payment plans for chiropractic and...
TRANSCRIPT

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
Payment Plans for Chiropractic and Massage To All New Patients: Please initial next to your method of payment _____ Cash/Private Pay Patient: To receive our discounted rate, payment is required at the time services are rendered. If payment is not made at the time of service, you will be charged our full rate, which is currently $71. We accept Visa, MasterCard, Discover Card and personal checks. _____ Insurance Patient: You need to provide our office with your insurance information. We do not verify benefits; it is your responsibility to call your insurance company to verify that they will cover our doctors & X-rays. You should also know if you have a deductible & the amount of your co‐pay, if any. We will bill your insurance as a courtesy to you, with the understanding that you are ultimately responsible for your account in our office. All co‐pays are expected at the time of service. If you do not know what your copay is, you will be required to pay $25 per visit until the correct amount of your copay has been determined. _____ Personal Injury Patient: It is your responsibility to provide our office with any and all insurance information; including PIP, third party, health insurance, etc. We need all claim numbers and insured person’s name, address, and phone numbers. You are responsible for payment to our office for any services rendered. _____ Labor & Industries Patient: You are responsible for filling out Labor & Industries long form or the form for self‐insured L&I. You are also to have an accident report filed with your employer. If your claim is not accepted, you will be responsible for your account balance. _____ ***I understand that any missed massage appointments without 24 hour notice, or arriving more than 15 minutes late will incur a $30 fee*** ________________________________________________________________ Patient Signature Date

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
�Terms of Acceptance When a patient seeks chiropractic health care and we accept a patient for such care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is important that each patient understand both the objective and the method that will be used to attain it. This will prevent any confusion or disappointment. Adjustment: An adjustment is the specific application of forces to facilitate the body's correction of vertebral subluxation. Our chiropractic method of correction is by specific adjustment of the spine. Health: A state of optimal physical, mental and social well‐being, not merely the absence of disease or infirmity. Vertebral Subluxation: A misalignment of one or more of the 24 vertebrae in the spinal column which causes alteration of nerve function and interference to the transmission of mental impulses, resulting in a lessening of the body's innate ability to express its maximum health potential. We do not offer to diagnose or treat any disease or condition other than vertebral subluxation. However, if during the course of a chiropractic spinal examination, we encounter non‐chiropractic or unusual findings, we will advise you. If you desire advice, diagnosis or treatment for those findings, we will recommend that you seek the services of a health care provider who specializes in that area. Regardless of what the disease is called, we do not offer to treat it. Nor do we offer advice regarding treatment prescribed by others. OUR ONLY PRACTICE OBJECTIVE is to eliminate a major interference to the expression of the body's innate wisdom. Our only method is specific adjusting to correct vertebral subluxation. I, ________________________________________, have read and fully understand the above statements. All questions regarding the doctors' objective pertaining to my care in this office have been answered to my complete satisfaction. I therefore, accept chiropractic care on this basis.

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
Pregnancy Release This is to certify that to the best of my knowledge I am not pregnant and the above doctors at Rody Chiropractic and their associates have my permission to perform an x‐ray evaluation. I have been advised that x‐ray can be hazardous to an unborn child. Date of Last Menstrual Period: __________________ � ________________________________________________________________ Patient Signature Date
Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
Notice of Privacy Practices We are committed to preserving the privacy of your personal health information. In fact, we are required by law to protect the privacy of your medical information and to provide you with notice describing: HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN ACCESS THIS INFORMATION. We may require your written consent before we use or disclose to others your medical information for purposes of providing or arranging for your health care, the payment or reimbursement of the care that we provide to you, and the related administrative activities supporting your treatment. We may be required or permitted by certain laws to use and disclose your medical information for other purposes without your consent or authorization. As our patient, you have important rights relating to inspecting and copying your medical information that we maintain, amending or correcting that information, obtaining an accounting of our disclosures of your medical information, requesting that we communicate with you confidentially, requesting that we restrict certain uses and disclosures of your health information, and complaining if you think your rights have been violated. We have available a detailed Notice of Privacy Practice which fully explains your rights and our obligations under the law. We may revise our Notice from time to time. The effective date at the top right hand side of this page indicates the date of the most current Notice in effect. You have the right to receive a copy of our most current Notice in effect. If you have not yet received a copy of our current Notice, please ask at the front desk and we will provide you with a copy. If you have any questions, concerns or complaints about the Notice or your medical information, please contact Patty Ann at our office (253) 535‐6006 x306. ________________________________________________________________ Patient Signature Date

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
FINANCIAL AGREEMENT We are committed to providing you with the best possible care. If you have medical insurance, we are anxious to help you receive your maximum allowable benefits. In order to achieve these goals, we need your assistance and your understanding of our payment policy. Payment for services is due at the time of your visit unless payment arrangements have been made in advance with our staff. We accept checks, MasterCard or Visa. We will be happy to process your insurance claim. Returned checks and balances older than 30 days may be subject to additional collection fees and interest charges of 1% per month. We will gladly discuss your proposed treatment and answer any questions relating to your insurance. You must realize, however, that:
1. Your insurance is a contract between you, your employer, and the insurance company. We are not a party to that contract.
2. Our fees are generally considered to fall within the acceptable range by most companies, and therefore are covered up to the maximum allowance determined by each carrier. This applies only to companies who pay a percentage (such as 50% or 80%) of UCR. UCR is defined as usual, customary and reasonably fees for this region.
3. Not all services are a covered benefit in all contracts. Some insurance companies arbitrarily select certain services they will not cover.
We must emphasize that as chiropractic care providers, our relationship is with you, not your insurance company. While filing of insurance claims is a courtesy that we extend to our patients, all charges are your responsibility from the date the services are rendered. We realize that temporary financial problems may affect timely payment of your account. If such problems do arise, we encourage you to contact us promptly for assistance in the management of your account. No show or cancellation policy for massage: Same day cancellation or no show will be charged $30.00. Sorry, no exceptions! If you have any questions about the above information or any uncertainty regarding insurance coverage, PLEASE don't hesitate to ask us. We are here to help you. ________________________________________________________________ Patient Signature Date
Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
Patient-Doctor Agreement The purpose of this agreement is to allow us to serve you more completely and to get the best treatment results in the shortest amount of time. It is our experience that those patients who adhere to the following agreement get the best results. SIGNING IN: When you arrive at our clinic, we ask that you sign in on our sheet. Please print your name. Patients will be called and assigned a treatment room in the order they arrive for their scheduled appointments. If you are late for your appointment (more than 15 minutes) or are not scheduled at that time, you will need to wait until we have an opening. When you go to the assigned treatment room, it is recommended that you lie down and relax on the adjusting table. APPOINTMENTS: We have set up a specific course of treatment for you care. A certain number of treatments in a set amount of time is required for us to achieve the results we both desire. If you need to change your appointment, we ask that you give us 24‐hour notice and that you make another appointment in one week or less. If you have an emergency and cannot give us 24‐hour notice, you may leave a voice message. While we allow walk‐in patients, an appointment is preferred. Patients who choose to walk‐in without an appointment will be placed in order behind those with a scheduled appointment and assigned a room as time permits. NO SHOW OR CANCELLATION FOR MASSAGE: Same day cancellation, more than 15 minutes late, or no show will be charged $30.00. Sorry, no exceptions! UPSETS AND CONCERNS: We are here to serve you. Please speak to your Doctor about any upsetting matters (long waits, staff insensitivity, etc.) We seek your comments to help us serve you and others better. ________________________________________________________________ Patient Signature Date

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
�Release of Information & Assignment of Benefits PLEASE READ & SIGN THE FOLLOWING I understand that health and accidental insurance policies are an arrangement between the insurance company and myself; that this office will prepare any necessary reports and forms to assist me in making collection from my insurance company; and that any amount authorized to be paid for given services is to be paid directly to the doctor's office and will be credited to my account upon receipt. However, I clearly understand and agree that all services rendered to me are charged directly to me and that I am personally responsible for payment. I also understand that should I suspend or terminate my care or treatment, any and all fees for professional services rendered to me will be immediately due and payable within 30 days. I also agree that any unpaid balance after 60 days will be charged a 1% fee per month or 12% per year interest. I further agree that if it becomes necessary to send my account to collections, I will pay all attorney, court and collection fees, including a collection fee of $30.00. I am also aware that there will be a $25.00 service charge for any returned checks. I hereby authorize the Doctor to treat my condition through the use of manipulation throughout my spine. It is understood and agreed the amount paid the Doctor, for X‐rays is for examination only and the x‐ray negatives will remain the property of this office, being on file where they may be seen at any time while a patient of this office. ________________________________________________________________ Patient Signature Date

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
�Insurance Coverage Questions PLEASE COMPLETE & RETURN Name of Patient________________________________ Date of Birth____________ Name of insurance representative_________________________________________
1. Coverage of Chiropractic Services �_____Number of visits per year: _____Chiropractic X‐Ray Coverage: _____% of Regular Office Call Covered: _____Co‐Pay? _____How much is my deductible? _____Has my deductible been met this year? _____Effective date of policy: A $25 COPAY IS REQUIRED AT EACH VISIT UNTIL THIS COMPLETED FORM IS RETURNED.
2. Massage Therapy Coverage _____Number of massages allowed per year: _____Length of time allowed for massage (30 min, 60 min etc) _____Co‐Pay? _____Referral required? (from Chiropractor or MD?)
Is your massage covered by a: Licensed Massage Practitioner | Chiropractor | Physical Therapist (Please circle all covered practitioners)
Names of massage therapists covered under my plan: _____Mel Ruchalski _____Sabrina Laville _____Joe Warness _____Haley Tracey _____Maren Kreun ________________________________________________________________ Patient Signature Date

Gordon M. Rody, D.C., B.C.A.O., D.A.C.S. Amy J. Rody, D.C., B.C.A.O., B.S. Jon A. Getbehead, D.C., B.C.A.O.
Rody Chiropractic 10614 Canyon Road East Puyallup, Washington 98373
Phone: 253-535‐6006 | Fax: 253-535‐6226 | rody‐chiropractic.com �
Clinical Quality Measure ________________________________________________________________ Patient Name Date Are you currently on any medications? Yes or No If so, please list them: ________________________________________________________________ ________________________________________________________________ ________________________________________________________________ Do you have any drug allergies? Yes or No If yes, please list them: ________________________________________________________________ ________________________________________________________________ ________________________________________________________________ Are you a smoker? Yes or No If yes, how often do you smoke? ___________
For women 40-69 years only Date of last mammogram ___________ (List only if within 2 years)
For patients 50-75 years only Date of last Colonoscopy ___________ (List only if in the last 10 years) Date of last Flexible Sigmoidoscopy ___________ (List only if in the last 5 years) Have you been diagnosed with Colorectal Cancer? Yes or No
For patients 50 years of age and over Have you had an Influenza Vaccine during flu season (Sept‐Feb)? Yes or No
For patients 64 years of age and over Have you ever had a Pneumonia Vaccine? Yes or No

CHIROPRACTICHEALTH QUESTIONNAIRE
Symptoms related to the Autonomic Nervous SystemChiropractic deals with the relationship
between your spine and nervous system
The Nervous System's function is to control and co-ordinate all the
other organs and structures. Pinched or irritated nerves may
interfere with this function and thus cause a wide variety of
symptoms.
Pain Pain Pain Pain
Stiff Stiff
Noise Noise Stiff Stiff
LEFT RIGHT
LEFT RIGHT
Pain Pain
Stiff Stiff Pain Pain
Noise Noise
Stiff Stiff
FORWARD BACK
(FLEXION) (EXTENSION) LEFT RIGHT
Pain Pain Pain Pain
Stiff Stiff Stiff Stiff
Noise Noise Noise Noise
LEFT RIGHT
BEND BACK BEND FORWARD
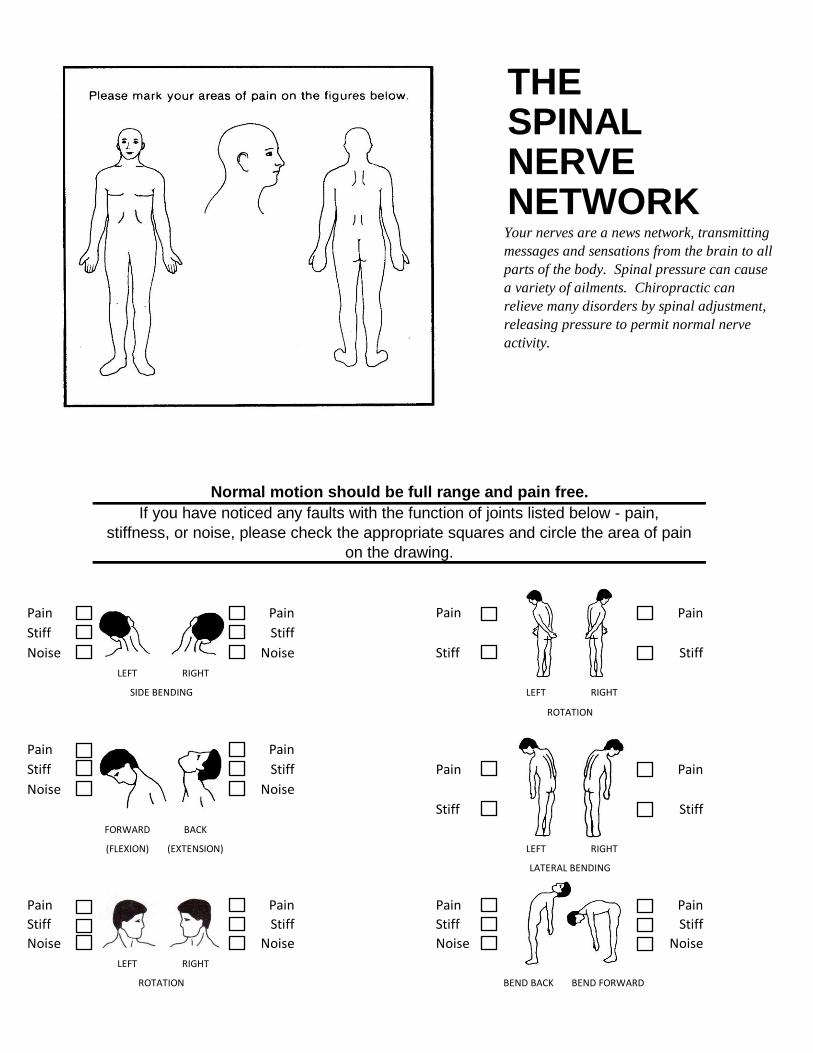
Normal motion should be full range and pain free.
If you have noticed any faults with the function of joints listed below - pain,
stiffness, or noise, please check the appropriate squares and circle the area of pain
on the drawing.
THESPINALNERVE
ROTATION
LATERAL BENDING
ROTATION
Your nerves are a news network, transmitting
messages and sensations from the brain to all
parts of the body. Spinal pressure can cause
a variety of ailments. Chiropractic can
relieve many disorders by spinal adjustment,
releasing pressure to permit normal nerve
activity.
NETWORK
SIDE BENDING

Pas
t
Pre
sen
t
No
Scalp Disorders
Head Pain or Headaches
Neck Pain
Tennis Elbow
Loss of Arm Power Auto Other
Loss of Grip Have you had any previous treatment for this or similar
Yes No When?
Mid Back Pain
Mid Back Tension
Pain in Ribs Yes No
Low Back Pain List all previous accidents or injuries:
List any operations:
Tingling, Numbness,
Yes No
Yes No
period: (month & day)
Is there any possibility that you might be pregnant?
Please enter date of the first day of your last menstrual
Leg Cramps
Describe:
Knee Trouble
Foot Trouble
Name:
Main complaint & its symptoms:
When did you first notice this problem?
working?
Treated for how long?
Who treated you?
Results?
Who treated you?
List any major illnesses:
For what:
Was your condition caused by:
Hip Pain or Stiffness
Buttock Pain
Symptoms that can be related to Spinal Nerves
Arm Pain/Tingling
or Numbness
Shoulder Pain or
Stiffness
Tingling, Numbness,
or Pain of Leg
Tingling, Numbness,
or Pain of Hand
Low Back Weakness
Low Back Stiffness
or Pain of Foot
On the Job Injury
conditions?
Have you had previous chiropractic care?
How does this condition interfere with normal living or
Are you currently under any doctor's care? (Who & why):
Are you currently taking any medication?
M.I.
Apt/Lot # City State Zip Code
City State Zip Code
Birth Date Age Sex
Mo Day Year ( ) M F
Employer
City State Zip Code
City State Zip Code
Employer City State
City State
Referred to this office by
Last Name M.I.
City State Zip Code
Employer Work Phone #
Subscriber Spouse
Address Phone Number
ID#
Address
ID#
Date:
Cash Check
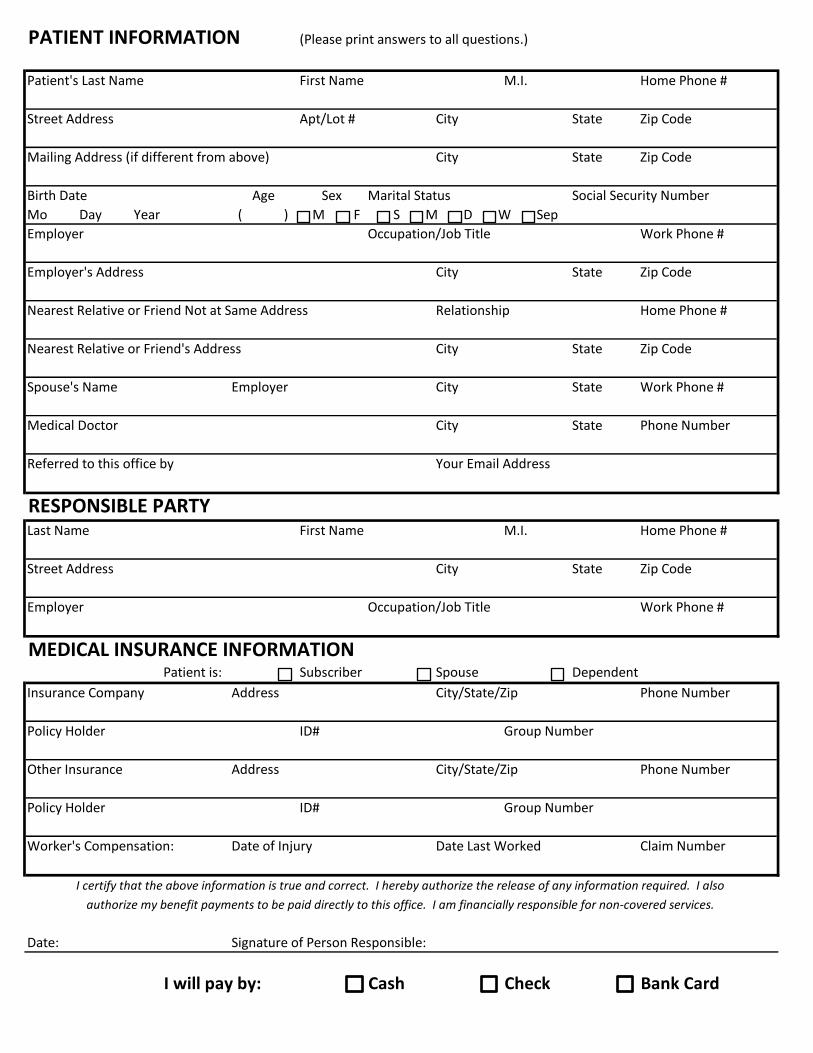
PATIENT INFORMATION (Please print answers to all questions.)
Patient's Last Name First Name Home Phone #
Street Address
Mailing Address (if different from above)
Social Security NumberMarital Status
S M D W Sep
Occupation/Job Title
Employer's Address
Nearest Relative or Friend Not at Same Address Relationship Home Phone #
Work Phone #
Nearest Relative or Friend's Address
Spouse's Name Work Phone #
Street Address
Occupation/Job Title
MEDICAL INSURANCE INFORMATION
Medical Doctor Phone Number
RESPONSIBLE PARTYFirst Name Home Phone #
Your Email Address
DependentPatient is:
Insurance Company City/State/Zip
Policy Holder Group Number
Other Insurance City/State/Zip Phone Number
Policy Holder Group Number
authorize my benefit payments to be paid directly to this office. I am financially responsible for non-covered services.
Signature of Person Responsible:
I will pay by: Bank Card
Worker's Compensation: Date of Injury Date Last Worked Claim Number
I certify that the above information is true and correct. I hereby authorize the release of any information required. I also

Name:__________________________________ Date:______________________
Please label the diagram using the letters below to best describe your current pain: (B) Burning (T) Tightness/Tension (S) Stiffness (P) Pain (N) Numbness/ Tingling
Pain Scale
0 No pain. Feeling perfectly normal. MINOR: Does not interfere with most activities. Ability to adapt to pain psychologically and with medication or devices such as cushions.
1 Very Mild
Very light or barely noticeable pain, such as a mosquito bite.
2 Discomfort
Minor pain; such as a pinch between fingers.
3 Tolerable
Very noticeable pain, such as an accidental cut or flu shot. A pain that is not so strong that you cannot get used to.
MODERATE: Interferes with many activities. Requires lifestyle changes but patient remains independent. Unable to adapt to pain
4 Distressing
Strong, deep pain such as a toothache, a bee sting, or stubbing your toe. Strong enough to notice the pain all the time and cannot completely adapt.
5 Very
Distressing
Strong, deep, piercing pain such as standing incorrectly on a sprained ankle. Noticeable all the time, preoccupied with managing it that normal activities are interfered with.
6 Intense
Strong, deep, and piercing pain so strong it seems partially dominate your senses, interrupting your though process. Comparable to non-migraine headache.
SEVERE: Unable to engage in normal activities. You are disabled and unable to function independently.
7 Very Intense
Same as 6 except pain completely dominates senses, causing unclear thinking half the time. Comparable to an average migraine headache.
8 Utterly
Horrible
Pain so intense you can’t think clearly, personality changes. Comparable to childbirth or a severe migraine.
9 Excruciating Unbearable
Pain so intense you can’t tolerate and demand drugs or surgery no matter what the side effects/risks. Comparable to cancer.
10 Unimaginable Unspeakable
Pain so intense you will go unconscious shortly. Most have never experienced this pain level. Those who have, likely passed kidney stones or suffered a crushed hand.
Please Rate Pain Levels 0-10
Neck: _______
Upper Back: _______
Mid Back: ______
Lower Back: ______
Legs: ______
Arms: ______