plasma based biomarkers in advanced prostate cancer based biomarkers in advanced prostate cancer...
TRANSCRIPT
Plasma based biomarkers in
advanced prostate cancer
Gerhardt Attard MD MRCP PhD
Cancer Research UK Clinician Scientist and
Consultant Medical Oncologist
Treatment Resistance Group, Centre for Evolution and Cancer
The Institute of Cancer Research and
the Royal Marsden NHS Foundation Trust
Disclosures relevant to presentation
• Employee of the Institute of Cancer Research (ICR) that has
a commercial interest in abiraterone. I’m on The ICR
rewards to inventors list of abiraterone.
• PI for trials sponsored by Janssen, Medivation, Astellas,
Arno.
• Received:-
– Consulting fees and travel support from Janssen,
Astellas, Medivation, Essa, Arno, Sanofi.
– Speaker’s fees from Janssen, Astellas and Sanofi.
– Grant support from Janssen, AstraZeneca, Arno, Innocrin.
Plasma DNA studies in CRPC
• Cell-free DNA is invariably
present in plasma
• ctDNA (tumor) can constitute
<1% to >90% of total cfDNA
• Amenable to repeated and
real-time sampling
• Different processing required
for mRNA (eg AR-V7)

Clinical implementation of plasma DNA
In January 2015, the EMA extended the label of erlotinib to
include patients with detection of EGFR mutations in plasma DNA
Wan et al. Nat. Rev. Cancer 2017
Liquid biopsies in APC
Data shows strong associations with outcome in a
range of contexts,
but no evidence that patient outcome will be
improved or not harmed by using a liquid biopsy
test to choose treatment
Is the absence of data a justification for the use of
potentially inaccurate information?
Liquid biopsies in APC
Data shows strong associations with outcome in a
range of contexts,
but no evidence that patient outcome will be
improved or not harmed by using a liquid biopsy
test to choose treatment.
Is the absence of data a justification for the use of
potentially inaccurate information?
Or can we reach a consensus that liquid biopsy
tests should not be used to select patient treatment
outside the setting of a clinical trial?
Tu
mo
ur
Vo
lum
e a
nd
Ac
tivit
y
Local
therap
y
LHRH
analogue +/-
docetaxel
Abiraterone and
prednisolone/
Enzalutamide
Docetaxel
chemotherapy
Cabazitaxel
second line
chemotherapy
and/or trials
Castrate Sensitive Castrate Resistant Disease
Time
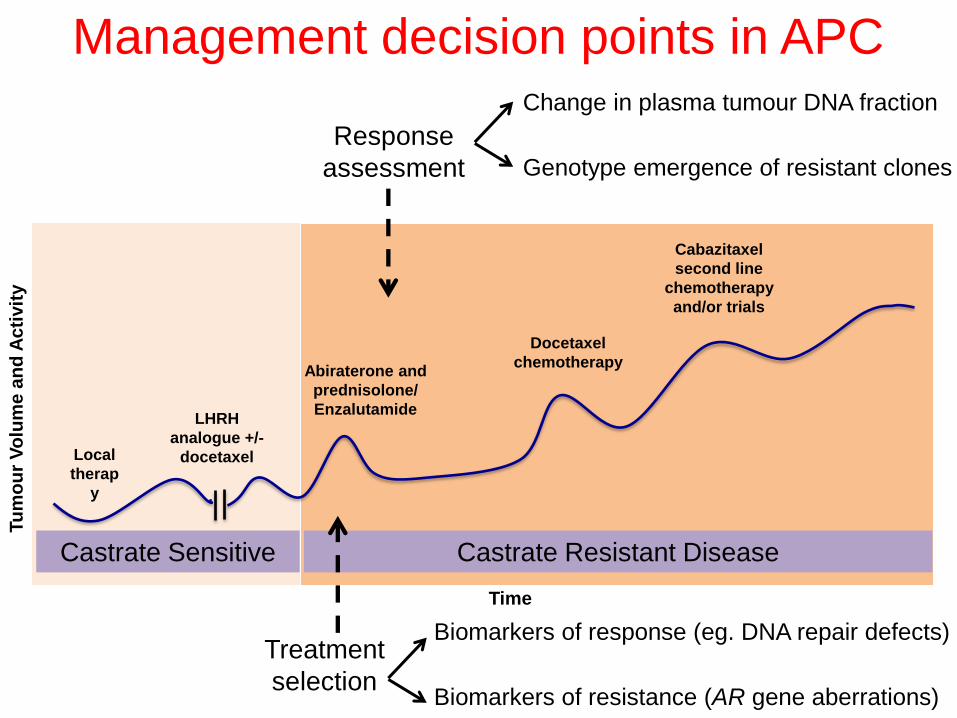
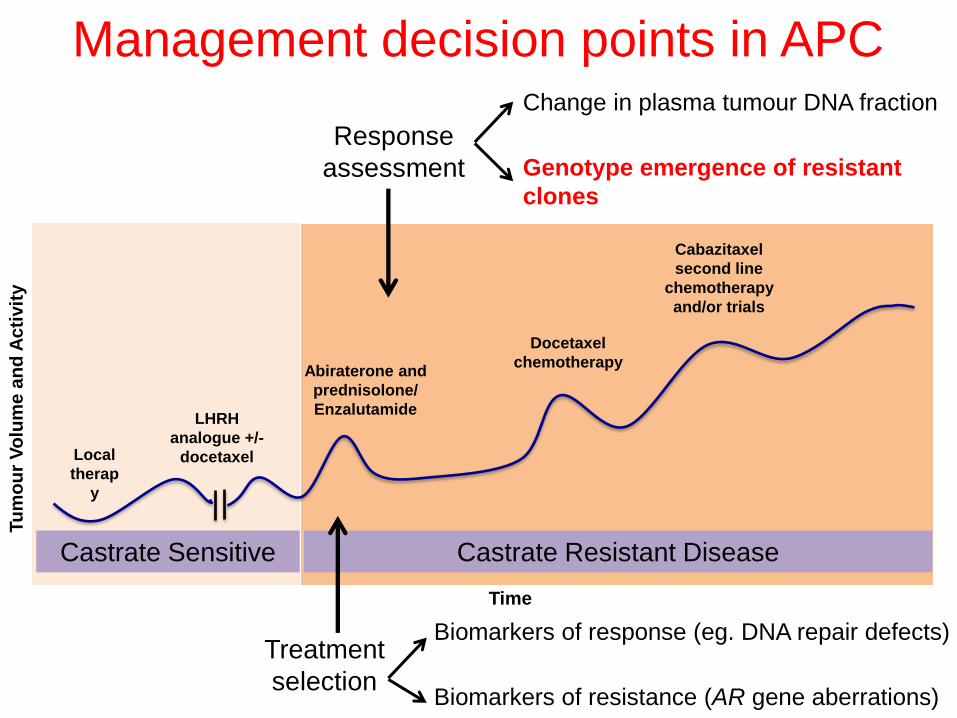
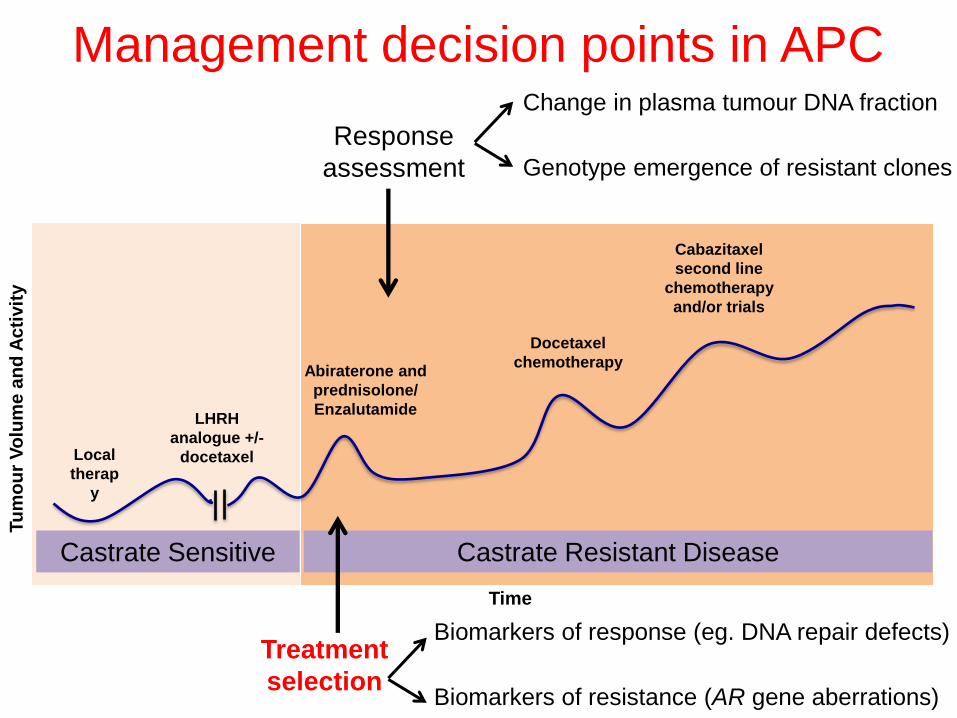
Management decision points in APC
Treatment
selection
Response
assessment
Biomarkers of response (eg. DNA repair defects)
Biomarkers of resistance (AR gene aberrations)
Change in plasma tumour DNA fraction
Genotype emergence of resistant clones

Quantitation of plasma tumour DNA fraction
Variable fraction of
normal DNA mixed with
DNA from multiple
heterogeneous tumour
clones
Accurate quantitation
of tumour DNA fraction
needed for:
Genotyping resistant
clones
Estimations of CNA
Treatment monitoring
Prognostication
Carreira, Romanel et al, Sci. Transl. Med. 2014; 254ra125

Tracking somatic CNA in plasma
Ulz et al, Nat. Commun. 2016, 22;7:12008
• Shallow Whole Genome Sequencing
• Can inform on ctDNA fraction
• Sensitivity dependent on magnitude of CNAs
• 60-80£/sample; 72 hours – 2 week turn around
• New focal AR amplification at progression on castration
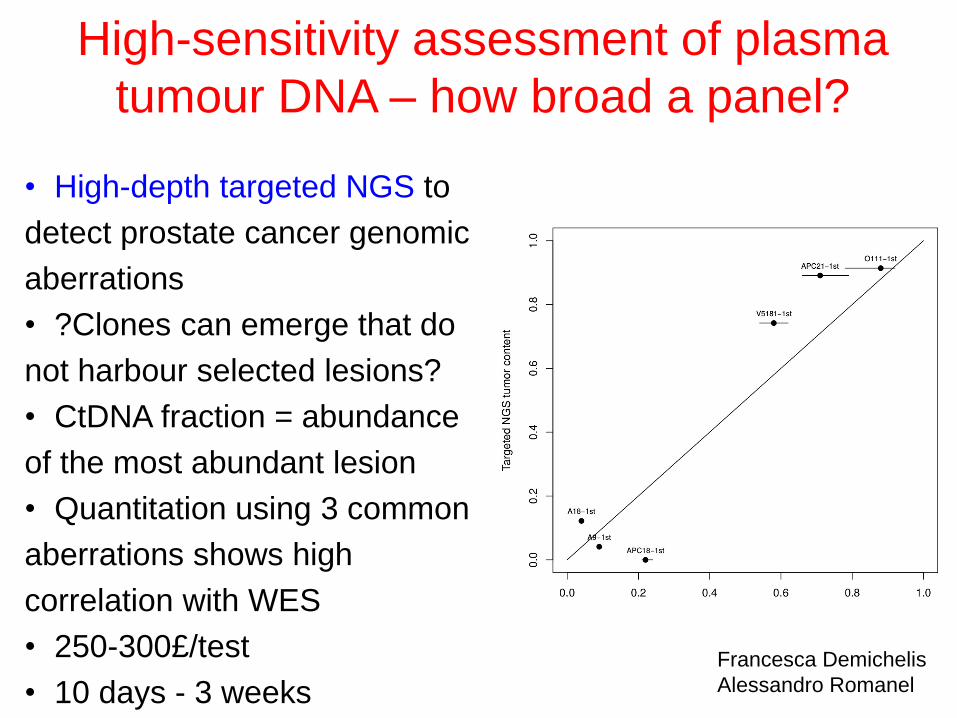
High-sensitivity assessment of plasma
tumour DNA – how broad a panel?
• High-depth targeted NGS to
detect prostate cancer genomic
aberrations
• ?Clones can emerge that do
not harbour selected lesions?
• CtDNA fraction = abundance
of the most abundant lesion
• Quantitation using 3 common
aberrations shows high
correlation with WES
• 250-300£/test
• 10 days - 3 weeks
Francesca Demichelis
Alessandro Romanel
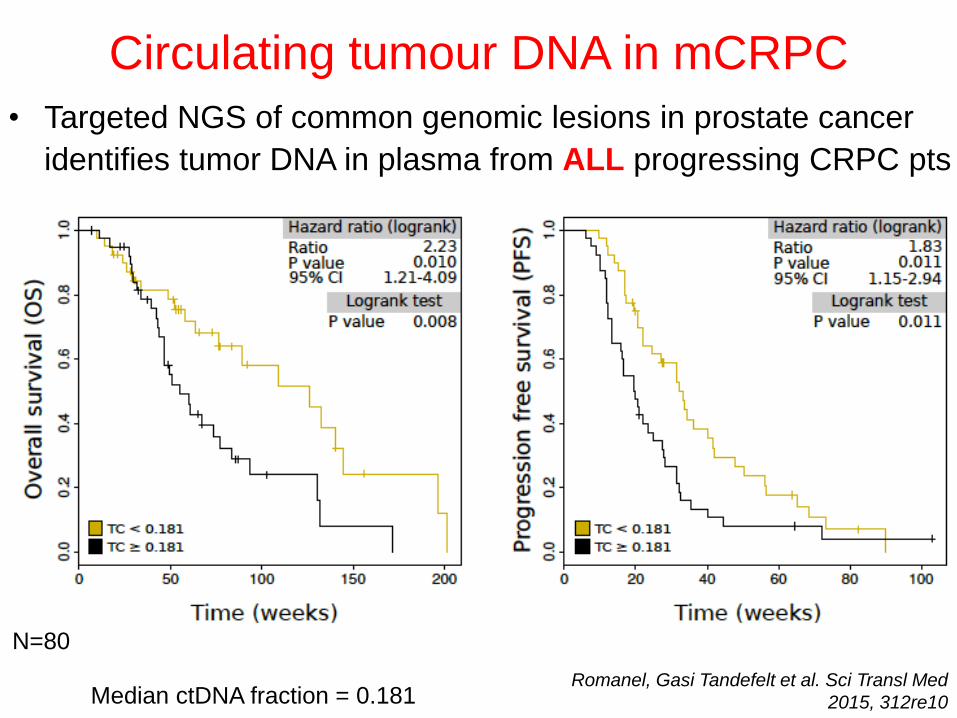
Circulating tumour DNA in mCRPC
Median ctDNA fraction = 0.181
• Targeted NGS of common genomic lesions in prostate cancer
identifies tumor DNA in plasma from ALL progressing CRPC pts
Romanel, Gasi Tandefelt et al. Sci Transl Med
2015, 312re10
N=80
21q
del
8p
del
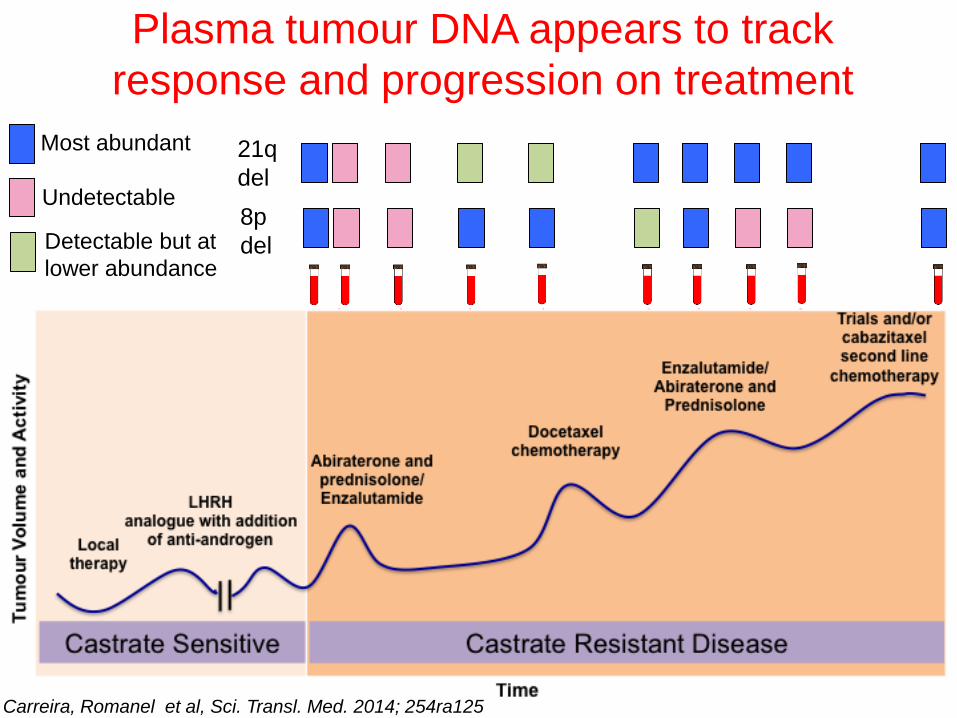
Plasma tumour DNA appears to track
response and progression on treatment
Most abundant
Undetectable
Detectable but at
lower abundance
Carreira, Romanel et al, Sci. Transl. Med. 2014; 254ra125
Tu
mo
ur
Vo
lum
e a
nd
Ac
tivit
y
Local
therap
y
LHRH
analogue +/-
docetaxel
Abiraterone and
prednisolone/
Enzalutamide
Docetaxel
chemotherapy
Cabazitaxel
second line
chemotherapy
and/or trials
Castrate Sensitive Castrate Resistant Disease
Time
Management decision points in APC
Treatment
selection
Response
assessment
Biomarkers of response (eg. DNA repair defects)
Biomarkers of resistance (AR gene aberrations)
Change in plasma tumour DNA fraction
Genotype emergence of resistant
clones
Days
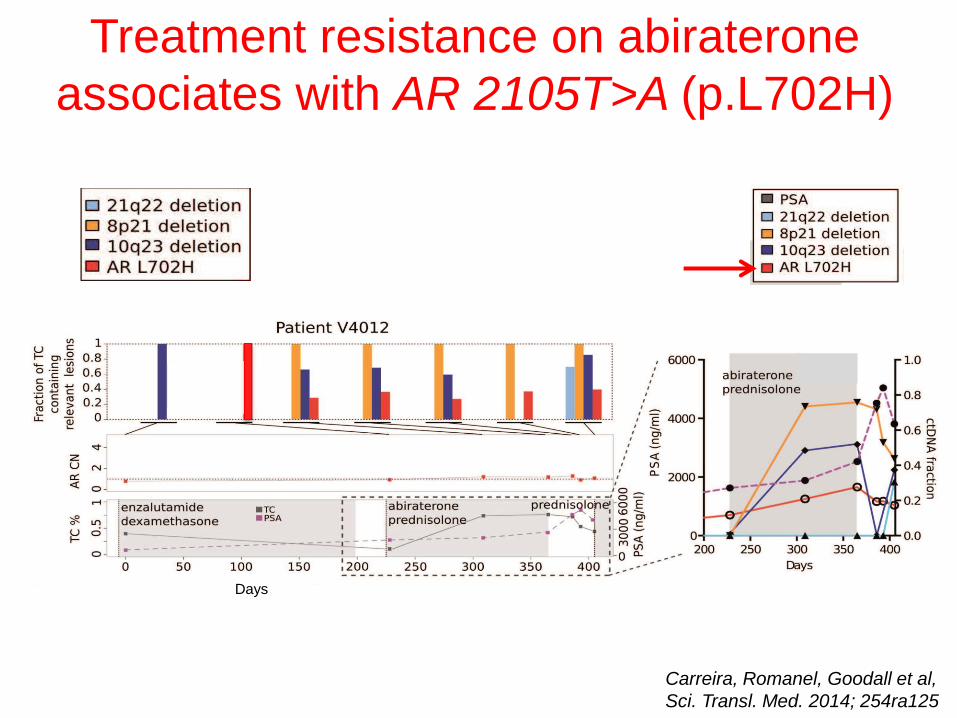
Treatment resistance on abiraterone
associates with AR 2105T>A (p.L702H)
Carreira, Romanel, Goodall et al,
Sci. Transl. Med. 2014; 254ra125
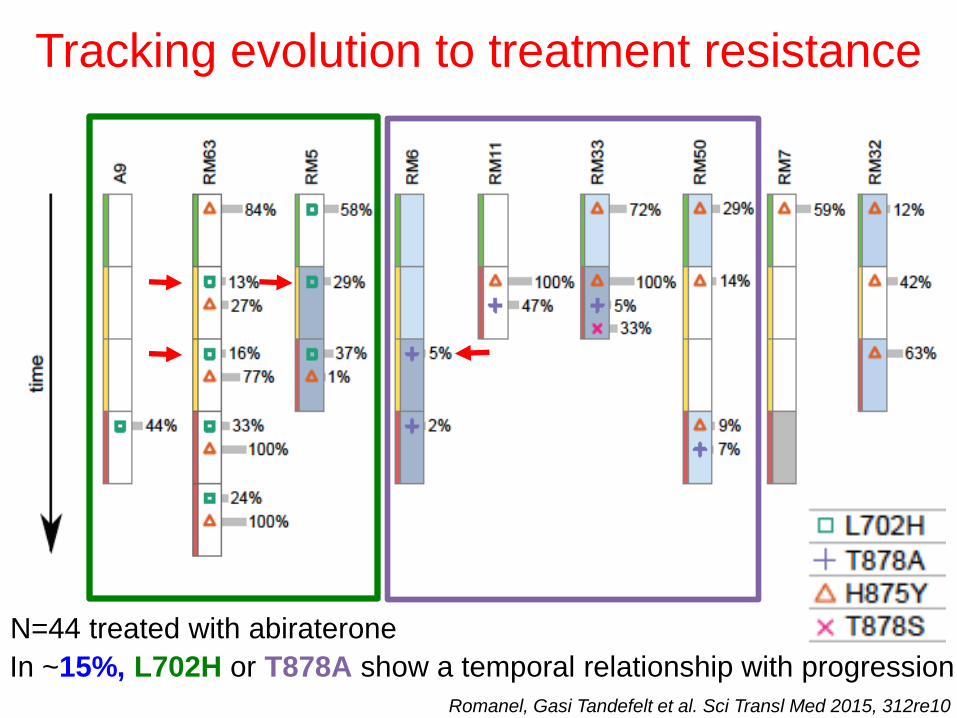
Tracking evolution to treatment resistance
In ~15%, L702H or T878A show a temporal relationship with progression
N=44 treated with abiraterone
Romanel, Gasi Tandefelt et al. Sci Transl Med 2015, 312re10
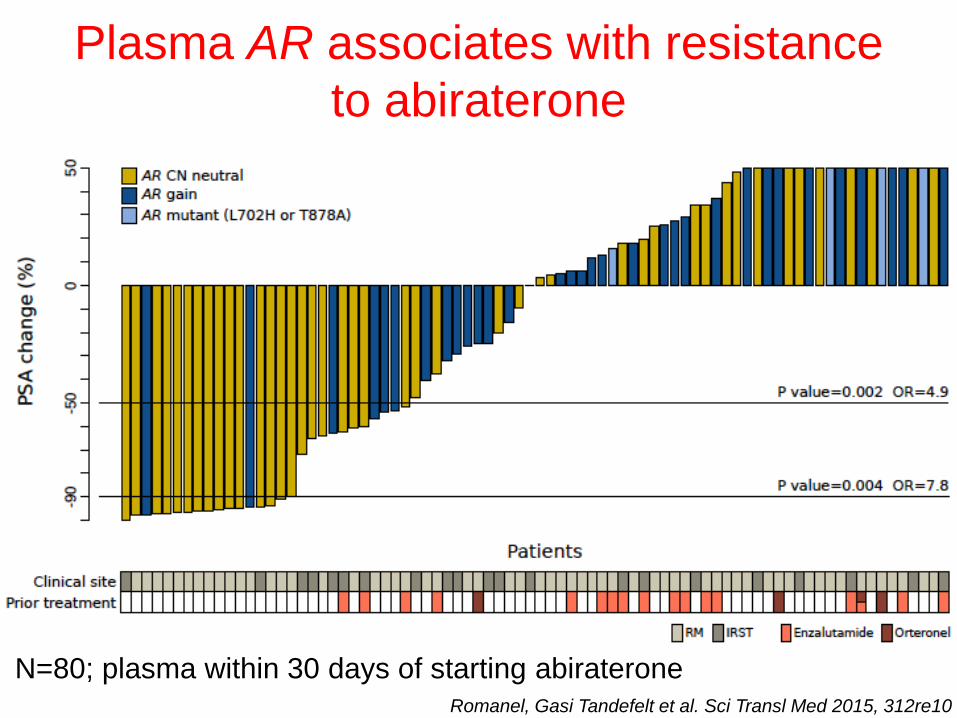
Plasma AR associates with resistance
to abiraterone
N=80; plasma within 30 days of starting abiraterone Romanel, Gasi Tandefelt et al. Sci Transl Med 2015, 312re10
Tu
mo
ur
Vo
lum
e a
nd
Ac
tivit
y
Local
therap
y
LHRH
analogue +/-
docetaxel
Abiraterone and
prednisolone/
Enzalutamide
Docetaxel
chemotherapy
Cabazitaxel
second line
chemotherapy
and/or trials
Castrate Sensitive Castrate Resistant Disease
Time
Management decision points in APC
Treatment
selection
Response
assessment
Biomarkers of response (eg. DNA repair defects)
Biomarkers of resistance (AR gene aberrations)
Change in plasma tumour DNA fraction
Genotype emergence of resistant clones
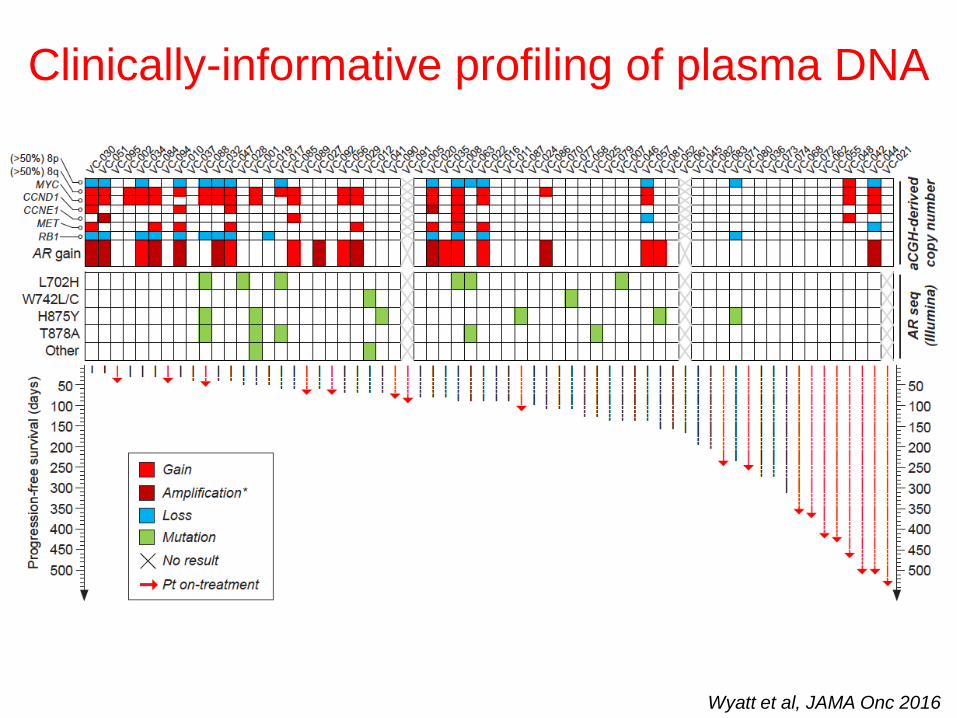
Clinically-informative profiling of plasma DNA
Wyatt et al, JAMA Onc 2016
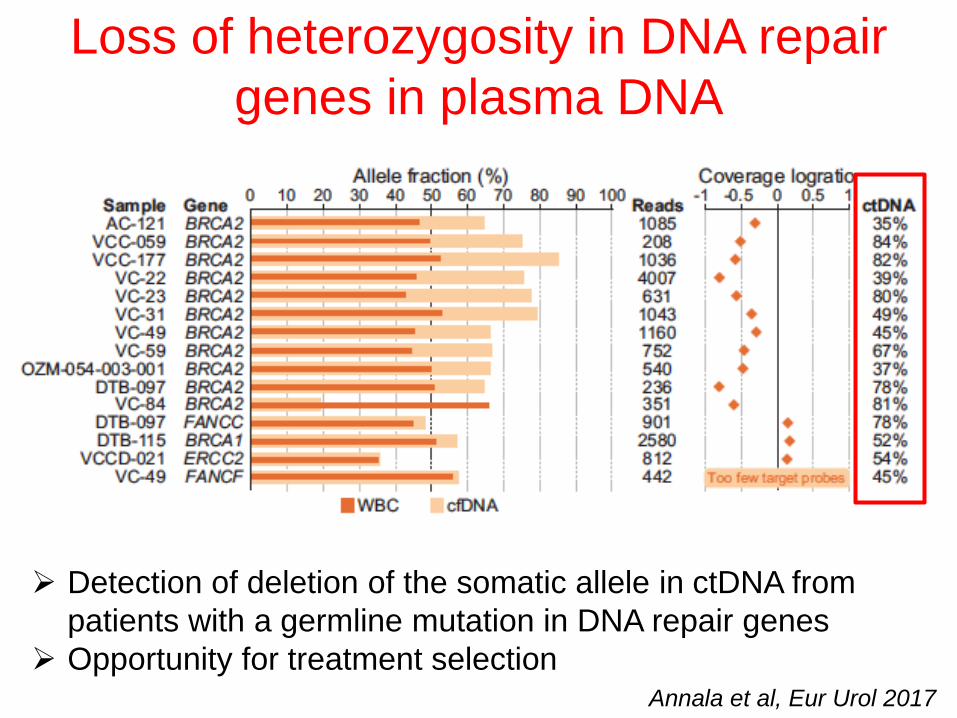
Loss of heterozygosity in DNA repair
genes in plasma DNA
Annala et al, Eur Urol 2017
Detection of deletion of the somatic allele in ctDNA from
patients with a germline mutation in DNA repair genes
Opportunity for treatment selection
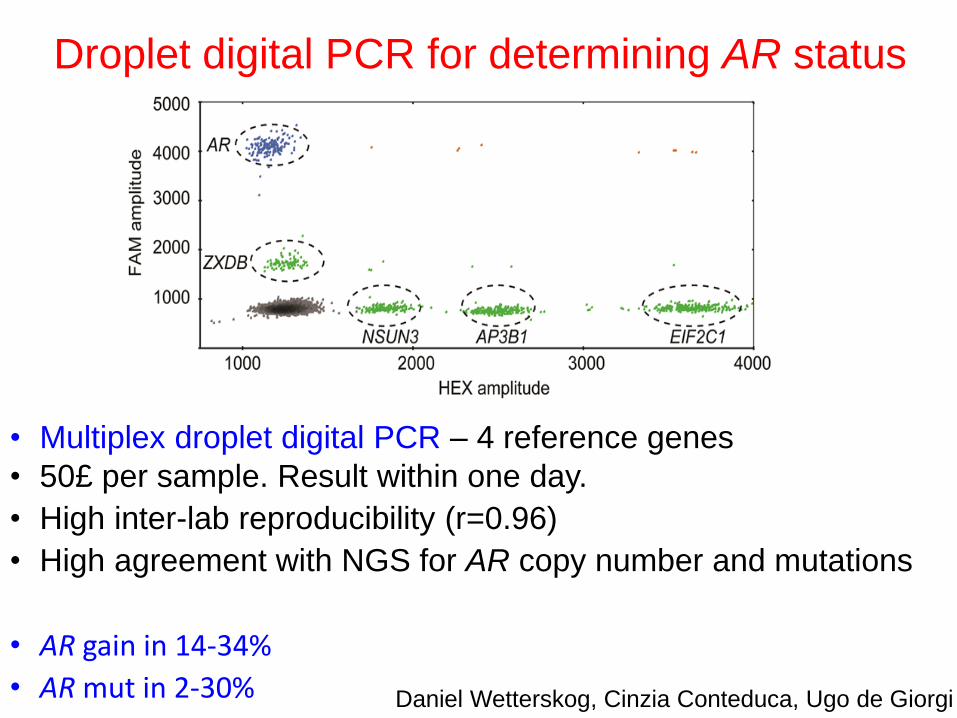
Droplet digital PCR for determining AR status
• Multiplex droplet digital PCR – 4 reference genes
• 50£ per sample. Result within one day.
• High inter-lab reproducibility (r=0.96)
• High agreement with NGS for AR copy number and mutations
• AR gain in 14-34%
• AR mut in 2-30% Daniel Wetterskog, Cinzia Conteduca, Ugo de Giorgi
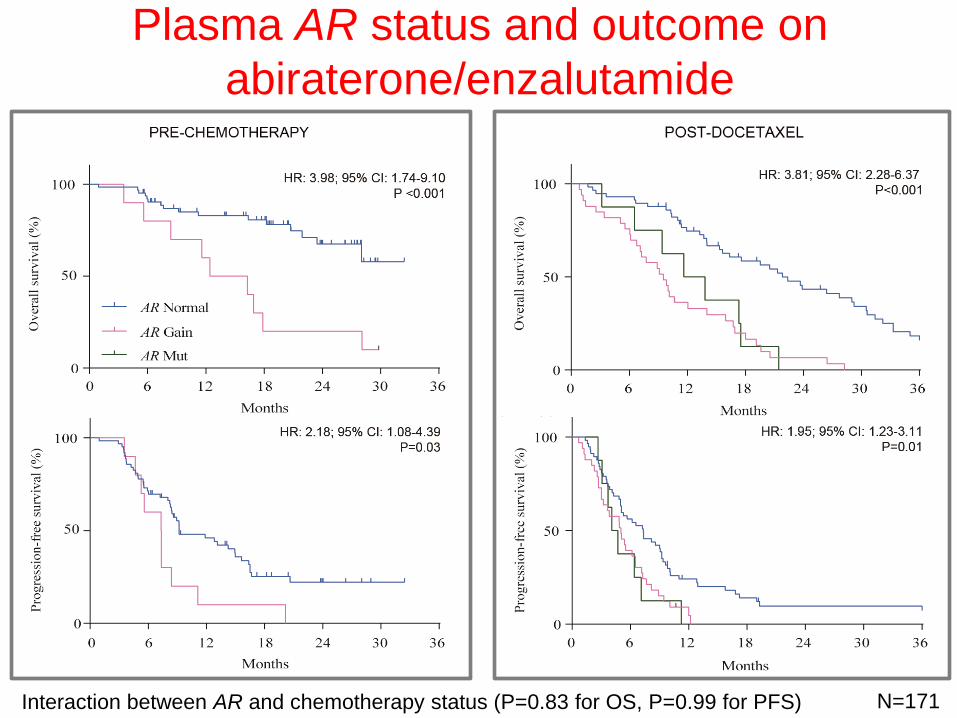
Plasma AR status and outcome on
abiraterone/enzalutamide
N=171 Interaction between AR and chemotherapy status (P=0.83 for OS, P=0.99 for PFS)
Qualification of plasma AR in PREMIERE trial
PREMIERE team:
Enrique Grande
María Piedad Fernández Pérez
Albert Font
Sergio Vázquez Estévez
Aránzazu González del Alba
Begoña Mellado
Ovidio Fernández Calvo
María José Méndez-Vidal
Miguel Angel Climent
Ignacio Duran
Enrique Gallardo
Angel Rodríguez
Carmen Santander
M Isabel Sáez
Javier Puente
Teresa Alonso
Julián Tudela
Alberto Martínez
Daniel Castellano
Enrique González Billalabeita
• Biomarker trial
• 98 mCRPC (PREVAIL criteria) treated
with enzalutamide in 16 Spanish
hospitals
• Plasma collected pre-treatment from 94
• Sponsored and conducted by the
Spanish
Genito-Urinary oncology Group (SOGUG)
• Support from Astellas
• Designed to analyze the predictive value
of TMPRSS2-ETS
• Included exploratory analyses of
associations with outcome for AR-V7
detected in CTCs* and plasma AR
*Grande E, Ann Oncol 2016;
27(Suppl 6): vi243-vi265
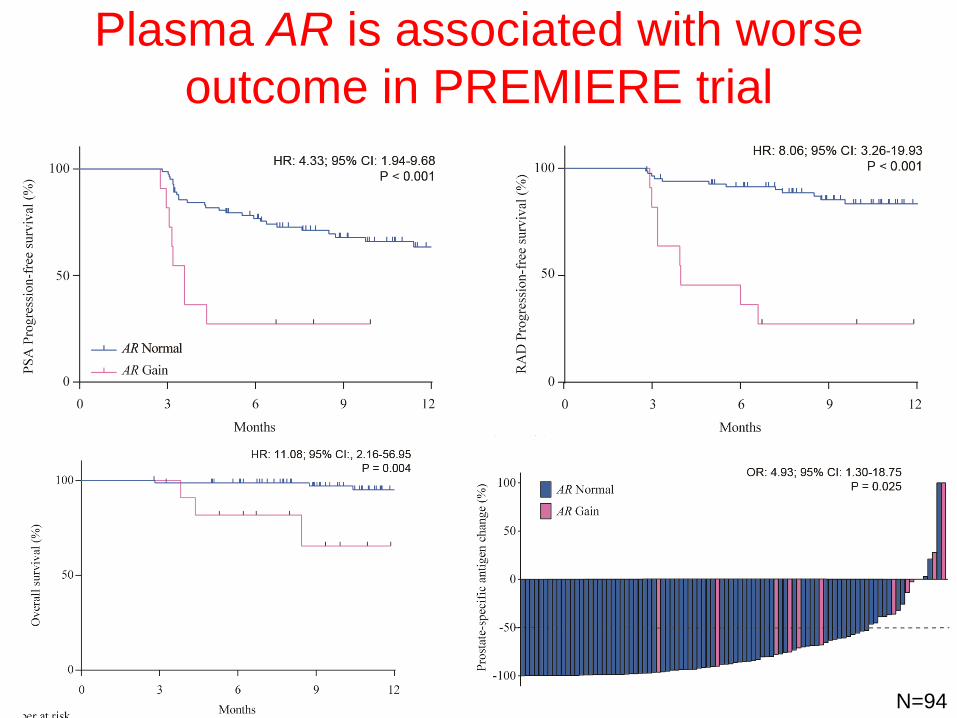
Plasma AR is associated with worse
outcome in PREMIERE trial
N=94

Future directions
• Collection of plasma in prospective trials
• Prospective trials to clinically qualify
associations with outcome
• Trials evaluating plasma DNA based treatment
selection
• Robust, analytically validated APC-specific NGS
assays
• Composite assays that include mRNA analysis
Future directions
• Collection of plasma in prospective trials
• Prospective trials to clinically qualify
associations with outcome
• Trials evaluating plasma DNA based treatment
selection
• Robust, analytically validated APC-specific NGS
assays
• Composite assays that include mRNA analysis –
overlap between AR CN and AR-V7
G Attard,
Marsden
K Chi,
Vancouver
M Rubin,
Cornell
F Demichelis,
Trento
E Van Allen,
DFCI C Maher,
Wash U
H Beltran,
Cornell
A Wyatt,
Vancouver A Armstrong,
Duke
PCF SELECT (Specific Evaluation in Liquid
biopsies of Established prostate Cancer Targets)
plasma DNA assay
To accelerate the development and achieve the implementation of a plasma DNA test for metastatic prostate cancer into widespread clinical practice within 5 years
• We recognize that each of our institutions is capable of establishing our own ctDNA assay for prostate cancer.
• However, by working together as a team we are best positioned to gain the widest acceptance for a community-relevant assay for advanced prostate cancer.
@PCF_SELECT
Aim 1: To design a prostate-cancer specific,
clinically-applicable targeted NGS panel optimised
for treatment selection and response surrogacy in
metastatic prostate cancer.
Aim 2: To develop and optimize the assay in a
central CLIA/CLEP approved molecular genomics
laboratory based on the consortium specifications.
Aim 3: To implement the assay at consortium sites
and collaborators to obtain stage 1 clinical
qualification in a range of scenarios and
interrogate biological and biomarker questions
@PCF_SELECT

Conclusions
• Using high-coverage NGS, circulating tumor DNA is
detected in plasma from all progressing mCRPC patients
• Plasma DNA is representative of clinically relevant
progressing metastases
• Plasma DNA could be used to select targeted treatment –
challenge of ctDNA fraction.
• Plasma AR copy number gain or mutations strongly
associate with worse outcome on abiraterone or
enzalutamide in both chemo-naïve and post-docetaxel
mCRPC
• Prospective evaluation of plasma-based treatment
decisions is now warranted and required to confirm clinical
utility