pharmacological approaches to remediate …
TRANSCRIPT


PHARMACOLOGICAL APPROACHES TO REMEDIATE NEUROCOGNITIVE
IMPAIRMENT IN COCAINE-DEPENDENT INDIVIDUALS
A Dissertation Presented to the
Faculty of the College of Education
University of Houston
In Partial Fulfillment
of the Requirements for the Degree
Doctor of Philosophy
by
James J. Mahoney, III
May 2014
PHARMACOLOGICAL APPROACHES TO REMEDIATE NEUROCOGNITIVE
IMPAIRMENT IN COCAINE-DEPENDENT INDIVIDUALS
A Dissertation for the Degree
Doctor of Philosophy
by
James J. Mahoney, III
Approved by Dissertation Committee:
________________________________
Dr. Tam K. Dao, Chairperson
___________________________________________
Dr. Susan X Day, Committee Member
________________________________________
Dr. Norma Olvera, Committee Member
________________________________________
Dr. Richard De La Garza, II, Committee Member
________________________________________
Dr. Robert H. McPherson, Dean
College of Education
May 2014

PHARMACOLOGICAL APPROACHES TO REMEDIATE NEUROCOGNITIVE
IMPAIRMENT IN COCAINE-DEPENDENT INDIVIDUALS
An Abstract
of a Dissertation Presented to the
Faculty of the College of Education
University of Houston
In Partial Fulfillment
of the Requirements for the Degree
Doctor of Philosophy
by
James J. Mahoney, III
May 2014

Mahoney, III, James J. Pharmacological Approaches to Remediate Neurocognitive
Impairment in Cocaine-Dependent Individuals
Abstract
The goal of this study was to determine whether demographic (e.g. ethnicity, gender,
etc.), drug use (e.g. years of cocaine use, days cocaine used in the past 30, comorbid
substance use, etc.), or mood (BDI-II, LSC-R, and ASI-Lite scores) variables affected
neurocognitive functioning in cocaine-dependent participants. In addition, two candidate
medications were evaluated to assess whether they have the potential to improve
neurocognitive functioning in cocaine-dependent individuals. There were two separate
studys as part of this dissertation. Study 1 involved the investigation of demographic and
drug use variables contributing to neurocognitive deficits in 125 cocaine dependent
individuals. Study 2 compared the efficacy of two acetylcholinesterase inhibitors:
rivastigmine and huperzine (as well as a control group randomized to receive placebo) as
potential treatments for cocaine-induced neurocognitive impairment. Twenty-eight
individuals were randomized to receive rivastigmine, 29 were randomized to receive
huperzine, and 15 were randomized to receive placebo. Before study medication
randomization, participants completed a battery of neurocognitive assessments and
completed the same battery of assessments following 8 days of medication/placebo
treatment. One of the factors that detrimentally affects cocaine-dependent individuals as
they seek treatment is the presence of neurocognitive deficits produced or exacerbated by
cocaine use. Since long-term, high-dose cocaine use is a risk factor for the onset of
neurocognitive impairment in humans, it is critical that these deficits be addressed in
order to improve treatment outcomes. Study 1 utilized only baseline data (independent of
any medication treatment) and Study 2 used both pre-treatment (baseline, before
vi
medication administration) and post-treatment (following medication administration)
data. Pearson product moment correlations and analysis of variance (ANOVA) were
used to evaluate the association between demographic and drug use variables and
performance on the neurocognitive measures. ANOVA was used to evaluate medication
versus placebo effects on test performance pre- and post-treatment. Study 1 revealed that
there were no gender or race differences in neurocognition between groups. Further,
comorbid substance use (e.g. nicotine, alcohol, or marijuana) did not affect
neurocognition. Study 2 showed that treatment with rivastigmine significantly improved
episodic memory, though treatment with huperzine did not affect neurocognition. On the
basis of outcomes from Study 1 and Study 2, we contend that cocaine associated
neurocognitive impairment remains an important target of treatment. Given that cocaine
addiction is associated with widespread functional difficulties, such as unemployment
and relapse to dependence, it is plausible that reversing neurocognitive impairments will
ameliorate these functional difficulties.

vii
TABLE OF CONTENTS
Chapter Page
I. INTRODUCTION
A. The Problem and Consequences of Cocaine Use ………...…………………………………………...1
II. REVIEW OF RECENT LITERATURE
A. Neurocognitive Deficits in Cocaine-dependent Individuals…………………………...……………...2
B. Research Questions and Hypotheses…………………………………………………………………..9
C. Implications…………………………………………………………………………………………..10
III. METHODOLOGY
A. Procedure - Assessments……………………………………………………………………………...11
B. Procedures - Neurocognitive Battery…………………………………………………………….......14
C. Study 1 – Demographic/drug use variables which may affect neurocognition…………………...…17
(Gender; Race; Smoking Status; Years, Recent, Daily Cocaine Use, etc.)
D. Study 2 – Rivastigmine or Huperzine as a treatment for neurocognitive impairment……………….18
IV. Results
A. Study 1 – Demographic and drug use variables which may affect neurocognition………………….20
B. Study 2 – Rivastigmine or Huperzine as a treatment for neurocognitive impairment……………….34
V. Conclusion and Summary
A. Study 1 – Demographic and drug use variables which may affect neurocognition…………………..40
B. Study 2 – Rivastigmine or Huperzine as a treatment for neurocognitive impairment……………......50
C. Overall Conclusion and Summary……………………………………………………………............52
VI. References………………………………………………………………………………………………..54

viii
List of Tables
Table Page
1. Demo/Drug Use Statistics and overall Neurocognitive Performance for the entire
sample………………………………………………………………………………..21
2. Neurocognitive Functioning in Males versus Females………………………………23
3. Neurocognitive Functioning in African Americans versus Caucasians……………..25
4. Neurocognitive Functioning in Cigarette Smokers versus Non-Smokers…………...27
5. Neurocognitive Functioning in Alcohol Drinkers versus Non-Drinkers…………….29
6. Neurocognitive Functioning in Marijuana Smokers versus Non-Smokers………….31
7. Correlations between Demographic, Drug Use, and Mood Variables and
Neurocognitive Performance………………………………………………………...33
8. Demo/Drug Use Statistics for Study 2……………………………………………….37
9. Neurocognitive Performance on those Randomized to Rivastigmine versus
Placebo……………………………………………………………………………….38
10. Neurocognitive Performance on those Randomized to Huperzine versus Placebo….39

CHAPTER I
INTRODUCTION
A. THE PROBLEM AND DEFINITION OF COCAINE-DEPENDENCE
Cocaine is one of the most commonly abused psychoactive substances in North
America. Before understanding the consequences and repercussions of cocaine use and
the behavioral manifestations which coincide with cocaine dependence, one must first
understand what cocaine dependence entails. As defined by the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR; American
Psychiatric Association, 2000), cocaine dependence includes a maladaptive pattern of
substance use leading to clinically significant distress, as manifested by three (or more)
of the following, occurring within a 12-month period: 1) tolerance to the cocaine (a need
for more amounts of the cocaine to achieve intoxication or a diminished effect with
continued use of the same amount of the drug); 2) withdrawal from the cocaine
(including taking more cocaine to avoid symptoms of withdrawal); 3) taking more
cocaine in larger amounts or over a longer period than originally intended; 4) a persistent
desire or unsuccessful efforts to cut down on cocaine usage; 5) a great deal of time spent
in activities necessary to obtain the cocaine (contacting and meeting suppliers), using the
cocaine (repeatedly using cocaine) and recovering from the effects produced by cocaine
(during withdrawal); 6) important social, occupational, or recreational activities given up
or reduced because of cocaine use; 7) cocaine use continued despite knowledge of having
a persistent or recurrent physical or psychological problem that is likely to have been
caused or exacerbated by the substance.

CHAPTER II
REVIEW OF RECENT LITERATURE
A. NEUROCOGNITIVE DEFICITS AND COCAINE-DEPENDENCE
One of the factors that impedes on treatment success for cocaine-dependent
individuals is the presence of neurocognitive deficits produced or exacerbated by cocaine
use. Long-term, high-dose cocaine use is a risk factor for the onset of neurocognitive
impairment in humans (e.g. Bolla & Cadet, 2007; Jovanovski, Erb, & Zakzanis, 2005).
Jovanovski (2005) conducted a meta-analytic review (15 studies that included 586
matched controls and 481 abstinent cocaine users), which revealed effect sizes of
moderate or greater magnitude for attention, episodic memory, and working memory,
demonstrating that cocaine-dependent individuals experience dysfunction in these
domains. Specifically, these neurocognitive impairments affect day-to-day functioning;
for example, the presence of cocaine-associated neurocognitive impairment is associated
with poor treatment retention (Aharonovich, Amrhein, Bisaga, Nunes, & Hasin, 2008).
These neurocognitive deficiencies are critical as they affect treatment and cocaine
abstinence. For example, if there are deficits in attention, cocaine-dependent individuals
may be unable to maintain focus, attend, and follow through on treatment plans and goals
provided during the therapy process. In addition, if there are deficits in episodic memory,
these individuals may have a difficult time remembering both the positive and negative
events (including triggers) in their life or specific techniques taught during treatment that
may also impede their progress. Also, if their cocaine use has caused deficits in working
memory, reasoning, and comprehension, then it is possible that information processing
will be affected adversely. Thus, it is important to take all of these factors and
3
neurocognitive deficiencies into consideration when attempting to treat someone with
cocaine-dependence.
It also is important to consider possible drug use and demographic variables that
may play a role in neurocognitive functioning. Previous investigations suggested that, in
nondrug using individuals, gender moderates neurocognition. In one report of healthy
individuals, males performed significantly better than females in spatial and object
versions of the n-back working memory task (Lejbak, Crossley, & Vrbancic, 2011).
Also, males tended to perform slightly better than females on the Iowa Gambling Task, a
measure of decision making and executive functioning (Bechara & Martin, 2004; Bolla,
Eldreth, Matochik, & Cadet, 2004). In addition, males performed significantly better
than females on several visuospatial tests, including mental rotation (Peters, Manning, &
Reimers, 2007), fine motor tasks (Nicholson & Kimura, 1996), and spatial navigation
memory (Rahman, Wilson, & Abrahams, 2003; Voyer, Voyer, & Bryden, 1995).
Conversely, when comparing the performance on tasks focused on verbal memory,
females have performed significantly better than males in verbal recall tasks across
different age groups (Bleecker, Bolla-Wilson, Agnew, & Meyers, 1988). Similarly,
females were significantly better than men on tests of verbal memory, perceptual speed,
and spatial memory for object locations (Herlitz, Nilsson, & Backman, 1997; Rahman et
al., 2003). However, the often cited female advantage in verbal fluency is less clear, with
the advantage apparent on specific semantic items and higher order category fluency (e.g.
Rahman, van Turennout, & Levelt, 2003), but less apparent on letter fluency (Herlitz et
al., 1997).
4
While the literature on gender differences and neurocognitive performance in
stimulant dependent individuals is sparse, the topic is of considerable interest considering
the differential effects stimulant use has on male versus female users, especially
considering that the results from published reports are mixed. For example, long-term
cocaine use is associated with more debilitating effects on women (Anker & Carroll,
2011), and this finding may extend to differences in neurocognition. Conversely,
Rahman and Clarke (2005) found that among recreational cocaine users who had been
abstinent for three days, males exhibited poorer attention and more verbal recognition
errors than female users. In addition, in a meta-analytic review by Scott and colleagues
(2007), the primary conclusion was that methamphetamine may differentially affect
cognitive function in males compared to females. In a separate report, it was found that
there were no overall gender differences with regard to neurocognition, specifically in the
domains of verbal learning and memory (Chang et al., 2005). Conversely, Price and
colleagues found that female cocaine users had fine motor impairment, and this may be
attributed to frequency of use in the months prior to testing (Price et al., 2011).
While the role of race variability on the neurocognitive performance of cocaine-
dependent individuals is not well described in the literature, it has been reported that, in
non-drug using, neurologically normal individuals, African Americans tend to perform
more poorly than Caucasians on tests of cognitive functioning (Ford, Haley, Thrower,
West, & Harrell, 1996; Kuller et al., 1998; Manly et al., 1998). The data suggest that
African Americans may be at greater risk to be misdiagnosed with learning disabilities or
general cognitive impairment. There are several possible reasons for this disparity,
including parental influence and early educational experiences. Specifically, African

5
Americans with lower neurocognitive functioning were more likely than their Caucasian
counterparts to have parents who did not graduate from high school and reported having
non-reading related disabilities (Byrd, Walden Miller, Reilly, Weber, Wall, & Heaton,
2006). While race differences regarding neurocognition have been noted in healthy
controls, there have not yet been any published studies investigating this factor in
cocaine-dependent individuals.
Previous research suggests that the length of abstinence from cocaine affects
neurocognitive functioning in cocaine-dependent participants. For example, on one
particular test of executive function, impairment was noted 2-4 weeks following the last
cocaine use (Ardila, Rosselli, & Strumwasser, 1991) whereas this impairment was not
present during shorter periods of abstinence (within 3 days of last drug use) (Berry et al.,
1993). Another factor that needs to be considered as well is co-morbid substance abuse,
including cigarettes, alcohol, and marijuana. When compared to healthy control subjects,
cocaine-dependent individuals are more likely to smoke cigarettes, and the frequency of
cigarette smoking is positively correlated with their concurrent use of cocaine (Budney,
Higgins, Hughes, & Bickel, 1993; Roll, Higgins, Budney, Bickel, & Badger, 1996).
Neurocognitive deficits, including attention, memory, executive and motor functions,
are commonly impaired in alcohol-dependent individuals (Beatty, Tivis, Stott, Nixon, &
Parsons, 2000; Ikeda et al., 2003; Parsons & Nixon, 1993); however, there has not been
a wealth of literature exploring the neurocognitive effects of concurrent cocaine and
alcohol use. In addition, marijuana use interferes with memory as well as a variety of
cognitive processes, including attention and processing speeding (Pope & Yurgelun-
Todd, 1996). While the impact of other substances, such as nicotine, alcohol, and

6
marijuana, on neurocognition has been reported in the literature, the impact of concurrent
cocaine use and those substances on neurocognition has not yet been discussed.
One critical question is whether stimulant-induced neurocognitive impairment can
be reversed or ameliorated using cognition enhancing interventions. For example,
following administration of 20 mg of oral methylphenidate (a medication used to enhance
cognitive functioning in individuals with attention deficit/hyperactivity disorder),
cocaine-dependent individuals made fewer errors on a computerized cognitive salience
task (in which participants viewed a drug-related or neutral word on a screen written in
blue, green, red, or yellow font, then pressed the matching colored button on a key pad)
(Goldstein et al., 2010). Similarly, in a sample of methamphetamine-dependent
individuals who demonstrated relatively poor neurocognitive performance at baseline,
administration of 400 mg of modafinil for three days significantly improved response
accuracy on measures of working memory in study participants (Kalechstein, De La
Garza, & Newton, 2010). Another study in methamphetamine-dependent volunteers
showed that a single dose of 200 mg modafinil improved performance on a reversal
learning task (Ghahremani, Tabibnia, Monterosso, Hellemann, Poldrack, & London,
2011). Similarly, the results of a recent study indicate that modafinil improved working
memory in cocaine-dependent individuals, measured by the n-back task (Kalechstein,
Yoon, Mahoney, & De La Garza, 2012).
Several reasons support the decision to focus on treating cocaine-induced
neurocognitive impairment not only with medications such as methylphenidate or
modafinil, but also acetylcholinesterase inhibitors such as rivastigmine and huperzine.
For example, rivastigmine is a cognition-enhancing agent used for the treatment of

7
Alzheimer’s disease (Hasselmo & Sarter, 2011) and, in double-blind, placebo-controlled
studies, administration of rivastigmine was associated with improved performance on
tests of attention and memory in individuals diagnosed with Alzheimer’s disease
(Feldman & Lane, 2007; Frankfort et al., 2007) and traumatic brain injury (Silver et al.,
2009; Tenovuo, Alin, & Helenius, 2009). In these studies, the efficacy of rivastigmine
was greatest at higher doses (Silver et al., 2009); however, because the efficacy of
rivastigmine has not been evaluated in cocaine-dependent individuals, we sought to
determine whether relatively low-dose, short-term administration of rivastigmine would
be associated with improved performance on measures of attention, information
processing speed, episodic memory, and working memory in this population.
A separate acetylcholinesterase inhibitor, huperzine, has been evaluated in several
trials involving several hundred human patients (Li, Wu, Zhou, Liu, & Dong, 2008;
Little, Walsh, & Aisen, 2008; Wang, Yan, & Tang, 2006; Zangara, 2003). Of particular
interest, huperzine has been shown to ameliorate deficits in learning and memory. A trial
investigating potential treatments for Alzheimer’s disease revealed that huperzine
significantly improved memory deficits in elderly people with benign senescent
forgetfulness and in patients with Alzheimer’s disease and vascular dementia. These
beneficial effects were observed with minimal peripheral cholinergic side effects and no
unexpected toxicity, demonstrating that it is not only efficacious, but also safe and well-
tolerated.
In conclusion, acetylcholinesterase inhibitors have been shown to improve
cognition, reinforcing that these agents may be similarly useful in treating substance
abuse disorders, specifically cocaine-dependence. Ameliorating these cognitive deficits
8
is of great relevance and importance since exposure to cocaine and other drugs of abuse
is associated with cognitive deficits in humans, and, as mentioned earlier, intact cognitive
functioning has been shown to be positively associated with favorable outcomes in
outpatient clinical trials in cocaine-dependent subjects (Aharonovich, Nunes, & Hasin,
2003).
Research Questions
1. Do gender differences exist with regard to neurocognitive functioning in cocaine-
dependent individuals?
2. Do race differences exist with regard to neurocognitive functioning in cocaine-
dependent individuals?
3. Does comorbid substance use (e.g. nicotine, alcohol, marijuana) exacerbate
neurocognitive deficits in cocaine-dependent individuals?
4. What is the relationship between drug use variables (e.g. years of cocaine use,
days cocaine used in the past 30, etc.) and neurocognitive functioning in cocaine-
dependent individuals?
5. What is the relationship between mood variables (e.g. BDI-II, LSC-R, and ASI-
Lite scores) and neurocognitive functioning in cocaine-dependent individuals?
6. Do two different acetylcholinesterase inhibitors (rivastigmine and huperzine) have
the capability of improving neurocognitive functioning and ameliorating deficits
in cocaine-dependent individuals?
9
Hypotheses
1. It is hypothesized that males and females will differ in neurocognitive tasks, with
females significantly outperforming males on tests of attention and verbal
memory.
2. Based on the literature in non-drug using controls, when matching for education
and IQ, it is hypothesized that Caucasians will perform comparably on various
neurocognitive tests when compared to their African American counterparts.
3. It is hypothesized that comorbid substance use will result in further
neurocognitive deficits then when compared to those whom only use cocaine.
4. It is hypothesized that that there will be a significantly negative correlation
between the drug use variables (e.g. years of cocaine use, amount of cocaine used
per day, etc.) and neurocognitive functioning across a variety of domains.
5. It is hypothesized that that there will be a significantly negative correlation
between mood variables (e.g. BDI-II, LSC-R, and ASI-Lite scores) and
neurocognitive functioning across a variety of domains.
6. It is hypothesized that both rivastigmine and huperzine will significantly improve
various domains of neurocognitive functioning, including attention, verbal
memory, and working memory, when compared to placebo.
C. Implications
A major factor that detrimentally affects progress in treatment for cocaine-
dependent individuals seeking treatment is the presence of neurocognitive deficits
generated or exacerbated by cocaine use. Since long-term, high-dose cocaine use is a risk

10
factor for the onset of neurocognitive impairment in humans, it is critical that these
deficits be addressed in order to improve treatment outcomes. Specifically, deficits in
attention or memory may lead to unfavorable outcomes for several reasons. For example,
deficits in attention may cause the cocaine-dependent individual to be unable to maintain
focus, attend, and follow through on treatment plans and goals provided during the
therapy process. In addition, deficits in memory may cause these individuals to have a
difficult time remembering both the positive and negative times in their life or specific
techniques taught during treatment which would also impede their progress. Also,
deficits in memory may cause their reasoning, comprehension, and information
processing to be adversely affected causing less favorable treatment outcomes. Thus, it is
important to take these factors and neurocognitive deficiencies into consideration when
attempting to treat someone with cocaine-dependence. The implications of this study are
critical as they will not only determine whether the aforementioned candidate
medications are effective for treating neurocognitive impairments, but will also determine
which demographic or drug use variables contribute to these neurocognitive deficits so
that appropriate treatment plans can be initiated.

CHAPTER III
METHODOLOGY
Procedure – Recruitment/Screening
Participants were recruited from the Houston metropolitan area through
newspaper and radio advertisements. The study was approved by the Baylor College of
Medicine and Michael E. DeBakey Veterans Association Medical Center (MEDVAMC)
Internal Review Boards. All participants completed an initial telephone screen in order to
assess basic eligibility. Candidates were then invited to complete an in-person assessment
at the Research Commons of the MEDVAMC. During the in-person interview,
candidates received an explanation of the study purpose and requirements and were
allowed to review, inquire about, and sign the informed consent form. Eligible
individuals were required to be between 18-55 years of age, provide at least one urine
specimen that was positive for cocaine within the two weeks prior to study enrollment,
met DSM-IV criteria for cocaine-dependence, and were experienced with respect to
smoking and/or injecting cocaine. Participants were excluded if they had psychiatric or
medical illness, serious neurological or seizure disorder, use of any psychoactive
medication, and drug or alcohol dependence excluding cocaine, marijuana, and nicotine.
Women were classified as ineligible for the study if they were pregnant, breast feeding,
or not using a reliable form of birth control. In addition, participants completed a
demographic/drug and alcohol use inventory, ASI-Lite, LSC-R, and BDI-II. Participants
were compensated with a $40 gift card for completing the in-person screen. These
recruitment and screening procedures described above were the same used for Study 2.
12
A. Procedure – Assessments
Drug and Alcohol Use Questionnaire
Drug use was assessed with a 14-item, self-report questionnaire with frequency
assessed in terms of date of last use, days used in the past 30, years of use, grams used
per day, and route of administration. In addition to cocaine, substance use frequency was
also assessed for alcohol, methamphetamine, opiates, marijuana, and nicotine. In
addition, recent drug use was assessed and confirmed via qualitative urine toxicology
(testing for cocaine metabolites, amphetamine, methamphetamine, marijuana, and
opiates).
Life Stressor Checklist- Revised (LSC-R)
The LSC-R (Wolfe & Kimerling, 1997) measures life stress in 30 areas that could
elicit PTSD responses (e.g., being mugged, the death of a loved one, a sexual assault).
The LSC-R assesses for whether or not each stressful event occurred, at what ages the
events occurred, how many times each event occurred, how dangerous the event was, and
whether the individual had an intense emotional reaction to the event(s). The total LSC-
R score is obtained by adding up the total number of experiences endorsed (thus the
range is 0 – 30 with 30 indicating endorsement of all experiences). There are 30 events
included on the checklist involving experiences such as natural disasters, assault, death of
family/friends, etc. It should be noted that some of the items are not necessarily
traumatic in nature, but would likely be stress-inducing. Test-retest reliability measures
indicate that kappa values range from 0.52-0.97 across life stress domains on the LSC-R
(McHugo et al., 2005). Additionally, the LSC-R has good concurrent validity with the
Impact of Event Scale – Revised (IES-R) and the Symptom Checklist – 90 – Revised
13
(SCL-90-R), as well as high agreement with clinician ratings (Ungerer et al., 2009). The
LSC-R has demonstrated good criterion validity for PTSD in populations with comorbid
mental health and substance abuse disorders (McHugo et al., 2005).
Addiction Severity Index-Lite (ASI-Lite)
The ASI-Lite (McLellan, Cacciola, Alterman, Rikoon, & Carise, 2006) is a
shortened version of the ASI which is a semi-structured assessment used to evaluate
lifetime and recent (past 30 days) problem behaviors. As mentioned earlier, the ASI-Lite
is divided into 7 separate composite scores: medical, employment, alcohol use, drug use,
family, legal, and psychiatric. The total ASI-Lite score, as well as the composite scores,
are intended to provide the clinician/researcher a more detailed perspective of issues
surrounding ongoing drug use. In general, the ASI-Lite has been found to have good
test-retest reliability with kappa values of approximately 0.60 (Drake & Noordsy, 1995).
Inter-rater reliability measures of the ASI-Lite range from 0.83-1.00 (Stoffelmayr Mavis
&, Kasim, 1994). In cocaine-dependent samples specifically, the ASI-Lite has shown
good test-retest reliability, especially in the domains of lifetime medical, psychiatric, and
substance abuse history (Cacciola, Koppenhaver, McKay, & Alterman 1999).
Beck Depression Inventory – II (BDI-II)
The BDI-II (Beck, 2006) is a 21-question, self-report inventory that evaluates the
presence of depressive symptoms, such as hopelessness and irritability, cognitions such
as guilt or feelings of being punished, as well as physical symptoms such as fatigue,
weight loss, and lack of interest in sex.

14
B. Procedure – Neurocognitive Battery
Participants were provided with standardized instructions, both oral and written,
before the administration of each task. Additionally, participants were reminded to
respond as quickly and as accurately as possible. The tests were selected based on
studies demonstrating that these and or similar measures were shown to be valid and
reliable with respect to differentiating between cocaine-dependent individuals and
matched controls (Gooding, Burroughs, & Boutros, 2008; Verdejo-Garcia, Vilar-Lopez,
Perez-Garcia, Podell, & Goldberg, 2006).
Wechsler Adult Intelligence Scale-III (WAIS-III). The Vocabulary and Matrix
Reasoning subtests of the WAIS-III were administered. The raw scores from these
subtests were included in an algorithm, the Oklahoma Premorbid Intelligence Estimation
algorithm (Schoenberg, Scott, Duff, & Adams, 2002), which estimates level of
intellectual function prior to the onset of drug use (Wechsler, 2007).
Continuous Performance Test-II (CPT- II). The CPT-II measures sustained
attention. Participants were instructed to press the space bar whenever any letter, except
for X, appeared on the computer screen. The letters were presented for 250 milliseconds,
and new letters appeared at intervals of 1, 2, or 4 seconds. The inter-stimuli time intervals
varied pseudo-randomly.
The variables of interest included three measures of inattention: sensitivity – level
of discrimination between signal (X) and non-signal responses; omissions – failure to
press the space bar when letters other than X appear; and hit rate – reaction time in
milliseconds for correct responses. The indices will be transformed into standard scores,
i.e. T-scores, for the data analysis (Conners, 2002).

15
Hopkins Verbal Learning Test-Revised (HVLT-R). The HVLT-R is a measure of
verbal learning and memory that includes six different forms. Participants were initially
read a list of 12 words, approximately one word per second, and asked to repeat back as
many words as possible. This procedure was repeated twice, for a total of three learning
trials. Following a 20 to 25 minute delay period (the Dual N-Back assessment was
administered during the delay period), participants were asked to recall the words without
the aid of reminders. The 2 dependent variables of interest for the HVLT-R were the
standard scores (T-scores) for the total words recalled during all of the three learning
trials and the number of words remembered following the 20 to 25 minute delay period
(Brandt, 2005).
Dual N-back Task. For this computerized working memory task developed by
Susanne Jaeggi, participants were presented with a series of visual stimuli (blue squares)
and auditory stimuli (letters) simultaneously presented across 20 blocks of 21 trials each.
The visual stimulus was presented in one of eight locations on the screen, and the
auditory stimulus was one of eight different letters. For each trial, stimuli were presented
simultaneously for 500 milliseconds, with a 2500 millisecond latency period between the
presentation of stimuli.
Participants started with the 1-back condition, where they were required to
provide a "yes” response (pressing a blue button with the left forefinger) if the location of
the presented visual stimulus matched the location of the stimulus presented immediately
beforehand. Similarly, if the auditory stimulus matched the stimulus presented
immediately beforehand, the participants were required to provide a "yes" response
(pressing a red button with the right forefinger). If both the visual and auditory stimuli

16
matched those presented in the previous trial, then participants were expected to
concurrently press the red and blue buttons, and finally, no response was required if none
of the stimuli matched.
While completing the 20 blocks, the task difficulty varied as a function of
participants’ performance. Specifically, if participants achieved at least 90% accuracy
rate for both visual and auditory modalities in a particular block, the n-back level
increased by one (e.g., from 1-back to 2-back). Conversely, participants regressed to
simpler conditions, e.g., from 2-back to 1-back, if they achieved less than 70% accuracy
for either the visual and auditory modalities in a particular block. Finally, the n-back level
stayed the same if participants performed at an accuracy level between 70 and 90%. For
all levels, a "yes” response was required if the presented visual stimulus or auditory
stimulus matched the stimulus that was presented n trials previously. Dependent
variables were mean n-back level reached in those 20 + n blocks, maximum n-back level
reached, visual accuracy, and auditory accuracy (defined as the ratio of accurate
responses to total responses) (Jaeggi, Buschkuehl, Jonides, & Perrig, 2008).
Order of Test Administration: The battery of neurocognitive tests were administered in
the following order: the HVLT-R learning recall trials, the dual N-back tests, delayed
recall of the HVLT-R, and lastly the CPT-II. The average duration of these
neurocognitive procedures was an hour and a half. The reaction time tests were
programmed on a laptop computer. The WAIS-III was administered on a separate day,
after verifying that the volunteer was not experiencing withdrawal symptoms from
cocaine, and before randomization into the study arms.

17
C. Study 1 - Overview
This study investigated the demographic (e.g. gender, ethnicity, age), drug use
(e.g. years, recent, and daily cocaine use and smoking status) variables that may affect
neurocognition. In addition, we also investigated other variable such as LSC-R, ASI-
Lite, and BDI-II scores and their potential impact on neurocognition.
Study 1 - Participants
The final sample size for Study 1 included 125 cocaine-dependent participants
who were not seeking treatment for their cocaine-dependence at time of the assessment.
Study 1 - Procedures
All eligible participants who completed a baseline neurocognitive battery (before
randomization to one of the many study medication evaluated in the laboratory) were
included in this study.
Study 1 - Statistical Analysis
To alleviate the potential confound of demographic and drug use variability when
assessing gender differences, female cocaine users (n= 21) were matched with male
counterparts (n= 21) on the following variables: age, education, IQ, years of stimulant
use, recent stimulant use, and amount of stimulant used per day. In similar fashion,
Caucasians (n= 16) were matched with their African Americans counterparts to
determine race differences, non-cigarette smokers (n= 17) were matched with cigarette
smokers to determine the impact of cigarette smoking on neurocognitive performance,
alcohol users (n= 15) were matched with non-alcohol users to determine the impact of
alcohol use on neurocognitive performance, and marijuana smokers (n= 20) were
matched with non-marijuana smokers to determine the impact of marijuana smoking on

18
neurocognitive performance. One-way analysis of variance (ANOVA) was utilized to
detect gender, race, or other drug use differences on neurocognition. Since females,
Caucasians, non-smokers, non-dependent alcohol and marijuana users rarely enroll in our
ongoing studies for cocaine-dependent individuals, the distribution was skewed, which
served as the rationale for matching these participants to an equal number of their
counterparts on the aforementioned characteristics. Pearson product moment correlations
were used to evaluate the association between continuous demographic variables (e.g.
age, education, and IQ) and performance on neurocognitive measures. Similarly, Pearson
product moment correlations were used to evaluate the association between continuous
drug use variables (e.g. years of cocaine use, recent cocaine use in the past 30 days, and
daily use of cocaine in grams) and performance on the neurocognitive measures. In
addition, Pearson product moment correlations were used to evaluate the association
between mood symptoms, stress, and addiction severity (e.g. BDI-II, LSC-R, ASI-Lite
scores) and performance on the neurocognitive measures. For demographic, drug use,
and mood comparisons, significance was set at p < 0.05, and when assessing
neurocognitive performance, significance was set at p < 0.006 after incorporating a
Bonferroni correction for multiple comparisons. All analyses were conducted with SPSS
version 17.
Study 2 - Overview
This study investigated the independent efficacy of rivastigmine and huperzine as
potential treatments to ameliorate cocaine-induced neurocognitive impairment.
D. Study 2 - Participants
The sample size for Study 2 included 72 cocaine-dependent participants who were
19
not seeking treatment for their cocaine-dependence at time of the assessment.
Study 2 - Procedures
The study involved a between-subjects, double-blind, placebo-controlled design.
Baseline neurocognitive testing was performed on Day 0 prior to randomization to study
medication. Medication of placebo was administered twice daily beginning on Day 2. 28
participants were randomized to rivastigmine, 29 participants were randomized to
huperzine, and 15 were randomized to placebo. Neurocognitive testing was repeated on
Day 9 following seven days of medication administration which was sufficient for each
drug to reach steady state levels.
Study 2 - Statistical Analysis
Initially, if there were differences between groups at baseline, a within-subjects,
repeated measures ANOVA would have been utilized to evaluate the effects of
rivastigmine, huperzine, and placebo on test performance at baseline (Day 0) and at the
point in time at which sustained rivastigmine or huperzine exposure results in peak blood
levels of the medication (Day 9). However, after preliminary analysis, there were no
differences between any of the groups at baseline (Day 0) so only post-medication (Day
9) groups were compared using one-way ANOVA. For demographic and drug use
comparisons, significance was set at p < 0.05, and when assessing neurocognitive
performance, significance was set at p < 0.006 after incorporating a Bonferroni correction
for multiple comparisons. All analyses were conducted with SPSS version 17.

CHAPTER IV
RESULTS
A. Study 1 – Demographic and drug use variables which may affect neurocognition
Demographic and drug use characteristics for the entire sample (n = 125) can
be found in Table 1. Cocaine-dependent participants were primarily African American
and ~45 years of age. Participants reported using cocaine for ~18 years, 17 days out of
the last 30, and used ~2.0 grams of cocaine/day. A majority of participants also reported
concurrent use of nicotine, alcohol, and/or marijuana.

21
Table 1
Demo/Drug Use Statistics and overall Neurocognitive Performance for the entire sample
Participant Characteristics Cocaine-Dependent Pts
(N = 125)
Demographics
Males
Females
104 (83%)
21 (17%)
Caucasian
African American
29 (23%)
96 (77%)
Age (years) 44.9±0.60
Education (years) 12.4±0.1
IQ (WAIS-III) 97.7±1.1
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
100%
17.5±0.7
16.7±0.8
2.0±0.2
Cigarette
Years of Use
Cigarettes/day
86%
22.6±0.8
13.6±0.8
Alcohol
Years of Use
Days used in past 30
89%
21.3±0.9
10.4±0.9
Marijuana
Years of Use
Days used in past 30
64%
18.8±1.2
5.0±0.9
Neurocognitive Performance
CPT-II Performance
D’ (Sensitivity) 49.74±0.81
Hit Rate – RT^ 49.85±1.27
Omissions^^ 66.58±3.02
HVLT-R Performance
Trials 1-3 36.78±0.96
Delayed Recall 39.14±1.07
N-Back Performance
Auditory Accuracy 0.58±0.02
Visual Accuracy 0.46±0.01
N-value (mean) 1.42±0.03
N-value (max) 2.02±0.06
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance

22
Neurocognitive Functioning in Males versus Females
When investigating neurocognitive differences between genders, cocaine-
dependent males (n=21) and females (n= 21) were statistically similar with regard to all
demographic/drug use variables (Table 2). Cocaine-dependent participants were
primarily African American and ~42 years of age. Participants reported using cocaine for
~15 years, ~15 days out of the last 30, and used ~2.0 grams of cocaine/day.
Males and females did not differ on measures of sustained attention as
measured by the CPT, including sensitivity (F1,40 = 0.368, p = 0.548), hit rate (F1,40 =
1.670, p = 0.204), and omissions (F1,40 = 1.178, p = 0.284). In addition, males and
females scored similarly on measures of immediate episodic memory (F1,40 = 1.858, p =
0.181) nor delayed episodic memory (F1,40 = 4.536, p = 0.039) as measured by the HVLT.
Finally, males and females did not differ on indices of working memory as measured by
the dual n-back, including mean length of the n-back trials for each block working
memory (F1,40 = 0.114, p = 0.738), maximum block length during each assessment (F1,40 =
0.780, p = 0.382), accuracy of responding to auditory stimuli (F1,40 = 0.383, p = 0.540),
and accuracy of responding to visual stimuli (F1,40 = 0.429, p = 0.516).

23
Table 2
Neurocognitive Functioning in Males versus Females
Participant Characteristics
Males
(N = 21)
Females
(N = 21)
p
Demographics
Males
Females
21 (100%)
0
0
21 (100%)
Caucasian
African American
6 (29%)
15 (71%)
6 (29%)
15 (71%)
Age (years) 41.5±1.4 43.9±1.5 .26
Education (years) 11.8±0.3 12.3±0.5 .39
IQ (WAIS-III) 96.3±3.2 93.5±3.4 .56
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
16.3±1.4
16.5±1.9
2.1±0.7
15.0±2.1
15.4±2.1
2.0±0.4
.59
.71
.97
Cigarette
Years of Use
Cigarettes/day
95% 86%
20.7±1.6
13.2±1.9
22.4±2.5
15.7±1.9
.56
.83
Alcohol
Years of Use
Days used in past 30
86% 86%
16.8±1.9
11.6±2.4
18.8±2.5
9.8±2.6
.55
.63
Marijuana
Years of Use
Days used in past 30
62% 52%
20.3±2.4
6.6±2.6
13.7±3.3
6.3±2.9
.11
.93
Neurocognitive Performance
CPT-II Performance
D’ (Sensitivity) 51.85±1.79 49.97±2.53 .55
Hit Rate – RT^ 44.49±3.83 50.47±2.61 .20
Omissions^^ 59.17±5.43 68.03±6.09 .28
HVLT-R Performance
Trials 1-3 35.62±2.11 39.90±2.33 .18
Delayed Recall 35.57±2.59 43.10±2.41 .04
N-Back Performance
Auditory Accuracy 0.61±0.22 0.56±0.24 .54
Visual Accuracy 0.43±0.03 0.46±0.03 .52
N-value (mean) 1.40±0.10 1.36±0.07 .74
N-value (max) 2.05±0.18 1.86±0.13 .38
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.05
**p<0.006

24
Neurocognitive Functioning in African Americans versus Caucasians
When investigating neurocognitive differences between races, cocaine-dependent
African Americans (n = 16) and Caucasians (n = 16) were statistically similar with regard
to all demographic/drug use variables with the exception of years of nicotine use (F1,28 =
5.461, p = 0.027), cigarettes per day (F1,28 = 11.567, p=0.002), and years of marijuana use
(F1,22 = 5.467, p = 0.029) where Caucasians reported using significantly more cigarettes
and marijuana than African Americans (Table 3). Cocaine-dependent participants were
primarily male and ~43 years of age. Participants reported using cocaine for ~16 years,
~17 days out of the last 30, and used ~2.5 grams of cocaine/day.
African Americans and Caucasians did not differ on measures of sustained
attention as measured by the CPT, including sensitivity (F1,30 = 2.884, p = 0.100), hit rate
(F1,30 = 0.151, p = 0.700), omissions (F1,30 = 0.135, p = 0.716). In addition, African
Americans and Caucasians did not differ on measures of immediate or delayed episodic
memory. Specifically, African Americans and Caucasians did not differ with respect to
performance over three learning trials (F1,30 = 0.004, p = 0.951), nor did they differ
following a 15 minute delay period (F1,30 = 0.122, p = 0.730). Finally, African
Americans and Caucasians did not differ on indices of working memory as measured by
the dual n-back, including mean length of the n-back trials for each block working
memory (F1,30 = 2.543, p = 0.0121), maximum block length during each assessment
(F1,30 = 0.429, p = 0.518), accuracy of responding to auditory stimuli (F1,30 = 0.293, p =
0.592), and accuracy of responding to visual stimuli (F1,30 = 0.459, p = 0.503).

25
Table 3
Neurocognitive Functioning in African Americans versus Caucasians
Participant Characteristics
African- American
(N = 16)
Caucasian
(N = 16)
p
Demographics
Males
Females
14 (88%)
2 (12%)
13 (81%)
3 (19%)
Caucasian
African American
0
16 (100%)
16 (100%)
0
Age (years) 43.1±0.50 43.2±1.9 .98
Education (years) 12.6±0.3 12.9±0.5 .50
IQ (WAIS-III) 99.1± 3.15 102.0±2.39 .48
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
16.8±1.2
17.8±2.0
2.5±0.9
15.8±2.5
16.8±2.7
2.5±1.0
.74
.76
.98
Cigarette
Years of Use
Cigarettes/day
100% 88%
19.4±1.8
10.6±1.5
26.1±2.2
18.6±1.9 .03*
.002** Alcohol
Years of Use
Days used in past 30
88% 94%
19.9±2.1
11.6±2.3
25.8±2.2
8.7±2.5
.06
.42
Marijuana
Years of Use
Days used in past 30
81% 69%
14.2±2.7
1.5±0.4
23.3±2.7
6.0±2.7 .03*
.09
Neurocognitive Performance
CPT-II Performance
D’ (Sensitivity) 49.86±1.83 54.51±2.03 .10
Hit Rate – RT^ 47.60±3.36 45.60±3.89 .70
Omissions^^ 58.44±5.04 60.85±4.19 .72
HVLT-R Performance
Trials 1-3 39.25±2.49 39.0±3.19 .95
Delayed Recall 42.60±3.16 41.13±2.82 .73
N-Back Performance
Auditory Accuracy 0.61±0.03 0.63±0.03 .59
Visual Accuracy 0.48±0.04 0.51±0.02 .50
N-value (mean) 1.41±0.07 1.57±0.08 .12
N-value (max) 2.13±0.13 2.25±0.14 .52
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.05
**p<0.006

26
Neurocognitive Functioning in Cigarette Smokers versus Non-Cigarette Smokers
When investigating neurocognitive differences between cigarette smokers and
non-smokers, cocaine-dependent cigarette smokers (n = 17) and non-cigarette smokers (n
= 17) were statistically similar with regard to all demographic/drug use variables with the
exception of years (F1,27 = 6.995, p = 0.013) and recent alcohol use (F1,27 = 4.236, p =
0.049) (Table 4). Cocaine-dependent participants were primarily male, African
American and ~46 years of age. Participants reported using cocaine for ~17 years, ~16
days out of the last 30, and used ~2.0 grams of cocaine/day. Those cigarette smokers
included in the analyses reporting using cigarettes for ~27 years and smoked ~23
cigarettes per day.
Cigarette smokers and non-cigarette smokers did not differ on measures of
sustained attention as measured by the CPT, including sensitivity (F1,32 = 0.609, p =
0.441), hit rate (F1,32 = 0.305, p = 0.584), and omissions (F1,32 = 0.040, p = 0.844). In
addition, cigarette smokers and non-cigarette smokers did not differ on measures of
immediate or delayed episodic memory. Specifically, cigarette smokers and non-
cigarette smokers did not differ with respect to performance over three learning trials
(F1,32 = 0.178, p = 0.676), nor did they differ following a 15 minute delay period (F1,32 =
0.034, p = 0.855). Finally, cigarette smokers and non-cigarette smokers did not differ on
indices of working memory as measured by the dual n-back, including mean length of the
n-back trials for each block working memory (F1,32 = 0.373, p = 0.545), maximum block
length during each assessment (F1,32 = 2.299, p = 0.139), accuracy of responding to
auditory stimuli (F1,32 = 1.381, p = 0.249), and accuracy of responding to visual stimuli
(F1,32 = 0.809, p = 0.375).

27
Table 4
Neurocognitive Functioning in Cigarette Smokers versus Non-Smokers
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.05
**p<0.006
Participant Characteristics Smoker
(N = 17)
Non-Smoker
(N = 17)
p
Demographics
Males
Females
14 (82%)
3 (18%)
14 (82%)
3 (18%)
Caucasian
African American
4 (12%)
13 (76%)
6 (35%)
11 (65%)
Age (years) 46.7±1.1 46.6±1.2 .94
Education (years) 12.5±0.3 12.5±0.3 .90
IQ (WAIS-III) 98.3±3.0 99.3±3.4 .84
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
17.6±2.1
18.8±2.4
1.8±0.3
17.8±1.8
14.0±2.0
1.8±0.3
.97
.13
.97
Cigarette
Years of Use
Cigarettes/day
27.0±7.9
22.8±5.6
-
- <.001**
<.001** Alcohol
Years of Use
Days used in past 30
76% 94%
24.9±2.9
14.2±3.5
16.2±1.8
6.6±1.8 .01*
.05* Marijuana
Years of Use
Days used in past 30
47% 41%
20.9±4.3
2.4±1.0
19.0±2.2
5.1±4.2
.70
.52
Neurocognitive Performance
CPT-II Performance
D’ (Sensitivity) 50.91±1.98 53.23±2.22 .44
Hit Rate – RT^ 49.60±3.98 46.70±3.42 .58
Omissions^^ 68.38±6.89 71.11±11.88 .84
HVLT-R Performance
Trials 1-3 37.88±3.07 36.24±2.42 .68
Delayed Recall 39.35±2.49 38.63±3.09 .86
N-Back Performance
Auditory Accuracy 0.62±0.05 0.51±0.07 .25
Visual Accuracy 0.44±0.03 0.47±0.03 .38
N-value (mean) 1.37±0.07 1.43±0.09 .55
N-value (max) 1.82±.0.13 2.12±0.15 .14

28
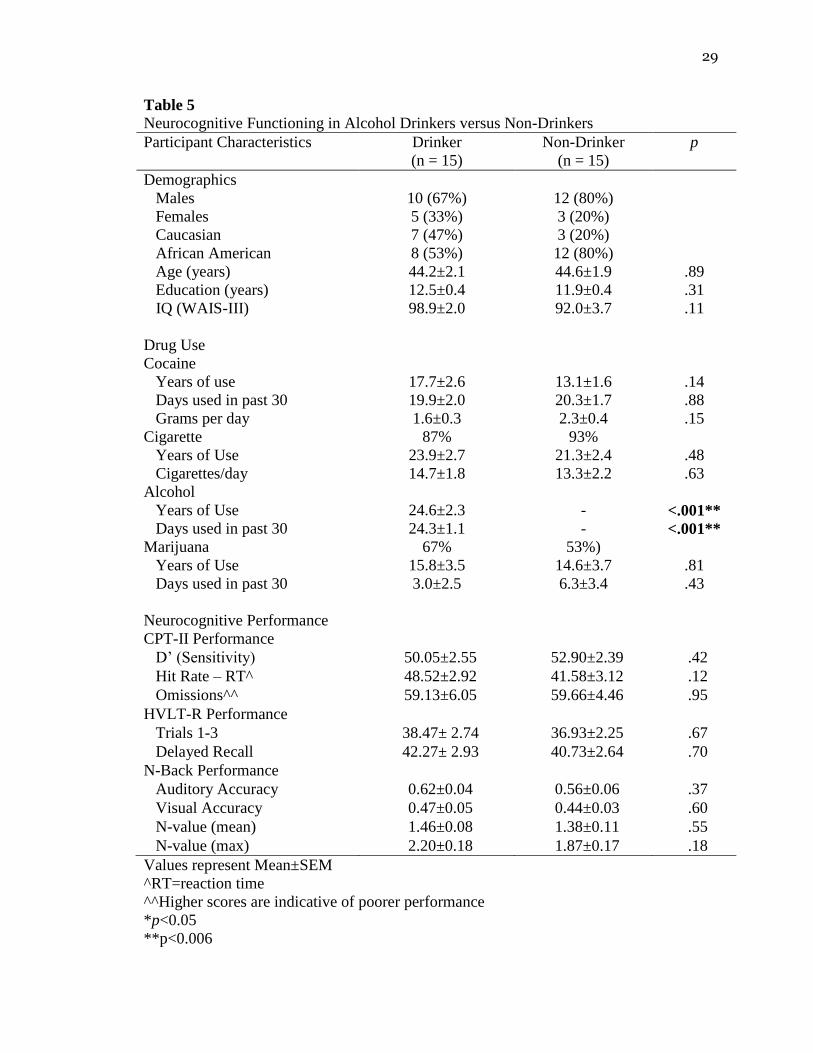
Neurocognitive Functioning in Alcohol Drinkers versus Non-Drinkers
When investigating neurocognitive differences between alcohol users and non-
users, cocaine-dependent alcohol users (n = 15) and non-alcohol users (n = 15) were
statistically similar with regard to all demographic/drug use variables (Table 5).
Cocaine-dependent participants were primarily male, African American and ~44 years of
age. Participants reported using cocaine for ~15 years, ~20 days out of the last 30, and
used ~2.0 grams of cocaine/day. Those alcohol users included in the analyses reporting
using alcohol for ~25 years and ~25 days out of the past 30.
Alcohol users and non-alcohol users did not differ on measures of sustained
attention as measured by the CPT, including sensitivity (F1,28 = 0.668, p = 0.421), hit rate
(F1,28 = 2.630, p = 0.116), and omissions (F1,28 = 0.005, p = 0.945). In addition, alcohol
users and non-alcohol users did not differ on measures of immediate or delayed episodic
memory. Specifically, alcohol users and non-alcohol users did not differ with respect to
performance over three learning trials (F1,28 = 0.187, p = 0.669); nor did they differ
following a 15 minute delay period (F1,28 = 0.151, p = 0.700). Finally, alcohol users and
non-alcohol users did not differ on indices of working memory as measured by the dual
n-back, including mean length of the n-back trials for each block working memory (F1,28
= 0.360, p = 0.554), maximum block length during each assessment (F1,28 = 1.923, p =
0.176), accuracy of responding to auditory stimuli (F1,28 = 0.819, p = 0.373), and accuracy
of responding to visual stimuli (F1,28 = 0.275, p = 0.604).
29
Table 5
Neurocognitive Functioning in Alcohol Drinkers versus Non-Drinkers
Participant Characteristics
Drinker
(n = 15)
Non-Drinker
(n = 15)
p
Demographics
Males
Females
10 (67%)
5 (33%)
12 (80%)
3 (20%)
Caucasian
African American
7 (47%)
8 (53%)
3 (20%)
12 (80%)
Age (years) 44.2±2.1 44.6±1.9 .89
Education (years) 12.5±0.4 11.9±0.4 .31
IQ (WAIS-III) 98.9±2.0 92.0±3.7 .11
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
17.7±2.6
19.9±2.0
1.6±0.3
13.1±1.6
20.3±1.7
2.3±0.4
.14
.88
.15
Cigarette
Years of Use
Cigarettes/day
87% 93%
23.9±2.7
14.7±1.8
21.3±2.4
13.3±2.2
.48
.63
Alcohol
Years of Use
Days used in past 30
24.6±2.3
24.3±1.1
-
- <.001**
<.001** Marijuana
Years of Use
Days used in past 30
67% 53%)
15.8±3.5
3.0±2.5
14.6±3.7
6.3±3.4
.81
.43
Neurocognitive Performance
CPT-II Performance
D’ (Sensitivity) 50.05±2.55 52.90±2.39 .42
Hit Rate – RT^ 48.52±2.92 41.58±3.12 .12
Omissions^^ 59.13±6.05 59.66±4.46 .95
HVLT-R Performance
Trials 1-3 38.47± 2.74 36.93±2.25 .67
Delayed Recall 42.27± 2.93 40.73±2.64 .70
N-Back Performance
Auditory Accuracy 0.62±0.04 0.56±0.06 .37
Visual Accuracy 0.47±0.05 0.44±0.03 .60
N-value (mean) 1.46±0.08 1.38±0.11 .55
N-value (max) 2.20±0.18 1.87±0.17 .18
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.05
**p<0.006
30
Neurocognitive Functioning in Marijuana Smokers versus Non-Smokers
When investigating neurocognitive differences between marijuana smokers and
non-smokers, cocaine-dependent marijuana smokers (n = 20) and non-marijuana smokers
(n= 20) were statistically similar with regard to all demographic/drug use variables
(Table 6). Cocaine-dependent participants were primarily male, African American and
~43 years of age. Participants reported using cocaine for ~14 years, ~18 days out of the
last 30, and used ~2.0 grams of cocaine/day. Those marijuana users included in the
analyses reporting using marijuana for ~24 years and ~16 days out of the past 30.
Marijuana smokers and non-marijuana smokers did not differ on measures of
sustained attention as measured by the CPT, including sensitivity (F1,38 = 0.199, p =
0.658), hit rate (F1,38 = 0.070, p = 0.792), and omissions (F1,38 = 0.529, p = 0.471). In
addition, marijuana smokers and non-marijuana smokers did not differ on measures of
immediate or delayed episodic memory. Specifically, marijuana smokers and non-
marijuana smokers did not differ with respect to performance over three learning trials
(F1,38 = 1.157, p = 0.289), nor did they differ following a 15 minute delay period (F1,38 =
1.964, p = 0.169). Finally, marijuana smokers and non-marijuana smokers did not differ
on indices of working memory as measured by the dual n-back, including mean length of
the n-back trials for each block working memory (F1,38 = 0.063, p = 0.804), maximum
block length during each assessment (F1,38 = 0.239, p = 0.628), accuracy of responding to
auditory stimuli (F1,38 = 0.976, p = 0.329), and accuracy of responding to visual stimuli
(F1,38 = 0.086, p = 0.771).

31
Table 6
Neurocognitive Functioning in Marijuana Smokers versus Non-Smokers
Participant Characteristics
Marijuana
(n = 20)
Non-Marijuana
(n = 20)
p
Demographics
Males
Females
17 (85%)
3 (15%)
16 (80%)
4 (20%)
Caucasian
African American
6 (30%)
14 (70%)
5 (20%)
15 (75%)
Age (years) 43.3±2.0 42.1±1.5 .65
Education (years) 12.2±0.3 12.2±0.2 1.00
IQ (WAIS-III) 95.8±11.6 97.5±12.3 .68
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
15.8±1.8
20.4±1.8
1.5±0.2
13.7±1.1
16.3±1.5
1.6±0.2
.33
.09
.72
Cigarette
Years of Use
Cigarettes/day
85% 85%
23.5±2.3
13.5±1.6
20.1±1.9
11.7±1.7
.27
.45
Alcohol
Years of Use
Days used in past 30
90% 80%
21.1±1.9
9.2±2.0
16.6±2.5
7.6±1.6
.15
.54
Marijuana
Years of Use
Days used in past 30
24.2±7.52
16.2±8.58
-
- <.001**
<.001**
Neurocognitive Performance
CPT-II Performance
D’ (Sensitivity) 49.58±2.20 48.08± 2.51 .66
Hit Rate – RT^ 50.29±3.34 48.90± 4.01 .79
Omissions^^ 71.00±9.47 62.59± 6.63 .47
HVLT-R Performance
Trials 1-3 33.25±2.0 36.0± 1.59 .29
Delayed Recall 34.65±2.40 39.42± 2.41 .17
N-Back Performance
Auditory Accuracy 0.63±0.05 0.57±0.04 .33
Visual Accuracy 0.44±0.03 0.45±0.04 .77
N-value (mean) 1.44±0.09 1.41±0.08 .80
N-value (max) 1.95±0.15 2.05±0.14 .63
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.05
**p<0.006
32
Correlations between Demographic, Drug Use, and Mood Variables and Neurocognitive
Performance
Despite considerable heterogeneity in responses among participants, Pearson
product-moment correlation revealed that age was negatively and significantly correlated
with mean length of the n-back trials for each block working memory (p < 0.001) and
maximum length of the n-back trials for each block of working memory; however, the r
values were very low (r < 0.400 for all measures) indicating that these relationships were
more likely explained by other factors. Pearson product-moment correlation revealed
that IQ was positively and significantly correlated with respect to episodic memory
performance over three learning trials (p < 0.001), delayed performance over three
learning trials (p < 0.001), accuracy of responding to auditory stimuli (p < 0.001), mean
length of the n-back trials for each block working memory (p < 0.001), maximum block
length during each assessment (p < 0.001); however, the r values were all quite low (r <
0.460 for all measures) indicating that these relationships were more likely explained by
other factors. All other demographic, drug use, and mood variables were not
significantly correlated with neurocognitive performance (p>0.006).

33
Table 7
Correlations between Demographic, Drug Use, and Mood Variables and Neurocognitive Performance
Demographic Cocaine Use Mood
Age Education IQ Years Recent Daily BDI LSC-R ASI
CPT-II
D’ (Sensitivity) -.135 .058 .036 -.044 -.114 .022 -.010 .148 .108
Hit Rate – RT^ .190 -.082 -.040 .127 .026 -.172 .024 -.010 .029
Omissions^^ .056 .023 .083 .052 -.066 .076 -.017 .013 .043
HVLT-R
Trials 1-3 .004 .077 .437* .089 -.013 .163 -.062 -.067 .015
Delayed Recall -.041 .056 .348* -.047 -.102 .122 -.125 -.071 .009
N-Back
Auditory Accuracy -.099 .021 .176 -.157 -.039 .120 -.096 .029 -.056
Visual Accuracy -.152 -.005 .418* .135 .172 -.007 .018 .093 .161
N-value (mean) -.379* .178 .455* -.065 .147 -.091 -.025 .153 .172
N-value (max) -.335* .115 .422* -.081 .065 -.108 -.041 .132 .180
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.006

34
B. Study 2 – Rivastigmine and Huperzine as treatments for neurocognitive
impairment
Demographic and drug use characteristics of the 72 completers in the treatment
groups are presented in Table 8. A total of 75 participants were enrolled in the study (3
participants withdrew for personal reasons). Cocaine-dependent participants were
primarily African American and ~43 years of age. Participants reported using cocaine for
~16 years, 18 days out of the last 30, and used ~2 grams of cocaine/day. The treatment
groups did not differ for any basic demographic or drug use variables (all p-values >
0.05).
Preliminary analyses revealed that demographic indices, including age, years of
education, estimated level of premorbid IQ, and substance use indices, including lifetime
and recent use of alcohol, cocaine, and nicotine, did not correlate with performance on
indices of sustained attention, learning and memory, or working memory performance
(all p’s > 0.05). Thus, no covariates were included in the primary analyses.
The effects of rivastigmine on neurocognitive functioning
Table 9 includes the results of performance on measures of sustained attention,
episodic memory, and working memory when comparing those participants receiving 3
or 6 mg rivastigmine and placebo.
Participants randomized to rivastigmine versus placebo did not differ on measures
of sustained attention as measured by the CPT, including sensitivity (F1,41 = 0.014, p =
0.908), hit rate (F1,41 = 0.280, p = 0.600), omissions (F1,41 = 0.016, p = 0.899). However,
rivastigmine administration was associated with significantly improved performance on
measures of immediate memory. Specifically, participants randomized to rivastigmine

35
had significantly elevated performance over three learning trials (F1,41 = 11.856, p <
0.001). However, there were no differences between groups on performance following a
15 minute delay period (F1,41 = 1.947, p = 0.170). Rivastigmine administration was not
associated with significantly improved performance on two indices of working memory,
including mean length of the n-back trials for each block working memory (F1,41 = 5.010,
p = 0.031) and maximum block length during each assessment (F1,41 = 7.493, p = 0.009).
Rivastigmine and placebo groups did not differ on accuracy of responding to auditory
stimuli (F1,41 = 3.884, p = 0.056) nor accuracy of responding to visual stimuli (F1,41 =
0.911, p = 0.345).
The effects of huperzine on neurocognitive functioning
Table 10 includes the results of performance on measures of sustained attention,
episodic memory, and working memory when comparing those participants receiving 0.4
or 0.8 mg huperzine and placebo.
Participants randomized to 0.4 or 0.8 mg huperzine and placebo did not differ on
measures of sustained attention as measured by the CPT, including sensitivity (F1,42 =
0.226, p = 0.637), hit rate (F1,42 = 0.046, p = 0.831), and omissions (F1,42 = 0.077, p =
0.783). Participants randomized to huperzine or placebo did not differ on measures of
immediate or delayed episodic memory. Specifically, groups did not differ with regard to
performance over three learning trials (F1,42 = 1.262, p = 0.268), nor did they differ on
performance following a 15 minute delay period (F1,42 = 0.449, p = 0.506). Participants
randomized to huperzine or placebo did not differ on measures of working memory as
assessed by the n-back, including mean length of the n-back trials for each block working
memory (F1,42 = 0.005, p = 0.945), maximum block length during each assessment (F1,42 =

36
0.345, p = 0.560), accuracy of responding to auditory stimuli (F1,42 = 2.442, p = 0.126),
and accuracy of responding to visual stimuli (F1,42 = 0.159, p = 0.692).

37
Table 8
Demo/Drug Use Statistics for Study 2
Placebo
(N = 15)
Rivastigmine
(N = 28)
Huperzine
(N = 29)
p
Demographics
Males
Females
13 (87%)
2 (13%)
22 (79%)
6 (21%)
22 (76%)
6 (24%)
Caucasian
African American
4 (27%)
11 (73%)
8 (29%)
20 (71%)
8 (28%)
21 (72%)
Age (years) 39.7±2.0 43.9±1.0 43.2±7.6 .16
Education (years) 12.1±0.3 12.9±0.3 12.7±0.4 .36
IQ (WAIS-III) 96.5±3.8 101.1±1.1 97.0±2.4 .39
Drug Use
Cocaine
Years of use
Days used in past 30
Grams per day
15.7±1.9
15.8±1.8
1.8±0.3
16.1±1.5
18.6±1.5
2.3±0.5
16.0±1.5
17.6±1.8
2.1±0.3
.98
.72
.60
Cigarette
Years of Use
Cigarettes/day
87% 89% 93%
17.4±2.3
20.2±2.8
21.3±1.7
26.5±1.7
20.66±1.6
26.37±1.5
.37
.07
Alcohol
Years of Use
Days used in past 30
93% 82% 79%
18.7±2.4
9.9±8.2
20.8±1.5
10.3±1.7
22.3±1.8
10.2±1.9
.42
.99
Values represent Mean±SEM
*p<0.05

38
Table 9
Neurocognitive Performance on those Randomized to Rivastigmine versus Placebo
Placebo
(N = 15)
Rivastigmine
(N = 28)
p
Neurocognitive Performance Post-tx Post-tx
CPT-II Performance
D’ (Sensitivity) 50.23±2.99 49.87±1.58 .91
Hit Rate – RT^ 46.93±3.86 49.26±2.48 .60
Omissions^^ 60.61±5.06 61.61±5.05 .90
HVLT-R Performance
Trials 1-3 31.73±2.13 40.43±1.46 <.001*
Delayed Recall 32.13±2.78 37.29±2.25 .17
N-Back Performance
Auditory Accuracy 0.52±.05 0.62±0.02 .06
Visual Accuracy 0.50±0.05 0.55±0.03 .35
N-value (mean) 1.55±0.11 1.84±0.08 .03
N-value (max) 2.07±0.18 2.61±0.11 .01
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
*p<0.006

39
Table 10
Neurocognitive Performance on those Randomized to Huperzine versus Placebo
Placebo
(N = 15)
Huperzine
(N = 29)
p
Neurocognitive Performance Post-tx Post-tx
CPT-II Performance
D’ (Sensitivity) 50.23±2.99 51.70±1.61 .64
Hit Rate – RT^ 46.93±3.86 47.90±2.57 .83
Omissions^^ 60.61±5.06 63.95±8.22 .78
HVLT-R Performance
Trials 1-3 31.73±2.13 35.28±1.98 .27
Delayed Recall 32.13±2.78 34.55±2.16 .51
N-Back Performance
Auditory Accuracy 0.52±0.05 0.61±0.03 .13
Visual Accuracy 0.50±0.05 0.48±0.03 .69
N-value (mean) 1.55±0.11 1.56±0.09 .95
N-value (max) 2.07±0.18 2.21±0.14 .56
Values represent Mean±SEM
^RT=reaction time
^^Higher scores are indicative of poorer performance
**p<0.006

CHAPTER V
CONCLUSION AND SUMMARY
A. Study 1 – Demographic and drug use variables which may affect neurocognition
Overall, as compared to age-matched normative data, the current results indicate
that cocaine users perform at a lower level on neurocognitive assessments. Specifically,
cocaine-dependent participants tended to perform more poorly in the domains of working
memory (since scores on the n-back fell well below the scores of healthy controls
reported by Jaeggi, 2008) and episodic memory (since the t-scores on the HVLT were
well below the normed 43-55 average range). These data demonstrate that
neurocognitive deficits exist in cocaine-dependent individuals irrespective of
demographic, drug use, and behavioral characteristics. Importantly, the current results
coincide with the meta-analysis performed by Jovanovski (2005) which revealed that
cocaine-dependent individuals experienced dysfunction in episodic memory and working
memory.
The data did not reveal gender differences in the domains of attention, working
memory, verbal memory. This finding is of considerable interest since there have been
notable gender differences reported for several neurocognitive domains in the literature in
both healthy controls and cocaine users. Some explanations as to why males and females
performed similarly on neurocognitive tasks warrants discussion. When investigating the
subjective effects of cocaine, males, when compared to females, detected cocaine’s
effects faster and reported more intense positive (e.g. euphoria) and negative (e.g.
dysphoria) subjective responses (Lukas, 1996). In addition, after receiving cocaine in the
laboratory, males who received the same mg/kg dose of cocaine as females, achieved

41
significantly higher plasma cocaine levels when compared to women (Lukas, 1996).
Moreover, females achieve similar cardiovascular increases in heart rate when compared
to males suggesting that females may be more sensitive to the cardiovascular effects of
cocaine when taking into consideration these differences in plasma cocaine levels. It has
previously been reported that elevated levels of progesterone markedly increased the
cardiotoxic effects produced by cocaine (Woods & Plessinger, 1990; Sharma, Plessinger,
Sherer, Liang, Miller, & Woods 1992; Plessinger & Woods, 1990). This may further
explain the impact of hormones on gender differences and stimulant use. While not
directly correlated with neurocognition, gender differences in the behavioral and
cardiovascular responses to cocaine may provide insight into potential mediators into
cocaine’s effect on brain function and neurocognitive performance. However, it must be
noted that the gender differences mentioned above were reported following acute cocaine
administration, which may explain the inconsistency between the findings mentioned in
the literature and our current findings. In our studies, the participants had been abstinent
from cocaine for >3 days, the acute effects of the drug were not present (i.e. the intention
was to determine the effects of long-term, chronic cocaine use rather than evaluating
performance in an intoxicated state). The finding that males and females performed
statistically similar in the cocaine-abstinent condition provides the first evidence that
gender differences do not exist with respect to the long lasting effects of cocaine on
neurocognition. Future studies could assess neurocognition immediately following acute
cocaine administration to determine whether gender differences emerge in that situation.
For example, a recent study by our group demonstrated that acute methamphetamine
exposure improved neurocognition (specifically attention and working memory);

42
however, the sample had an insufficient number of females to conduct a gender analysis
(Mahoney, 2012).
The finding that there were no neurocognitive deficits in cocaine-dependent
individuals who were concurrent cigarette smokers as compared cocaine users alone is
interesting due to the neurocognitive stimulating effects (e.g. improved attention) as well
as deficits produced by nicotine (Mancuso, Lejeune, & Ansseau, 2001). In a recent
review of the literature, cigarette smoking was associated with deficiencies in executive
functioning, cognitive flexibility, general intellectual abilities, learning, episodic
memory, processing speed, and working memory (Durazzo, Meyerhoff, & Nixon, 2010).
Specifically, cigarette smokers exhibit poorer working memory as measured by the n-
back task (similar to the task used in the current study) when compared to non-smokers
(Ernst, Heishman, Spurgeon, & London, 2001, Jacobsen, Krystal, Mend, Westerveld,
Frost, & Pugh, 2005), and perform poorly on tasks focusing on visuospatial working
memory (George et al., 2002). In addition, smokers performed worse than non-smokers
on measure of auditory-verbal memory as measured by assessment such as the Wechsler
Memory Scale (Fried, Watkinson, & Gray, 2006; Cerhan et al., 1998). Conversely, other
studies noted no differences on measures of auditory-verbal learning and memory and
verbal fluency (Kalmijn, van Boxtel, Verschuren, Jolles, & Launer, 2002; Sakurai &
Kanazawa, 2002). Heavy smokers (defined as those who smoked ~40 cigarettes a day)
performed worse than light smokers (defined as those who smoked ~5 cigarettes a day)
on the Wisconsin Card Sorting Task (an assessment of executive functioning (Razani,
Boone, Lesser, & Weiss, 2004). In addition, other reports found that smokers and non-
smokers did not differ on some tasks of executive functioning such as the Trail Making

43
Test B and the Paced Auditory Serial Attention Task (Elwan et al., 1997). Due to the
cognitive deficits produced by cigarette smoking alone (with the exception of the few
studies mentioned), one may assume that comorbid cigarette smoking and cocaine use
may exacerbate cognitive deficiencies; however, the results of this study do not support
this assumption. One potential explanation for this is perhaps that the cocaine use had
caused deficits severe enough that concurrent cigarette smoking caused minimal
additional impairment (the concept of “floor” effects will be discussed later).
The finding that there were no neurocognitive deficits in cocaine-dependent
individuals who were concurrent alcohol users when compared to those whom were
cocaine-dependent alone is interesting due to the neurocognitive deficits produced by
alcohol. Evidence indicated that chronic (long-term, consistent) alcohol exposure may
result in brain shrinkage which can affect numerous cognitive abilities. For example,
psychomotor speed (the speed at which you are able to physically perform tasks) and
visuospatial abilities (those involving conceptualizing and understanding physical
properties of objects) are both affected by chronic alcohol abuse (Lezak, Howieson, &
Loring, 2004; Parsons & Farr, 1981; Ryan & Butters, 1986). However, other skills, such
as language and arithmetic abilities, are less affected which may lead one to believe that
the chronic alcohol use is not affecting them. In addition, the onset age of alcohol
drinking may account for positive relationships between age/duration and level of
cognitive dysfunction (Pishkin, Lovallo, & Bourne, 1985). Also, it has been reported that
alcohol abuse causes accelerated aging in the brain (Blusewicz, Dustman, Schenkenberg,
& Beck 1977; Graff-Radford, Heaton, Earnest, & Rudikoff, 1982) which in turn causes
impairments of problem-solving skills, memory, and learning (Craik, 1977). While
44
memory may remain intact initially, as the difficulty of tasks increase, performance of
memory functioning gradually declines. It has also been reported that alcohol abuse
leads to deficits in executive functioning. Executive functioning involves several
different aspects of day- to-day life including inhibitory control (being able to stop doing
something inappropriate), initiation (starting a process rather than waiting for someone
else to start it for you), and working memory (holding information in your short-term
memory). In addition, those whom abuse alcohol have problem-solving issues, decreased
flexibility in thinking, as well as problems remembering, which are all related to
executive functioning.
During the detoxification period (which occurs over the 2 weeks following the
stoppage of alcohol use), there are neurocognitive deficits across several cognitive
domains, even those that remain unaffected during active alcohol usage (Ryan,
1986). However, the brain is resilient and has the ability to “bounce back.” So many
cognitive deficits, such as memory and learning abilities, are restored following
abstinence. Memory deficits include problems with declarative memory (long-term
memory where facts and knowledge are stored) and includes anterograde (creating new
memories) and retrograde (remembering old memories) deficits (Butters & Stuss, 1989;
O’Connor & Verfaillie, 2002).
Due to the numerous cognitive deficits produced by alcohol alone, one may
assume that comorbid alcohol and cocaine use may exacerbate or have more of an
additive effect to these cognitive deficiencies; however, the results of this study indicate
that cocaine users alone when compared to concurrent cocaine and alcohol users, do not
differ with respect to neurocognitive functioning. One potential explanation for the

45
groups being statistically similar in the current study is because none of the individuals
included in this study met criteria for alcohol-dependence (the dependence criteria for
alcohol is identical to the criteria for dependence criteria for cocaine mentioned on page
7). Thus, since these individuals were not alcohol-dependent, their regular patterns of
daily alcohol use may not have affected nor caused further decrements in neurocognitive
capabilities. Future studies should investigate the differences between cocaine-
dependent and comorbid cocaine- and alcohol-dependent individuals to further explore
the deficits caused by this comorbidity.
The finding that there were no neurocognitive deficits in cocaine-dependent
individuals who were concurrent marijuana users when compared to those whom were
cocaine-dependent alone is interesting due to the neurocognitive deficits produced by
marijuana. Marijuana interferes with memory as well as a variety of cognitive processes,
leaving the chronic user less able to adapt, excel, and respond to typical life challenges
(Pope, Gruber, & Yurgelun-Todd, 1996). The cognitive effects produced by marijuana
should be divided into 3 different categories: acute (during marijuana intoxication),
residual (when intoxication wears off, but marijuana is still present in the system), and
chronic (long after marijuana is out of the system) (Solowij, 1999). During the acute
phase, very high doses of marijuana may result in psychotic-like states (Brust, 1993;
Colback & Crowe, 1970). The acute effects of marijuana are noticed in reactive
emotional states including perceptual changes and psychomotor slowing. While several
studies have also reported equivocal results for behavior and cognitive changes following
acute marijuana exposure, there have been reports demonstrating reduced memory
capabilities while under the influence of marijuana (Brust, 2000). However, it has also
46
been reported that, despite subjective report of intoxication, these individuals perform
fairly well on tests of attention while deficits are noted on factual memory and short-term
recall (Iverson, 2000). With regard to the subacute consequences of marijuana use, there
have been reports of decreased performance on tests of attention, memory, and motor
abilities (for review see Pope, Gruber, & Yurgelun-Todd, 1996; Sofuoglu, Sugarman, &
Carroll, 2010). However, in a separate review, when setting stringent criteria including
the inclusion of studies where there was a subacute presence of marijuana and not
intoxication, it was reported that only 55% of individuals demonstrated a level of
cognitive impairment (Gonzalez, Carey, & Grant, 2002). As a result, the long-term
consequences (residual effects) of marijuana usage is not quite clear. The literature has
demonstrated that learning and reaction time tests in marijuana users and controls
demonstrated no differences (Lezak et al., 2004). While there appear to be no significant
long-term cognitive deficits in marijuana users, there are noted personality changes. For
example, it has been reported that marijuana users express apathy (a general “not
caring”), restlessness, and sluggishness (Brust, 1993; Carlin & O’Malley, 1996). These
characteristics lead to lessened motivation, poor relationships, and not being able to
perform tasks as usual. It must be noted though that these reports have been subjected to
great debate since several other studies have found no long-term deficits (Lezak et al.,
2004). The reduced memory capabilities may be a result of poor attention. Also, since
marijuana is frequently used with alcohol, there may be additive effects which may lead
to impaired functioning and may contribute to poor decision making resulting in unsafe
behaviors (e.g. driving under the influence).
47
Due to all of the cognitive deficits produced by marijuana alone, one may assume
that comorbid marijuana and cocaine use may exacerbate cognitive deficiencies;
however, the results indicate that cocaine users alone when compared to concurrent
cocaine and marijuana users, do not differ with respect to neurocognitive functioning.
One potential explanation for the groups being statistically similar is that none of the
individuals included in this study met criteria for marijuana-dependence (the dependence
criteria for marijuana is identical to the criteria for dependence criteria for cocaine
mentioned on page 7). . Thus, since these individuals were not marijuana-dependent,
their casual use of marijuana appears to not affect neurocognition. Future studies could
investigate the differences between cocaine-dependent and comorbid cocaine- and
marijuana-dependent individuals.
Despite the detailed and informative outcomes presented in the studies conducted,
some methodological limitations should be noted. First of all, the sample sizes are
relatively small and much larger sample sizes should be obtained before making
conclusive statements as to whether gender, ethnic, or comorbid drug use differences
exist in cocaine users. Secondly, since this neurocognitive battery only focused on
working memory, attention, and verbal learning and memory, a more comprehensive
battery may demonstrate differences in other domains. In addition, the study would have
been strengthened by including a comparison of a non-drug using, healthy control group
to determine exactly how prevalent the neurocognitive deficits are in cocaine-dependent
individuals (rather than relying on the age-matched normative values as a comparison).
Notwithstanding, the current results demonstrate that gender, ethnic, or comorbid drug

48
use differences in neurocognitive performance in cocaine-dependent participants may not
be prevalent.
Although there were no strong correlations between demographic and drug use
variables and neurocognition, there were some interesting findings by on the significance
values. For example, when comparing the oldest and youngest participants, younger
participants performed significantly better on 2 separate indices of working memory.
This supports the notion that prefrontal cortex functioning worsens over time. In addition,
there were no differences between those with the highest education versus those with the
lowest education. This is a critical finding because it demonstrates that level of education
(or years of formal learning) did not affect neurocognitive processes. Interestingly,
however, participants with the highest IQ’s performed significantly better when
compared to those with the lowest IQ’s across several domains including episodic
memory (both immediate and delayed) and working memory. These data support the
rationale for matching groups (involved in the gender, ethnic, and comorbid substance
use comparisons) on IQ in addition to the other demographic variables (e.g. age,
education, drug use variables, etc.). Moreover, this finding may demonstrate that IQ may
be protective against deficits caused by cocaine use in the domains of verbal and working
memory.
It has previously been reported that cocaine induced neurocognitive deficits are
correlated with the severity of cocaine use, suggesting a dose related effect (Bolla,
Rothman, and Cadet, 1999). Our findings indicate that individuals who used cocaine for
more years and for more days in the past 30 did not differ from those individuals that
used for the fewest years and the fewest days in the past 30. However, those individuals

49
who used more grams per day had significantly higher auditory accuracy (a measure of
working memory) when compared to those reporting using fewer grams per day. It may
be logically hypothesized that more years of use, recent use, and grams per day would
lead to further cognitive impairment which makes this finding especially interesting. One
potential explanation for this unexpected finding is that once a certain threshold is met,
further impairment does not occur. In other words, if an individual uses cocaine for a
certain number of years, it appears that the neurocognitive damage is done and further
years of use do not exacerbate those deficits. Similarly, if an individual uses for a certain
number of days per month or uses a certain amount of cocaine per day, those
neurocognitive deficits occur and remain at a consistent “steady state”, so that additional
use does not cause further impairment. This is speculation, however, and would need to
be evaluated in future studies.
With regard to the behavioral questionnaires (BDI-II, LSC-R, and the ASI-LITE),
there were no differences in neurocognition between those who scored the highest (e.g.
endorsed the most symptoms) versus those who scored the lowest (e.g. endorsed the
fewest symptoms) indicating that these behavioral variables may not affect
neurocognition. Memory deficits caused by clinical depression is a common occurrence
and has been termed “pseudodementia” (Patterson, 1986; Wells, 1979) which may lead to
speculation that increased BDI-II scores (endorsing more depressive symptoms) may
result in deficits in episodic or working memory; however, this was not found in the
current study. One possible explanation for this finding is that none of the individuals
had an Axis I psychiatric diagnosis of depression (rather they simply endorsed depressive
symptoms without meeting actual diagnostic criteria. Factors related to and potentially

50
affecting BDI-II symptomatology include lifetime stress and addiction severity. Previous
research has found that individuals with higher lifetime stress have significantly higher
BDI-II scores as well as addiction severity (Mahoney, Newton, Omar, Ross, & De La
Garza, 2012). In addition, chronic stress leads to deficits in declarative memory
(McEwen, 2004). In addition, higher ASI-LITE scores indicate elevated levels of
psychosocial dysfunction which may result in higher reported stress. However, in the
current study, those individuals with higher LSC-R scores and ASI-LITE scores did not
endorse more neurocognitive deficits. One potential explanation for these findings is that
their cocaine usage resulted in neurocognitive deficits, but they were not further affected
by stress nor addiction severity.
B. Study 2 – Rivastigmine or Huperzine as a treatment for neurocognitive impairment
The findings from this study demonstrated that while there was no effect of
rivastigmine on sustained attention, rivastigmine administration did significantly improve
episodic memory (as measured by increased immediate recall on the HVLT) and
working memory (by increased values on both the mean and max block length on the n-
back assessment). Since rivastigmine has previously been shown to reduce the positive
subjective effects (e.g. desire and likely to use) produced by the stimulant
methamphetamine, the cognitive enhancing effects of rivastigmine found in this
population of cocaine-dependent individuals is critical. A current trend in the
development of pharmacotherapies for cocaine-dependence involves the utilization of
combination medications (more than one medication that have different brain or
neurochemical targets to combat the various effects produced by cocaine use). Thus, one
solution would be to pair a cognitive enhancing agent with another medication that

51
decreases the reinforcing or positive effects produced by cocaine in an attempt to
maximize the potential benefit and outcomes. However, rivastigmine alone may
accomplish both of these tasks – by improving neurocognition and reducing the positive
subjective effects associated with cocaine usage. This is of great importance because
isolating a single efficacious compound may result in fewer side effects, less time
titrating to the most effective dose since there is only one medication being utilized, and
also eliminate the potential for adverse medication-medication interactions. Furthermore,
the results of this study are especially interesting given the fact that the same doses of
rivastigmine (3 and 6 mg) for a similar duration (6 days) showed no effect on
neurocognition in methamphetamine-dependent individuals (Kalechstein, 2011). This
demonstrates that the neurocognitive deficits produced by cocaine use may be more
easily treated by rivastigmine when compared to those deficits produced by
methamphetamine.
It is important to concede some limitations with this study that may have affected
the outcomes. Specifically, rivastigmine administration was most likely to be associated
with improved neurocognitive function in studies that utilized higher doses, e.g., up to 12
mg per day for much longer period of times, e.g., 39 weeks (Silver et al., 2009); for this
study, the maximum dose was 6 mg for a period of 8 days. It is plausible that this aspect
of the study design mitigated the efficacy of rivastigmine, especially on the domain of
attention where no effect was demonstrated as well as other domains of neurocognitive
functioning which were not evaluated.
There were no changes in neurocognition with respect to the domains of attention,
episodic memory, or working memory following huperzine administration. Since there is

52
no published literature on the effects of huperzine on neurocognition in cocaine-
dependent individuals, speculation as to why huperzine did not improve cognition in this
population warrants further discussion. Huperzine administration was most likely to be
associated with improved neurocognitive function in studies that utilized a longer
duration of treatment, e.g., 12 weeks (Xu, Liang, Juan-Wu, Zhang, Zhu, & Jiang2012),
whereas in this study, the maximum dose was 0.8 mg for a period of 8 days. It is
plausible that this aspect of the study design mitigated the efficacy of huperzine across all
domains. Because huperzine is characterized as a cognition enhancing agent that
modulates the acetylcholine system, it seemed reasonable to study whether low-dose,
short-term huperzine administration might remedy, at least in part, cocaine associated
neurocognitive impairment. Another explanation is that participants were exposed to
low-dose cocaine (40 mg) during the study; nonetheless, it probably was not a confound
given that exposure was identical for each study arm with regard to the amount and
timing of the cocaine dose.
C. Overall Conclusion and Summary
Respective of these outcomes from Study 1 and Study 2, we contend that cocaine
associated neurocognitive impairment remains an important target of treatment. This
perception is consistent with that of other leading researchers in the field, particularly
given the prevalence of cocaine associated neurocognitive impairment and the fact that
the condition does not resolve with protracted abstinence (Sofuoglu, 2010). Furthermore,
the association between neurocognitive impairment and functional outcomes, such as
employment status for participants diagnosed with other disorders, e.g., traumatic brain
injury, epilepsy, and HIV, is well-documented (Kalechstein, Newton, & van Gorp, 2003).

53
Given that cocaine addiction is associated with widespread functional difficulties, such as
unemployment and relapse to dependence, it is plausible that reversing neurocognitive
impairments associated with this disease will concurrently ameliorate these functional
difficulties as well.
Future studies might also examine the degree to which improved neurocognition
influences day-to-day functioning in long-term, high-dose cocaine users. While
laboratory-based studies, such as those conducted above, provide potentially important
information regarding the possibility of remediating cocaine-associated neurocognitive
impairment, the ultimate determination of medication efficacy will be whether
administration of a medication will confer some sort of benefit in terms of important
daily activities. For example, such individuals are often required to complete treatment
for the initiation and maintenance of abstinence from cocaine. Moreover, previous
studies have revealed an associated between poor working memory function and
increased likelihood of dropout from treatment (Jovanovski et al., 2005). Thus, a future
study might examine whether administration of rivastigmine concurrently improves
performance on episodic and working memory tasks and treatment outcome.
54
References
Aharonovich, E., Amrhein, P.C., Bisaga, A., Nunes, E.V., & Hasin, D.S. (2008).
Cognition, commitment language, and behavioral change among cocaine-
dependent patients. Psychology of Addictive Behaviors, 22(4), 557-562.
Aharonovich, E., Nunes, E., & Hasin, D. (2003). Cognitive impairment, retention and
abstinence among cocaine abusers in cognitive-behavioral treatment. Drug and
Alcohol Dependence, 71(2), 207-211.
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental
Disorders, Fourth Edition, Text Revision, DSM-IV-TR. Washington, DC:
American Psychiatric Association.
Anker, J.J., & Carroll, M.E. (2011). Females are more vulnerable to drug abuse than
males: evidence from preclinical studies and the role of ovarian hormones.
Current Topics in Behavioral Neuroscience, 8, 73-96.
Ardila, A., Rosselli, M., & Strumwasser, S. (1991). Neuropsychological deficits in
chronic cocaine abusers. International Journal of Neuroscience, 57(1-2), 73-79.
Beatty, W.W., Tivis, R., Stott, H.D., Nixon, S.J., & Parsons, O.A. (2000).
Neuropsychological deficits in sober alcoholics: influences of chronicity and
recent alcohol consumption. Alcohol: Clinical and Studyal Research, 24(2), 149-
154.
Bechara, A., & Martin, E.M. (2004). Impaired decision making related to working
memory deficits in participants with substance addictions. Neuropsychology,
18(1), 152-162.
55
Beck, A.T. (2006). Depression: Causes and Treatment. Philadelphia: University of
Pennsylvania Press.
Berry, J., van Gorp, W.G., Herzberg, D.S., Hinkin, C., Boone, K., Steinman, L., et al.
(1993). Neuropsychological deficits in abstinent cocaine abusers: preliminary
findings after two weeks of abstinence. Drug and Alcohol Dependence, 32(3),
231-237.
Bleecker, M.L., Bolla-Wilson, K., Agnew, J., & Meyers, D.A. (1988). Age-related sex
differences in verbal memory. Journal of Clinical Psychologyl, 44(3), 403-411.
Blusewicz, M.J., Dustman, R.E., Schenkenberg, T., & Beck, E.C. (1977).
Neuropsychological correlates of chronic alcoholism and aging. Journal of
Nervous and Mental Disease, 165, 348-355.
Bolla, K.I., Rothman, R., & Cadet J.L. (1986) Dose-related neurobehavioral effects of
chronic cocaine use. Canadian Family Physician, 32, 2607-2610.
Bolla, K. I., Eldreth, D.A., Matochik, J.A., & Cadet, J.L. (2004). Sex-related differences
in a gambling task and its neurological correlates. Cerebral Cortex, 14(11), 1226-
1232.
Bolla, K.C., & Cadet, J.L. (2007). Cocaine. In: Kalechstein, A., van Gorp, W.
(Eds.), Neuropsychology and Substance Use. Taylor and Francis, New York,
New York.
Brandt, J.B. (2005). Hopkings Verbal Learning Test - Revised (HVLT-R). Lutz, FL:
Psychological Assessment Resources, Inc.
Brust, J. (1993). Neurological aspects of substance abuse. Boston: Butterworth-
Heinmann.
56
Brust, J. (2000). Cannabis. In P.S. Spencer & H.H Schaumberg (Eds.), Studyal and
clinical neurotoxicology (2nd
ed.). New York: Oxford University Press.
Buss, A.H., & Perry, M. (1992). The aggression questionnaire. Journal of Personality
and Social Psycholology, 63(3), 452–459.
Budney, A.J., Higgins, S.T., Hughes, J.R., & Bickel, W.K. (1993). Nicotine and caffeine
use in cocaine-dependent participants. Journal of Substance Abuse, 5(2), 117-130.
Butters, N., & Stuss, D.T. (1989). Diencephalic amnesia. In F. Boller & J. Grafman
(Eds.), Handbook of Neuropsychology (Vol. 3). Amsterdam: Elsevier.
Byrd, D.A., Miller, S., Reilly, J., Weber, S., Wall, T.L., & Heaton, R.K. (2006). Early
environmental factors, ethnicity, and adult cognitive test performance. Clinical
Neuropsychology, 20(2), 243-260.
Cacciola, J.S., Koppenhaver, J.M., McKay, J.R., & Alterman, A.I. (1999). Test-Retest
reliability of the lifetime items on the Addiction Severity Index. Psychological
Assessment, 11, 86-93.
Carlin, A.S., & O’Malley (1996). Neuropsychological consequences of drug abuse. In I.
Grant & K.M. Adams (Eds.), Neuropsychological assessment of neuropsychiatric
disorders. New York: Oxford University Press.
Cerhan, J.R., Folsom, A.R., Mortimer, J.A., Shahar, E., Knopman, D.S., McGovern,
P.G., et al. (1998). Correlates of cognitive function in middle-aged adults.
Atherosclerosis Risk in Communities (ARIC) Study Investigators. Gerontology
44, 95-105.

57
Chang, L., Cloak, C., Patterson, K., Grob, C., Miller, E.N., & Ernst, T. (2005). Enlarged
striatum in abstinent methamphetamine abusers: a possible compensatory
response. Biological Psychiatry, 57(9), 967-974.
Colbach, E.M., & Crowe, R.R (1970). Marijuana associated psychosis in Vietnam.
Military Medicine, 135, 571-573
Conners, C. K. (2002). Conners' Continuous Performance Test - II (CPT-II): Multi-
Health Systems, Inc.
Craik, F. (1977). Similarities between the effects of aging and alcoholic intoxication on
memory performance, construed within a “levels of processing” framework. In
I.M. Birnbaum & E.S. Parker (Eds.), Alcohol and human memory. Hillsdale, NJ:
Erlbaum.
Drake, R.E., & Noordsy, D.L. (1995). The role of inpatient care for patients with co-
occurring severe mental disorder and substance use disorder. Community Mental
Health Journal, 31,279-282.
Durazzo, T.C., Meyerhoff, D.J., & Nixon, S.J. (2010). Chronic cigarette smoking:
implications for neurocognition and brain neurobiology. International Journal of
Environmental Research and Public Health. 7(10), 3760-91.
Elwan, O., Hassan, A.A., Abdel Naseer, M., Elwan, F., Deif, R., El Serafy, O., et al.
(1997). Brain aging in a sample of normal Egyptians cognition, education,
addiction and smoking. Journal of the Neurological Sciences, 148, 79-86.
Ernst, M., Heishman, S.J., Spurgeon, L., & London, E.D. (2001). Smoking history and
nicotine effects on cognitive performance. Neuropsychopharmacology, 25, 313-
319.

58
Feldman, H.H., & Lane, R. (2007). Rivastigmine: a placebo controlled trial of twice daily
and three times daily regimens in patients with Alzheimer's disease. Journal of
Neurology, Neurosurgery and Psychiatry,78(10), 1056-1063.
Ford, G.R., Haley, W.E., Thrower, S.L., West, C.A., & Harrell, L.E. (1996). Utility of
Mini-Mental State Exam scores in predicting functional impairment among white
and African American dementia patients. Journal of Gerontology Series A, 51(4),
185-188.
Frankfort, S.V., Appels, B.A., de Boer, A., Tulner, L.R., van Campen, J.P., Koks, C. et
al. (2007). Identification of responders and reactive domains to rivastigmine in
Alzheimer's disease. Pharmacoepidemiology and Drug Safety, 16(5), 545-551.
Fried, P.A., Watkinson, B., & Gray, R. (2006). Neurocognitive consequences of cigarette
smoking in young adults—A comparison with pre-drug performance.
Neurotoxicology and Teratology, 28(4), 517-525.
George, T.P., Vessicchio, J.C., Termine, A., Sahady, D.M., Head, C.A., Pepper, W.T., et
al. (2002). Effects of smoking abstinence on visuospatial working memory
function in schizophrenia. Neuropsychopharmacology, 26, 75-85.
Ghahremani, D.G., Tabibnia, G., Monterosso, J., Hellemann, G., Poldrack, R.A., &
London, E.D. (2011). Effect of modafinil on learning and task-related brain
activity in methamphetamine-dependent and healthy participants.
Neuropsychopharmacology,36(5), 950-959.
Goldstein, R.Z., Woicik, P.A., Maloney, T., Tomasi, D., Alia-Klein, N., Shan, J., et al.
(2010). Oral methylphenidate normalizes cingulate activity in cocaine addiction

59
during a salient cognitive task. Proceedings of the National Academy of Science
USA, 107(38), 16667-16672.
Gooding, D.C., Burroughs, S., & Boutros, N.N. (2008). Attentional deficits in cocaine-
dependent patients: converging behavioral and electrophysiological evidence.
Psychiatry Research, 160(2), 145-154.
Gonzalez, R., Carey, C., & Grant, I. (2002). Nonacute (residual) neuropsychological
effects of cannabis use: a qualitative analysis and systematic review. Journal of
Clinical Pharmacology, 42, 48S-57S.
Graff-Radford, N.R., Heaton, R.K., Earnest, M.P., & Rudikoff, J.C. (1982). Brain
atrophy and neuropsychological impairment in young alcoholics. Journal of
Studies on Alcohol, 43, 859-868.
Haney, M., Foltin, R.W., & Fischman, M.W. (1998). Effects of pergolide on
intravenous cocaine self-administration in men and women. Psychopharmacology
137(1), 15–24.
Hasselmo, M.E., & Sarter, M. (2011). Modes and models of forebrain cholinergic
neuromodulation of cognition. Neuropsychopharmacology, 36(1), 52-73.
Herlitz, A., Nilsson, L. G., & Backman, L. (1997). Gender differences in episodic
memory. Memory and Cognition, 25(6), 801-811.
Ikeda, H., Ikeda, N., Miura, H., Tominaga, H., Yamada, Y., & Saito, T. (2003).
Difference between alcohol dependence and nicotine dependence in cognitive
dysfunction. Nihon Arukoru Yakubutsu Igakkai Zasshi, 38(6), 512-518.
Iverson, L.L. (2000). The science of marijuana. New York: Oxford University Press.

60
Jacobsen, L.K., Krystal, J.H., Mencl, W.E., Westerveld, M., Frost, S.J., & Pugh, K.R.
Effects of smoking and smoking abstinence on cognition in adolescent tobacco
smokers. Biological Psychiatry, 57, 56-66.
Jaeggi, S.M., Buschkuehl, M., Jonides, J., & Perrig, W.J. (2008). Improving fluid
intelligence with training on working memory. Proceedings of the National
Academy of Science USA, 105(19), 6829-6833.
Jovanovski, D., Erb, S., & Zakzanis, K.K. (2005). Neurocognitive deficits in cocaine
users: a quantitative review of the evidence. Journal of Clinical and Studyal
Neuropsychology, 27(2), 189-204.
Kalechstein, A., Yoon, J., Mahoney, J.J., & De La Garza, R. (2013). Modafinil
Pretreatment Improves Working Memory, but not Episodic Memory or Sustained
Attention, in Long—term, High—Dose Cocaine Users.
Neuropsychopharmacology, 64(1), 472-478.
Kalechstein, A.D., Newton, T.F., & van Gorp, W.G. (2003). Neurocognitive functioning
is associated with employment status: a quantitative review. Journal of Clinical
Pharmacology, 25(8), 1186-91.
Kalmijn, S., van Boxtel, M.P., Verschuren, M.W., Jolles, J., & Launer, L.J. (2002).
Cigarette smoking and alcohol consumption in relation to cognitive performance
in middle age. American Journal of Epidemiology. 156, 936-944.
Kimura, D. (1999). Sex and cognition. Cambridge, Mass.: MIT Press.
Kleber, H. D. (1994). Our current approach to drug abuse--progress, problems, proposals.
New England Journal of Medicine, 330(5), 361-365.

61
Kuller, L. H., Shemanski, L., Manolio, T., Haan, M., Fried, L., Bryan, N., et al. (1998).
Relationship between ApoE, MRI findings, and cognitive function in the
Cardiovascular Health Study. Stroke, 29(2), 388-398.
Lejbak, L., Crossley, M., & Vrbancic, M. (2011). A male advantage for spatial and object
but not verbal working memory using the n-back task. Brain Cognition, 76(1),
191-196.
Lezak, M.D., Howieson, D.B., & Loring, D.W. (2004). Neuropsychological Assessment.
(4th ed.). New York: Oxford University Press.
Li, J., Wu, H. M., Zhou, R.L., Liu, G.J., & Dong, B.R. (2008). Huperzine A for
Alzheimer's disease. Cochrane Database System Reviews (2), CD005592.
Little, J.T., Walsh, S., & Aisen, P.S. (2008). An update on huperzine A as a treatment for
Alzheimer's disease. Expert Opinion on Investigational Drugs, 17(2), 209-215.
Lukas, S.E., Sholar, M., Lundahl, L.H., Lamas, X., Kouri, E., Wines, J.D., et al. (1996).
Sex differences in plasma cocaine levels and subjective effects after
acute cocaine administration in human volunteers. Psychopharmacology, 12,
346-54.
Mancuso, G., Lejeune, M., & Ansseau, M. (2001). Cigarette smoking and attention:
processing speed or specific effects? Psychopharmacology, 155, 372-8.
Mahoney, J.J., Newton, T.F., Omar, Y., Ross, E.L., & De La Garza, R. (in press). The
relationship between lifetime stress and addiction severity in cocaine-dependent
participants. European Neuropsychopharmacology.

62
Manly, J.J., Jacobs, D.M., Sano, M., Bell, K., Merchant, C.A., Small, S.A., et al. (1998).
Cognitive test performance among nondemented elderly African Americans and
whites. Neurology, 50(5), 1238-1245.
McEwen, B.S. (2004). Protection and damage from acute and chronic stress: allostasis
and allostatic overload and relevance to the pathophysiology of psychiatric
disorders. Annals of the New York Academy of Science, 32, 1-7.
McLellan, A.T., Cacciola, J.C., Alterman, A.I., Rikoon, S.H., & Carise, D. (2006). The
Addiction Severity Index at 25: origins, contributions and transitions. American
Journal on Addictions, 15, 113-124.
McHugo, G.J., Caspi, Y., Kammerer, N., Mazelis, R., Jackson, E.W., Russell, L., et al.
(2005). The assessment of trauma history in women with co-occurring substance
abuse and mental disorders and a history of interpersonal violence. The Journal
of Behavioral Health Services & Research, 32, 113-127.
Nicholson, K. G., & Kimura, D. (1996). Sex differences for speech and manual skill.
Perceptual and Motor Skills, 82(1), 3-13.
O’Connor, M., & Verfaillie, M. (2002). The amnestic syndrome: Overview and subtypes.
In A.D. Baddelley et al. The handbook of memory disorders. Chichester,
UK: Wiley.
Parsons, O.A. & Farr, S.P. (1981). The neuropsychology of alcohol and drug use. In S.B.
Filskov & T.J. Boll (Eds.), Handbook of clinical neuropsychology. New York:
Wiley Interscience.
Parsons, O. A., & Nixon, S. J. (1993). Neurobehavioral sequelae of alcoholism.
Neurology Clinic, 11(1), 205-218.

63
Patterson C. (1986). The Diagnosis and Differential Diagnosis of Dementia and Pseudo-
dementia in the Elderly. Canadian Family Physician, 32, 2607-2610.
Peters, M., Manning, J.T., & Reimers, S. (2007). The effects of sex, sexual orientation,
and digit ratio (2D:4D) on mental rotation performance. Archives of Sex and
Behavior, 36(2), 251-260.
Pishkin, V., Lovallo, W.R., & Bourne, L.E. (1985). Chronic alcoholism in males:
Cognitive deficit as a function of age of onset, age, and duration. Alcoholism:
Clinical and Studyal Research, 9, 400-405.
Plessinger, M.A., & Woods, J.R. (1990). Progesterone increases cardiovascular toxicity
to cocaine in nonpregnant ewes. American Journal of Obstetrics and
Gynecology, 63, 1659-1664.
Pope, H.G., & Yurgelun-Todd, D. (1996). The residual cognitive effects of heavy
marijuana use in college students. Journal of the American Medical Association,
275, 521-527.
Pope, H.G., Gruber, A.J., & Yurgelun-Todd, D. (1995). The residual neuropsychological
effects of cannabis: The current status of research. Drug and Alcohol
Dependence, 38, 25-34.
Solowij, N. (1998). Cannabis and cognitive functioning. New York: Cambridge
University Press.
Price, K.L., DeSantis, S.M., Simpson, A.N., Tolliver, B.K., McRae-Clark, A.L., Saladin,
M.E., et al. (2011). The impact of clinical and demographic variables on cognitive
performance in methamphetamine-dependent participants in rural South Carolina.
American Journal on Addictions, 20(5), 447-455.
64
Rahman, Q., & Clarke, C.D. (2005). Sex differences in neurocognitive functioning
among abstinent recreational cocaine users. Psychopharmacology (Berl), 181(2),
374-380.
Rahman, Q., Wilson, G.D., & Abrahams, S. (2003). Sexual orientation related differences
in spatial memory. Journal of International Neuropsycholological Society, 9(3),
376-383.
Rahman, R.A., van Turennout, M., & Levelt, W.J. (2003). Phonological encoding is not
contingent on semantic feature retrieval: an electrophysiological study on object
naming. Journal of Studyal Psychology Learning Memory and Cognition, 29(5),
850-860.
Rawson, R. A., Huber, A., McCann, M., Shoptaw, S., Farabee, D., Reiber, C., et al.
(2002). A comparison of contingency management and cognitive-behavioral
approaches during methadone maintenance treatment for cocaine dependence.
Archives of General Psychiatry, 59(9), 817-824.
Razani, J., Boone, K., Lesser, I., & Weiss, D. (2004). Effects of cigarette smoking
history on cognitive functioning in healthy older adults. American Journal of
Geriatric Psychiatry, 12, 404-411.
Roll, J.M., Higgins, S.T., Budney, A.J., Bickel, W.K., & Badger, G.J. (1996). A
comparison of cocaine-dependent cigarette smokers and non-smokers on
demographic, drug use and other characteristics. Drug and Alcohol Dependence,
40(3), 195-201.
Ryan, C., & Butters, N. (1986). Neuropsychology of alcoholism. In D. Wedding, A.M.
Hosrton, Jr., & J.S. Webster (Eds.), The neuropsychology handbook. New York:

65
Springer.
Sakurai, Y., & Kanazawa, I. (2002). Acute effects of cigarettes in non-deprived smokers
on memory, calculation and executive functions. Human Psychopharmacology,
17, 369-373.
Schoenberg, M. R., Scott, J. G., Duff, K., & Adams, R. L. (2002). Estimation of WAIS-
III intelligence from combined performance and demographic variables:
development of the OPIE-3. Clinical Neuropsychology, 16(4), 426-437.
Scott, J. C., Woods, S. P., Matt, G. E., Meyer, R. A., Heaton, R. K., Atkinson, J. H., et al.
Neurocognitive effects of methamphetamine: a critical review and meta-analysis.
Neuropsychology Reviews, 17(3), 275-297.
Sharma, A., Plessinger, M.A., Sherer, D.M., Liang, C.S., Miller, R.K., & Woods, J.R.
(1992). Pregnancy enhances cardiotoxicity of cocaine: role of progesterone.
Toxicology and Applied Pharmacology, 113, 30-5.
Silver, J. M., Koumaras, B., Meng, X., Potkin, S. G., Reyes, P. F., Harvey, P. D., et al.
(2009). Long-term effects of rivastigmine capsules in patients with traumatic
brain injury. Brain Injury, 23(2), 123-132.
Sinha, R. (2001). How does stress increase risk of drug abuse and relapse?
Psychopharmacology, 158, 343–359.
Sofuogluy, M., Sugarman, D.E., & Carroll, K.M. (2010). Cognitive function as an
emerging treatment target for marijuana addiction. Studyal and Clinical
Psychopharmacology, (18)2, 109-119.
Stoffelmayr, B.E., Mavis, B.E., & Kasim, R.M. (1994). The longitudinal stability of the
Addiction Severity Index. Journal of Substance Abuse Treatment, 11, 373-378.

66
Tenovuo, O., Alin, J., & Helenius, H. (2009). A randomized controlled trial of
rivastigmine for chronic sequels of traumatic brain injury-what it showed and
taught? Brain Injury, 23(6), 548-558.
Ungerer, O., Deter, H.C., Fikentscher, E., & Konzag, T.A. (2009). Improved diagnostics
of trauma-related disease through the application of the Life-Stressor Checklist.
Psychotherapie, Psychosomatik, Medizinische Psychologie, 60, 434-441.
Verdejo-Garcia, A., Vilar-Lopez, R., Perez-Garcia, M., Podell, K., & Goldberg, E.
(2006). Altered adaptive but not veridical decision-making in substance
dependent participants. Journal of the International Neuropsychological Society,
12(1), 90-99.
Voyer, D., Voyer, S., & Bryden, M. P. (1995). Magnitude of sex differences in spatial
abilities: a meta-analysis and consideration of critical variables. Psychology
Bulletin, 117(2), 250-270.
Wang, R., Yan, H., & Tang, X. C. (2006). Progress in studies of huperzine A, a natural
cholinesterase inhibitor from Chinese herbal medicine. Acta Pharmacologica
Sinica, 27(1), 1-26.
Wechsler, D. (2007). Wechsler Adult Intelligence Scale – III. San Antonio, TX: The
Psychological Corporation.
Wells C.E. (1979). Pseudodementia. American Journal of Psychiatry, 136, 895-900.
Wolfe, J., & Kimerling, R. (1997). Gender issues in the assessment of posttraumatic
stress disorder. Guilford, New York.
Woods, J.R., & Plessinger, M.A. (1990). Pregnancy increases cardiovascular toxicity
to cocaine. American Journal of Obstetrics and Gynecology 162(2), 529-33.

67
Xu, Z.Q., Liang, X.M., Juan, W., Zhang, Y.F., Zhu, C.X., & Jiang, X.J. (2012).
Treatment with Huperzine A improves cognition in vascular dementia patients.
Cell Biochemistry and Biophysics, 62(1), 55-58.
Zangara, A. (2003). The psychopharmacology of huperzine A: an alkaloid with cognitive
enhancing and neuroprotective properties of interest in the treatment of
Alzheimer's disease. Pharmacology, Biochemistry, and Behavior, 75(3), 675-686.