biomarkers in prostate cancer prostate cancer symposium the prostate net september 17, 2011 steven...
TRANSCRIPT
Biomarkers in Prostate Cancer
Prostate Cancer SymposiumThe Prostate Net
September 17, 2011Steven Lucas
Wayne State University School of MedicineKarmanos Cancer Institute
Why are Biomarkers Important
• Prostate Cancer diagnosed in 200,000 men annually in the united states
• 30,000 cancer specific deaths per year
• Yet, a substantial portion of cancers diagnosed through PSA screening do not progress to clinically significant disease.
Problem with PSA screening
• It is not specific, resulting in a negative biopsy rate of up to 70% in some series
• European randomized trial: 1410 men screened and 48 treated to prevent 1 death from prostate cancer
• Sweedish Randomized trial of watchful waiting:– Relative risk for surgery: 0.62 (0.44-0.87)– NNT 15 overall and 7 for men younger than 65y
How do we improve screening and treatment decisions?
• Clinical nomograms– Include Gleason Score, positive cores, percent
involvement of cores, and PSA– Other risk factors: family history, age, race
• Biomarkers– Supplement known clinical information
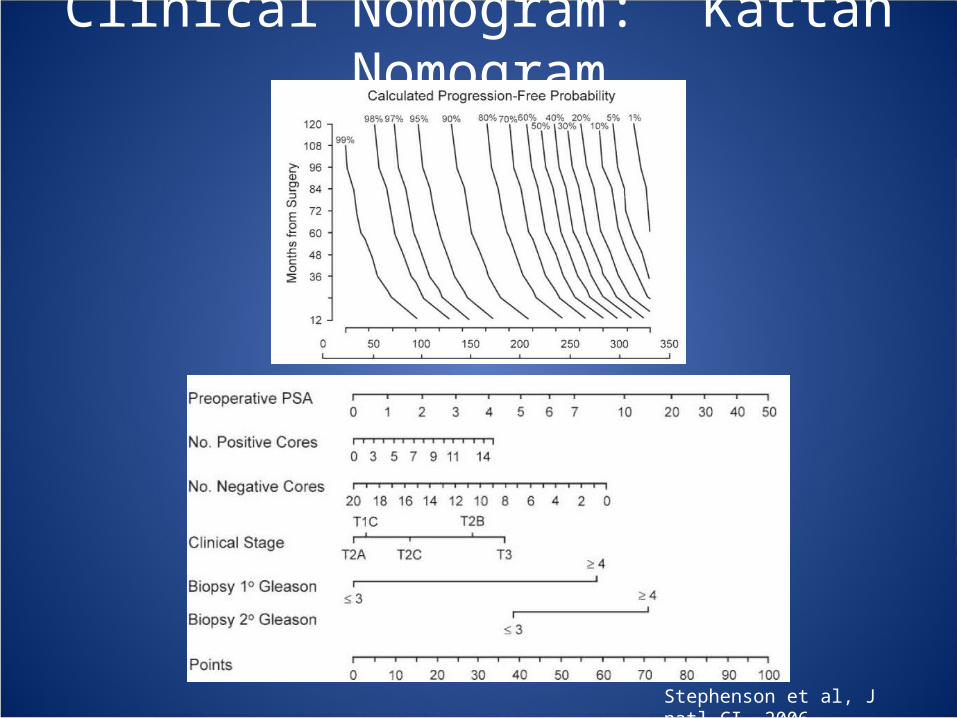
Clinical Nomogram: Kattan Nomogram
Stephenson et al, J natl CI, 2006

How can biomarkers improve management?
Categories of biomarkers
Urine Based Blood Based Tissu Based
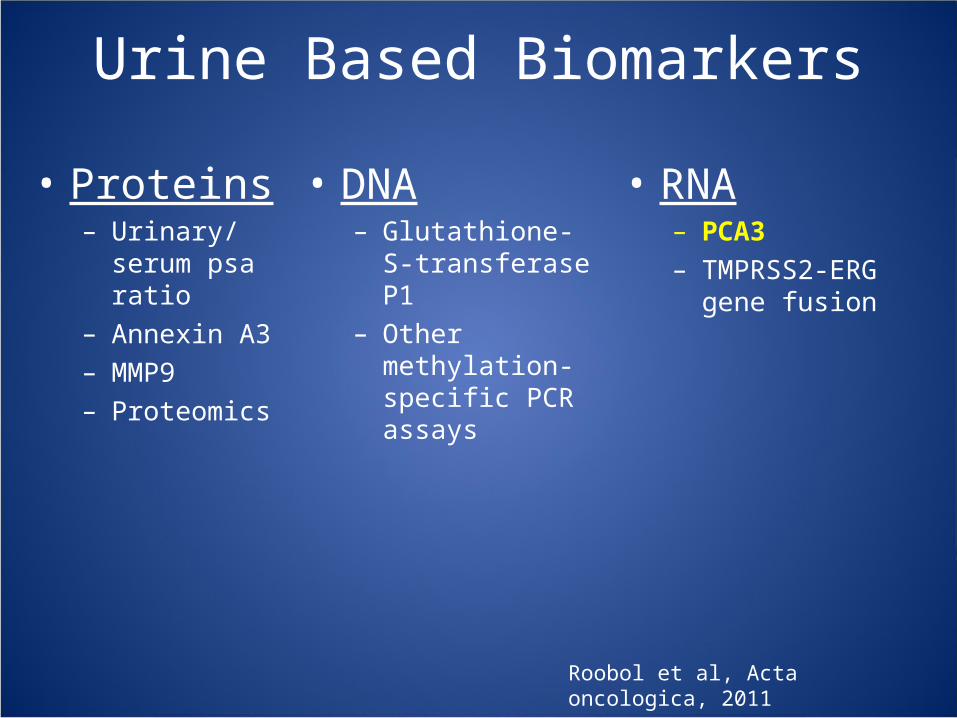
Urine Based Biomarkers
• Proteins– Urinary/serum
psa ratio– Annexin A3– MMP9– Proteomics
• DNA– Glutathione-S-
transferase P1– Other methylation-
specific PCR assays
• RNA– PCA3– TMPRSS2-ERG
gene fusion
Roobol et al, Acta oncologica, 2011
Urinary PCA3• Developed from differential expression of
noncoding RNA’s in prostate cancer versus other prostate conditions
• Commercially available, approved diagnostic test
• Collected from urine sample following a firm DRE
• Could function as a first line screen or prognostic indicator

Urinary PCA3: First line screen• Several studies show superior overall specificity to PSA:
80-90%, but include only patients with elevated PSA– In the REDUCE trial the placebo test characteristics for PSA
were: Se = 0.518 Sp = 0.629
• PCA3 in patients with PSA 4-10ng/ml:– Specificity: 71-93% Sensitivity: 53-84%
Is PCA3 Better than PSA for CaP diagnosis?• ERSPC: prostate biopsy trigger:
PSA ≥ 3 or PCA3 ≥ 10• In 721 biopsied, PCA3 performed only marginally better: AUC: PCA3=0.64 PSA=0.58
Roobol et al, Eur Urol, 2010

PCA3 and TMPRSS2-ERG fusion
• Fusion of a strong androgen promoter (transmembrane serine protease) and an oncogene
• Further improved diagnostic accuracy (AUC) – PCA3: 0.65 PCA3 + Fusion: 0.77– PCA3 + gene-fusion + PSA: 0.80
Aubin et al, J Urol, 2008

PCA3: prognostic indicator
• Conflicting studies show a positive relationship1 with cancer aggressiveness or no relationship2
• Reduce Trial- chemoprevention of CaP with Dutasteride3:– Weak association of PCA3 with Gl 7 or higher cancer
– OR: 1.017 (CI95%: 1.01-1.03)
– Though low numbers of high grade prostate cancer weakens the analysis
1. Hessels et al, Prostate, 2010 2. Whitman et al, J Urol, 2008 3. Aubin et al, Urology, 2011

Blood Based biomarkers• Diagnosis
– PSA– PSA velocity– Free PSA– Pro-PSA– BPH-associated PSA
• Prognosis– Human Kallikrein 2– Urokinase plasminogen
activator– Transforming Growth
factor β1– Interleukin-6– Endoglin

Limitations of Total PSA• Neoplastic cells produce varying levels of PSA• Biologic variation:
– Oscillations of PSA up to 30% in range of 0.1-20ng/ml
• Different Assays (WHO standard)• Sensitivity: 52% Specificity: 63%
What Cut-off?
PSA (ng/ml) Percent CaP (%)
<0.6 6.6
0.6-1.0 10.1
1.1-2.0 17.0
2.1-3.0 23.9
3.1-4.0 26.9
PCPT
Thompson et al, NEJM, 2004
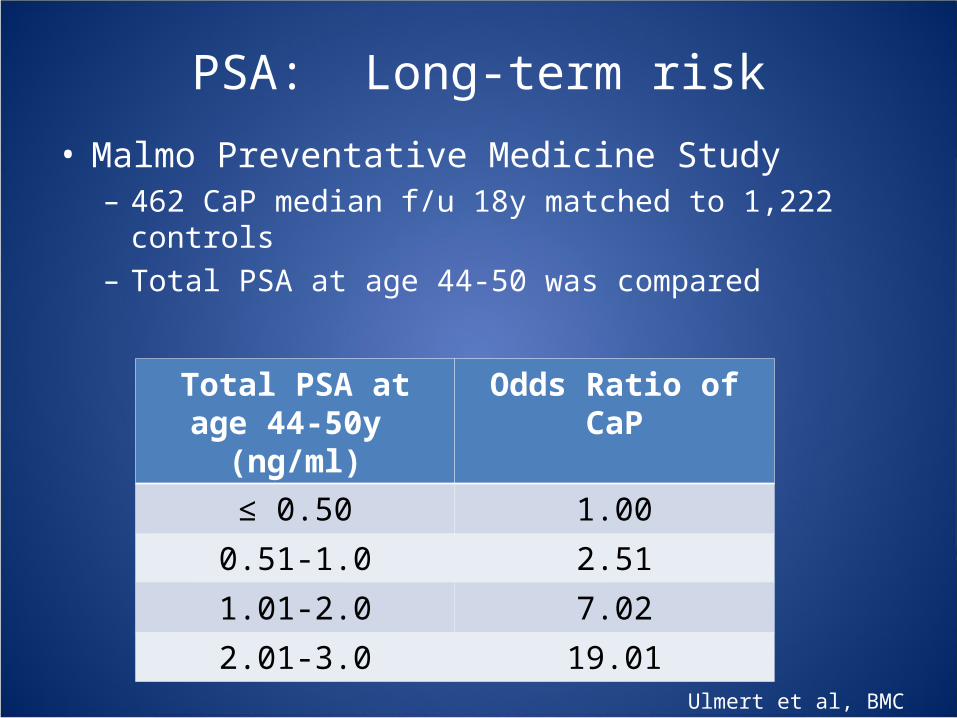
PSA: Long-term risk
• Malmo Preventative Medicine Study– 462 CaP median f/u 18y matched to 1,222 controls– Total PSA at age 44-50 was compared
Total PSA at age 44-50y (ng/ml)
Odds Ratio of CaP
≤ 0.50 1.00
0.51-1.0 2.51
1.01-2.0 7.02
2.01-3.0 19.01
Ulmert et al, BMC Med, 2008

PSA Velocity
• Measurement of change in total PSA over time• Two large prospective trials found no independent
predictive value beyond total PSA and other standard variables (PCPT and ERSPC)
1. Shariat et al, Acta Onc, 2011 2. D’amico et al, NEJM, 2004 3. Carter et al, J NCI, 2006
Diagnosis
• Increase risk of death determined at PSAv levels greater than 0.35 – 2.0 ng/ml per year
• May not predict early progression but an indication of aggressive disease beyond treatment window
Prognosis

Percent Free PSA• Isoform of PSA that remains unbound in plasma• Percent free PSA relative to the total PSA is
FDA approved as an adjunct to total PSA between 4-10ng/ml– fPSA < 25% used as a trigger for biopsy
• Multicenter, prospective trial– Specificity: 95%, Sensitivity: 20% over PSA– AUC: %fPSA = 0.72 PSA: 0.53– When use 10-12 core biopsy: efficiency
decreases
1. Catalona et al, JAMA, 19982. Canto et al, J Urol, 2004

Combined panel of PSA isoforms
• ERSPC: For every 1,000 unscreened men, the model, if used to determine biopsy:– Reduce biopsy rates by 573 – Miss 31/152 low grade CaP 3/40 high grade CaP
Vickers et al, BMC Med, 2008

• Endoglin: CD 105, a cell surface co-receptor for TGFβ1 and 3– Found on immature blood vessels: Angiogenesis– Pre-prostatectomy levels may predict higher gleason score
and PSA recurrence
Svatek et al, CCR 2008
Combining Panel of Markers and Nomogram
• Biomarkers used to supplement not replace clinical data to improve accuracy of prognosis
• Kattan nomogram + biomarker panel:– TGF-β1, IL-6R, IL-6, endoglin, VEGF, VCAM-1
• Predictive accuracy of the Kattan nomogram improved by 15%– 71.6% versus 86.6%
Shariat et al, Acta Onc, 2011
Tissue Based Biomarkers
• Diagnostic– High molecular
weight cytokeratin– p63– AMACR
• Prognostic– Human kallikrein type 2– Prostate specific
membrane antigen– Ki-67– Androgen receptor– Gene fusions– PTEN– P53– SPINK1/TATI– MSMB– EZH2– Heat shock proteins– DNA methylation– HER2

Prostate Specific Membrane Antigen• Transmembrane glycoprotein negatively regulated by
androgens and overexpressed in androgen independent CaP
Increased expression associated with higher grade and biochemical recurrence
Perner S, et al, Human Path, 2007

Translating biomarkers into therapeutic Targets
• PSMA– PSMA- antibody drug conjugate currently in
phase 1 trial– Castration-resistent metastatic CaP
• Endoglin– TRC105 is a human/murine chimeric
monoclonal antibody that binds to endoglin, thus inhibiting angiogenesis
– Phase 1 / phase 2 trial for CRPC
www.nih.gov, 2011
Summary
• Biomarkers serve as a powerful adjunct to the diagnosis and management of prostate cancer
• Biomarkers are testable in the urine, blood, and prostate cancer tissue
• Further validation of these biomarkers and research into potential therapeutic targets is needed