pathogens important to infection prevention and control
TRANSCRIPT

Pathogens Important to Infection Prevention and Control

Learning objectives
1. List special pathogens of interest to IP&C, and for each, describe the impact on the IP&C programme
2. Explain how antibiotic-resistant bacteria cause problems in healthcare
3. Outline preventive measures for a given special pathogen
Dec
emb
er 1
, 20
13
2

Time involved
• 90 minutes
Dec
emb
er 1
, 20
13
3

Special pathogens
• Everyday problem microorganisms for infection prevention and control include:• Mycobacterium tuberculosis • Clostridium difficile• Antibiotic resistant organisms
• MRSA, VRE• Gram-negative multiply resistant organisms
• Enterobacteria (Escherichia coli, Klebsiella pneumoniae)• Pseudomonas aeruginosa• Acinetobacter baumanii
Dec
emb
er 1
, 20
13
4

Mycobacterium tuberculosis• Mycobacterium tuberculosis causes tuberculosis (TB)• TB affects 1/3 of the world’s population• 9.4 million new cases in 2008• 1.8 million deaths in 2008• Leading cause of death in people living with human
immunodeficiency virus (HIV)
Dec
emb
er 1
, 20
13
5

Transmission and pathogenesis of TB - 1
• Spread by the airborne route when someone with active disease and positive sputum smear coughs, talks, sneezes, or spits
• Bigger droplets spread up to 1 m, smaller spread by air
• Bacteria inhaled into lungs• In lung tissue and lymph nodes the bacteria grow
and reproduce
• Can travel to any location in the body
Dec
emb
er 1
, 20
13
6

Transmission and pathogenesis of TB - 2• Latent TB – bacteria contained in the body• 10% of people with latent TB will develop active
disease• Most commonly affected organ - Lungs• Untreated, a person with active disease can infect
10 to 15 people a year
Dec
emb
er 1
, 20
13
7

Clinical forms• Pulmonary TB (active)
• Cough with thick cloudy, sometimes bloody sputum
• Tiredness• Appetite loss/unexplained weight loss• Night sweats• Fever/chills• Shortness of breath
• Extra pulmonary TB • Signs and symptoms vary with site of infection• Other common sites include central nervous
system, bones, joints, and genitourinary system
Dec
emb
er 1
, 20
13
8

Risk Factors• Weakened immune
system • Contact with someone
with active TB• Caring for active TB
patients• Living or working in
crowded conditions with someone with active TB• e.g., prisons, nursing
homes, homeless shelters
• Poor access to healthcare
• Alcohol or drug abuse• Travel to places where
TB is endemic• Being born in a
country where TB is endemic
• Some medications for rheumatoid arthritis
Dec
emb
er 1
, 20
13
9

Vaccination
• BCG strain of Mycobacterium bovis is used as a vaccine
• BCG is given to infants (best soon after birth)
• Vaccination against TB does not protect against infection but only against severe forms of disease• Meningitis• Disseminated TB (miliary)
Dec
emb
er 1
, 20
13
10

Diagnosis & Management
• Chest x-ray• Sputum smear for acid fast bacilli• Tuberculin skin test (TST)
• Can take up to 3 months for those newly exposed to develop positive test
• May be falsely positive because of BCG vaccination
• Interferon gamma release assays (IGRA) in vaccinated persons
• Culture (can take up to six weeks) and sensitivity test
Dec
emb
er 1
, 20
13
11

Management & Treatment
Management of Exposure• Confirmation of positive infection• Medical evaluation to determine follow up
Treatment of patients• Treatment for latent or active TB should follow
World Health Organization recommendations• Incomplete treatment can cause resistance• Adherence to therapy is critical
Dec
emb
er 1
, 20
13
12

IP&C MeasuresEngineering controls
• Negative pressure rooms • High efficiency particulate air (HEPA) filtration
system• Enhanced ventilation• Ultraviolet irradiation (only in empty room)• Sunlight exposure• Open window (last resort if no other options)
Dec
emb
er 1
, 20
13
13

Negative presssure room
Air flow
Patient with active TB isolated in negative pressure room
HEPA filter
Dec
emb
er 1
, 20
13
14

IP&C Measures - 1Administrative Controls
• Identify patients with signs and symptoms of TB
• Additional precautions for patients suspected to have active TB
• Prompt treatment• Vaccination of healthcare
personnel• Respiratory etiquette
Dec
emb
er 1
, 20
13
15

IP&C Measures - 2Personal Protective Equipment*
• N-95 fit tested masks for healthcare workers• If not available, then surgical masks
• Surgical masks for patients leaving their rooms Dec
emb
er 1
, 20
13
16
* Typically used for pulmonary TB if the patient is expectorating or has an open lesion

Conclusion
• Despite the high global impact of TB, it is treatable and preventable
• Occupation exposures remain a significant risk for healthcare workers
• IP&C measures are needed to decrease exposures to patients and healthcare workers
Dec
emb
er 1
, 20
13
17

Clostridium difficile: Background
• There is a global increase in Clostridium difficile infections (CDI) and outbreaks over the past 10 years; however the illness is not a problem in all countries
• CDI primarily occurs in those patients exposed to antibiotics in healthcare facilities
Dec
emb
er 1
, 20
13
18

Pathology - 1
• A Gram-positive spore forming anaerobic bacillus• Widely distributed in the environment• In its vegetative state
• Produces toxins• Can be killed by antibiotics
• Spore form • Dormant• No toxin production• Resistant to antibiotics and disinfectants• Can persist for months in the environment
Dec
emb
er 1
, 20
13
19

Pathology - 2
• Produces 2 toxins • Toxin A and Toxin B
• Bind to intestinal epithelial cells causing inflammation and diarrhea
• Toxins are cytotoxic and enteropathic• Alteration of the gut flora by antibiotics
an important risk factor (decrease of normal gut flora)
Dec
emb
er 1
, 20
13
20

Clinical Significance
• Mild disease • Non-bloody diarrhoea, often mucoid and foul
smelling, cramping, nausea, dehydration, low grade fever, leukocytosis
• Severe disease • Colitis, watery diarrhoea, abdominal pain,
fever, nausea, abdominal distension, pseudomembranes in the gut, toxic mega colon, death
Dec
emb
er 1
, 20
13
21

New Strain
• Increased incidence of B1/NAP1/027 strain• Causes severe disease• More resistant to standard therapy• More likely to relapse• Associated with higher mortality• 16x more toxin A; 23x more toxin B• Related to excessive use of certain
drugs/antibiotics
Dec
emb
er 1
, 20
13
22

Colonisation
• Approximately 3-5% of healthy adults and 20 to 40% of hospitalised patients may be colonised
• Colonised patients generally are not symptomatic• May be a potential reservoir for transmission
• Evidence suggest spores on the skin of asymptomatic patients can contaminate the hands of the healthcare worker
• No recommendations to treat carriers nor to perform admission screening
Dec
emb
er 1
, 20
13
23

Patients at Risk Previous antibiotic useSevere underlying illnessProlonged hospital stayAdvanced ageGastrointestinal surgery/manipulationHistory of irritable bowel diseasePatients on proton pump inhibitors
Admission Screening NoRoute of Transmission ContactIsolation Precautions YesAccommodation Single room preferred
Separate toileting facilitiesDocumentation (flagging of patients) May be of benefit to implement a system to designate patients known to be
colonised or infected for early notification on readmissionEnvironmental Cleaning Routine cleaning with attention to high touch surfaces and use of a sporicidal
agentConsider double-cleaning for outbreak situations
Discontinuation of Precautions No diarrhoea for at least 48 hoursFollow-up of Contacts NoPoint Prevalence NoAdditional Outbreak Measures Strict cleaning of multi-use equipment between patients
Dedicated patient equipment to positive casesEducation of staff, patients and visitorsAuditing of outbreak unit/area including hand hygiene, isolation
practices and environmental cleaning
Transmission and Control Measures
Dec
emb
er 1
, 20
13
24

Additional Control Measures
• Discontinuation of all antibiotics in a symptomatic patient (except for CDI)
• Facility-wide antibiotic control policies• Early notification of patients with
diarrhoea to the IC team • Not recommended
• Routine identification of carriers • Repeat testing post treatment for clearance
Dec
emb
er 1
, 20
13
25

Antibiotic Resistant Microorganisms
Dec
emb
er 1
, 20
13
26

Methicillin Resistant Staphylococcus aureus (MRSA)
Dec
emb
er 1
, 20
13
27

Background• Staphylococcus aureus is a Gram-positive
bacteria• 30% of people are permanently colonised
• Nose• Pharynx • Perineum
• Transient colonisation occurs, mainly on hands
• Colonisation although harmless, increases the risk of infection and transmission
Dec
emb
er 1
, 20
13
28

Clinical Significance of MRSA
• First a problem in 1960s• Globally has reached epidemic
proportions• Both community associated (CA) and
healthcare associated (HA) strains of MRSA
• Rates vary by • Country• Region• Individual healthcare facility
Dec
emb
er 1
, 20
13
29

Patients at Risk Previous antibiotic useSevere underlying illnessProlonged hospital stayPrevious contact with medical facilityUse of invasive proceduresClose proximity to a patient colonised or infected with MRSA
Admission Screening Sites Yes, based on patient risk factorsNares, rectal, wounds, exit sites
Route of Transmission Contact (plus droplet for symptomatic patients with pneumonia)
Isolation Precautions Yes
Accommodation Single room preferred
Documentation (flagging of patients) May be of benefit to implement a system to designate patients known to be colonised or infected for early notification on readmission
Environmental Cleaning Routine cleaning with attention to high touch surfaces
Discontinuation of Precautions Unresolved issue:Some institutions use the following criteria:Negative results from all colonised/infected body sites- 3 consecutive cultures taken at least one week apart in the absence of antibiotic therapyNote: Re-colonisation is known to occur so on-going monitoring is recommendedConsider maintaining isolation precautions in an outbreak setting
Follow-up of Contacts Two sets of specimens taken on different days with one taken a minimum of 7 days after the last exposure, especially in an outbreak setting
Point Prevalence In an outbreak setting:Conduct serial (e.g., weekly) unit specific point prevalence cultures to determine if transmission has decreased or ceasedConsider discharge and/transfer screening of patients until transmission has decreased or ceased
Additional Outbreak Measures Strict cleaning of multi-use equipment between patientsDedicated patient equipment to positive casesEducation of staff, patients and visitorsAuditing of outbreak unit/area including hand hygiene, isolation practices and environmental cleaning
MRSA Transmission and Control Measures
Dec
emb
er 1
, 20
13
30

VISA and VRSA• Vancomycin is drug of choice for treating
MRSA infections• Staphylococcus aureus with decreased
(intermediate) susceptibility to vancomycin = VISA
• Staphylococcus aureus with resistance genes Van A or Van B = VRSA• So far only few isolates in different parts of the
world
Dec
emb
er 1
, 20
13
31

Dec
emb
er 1
, 20
13
32
Vancomycin Resistant Enterococcus (VRE)

Background• Enterococci are normal gut bacteria• May also be present in the oropharynx, vagina,
or on skin• Causes serious bacterial infections
• Wound infections• Urinary tract infections• Endocarditis • Sepsis
• Often resistant to ampicillin (the drug of choice); infections then treated with glycopeptides
Dec
emb
er 1
, 20
13
33

VRE Epidemiology
• VRE is enterococcus that is resistant to the glycopeptide vancomycin
• First isolated in the 1980’s• Spread globally causing asymptomatic
colonization, infections, and outbreaks• The prevalence of VRE varies worldwide
Dec
emb
er 1
, 20
13
34

Clinical Significance
• Clinically relevant strains carry Van A or Van B resistance genes
• Limited antibiotics to treat VRE infections• Transfer of resistance genes to other
microorganisms such as MRSA is a great concern
Dec
emb
er 1
, 20
13
35

Patients at Risk Previous antibiotic useSevere underlying illnessProlonged hospital stayPrevious contact with medical facilityUse of invasive proceduresClose proximity to a patient colonised or infected with VRE
Admission Screening Sites Yes, based on patient risk factors. RectumRoute of Transmission Contact
Isolation Precautions YesAccommodation Single room preferred
Separate toileting facilitiesDocumentation (flagging of patients) May be of benefit to implement a system to designate patients known to be colonised or infected
for early notification on readmissionEnvironmental Cleaning Routine cleaning with attention to high touch surfaces
Consider double cleaning in outbreak situationsDiscontinuation of Precautions Unresolved issue:
Some institutions use the following criteria:Negative results from all colonised /infected body sites- 3 consecutive cultures taken at least one week apart in the absence of antibiotic therapyNote: Re-colonization is known to occur so on-going monitoring is recommended. Consider maintaining isolation precautions in an outbreak setting
Follow-up of Contacts Two sets of specimens taken on different days with one taken a minimum of 7 days after the last exposure, especially in an outbreak setting
Point Prevalence In an outbreak setting:Conduct serial (e.g., weekly) unit specific point prevalence cultures to determine if transmission has decreased or ceasedConsider discharge and/transfer screening of patients until transmission has decreased or ceased
Additional Outbreak Measures Strict cleaning of multi-use equipment between patientsDedicated patient equipment to positive casesEducation of staff, patients and visitorsAuditing of outbreak unit/area including hand hygiene, isolation practices and environmental cleaning
VRE Transmission and Control Measures
Dec
emb
er 1
, 20
13
36

Dec
emb
er 1
, 20
13
37
Multi-Drug Resistant Gram- Negative Microorganisms
(MDRGN)

MDRGN - 1
• The “Enterobacteriaceae” family of bacteria are a normal part of the gastrointestinal flora
• The most frequent isolates are:• Escherichia coli• Klebsiella pneumoniae• Serratia marcescens• Enterobacter species
Dec
emb
er 1
, 20
13
38

Mechanisms of Resistance
Escherichia coli and Klebsiella pneumoniae can have extended spectrum beta-lactamase (ESBL) enzymes that cause resistance to beta-lactam antibiotics including:
• Penicillins• Cephalosporins• Cephamycins• Monobactams
Dec
emb
er 1
, 20
13
39

Epidemiology of ESBL strains
• There are various types of ESBLs including • TEM• SHV • CTX-M
• ESBLs were first detected in Europe in 1980s• Surveillance data from several surveillance
systems indicate high rates of ESBLs in many parts of the world including USA, Canada, Europe, China, India and Latin America
Dec
emb
er 1
, 20
13
40

Epidemiology of CRE
• Carbapenem antibiotics are the treatment of choice for serious infections due to ESBL-producing bacteria
• Carbapenem Resistant Enterobacteriaceae (CRE) has also been reported
• Carbapenemases of importance include KPC, VIM, OXA and NDM-1
• CREs have been reported in many areas of the world and have also been associated with outbreaks
Dec
emb
er 1
, 20
13
41

MDRGN - 2
• The following bacteria are present in aquatic environments• Acinetobacter baumannii• Pseudomonas aeruginosa
• Opportunistic pathogens in humans • A major cause of healthcare-associated
infections• Septicemia• Ventilator-associated pneumonia • Urinary tract infections
Dec
emb
er 1
, 20
13
42

MDR P. aeruginosa and MDR A. baumannii
• These microorganisms have intrinsically lower susceptibility to antibiotics
• Acquiring additional resistance genes (ESBL genes, other genes for resistance to beta lactam antibiotics, resistance genes for aminoglycosides and fluoroquinolones) very often means that they are • susceptible only to carbapenems or• colistin or• resistant to all antibiotics (panresistant)
Dec
emb
er 1
, 20
13
43

Clinical Significance
• MDRGN (including ESBLs, CREs, MDR PA and MDR AB) pose a significant treatment challenge including • Increased length of stay• Increased mortality • Increased cost
• Contributes to the global crisis of antimicrobial resistance
• Control requires an aggressive world-wide strategy
Dec
emb
er 1
, 20
13
44
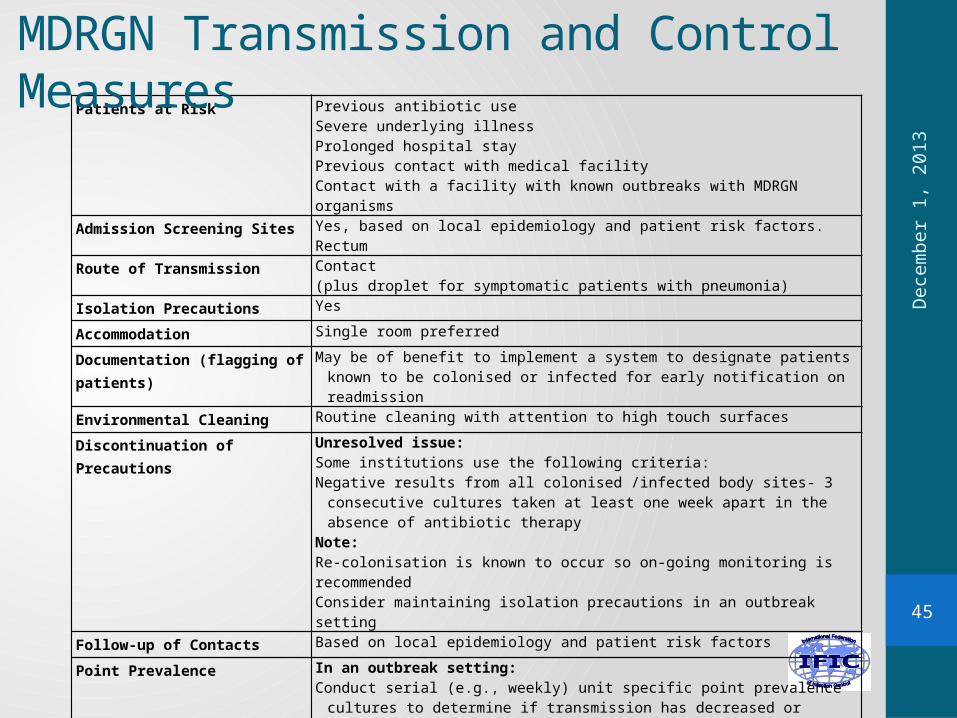
Patients at Risk Previous antibiotic useSevere underlying illnessProlonged hospital stayPrevious contact with medical facilityContact with a facility with known outbreaks with MDRGN organisms
Admission Screening Sites Yes, based on local epidemiology and patient risk factors. Rectum
Route of Transmission Contact (plus droplet for symptomatic patients with pneumonia)
Isolation Precautions Yes
Accommodation Single room preferred
Documentation (flagging of patients) May be of benefit to implement a system to designate patients known to be colonised or infected for early notification on readmission
Environmental Cleaning Routine cleaning with attention to high touch surfaces
Discontinuation of Precautions Unresolved issue:Some institutions use the following criteria:Negative results from all colonised /infected body sites- 3 consecutive cultures taken at
least one week apart in the absence of antibiotic therapyNote: Re-colonisation is known to occur so on-going monitoring is recommendedConsider maintaining isolation precautions in an outbreak setting
Follow-up of Contacts Based on local epidemiology and patient risk factors
Point Prevalence In an outbreak setting:Conduct serial (e.g., weekly) unit specific point prevalence cultures to determine if
transmission has decreased or ceasedConsider discharge and/transfer screening of patients until transmission has decreased or
ceased
Additional Outbreak Measures Strict cleaning of multi-use equipment between patientsDedicated patient equipment to positive casesEducation of staff, patients and visitorsAuditing of outbreak unit/area including hand hygiene, isolation
practices and environmental cleaning
MDRGN Transmission and Control Measures
Dec
emb
er 1
, 20
13
45

Management of Pathogens in Low Resource Countries • IP&C measures vary based on institutional
setting and available resources• Hand hygiene should be a routine part of
patient care in all settings• Additional precautions may be considered
depending on the pathogen, the institutional setting and outbreak circumstances
Dec
emb
er 1
, 20
13
46

Conclusion
• Antimicrobial resistance is a world-wide public health problem
• Solutions require a multi-faceted approach• Improving behaviours is essential• Global awareness and surveillance is required• Implementation of appropriate IP&C practices
and antimicrobial stewardship processes may be beneficial
Dec
emb
er 1
, 20
13
47

Key Points
• Tuberculosis and multi-drug resistant bacteria are important infection prevention and control issues
• Many have developed resistance to antimicrobials making them less effective
• Control measures vary by organism, setting and resources
Dec
emb
er 1
, 20
13
48

Further reading• Apisarnthanarak A, Fraser VJ. Feasibility and efficacy of
infection control interventions to reduce the number of nosocomial infections and drug resistant microorganisms in developing countries: what else do we need? CID 2009;48:22-24
• EARS-Net. http://www.ecdc.europa.eu/en/activities/surveillance/EARS-Net/Pages/index.aspx
• WHO 2010. Global tuberculosis control http://www.who.int/mediacentre/factsheets/fs104/en/index.html
• Special pathogens, in Damani N. Manual of infection prevention and control, 3rd ed. Oxford University Press, Oxford, 2012:183-249.
Dec
emb
er 1
, 20
13
49

Quiz
1. When a patient with active tuberculosis has to leave the isolation room for tests, s/he has to wear a N95 mask. T/F?
2. Admission screening for MRSA encompasses the following specimens:
a. Nares aloneb. Nares, wounds, exit sitesc. Nares, woundsd. Nares, exit sites
3. ESBL genes are transmitted by plasmids and are restricted to Enterobacteriaceae. T/F?
Dec
emb
er 1
, 20
13
50

International Federation of Infection Control• IFIC’s mission is to facilitate international networking in
order to improve the prevention and control of healthcare associated infections worldwide. It is an umbrella organisation of societies and associations of healthcare professionals in infection control and related fields across the globe .
• The goal of IFIC is to minimise the risk of infection within healthcare settings through development of a network of infection control organisations for communication, consensus building, education and sharing expertise.
• For more information go to http://theific.org/
Dec
emb
er 1
, 20
13
51