current pharmacological treatment approaches for alcohol...
TRANSCRIPT

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ieop20
Download by: [Inova Fairfax Hospital] Date: 07 January 2017, At: 22:30
Expert Opinion on Pharmacotherapy
ISSN: 1465-6566 (Print) 1744-7666 (Online) Journal homepage: http://www.tandfonline.com/loi/ieop20
Current pharmacological treatment approachesfor alcohol dependence
Christian A Müller MD, Olga Geisel MD, Roman Banas & Andreas Heinz MD
To cite this article: Christian A Müller MD, Olga Geisel MD, Roman Banas & Andreas Heinz MD(2014) Current pharmacological treatment approaches for alcohol dependence, Expert Opinionon Pharmacotherapy, 15:4, 471-481, DOI: 10.1517/14656566.2014.876008
To link to this article: http://dx.doi.org/10.1517/14656566.2014.876008
Published online: 23 Jan 2014.
Submit your article to this journal
Article views: 1417
View related articles
View Crossmark data
Citing articles: 2 View citing articles
1. Introduction
2. New pharmacological
treatment approaches
3. Expert opinion
Review
Current pharmacologicaltreatment approaches for alcoholdependenceChristian A Muller†, Olga Geisel, Roman Banas & Andreas Heinz†Charite -- Universitatsmedizin Berlin, Department of Psychiatry, Campus Charite Mitte, Berlin,
Germany
Introduction: At present, the substances acamprosate, naltrexone and
disulfiram are available for pharmacotherapy in alcohol dependence, but
clinical studies found only modest effect sizes of these treatment options.
Areas covered: This article focuses on current pharmacological treatment
approaches for alcohol dependence, which have been evaluated in random-
ized, placebo-controlled trials (RCTs).
Expert opinion: Besides the opioid system modulator nalmefene, which has
recently been approved as a medication for the reduction of alcohol
consumption, several compounds have been investigated in patients with
alcohol dependence using a randomized, placebo-controlled design. In these
studies, the antiepileptic drugs topiramate and gabapentin were found to be
effective in improving several drinking-related outcomes, whereas levetirace-
tam failed to show efficacy in the treatment of alcohol dependence. Clinical
studies using (low-dose) baclofen, a selective GABA-B receptor agonist,
produced conflicting results, so that results of further trials are needed.
Varenicline has also shown mixed results in two RCTs, but might possibly be
useful in patients with comorbid nicotine dependence. The a1 adrenergic
antagonist prazosin is currently under investigation in alcohol dependence
with and without comorbid posttraumatic stress disorder (PTSD). Finally, first
clinical evidence suggests that the 5-HT3 antagonist ondansetron might possi-
bly be used in future within a pharmacogenetic treatment approach in
alcohol dependence.
Keywords: alcohol dependence, pharmacotherapy, reduced drinking, relapse prevention
Expert Opin. Pharmacother. (2014) 15(4):471-481
1. Introduction
Alcohol use disorders (AUDs) represent common and serious diseases, which in mostcases require intensive medical treatment; up to 40% of hospitalized patients sufferfrom AUDs [1]. An alcohol detoxification is often the first step in the treatment ofalcohol dependence and mainly addresses the complications of the underlyingdisease. After detoxification, the vast majority of alcohol-dependent patients (up to85%) suffer from relapses [2]. Improvement of the treatment outcome can beachieved by combining psychosocial with pharmacological interventions. However,since alcohol dependence represents a heterogeneous disorder that results fromgene � environment interactions, which differ from patient to patient, it seemsunlikely that one single medication will show efficacy in all alcohol-dependentpatients [3]. Currently, the anti-craving substances acamprosate and naltrexone aswell as the aversion therapeutic agent disulfiram are available for pharmacotherapyof alcohol dependence. Acamprosate was thought to modulate glutamatergic trans-mission by inhibition of N-methyl-D-aspartate (NMDA) and metabotropic gluta-mate (mGluR5) receptors [4]. However, a recent study suggests that acamprosate
10.1517/14656566.2014.876008 © 2014 Informa UK, Ltd. ISSN 1465-6566, e-ISSN 1744-7666 471All rights reserved: reproduction in whole or in part not permitted

might act through calcium [5]. In a meta-analysis including24 clinical trials [6], acamprosate has been shown to signifi-cantly reduce the risk of relapse to 86% of the risk of the pla-cebo group and to increase cumulative abstinence duration by11% compared to placebo. In terms of tolerability, diarrheawas the only side effect that occurred more frequently inpatients treated by acamprosate than placebo. With regard tothe opioid antagonist naltrexone, a meta-analysis including47 clinical trials [7] found a significant risk reduction for relapseto heavy drinking (defined as ‡ 5 standard drinks/day formen; ‡ 4 standard drinks/day for women, 1 standarddrink = 12 g of alcohol) to 83% of the risk of the placebogroup and a reduction of drinking days by 4% compared toplacebo. Gastrointestinal and sedative effects were the mostcommon side effects of naltrexone. However, these meta-analyses found only modest effect sizes of these treatmentapproaches, with a number needed to treat (NNT) of 9 forboth acamprosate and naltrexone. Moreover, some large trialsfailed to replicate the positive effects of acamprosate [8,9].The aldehyde dehydrogenase inhibitor disulfiram has been
evaluated in numerous trials in alcohol dependence showinginconsistent results [10,11]. Most of these studies possessedrelevant methodological limitations [10]; only three trialsinvestigated (unsupervised) disulfiram using a randomized,double-blind, placebo-controlled design. One study in a smallsample of adolescent patients reported a higher abstinence rate(54 vs 15%) and a higher cumulative abstinence duration(69 vs 30 days) for disulfiram [12]. In contrast, two large stud-ies could not show unsupervised disulfiram to be superiorwith regard to total abstinence compared to placebo [13,14].Interestingly, disulfiram has shown preliminary efficacy inreducing craving and relapse rates in cocaine dependence [15].
These effects might possibly be related to the ability ofdisulfiram to inhibit the dopamine beta-hydroxylase (DBH),leading to an increase in dopamine concentrations whiledecreasing the concentrations of norepinephrine in thebrain [16-18].
In summary, given the high relapse rates and the sufferingof dependent patients, further research is urgently needed todevelop more effective pharmacotherapies for the treatmentof alcohol dependence.
2. New pharmacological treatmentapproaches
2.1 Approved medications
2.1.1 NalmefeneNalmefene, an opioid system modulator structurally related tonaltrexone, possesses antagonistic properties at the µ- andd-receptor and partial agonistic properties at the k-receptor[19]. It has already been evaluated in several randomized,placebo-controlled trials (RCTs) in alcohol dependence [20-22].With the exception of one study [23], all trials reported areduction of heavy drinking during the treatment withnalmefene. Recently, the results of two large multicenterRCTs have been published [24,25]; in both studies, alcohol-dependent patients received an ‘as-needed’ treatment withnalmefene (-18 mg/day) or placebo over 24 weeks.
The first study in a sample of 604 patients reported agreater reduction of heavy-drinking days (-2.3 days/month)and total alcohol consumption (-11.0 g/day) in the nalmefenegroup compared to placebo [24]. Side effects were more com-mon in the nalmefene group and included nausea, dizziness,fatigue, sleep disorder, insomnia, hyperhidrosis and vomiting.Thirty-eight serious adverse events (AEs) were reported(18 nalmefene vs 20 placebo). The authors reported moredropouts due to side effects in the nalmefene group(23 vs 7%).
The second study in 718 patients found a significant reduc-tion in heavy-drinking days (group diff.: -1.7 days/month),but no significant reduction in total alcohol consumption(group diff.: -5.0 g/day, p = 0.088) [25]. The most commonside effects were dizziness, nausea and insomnia, with an inci-dence two times higher in the nalmefene group compared toplacebo. The rate of dropouts due to side effects did not differbetween the groups (6.7 nalmefene vs 5.9% placebo). SeriousAEs occurred in 25 patients (8 nalmefene vs 17 placebo).
In February 2013, nalmefene has been approved by the Euro-pean Medicines Agency (EMA) for the reduction of alcoholconsumption in alcohol-dependent patients who have a highdrinking-risk level without physical withdrawal symptomsand who do not require immediate detoxification [26].
2.2 Off-label medications (Table 1)2.2.1 LevetiracetamLevetiracetam is a second-generation antiepileptic drug thathas recently been investigated in several preclinical and
Article highlights.
. The efficacy of topiramate has repeatedly been reportedby well-designed randomized, placebo-controlled trials(RCTs), but its use might be limited by its side effects.
. The anticonvulsant gabapentin has been found to beeffective and well tolerated in two independent clinicaltrials, but further studies are needed to define its futurerole in the treatment of alcohol dependence.
. RCTs using low-dose baclofen produced conflictingresults in terms of efficacy. The efficacy and tolerabilityof high-dose baclofen are currently under investigation.
. Varenicline has shown mixed results in two RCTs, butmight possibly be useful in patients with comorbidnicotine dependence.
. Based on the findings from one pilot trial usingprazosin, further studies investigating its effects inalcohol dependence with and without comorbid PTSDare currently ongoing.
. First clinical evidence suggests that ondansetron mightpossibly be used in future within a pharmacogenetictreatment approach in alcohol dependence.
This box summarizes key points contained in the article.
C. A. Muller et al.
472 Expert Opin. Pharmacother. (2014) 15(4)
Table
1.Studych
aracteristicsandoutcomesofrandomized,placebo-controlledtrials
investigatingoff-labelmedicationsin
alcoholdependence.
Study
NDuration
Dose
Efficacy
Tolerabilty
Levetiracetam
Richteretal.[39]
201
16weeks
Targetdose:
2000mg/day
Levetiracetam
=placebo:rate
ofsevere
relapse,timeto
severe
relapse,abstinence
rate
Nodifferencesin
AEsandSAEs
Fertig
etal.[40]
130
16weeks
Targetdose:
2000mg/day
extended-release
Levetiracetam
=placebo:percentof
heavy-drinkingdays,percentofsubjectswith
noheavy-drinkingdays
Levetiracetam:fatigue,nodifferences
inSAEs
Topiramate
Johnsonetal.[46]
150
12weeks
25--300mg/day
Topiramate
>placebo:drinksperday,
drinks
perdrinkingday,
fewerheavy-drinkingdays,
days
abstinent
Topiramate:dizziness,paraesthesia,
psychomotorslowing,memory
or
concentrationim
pairment,weightloss,
noSAEs
Johnsonetal.[47]
371
14weeks
upto
300mg/day
Topiramate
>placebo:percentageof
heavy-drinkingdays
Topiramate:paraesthesia,taste
perversion,anorexia,difficultywith
concentration/attention,pruritus;
no
differencesin
SAEs
Baltierietal.[48]
155
12weeks
Targetdose:
300mg/day
Topiramate
=naltrexon>placebo:timeto
firstrelapse,cumulative
abstinence
duration,
weeksofheavy
drinking
Nodifferencesin
AEs,noSAEs
Rubio
etal.[49]
76
12weeks
upto
250mg/day
Topiramate
>placebo:drinksperdrinking
day,
percentageofheavy-drinkingdays,
percentageofabstinentdays
Nodetailedreport
Gabapentin
Furierietal.[50]
60
4weeks
600mg/day
Gabapentin>placebo:drinksperday,
percentageofheavy-drinkingdays,
percentageofabstinentdays
Nodifferencesin
AEs,noSAEs
Masonetal.[51]
150
12weeks
900and
1800mg/day
Gabapentin1800mg/day>gabapentin
900mg/day>placebo:rate
ofabstinence,
rate
ofnoheavy
drinking
Nodifferencesin
AEs,
nodrug-relatedSAEs
Baclofen
Addolorato
etal.[61]
39
4weeks
30mg/day
Baclofen>placebo:abstinence
rate,
cumulative
abstinence
duration
Nodifferencesin
AEs,noSAEs
Addolorato
etal.[62]
84
12weeks
30mg/day
Baclofen>placebo:abstinence
rate,
cumulative
abstinence
duration
Nodifferencesin
AEs,noSAEs
AEs:Adverseevents;SAEs:
Seriousadverseevents.
Current pharmacological treatment approaches for alcohol dependence
Expert Opin. Pharmacother. (2014) 15(4) 473

Table
1.Studych
aracteristicsandoutcomesofrandomized,placebo-controlledtrials
investigatingoff-labelmedicationsin
alcoholdependence
(continued).
Study
NDuration
Dose
Efficacy
Tolerabilty
Garbutt
etal.[63]
80
12weeks
30mg/day
Baclofen=placebo:percentageof
heavy-drinkingdays,percentageabstinent
days
Nodifferencesin
AEs,
noSAEs
Addolorato
etal.[64]
42
12weeks
30and
60mg/day
Baclofen=placebo:heavy-drinkingdays,
abstinent.days,timeto
firstlapse,timeto
firstrelapse.Secondary
analysis:
baclofen
60mg/day>baclofen
30mg/day>placebo:number
ofdrinksperday
Nodifferencesin
AEs,
noSAEs
Varenicline
Plebanietal.[69]
40
13weeks
2mg/day
Varenicline=placebo:alcoholuse
Varenicline>placebo:rate
ofcigarette
smoking
Nodifferencesin
AEs,
noSAEs
Littenetal.[70]
200
13weeks
2mg/day
Varenicline>placebo:percentheavy-drinking
days,drinksperday,
drinksperdrinkingday,
numberofcigarettessm
oked
Varenicline:nausea,abnorm
aldreams,
constipation;nodifferencesin
SAEs
Prazo
sin
Sim
psonetal.[72]
24
6weeks
16mg/day
Prazosin>placebo:numberofdrinkingdays,
numberofdrinks
Nodifferencesin
AEs,
noSAEs
Ondansetron
Johnsonetal.[74]
271
11weeks
2,8or
32µg
/kgperday
Ondansetron(alldosages)
>placeboin
early-onsetAD:numberofdrinksperday,
drinksperdrinkingday
Nodifferencesin
AEs,
noSAEs
Johnsonetal.[75,76]
283
11weeks
8µg
/kgperday
Ondansetron=placebo;
withsubgroupsaccordingto
genotype:ondansetron>placebo:
drinksperdrinkingday,
percentageofdays
abstinent,percentageofheavy-drinking
days
[76]
Ondansetron:fatigue,nomedication-
relatedSAEs
CorreaFilhoand
Baltieri
[77]
102
12weeks
16mg/day
Ondansetron=placebo:percentageof
abstinentdays,percentageofheavy-drinking
days
Nodifferencesin
AEs,
noSAEs
AEs:Adverseevents;SAEs:
Seriousadverseevents.
C. A. Muller et al.
474 Expert Opin. Pharmacother. (2014) 15(4)

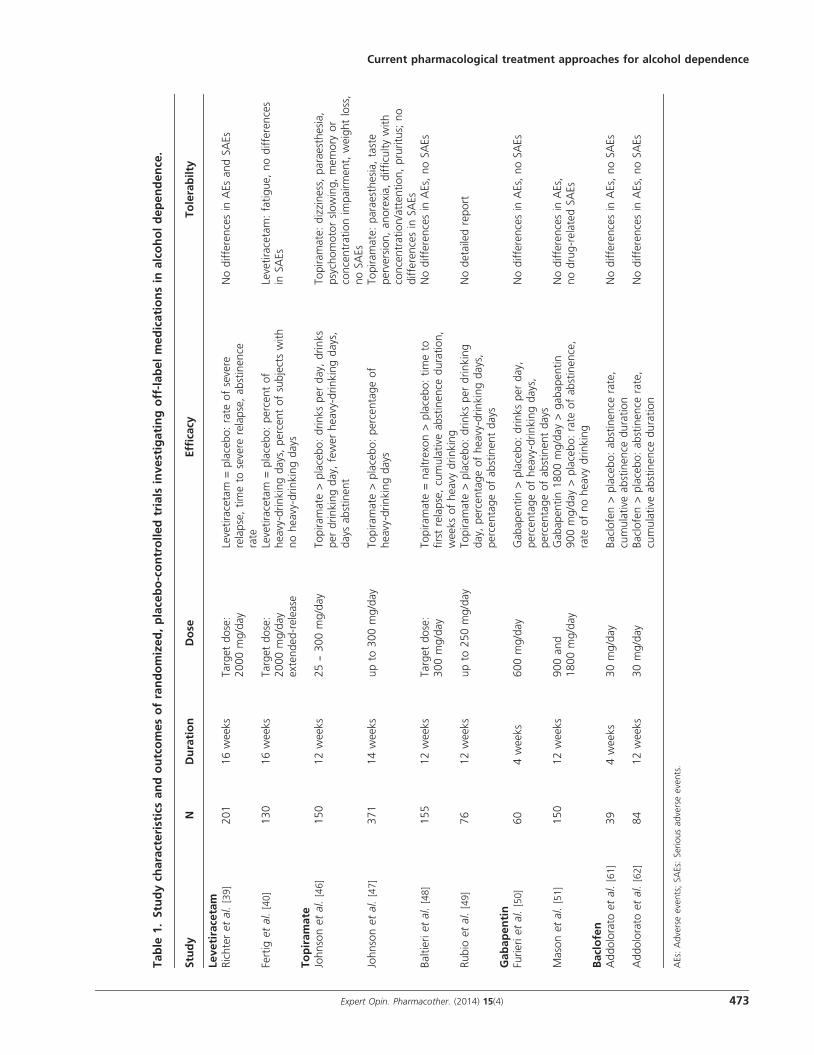
clinical studies in alcohol dependence [27,28]. The precisemechanism of action of levetiracetam is still unclear. It hasno significant affinity to gamma-aminobutyric acid (GABA)or glutamate receptors and does not directly interact withthe benzodiazepine binding site [29-31]. Levetiracetam wasreported to bind to the synaptic vesicle protein 2A, which isinvolved in synaptic vesicle function and calcium-dependentregulation of neurotransmitter release during repetitivestimulation [30,32-35]. In alcohol-dependent mice, levetirace-tam has been shown to reduce the alcohol withdrawalsyndrome [36]. Two open-label trials provided some evidencethat levetiracetam might also be safe and efficacious in thein- and outpatient treatment of alcohol withdrawalsyndrome [28,37], whereas one RCT failed to show superiorityof levetiracetam in the treatment of alcohol withdrawalsyndrome compared to placebo [38]. With regard to relapseprevention in alcohol-dependent patients, two RCTs havebeen conducted to date. In a multicenter, 16-week RCT,the efficacy and safety of levetiracetam have been investigatedin a sample of 201 recently detoxified alcohol-dependentpatients using target dosages of 2000 mg per day [39]. At studyend, no significant differences between the levetiracetam andthe placebo group were observed for the endpoints ‘rate ofsevere relapse’ (defined as any alcohol consumptionof > 60 g/day for men and > 48 g/day for women; 45 vs40%), ‘time to severe relapse’ (77.4 vs 76.4 days) and‘abstinence rate’ (35 vs 34%). The overall incidence of AEsdid not differ between the levetiracetam and the placebogroup (73 vs 71%); also, no differences in serious AEsbetween both groups were found (2 vs 3%). The study reten-tion rate was similar in the levetiracetam and the placebogroup (82 vs 75%). In a further multisite, 16-week RCT,levetiracetam XR (extended-release) has been evaluated in130 very heavy drinking alcohol-dependent patients (definedas 10 or more drinks/drinking day for men, 8 or moredrinks/drinking day for women at least 40% of the days dur-ing the last month) with a target dose of 2000 mg/day [40]. Nosignificant differences between the levetiracetam XR and theplacebo group were found in terms of percent of heavy-drinking days (LSMEAN 45.8 vs 41.2), percent of subjectswith no heavy-drinking days (14 vs 18%) or in other second-ary drinking outcomes. Except for fatigue (with a prevalencerate in the levetiracetam XR group of 53 vs 24% in theplacebo group), the number of AEs did not differ betweenboth groups. A total of 13 serious AEs occurred duringthe study period (3 in the levetiracetam XR group, 10 in theplacebo group). The study retention rate was similar in thelevetiracetam and the placebo group (78 vs 85%).
2.2.2 TopiramateThe anticonvulsant topiramate has been hypothesized toantagonize the rewarding effects of alcohol by inhibition ofmesolimbic dopamine release, mediated through the facilita-tion of GABAergic function via a non-benzodiazepine siteon the GABA-A receptor and antagonism of a-Amino-3-
hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) andkainate glutamate receptors [41-43]. In preclinical studies, top-iramate has been shown to suppress ethanol drinking and toreduce stress-induced increases in alcohol consumption inmice [44,45]. Until now, four RCTs have been conducted inpatients with alcohol dependence. In a first 12-week RCT[46], 150 patients received either topiramate in escalatingdosages of 25 -- 300 mg per day or placebo; both groupsalso received a standardized medication compliance manage-ment program. At study end, topiramate was significantlymore effective than placebo in improving several drinkingoutcomes: patients receiving topiramate had 2.9 fewer drinksper day, 3.1 fewer drinks per drinking day, 28% fewer heavy-drinking days and 26% more days abstinent in comparison topatients who received placebo. AEs that were reported morefrequently in the topiramate than in the placebo group weredizziness (28 vs 10%), paraesthesia (57 vs 19%), psychomotorslowing (27 vs 12%), memory or concentration impairment(19 vs 5%) and weight loss (55 vs 27%). The study comple-tion rate did not differ between both groups. No seriousAEs have been reported.
In a second, 14-week, multicenter RCT [47], topiramate hasbeen evaluated in 371 alcohol-dependent patients withdosages up to 300 mg per day. In this trial, topiramate wasmore effective in reducing the percentage of heavy-drinkingdays from baseline to week 14 than placebo (mean difference8.4%). Furthermore, topiramate significantly decreased thepercentage of heavy-drinking days compared to placebo(mean difference: 16.2%). AEs that occurred more frequentlyin the topiramate group were paraesthesia (51 vs 11%), tasteperversion (23 vs 5%), anorexia (20 vs 7%), difficulty withconcentration/attention (15 vs 3%) and pruritus (10 vs 1%).Four participants of both treatment groups experienced aserious adverse event. At study end, the retention rates inboth groups differed significantly (topiramate 61 vs placebo77%), and the attrition rates due to AEs were 19% for thetopiramate group and 4% for the placebo group.
In a third 12-week RCT, the efficacy and safety of topira-mate (target dose 300 mg/day) have been compared with nal-trexone (50 mg/day) and placebo in 155 alcohol-dependentpatients who had received a 1-week detoxification prior tothe initiation of the relapse prevention treatment [48]. Topira-mate was superior to placebo in terms of ‘time to first relapse’(7.8 vs 5.0 weeks), ‘cumulative abstinence duration’ (8.2 vs5.6 weeks) and ‘weeks of heavy drinking’ (3.4 vs 5.9). No sig-nificant differences between topiramate and naltrexone werefound. The overall incidence of AEs did not differ betweenthe groups, and no serious AEs were reported. Dropout rateswere significantly lower in the topiramate group compared toplacebo (36 vs 57%).
Rubio and colleagues conducted a fourth RCT using topir-amate for 12 weeks with a daily dose of 250 mg/day in asample of 76 alcohol-dependent patients [49]. Patients of thetopiramate group consumed fewer drinks per drinking day(6.5 vs 8.8), had a lower percentage of heavy-drinking days
Current pharmacological treatment approaches for alcohol dependence
Expert Opin. Pharmacother. (2014) 15(4) 475

(33 vs 51%) and a higher percentage of abstinent days (52 vs37%). No detailed information on occurrence of AEs or seri-ous AEs was given. Three patients of the topiramate groupand one patient of the placebo group withdrew because ofside effects.
2.2.3 GabapentinGabapentin, a non-benzodiazepine anticonvulsant GABAanalog, has been evaluated in two clinical trials in alcoholdependence. A 4-week RCT in 60 patients investigated thecompound using dosages of 300 mg twice per day [50]. Com-pared to placebo, patients receiving gabapentin showed a sig-nificant reduction in number of drinks per day and percentageof heavy-drinking days. Also, the percentage of abstinent dayswas significantly increased in this group. Side effects occurredin the form of insomnia, sleepiness and headache withno differences between the groups. No serious AEs werereported. The retention rate was higher in the gabapentingroup compared to placebo.In a recent 12-week RCT, gabapentin was administered in
150 alcohol-dependent patients with dosages of 900 and1800 mg per day, respectively [51]. Patients receiving gabapen-tin showed a significantly higher rate of abstinence in compar-ison to placebo (17% in the 1800 mg/day group vs 11% inthe 900 mg/day group vs 4% in the placebo group) with anNNT of 8 for 1800 mg/day. With regard to the co-primaryendpoint ‘no heavy drinking’ rate, gabapentin was also supe-rior compared to placebo (48% in the 1800 mg/day groupvs 30% in the 900 mg/day group vs 23% in the placebogroup; NNT = 5 for 1800 mg/day). Side effects such as head-ache, fatigue and insomnia were reported, but no significantdifferences between the treatment groups were found. Also,no serious drug-related AEs occurred during the study. Theretention rates were similar in all groups.
2.2.4 BaclofenBaclofen, a selective GABA-B receptor agonist, is approvedfor the treatment of spasticity resulting from various neuro-logical conditions [52]. In the past years, several lines of exper-imental evidence have demonstrated a role of GABA-Breceptors and baclofen in affecting different alcohol-relatedbehaviors in rodents. The GABA-B receptor is located withinthe mesolimbic reward system of the brain and has beenhypothesized to modulate dopaminergic neurotransmis-sion [53,54], which plays a crucial role in the development ofalcohol dependence [55]. In preclinical studies, baclofen wasfound to suppress acquisition and maintenance of alcohol-drinking behavior in rats [56,57], the increase in alcohol intakeafter a period of alcohol abstinence in rats [58], and oral self-administration of alcohol in rats and mice trained to lever-press for alcohol [59,60]. In alcohol-dependent patients, fourRCTs using baclofen have been published until now. In a firstclinical trial, 39 alcohol-dependent patients received 30 mg ofbaclofen per day or placebo for 4 weeks [61]. Compared toplacebo, there was a higher proportion of patients who
achieved and maintained alcohol abstinence during the studyin the baclofen group (70 vs 21%). Furthermore, the cumula-tive abstinence duration was significantly higher in the baclo-fen group (19.6 vs 6.3 days). The occurrence of AEs did notdiffer between both groups, and also, no serious AEs werereported. The study retention rate was similar in both groups.
A second RCT assessed the efficacy and safety of 30 mg ofbaclofen per day in 84 patients with alcohol dependence andcomorbid liver cirrhosis during a 12-week study period [62]. Inthis trial, a significantly higher number of patients achievedand maintained abstinence in the baclofen group in compari-son to the placebo group (71 vs 29%). The cumulative absti-nence duration was significantly higher in the group ofpatients who received baclofen (62.8 vs 30.8 days). Tolerabil-ity of the study medication was similar in both groups, and noserious AEs were reported. The study retention rate did notdiffer between the baclofen and the placebo groups.
A third RCT has been conducted in 80 alcohol-dependentpatients using 30 mg of baclofen per day or placebo for12 weeks [63]. With regard to the endpoints ‘percentage ofheavy-drinking days’ and ‘percentage abstinent days,’ no dif-ferences between the baclofen and the placebo group werefound (26 vs 26%; 50 vs 51%). The rates of reported AEsand the study completion rate did not differ between bothtreatment groups. No serious AEs occurred during the studyperiod.
In a fourth 12-week RCT, baclofen has been investigated in42 alcohol-dependent patients using target dosages of 30 and60 mg per day in comparison to placebo [64]. Regarding theendpoints ‘heavy-drinking days,’ ‘abstinent days,’ ‘time tofirst lapse’ and ‘time to first relapse,’ no significant differencesbetween the groups were found. In a secondary analysis,patients receiving 30 mg of baclofen per day had a 53%reduction in the number of drinks per day and patients receiv-ing 60 mg of baclofen had a 68% reduction in the number ofdrinks per day compared to placebo. Occurrence of AEs andstudy completion rates were similar in all treatment groups,and no serious AEs have been reported.
In line with a recent review of baclofen for the treatment ofsubstance use disorders [65], final conclusions regarding itsefficacy and safety for the treatment of alcohol dependencecan currently not be drawn due to the divergent results frompast RCTs.
2.2.5 VareniclineVarenicline is a partial agonist at the a4b2 nicotinic acetylcho-line receptor subtype and is approved for smoking cessation.Based on the positive results from preclinical studies [66] aswell as clinical trials in heavy-drinking smokers [67,68], vareni-cline has been evaluated in alcohol dependence in two RCTs.In a pilot study [69], 40 alcohol-dependent patients received2 mg/day of varenicline/placebo for a 13-week treatmentperiod. At study completion, no significant difference betweentreatment groups for the primary endpoint ‘alcohol use’ wasfound. With regard to nicotine consumption, a significantly
C. A. Muller et al.
476 Expert Opin. Pharmacother. (2014) 15(4)

lower rate of cigarette smoking was detected for the vareniclinegroup compared to placebo. Common side effects were head-ache, sleep disturbances, nausea and diarrhea, with nosignificant differences between the groups. No serious AEswere reported.
In a recent multicenter RCT, varenicline has been investi-gated in a sample of 200 alcohol-dependent patients [70].Patients received 2 mg/day of varenicline or placebo for13 weeks in combination with a computerized behavioralintervention. Compared to placebo, the varenicline grouphad lower weekly percent heavy-drinking days (adjustedmean diff.: 10.4), less drinks per day (4.4 vs 5.3) and drinksper drinking day (5.8 vs 6.8). Moreover, a lower number ofcigarettes smoked per day was found for the varenicline group(7.4 vs 11.7). Side effects like nausea, abnormal dreams andconstipation occurred with significantly higher rates in thevarenicline group compared to the placebo group. Fourserious AEs were reported (two in the varenicline, two in theplacebo group). The retention rates were similar in bothtreatment groups (88% varenicline vs 84% placebo).
2.2.6 PrazosinBased on the findings from preclinical studies showing that thea1 adrenergic antagonist prazosin reduces self-administrationof ethanol in rats [71], the substance has been evaluated in a6-week RCT in a small sample of 24 alcohol-dependentpatients using a target dose of 16 mg/day. [72]. Patients whoreceived prazosin reported fewer drinking days per week andfewer drinks per week during the final 3 weeks of the study.The average total number of drinking days was 0.9 for theprazosin group and 5.7 for the placebo group, and average totalnumber of drinks was 2.6 for the prazosin group and 20.8 forthe placebo group. Side effects were dizziness, lack of energyand drowsiness, with no differences between the groups. Noserious AEs occurred during the treatment period. The reten-tion rates were similar in both groups. Currently, severalRCTs investigate the efficacy and safety of prazosin in alcoholdependence with and without comorbid PTSD.
2.2.7 OndansetronThe selective 5-hydroxytryptamine 3 (5-HT3) receptor antago-nist ondansetron is an antiemetic drug that has been shown toreduce ethanol consumption in rodents [73]. In a first RCT,271 patients received ondansetron in dosages of 1, 4 or16 µg/kg twice per day for 11 weeks [74]. Compared to placebo,ondansetron decreased the number of drinks per day (1.9,1.6 and 1.9 vs 3.3) and drinks per drinking day (4.8, 4.3 and5.2 vs 6.9) in early-onset (< 25 years of age) but not in late-onset alcohol-dependent patients. Common side effects wereheadache, constipation, tachycardia and pruritus; no differen-ces between the treatment groups were observed, and also, noserious AEs were reported. The dropout rates did not differbetween the treatment groups.
A pharmacogenetic RCT investigated the efficacy of ondan-setron (4 µg/kg twice per day) versus placebo in 283 alcohol-
dependent patients over 11 weeks [75]. In this study, patientswere subgrouped based on their 5¢-HTTLPR and rs1042173genotypes in the serotonin transporter (5-HTT) geneSLC6A4. The authors reported that carriers of SLC6A4-LL/TT who were treated with ondansetron had fewer standarddrinks per drinking day (-2.6) and a percentage of daysabstinent 17% higher in comparison to noncarriers of thatgenotype. However, no significant effect of ondansetroncompared to placebo was found when patients were notsubgrouped according to these genotypes. With regard toside effects, only fatigue occurred more frequently in theondansetron group compared to placebo. Further side effectsincluded insomnia, headache, appetite disturbances and diar-rhea, with no significant differences between the groups. Nomedication-related serious AEs were reported. The retentionrate did not differ among the treatment groups.
A further analysis within the same trial found that also poly-morphisms of the HTR3A and HTR3B genes (which encodethe 5-HT3 receptor subunits A and B) predicted treatmentresponse to ondansetron [76]. For patients carrying one ormore of the genotypes rs1150226-AG and rs1176713-GG inHTR3A and rs17614942-AC in HTR3B, a mean differencein drinks per drinking day (2.5), percentage of heavy-drinkingdays (20.6%) and percentage of days abstinent (18.2%) forondansetron versus placebo was found.
A recent 12-week RCT assessed the efficacy and safety ofondansetron in 102 alcohol-dependent patients using dosagesof 16 mg/day [77]. No significant difference between the groupsregarding the percentage of abstinent days (76 placebo vs 89%ondansetron) was found. Also, there was no significant differ-ence regarding percentage of heavy-drinking days (10 placebovs 6% ondansetron). Side effects occurred in the form of head-ache, dyspepsia and constipation, with no differences betweenthe groups. No serious AEs were reported. The dropout ratesdid not differ significantly between the groups.
Table 1 shows the study characteristics and outcomesof RCTs investigating off-label medications in alcoholdependence.
3. Expert opinion
Based on the findings from two meta-analyses [6,7], theanti-craving substances acamprosate and naltrexone seem torepresent efficacious and safe treatment options for alcoholdependence, but the reported effect sizes are only moderate.
Although disulfiram has been evaluated in several clinicalstudies, no clear conclusions can currently be drawn due tomethodological limitations of these studies.
As a further treatment option, the opioid system modulatornalmefene has shown efficacy in several RCTs [22,24,25] andhas recently been approved by the EMA for the reduction ofalcohol consumption in alcohol-dependent patients. Thus,patients who are not able or willing to abstain from alcoholcan be included in treatment programs aimed to reduce
Current pharmacological treatment approaches for alcohol dependence
Expert Opin. Pharmacother. (2014) 15(4) 477

alcohol intake and dosing as needed, thereby offering a way toreduce harm in those patients.RCTs (single- and multisite) using levetiracetam with
dosages up to 2000 mg per day for the treatment of alcoholwithdrawal syndrome or for the prevention of alcohol relapsecould not show its efficacy in comparison to placebo [38-40].Thus, there is currently no good evidence for its use as anoff-label medication in the treatment of alcohol dependence.In contrast, topiramate has repeatedly been shown to be
effective in improving several drinking outcomes in fourwell-designed RCTs using dosages of up to 300 mg perday [46-49]. However, its widespread use in alcohol-dependentpatients might be limited by the reported, frequently occur-ring side effects such as weight loss and cognitive impair-ments. Another disadvantage of topiramate in a clinicalsetting might be the long titration phase (up to 8 weeks fora dose of 300 mg/day). On the other hand, an improvementof physical and psychosocial well-being in alcohol-dependentpatients receiving topiramate has been reported [78]. Takentogether, the off-label use of topiramate can be considered asevidence based, but its future role in the treatment of alcoholdependence needs to be determined.The anticonvulsant gabapentin has been evaluated posi-
tively in two independent RCTs using dosages up to1800 mg/day [50,51]. Both trials also reported a high tolerabilityof gabapentin in alcohol-dependent patients. Thus, this com-pound possibly represents a further pharmacological treatmentoption in alcohol dependence, but these findings have to bereplicated in future studies to draw final conclusions.With regard to baclofen, four RCTs have reported a high
tolerability in alcohol-dependent patients (also in patientswith comorbid liver cirrhosis [62] -- the EASL clinical practicalguidelines recommend its use in patients with advanced alco-holic liver disease [79]) but conflicting results in terms ofefficacy [61-64]. These inconsistent findings might possibly berelated to the rather low dosages of baclofen used in these tri-als (30 -- 60 mg/day). Based on the preclinical observations ofa dose-dependent effect of baclofen on alcohol consumption
in rats treated with dosages up to 3 mg/kg [80] as well as twocase reports in alcohol-dependent patients receiving high-dose baclofen with up to 270 mg/day [81,82], three ongoingRCTs investigate the efficacy and safety of high-dose baclofen(up to 300 mg/day) in alcohol-dependent patients (Cinical-trials.gov: NCT01266655; NCT01738282; NCT01604330).Since the evidence for baclofen in the treatment of alcoholdependence is low and its risk profile (high-dose baclofen)has not been extensively studied until now, the broadeneduse of baclofen can, currently, not be recommended.
Varenicline, a substance approved for smoking cessation,has shown mixed results in two recent RCTs in alcoholdependence [69,70]. If varenicline were to be found to be effec-tive in future trials, this approach might be a useful extensionof the currently available medications, given that nicotinedependence represents one of the most common comorbiditesin alcohol-dependent patients [83].
Prazosin has shown efficacy in a pilot trial within a smallsample of patients with alcohol dependence [72]. Currently,several clinical trials are ongoing to investigate its efficacy inpatients with and without comorbid PTSD.
The antiemetic drug ondansetron has been assessed in threeRCTs [74-77], showing efficacy in patients with early-onsetalcohol dependence in one trial [74] and in two pharmacoge-netic studies within one trial, when patients were subgroupedaccording to their genotypes of the serotonin transporter(5-HTT) gene and the 5-HT3 receptor subunits A and B genes[75,76]. Without subgrouping, no differences between the treat-ment groups were found. A further trial investigating ondanse-tron in alcohol dependence reported negative results [77]. Thus,first clinical evidence suggests that ondansetron might be afurther pharmacological strategy for alcohol dependencewhen used within a pharmacogenetic treatment approach.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of this manuscript.
C. A. Muller et al.
478 Expert Opin. Pharmacother. (2014) 15(4)
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. de Wit M, Jones DG, Sessler CN, et al.
Alcohol-use disorders in the critically ill
patient. Chest 2010;138(4):994-1003
2. Boothby LA, Doering PL. Acamprosate
for the treatment of alcohol dependence.
Clin Ther 2005;27(6):695-714
3. Litten RZ, Egli M, Heilig M, et al.
Medications development to treat alcohol
dependence: a vision for the next decade.
Addict Biol 2012;17(3):513-27
4. Mann K, Kiefer F, Spanagel R, Littleton J.
Acamprosate: recent findings and future
research directions. Alcohol Clin Exp Res
2008;32(7):1105-10
5. Spanagel R, Vengeliene V, Jandeleit B,
et al. Acamprosate produces its
anti-elapse effects via calcium.
Neuropsychopharmacology
2013; doi: 10.1038/npp.2013.264.
[Epub ahead of print]
. An interesting study on the mechanism
of action of acamprosate suggesting
that calcium is the active component
of acamprosate.
6. Rosner S, Hackl-Herrwerth A, Leucht S,
et al. Acamprosate for alcohol
dependence. Cochrane Database Syst Rev
2010(9):CD004332
7. Rosner S, Hackl-Herrwerth A, Leucht S,
et al. Opioid antagonists for alcohol
dependence. Cochrane Database Syst Rev
2010(12):CD001867
8. Anton RF, O’Malley SS, Ciraulo DA,
et al. Combined pharmacotherapies and
behavioral interventions for alcohol
dependence: the COMBINE study:
a randomized controlled trial. JAMA
2006;295(17):2003-17
.. This large multi-center trial assessed
the efficacy of pharmacological and
behavioural interventions as well as
their combinations.
9. Mann K, Lemenager T, Hoffmann S,
et al. Results of a double-blind,
placebo-controlled pharmacotherapy trial
in alcoholism conducted in Germany and
comparison with the US COMBINE
study. Addict Biol 2013;18(6):937-46
10. Suh JJ, Pettinati HM, Kampman KM,
O’Brien CP. The status of disulfiram:
a half of a century later.
J Clin Psychopharmacol
2006;26(3):290-302
. A comprehensive review of disulfiram
for the treatment of addictive diseases.
11. Jorgensen CH, Pedersen B, Tonnesen H.
The efficacy of disulfiram for the
treatment of alcohol use disorder.
Alcohol Clin Exp Res
2011;35(10):1749-58
12. Niederhofer H, Staffen W. Comparison
of disulfiram and placebo in treatment of
alcohol dependence of adolescents.
Drug Alcohol Rev 2003;22(3):295-7
13. Fuller RK, Roth HP. Disulfiram for the
treatment of alcoholism. An evaluation in
128 men. Ann Intern Med
1979;90(6):901-4
14. Fuller RK, Branchey L, Brightwell DR,
et al. Disulfiram treatment of alcoholism.
A Veterans Administration cooperative
study. JAMA 1986;256(11):1449-55
15. Pani PP, Trogu E, Vacca R, et al.
Disulfiram for the treatment of cocaine
dependence. Cochrane Database Syst Rev
2010(1):CD007024
16. Vaccari A, Saba PL, Ruiu S, et al.
Disulfiram and diethyldithiocarbamate
intoxication affects the storage and
release of striatal dopamine.
Toxicol Appl Pharmacol
1996;139(1):102-8
17. Muller CA, Banas R. Disulfiram:
an anticraving substance? Am J Psychiatry
2011;168(1):98; author reply -9
18. Weinshenker D. Cocaine sobers up.
Nat Med 2010;16(9):969-70
. This article discusses the possible
mechanism(s) of action of disulfiram
in the treatment of cocaine dependence
focusing on its ability to inhibit
dopamine b-hydroxylase (DBH).
19. Bart G, Schluger JH, Borg L, et al.
Nalmefene induced elevation in serum
prolactin in normal human volunteers:
partial kappa opioid agonist activity?
Neuropsychopharmacology
2005;30(12):2254-62
20. Mason BJ, Ritvo EC, Morgan RO, et al.
A double-blind, placebo-controlled pilot
study to evaluate the efficacy and safety
of oral nalmefene HCl for alcohol
dependence. Alcohol Clin Exp Res
1994;18(5):1162-7
21. Mason BJ, Salvato FR, Williams LD,
et al. A double-blind, placebo-controlled
study of oral nalmefene for alcohol
dependence. Arch Gen Psychiatry
1999;56(8):719-24
22. Karhuvaara S, Simojoki K, Virta A, et al.
Targeted nalmefene with simple medical
management in the treatment of heavy
drinkers: a randomized double-blind
placebo-controlled multicenter study.
Alcohol Clin Exp Res 2007;31(7):1179-87
23. Anton RF, Pettinati H, Zweben A, et al.
A multi-site dose ranging study of
nalmefene in the treatment of alcohol
dependence. J Clin Psychopharmacol
2004;24(4):421-8
24. Mann K, Bladstrom A, Torup L, et al.
Extending the treatment options in
alcohol dependence: a randomized
controlled study of as-needed nalmefene.
Biol Psychiatry 2013;73(8):706-13
25. Gual A, He Y, Torup L, et al.
A randomised, double-blind,
placebo-controlled, efficacy study of
nalmefene, as-needed use, in patients
with alcohol dependence.
Eur Neuropsychopharmacol
2013;23(11):1432-42
26. European Medicines Agency (EMA).
2013. Available from: http://www.ema.
europa.eu/ema/index.jsp?curl=pages/
medicines/human/medicines/002583/
human_med_001620.jsp&mid=WC0b01
ac058001d124 [Accessed 18 September
2013]
27. Bennett B, Lamberty Y, Bizot JC, et al.
Levetiracetam prevents signs of alcohol
withdrawal in mice [abstract NR689].
New Research Program and Abstracts of
the 156th Annual Meeting of the
American Psychiatric Association;
21 May 2003; San Francisco;
2003. p. 58
28. Muller CA, Schafer M, Schneider S,
et al. Efficacy and safety of levetiracetam
for outpatient alcohol detoxification.
Pharmacopsychiatry 2010;43(5):184-9
29. Gower AJ, Noyer M, Verloes R, et al.
ucb L059, a novel anti-convulsant drug:
pharmacological profile in animals.
Eur J Pharmacol 1992;222(2-3):193-203
30. Noyer M, Gillard M, Matagne A, et al.
The novel antiepileptic drug
levetiracetam (ucb L059) appears to act
via a specific binding site in CNS
membranes. Eur J Pharmacol
1995;286(2):137-46
31. Margineanu DG, Klitgaard H.
Levetiracetam has no significant
Current pharmacological treatment approaches for alcohol dependence
Expert Opin. Pharmacother. (2014) 15(4) 479

gamma-aminobutyric acid-related effect
on paired-pulse interaction in the dentate
gyrus of rats. Eur J Pharmacol
2003;466(3):255-61
32. Fuks B, Gillard M, Michel P, et al.
Localization and photoaffinity labelling
of the levetiracetam binding site in rat
brain and certain cell lines.
Eur J Pharmacol 2003;478(1):11-19
33. Lynch BA, Lambeng N, Nocka K, et al.
The synaptic vesicle protein SV2A is the
binding site for the antiepileptic drug
levetiracetam. Proc Natl Acad Sci USA
2004;101(26):9861-6
34. Gillard M, Chatelain P, Fuks B. Binding
characteristics of levetiracetam to synaptic
vesicle protein 2A (SV2A) in human
brain and in CHO cells expressing the
human recombinant protein.
Eur J Pharmacol 2006;536(1-2):102-8
35. Stahl SM. Psychopharmacology of
anticonvulsants: levetiracetam as a
synaptic vesicle protein modulator.
J Clin Psychiatry 2004;65(9):1162-3
36. Bennett B, Lamberty Y, Bizot JC, et al.
Levetiracetam prevents signs of alcohol
withdrawal in mice [abstract NR689].
New Research Program and Abstracts of
the 156th Annual Meeting of the
American Psychiatric Association;
21 May 2003; San Francisco;
2003. p. 58
37. Krebs M, Leopold K, Richter C, et al.
Levetiracetam for the treatment of
alcohol withdrawal syndrome:
an open-label pilot trial.
J Clin Psychopharmacol
2006;26(3):347-9
38. Richter C, Hinzpeter A, Schmidt F,
et al. Levetiracetam for the treatment of
alcohol withdrawal syndrome:
a multicenter, prospective, randomized,
placebo-controlled trial.
J Clin Psychopharmacol
2010;30(6):720-5
39. Richter C, Effenberger S, Bschor T, et al.
Efficacy and safety of levetiracetam for
the prevention of alcohol relapse in
recently detoxified alcohol-dependent
patients: a randomized trial.
J Clin Psychopharmacol
2012;32(4):558-62
40. Fertig JB, Ryan ML, Falk DE, et al.
A double-blind, placebo-controlled trial
assessing the efficacy of levetiracetam
extended-release in very heavy drinking
alcohol-dependent patients. Alcohol Clin
Exp Res 2012;36(8):1421-30
41. Johnson BA. Recent advances in the
development of treatments for alcohol
and cocaine dependence: focus on
topiramate and other modulators of
GABA or glutamate function.
CNS Drugs 2005;19(10):873-96
42. White HS, Brown SD, Woodhead JH,
et al. Topiramate modulates
GABA-evoked currents in murine cortical
neurons by a nonbenzodiazepine
mechanism. Epilepsia
2000;41(Suppl 1):S17-20
43. Moghaddam B, Bolinao ML.
Glutamatergic antagonists attenuate
ability of dopamine uptake blockers to
increase extracellular levels of dopamine:
implications for tonic influence of
glutamate on dopamine release. Synapse
1994;18(4):337-42
44. Farook JM, Lewis B, Littleton JM,
Barron S. Topiramate attenuates the
stress-induced increase in alcohol
consumption and preference in male
C57BL/6J mice. Physiol Behav
2009;96(1):189-93
45. Nguyen SA, Malcolm R, Middaugh LD.
Topiramate reduces ethanol consumption
by C57BL/6 mice. Synapse
2007;61(3):150-6
46. Johnson BA, Ait-Daoud N, Bowden CL,
et al. Oral topiramate for treatment of
alcohol dependence: a randomised
controlled trial. Lancet
2003;361(9370):1677-85
47. Johnson BA, Rosenthal N, Capece JA,
et al. Topiramate for treating alcohol
dependence: a randomized controlled
trial. JAMA 2007;298(14):1641-51
48. Baltieri DA, Daro FR, Ribeiro PL,
de Andrade AG. Comparing topiramate
with naltrexone in the treatment of
alcohol dependence. Addiction
2008;103(12):2035-44
49. Rubio G, Martinez-Gras I, Manzanares J.
Modulation of impulsivity by topiramate:
implications for the treatment of alcohol
dependence. J Clin Psychopharmacol
2009;29(6):584-9
50. Furieri FA, Nakamura-Palacios EM.
Gabapentin reduces alcohol consumption
and craving: a randomized, double-blind,
placebo-controlled trial. J Clin Psychiatry
2007;68(11):1691-700
51. Mason BJ, Quello S, Goodell V, et al.
Gabapentin treatment for alcohol
dependence: a randomized clinical trial.
JAMA Intern Med
2013. doi: 10.1001/
jamainternmed.2013.11950. [Epub ahead
of print]
52. Davidoff RA. Antispasticity drugs:
mechanisms of action. Ann Neurol
1985;17(2):107-16
53. Bowery NG, Hudson AL, Price GW.
GABAA and GABAB receptor site
distribution in the rat central nervous
system. Neuroscience 1987;20(2):365-83
54. Fadda P, Scherma M, Fresu A, et al.
Baclofen antagonizes nicotine-, cocaine-,
and morphine-induced dopamine release
in the nucleus accumbens of rat. Synapse
2003;50(1):1-6
55. Heinz A. Dopaminergic dysfunction in
alcoholism and schizophrenia--
psychopathological and behavioral
correlates. Eur Psychiatry
2002;17(1):9-16
56. Colombo G, Serra S, Brunetti G, et al.
The GABA(B) receptor agonists baclofen
and CGP 44532 prevent acquisition of
alcohol drinking behaviour in alcohol-
preferring rats. Alcohol Alcohol
2002;37(5):499-503
57. Daoust M, Saligaut C, Lhuintre JP, et al.
GABA transmission, but not
benzodiazepine receptor stimulation,
modulates ethanol intake by rats. Alcohol
1987;4(6):469-72
58. Colombo G, Serra S, Brunetti G, et al.
Suppression by baclofen of alcohol
deprivation effect in Sardinian alcohol-
preferring (sP) rats. Drug Alcohol
Depend 2003;70(1):105-8
59. Anstrom KK, Cromwell HC,
Markowski T, Woodward DJ. Effect of
baclofen on alcohol and sucrose
self-administration in rats. Alcohol Clin
Exp Res 2003;27(6):900-8
60. Besheer J, Lepoutre V, Hodge CW.
GABA(B) receptor agonists reduce
operant ethanol self-administration and
enhance ethanol sedation in C57BL/6J
mice. Psychopharmacology (Berl)
2004;174(3):358-66
61. Addolorato G, Caputo F, Capristo E,
et al. Baclofen efficacy in reducing
alcohol craving and intake: a preliminary
double-blind randomized controlled
study. Alcohol Alcohol 2002;37(5):504-8
62. Addolorato G, Leggio L, Ferrulli A, et al.
Effectiveness and safety of baclofen for
maintenance of alcohol abstinence in
alcohol-dependent patients with liver
cirrhosis: randomised, double-blind
C. A. Muller et al.
480 Expert Opin. Pharmacother. (2014) 15(4)
controlled study. Lancet
2007;370(9603):1915-22
. The first RCT using low-dose baclofen
in a sample of alcohol-dependent
patients with comorbid liver cirrhosis.
63. Garbutt JC, Kampov-Polevoy AB,
Gallop R, et al. Efficacy and safety of
baclofen for alcohol dependence:
a randomized, double-blind, placebo-
controlled trial. Alcohol Clin Exp Res
2010;34(11):1849-57
64. Addolorato G, Leggio L, Ferrulli A, et al.
Dose-response effect of baclofen in
reducing daily alcohol intake in alcohol
dependence: secondary analysis of a
randomized, double-blind, placebo-
controlled trial. Alcohol Alcohol
2011;46(3):312-17
65. Agabio R, Preti A, Gessa GL. Efficacy
and tolerability of baclofen in substance
use disorders: a systematic review.
Eur Addict Res 2013;19(6):325-45
66. Ericson M, Lof E, Stomberg R,
Soderpalm B. The smoking cessation
medication varenicline attenuates alcohol
and nicotine interactions in the rat
mesolimbic dopamine system.
J Pharmacol Exp Ther
2009;329(1):225-30
67. Mitchell JM, Teague CH, Kayser AS,
et al. Varenicline decreases alcohol
consumption in heavy-drinking smokers.
Psychopharmacology (Berl)
2012;223(3):299-306
68. Fucito LM, Toll BA, Wu R, et al.
A preliminary investigation of varenicline
for heavy drinking smokers.
Psychopharmacology (Berl)
2011;215(4):655-63
69. Plebani JG, Lynch KG, Rennert L, et al.
Results from a pilot clinical trial of
varenicline for the treatment of alcohol
dependence. Drug Alcohol Depend
2013;133(2):754-8
70. Litten RZ, Ryan ML, Fertig JB, et al.
A double-blind, placebo-controlled trial
assessing the efficacy of varenicline
tartrate for alcohol dependence.
J Addict Med 2013;7(4):277-86
71. Rasmussen DD, Alexander LL,
Raskind MA, Froehlich JC. The
alpha1-adrenergic receptor antagonist,
prazosin, reduces alcohol drinking in
alcohol-preferring (P) rats. Alcohol Clin
Exp Res 2009;33(2):264-72
72. Simpson TL, Saxon AJ, Meredith CW,
et al. A pilot trial of the alpha-1
adrenergic antagonist, prazosin, for
alcohol dependence. Alcohol Clin
Exp Res 2009;33(2):255-63
73. Tomkins DM, Le AD, Sellers EM. Effect
of the 5-HT3 antagonist ondansetron on
voluntary ethanol intake in rats and mice
maintained on a limited access
procedure. Psychopharmacology (Berl)
1995;117(4):479-85
74. Johnson BA, Roache JD, Javors MA,
et al. Ondansetron for reduction of
drinking among biologically predisposed
alcoholic patients: a randomized
controlled trial. JAMA
2000;284(8):963-71
75. Johnson BA, Ait-Daoud N,
Seneviratne C, et al. Pharmacogenetic
approach at the serotonin transporter
gene as a method of reducing the severity
of alcohol drinking. Am J Psychiatry
2011;168(3):265-75
. This study shows the efficacy of
ondansetron within a pharmacogenetic
treatment approach.
76. Johnson BA, Seneviratne C, Wang XQ,
et al. Determination of genotype
combinations that can predict the
outcome of the treatment of alcohol
dependence using the 5-HT(3)
antagonist ondansetron. Am J Psychiatry
2013;170(9):1020-31
77. Correa Filho JM, Baltieri DA. A pilot
study of full-dose ondansetron to treat
heavy-drinking men withdrawing from
alcohol in Brazil. Addict Behav
2013;38(4):2044-51
78. Johnson BA, Rosenthal N, Capece JA,
et al. Improvement of physical health
and quality of life of alcohol-dependent
individuals with topiramate treatment:
US multisite randomized controlled trial.
Arch Intern Med 2008;168(11):1188-99
79. European Association for the Study of
Liver. EASL clinical practical guidelines:
management of alcoholic liver disease.
J Hepatol 2012;57(2):399-420
80. Colombo G, Vacca G, Serra S, et al.
Baclofen suppresses motivation to
consume alcohol in rats.
Psychopharmacology (Berl)
2003;167(3):221-4
81. Ameisen O. Complete and prolonged
suppression of symptoms and
consequences of alcohol-dependence
using high-dose baclofen: a self-case
report of a physician. Alcohol Alcohol
2005;40(2):147-50
82. Bucknam W. Suppression of symptoms
of alcohol dependence and craving using
high-dose baclofen. Alcohol Alcohol
2007;42(2):158-60
83. Miller NS, Gold MS. Comorbid
cigarette and alcohol addiction:
epidemiology and treatment.
J Addict Dis 1998;17(1):55-66
AffiliationChristian A Muller† MD, Olga Geisel MD,
Roman Banas & Andreas Heinz MD†Author for correspondence
Charite -- Universitatsmedizin Berlin,
Department of Psychiatry, Campus Charite
Mitte, Chariteplatz 1, 10117 Berlin, Germany
E-mail: [email protected]
Current pharmacological treatment approaches for alcohol dependence
Expert Opin. Pharmacother. (2014) 15(4) 481