having an isolated deficiency of PF3 is indicated and may reveal that in many, perhaps even most, the primary abnormality is failure of the release mechanism. Accordingly, a
25

detailed review of the rather confusing literature on thrombocy- topathies would be untimely and the subject will be dealt with only briefly.
In most patients thought to have a deficiency of PFz, bleeding symptoms have been mild, as in the case of patients with defects of platelet release (see above). Many family groups have been described in whom bleeding manifestations appeared at an early age (27). Inheritance has variably been described as autosomal or sex-linked recessive. In most, the bleeding time has been prolonged. In other reports, PF z deficiency appeared to be acquired in the course of some other illness, such as renal or hepatic failure or macroglobulinemia.
One fairly well defined group in which deficiency of PF z may be an isolated abnormality is characterized by the presence of giant platelets, 2-10 times normal size, having an abnormal ultrastructure (28). The disorder is familial. Many of the patients have mild to moderate thrombocytopenia.
DEFECTIVE CLOT RETRACTION
Of the disorders discussed thus far, only patients with Glanz- mann's disease have defective clot retraction. A single patient has been described in whom impaired clot retraction apparently is due to the congenital absence of a previously unrecognized plasma cofactor necessary for the retraction process.
DEFICIENCIES OF PLASMA COFACTORS REQUIRED FOR PLATELET FUNCTION
With the exception of the single patient just noted who appears to lack a plasma protein necessary for clot retraction, only patients with severe congenital deficiency of fibrinogen have been shown to have platelet malfunction due to a congenital plasma abnormality. In such individuals, the bleeding time is prolonged and platelet adhesion, platelet aggregation and PF3 release are greatly impaired. All the abnormalities can be corrected by addition of fibrinogen in vitro or by the infusion of fibrinogen in vivo. In the light of these studies and others showing that fibrinogen is a necessary cofactor for platelet
26
adhesion and aggregation, it is possible to make a strong case for platelet dysfunction in these patients being secondary to the deficiency of plasma fibrinogen. Whether apparent platelet dys- function in other disorders (such as yon Willebrand's disease) is due to deficiency of other as yet unrecognized plasma factors is presently conjectural.
DEFECTIVE PLATELET PHAGOCYTOSIS
For completeness, the Wiskott-Aldrich syndrome may be mentioned as illustrating a type of platelet dysfunction quite different from the others discussed above. The disorder is characterized by thrombocytopcnia, which usually is mild, eczema and a stisceptibility to infection, which usually results in death at an early age.. The chief abnormality appears to be an immunologic one: failure to recognize and to produce antibodies against polysaccharide antigens. Platelets from patients with this disorder are smaller than normal and have been shown by electron microscopy to lack the alpha granules typically found in normal platelets. An intrinsic platelet defect results in a marked- ly reduced survival time of these platelets. Aggregation by ADP, collagen and epinephrine is impaired. PF 3 activity is diminished. A striking abnormality is the lack of platelet citric acid cycle stimulation in the presence of latex particles. The primary functional abnormality of such platelets may thus be a total inability to "phagocytize" particulate material--an energy-re- quiring process, and one dependent on oxidative phosphorylation (7). What connection, if any, this extraordinarily interesting defect may have with the inability of such patients to combat infection requires further investigation. .
I I I . Thrombocytopenia BLEEDING IN THROMBOCYTOPENIC STATES
Controversy regarding the mechanisms by x~'hich platelets function in hemostasis notwithstanding, clinicians are well aware that diminished platelet levels are associated with a tendency to bleed. Even in the absence of external bleeding there may be an increase in capillary permeability. For example, erythrocytes are
27

commonly found in the thoracic duct lymph of thrombocyto- penic animals.
In man, the most frequent manifestation of thrombocytopenia is petechial hemorrhage. Showers of such lesions, pinhead-size extravasations of blood, are most commonly seen on the distal upper and lower extremities, where venous pressure is greatest, but may appear anywhere. In Negroes, they are extremely difficult to detect in the skin and should be sought in the conjunctivae and oral mucosa. Coalescence of multiple petechiae results in the more extensive, purple-hued discoloration of the skin usually designated "purpura." "Ecchymoses" occur in deeper tissues, usually in areas subject to trauma. Bleeding into joints is extremely rare. Retinal hemorrhage, too, is most unusual but occurs on occasion in patients who are also anemic. Gastrointestinal and urinary tract bleeding is not uncommon in severely affected patients, but the possibility that a tumor, ulcer or other lesion may be associated should not be overlooked. Hemorrhagic bullae within the mouth are seen only when platelet levels are extremely low--less than 5,000 per cu. mm. in most instances.
Spontaneous bleeding rarely occurs in patients whose platelet concentrations are greater than 50,000 per cu. mm. Below this level, the severity of bleeding is, generally speaking, inversely related to the platelet concentration. Yet there is gt'eat variation in the bleeding manifestations of different patient s with the same degree of thrombocytopenia. For example, we have seen a patient with idiopathic thrombocytopenic purpura (ITP) whose platelets ranged from 2,000 to 4,000 per cu. mm. for more than a year without a single major bleeding episode, and another who
TABLE 4.--FACTORS THAT ]~IAY AFFECT BLEEDING TENDENCY IN THRO~,~BOCYTOPENIC PATIENTS
l. Platelet age Newly formed platelets more effective in hemostasis
2. Infiltrative disease Predisposes to hemorrhage (especially acute leukemia)
3. Fibrinolysis Potentiates bleeding 4. Inhibitors of platelet Drugs especially dangerous in patients
function with thrombocytopenia? 5. Corticosteroids Act directly to enhance vascular integrity?
28

has had only occasional nosebleeds despite a platelet concentra- tion of 10,000 per cu. ram. for nearly 20 years. Patients with acute leukemia, on the other hand, all too commonly have fatal intracranial hemorrhage when platelet levels are as high as 20,000 per cu. mm. (29).
A number of factors probably are responsible for the lack of an absolute correlation between platelet levels and the tendency to bleed. Among the most important are those listed in Table 4, each of which is discussed separately, below, with respect to its possible role in potentiating or preventing hemorrhage in throm- bocytopenic patients.
FACTORS THAT MAY AFFECT THE TENDENCY OF TIIROMBOCYTOPENIC PATIENTS TO BLEED
1. PLATELET AGE.--It is now recognized that platelets under- go striking biochemical and structural changes during their stay in the circulation. In particular, they lose the capacity to synthesize protein, become depleted of phospholipid, glycogen and adenosine triphosphate (ATP), diminish in size and, per- haps most importantly, aggregate less readily than when they were newly formed (30-32). That aging of platelets is accom- panied by a general decrease in their hemostatic effectiveness is indicated by studies showing that, at a given platelet level, the bleeding time is considerably shorter when a young population of platelets is circulating than when platelets of average age are present (33). This observation may explain, at least in part, why bleeding is relatively uncommon in patients with thrombocyto- penia due to accelerated platelet destruction where there is a high proportion of newly produced platelets, yet occurs rather frequently in patients in whom thrombocytopenia is due to defective platelet production and in whom the age distribution of circulating cells is, consequently, normal. The suggestion has also been made that platelets newly released from the marrow spend I or 2 days in the spleen before venturing into the peripheral blood (33). This may explain why the bleeding tendency of thrombocytopenic patients sometimes is reduced by splenectomy even though there may be little or no change in platelet levels.
2. INFILTRATIVE DISEASE.I-That infiltrative disease should
29

predispose to bleeding is hardly surprising. This appears to be particularly true of patients with acute leukemia in whom a lesion consisting of perivascular cuffing of malignant cells in the brain and meninges appears to be associated with a high probability of intracranial hemorrhage. Prophylactic transfusion of platelets to maintain levels in excess of 20,000 per cu. mm. while attempting to induce remission with chemotherapy has been advocated (29).
3. FIBRINOLYSIS.--It is not widely recognized that fibrinolysis may markedly potentiate hemorrhage in thrombocytopenic states. The most definitive studies on this point are those of Salmon (34), who showed (in rats) that neither thrombocyto- penia nor fibrinolysis alone caused bleeding but that the combi- nation of the two resulted in a striking hemorrhagic tendency. In more limited studies, similar observations were made in human subjects (34). The reason for this is by no means clear. Fibrinogenl which is an important constituent of the platelet surface and which is necessary for normal platelet adhesiveness and aggregation, can be attacked by the fibrinolytic enzyme plasmin. Alternatively, split products of plasma fibrinogen, known to be potent inhibitors of platelet function (Section II), may be responsible for the observed effects. Whatever the mechanism, more attention should perhaps be paid to the possible deleterious effects in thrombocytopenic patients of drugs, exercise, excitement and other stimuli that may activate fibrinolysis. From an experimental standpoint, the possible value of fibrinolytic inhibitors such as c-aminocaproic acid in prevent- ing hemorrhage in thrombocytopenic subjects ma3? be worthy of consideration.
4. INHIB1TORS OF PLATELET FUNCTION.--Many drugs in common clinical use--such as aspirin and antihistaminics (Sec- tion II ) - -are known to affect platelet function by inhibiting the release reaction, in some cases for as long as a week after a single dose. The effects of such drugs in potentiating the bleeding tendency of severe hemophiliacs is dramatic (15). Although controlled studies are not yet available, it is reasonable to expect that the administration of such drugs to patients who are already thrombocytopenic may be extremely hazardous. As the spec- trum of drugs that inhibit platelet function is broad (Section II) and has not yet been fully defined, all drugs not absolutely
30

essential for the patient's welfare should, in our opinion, be withdrawn from thrombocytopenic individuals.
5. CORTICOSTEROIOS.--Finally, the possible usefulness of ad- renal cortical steroids in treating thrombocytopenic patients deserves brief mention. In idiopathic thrombocytopenic purpura (ITP), the value of steroids is unquestioned, as they adt to inhibit sequestration of antibody-coated platelets in the sl~leen, thus prolonging their life span and relieving the thrombocytope- nia. Not uncommonly, however, a decrease in capillary fragility and a shortening of the bleeding time occur even before there has been a significant change in platelet levels (35). The same improvement occasionally is seen in patients with other types of thrombocytopenia.
Whether the apparent enhancement of capillary integrity is due to a direct effect of corticosteroids on the vessels themselves has not yet been ascertained. The clinical impression that corticosteroids reduce the bleeding tendency of thrombocytopen- ic patients is widely held, however, and their use, at least in small doses, in thrombocytopenic states of diverse etiology is advocated by many clinicians.
APPROACH TO THE PATIENT x, VITH THROMBOCYTOPENIA
Like the anemias, thrombocytopenic disorders may be con- veniently classified into those due to insufficient platelet produc- tion and those resulting from premature platelet destruction (Table 5). In addition, tbrombocytopcnia may be due to pooling or sequestration of platelets in some special portion of the circulation, as in patients with splenomegaly and "hypersple- nism." PIatelet depletion also occurs in patients transfused with large quantities of stored blood because of the inability of the bone marrow to respond acutely to removal of circulating platelets. A detailed description of tile various thrombocytopenic disorders listed in Table 5 is beyond the scope of this discussion, and only the general approach to the patient with thrombocyto- penia will be considered.
HISTORY.--In patients with a history of bleeding going back to childhood, one of the hereditary thrombocytopenias should be considered, but these are quite rare (36). When thrombocyto- penia is of recent onset, inquiry should be made about exposure
31

to drugs or other potential toxins that may lower platelet levels by several different mechanisms (Table 5) . Quinine, present in certain soft drinks and patent remedies, and quinidine account for the great majority of immunologic drug-induced thrombocy- topenias. More common, however, is thrombocytopenia due to ingestion of thiazide diuretics or alcohol, both of which proba- bly act by suppressing platelet production. In children, viral in- fections such as rubella, chickenpox or, more often, nonspecifie upper respiratory infections, often precede the onset of acute "idiopathic" thrombocytopenic purpura.
TABLE 5.----TilE TItROMBOCYTOPENIAS
I. Due to De/ec t ive or Decreased Platelet Product ion
A. Congenital l. Amegakaryocytic thrombocytopenia with congenital
malformations 2. Aplastic anemia (Fanconi's syndrome) 3. Deficiency of thrombopoietin? 4. Hereditary thrombocytopenias 5. Myelophthisic disease (congenitalleukemia) 6. Rubella 7. Secondary to maternal ingestion of thiazide diuretics
B. Acquired 1. Aplastic anemia 2. Ionizing radiation, radiomimetic drugs 3. Myelophthisic disease (carcinoma, leukemia) 4. Drugs that inhibit platelet production
(thiazides?, estrogens, alcohol) 5. Cyclic thrombocytopenia 6. Nutritional deficiency (B1._,, fotic acid) 7. Paroxysmal nocturnal hemoglobinuria
II. Due to Increased Platelet Des truc t ion A. Congenital
1. Nonimmune a) In erythroblastosis fetalis b) Infection (cytomegalic inclusion disease, syphilis,
toxoplasmosis) c) Thrombocytopenia-hemangioma (Kasabach-Merritt)
syndrome 2. Immune.
a) Maternal drug sensitivity (quinine, quinidine) b) Isoimmune neonatal thrombocytopenia c) Associated with maternal "'idiopathic" thrombocytopenic
purpura
32

TABLE 5.---TItE THROMBOCYTOPENIAS (Cont.) B. Acquired
1. Nonimmune a) Secondary to infection (e.g., gram-negative sepsis) b) Disseminated intravascular coagulation c) Hemolytic-uremic syndrome d) Thrombotic thrombocytopenic purpura (TTP) e) Drug-induced (ristocetin)
2. Immune a) Drug-induced (quinine, quinidine, stibophen, arsenicals) b) Post-transfusion purpura c) "Idiopathic" thrombocytopenic purpura
i) acute (postinfectious) ii) chronic
III. Due to Abnormal Distribution o] Platelets
1. "Hypersplenic" thrombocytopenia 2. Hypothermia
IV. Due to Loss o] Platelets
1. Multiple transfusions with stored blood 2. Cardiac bypass
PHYSICAL EXAMINATION.----The bleeding stigmata of throm- bocytopenia are discussed above. An enlarged spleen in a patient with reduced platelets should suggest the possibility of tubercu- losis or other granulomatous disease, lymphoma or lupus erythe- matosus. Most commonly, however, splenomegalic patients have "hypersplenic" thrombocytopenia due to pooling of platelets in the enlarged organ (37) . Cavernous hemangiomas in infants and, less commonly, in older children and even adults may cause thrombocytopenia, probably due to coagulation within the tu- mor. Diagnosis may be especially difficult when the lesion involves the liver or spleen and may be aided by detection of a bruit over the enlarged organ.
LABORATORY FINDINGS.---The importance of routinely exam- ining blood smears for the presence of platelets cannot be overemphasized. All too often, thrombocytopenia is discovered only after several weeks of hospitalization, because platelets were not specifically lookcd for on admission.
The bleeding time, although useful in patients with qualitative platelet defects or von Willebrand's disease, serves only to
33

confirm what is already known in patients with severe thrombo- cytopenia and is rarely necessary. Moreover, bleeding from the incision may be prolonged and distressing to the patient. Occa- sionally, it may be of value to use the bleeding time to confirm the beneficial effects of corticosteroids or platelet transfusions. In this case, the Ivy rather than the Duke method should be used, as the former is more sensitive and pressure can be applied more conveniently after completion of the test.
White blood cell changes consistent with infection should be specifically sought because thromboeytopenia is particularly common in patients with gram-negative sepsis and may occur in the absence of any other coagulation abnormalities (38) . Men- ingococcemia, in particular, often presents with thrombocytope- nia and purpura and occasionally is diagnosed as "idiopathic" thrombocytopenia with disastrous consequences.
Red cells should be examined specifically for microangiopath- ic changes (Fig. 4) , the presence of which may suggest the diagnosis of thrombocytopenia-fiemangioma syndrome, dissemi-
FIG. 4.--Microangiopathic red cell changes of the type seen in patients with the thrombocytopenia-hemangioma syndrome, thrombotic throm- bocytopenic purpura or disseminated intravascular coagulation. (From R. P. Propp and W. B. Scharfman, Blood 28:623, 1966.)
g, 7o 34
nated intravascular coagulation or thrombotic thrombocytopenic purpura. Coagulation studies are of great importance in all patients with thrombocytopenia of unknown etiology because disseminated intravascular coagulation, which may occur in a wide variety of clinical settings, is one of the most common causes of reduced platelet levels in adults. Typically, fibrinogen and factors V and VIII are subnormal, the thrombin time, partial thromboplastin time and prothrombin time are pro- longed, and products of fibrinogen and fibrin breakdown are present in the plasma.
Platelet antibodies reacting with quinidine may be detected in patients with drug-induced thrombocytopenia. Inhibition of clot retraction in a mixture of normal blood, the patient's serum and the suspected drug is the simplest bedside technic (39), but negative test results do not rule out sensitivity.
A bone marrow aspiration is a most important diagnostic procedure because, generally speaking, the presence of normal or increased numbers of megakaryocytes indicates that throm- bocytopenia is due to accelerated platelet destruction, whereas a marked decrease indicates inadequate platelet production. Meg- akaryocytes in patients with thrombocytopenia due to premature platelet destruction, and particularly in those with idiopathic thrombocytopenic purpura, often are less granular, more baso- philic and smoother in contour than those of normal marrow and, consequently, often are described as "nonbudding." It is now generally recognized that these changes are due to the relative immaturity of such cells or to the premature release of platelets rather than to any intrinsic abnormality.
Studies of platelet survival time are not of paramount impor- tance for diagnosis in most instances but are helpful in selected cases. As shown in Figure 5, three different patterns are observed using 51Cr-labeled cells: (1) normal recovery and survival of transfused platelets in patients with a production defect, (2) shortened survival in patients with accelerated platelet destruction and (3) low recovery and normal or nearly normal life span in patients with "hypersplenism." Autologous platelets may be labeled in patients with platelets greater than 20,000 per cu. mm. (40) and are much to be preferred over isologous platelets, the life span of which may be shortened by isoantibodies stimulated by pregnancy or previous transfusion.
35

I00
80
60
i... 40 ba
201
0
~.,,.
"~.Q Normal ITP . . f
' ~ "-.. gypetsplenism
2 4 6 8 I0 12
DA YS
Fxo. 5.--Typical platelet survival pattern of a normal subject (or a sub- ject with defective platelet production), a patient with accelerated platelet destruction (ITP) and a patient with "hypersplenism."
IV. Thrombocythemia and Thrombocytosis
Platelet counts in excess of normal are encountered in a variety of clinical circumstances (Table 6). In all instances, the increase appears to be due to an accelerated rate of platelet production rather than to prolongation of platelet life span.
The term "thrombocythemia" often is used to describe a marked and persistent elevation of the platelet coun't occurring as part of a myeloproliferative disorder. Thromb0cythemia may be complicated either by an abnormal bleeding state or by thromboembolism.
"Thrombocytosis," on the other hand, refers to a more moderate, usually short-lived and symptomless platelet elevation that occurs in association with certain specific underlying disease processes.
It may be that thrombocythemia is a form of neoplasia involving the megakaryocyte line that makes these cells unre- sponsive to normal regulatory influences. In thrombocytosis, however, regulating mechanisms may be at least partially opera- tive (41) .
36

TABLE 6.--CAUSES OF ELEVATION OF PLATELET COUNT*
Thrombocylhenlia Essential (primary) thrombocythemia Polycythemia vera Myelofibrosis Chronic myelogenous leukemia
Thrombocytosis Postsplenectomy Postoperative (51) Postpartum Post-traumatic Infection Carcinoma (50) Iron deficiency Acute blood loss Hemolytic anemia Pernicious anemia in remission Hodgkin's disease Rheumatoid arthritis Ulcerative colitis
*References supplied on request.
A detailed review of the regulation of platelet production is beyond the scope of this report. For further information on this subject, the reader may refer to some recent reports (41-43) .
TIIROMBOCYTHEMIA.--An elevated platelet count may occur as an isolated phenomenon, "essential hemorrhagic thrombocy- themia," but more often features of polycythemia vera, myelofi- brosis or chronic myeloid leukemia are also present. Occasional- ly, the disorder seems to be precipitated by splenectomy per- formed in the course of a myeloproliferative disorder.
Gastrointestinal bleeding is common in patients with throm- bocythemia, as are spontaneous bruising, massive hematoma formation, epistaxis, menorrhagia and prolonged bleeding fol- lowing tooth extraction, minor trauma or at operation (44) . Venous thrombosis and thromboembolism have also been noted and, recently, attention has been drawn to the occurrence of transient ischemic attacks, strokes, myocardial infarction, mes- enteric thrombosis and peripheral gangrene.
It is well known that at extremely high concentrations plate- lets may impede the generation of thromboplastin in vitro. The
37
bleeding state sometimes seen in patients with thrombocythemia has, therefore, been ascribed to an anticoagulant effect of excessive platelet numbers. It seems probable, however, that platelet function may also be impaired, since defective secondary aggregation and diminished PF 3 activity have been described in some patients with essential thrombocythemia, polycythemia vera and myelofibrosis (45), as have a prolongation of the bleeding time and diminished in vivo platelet adhesiveness.
Bleeding in these patients often may be controlled simply by lowering the platelet count. Alkylating agents or 3ephosphorus may be used for this purpose. Thrombocytopheresis recently has been advocated as a means for lowering the platelet count acutely in life-threatening situations (46). Correction of the disordered platelet function has been noted in the majority of patients following treatment with 3zp or myleran, but exceptions have been noted.
When thrombosis constitutes the major problem, treatment shoiald again be directed toward lowering the platelet count. The place of anticoagulants or, perhaps more pertinently, platelet- active drugs such as aspirin or dipyridamole is somewhat controversial but worthy of further consideration (47). One approach to this problem may be to study platelet function in patients with thrombocythemia prior to instituting therapy. In patients with thrombotic, rather than hemorrhagic, complica- tions, platelet function might well prove to be normal, or supernormal, with drug therapy strongly indicated.
THROMBOCYTOSIS.-----A number of disease states (Table 6) may be associated with an elevated platelet count; apparently as a secondary phenomenon.
The most consistent and significant elevations follow splenec- tomy. The rise in platelet count usually reaches a peak at the end of the second week and gradually subsides within the subsequent 3 months. In our experience, the maximal level has averaged 772,000 per cu. mm. It is exceptional for thromboembolism to occur in these circumstances, yet an extremely high platelet count becomes disturbing to the physician. Our own policy has been to administer heparin only on the rare occasions when platelet levels rise above 2,000,000 per cu. mm. unless the patient remains bed-ridden and is, therefore, a prime candidate for thrombosis. In the latter case, heparin is given if platelets rise
38

above 1,000,000 per cu. mm. Thromboembolic complications occurred in only 1 of our 32 spleneetomized patients. As no large, carefully controlled study of the relationship betv~en thrombosis, platelet levels and anticoagulant therapy has been carried out in such patients, it is impossible to recommend any firm guidelines.
In patients who remain anemic after splenectomy--especially if the operation was performed in the course of a sideroblastic or hemolytic anemia--the elevation in platelet count is likely to be more pronounced and persistent. This latter group seems to be particularly prone to develop thromboembolic complications (48). Elevation of hemoglobin concentration to normal by means of blood transfusion has been suggested as a means of lowering the platelet count at times when the risk of thrombosis is increased---e.g., should operation be necessary.
Splenectomy in the course of a myeloproliferative disorder is especially likely to be complicated by a profound elevation in platelet count, with serious risk of hemorrhage or thrombosis, and should not be performed without careful consideration (49).
Patients with carcinoma (50) and other disorders may, for unknown reasons, also have thrombocytosis (Table 6). The rise in platelet count is essentially asymptomatic, but may serve as a diagnostic clue.
Conclusion
Defects of either platelet number or function may underlie hemorrhagic or thrombotic states. Information regarding the precise details of platelet dysfunction in various diseases is accumulating rapidly and should make more effective forms of treatment possible. Of special importance is the observation that a wide variety of drugs may inhibit or potentiate platelet function. The clinical implications of such drug effects require further investigation, but their potential significance is great.
39
REFERENCES
1. Levin, J., and Bang, F. B.: A description of cellular coagulation in the limulus, Bull. Johns Hopkins Hosp. 115:337, 1964.
2. Luscher, E. F.: Current concepts of hemostasis. Progress report on platelet aggregation, Thromb., Diath., Haemorrh. (Supp.) 35:149, 1969.
3. Biggs, R., Denson, K. W. E., Riesenberg, D., and Mclntyre, C.: Coagulant activity of platelets, Brit. J. Haemat. 15:283, 1968.
4. Adelson, E., Rheingold, J. J., and Crosby, W. H.: The platelet as a sponge. A review, Blood 17:767, 1961.
5. Gimbrone, M. A., Aster, R. H., Cotran, R. S., Corkery, J., Jandl, J. H., and Folkman, J.: Preservation of vascular integrity in organs perfused in vitro with a platelet-rich medium, Nature, London 222:33, 1969.
6. Johnson, S. A., Balboa, R. S., Desel, B. H., Monto, R. W., Siegesmund, K. A., and Greenwalt, T. J.: The mechanism of the endothelial sup- porting function of intact platelets, Exper. & Molec. Path. 3:115, 1964.
7. Kuramoto, H., Steiner, M., and Baldini, M.: Lack of response to stimulation: A major defect in the platelets of the Wiskott-Aldrich syndrome, New England J. Med. 282:475, 1970.
8. Hirsh, J., Castelan, D. J., and Loder, P. B.: Spontaneous bruising associated with a defect in the interaction of platelets with connective tissue, Lancet 2:18, 1967.
9. Hellem, A. J.: Platelet adhesiveness, Seminars Hemat. 1:99, 1968. 10. Hampton, J. R., and Mitchell, J. R. A.: Effect of aggregating agents
on platelet electrophoretic behaviour, Brit. M. J. 1:1074, 1966. 11. Vigliano, E. M., and Horowitz, H. I.: Bleeding syndrome in a patient
with IgA myeloma: Interaction of protein and connective tissue, Blood 29:823, 1967.
12. Weiss, H. J.: Platelet aggregation, adhesion, and adenosine diphosphate release in thrombopathia (platelet factor 3 deficiency), Am. J. Med. 43:570, 1967.
13. Caen, J., Sultan, Y., and Larrieu, M.: A new familial platelet disease, Lancet 1:203, 1968.
14. Hardisty, R. M., and Hutton, R. A.: Bleeding tendency associated with "new" abnormality of platelet behaviour, Lancet 1:983, 1967.
15. Quick, A. J.; Acetylsalicylic acid as a diagnostic aid in hemostasis, Am. J. M. Sc. 254:392, 1967.
16. Kaneshiro, M. M., Mielke, C. H., Kasper, C. K., and Rapaport, S. I.: Bleeding time after aspirin in disorders of intrinsic clotting, New England J. Med. 281:1039, 1969.
17. Silverman, J. L., and Wurzel, H. A.: The effect of glyceryl guaiacolate on platelet function and other coagulation factors in vivo, Am. J. Clin. Path. 51:35, 1969.
18. Didisheim, P.: Inhibition by dipyridamole of arterial thrombosis in rats, Thromb., Diath., Haemorrh. 20:257, 1968.
19. Sullivan, J. M., Harken, D. E., and Gorlin, R.: Pharmacologic control of thromboembolie complications of cardiac-valve replacement, New England J. Med. 279:576, 1968.
40

20. Gent, A. E., Brook, C. G. D., Foley, T. H., and Miller, T. N.: Dipyridamole: A controlled trial of its effect in acute myocardial infarction, Brit. M. J. 2:366, 1968.
21. Weiss, H. J.: The effect of clinical dextran on platelet aggregation, adhesion, and ADP release in man: In vivo and in vitro studies, J. Lab. & Clin. Med. 69:37, 1967.
22. Michal, F., and Firkin, B. G.: Physiological and pharmacological aspects of the platelet, Ann. Rev. Pharmacol. 9:95, 1969.
23. Castaldi, P. A., Rozenberg, M. C., and Stewart, J. H.: The bleeding disorder of uraemia, Lancet 2:66, 1966.
24. Salzman, E. N., and Neri, L. L.: Adhesiveness of blood platelets in uremia, Thromb., Diath., Haemorrh. 15:84, 1966.
25. Eknoyan, G., Wacksman, S. J., Glueck, H. I., and Will, J. J.: Platelet function in renal failure, New England J. Med. 280:677, 1969.
26. Thomas, D. P., Ream, J. V., and Stuart, R. K.: Platelet aggregation in patients with Laennec's cirrhosis of the liver, New England J. Med. 276:1344, 1967.
27. Ulutin, O. N.: Primary thrombocytopathy, Israel J. M. Sc. 12:857, 1965.
28. Kanska, B., Niewiarowski, J., Ostrowski, L., Poplawski, A., and Prokopowicz, J.: Macrothrombocytic thrombopathia. Clinical, coagu- lation and hereditary aspects, Thromb., Diath., Haemorrh. 10:88, 1963.
29. Gaydos, L. A., Freireich, E. J, and Mantel, N.: The quantitative relationship between platelet count and hemorrhage in patients with acute leukemia, New England J. Med. 266:905, 1962.
30. Ginsburg, A. D., and Aster, R. H.: Changes associated with platelet aging, Clin. Res. 17:325, 1969.
31. Hirsh, J., Glynn, M. F., and Mustard, J. F.: The effect of platelet age on platelet adherence to collagen, J. Clin. Invest. 47:466, 1968.
32. Steiner, M., and Baldini, M.: Protein synthesis in aging blood platelets, Blood 33:628, 1969.
33. Shulman, N. R., Watkins, S. P., Itscoitz, S. B., and Students, A. B.: Evidence that the spleen retains the youngest and hemostatically most effective platelets, Tr. A. Am. Physicians 81:302, 1968.
34. Salmon, J.: Fibrinolyse et Pathologie Vasculaire (Brussels: Editions Arscia S. A. 1964).
35. Faloon, W. W., Greene, R. W., and Losner, G. L.: The hemostatic defect in thrombocytopenia as studied by the use of ACTH and cortisone, Am. J. Med. 13:12, 1952.
36. b, lurphy, S., Oski, F. A., and Gardner, F. H.: Hereditary thrombo- cytopenia with an intrinsic platelet defect, New England J. Med. 281:857, 1969.
37. Aster, R. H.: Pooling of platelets in the spleen: Role in the patho- genesis of "hypersplenic" thrombocytopenia, J. Clin. Invest. 45:645, 1966.
38. Corrigan, J. J., Walker, R. L., and May, N. M.: Changes in the blood
41

coagulation system associated with septicemia, New England J. b, led. 279:851, 1968.
39. Horowitz, H. I., and Nachman, R. L.: Drug purpura, Seminars Hemat. 2:287, 1965.
40. Aster, R. H., and Keene, W. R.: Sites of platelet destruction in idio- pathic thrombocytopenic purpura, Brit. J. Haemat. 16:61, 1969.
41. Harker, L. A., and Finch, C. A.: Thrombokinetics in man, J. Clin. Invest. 48:963, 1969.
42. Evatt, B. L., and Levin, J.: Measurement of thrombopoiesis in rabbits using 75selenomethionine, J. Clin. Invest. 48:1615, 1969.
43. Abildgaard, C. F., and Simone, J. V.: Thrombopoiesis, Seminars Hemat. 4:424, 1967.
44. Gunz, F. W.: Hemorrhagic thrombocythaemia: A critical review, Blood 15:706, 1960.
45. Spaet, T. H., Lejnieks, I., Gaynor, E., and Golstein, M. L.: Defective platelets irt essential thrombocythemia, Arch. Int. Med. 124:135, 1969.
46. Colman, R. N., Sievers, C. A., and Pugh, R. P.: Thrombocytopheresis: A rapid and effective approach to symptomatic thrombocytosis, J. Lab. & Clin. Med. 68:389, 1966.
47. Rodriguez-Erdmann, F., Goldberg, M. E., Davey, F., and Moloney, W. C.: Treatment of symptomatic thrombocythemia, New England J. Med. 281:854, 1969.
48. Hirsh, J., and Dacie, J. V.: Persistent post-splenectomy thrombo- cytosis and thromboembolism: A consequence of continuing anaemia, Brit. J. Haemat. 12:44, 1966.
49. Meilleur, P. A., and Meyer, M. C.: Thrombocytosis: A postsplenec- tomy complication in agnogenic myeloid metaplasia, Am. J. M. Sc. 241:110, 1961.
50. Levin, J., and Conley, C. L.: Thrombocytosis associated with malignant disease, Arch. Int. Med. 114:497, 1964.
51. Breslow, A., Kaufman, R. M., and Lawsky, A. R.: The effect of surgery on the concentration of circulating megakaryocytes and platelets, Blood 32:393, 1968.
49