infection prevention and control: guidelines for long-term ... infection prevention and control...
TRANSCRIPT

Infection Prevention and Control:
Guidelines for
Long-Term Care Facilities
June 2015
Infection Prevention and Control Nova Scotia (IPCNS), Department of Health and Wellness
2
Acknowledgements:
Infection Prevention and Control Nova Scotia (IPCNS) would like to acknowledge the contribution and
expertise of the following individuals in the development of this guideline.
Principal Authors:
Kim Allain BScN RN MHS CIC Suzanne Rhodenizer Rose RN BScN MHS CIC
Provincial Infection Control Consultant Director, Quality, Patient Safety & IPCNS
Nova Scotia Department of Health & Wellness (DHW) Nova Scotia DHW
Halifax, Nova Scotia Halifax, Nova Scotia
IPCNS would like to acknowledge the contribution and expertise of the following individuals in providing
subject matter expertise for this document.
Dawn Cann RN BScN GNC(c), Infection Control Practitioner, Nova Scotia Health Authority-Central Zone
Danielle Henri RN, Occupational Health Nurse/Educator, Shannex Annapolis Valley
Leah MacDonald RN BSc BScN IIWCC Infection Control Practitioner, Nova Scotia Health Authority-Central Zone
Anne Mason BScN RN, Nurse Manager, Oakwood Terrace
Daphne Murray RN, Infection Control Practitioner, Nova Scotia Health Authority-Central Zone
Patsy Rawding RN BScN CIC, Site Manager, Shannex Annapolis Valley Pam Smith RN, Resource Coordinator, Western Region Home Support IPCNS would like to extend our thanks to the DHW Continuing Care branch, the Communicable Disease Prevention and Control Division (Public Health branch) and the membership of the Long-Term Care Facilities Working Group for their contribution, feedback and support of this guideline.
IPCNS would like to provide recognition and thanks to Eva Hatzis BSc CPHI(C) CIC, former Provincial Infection Control Consultant with the DHW, who was the initial lead and author for this guideline.
3
Table of Contents
1. Glossary of Terms .................................................................................................................................. 5
2. General Assumptions ............................................................................................................................ 9
3. Introduction ........................................................................................................................................ 11
4. Infection Prevention and Control ........................................................................................................ 12
5. Hierarchy of Controls .......................................................................................................................... 13
5.1 Engineering Controls ................................................................................................................. 13
5.2 Administrative Controls ............................................................................................................. 14
5.3 Personal Protective Equipment ................................................................................................. 14
6. The Chain of Infection ......................................................................................................................... 15
7. Routine Practices ................................................................................................................................. 18
7.1 Point-Of-Care Risk Assessment (PCRA) ..................................................................................... 18
7.2 Hand Hygiene ............................................................................................................................ 20
7.3 Personal Protective Equipment ................................................................................................. 24
7.4 Administrative Controls ............................................................................................................. 28
7.5 Environmental Cleaning and Disinfection ................................................................................. 29
7.5.1 Blood or body fluid clean-up ....................................................................................... 33
7.6 Non-critical resident care equipment and personal care supplies ............................................ 34
7.7 Linen .......................................................................................................................................... 35
7.8 Sharps safety and prevention of exposure to bloodborne pathogens ...................................... 36
7.8.1 Injection Safety and Aseptic Technique ...................................................................... 36
7.8.2 Multi-dose Vials ........................................................................................................... 37
7.8.3 Glucose Monitoring ..................................................................................................... 38
7.9 Pet therapy and animal visitation .............................................................................................. 38
8. Additional Precautions ........................................................................................................................ 40
4
8.1 Contact Precautions .................................................................................................................. 42
8.2 Droplet Precautions ................................................................................................................... 45
8.3 Droplet/Contact Precautions ..................................................................................................... 47
8.4 Airborne Precautions ................................................................................................................. 49
9. Surveillance ......................................................................................................................................... 53
10. Outbreaks ............................................................................................................................................ 54
11. Clostridium difficile Infections ............................................................................................................. 55
12. Antibiotic Resistant Organisms ........................................................................................................... 55
13. References ........................................................................................................................................... 56
Appendix A: Persons with Cognitive Impairment: Implications for IPAC Practices......................... 58
Appendix B: How to Handrub .......................................................................................................... 59
Appendix C: How to Handwash ....................................................................................................... 60
Appendix D: Sample Posters for Putting On and Removing Personal Protective Equipment ......... 61
Appendix E: Sample Contact Precautions Signage .......................................................................... 63
Appendix F: Four Moments for Hand Hygiene in LTCF ................................................................... 64
Figures
FIGURE 1: HIERARCHY OF CONTROLS .................................................................................................................. 13
FIGURE 2: THE CHAIN OF INFECTION ................................................................................................................... 15
FIGURE 3: POINT OF CARE RISK ASSESSMENT ....................................................................................................... 19
FIGURE 4: FOUR MOMENTS FOR HAND HYGIENE IN LTCFS .................................................................................... 23
FIGURE 5: PERSONAL PROTECTIVE EQUIPMENT .................................................................................................... 25
FIGURE 6: SAMPLE PROCEDURE FOR ROUTINE CLEANING OF A RESIDENT ROOM (DOES NOT INCLUDE ROOMS ON
ADDITIONAL PRECAUTIONS) ...................................................................................................................... 32
FIGURE 7: CLEANING A BLOOD OR BODY FLUID SPILL ............................................................................................ 33
FIGURE 8: CLEANING A BLOOD OR BODY FLUID SPILL ON CARPET ............................................................................ 34
FIGURE 9: ADDITIONAL PRECAUTIONS BASED ON MODE OF TRANSMISSION .............................................................. 42
FIGURE 10: TUBERCULOSIS SCREENING FOR NEW RESIDENTS ................................................................................. 49

5
1. Glossary of Terms Additional Precautions: Precautions (i.e. Contact, Droplet, Airborne) that are applied, in addition to Routine Practices, when infection, caused by microorganisms transmitted by these routes, is suspected or diagnosed. They include the physical separation of infected residents from other individuals and the use of barriers (e.g. gowns, gloves, face protection) to prevent the transmission of the infectious agent from infected residents to those who are susceptible to infection or may spread the infectious agent to others. Airborne exposure: Exposure to aerosols capable of being inhaled. Airborne transmission: Transmission of microorganisms via inhalation of aerosols that results in an infection in a susceptible host. Alcohol-based hand rub (ABHR): A liquid, gel or foam formulation of alcohol (60-90%) (e.g. ethanol, isopropanol) which is used to reduce the number of microorganisms on hands in clinical situations when the hands are not visibly soiled. Aseptic technique: The purposeful prevention of transfer of microorganisms from the resident’s body surface to a normally sterile body site or from one person to another by keeping the microbe count to an irreducible minimum. Also referred to as sterile technique. Cleaning: The physical removal of foreign material (e.g., dust, soil, organic material such as blood, secretions, excretions and microorganisms). Cleaning physically removes rather than kills microorganisms. It is accomplished using water and detergents in conjunction with mechanical action. Cohorting: The assignment of a geographical area such as a room or a resident care area to two or more residents who are infected or colonized with the same microorganism. In some instances, staffing assignments may be restricted to the cohorted group of residents. Cohort staffing: The practice of assigning specified workers to care only for residents known to be colonized or infected with the same microorganism. Can be used in addition to resident cohorting and geographical cohorting by assigning dedicated staff to care for either those residents who are infected, or those who are not. Colonization: The presence of a microorganism in or on a body with growth and multiplication, but without tissue invasion or cellular injury. The resident will be asymptomatic. Contact exposure: Contact exposure occurs when infectious agents are transferred through physical contact between an infected source and a host or through the passive transfer of the infectious agent to a host via an intermediate object. Contact Precautions: The type of Additional Precautions used to reduce the risk of transmitting infectious agents via direct or indirect contact with an infectious person. Contact Precautions are used in addition to Routine Practices.

6
Contamination: The presence of an infectious agent on a body surface, on clothes, gowns, gloves, bedding, toys, surgical instruments, dressings, or other inanimate objects. Diarrhea: Loose/watery bowel movements (conform to the shape of the container) and the bowel movements are unusual or different for the resident. Direct care: Providing hands-on care, such as bathing, washing, turning resident, changing clothes/incontinent products, dressing changes, care of open wounds/lesions, or toileting. Feeding, pushing a wheelchair and routine housekeeping are not classified as direct care. Disinfection: The inactivation of disease-producing microorganisms. Disinfection does not destroy bacterial spores. Medical equipment/devices must be thoroughly cleaned before effective disinfection can take place. Droplet: Solid or liquid particles suspended in the air, whose motion is governed principally by gravity and whose particle size is greater than 10 µm. Droplets are generated primarily as the result of an infected source coughing, sneezing or talking. Droplet exposure: Droplet exposure may occur when droplets that contain an infectious agent are propelled a short distance (i.e., within two metres) through the air and are deposited on the mucous membranes of the eyes, nose or mouth of a host. Drug Identification Number (DIN): The number located on the label of prescription and over-the-counter drug products that have been evaluated by the Therapeutic Products Directorate and approved for sale in Canada. Emerging respiratory infections: Acute respiratory infections of significant public health importance, including infections caused by either re-emergence of known respiratory pathogens (e.g., SARS) or emergence of as yet unknown pathogens (e.g., novel influenza viruses). Eye protection: Eye protection may include masks with built-in eye protection, safety glasses or face shields. Facial protection: Facial protection includes masks and eye protection, or face shields, or masks with visor attachment. Fit test: The use of a qualitative or quantitative method to evaluate the fit of a specific make, model and size of respirator on an individual. Fomites: Those objects in the inanimate environment that may become contaminated with microorganisms and serve as a vehicle of transmission. Hand hygiene: A general term referring to any action of hand cleaning. Hand hygiene relates to the removal of visible soil and removal or killing of transient microorganisms from the hands. Hand hygiene may be accomplished using soap and running water or an alcohol-based hand rub. Healthcare-associated infection: A term relating to an infection that is acquired during the delivery of health care.
7
Healthcare worker (HCW): Individuals who provide health care or support services such as nurses, physicians , dentists , nurse practitioners, paramedics, allied health professionals, temporary workers from agencies, unregulated health care providers (CCA, PCW, RCW), students , volunteers and workers who provide support services (e.g. food, laundry, housekeeping). High-touch surfaces: High-touch surfaces are those that have frequent contact with hands. Examples include doorknobs, call bells, bedrails, light switches, and wall areas around the toilet and edges of privacy curtains. Hospital-grade disinfectant: A disinfectant that has a drug identification number (DIN) from Health Canada indicating approval for use in Canadian hospitals. Infection: The entry and multiplication of an infectious agent in the tissues of the host. Asymptomatic or subclinical infection is an infectious process running a course similar to that of clinical disease but below the threshold of clinical symptoms. Symptomatic or clinical infection is one resulting in clinical signs and symptoms (disease). Infection is different from colonization (see definition). Infection prevention and control: Evidence-based practices and procedures that, when applied consistently in healthcare settings, can prevent or reduce the risk of transmission of microorganisms to healthcare workers, other residents, and visitors. Infection Control Professional(s) (ICPs): Trained individual(s) responsible for a healthcare setting’s infection prevention and control activities, such as the designated infection prevention and control expert in the facility, or individuals with specific infection prevention and control training and expertise. Ideally, ICPs should be board-certified (CIC designation) through the Certification Board of Infection Control and Epidemiology (CBIC). Infectious agent: A microorganism, such as a bacterium or virus, that is capable of invading body tissues, multiplying, and causing disease. Long-term care settings/facilities: Nursing Homes, Homes for the Aged, Residential Care Facilities, and Community Based Options Settings. Non-critical items: Items that touch only intact skin but not mucous membranes. Reprocessing of non-critical items involves thorough cleaning and low-level disinfection. Personal protective equipment (PPE): One element in the hierarchy of controls. Personal protective equipment consists of gowns, gloves, masks, facial protection (i.e., masks and eye protection, face shields or masks with visor attachment) or respirators that can be used by HCWs to provide a barrier that will prevent potential exposure to infectious microorganisms. Resident environment: The immediate space around a resident that may be touched by the resident and may also be touched by the healthcare worker when providing care. The resident environment includes equipment, medical devices, furniture (e.g. bed, chair, bedside table), telephone, curtains and personal belongings (e.g. clothes, books). In a multi-bed room, the resident environment is the area inside the individual’s curtain.

8
Point-of-care: The place where three elements occur together: the resident, the healthcare worker and care or treatment involving contact with the resident or his/her surroundings. Point-of-care products should be accessible without leaving the resident zone. Point-of-care Risk Assessment (PCRA): A PCRA is an activity whereby HCWs (in any healthcare setting across the continuum of care): 1) Evaluate the likelihood of exposure to an infectious agent
a. for a specific interaction b. with a specific resident c. in a specific environment (e.g., single room, hallway) d. under available conditions (e.g., no designated handwashing sink)
2) Choose the appropriate actions/PPE needed to minimize the risk of exposure for the specific resident, other residents in the environment, the HCW, other staff, visitors, contractors, etc. Public Health Agency of Canada (PHAC): A national agency focused on efforts to prevent chronic diseases and injuries and responsive to public health emergencies and infectious disease outbreaks by working closely with provinces and territories to help reduce pressures on the healthcare system. These activities were originally part of Health Canada and, in this document, Health Canada and PHAC are referred to synonymously. Reservoir: Any person, animal, or environmental surface in which an infectious agent survives or multiplies. Routine Practices: The system of infection prevention and control practices to be used with all residents during all care to prevent and control transmission of microorganisms in all health care settings. Routine Practices are based on the premise that all residents are potentially infectious, even when asymptomatic, and that the same safe standards of practice should be used routinely with all residents to prevent exposure to blood, body fluids, secretions, excretions, mucous membranes, non-intact skin or soiled items to prevent the spread of microorganisms. In LTCFs, residents colonized with specific microorganisms (e.g. Methicillin-resistant Staphylococcus aureus) are cared for using Routine Practices, instead of Additional Precautions used in acute care settings.
Staff: Anyone conducting activities within a healthcare setting that will bring him/her into contact with residents including: all healthcare providers (e.g. emergency service workers, physicians, dentists, nurses, CCAs/PCWs/RCWs, respiratory therapists, and other allied health professionals, students), support services (e.g. housekeeping), volunteers, and contract workers. Surveillance: The systematic ongoing collection, collation, and analysis of data with timely dissemination of information to those who require it in order to take action. Terminal cleaning: The cleaning of a resident room or bed space following discharge or transfer, in order to remove contaminating microorganisms that might be acquired by subsequent occupants. Terminal cleaning methods vary, but usually include removing all detachable objects in the room. In some instances, terminal cleaning might be implemented once some types of Additional Precautions have been discontinued. Virucide: A disinfectant capable of destroying or deactivating any specific virus. To be used in healthcare facilities, the virucide still requires a DIN from Health Canada.

9
2. General Assumptions Best practices in this document are based on the assumption that long-term care facilities (LTCF) in Nova
Scotia already have basic infection prevention and control measures in place.
Best practices are based on the following assumptions and principles:
1. LTCFs routinely implement best practices to prevent and control the spread of infectious diseases.
Best practices documents and guidelines applicable to healthcare facilities in Nova Scotia are
available on Infection Prevention and Control Nova Scotia’s website at: https://ipc.gov.ns.ca/.
2. LTCFs devote adequate resources to infection prevention and control (IPAC) which includes a
designated, trained person with responsibility for oversight of IPAC within the facility. Guidelines
and practice standards recommend that healthcare facilities have trained Infection Control
Practitioners (ICP) or trained staff as well as the resources to implement an IPAC program that is
proportional to the size, complexity, case mix and estimated risk of the populations served by the
facility.
3. LTCFs have effective working relationships with their local Public Health. They maintain clear lines
of communication, contact Public Health for information, and fulfill their obligations to report
notifiable diseases and conditions as per “It’s the Law: Reporting Notifiable Diseases and
Conditions”.
Link: http://novascotia.ca/DHW/CDPC/documents/06026_ItsTheLawPoster_En.pdf
4. LTCFs have programs in place that promote good hand hygiene practices and ensure adherence
to guidelines for hand hygiene.
5. LTCFs devote adequate resources to environmental services/housekeeping that include written
procedures for cleaning and disinfection of resident rooms and equipment, education of new
environmental services/housekeeping staff and continuing education for all staff, regular auditing
and an ongoing review of procedures and policy.
6. ICPs or designate provide regular education (including orientation and continuing education) and
support to enable healthcare workers to implement appropriate infection prevention and control
practices. Education programs are flexible enough to meet the diverse needs of the range of
healthcare providers and other staff who work in the healthcare setting.
7. LTCFs regularly assess and evaluate the effectiveness of their IPAC education programs and their
impact on practices, and use that information to refine their programs.
10
8. LTCFs promote collaboration and partnerships between all staff and professionals involved in the
facility, in implementing and maintaining appropriate infection prevention and control standards
that protect workers and residents.
9. There is clear delineation of cleaning and disinfection responsibilities and practices among
healthcare workers (i.e. environmental services, nursing staff, and other support staff) to ensure
the safety and cleanliness of environmental surfaces and resident care equipment.
10. There is communication between LTCFs and Emergency Health Services and receiving facilities
regarding transfers of residents to and from LTCFs when there are concerns about infectious
diseases.
11. LTCFs have a process for selecting personal protective equipment (PPE) to ensure it meets quality
standards where applicable.
12. LTCFs access the infection prevention and control resources and expertise available to them.
Infection prevention and control expertise in Nova Scotia includes; within the Department of
Health and Wellness, Infection Prevention Control Nova Scotia (IPCNS) at the DHW
https://ipc.gov.ns.ca/ ; the provincial chapter of Infection Prevention and Control Canada (IPAC
Canada)-Infection Prevention and Control Nova Scotia (IPAC NS) http://www.ipac-
canada.org/IPAC-NS/index.php ; Food Safety Specialists within the Nova Scotia Department of
Agriculture; infection control practitioners with the Nova Scotia Health Authority (NSHA) and IWK
Health Centre and the local Medical Officer of Health
http://novascotia.ca/dhw/publichealth/cpho-contact-information.asp and through local public
health offices http://novascotia.ca/dhw/publichealth/phs-offices.asp.
13. LTCFs have established procedures for receiving and responding appropriately to all local health,
regional and international advisories. They also communicate health advisories promptly to all
staff responsible for case finding/surveillance and provide regular updates. Current advisories are
available from local Public Health Services, DHW, Health Canada and Public Health Agency of
Canada websites, and IPCNS.

11
3. Introduction Healthcare-associated infections occur in all health care settings including long-term care facilities (LTCF).
Implementing infection prevention and control (IPAC) measures decreases the occurrence and spread of
healthcare-associated infections and outbreaks in LTCF.
Infection Prevention and Control: Guidelines for Long-Term Care Facilities been developed to provide
guidance and support for IPAC practices for LTCFs in Nova Scotia.
These guidelines are based on the comprehensive and well-researched documents produced by various
government partners, including Routine Practices and Additional Precautions for Preventing the
Transmission of Infection in Healthcare Settings by the Public Health Agency of Canada, Routine Practices
and Additional Precautions by the Provincial Infectious Diseases Advisory Committee of Public Health
Ontario and Take Control Prevent Infection Guide to Infection Prevention and Control in Long-Term Care
Facilities by Peel Public Health. IPCNS would like to recognize the value of these resources in the
development of this document.
These guidelines are intended to provide a source of information for those responsible for developing
guidelines and policies in long-term care including infection prevention and control professionals,
administrators and policy-makers. The information should be integrated with existing infection
prevention and control programs and policies in each facility and used as part of a comprehensive effort
to implement accepted standards and best practices for infection prevention and control. They may be
tailored to accommodate the specific needs of the resident population, unique infrastructure and services
provided in each facility. It is important to recognize that IPAC practices in LTCFs can be challenging due
to the resident populations affected with dementias and other cognitive impairments. Implementing IPAC
practices for some residents with cognitive impairment may necessitate a holistic and creative approach
(refer to Appendix A: Persons with Cognitive Impairment: Implications for IPAC Practices).
The guidelines are not regulatory, however, we recommend they be used to standardize infection
prevention and control practices throughout NS. A consistent approach will reduce confusion and
promote a better understanding by all of the required practices.
LTCF in Nova Scotia have access to IPAC expertise from a range of sectors including Infection Prevention
and Control Nova Scotia (IPCNS) within the Department of Health and Wellness, Infection Prevention and
Control Nova Scotia (IPAC NS), and staff dedicated to infection prevention and control in LTCFs. Expertise
related to communicable disease outbreaks exclusive of food safety issues can be found through local
public health and the Medical Officer of Health. Facilities are encouraged to contact these parties for
information and assistance in infection control matters.

12
4. Infection Prevention and Control Infection prevention and control (IPAC) describes the policies, knowledge, measures and practices that
must be in place in health care settings to prevent the spread of infection. Consistent and effective IPAC
practice is supported by following key principles developed by the Public Health Agency of Canada (PHAC).
The remainder of this document is an elaboration of the key principles by PHAC.
Consistent application of Routine Practices is expected for the care of all residents, at all times, across the continuum of care.
Adherence to Routine Practices will reduce the transmission of microorganisms in healthcare settings.
The need for individual components of Routine Practices is determined by a point-of-care risk assessment (PCRA) that includes an assessment of the task/care to be performed, the resident’s clinical presentation, physical state of the environment and the healthcare setting.
Microorganisms may be transmitted from symptomatic and asymptomatic individuals, emphasizing the importance of adhering to Routine Practices at all times for all residents in all healthcare settings.
In addition to Routine Practices, Additional Precautions should be used for residents with suspected or known infection with microorganisms for which Routine Practices may be insufficient to prevent transmission.
Additional Precautions should be used empirically, based on the resident’s condition or clinical presentation as well as when there is diagnostic confirmation of an infectious disease.
The primary goal of IPAC programs is to reduce the risk of acquiring a healthcare-associated infection to a minimum level; zero risk may not be attainable in every circumstance but should be strived for.
Local epidemiology should be considered in the application of Additional Precautions. For example, if there is high influenza activity occurring locally in the community, then the LTCF should suspect influenza if a resident displays compatible respiratory symptoms. In these instances, implement droplet and contact precautions for the resident, as well as, being on the look-out for other cases.
ROUTINE PRACTICES AND ADDITIONAL PRECAUTIONS FOR PREVENTING THE
TRANSMISSION OF INFECTION IN HEALTHCARE SETTINGS, PHAC
13
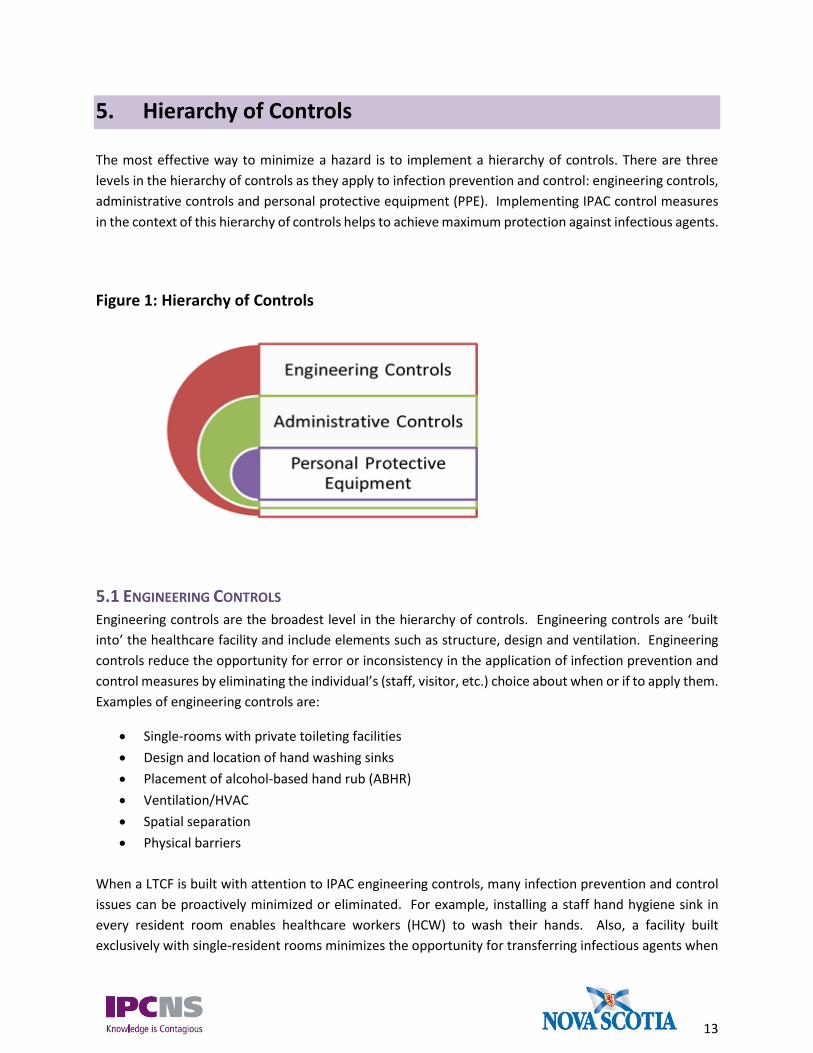
5. Hierarchy of Controls The most effective way to minimize a hazard is to implement a hierarchy of controls. There are three
levels in the hierarchy of controls as they apply to infection prevention and control: engineering controls,
administrative controls and personal protective equipment (PPE). Implementing IPAC control measures
in the context of this hierarchy of controls helps to achieve maximum protection against infectious agents.
Figure 1: Hierarchy of Controls
5.1 ENGINEERING CONTROLS Engineering controls are the broadest level in the hierarchy of controls. Engineering controls are ‘built
into’ the healthcare facility and include elements such as structure, design and ventilation. Engineering
controls reduce the opportunity for error or inconsistency in the application of infection prevention and
control measures by eliminating the individual’s (staff, visitor, etc.) choice about when or if to apply them.
Examples of engineering controls are:
Single-rooms with private toileting facilities
Design and location of hand washing sinks
Placement of alcohol-based hand rub (ABHR)
Ventilation/HVAC
Spatial separation
Physical barriers
When a LTCF is built with attention to IPAC engineering controls, many infection prevention and control
issues can be proactively minimized or eliminated. For example, installing a staff hand hygiene sink in
every resident room enables healthcare workers (HCW) to wash their hands. Also, a facility built
exclusively with single-resident rooms minimizes the opportunity for transferring infectious agents when

14
providing care to roommates. Although the HCW does not have direct control over engineering control
measures, it is important to be aware of how the structural environment influences the opportunity for
transmission of infections. This element is especially important for facility administrators to keep in mind
for the construction of new facilities or for facilities undergoing renovations.
5.2 ADMINISTRATIVE CONTROLS Administrative controls are the next level on the hierarchy of controls. Administrative controls are the
policies, procedures and resident care practices intended to prevent exposure and transmission of
microorganisms during the provision of care. Administrative controls require organizational commitment
and resources for their implementation and sustainability.
An Infection Prevention and Control Program and all of the components which fall within the program
constitute the administrative control measures in LTCF. Administrative controls are discussed further as
an element of Routine Practices in Section 7.4 Administrative Controls. LTCFs are expected to have
administrative control measures in place.
5.3 PERSONAL PROTECTIVE EQUIPMENT The use of PPE is the final step in the hierarchy of controls to minimize exposure to and subsequent
transmission of infectious agents. PPE provides a barrier between the HCW, visitor or other susceptible
host, from the infected source which may be a person, environmental surface or medical equipment.
Examples of PPE are gloves, gowns, masks, facial protection and respirators. PPE is highly dependent on
the user’s adherence and it is for this reason, the weakest tier in the hierarchy of controls. PPE must be
used in conjunction with the higher tiers of administrative and engineering controls. Nonetheless, correct
and appropriate use of PPE is important in healthcare interactions and will be discussed further under
Routine Practices in Section 7.3.

15
6. The Chain of Infection A model used to describe the disease transmission process is the chain of infection (Figure 2). The model
consists of a chain connected by six links. Each link on the chain represents an element required for a
disease to be transmitted and each link in the chain must be intact for an infection to occur. The
individual links are described in the following section.
Figure 2: The Chain of Infection
Organism/Infectious agent
The organism, also known as the microorganism or infectious agent, is the bacteria, virus, fungus or
parasite capable of causing an infection or disease. Depending on the infectious agent, there are
differences in the agent’s ability to cause disease, the severity of the disease caused and the quantity of
infectious agent needed to cause an infection. For some infections, very little quantity of an infectious
agent is needed to cause disease, for example, fewer than 18 viral particles are required to cause an
infection of Norovirus (reference: Public Health Ontario. Monthly Infectious Diseases Surveillance Report,
December, 2013).
Organism
Reservoir
Portal of Exit
Mode of Transmission
Portal of Entry
Susceptible Host
16
Reservoir
The reservoir is the source of the infectious agent. It is often the same place where the infectious agent
lives and reproduces. Humans, animals, water, soil and even food can be reservoirs. Humans and the
environment are the primary reservoirs of infectious agents relevant to healthcare.
Portal of exit
The portal of exit refers to the way the infectious agent leaves the reservoir. Portals of exit include the
respiratory tract through sneezing and coughing, the gastrointestinal tract through diarrhea and vomiting,
and non-intact skin through draining wounds and mucous membranes of the nose, mouth, and genital
tissue.
Mode of transmission
The mode or route of transmission describes the way in which an infectious agent ‘travels’ from a reservoir
to the next host. Routes of transmission of microorganisms which are of particular importance in
healthcare include contact, droplet, airborne and common vehicle transmission. The routes of
transmission vary with the microorganisms involved and some microorganisms can be transferred by
more than one route.
a. There are two types of contact transmission: direct contact with an infected person including
their secretions, excretions, body fluids (e.g. blood), or tissues, or indirect contact through
surfaces or other objects which have been contaminated with infectious agents. Infectious
agents which are transmitted by contact transmission include MRSA, VRE, Salmonella sp.,
Escherichia coli, scabies and norovirus. Either infection or colonization may result following
contact.
b. In droplet transmission, the infectious agent travels on the large respiratory droplets of
coughs, sneezes, from talking and from aerosol-generating medical procedures, travelling up
to 2 metres to land on the next person’s mucous membranes (eyes, nose or mouth) if they
are in the path of the droplets. Bacterial meningitis and pertussis (whooping cough) are
transmitted in this manner. Droplets may also contaminate the immediate environment
when they settle on surfaces and those that survive on surfaces contribute to contact
transmission.
c. In airborne transmission, the infectious agents travel on very small aerosols which are emitted
from coughs, sneezes or by talking and are able to remain suspended in the air or on dust
particles for long periods of time. The infectious agents can be dispersed in the same room
or over a longer distance by air currents or ventilation systems and can become inhaled by a
susceptible host. Diseases which are transmitted in this manner are chicken pox (varicella),
measles and tuberculosis.

17
d. In common vehicle transmission, a single contaminated source such as food or multi-dose
vials of medication contaminated with an infectious agent, act as vehicles to transmit
infection to multiple hosts.
Portal of entry
The portal of entry is the route by which the infectious agent enters the new host. Portals of entry include
mucous membranes of the eyes, nose and mouth, non-intact skin, the gastrointestinal tract via through
ingestion and through breaks in the skin from devices (e.g. an intravenous line).
Susceptible host
The susceptible host refers to the person who can become infected by entry of the infectious agent into
their body. Underlying health conditions, age, immunity and immunization status all play a role in the
susceptibility of the host to an infection and the severity of a resulting infection. Elderly people, including
residents in LTCFs, are generally more vulnerable to becoming ill with infectious diseases, often resulting
in more severe infections.
All six links in the chain must be intact in order for an
infection to be transmitted from one person to another. If
any single link in the chain is broken, infection cannot occur.
The goal of infection prevention and control is to break a link
on the chain of infection

7. Routine Practices Routine Practices are implemented as the standard of care to prevent exposure to blood, body fluids,
secretion, excretions, mucous membranes and non-intact skin which may contain potentially infectious
agents. Routine Practices are based on the assumption that every resident can potentially harbour an
infection, even when not showing signs or symptoms of an infection. Routine Practices should be used
at all times to prevent exposure of HCWs.
Routine Practices are made up of a number of elements which include: a point-of-care risk assessment,
hand hygiene, PPE, administrative controls, environmental cleaning and disinfection, aseptic technique
and sharps safety. Each of the elements of Routine Practices are described in further detail in the sections
below.
7.1 POINT-OF-CARE RISK ASSESSMENT (PCRA)
The PCRA is an assessment of the interaction between the HCW, the resident and/or the resident’s
environment to determine the potential for exposure to infectious agents.
Key things to assess when conducting a PCRA are:
i. the condition of the resident,
ii. the resident environment,
iii. the nature of the interaction.
ROUTINE PRACTICES ARE THE INFECTION PREVENTION AND CONTROL
PRACTICES FOR USE IN THE ROUTINE CARE OF ALL RESIDENTS AT ALL
TIMES IN ALL HEALTHCARE SETTINGS AND ARE DETERMINED BY THE
CIRCUMSTANCES OF THE RESIDENT, THE ENVIRONMENT AND THE TASK
TO BE PERFORMED.
Source: Routine Practices and Additional Precautions for Preventing the Transmission of Infection in Healthcare Settings, PHAC
19
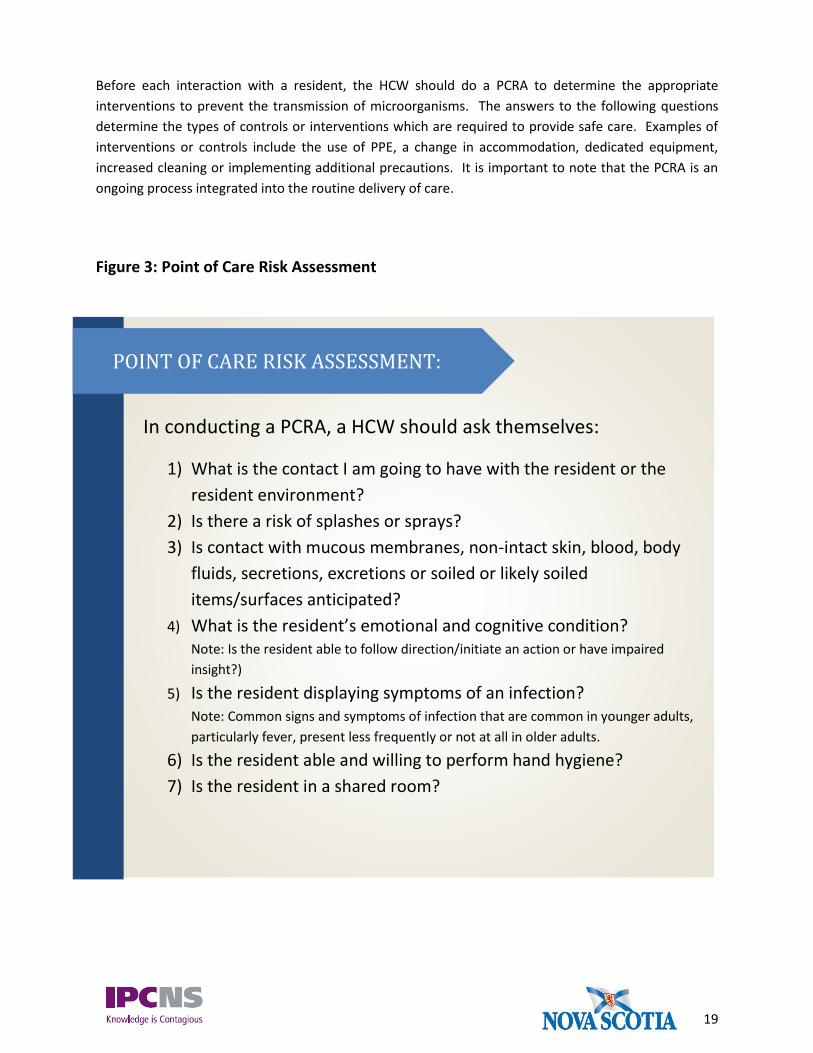
Before each interaction with a resident, the HCW should do a PCRA to determine the appropriate
interventions to prevent the transmission of microorganisms. The answers to the following questions
determine the types of controls or interventions which are required to provide safe care. Examples of
interventions or controls include the use of PPE, a change in accommodation, dedicated equipment,
increased cleaning or implementing additional precautions. It is important to note that the PCRA is an
ongoing process integrated into the routine delivery of care.
Figure 3: Point of Care Risk Assessment
In conducting a PCRA, a HCW should ask themselves:
1) What is the contact I am going to have with the resident or the
resident environment?
2) Is there a risk of splashes or sprays?
3) Is contact with mucous membranes, non-intact skin, blood, body
fluids, secretions, excretions or soiled or likely soiled
items/surfaces anticipated?
4) What is the resident’s emotional and cognitive condition? Note: Is the resident able to follow direction/initiate an action or have impaired
insight?)
5) Is the resident displaying symptoms of an infection? Note: Common signs and symptoms of infection that are common in younger adults,
particularly fever, present less frequently or not at all in older adults.
6) Is the resident able and willing to perform hand hygiene?
7) Is the resident in a shared room?
POINT OF CARE RISK ASSESSMENT:

20
7.2 HAND HYGIENE
The term hand hygiene encompasses hand washing with soap and water or hand antisepsis using alcohol-
based hand rub (ABHR) to clean hands. It also includes actions taken to maintain healthy hands and
fingernails. Hand hygiene prevents the transfer of microorganisms to and from a healthcare worker’s
hands onto a resident, environmental surface or themselves.
Alcohol-based Hand Rub
Hand hygiene with alcohol-based hand rub
(ABHR) at the point-of-care is the preferred
method of hand hygiene in LTC with a few
exceptions (see Hand Washing). Point-of-care
refers to the place where the resident, the
healthcare worker and the care procedure come
together. ABHR should be accessible without
leaving the patient zone and are generally
placed within arm’s reach of the HCW.
ABHR formulations should contain between 60% to 90% alcohol; concentrations of alcohol less than 60%
or greater than 90% will not be effective and should not be used in LTCF. ABHR formulations with ethanol,
isopropanol, or n-propanol are acceptable. Hand rubs with other chemical agents are not acceptable.
Technique is important when using ABHR to ensure that all the areas of the hands are covered with the
ABHR and for the correct amount of time. See Appendix B for correct technique when using ABHR.
Hand Washing
Hand washing using plain soap and water is an effective way to clean hands in LTCF. Hand washing is
actually recommended over ABHR in certain circumstances such as:
1. When hands are visibly soiled
2. When a build-up of ABHR feels uncomfortable
3. After caring for a resident with confirmed or suspect norovirus or Clostridium difficile or during an
outbreak of either of these organisms
4. After using the washroom
When there is exposure to norovirus or Clostridium difficile or during outbreaks of norovirus or Clostridium
difficile, hand washing with soap and water is recommended by PHAC. In the case of norovirus, ABHR
with at least a 70% concentration of alcohol and documented efficacy against norovirus or its surrogate
calicivirus, may be used if a dedicated hand wash sink is not available, followed by washing with soap and
water when a dedicated hand wash sink becomes available.
Hand hygiene is the most effective
way of preventing the transmission of
healthcare-associated infection (HAI)
to residents, staff and visitors in all
healthcare settings.

21
Hand washing technique is important to ensure that all the areas of the hands are covered for the correct
duration of time. See Appendix C for correct hand washing technique when using soap and water. It is
not acceptable for HCWs to use bar soap or shared towels for hand hygiene in LTCF.
Hand Health
Attention to hand health is vital to maintain ongoing and effective hand hygiene. Skin that is dry, cut or
otherwise painful, negatively affects adherence to hand hygiene. Furthermore, damaged skin is more
vulnerable to infection and also may shed more microorganisms.
A hand health program should be in place in LTCF to assess, prevent and manage skin problems on HCW
hands. Referrals to a dermatologist, evaluation of alternate products and prevention of contact
dermatitis are all components of the hand health program.
Nails
Long or artificial nails, gel nails, chipped nail polish or nail art are not recommended for HCWs.
Microorganisms can be trapped underneath long fingernails (artificial or natural), as well as, under
chipped nail polish. Furthermore, long nails and nail art can puncture gloves. Hand hygiene may be
compromised as HCWs protect artificial nails, nail art or long natural nails from damage by reducing hand
hygiene. Artificial fingernails, fingernail enhancements or extenders should not be worn when providing
resident care. Natural nails should be kept short, and nail polish, if worn, should not be chipped. There is
no evidence of an increase in bacterial load in the presence of intact nail polish on natural short nails.
Jewelry
Arm and hand jewelry such as bracelets, rings and wrist watches impede effective hand hygiene. Skin
underneath rings has been reported to be more heavily colonized with microorganisms than comparable
areas of skin on fingers without rings. Ideally, no hand or wrist jewelry should be worn when providing
resident care. Some LTCF may allow HCWs to wear a simple band.
Some LTCF assign staff to both resident care and food handler duties. The Nova Scotia Food Safety
Regulations and the Nova Scotia Retail and Food Services Code requires that food handlers remove any
objects (e.g. jewelry), which might fall into or contaminate food. Food handlers are expected to comply
with these requirements which are enforced by the Department of Agriculture.
Other Barriers
Extremity support devices, such as casts, splints, and complex bandages on the hands and forearms of
HCWs may impede effective hand hygiene. HCWs who wear such devices should be assessed by
occupational health services or delegate, in collaboration with, Infection Prevention and Control to
investigate whether they are able to perform adequate hand hygiene to be able to continue to provide
resident care.

22
A Hand Hygiene Program
Performing hand hygiene at the right time or moment is important to prevent the spread of infection. A
number of factors contribute to the ability or inability to comply with hand hygiene such as knowledge
about the moments to clean hands, competing demands for a HCWs time, availability of hand hygiene
infrastructure, such as ABHR at point-of-care, as well as support for hand hygiene within the organization.
Implementing a hand hygiene program will help the facility to address the barriers to hand hygiene and
provide the support to enable appropriate and effective hand hygiene at all times within the facility. A
hand hygiene program should include the following elements:
A multifaceted, multi-disciplinary and facility-wide committee to provide leadership and decision-
making
Education to HCWs about when and how to clean their hands
Environmental assessments and system supports to improve access to hand hygiene, including
ABHR at the point-of-care
A hand care program to maintain skin integrity, in collaboration with Occupational Health
Senior and middle management support and commitment to make hand hygiene an
organizational priority and address non-compliance
Ongoing auditing and observation of hand hygiene practices, with feedback provided to the HCWs
in real-time and processes to report performance indicator data internally
A strategy for resident engagement
Opinion leaders and champions modeling the desired behavior
A number of evidence-based hand hygiene programs have been developed in Canada. There are
resources available from IPAC Canada, the Just Clean Your Hands program with Public Health Ontario and
the STOP! Clean Your Hands program from the Canadian Patient Safety Institute. These resources will
have posters, audit tools/forms and videos to assist facilities in developing a comprehensive hand hygiene
program. A vital component of a hand hygiene program is the education of HCWs about the right times
to clean their hands. The instances when hand hygiene should be performed during the delivery of
healthcare have been simplified into four key moments (See Figure 4 and refer to Appendix F):
1. Moment 1: Before initial resident/resident environment contact
2. Moment 2: Before aseptic procedures
3. Moment 3: After body fluid exposure risk
4. Moment 4: After resident/resident environment contact

23
Figure 4: Four Moments for Hand Hygiene in LTCFs
Source: http://www.publichealthontario.ca/en/eRepository/4-moments-for-hand-hygiene-male-lg.pdf
Other instances when hands of HCWs should be cleaned include, but are not limited to:
Before and after eating
After using the washroom
After sneezing or coughing
After smoking
Before and after recreational activities
Before and after outings outside of the LTCF
Before and after contact with animals
Hand Hygiene for the Resident
Personal hand hygiene for residents is also very important. Residents should be provided with initial and
ongoing education on when and how to clean their hands effectively. Residents should be encouraged or
assisted to perform hand hygiene after toileting, leaving their room and prior to eating.
24
7.3 PERSONAL PROTECTIVE EQUIPMENT Personal protective equipment (PPE) refers to the barriers worn by HCWs to minimize exposure to blood,
body fluids, secretions or excretions. The barriers include gloves, gowns, masks, facial protection and
respirators. PPE protects the both the HCW and resident from exposure to infectious agents.
A point-of-care risk assessment (PCRA) should be undertaken before selecting PPE to help the HCW
identify hazards and select the optimal PPE for maximizing protection for both themselves and the
resident.
PPE should be put on immediately prior to the interaction with the resident or their environment and
removed immediately following the interaction. Inappropriate use of PPE may inadvertently put the
resident and HCW at greater risk for transmission of microorganisms.
PPE must be put on and removed in a manner that minimizes the risk of self-contamination. PPE should
also be placed immediately in the waste receptacle or laundry (e.g. for reusable gowns). HCW should be
trained and audited regularly on the correct sequence of putting on and removing PPE. Visual tools such
as posters are helpful. Refer to Appendix C for sample posters.
Examples of inappropriate PPE use are:
Wearing the same gloves from resident to resident
Not changing gloves between different tasks on the same resident, such as performing
incontinence care and feeding a resident
Wearing PPE in the hallway
Coming into work ill and wearing facial protection as a substitute for staying home
Reusing PPE
Washing hands while wearing gloves
Wearing facial protection (mask/ eye protection) that only covers the mouth and not the nose
Wearing a gown without securing ties
25
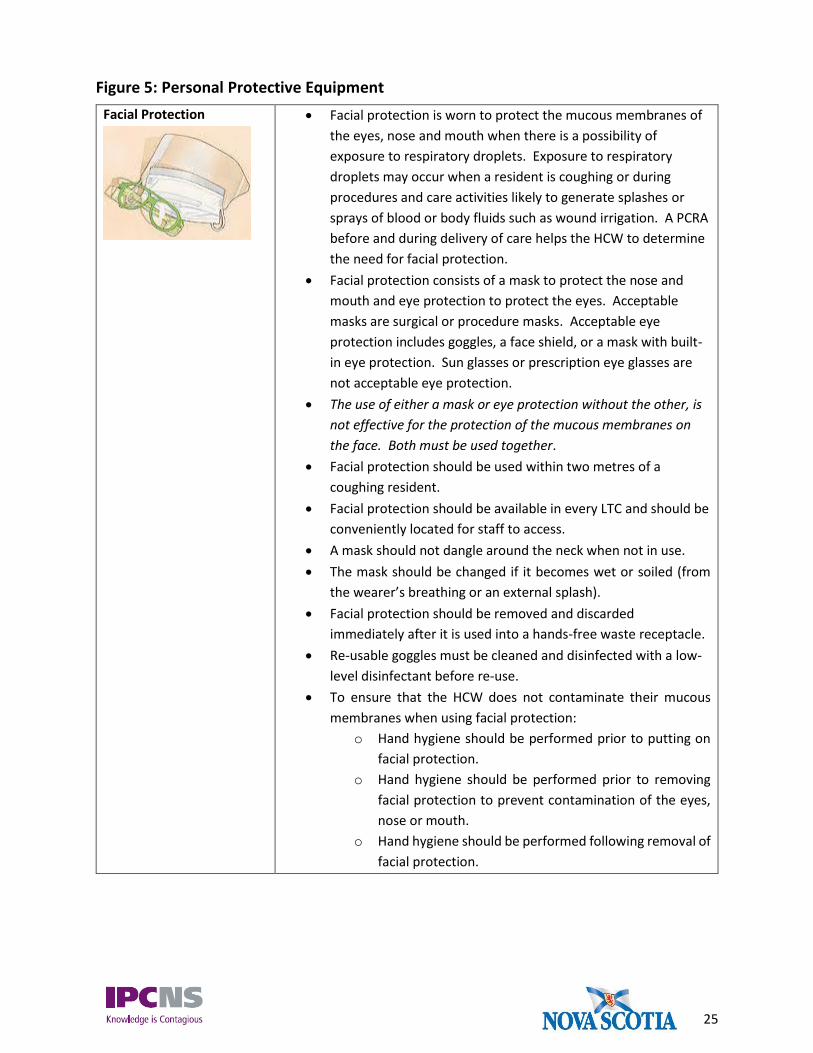
Figure 5: Personal Protective Equipment
Facial Protection
Facial protection is worn to protect the mucous membranes of
the eyes, nose and mouth when there is a possibility of
exposure to respiratory droplets. Exposure to respiratory
droplets may occur when a resident is coughing or during
procedures and care activities likely to generate splashes or
sprays of blood or body fluids such as wound irrigation. A PCRA
before and during delivery of care helps the HCW to determine
the need for facial protection.
Facial protection consists of a mask to protect the nose and
mouth and eye protection to protect the eyes. Acceptable
masks are surgical or procedure masks. Acceptable eye
protection includes goggles, a face shield, or a mask with built-
in eye protection. Sun glasses or prescription eye glasses are
not acceptable eye protection.
The use of either a mask or eye protection without the other, is
not effective for the protection of the mucous membranes on
the face. Both must be used together.
Facial protection should be used within two metres of a
coughing resident.
Facial protection should be available in every LTC and should be
conveniently located for staff to access.
A mask should not dangle around the neck when not in use.
The mask should be changed if it becomes wet or soiled (from
the wearer’s breathing or an external splash).
Facial protection should be removed and discarded
immediately after it is used into a hands-free waste receptacle.
Re-usable goggles must be cleaned and disinfected with a low-
level disinfectant before re-use.
To ensure that the HCW does not contaminate their mucous
membranes when using facial protection:
o Hand hygiene should be performed prior to putting on
facial protection.
o Hand hygiene should be performed prior to removing
facial protection to prevent contamination of the eyes,
nose or mouth.
o Hand hygiene should be performed following removal of
facial protection.

26
Gloves
Gloves should be worn when contact with blood, body fluids,
secretions, excretions, mucous membranes, draining wounds or
non-intact skin is anticipated during the provision of care. A PCRA
prior to and during the delivery of care will help the HCW to
determine the need for gloves during routine resident care.
Gloves should also be worn for handling items or touching surfaces
visibly or potentially soiled with blood, body fluids, secretions or
excretions.
Gloves should be worn while providing direct care if the HCW has
an open cut or abrasions on their hands.
Medical grade gloves should be available at every LTCF and should
be conveniently located for staff to use.
Sandwich gloves and other non-medical grade gloves are not
acceptable.
Hand hygiene should occur immediately before the gloves are put
on and immediately after they are taken off.
If gloves are not used correctly they become vehicles for disease
transmission. For example, wearing the same pair of gloves to
care for different residents.
Gloves should be removed and hand hygiene should be performed
when moving from ‘dirty’ to ‘clean’ tasks on the same resident.
Gloves are single-use and should not be reused, cleaned with
alcohol-based hand rub or washed.
Gloves should be removed and discarded into a hands-free waste
receptacle immediately following their intended use.
Hand hygiene should be performed immediately following the
removal of gloves.
The HCW should not touch their face when wearing gloves.
Gown
Gowns are used to protect the HCWs clothing or skin from
splashes or sprays of blood, body fluids, secretion or excretions. A
PCRA before and during the delivery of care will help the HCW to
determine the need for gowns during routine resident care.
Gowns should be available at every LTCF and should be
conveniently located for staff to access.
Gowns should be long-sleeved, wide enough to completely cover
the HCW, as well as long enough to cover from the neck to the
mid-thigh.
Gowns are single-use and should be disposed of in a hands-free
waste receptacle.
The same gown should never be worn when going from resident
to resident or between environments (e.g. accompanying a
resident to the dining room).

27
Gowns should be removed in a manner that will not contaminate
the HCW’s skin or clothing.
Gowns should be tied securely.
Respirator
HCWs who may need to wear a respirator (e.g. N95 respirator)
should be fit tested and receive appropriate training on how to
wear the respirator. Fit-testing refers to the use of a qualitative
or quantitative method to evaluate the fit of a specific make,
model and size of respirator on an individual.
In Nova Scotia, all LTCF are expected to have a respiratory
protection program as per the Occupational Health and Safety Act.
This means that as a minimum, enough core staff need to have
current respirator fit-testing to be able to provide continuous care
for residents in the event of a case or outbreak of an infectious
disease requiring airborne precautions. As well, there must be
adequate supplies in the facility.
Healthcare workers should remain clean shaven in the area of the
respirator seal to ensure facial seal.
Hand hygiene should be performed prior to putting on a
respirator.
A ‘Fit Check’ should be performed every time a respirator is put on
and before entry to the resident’s room.
Self-contamination should be avoided by not touching the
respirator on its external surface during use and disposal.
Respirators should be carefully removed by the straps.
A respirator should not dangle around the neck when not in use.
The respirator should be changed if it becomes wet or soiled (from
the wearer’s breathing or an external splash).
The respirator should be removed and discarded immediately
after its use outside of the room where it was required, into a
hands-free waste receptacle, followed by hand hygiene.

28
7.4 ADMINISTRATIVE CONTROLS The major administrative control in LTCF is the infection prevention and control (IPAC) program. Each
facility is expected to have a functioning IPAC program which reflects current best practices. The
components for the program should include:
IPAC policies and procedures that address Routine Practices and Additional Precautions,
outbreak management, point-of-care risk assessment, sharps safety, prevention of exposure to
bloodborne pathogens and immunization programs. Clear, easy-to-follow policies and procedures
will facilitate the day-to-day functioning of the facility as well as during emergency and outbreak
situations.
A system to detect and investigate infections and to detect, investigate and control outbreaks and
a system to notify local public health of reportable diseases and outbreaks.
Continuing education in IPAC for staff (hand hygiene, use of PPE, cleaning and disinfecting) and
general IPAC awareness.
An employee health program, which includes healthy workplace policies, that states that staff
should not come into work when ill with symptoms of an infectious respiratory or gastrointestinal
illness.
An environmental cleaning program which includes regular auditing or processes to ensure
cleaning and disinfection meets best practices.
An IPAC committee to oversee the program. If there is no IPAC committee, then IPAC should be
a standing agenda item for another appropriate meeting or within general meetings.
A hand hygiene program.
An immunization program for residents to ensure that immunizations are up-to-date, including
promotion and provision of annual influenza vaccine. A process or program should also be in place
to monitor staff immunization status.
Visitor policies which balance the residents’ and families’ needs with the protection of residents
from infectious diseases. Hand hygiene should be emphasized as well as restrictions on ill visitors
coming into the facility.
A clear process to determine resident placement, accommodation and flow. From an infection
prevention and control perspective, single-room accommodation is best. Given that single-rooms
may not be available in all LTCF, there should be guidelines for resident placement in shared
rooms. For example, residents with indwelling devices should not have residents with chronic or
draining wounds as roommates.

29
7.5 ENVIRONMENTAL CLEANING AND DISINFECTION Surfaces in LTCFs can become easily contaminated with infectious agents that can survive in the
environment, such as influenza and Clostridium difficile. Infectious agents can be picked up from surfaces,
transferred onto the hands of HCWs, residents, visitors or resident care equipment and transmitted to
other residents and staff, resulting in infections. High-touch surfaces have the greatest potential to
harbour infectious agents. High-touch surfaces are those that have frequent contact with hands and
include doorknobs, keyboards, elevator buttons and surfaces in close proximity to the resident such as
call bells, bedrails and bedside tables. Cleaning reduces the number of microorganisms in the
environment and disinfection kills or inactivates the remaining disease-causing microorganisms.
Environmental cleaning and disinfection are necessary to prevent transmission in health care and are key
components of Routine Practices.
General
There should be IPAC education and training provided for housekeeping/environmental services staff
which includes cleaning procedures, hand hygiene, Routine Practices and PPE.
There should be written protocols and procedures for environmental cleaning and disinfection which
include a schedule for cleaning and disinfection, record keeping, monitoring and verification of the
cleaning and disinfection process.
A comprehensive, thorough cleaning and disinfection of the resident’s room or bed space should be
scheduled at regular intervals (e.g. Spring and Fall Cleaning).
Safety, effectiveness and staff preference should be considered when selecting new products for
cleaning and disinfection.
There should be a system in place for enhanced cleaning and disinfection during an outbreak
Environmental services staff should be expected to use Routine Practices and Additional Precautions
in the course of their work (hand hygiene, gloves).
A discharge cleaning and disinfection protocol and/or checklists should be in place and implemented
to ensure rooms are cleaned and disinfected following resident discharge or transfer.
Floors should be constructed of resilient sheet or resilient tile, be durable, able to withstand the
cleaning frequencies and chemicals used in the facility.
Carpeting should not be installed in LTCFs.
If carpeting is present, it should be cleanable with hospital-grade cleaners and disinfectants.
Furnishings and equipment should be of a material and construction which can be readily cleaned and
disinfected.
30
Cleaning
High-touch surfaces (resident bed rails, resident aides, light switches, arms of resident chairs, hand
rails) should be cleaned and disinfected daily at a minimum and more frequently, as needed, in cases
of gross contamination and during outbreaks.
Low-touch surfaces such walls, ceilings and window coverings should be cleaned on a regular basis
and whenever they become soiled.
Cleaning should proceed from clean to dirty areas of the room and from high to low vertically.
Under normal circumstances, floor cleaning with a detergent is adequate and disinfection is not
needed. For further information on cleaning of blood and body fluid spills, see Section 7.5.1.
Tools (mops, buckets, rags) used for cleaning and disinfecting should be cleaned and dried after use.
Mops and rags should not be hung to dry. Dry these items in a dryer.
Mop heads should be changed between resident rooms, laundered daily and dried prior to storage or
re-use.
Cloth should not be ‘double dipped’ in cleaning solutions. This means soiled cloths are not dipped into
the disinfectant solution again after being used.
If re-usable bottles are filled with cleaners or disinfectants, ensure the bottles are pre-cleaned and
dried thoroughly, labelled with the product, the expiry date from the original bottle, the date the
bottle was filled, and never ‘topped-up’.
Equipment used to clean toilets (e.g., toilet brushes, toilet swabs) should not be carried from room-
to-room. The toilet brush should remain in the room; if not, consideration should be given to using
disposable toilet swabs.
Disinfection
Cleaning happens first. Disinfection follows cleaning.
Each disinfectant has a recommended wet-contact time by the manufacturer. The disinfectant must
have wet contact with the surface for the specified period of time in order for it to be effective.
The levels of disinfection applicable in LTCFs are low-level disinfection and high-level disinfection.
Another method that may be used in some LTCFs is sterilization. Sterilization is a method of removing
all microbial life from an item and is usually reserved for equipment that enters sterile tissue or sterile
body cavities.
Low-level disinfection is the level of disinfection required for environmental cleaning. Low-level
disinfection is achieved by using a product that is registered with Health Canada, has a Drug
Identification Number (DIN), and is labelled as either, a low-level disinfectant, a hospital disinfectant,
a hard surface disinfectant, a general disinfectant, a germicide or a microbicide.
31
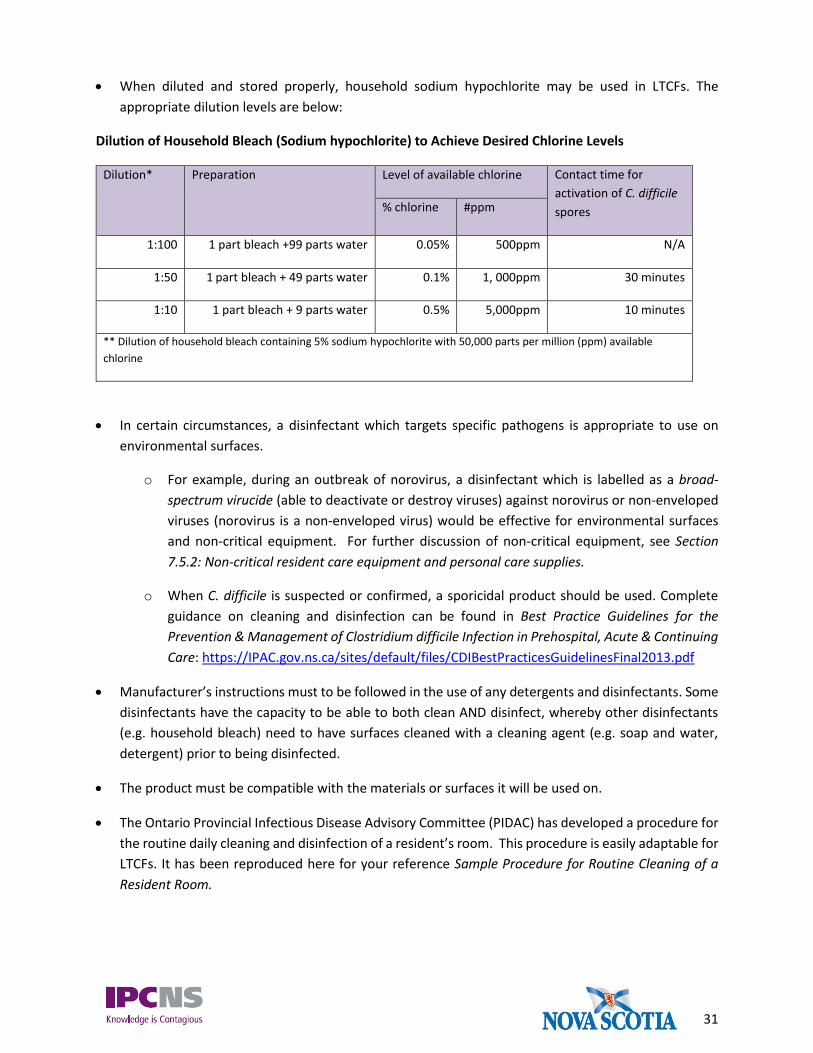
When diluted and stored properly, household sodium hypochlorite may be used in LTCFs. The
appropriate dilution levels are below:
Dilution of Household Bleach (Sodium hypochlorite) to Achieve Desired Chlorine Levels
Dilution* Preparation Level of available chlorine Contact time for
activation of C. difficile
spores % chlorine #ppm
1:100 1 part bleach +99 parts water 0.05% 500ppm N/A
1:50 1 part bleach + 49 parts water 0.1% 1, 000ppm 30 minutes
1:10 1 part bleach + 9 parts water 0.5% 5,000ppm 10 minutes
** Dilution of household bleach containing 5% sodium hypochlorite with 50,000 parts per million (ppm) available
chlorine
In certain circumstances, a disinfectant which targets specific pathogens is appropriate to use on
environmental surfaces.
o For example, during an outbreak of norovirus, a disinfectant which is labelled as a broad-
spectrum virucide (able to deactivate or destroy viruses) against norovirus or non-enveloped
viruses (norovirus is a non-enveloped virus) would be effective for environmental surfaces
and non-critical equipment. For further discussion of non-critical equipment, see Section
7.5.2: Non-critical resident care equipment and personal care supplies.
o When C. difficile is suspected or confirmed, a sporicidal product should be used. Complete
guidance on cleaning and disinfection can be found in Best Practice Guidelines for the
Prevention & Management of Clostridium difficile Infection in Prehospital, Acute & Continuing
Care: https://IPAC.gov.ns.ca/sites/default/files/CDIBestPracticesGuidelinesFinal2013.pdf
Manufacturer’s instructions must to be followed in the use of any detergents and disinfectants. Some
disinfectants have the capacity to be able to both clean AND disinfect, whereby other disinfectants
(e.g. household bleach) need to have surfaces cleaned with a cleaning agent (e.g. soap and water,
detergent) prior to being disinfected.
The product must be compatible with the materials or surfaces it will be used on.
The Ontario Provincial Infectious Disease Advisory Committee (PIDAC) has developed a procedure for
the routine daily cleaning and disinfection of a resident’s room. This procedure is easily adaptable for
LTCFs. It has been reproduced here for your reference Sample Procedure for Routine Cleaning of a
Resident Room.

32
Figure 6: Sample Procedure for Routine Cleaning of a Resident Room (does not include
rooms on Additional Precautions)
1. Assessment
Check for Additional Precautions signs and follow the precautions indicated
Walk through room to determine what needs to be replaced (e.g., toilet paper, paper towels, soap,
alcohol-based hand rub (ABHR), gloves, sharps container) and whether any special materials are
required; this may be done before or during the cleaning process
2. Assemble supplies
Ensure an adequate supply of clean cloths is available
Prepare or use fresh disinfectant solution according to manufacturer’s instructions
3. Clean hands using ABHR and put on gloves
4. Clean room, working from clean to dirty and high to low areas of the room:
Use fresh cloth(s) for cleaning each resident bed space:
o if a bucket is used, do not ‘double-dip’ cloth(s)
o do not shake out cloth(s)
o change the cleaning cloth when it is no longer saturated with disinfectant and after cleaning
heavily soiled areas such as toilet and bedpan cleaner
o if there is more than one resident bed space in the room, use fresh cloth(s) for each and
complete the cleaning in each bed space before moving to the next
Start by cleaning doors, door handles, push plates and frequently touched areas of door frame
Check walls for visible soiling and clean if required
Clean light switches and thermostats
Clean wall mounted items such as alcohol-based hand rub dispenser and glove box holder
Check and remove fingerprints and soil from low level interior glass partitions, glass door panels,
mirrors and windows with glass cleaner
Check privacy curtains for visible soiling and replace if required.
Clean all furnishings and horizontal surfaces in the room including chairs, window sill, television,
telephone, computer keypads, night table and other tables or desks. Lift items to clean the tables. Pay
particular attention to high-touch surfaces
Wipe any equipment on walls (i.e. top of suction bottle, intercom, blood pressure manometer)
Clean bedrails, bed controls and call bell
Clean bathroom/shower in patient room
Clean floors
5. Disposal
Place soiled cloths in designated container for laundering
Check sharps container and change when ¾ full (do not dust the top of a sharps container)
Remove soiled linen if bag is full
Place obvious waste in receptacles
Remove waste
6. Remove gloves and clean hands with ABHR; if hands are visibly soiled, wash with soap and water. DO NOT
LEAVE ROOM WEARING SOILED GLOVES.
7. Replenish supplies as required (e.g., gloves, ABHR, soap, paper towel)
8. Clean hands with ABHR
33
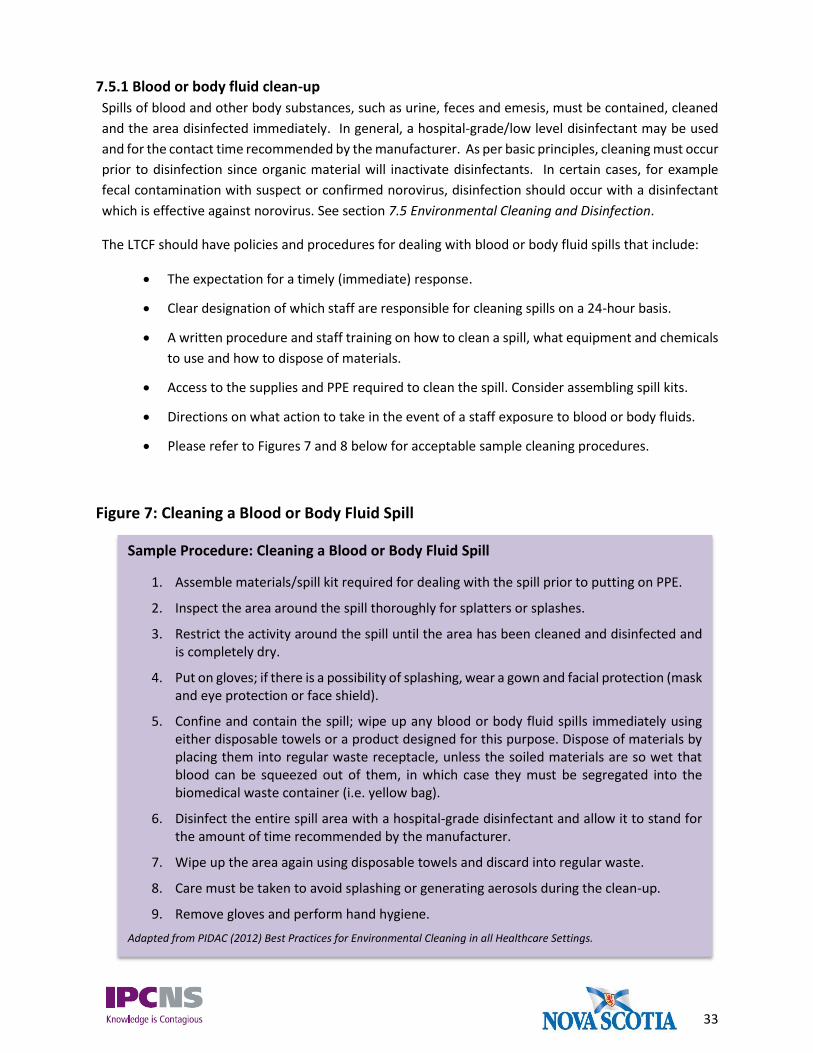
7.5.1 Blood or body fluid clean-up
Spills of blood and other body substances, such as urine, feces and emesis, must be contained, cleaned
and the area disinfected immediately. In general, a hospital-grade/low level disinfectant may be used
and for the contact time recommended by the manufacturer. As per basic principles, cleaning must occur
prior to disinfection since organic material will inactivate disinfectants. In certain cases, for example
fecal contamination with suspect or confirmed norovirus, disinfection should occur with a disinfectant
which is effective against norovirus. See section 7.5 Environmental Cleaning and Disinfection.
The LTCF should have policies and procedures for dealing with blood or body fluid spills that include:
The expectation for a timely (immediate) response.
Clear designation of which staff are responsible for cleaning spills on a 24-hour basis.
A written procedure and staff training on how to clean a spill, what equipment and chemicals
to use and how to dispose of materials.
Access to the supplies and PPE required to clean the spill. Consider assembling spill kits.
Directions on what action to take in the event of a staff exposure to blood or body fluids.
Please refer to Figures 7 and 8 below for acceptable sample cleaning procedures.
Figure 7: Cleaning a Blood or Body Fluid Spill
Sample Procedure: Cleaning a Blood or Body Fluid Spill
1. Assemble materials/spill kit required for dealing with the spill prior to putting on PPE.
2. Inspect the area around the spill thoroughly for splatters or splashes.
3. Restrict the activity around the spill until the area has been cleaned and disinfected and is completely dry.
4. Put on gloves; if there is a possibility of splashing, wear a gown and facial protection (mask and eye protection or face shield).
5. Confine and contain the spill; wipe up any blood or body fluid spills immediately using either disposable towels or a product designed for this purpose. Dispose of materials by placing them into regular waste receptacle, unless the soiled materials are so wet that blood can be squeezed out of them, in which case they must be segregated into the biomedical waste container (i.e. yellow bag).
6. Disinfect the entire spill area with a hospital-grade disinfectant and allow it to stand for the amount of time recommended by the manufacturer.
7. Wipe up the area again using disposable towels and discard into regular waste.
8. Care must be taken to avoid splashing or generating aerosols during the clean-up.
9. Remove gloves and perform hand hygiene.
Adapted from PIDAC (2012) Best Practices for Environmental Cleaning in all Healthcare Settings.

34
Figure 8: Cleaning a Blood or Body Fluid Spill on Carpet
7.6 NON-CRITICAL RESIDENT CARE EQUIPMENT AND PERSONAL CARE SUPPLIES Non-critical resident care equipment includes items such as stethoscopes, glucometers, blood pressure
cuffs and electronic thermometers which contact the resident’s intact skin or environmental surfaces.
Ideally, non-critical resident care equipment should be dedicated to an individual resident and
cleaned and disinfected according to a regular schedule.
Non-critical equipment should be cleaned and disinfected between uses on different residents.
There should be clear responsibility and accountability for routine cleaning and disinfection of
resident care equipment.
Bedpans and commodes pose a unique challenge in LTC. They carry a high-load of contamination
and must be handled carefully to prevent spread of infectious agents. Refer to the IPCNS SBAR
Guidelines for Management of Human Waste/Body Fluids in Long Term Care and Acute Care
Facilities, 2nd Edition for provincial recommendations on managing these items. This can be found
on the IPCNS website; https://ipc.gov.ns.ca/
Sample Procedure: Cleaning a Blood or Body Fluid Spill on Carpet
1. Assemble materials or collect spill kit required for dealing with the spill prior to putting
on PPE.
2. Restrict the activity around the spill until the area has been cleaned and disinfected and
is completely dry.
3. Put on gloves; if there is a possibility of splashing, wear a gown and facial protection
(mask and eye protection or face shield).
4. Mop up as much of the spill as possible using disposable towels.
5. Disinfect the entire spill area with a hospital-grade disinfectant and allow it to stand for
the amount of time recommended by the manufacturer.
6. Safely dispose of the cleanup materials and gloves by placing them in the waste
receptacle, unless the soiled materials are so wet that blood can be squeezed out of
them, in which case they must be segregated into the biomedical waste container (i.e.,
yellow bag).
7. Remove gloves and perform hand hygiene.
8. Arrange for the carpet to be cleaned with an industrial carpet cleaner as soon as
possible. Adapted from PIDAC (2012) Best Practices for Environmental Cleaning in all Healthcare Settings.

35
Increasingly, equipment or tools with electronic components are being used by clinicians.
Electronic equipment going from room to room should be cleaned and disinfected, however
electronic components may make this a challenge. Refer to the IPAC Canada Practice
Recommendations: Infection Prevention and Control Related to Electronic (IT) Devices in
Healthcare Settings for recommendations on how to manage these items. These are available
on-line at: http://www.ipac-canada.org/pdf/Electronic_Devices_Practice_Recommendations-
2012.pdf
Personal care supplies and toiletries which could contain blood or body fluids such as razors, nail
clippers, tooth brushes, creams in tubs or nippers are dedicated single-resident use. They should
be labelled and not shared with other residents. Individually purchased lotions and creams should
also be single-resident use and labelled with the resident’s name.
For lotions and creams supplied by the facility for multiple-resident use, products should be
dispensed in a manner that does not contaminate the remaining contents.
7.7 LINEN Soiled linen from healthcare settings should be handled as per Routine Practices.
Resident bed linen should be changed on a regular schedule and immediately if soiled, as well as
upon discontinuation of contact precautions and following resident discharge. Do not spray or
pre-rinse grossly soiled linens with water.
Soiled linen should be bagged or placed in a cart or receptacle at the point-of-care. If space allows,
receptacles should be placed inside the resident room. If space is limited, the location of the
receptacles placed in the hallway should be accessible for staff.
Soiled linen should be handled with a minimum of agitation to avoid contamination of air, surfaces
and persons.
Soiled linen should not be sorted and rinsed in resident care areas. Specialized personal items
and clothing may need to be carefully separated.
Heavily soiled linen should be rolled or folded to contain the heaviest soil in the centre of the
bundle. Large amounts of solid soil (e.g. feces) can be removed with a gloved hand and toilet
tissue and placed into a bedpan or toilet for flushing.
Hand hygiene should be performed after handling soiled linen.
Hand hygiene facilities with ABHR and/or a dedicated hand washing sink should be available in
the laundry area.
Clean linen should be transported and stored in a manner that prevents contamination and
maintains its cleanliness.
Clean and soiled linen should be separated during transport and storage.
36
Reusable linen bags should be washed after each use; they may be washed in the same cycle as
the linen contained in them.
Staff should not consume food or beverages in the laundry processing area.
7.8 SHARPS SAFETY AND PREVENTION OF EXPOSURE TO BLOODBORNE PATHOGENS A sharp is an item capable of penetrating or cutting the skin. Sharps include needles, lancets, blades,
sutures and clinical glass. Sharps pose a risk of cuts or punctures and potential transmission of bloodborne
pathogens if they are not handled safely.
Immediately dispose of needles and other single-use sharps after they are used into a designated-
puncture-resistant container that is easily accessible at the point-of-care.
Never recap needles.
Use safety-engineered sharps wherever possible as per the Safe Needles in Healthcare
Workplaces Act.
Cover open skin, lesions on hands or forearms with a dry dressing at all times while at work.
Occupational health should be consulted if hand hygiene is impeded by the dressing.
Do not over fill sharps containers. Remove the sharp container from use and seal when the fill line
has been reached.
Do not reach into sharps containers or any other waste containers.
Ensure all staff are aware of the procedure and follow-up required in the event of an occupational
sharps injury.
7.8.1 Injection Safety and Aseptic Technique
Transmission of Hepatitis B and Hepatitis C virus has been linked to the reuse of needles and/or syringes
used to withdraw agents from multiuse vials, inappropriate use of glucose monitoring equipment, and
reusing a single needle and syringe to administer medications to multiple residents (PHAC).
In order to inject medications safely, follow proper IPAC practices during the preparation and
administration of injectable medications and safe injection practices:
Perform hand hygiene at the point-of-care, prior to opening supplies, prior to putting on PPE as
well as at other moments in accordance with the 4 moments for hand hygiene. See Appendix E.
Prepare the resident’s skin with an appropriate antiseptic before performing an invasive
procedure.
Use alcohol to disinfect the rubber stopper or injection port of medication vials, infusion bags etc.
and wait for alcohol to dry prior to entering the port, vial or bag.
Use single-use sterile needles and syringes every time.

37
Always follow manufacturer’s instructions.
Do not administer medications from the same syringe to more than one resident, even if the
needle is changed.
Consider a syringe or needle to be contaminated after it has been used to enter or connect to a
resident’s intravenous infusion bag or administration set.
Do not enter a vial or bag/bottle with a used syringe or needle.
Do not use medications packaged as single-use vials for more than one resident.
Assign medications packaged as multi-use vials to a single resident whenever possible.
Do not administer medications or solutions from single-dose vials, ampules or syringes to multiple
residents and do not combine leftover contents for later use.
Use single-dose medication vials, prefilled syringes and ampules in clinical settings. If the product
is only available as multi-dose vial, see Section 7.6.2 Multi-dose Vials.
Use a sterile, single-use disposable needle and syringe for each medication/fluid withdrawal from
vials or ampules.
Use skin antisepsis and single-use disposable needles for lancets, blood sampling devices and
acupuncture.
7.8.2 Multi-dose Vials
When a product is only available for purchase in multi-dose vials, adhere to the following:
Restrict the multi-does vial to single resident use whenever possible.
Prepare syringes from multi-dose vials from a centralized medication preparation area (do not
take a multi-dose vial to the bedside).
Store multi-dose vials in a secure restricted access location away from the resident area, for
example, in a medication room or locked cart, and in accordance with manufacturer’s
recommendations.
Use a sterile, single-use needle and syringe each time the multi-dose vial is entered.
Never enter a multi-dose vial with a previously used needle or syringe.
Label the multi-dose vial with the date of first opening.
Discard the multi-dose vial according to the manufacturer’s expiry date or organizational policy,
whichever is shorter.
38
Inspect the multi-dose vial for clouding or particulate contamination prior to each use and
discarded it if clouding or particulate contamination is present.
Discard the multi-dose vial if sterility or product integrity is compromised.
7.8.3 Glucose Monitoring
Glucose monitoring is a procedure which is commonly performed in LTCFs which carries a risk for
transmission of infection of bloodborne pathogens if proper IPAC procedures are not followed.
Single-use, auto-disabling finger-stick blood sampling devices are preferred in LTCF. If multi-use
blood sampling devices (glucose sampling devices, fingerstick blood sampling devices) are used,
they must be used for only one resident. The lancet must be removed and replaced with a new
lancet for every use, even on the same resident.
Assign glucometers to individual residents and clean and disinfect between uses. If it is not
feasible to assign glucometers to individual residents, they should be cleaned and disinfected
according to manufacturer’s instructions, before use with another resident and Routine Practices
should be followed.
Ensure hands are cleaned and gloves are changed between each resident’s glucose monitoring.
7.9 PET THERAPY AND ANIMAL VISITATION Many LTCFs keep pets/residential animals for the comfort of their residents. While pets may be of
therapeutic value, they may also be the source of pathogenic organisms. Accordingly, where there are
pets in the facility, certain precautions should be taken regarding their care and housing.
Pets/Residential Animals
Pets are limited to domestic companion animals that are household pets (i.e. caged birds, cats,
dogs, fish).
Pets should be properly vaccinated.
Pets should be examined annually by a veterinarian and found to be free of diseases that could
be transmitted to staff or residents.
The facility has a designated individual(s) responsible for the personal needs of residential
animals.
Pets should be house (litter) trained.
Litter boxes should be the covered variety and be cleaned daily. Staff should wear gloves and
perform hand hygiene after cleaning litter boxes/pet excreta. A litter box should be located in a
suitable place. Places not suitable include soiled utility room, dining areas, food prep areas,
clean storage areas.
Pets must be provided with its own place for sleeping or eating.
Pets are not permitted in the clean storage areas, kitchen, kitchenette or dining room.

39
Residents and staff should perform hand hygiene before and after handling animals.
Animal Visitation
Animal visitation may include therapeutic animals (trained and certified for animal-assisted
therapy) or visiting animals.
LTCFs should have a policy and procedure governing animal visitation. This should be reviewed
and updated annually. The animal visitation policy should include:
o Acceptable animals for inclusion.
o Exclusion of unsuitable or restricted animals (e.g. reptiles, rodents, primates, farm
animals).
o Vaccination/veterinary and general health requirements for the animals.
o Criteria for visitation during an outbreak.
o Animal handler requirements including; self-screening for signs and symptoms of
communicable illness, hand hygiene, control of the animal (leash/carrying case).
o Protocols for visiting personal family pets.
NOTE: These guidelines do not apply to working animals.

40
8. Additional Precautions
Additional Precautions are based on the mode of transmission of
the suspected or confirmed infectious agent and must be instituted
as soon as symptoms which indicate an infection are observed.
There are three types of Additional Precautions: Contact
Precautions, Droplet Precautions and Airborne Precautions. The
transmission of certain infectious agents may require that two
types of Additional Precautions, such as contact and droplet
precautions, be used together. A PCRA helps the HCW to
determine the need for Additional Precautions in addition to
Routine Practices.
What is the difference between Routine Practices and Additional
Precautions?
Routine Practices and Additional Precautions share the same
elements, for example the use of PPE, a point-of-care risk
assessment and diligent attention to hand hygiene. Additional
Precautions provide an added level of protection for the cases in
which a disease or specific signs and symptoms of a disease have
been recognized by defining the required PPE, accommodation,
cleaning, activity modifications, signage and communication.
Additional Precautions are more restrictive and more prescriptive
than Routine Practices; a PCRA is still required for each resident
interaction.
Implementing Additional Precautions
Additional Precautions should be implemented as soon as
infectious disease or risk factors are suspected. A confirmed
diagnosis is not necessary for Additional Precautions to be started.
The LTCF should have clear policy and guidelines about who may
initiate Additional Precautions, and a plan to quickly communicate
that Additional Precautions have been implemented to the
infection control designate and others who need to know. As well,
increased surveillance for other residents and roommates should
occur as this could be indicative of an outbreak.
‘Additional Precautions are
enhanced IPAC
interventions used in
addition to Routine
Practices when Routine
practices also may not
interrupt transmission of an
infectious agent.
Additional Precautions are
based on the method of
transmission and applied
for specific clinical
presentations or
syndromes and pathogens.’
Source: Routine Practices and
Additional Precautions for Preventing the Transmission of Infection in Healthcare Settings,
PHAC
ADDITIONAL PRECAUTIONS

41
Examples of Syndromes requiring Additional Precautions:
Residents will display symptoms of an infection prior to a lab confirmation and, for this reason, it is
imperative to implement Additional Precautions at the onset of symptoms. Residents with an infectious
disease often present in the same way as younger patients do. However many elderly present with non-
specific clinical symptoms and non-specific functional decline. This makes an accurate assessment difficult
and may lead to a life-threatening delay of diagnosis and therapy. In older residents with unexplained
functional decline, healthcare providers should be aware of the possibility of a serious infection.
If Additional Precautions are delayed until a lab specimen is collected and confirmed, HCWs, other
residents and visitors will already have been exposed to a potentially infectious disease.
Examples of syndromes which require Additional Precautions include:
Abscesses or draining wounds not contained by a dressing.
A rash suggestive of chicken pox or measles.
Signs of an acute respiratory infection such as fever and new or worsening cough. Elderly people
and people who are immunocompromised may not have a febrile response to a respiratory
infection
Signs of an acute gastrointestinal infection including diarrhea and/or vomiting.
Risk factors and symptoms suggestive of active tuberculosis.
Signs of bacterial meningitis including a petechial/purpural rash with fever.
Discontinuing Additional Precautions
Additional Precautions should only be discontinued following consultation with the infection control
practitioner or their designate. Refer to Routine Practices and Additional Precautions for Preventing the
Transmission of Infection in Healthcare Settings in Part C: Transmission Characteristics and Precautions
by the Public Health Agency of Canada, for recommendations about discontinuing additional precautions
based on the confirmed or suspect infectious agent or clinical syndrome.
For outbreaks of notifiable diseases and conditions (as per It’s the Law Reporting Notifiable Diseases and
Conditions, link: http://novascotia.ca/dhw/cdpc/documents/06026_ItsTheLawPoster_En.pdf ), the
facility must work with public health to determine when to declare the outbreak over and discontinue
precautions.
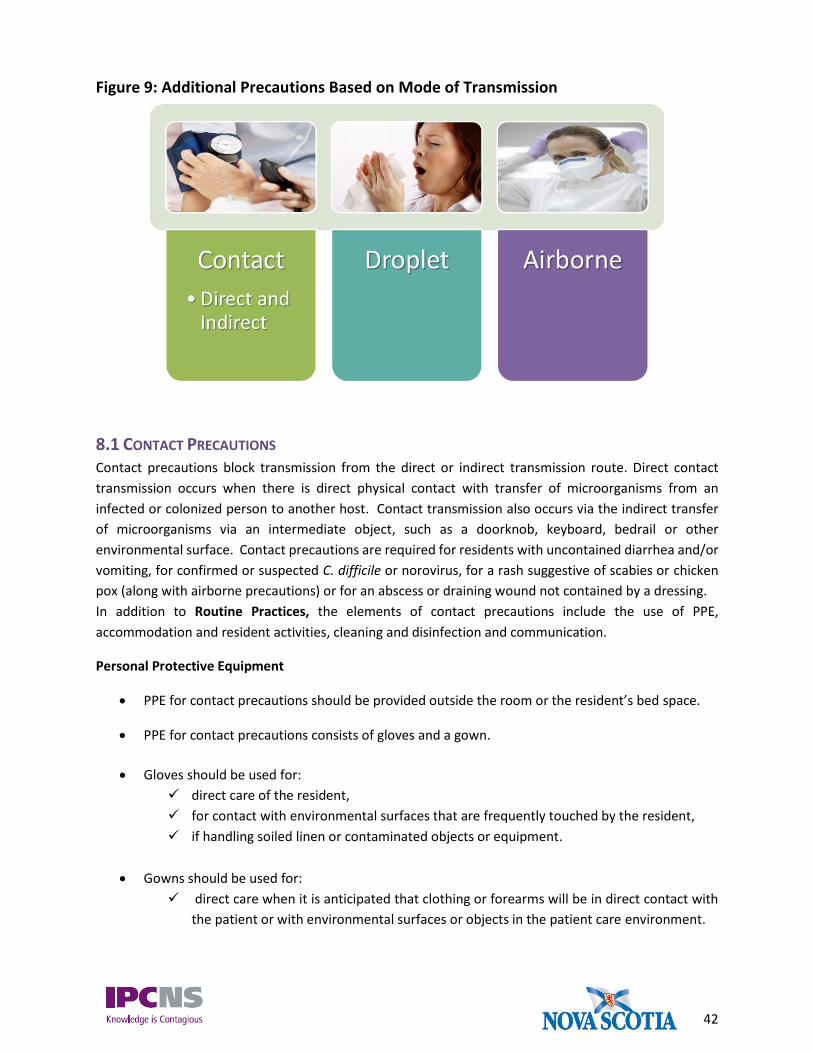
42
Figure 9: Additional Precautions Based on Mode of Transmission
8.1 CONTACT PRECAUTIONS Contact precautions block transmission from the direct or indirect transmission route. Direct contact
transmission occurs when there is direct physical contact with transfer of microorganisms from an
infected or colonized person to another host. Contact transmission also occurs via the indirect transfer
of microorganisms via an intermediate object, such as a doorknob, keyboard, bedrail or other
environmental surface. Contact precautions are required for residents with uncontained diarrhea and/or
vomiting, for confirmed or suspected C. difficile or norovirus, for a rash suggestive of scabies or chicken
pox (along with airborne precautions) or for an abscess or draining wound not contained by a dressing.
In addition to Routine Practices, the elements of contact precautions include the use of PPE,
accommodation and resident activities, cleaning and disinfection and communication.
Personal Protective Equipment
PPE for contact precautions should be provided outside the room or the resident’s bed space.
PPE for contact precautions consists of gloves and a gown.
Gloves should be used for:
direct care of the resident,
for contact with environmental surfaces that are frequently touched by the resident,
if handling soiled linen or contaminated objects or equipment.
Gowns should be used for:
direct care when it is anticipated that clothing or forearms will be in direct contact with
the patient or with environmental surfaces or objects in the patient care environment.
43
Hand hygiene must occur before gloves and a gown are put on.
Gloves and gown must be removed and discarded into a hands-free waste receptacle and hand
hygiene performed following the activity for which they were used or upon exiting the resident’s
room or designated bedspace.
The same PPE is not to be worn for more than one resident. If caring for more than one resident
in a shared room, PPE must be changed and hand hygiene performed between contacts with each
resident/bedspace in the same room.
Resident Accommodation and Activities
Residents should remain in their rooms and not participate in group activities while symptomatic.
Asymptomatic or colonized residents on contact precautions should not be excluded from group
activities. For example, residents colonized with MRSA or VRE.
Residents should perform hand hygiene or be assisted as necessary before leaving their room or
participating in group activities (for asymptomatic and colonized residents).
The door to the resident’s room can remain open.
Regular dishes and cutlery are acceptable.
In a shared room, a resident with diarrhea should not share a toilet with another resident. A
designated toilet or commode should be assigned to the resident with diarrhea. Disposal of
human waste from a commode or bedpan occurs in the soiled utility room in a hopper or through
a commercial flusher/disinfector.
Placement of residents requiring contact precautions should be reviewed on a case-by-case basis.
Infection risk to other occupants of the room must be considered when selecting roommates.
Given that cohorting of residents is not generally practical in LTC, assigning staff members to care
only for residents affected with the same signs and symptoms should be considered (cohort
nursing).
When transfer or movement is necessary, the resident should be provided with clean bedclothes
and bedding, draining wounds should be contained with clean dressings, infected areas of the
resident’s body should be covered and body substances should be contained.
Personnel in the area to which the resident is to be transported or EHS staff should be informed
of precautions to follow and requested to see the resident efficiently to minimize time in waiting
areas and reduce time spent outside of the resident room.
Care and services (e.g., appointments at foot care clinics, volunteer visiting and volunteer
transportation) that are not medically necessary should be postponed until residents are
asymptomatic.
44
Cleaning and Disinfection of Resident Environment & Equipment
In general, for most residents on contact precautions, routine cleaning & disinfection is acceptable
with attention to high touch surfaces. Please see Section 7.5 Cleaning and Disinfection for details.
o Enhanced environmental cleaning procedures and/or frequencies are required for
residents with VRE, C. difficile or norovirus.
Equipment should be dedicated to the resident.
Equipment must be cleaned and disinfected prior to use on another resident.
When cleaning, attention should be paid to high-touch surfaces in the room as well as all items
within the immediate vicinity of the resident.
Contact precautions should be discontinued only after the room/bed space and bathroom have
been cleaned and disinfected by a discharge or terminal clean. This includes paying special
attention to items that have been in direct contact with the patient or in contact with the patient’s
excretions, secretions, blood or body fluids.
All disposable items in the patient’s room should be discarded.
Reusable items in the room should be reprocessed as appropriate to the item.
Bedside tables, bedrails, mattress covers and all horizontal surfaces in the room should
be cleaned with a detergent/disinfectant.
Privacy and shower curtains should be changed.
Communication and Visitors
A mechanism to notify that a resident requires Contact Precautions should be visible on the
resident’s door or in the resident’s bed space that indicates the resident needs additional
precautions. This may include signage or another recognized communication cue for staff or
visitors. Any signage used should not disclose the resident’s confirmed or suspect diagnosis.
Residents, their visitors and families should be educated about the precautions being used, the
duration of precautions, as well as the prevention of transmission of disease to others with a
particular focus on hand hygiene.
Visitors who assist with resident care should use the same PPE as HCWs.
Visitors should be instructed to speak with a nurse before entering the resident room in order to
evaluate the risk to the health of the visitor, and the ability of the visitor to comply with
precautions.
45
Visitors should be restricted to visiting only one resident. If the visitor must visit more than one
resident, the visitor should visit the resident on contact precautions last. The visitor must adhere
to the PPE instructions for staff and perform hand hygiene.
8.2 DROPLET PRECAUTIONS Droplet precautions are used to protect the mucous membranes of the eyes, nose and mouth from
contamination by infectious agents which can be transmitted on large respiratory droplets. Pathogens
that can be transmitted by the droplet route commonly include; meningococcal disease, influenza,
mumps, Mycoplasma pneumonia and pertussis.
Droplet precautions are required for care of residents with symptoms of a droplet spread infection, when
within two metres of any resident who is experiencing new respiratory symptoms (cough), or if performing
procedures that may result in coughing by the resident.
Personal Protective Equipment
PPE for droplet precautions should be provided outside the room or the resident’s bedspace.
PPE for droplet precautions consists of facial protection and hand hygiene.
Facial protection (a surgical mask and protective eyewear/goggles) must be worn to provide direct
care and within 2 metres/6 feet of the resident on droplet precautions.
After resident interaction, facial protection should be removed at the doorway of the resident’s
room in a waste receptacle. If reusable googles are used, they should be placed in a labelled
container at the exit of the room indicating they requiring cleaning and disinfection before re-use.
Hand hygiene must be performed before contact with the resident/resident environment and
after PPE is removed.
For care of residents with rubella or mumps, facial protection may not needed if the HCW is
immune. However, consideration must be given to applying facial protection under Routine
Practices for any resident with respiratory symptoms (e.g. coughing, sneezing). Non-immune
personnel (rubella, mumps) should not enter the room unless it is essential, at which time facial
protection should be worn.
Resident Accommodation and Activities
The resident should remain in their room or bed space and not participate in group activities while
symptomatic.
The door to the resident’s room can remain open.
Maintain a two metre separation from others and draw the privacy curtain if in a shared room.

46
Placement of residents requiring droplet precautions should be reviewed on a case-by-case basis.
Infection risks to other patients in the room and available alternatives should be considered.
When transfer or movement outside of the room is necessary, the resident should wear a mask if
tolerated and perform hand hygiene. A two metre separation should be maintained between the
resident and unprotected people (e.g. other residents).
Personnel in the area to which the resident is to be transported should be informed of precautions
to follow and requested to see the resident efficiently to minimize time in waiting areas and
reduce time spent outside of the resident room.
Cleaning and Disinfection of Resident Environment and Equipment
Routine cleaning and disinfection is acceptable with attention to high touch surfaces for rooms
under droplet precautions. Microorganisms spread through the droplet route only do not have
the capacity to contaminate or spread through the contact route as they are unable to survive on
environmental surfaces. Please see Section 7.5 Cleaning and Disinfection for cleaning and
disinfection guidance.
Staff performing housekeeping responsibilities must wear facial protection when working within
two metres of a resident on droplet precautions.
Equipment should be dedicated to the resident where possible.
Equipment should be cleaned and disinfected prior to use on another resident.

47
Communication and Visitors
A mechanism to notify that a resident requires Droplet Precautions should be visible on the
resident’s door or in the resident’s bed space that indicates the resident needs additional
precautions. This may include signage or another recognized communication cue for staff or
visitors. Any signage used should not disclose the resident’s confirmed or suspect diagnosis.
Residents, their visitors and families should be educated about the precautions being used, the
duration of precautions, as well as the prevention of transmission of disease to others with a
particular focus on hand hygiene.
Visitors who assist with resident care should use the same PPE as HCWs.
Visitors should be instructed to speak with a nurse before entering the resident room in order to
evaluate the risk to the health of the visitor, and the ability of the visitor to comply with
precautions.
Visitors should visit only one resident. If the visitor must visit more than one resident, the visitor
should visit the resident on droplet precautions last.
Visitors should wear facial protection when within 2 meters of the resident. Visitors should
receive education regarding hand hygiene.
8.3 DROPLET/CONTACT PRECAUTIONS Many respiratory viruses, including influenza, adenovirus, coronavirus, human metapneumovirus,
parainfluenza virus, respiratory syncytial virus and rhinovirus may be transmitted through both the
droplet and indirect contact routes of transmission. For such agents, both droplet and contact precautions
are needed.
Personal Protective Equipment
PPE needed for residents on droplet/contact precautions includes all of the equipment required
for both droplet and contact transmission protection and includes gowns, gloves and facial
protection.
Resident Accommodation and Activities
The same considerations as per contact precautions and droplet precautions.
The resident should remain in their room or bed space while symptomatic.
Participation in group activities should be restricted while the resident is symptomatic.

48
The resident should wear a mask (if tolerated) within two metres of other residents while
symptomatic and perform hand hygiene if he or she needs to leave the room.
The door to the resident’s room can remain open.
Maintain a two metre separation from others and draw the privacy curtain if in a shared room.
In LTC, a PCRA should be performed to determine resident placement. Given that cohorting
residents may not be practical in LTCFs, assigning staff members to care only for residents affected
with the same signs and symptoms should be considered (cohort staffing).
Care and services (e.g., appointments at foot care clinics, volunteer visiting and volunteer
transportation) that are not medically necessary should be postponed until residents are
asymptomatic.
Cleaning and Disinfection of Resident Environment and Equipment
When cleaning and disinfecting, attention should be paid to high-touch items in the room as well
as all items within the immediate vicinity of the client/patient/resident.
Equipment should be dedicated to the resident and if this is not possible, it should be cleaned and
disinfected with a hospital-grade disinfectant between uses on different residents.
Staff performing environmental cleaning duties (e.g. housekeeping, support staff) should wear
facial protection when working within two metres of a resident on droplet/contact precautions.
Many viral respiratory pathogens including influenza, survive on environmental surfaces, thus
increased environmental cleaning is prudent for rooms under droplet/contact precautions.
Communication and Visitors
A mechanism to notify that a resident requires Droplet/Contact Precautions should be visible on
the resident’s door or in the resident’s bed space that indicates the resident needs additional
precautions. This may include signage or another recognized communication cue for staff or
visitors. Any signage used should not disclose the resident’s confirmed or suspect diagnosis.
Residents, their visitors, families and their decision-makers should be educated about the
precautions being used, the duration of precautions, as well as the prevention of transmission of
disease to others with a particular focus on hand hygiene.
o Visitors should receive education regarding hand hygiene. Facial protection should be
worn by visitors within two meters of the resident and gowns and gloves if providing
direct care.
Visitors should be instructed to speak with a nurse before entering the resident room in order to
evaluate the risk to the health of the visitor and the ability of the visitor to comply with
precautions.

49
Visitors should visit only one resident. If the visitor must visit more than one resident, the visitor
should visit the resident on droplet and contact precautions last.
8.4 AIRBORNE PRECAUTIONS Airborne precautions should be implemented in addition to Routine Practices for residents who are
suspected to have an illness transmitted through the airborne route such as suspect or confirmed
pulmonary or laryngeal tuberculosis, varicella (chickenpox) or disseminated herpes zoster, and measles.
Airborne precautions may also be recommended or required for new or emerging respiratory pathogens
for which transmission characteristics are not yet known.
Airborne precautions consist of control of air flow through special ventilation systems (negative pressure
rooms) and the use of respirators by HCWs.
Quick isolation in an appropriate environment and rapid diagnosis will assist in preventing transmission
of airborne infections to others. For measles and varicella, immunization is the primary means of control.
NOTE: It is recognized that most LTCFs in NS will not have access to negative pressure isolation rooms
in their facilities. In the event a resident requires airborne precautions, a timely assessment should be
completed to discuss plan of care. This evaluation should include exposure and risk to other residents,
consultation with the local public health officials, and possible transfer to a facility (acute care or
alternate LTCF) with the ability to provide airborne isolation accommodations.
Immunization/Infection Status
Immunization is an effective control measure to protect against varicella and measles. All staff
should have documented vaccination or immunity against these viruses.
The tuberculosis infection status of residents should be determined at the time of admission. For
recommendations on tuberculosis screening for new residents to LTCFs, refer to the guidance for
Tuberculosis Screening for New Residents to LTCFs In Nova Scotia in the following table:
Figure 10: Tuberculosis Screening for New Residents
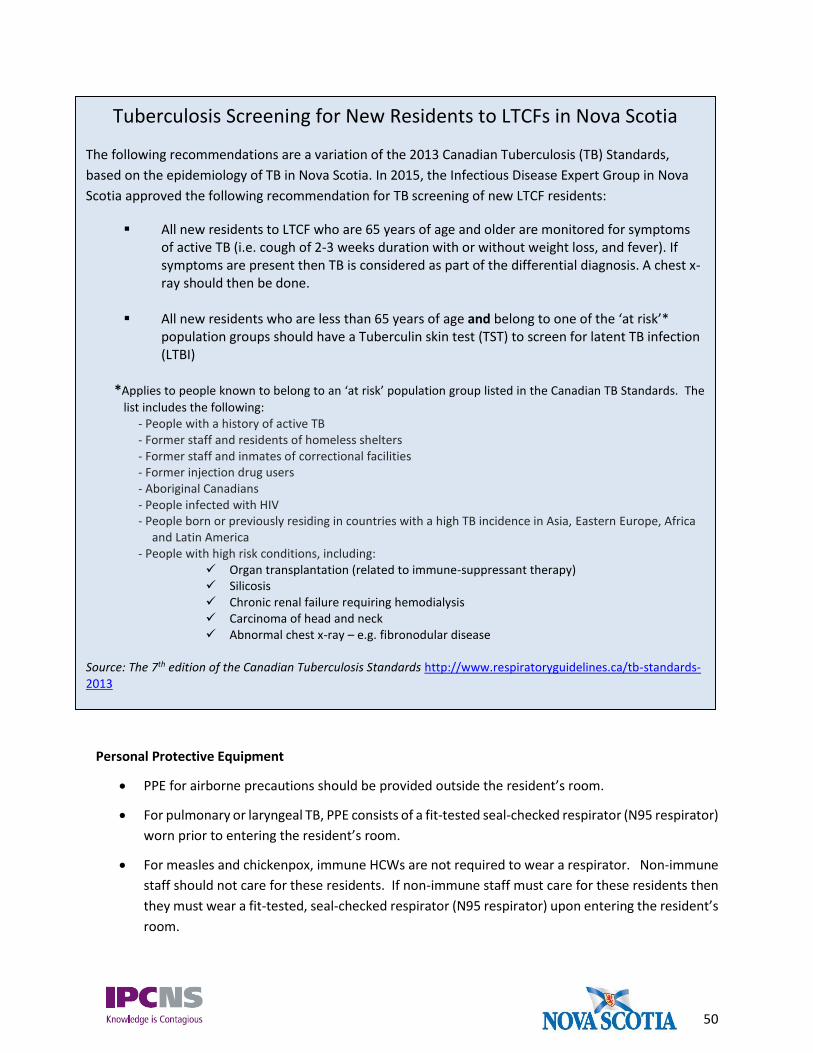
50
Personal Protective Equipment
PPE for airborne precautions should be provided outside the resident’s room.
For pulmonary or laryngeal TB, PPE consists of a fit-tested seal-checked respirator (N95 respirator)
worn prior to entering the resident’s room.
For measles and chickenpox, immune HCWs are not required to wear a respirator. Non-immune
staff should not care for these residents. If non-immune staff must care for these residents then
they must wear a fit-tested, seal-checked respirator (N95 respirator) upon entering the resident’s
room.
Tuberculosis Screening for New Residents to LTCFs in Nova Scotia
The following recommendations are a variation of the 2013 Canadian Tuberculosis (TB) Standards,
based on the epidemiology of TB in Nova Scotia. In 2015, the Infectious Disease Expert Group in Nova
Scotia approved the following recommendation for TB screening of new LTCF residents:
All new residents to LTCF who are 65 years of age and older are monitored for symptoms of active TB (i.e. cough of 2-3 weeks duration with or without weight loss, and fever). If symptoms are present then TB is considered as part of the differential diagnosis. A chest x-ray should then be done.
All new residents who are less than 65 years of age and belong to one of the ‘at risk’*
population groups should have a Tuberculin skin test (TST) to screen for latent TB infection (LTBI)
*Applies to people known to belong to an ‘at risk’ population group listed in the Canadian TB Standards. The
list includes the following: - People with a history of active TB - Former staff and residents of homeless shelters - Former staff and inmates of correctional facilities - Former injection drug users - Aboriginal Canadians - People infected with HIV - People born or previously residing in countries with a high TB incidence in Asia, Eastern Europe, Africa
and Latin America - People with high risk conditions, including:
Organ transplantation (related to immune-suppressant therapy) Silicosis Chronic renal failure requiring hemodialysis Carcinoma of head and neck Abnormal chest x-ray – e.g. fibronodular disease
Source: The 7th edition of the Canadian Tuberculosis Standards http://www.respiratoryguidelines.ca/tb-standards-2013

51
Some diseases require both airborne and contact precautions. This includes disseminated herpes
zoster and herpes zoster in immunocompromised residents.
Resident Accommodation and Activities
If an airborne infection isolation room is not available in the LTCF, the resident should be
transferred to a facility equipped to manage airborne infections.
Residents should be placed on airborne precautions, in an airborne infection isolation room (if
available) and not participate in group activities. This refers to placement in a single room with
air handling and negative pressure ventilation in accordance with Canadian Standards Association
(CSA) standards.
If transfer is delayed or not possible, place the patient in a single room with the door closed,
preferably without recirculation of air from the room and as far away from the rooms of other
patients as possible and limit the number of people entering the room (e.g., no non-essential
visitors)
Residents on airborne precautions should remain in the airborne infection isolation room unless
required to leave for medically essential procedures.
The door to the room must be kept closed, even if the resident is not in the room.
In the case of varicella, measles or disseminated herpes zoster, if all personnel and all other
residents in the facility are immune and if non-immune visitors can be excluded, then transfer to
a facility with an airborne infection isolation room may not be essential.
When transfer or movement outside of the room is necessary, residents suspected or confirmed
to have an airborne infection should wear a surgical mask at all times, if medically tolerated. A
mask is effective in trapping the large infectious particles expelled by coughing residents.
Residents must not wear N95 respirators.
If the resident cannot wear a mask, transport should be planned to limit the exposure of other
individuals (e.g., no waiting in the reception areas) and it should be communicated to
receiving/transferring personnel that airborne precautions need to be maintained.
Cleaning and Disinfection of Resident Environment
Routine cleaning is acceptable. Please see Section 7.5 Cleaning and Disinfection for details.
After resident transfer or discharge, the door must be kept closed and the airborne precautions
sign must remain on the door until sufficient time has elapsed to allow removal of aerosolized
droplet nuclei (dependent on air changes per hour) before housekeeping performs terminal
cleaning.
Air exchanges per hour Minutes Required for removal of airborne microorganisms

52
(Canadian Tuberculosis Standards, 7th edition, http://www.respiratoryguidelines.ca/tb-standards-2013)
It is unlikely that a resident with active TB would remain in a LTCF for an extended period of time,
however, environmental services staff entering a room on airborne precautions for tuberculosis,
must wear a fit-tested and seal-checked N95 respirator.
The N95 respirator should remain on until leaving the room and closing the door.
Communication and Visitors
A mechanism to notify that a resident requires Airborne Precautions should be visible on the
resident’s door or in the resident’s bed space that indicates the resident needs additional
precautions. This may include signage or another recognized communication cue for staff or
visitors. Any signage used should not disclose the resident’s confirmed or suspect diagnosis.
Visitors should be restricted to essential visitors and those that are immune.
If a visit is deemed essential, all visitors for a resident with tuberculosis or non-immune visitors in
the case of varicella or measles should undergo a risk assessment, including public health
consultation, to determine respiratory protection needs prior to being able to visit.
Visitors should be instructed to speak with a nurse before entering the resident’s room.
Visitors should be screened for acute infection prior to visiting.
For new or emerging respiratory infections
For novel influenza viruses or new or emerging respiratory pathogens, recommendations and
requirements will be provided by PHAC and/or the DHW.
99% removal 99.9% removal
2 138 207
4 69 104
6 46 69
12 23 35
15 18 28
20 14 21
50 6 8

53
9. Surveillance A surveillance system in a LTCF forms an integral part of an IPAC program aimed at reducing healthcare-associated infections. As a first step in the planning of a surveillance system, the LTCF should assess the:
Types of residents that it serves;
Key medical interventions and procedures that they undergo; and
Types of infections for which they are most at risk.
This assessment is done to establish priorities for the surveillance system.
Best practice guidelines for surveillance programs have been published by the Provincial Infections
Disease Advisory Committee (PIDAC) in the Best Practices for Surveillance of Health Care-associated
Infections in Patient and Resident Populations (2014), 3rd edition. LTCFs can use this document for
assistance in establishing, assessing and/or evaluating their surveillance program.
LTCFs should ensure they follow validated, standardized case definitions for healthcare-associated
infection when conducting surveillance. Case definitions were developed by McGeer et al. at a 1991
Canadian Consensus Conference for use in LTCFs. These definitions were developed, taking into account
the unique limitations of LTC surveillance (e.g., lack of radiology and microbiology data). These 1991
definitions have subsequently been reviewed, updated and published in Surveillance Definitions of
Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria by Stone et al (2012). This
publication can be found online through the journal of Infection Control and Hospital Epidemiology
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3538836/. When choosing case definitions, LTCFs must
also ensure they are consistent with the definitions established through Public Health Services in the
Communicable Disease Prevention and Control Manual which can be found at:
http://novascotia.ca/dhw/cdpc/cdc/
While it is recognized that all LTCFs may have challenges in establishing robust surveillance programs,
recommended best practice is to incorporate the case definitions into surveillance programs in the LTCF
whenever possible.
Consideration for inclusion of infections into LTCF surveillance programs include the following:
1) Upper and Lower Respiratory Tract Infections (including Influenza-like illness)
2) Pneumonia
3) Urinary Tract Infections
4) Skin and Soft Tissue Infections
5) Gastrointestinal Infection (e.g. gastroenteritis, norovirus and Clostridium difficile infection)
6) Primary Bloodstream Infections
7) Viral Conjunctivitis
Additional targeted surveillance initiatives should be based on local epidemiology and as requested.
54
10. Outbreaks
LTCFs should have written policies and procedures for managing outbreaks. These policies and
procedures should include mitigation strategies such as the formation of a multidisciplinary outbreak
team, lines of communication, staff and resident education, review of environmental and equipment
cleaning practices, review and audit of infection prevention and control strategies such as hand hygiene
adherence monitoring and environmental cleaning.
a. All suspected outbreaks are reported to the local Public Health office as per legislative
requirements under ‘It’s The Law: Reporting Notifiable Diseases and Conditions’.
Available at: http://novascotia.ca/dhw/cdpc/documents/06026_ItsTheLawPoster_En.pdf
b. Efforts to identify the source of the outbreak should be done through a comprehensive
investigation and review.
c. The multidisciplinary team with expertise in outbreak management should assist in determining
the course of action for resident admissions or transfers, resident activities, cancellations/delay
of non-essential service, and internal and external communication.
d. There should be regular communication between the facility and Public Health to monitor the
progress of the outbreak and to determine when it is over. The authority to declare an outbreak
over is under direction of the zone Medical Officer of Heath. This should be done in
collaboration with the outbreak management team of the facility, including the director of care,
medical director, infection control practitioner or designate.
e. An outbreak report, which includes lessons learned, should be completed and submitted by the
Outbreak Management team of the LTCF. The report should be shared with the senior leadership
team, the LTCF Infection Prevention and Control Committee or designated committee, and the
zone Medical Officer of Health, as requested.
Respiratory Outbreaks
For guidance in dealing with respiratory outbreaks in LTC, including influenza outbreaks, please refer to
the document Guide to Influenza Outbreak Control for Long-Term Care Facilities and Adult Residential
Centres for reporting and management guidelines. This document is updated annually and located on the
Department of Health and Wellness Communicable Disease Prevention and Control webpage at
http://novascotia.ca/dhw/cdpc/info-for-professionals.asp.
Gastrointestinal Outbreaks
Any suspected outbreaks of gastrointestinal illness must be reported immediately to local public health
office as per It’s The Law: Reporting Notifiable Diseases and Conditions.

55
11. Clostridium difficile Infections
For guidance on IPAC for Clostridium difficile in your facility including accommodation, cleaning and
Additional Precautions, please refer to the document: Best Practice Guidelines for the Prevention &
Management of Clostridium difficile Infection in Prehospital, Acute & Continuing Care, available at:
https://IPAC.gov.ns.ca/sites/default/files/CDIBestPracticesGuidelinesFinal2013.pdf
12. Antibiotic Resistant Organisms For guidance on IPAC management of Antibiotic Resistant Organisms (AROs) in your facility, including
accommodation, cleaning, Additional Precautions etc. please refer to Best Practice Guidelines for
Reducing Transmission of Antibiotic Resistant Organisms (AROs) In Acute & Long Term Care Settings, Home
Care & Prehospital Care (March 2012): https://ipc.gov.ns.ca/standards-and-practice-guidelines

56
13. References
1. Alberta Health Services (2014). Infection Prevention and Control Practice Scenarios Continuing Care
http://www.albertahealthservices.ca/9237.asp
2. Canadian Thoracic Society and the Public Health Agency of Canada. Canadian Tuberculosis Standards,
7th Edition 2013. Her Majesty the Queen in Right of Canada; February, 2014.
http://www.respiratoryguidelines.ca/sites/all/files/Canadian_TB_Standards_7th_Edition_ENG.pdf
3. Infection Prevention and Control Canada (2014). http://www.ipac-
canada.org/links_handhygiene.php
4. Infection Prevention and Control Canada (2012). Infection Prevention and Control Related to
Electronic (IT) Devices in Healthcare Settings for recommendations on how to manage these items.
http://www.ipac-canada.org/pdf/Electronic_Devices_Practice_Recommendations-2012.pdf
5. Nova Scotia Food Safety Regulations (Nova Scotia) Section 105 of the Health Protection Act S.N.S.
2004, c. 4 (Canada). Available at: http://www.novascotia.ca/just/regulations/regs/hpafdsaf.htm
6. Nova Scotia Department of Agriculture. Nova Scotia Food Retail and Food Services Code. January,
2011.
7. Nova Scotia Department of Health and Wellness. It’s the Law Reporting Notifiable Diseases and
Conditions. Available at: http://novascotia.ca/dhw/cdpc/documents/06026_ItsTheLawPoster_En.pdf
8. Occupational Safety General Regulations. (Nova Scotia) Section 82 of the Occupational Health and
Safety Act S.N.S. 1996, c. 7 (Canada). Available at:
http://www.novascotia.ca/just/regulations/regs/ohsgensf.htm
9. Ontario Agency for Health Protection and Promotion, Provincial Infectious Diseases Advisory
Committee. Routine Practices and Additional Precautions in All Health Care Settings. 3rd edition.
Toronto, ON: Queen’s Printer for Ontario; November 2012.
10. Ontario Agency for Health Protection and Promotion, Provincial Infectious Diseases Advisory
Committee. Best Practices for Environmental Cleaning for Prevention and Control of Infections in All
Health Care Settings. 2nd Revision. Toronto, ON: Queen’s Printer for Ontario; 2012.
11. Peel Public Health. Take Control Prevent Infection, a Guide to Infection Prevention and Control in
Long–Term Care Homes. 2013. Available at: http://www.peelregion.ca/health/discon/htmfiles/take-
control/
12. Public Health Agency of Canada, Infectious Disease Prevention and Control. Routine Practices and
Additional Precautions for Preventing the Transmission of Infection in Healthcare Settings. Her
Majesty the Queen in Right of Canada; 2012.
13. Public Health Agency of Canada, Infectious Disease Prevention and Control. Hand Hygiene Practices
in Healthcare Settings. Her Majesty the Queen in Right of Canada; 2012.

57
14. Public Health Ontario. (2014) Just Clean Your Hands. Available at:
http://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/JustCleanYourHands/Pag
es/JCYH-ltch-Education-and-training.aspx#.U7WasfldX08
15. Public Health Ontario (2013). Monthly Infectious Diseases Surveillance Report, December 2013.
http://www.publichealthontario.ca/en/DataAndAnalytics/Documents/PHO_Monthly_Infectious_Dis
eases_Surveillance_Report_-_December_2013.pdf
16. Safer Needles in Healthcare Workplaces Act. (Nova Scotia) 2006, c. 7, s. 1 (Canada). Available at:
http://nslegislature.ca/legc/statutes/safeneed.htm
17. Stone, N.D et al (2012). Surveillance definitions of infections in long-term care
facilities: Revisiting the McGeer criteria. Infection Control and Hospital Epidemiology; 33(10); 965-
977. Retrieved from, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3538836/

APPENDIX A: PERSONS WITH COGNITIVE IMPAIRMENT: IMPLICATIONS FOR IPAC PRACTICES
People with changes in their brains often behave and react to their environments differently. Their perception
of the world, their reality, is altered. These brain changes may result in care challenges because of changes in
their personality, attention span, retention and processing of information (both old and new), insight,
judgment, visual spatial abilities, recall and ability to communicate.
In considering implications in the education and/or implementation of IPAC practices, it is essential that
persons with cognitive impairment be creatively and respectfully cared for using a person-centred planning
process. IPAC practices may include education on hand washing, staff practices for use of PPE, initiating
additional precautions, personal hygiene or toileting practices etc.
It is important that HCWs working in LTCFs and other care settings think holistically about how IPAC measures
can negatively affect these vulnerable persons. Suggestions on how to approach residents:
Common Losses in
Brain Functioning
What Does This Impairment
Mean?
Implications for IPAC Practices
Amnesia Challenges with memory – short
term (new), long term (declarative
or procedural), sensory or habitual
Repeat instructions and provide explanations
Use familiar &/or easily identifiable products
Reintroduce self and task
Provide ongoing reassurance
Aphasia Impaired ability to give &/or
understand language (words)
Identify how person best communicates
Use written signage
Use slow /short/specific sentences,
optimize hearing aids/eyeglasses, minimize
distractions, use positive non-verbal expressions
Agnosia Difficulty recognizing people,
places, objects
Provide reassurance & memory triggers to cue,
mime using example/action
Apraxia Impairment in sequencing,
planning, executing movement
Break tasks into simple steps, use clear reassuring
communication techniques
Apathy Inability to initiate an action Initiate activity for person e.g. place soap in hand &
demonstrate hand washing
Altered
Perceptions
Misinterpretation of the
environment
Minimize the disruptions to routines & maintain
the familiar including visitors &
Activities. Provide reassurance
Anosognosia Impaired insight - no knowledge of
their disease/condition
Refrain from using logic or
persuasion – can contribute to
increased agitation, distrust,
and/oror fear
Read /respond to their body
language to calm and support
Adapted from ‘Special Considerations’ found at http://www.ipac-canada.org/pdf/MHIG_considerations.pdf
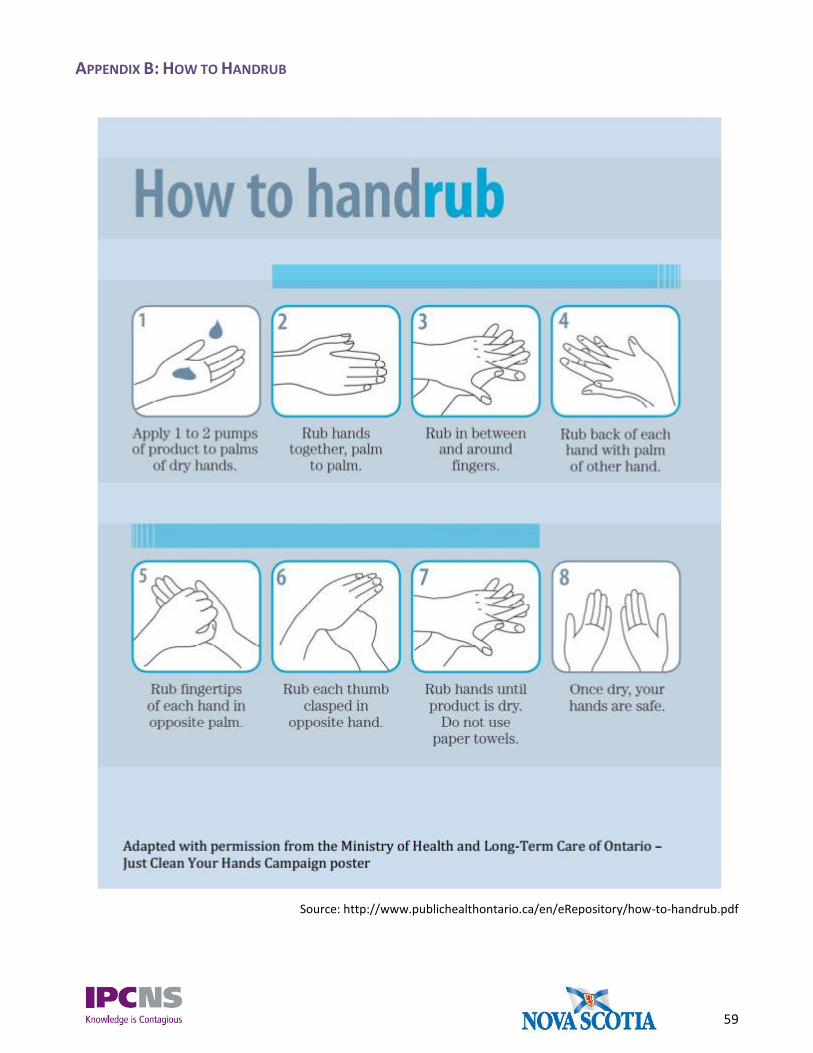
59
APPENDIX B: HOW TO HANDRUB
Source: http://www.publichealthontario.ca/en/eRepository/how-to-handrub.pdf

60
APPENDIX C: HOW TO HANDWASH
Source: http://www.publichealthontario.ca/en/eRepository/how-to-handwash.pdf

61
APPENDIX D: SAMPLE POSTERS FOR PUTTING ON AND REMOVING PERSONAL PROTECTIVE EQUIPMENT

62

63
APPENDIX E: SAMPLE CONTACT PRECAUTIONS SIGNAGE

64
APPENDIX F: FOUR MOMENTS FOR HAND HYGIENE IN LTCF
Source: http://www.publichealthontario.ca/en/eRepository/4-moments-for-hand-hygiene-male-lg.pdf