infection prevention and controldocs.firstnationsth.ca/vc10542/handouts/infection... · ·...
TRANSCRIPT

Infection Prevention and Control
101 Overview
March 2017
Overview
• Chain of Infection
• Infection Prevention and Control Basics
• Point of Care Risk Assessment
• Applying Principles

Resource
Infection Prevention and Control Guidelines: Community Health
• Recently Updated: January 2017
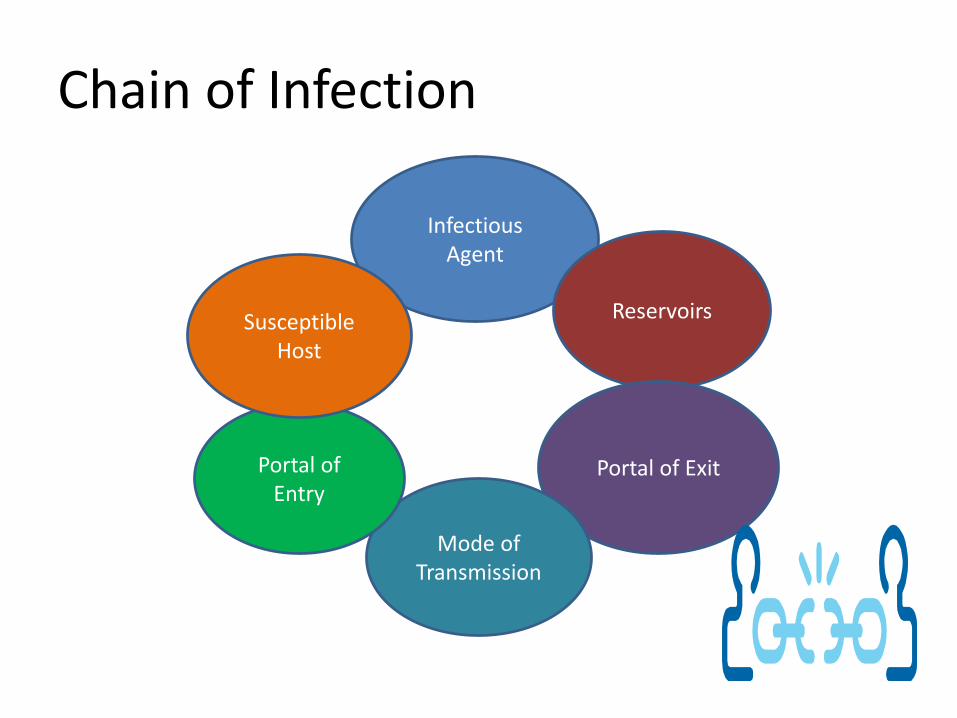
Chain of Infection
Infectious Agent
Reservoirs
Portal of Exit
Mode of Transmission
Portal of Entry
Susceptible Host

Chain of Infection
• Infectious/Causative Agent:
– Bacteria
– Fungi
– Viruses
– Parasites
– Prions
Infectious Agent

Chain of Infection
• Reservoirs:
– Humans
– Animals
– Environment
Reservoirs

Chain of Infection
• Portal of Exit:
– respiratory
– gastrointestinal
– Genitourinary
– skin/mucous
– transplacental
– blood
Portal of Exit

Chain of Infection
• Mode of Transmission:
– Contact
– Droplet
– Airborne
– Food
– Water
– Vector
Mode of Transmission

Chain of Infection
• Portal of Entry:
– Mucous Membrane
– Respiratory
– Gastrointestinal system
– Broken Skin
Portal of Entry

Chain of Infection
• Susceptible Host
– Immunosuppression/lack of immunity
– Diabetes
– Burns
– Surgery
– Age
Susceptible Host

Breaking the Chain of Infection
Source: Nunavut Health – Chain of Infection

INFECTION PREVENTION AND CONTROL BASICS
Routine Practices and Additional Precautions


IPC Basics
• Basic elements of Routine Practice include:
– Hand hygiene
– Point of Care Risk Assessment
– Risk Reduction Strategies/Personal Protective Equipment
– Education of Health Care Providers, Clients and Families, Visitors, Volunteers
Infection Prevention and Control Guidelines: Community Health, FNIHB AB Region 2017

HAND HYGIENE
The efficacy of hand disinfection in reducing nosocomial infections was initially recognized by Semmelweiss in 1847.
Source: “Hand Hygiene Practices in Health Care Settings” Public Health Agency of Canada, 2012

Definition
“Hand hygiene is a comprehensive term that refers to hand washing, hand antisepsis and actions taken to maintain healthy hands and fingernails.”
Appendix 1 - Guidelines

Definitions
• Hand washing: process for removal of soil and transient organisms from hands using soap and water
• Hand antisepsis: process for removal or destruction of resident and transient micro-organisms on the hands using an antiseptic agent, either by rubbing hands with alcohol-based hand rub or hand washing with an antiseptic soap

Microbiology Principles
• Microorganisms are present on skin and on inanimate objects
• Hand contamination does not require sustained contact with patients.
• Bacteria and viruses can persist on hands for hours.
• Contaminated hands may transmit microorganisms
• Hand hygiene may be ineffective if an inadequate amount of product is used or if inappropriate product/technique is used.

Microbiology Principles
Resident microorganisms (Normal flora):
• Survive and multiply on skin but do not generally cause illness.
• Implicated in infections linked to invasive procedures or when host is immunocompromised

Microbiology Principles
Transient microorganisms:
• Relatively scarce on clean skin and/or skin unexposed to contaminants.
• Frequently implicated in health-care associated infections

Recommendation
• “the use of an alcohol-based hand rub (ABHR) is the preferred method of hand hygiene in health care settings, unless exceptions apply.”
– Exceptions:
• hands visibly soiled with organic material
• exposure to norovirus; potential spore-forming pathogens (i.e. Clostridium difficile)

Agents Used
• Alcohol based hand rubs: (Ethanol, isopropanol, n-propanol)
– Action is to denature proteins: • excellent bactericidal and fungicidal activity• little to no activity against bacterial spores
– Most rapidly active of all agents: • Product formulation may influence efficacy (i.e. gels, rinses,
foams)
– Should have concentrations of 60 to 90% alcohol– Cautions:
• rub onto dry hands as sensitive to water dilution• Not to be used if visible/potential organic matter on hands• Products are flammable – need to be stored/used carefully

Agents Used
• Other Hand Rub products
– Products with no alcohol or with concentrations less than 60%
× No efficacy data and they should not be used in health care settings.
Hand Hygiene – ABHR
• Preferred product for HCW use
– Make sure no organic matter on hands
– Hands should be dry
– Apply “dose”
– Rub over entire hand until absorbed

Hand Hygiene - Handwashing
• Handwashingcomponents
– Soap
– Friction
– Rinsing
– Drying
– (moisturizing)
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998
Hand Hygiene - Handwashing
• Performed: – to remove visible soil or organic matter
– when build up of ABHR product feels uncomfortable
• Efficacy depends on the time taken and technique used:– Greatest reduction of transient bacteria was
within first 30 seconds

Agents Used
• Plain Soaps
– Limited antimicrobial activity – removes loose transient flora
– Cautions:
• Potential for contamination

Agents Used
• Antimicrobial Soaps
– Routine use is not necessary
– Recommended use:
• procedures requiring aseptic technique
• surgical procedures

Agents Used
• Hand Wipes
– May be used to remove soil or organic material and should be followed by use of ABHR
– NOT a substitute for ABHR or hand antisepsis
– May be a substitute for hand washing ifsoap/water not available
Hand Hygiene - Drying
• Dry hands are important as wet hands facilitate transmission of microorganisms
– Single use towels
– Avoid recontamination of hands
• Automatic hand dryers are not appropriate in clinic setting:
– Noisy, potential for aerosolization?
Hand Hygiene – Hand Care
Hand and fingernail care is very important
• Damaged skin sheds microorganisms
• Cracked hands and cuticles reduces hand-hygiene adherence
• Cautions:– Water too hot
– Applying soap before wetting hands
– Not using hand lotions
– Poor quality paper towels

Hand Hygiene – Nails, Jewelry
• Chipped nail polish increases bacterial load
• Bracelets, wrist watches and rings may prevent effective hand hygiene.

POINT OF CARE RISK ASSESSMENT

Point of Care Risk Assessment & Personal Protective Equipment in Health Care Workers
No Yes
Assess patient, environment, and interaction
Contact with patient
or environment
expected?
No PPE required
Hand hygiene
Splash or spray of
blood/body fluids
anticipated?
Facial protection
Contact with mucous
membranes, non-intact skin,
body fluids, secretions, or
soiled surfaces anticipated?
Hand hygiene before
leaving patient
environment
Put on gloves;
Put on a gown if soiling
of clothes is likely
Airborne Exposure*
potential?
Yes
No
No
Yes
Routine Practices
Yes
No
N95 Mask
*Airborne Exposure can include:
Infectious TB
Measles
some foot care practices
Methotrexate
spill.
On OneHealth


Personal Protective Equipment (PPE) used for Additional Precautions
Contact Precautions
For microorganisms of very low infective dose (i.e. Shigella) or situation of heavy environmental contamination
Gloves
Gown*
*if contamination of clothes can be expected from the patient or environment
Droplet Precautions
For microorganisms transmitted via small droplets such as most respiratory pathogens (i.e. Pertussis)
Facial mask for respiratory and ocular protection
Gloves*
Gown*
*if contamination of clothing expected from the patient or environment
Airborne Precautions
For microorganisms transmitted through air over extended period of time/space by small particles (i.e. TB)
N95 respirator
Gloves*
Gown*
Eye protection**
*if contamination of clothing expected from the patient or environment
**if splashing of blood/body fluids is possible
Respiratory
Contact and droplet: influenza
Airborne: infectious/suspected TB
Contact and airborne: health care worker (HCW) susceptible to measles and varicella
Droplet: pertussis and HCW susceptible to mumps
Gastrointestinal
Contact precautions for most organisms as well as patients who may soil environment
Neurological Syndromes
Droplet: bacterial and unknown organisms
Routine practices: viral organisms
Droplet and contact: bacterial and unknown organisms in children
Contact: viral organisms in children
Rash
Varies by the cause:
Airborne: HCW susceptible to measles
Contact and airborne: HCWs susceptible to zoster and varicella
Contact and droplet: streptococcal rashes (i.e. invasive group A strep)
Droplet: HCW susceptible to rubella
Contact: herpes simplex (neonatal only), scabies, and enteroviruses (in children)
Wounds
Contact: if drainage cannot be contained by dressing
Contact and droplet: necrotizing fasciitis or any other invasive group A streptococcal infection with or without drainage
Intramuscular/Subcutaneous Cytotoxic drugs (methotrexate)
Contact precautions
Facial/eye protection if splashing of blood/bodily fluids is anticipated
AROs (MRSA, VRE, ESBL)
Routine practices in home care setting
Contact precautions recommended for acute care
FNIHB AB Region April 2014 – Additional Precautions Chart

PERSONAL PROTECTIVE EQUIPMENT
Gloves
• Protects HCWs hands from contact with body substances
• Not a substitute for hand hygiene
• Change between clients
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998
Section 3.4 and Appendix 3A - Guidelines

Masks• Protects HCW from
organisms spread by droplet/aerosols
• Respiratory EtiquetteProcedure Mask
N95 Respirator
Surgical Mask
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998

Respiratory Etiquette
Visitors to health centres should have access to:• Signage: coughing/sneezing,
handwashing• Hand washing facilities:
soap, single-use hand towels, or ABHR
• Facial tissue and garbage receptacles
• Surgical or procedure masks for those coughing, especially during respiratory season or outbreaks.

Gowns
• Long sleeved gowns protect forearms and clothing of HCW from splashing and soiling with body substances
• Single use only
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998
Appendix 2 - Guidelines

Eye Protection
• Protects mucous membranes of eyes
– splashes or sprays of blood, body fluid, secretions or excretions
• Eye protection includes
– Safety glasses
– Safety goggles
– Face shields
– Visors (with mask)

Health Care Equipment
Standard: single use if available, if not:
• Follow guidelines* for:
– Cleaning
– Disinfection/sterilization
– Autoclave maintenance and procedures
*Reprocessing Reusable Medical and Dental Equipment: Policy and Protocols April 2015
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998

Health Care Equipment
Cleaning, Disinfection and Sterilization
• Level of reprocessing is determined by the classification of the instrument and invasiveness into tissues.
• Follow guidelines* for cleaning, disinfection and sterilization for all reusable medical and dental equipment
*Reprocessing Reusable Medical and Dental Equipment: Policy and Protocols and instructional manual April 2015
Appendix 7 - Guidelines

Environmental Control
• Ensure appropriate procedures are in place for routine cleaning of:
– Surfaces
– Toys
– High touch areas
– Public Areas• Kitchens
• bathrooms
Surface/Object Procedure FrequencyDisinfectant
Type
Surfaces:
- Examining
tables
- Baby weigh
scales
- Baby change
tables
- Beds, Bedrails
- Cribs
- Mattresses
- Call bells
- If soiled, first remove debris with a detergent solution and
rinse with warm clean water.
- Then, disinfect with a low level disinfectant as per
manufacturer’s instructions.
- Allow to air dry.
Between
patients
and when
visibly
soiled.Low level
Surfaces:
- Door
knobs/handles
- Handrails
- Countertops
- Tables, Chairs
- Phones, water
coolers
- Other common
items
- If soiled, first remove debris with a detergent solution and
rinse with warm clean water.
-Then, disinfect with a low level disinfectant as per
manufacturer’s instructions.
- Allow to air dry.
Daily
and/or
when
visibly
soiled. Low level
Toilets
Sinks and Taps
Water fountains
Clean and disinfect with a low level disinfectant.
Daily
and/or
when
visibly
soiled.
Low level
Walls
Windows
Blinds/Curtains
Clean with detergent, or launder.
Monthly or
when
soiled.
No disinfection
required
Floors Clean with detergent. Daily
and/or
when
visibly
soiled.
No disinfection
required
Carpets
Upholstery (sofas,
armchairs, etc)
Vacuum and shampoo as necessary
* Use vacuums equipped with HEPA filtration in patient-
care rooms
Daily
and/or
when
visibly
soiled.
No disinfection
required
Toys
* Toys should be
non-porous and not
plush
** Toys to be
removed during
outbreaks
- Wash with detergent and rinse.
- Disinfect with a low level disinfectant as per
manufacturer’s instructions.
- Allow to air dry.
Daily
and/or
when
visibly
soiled.
Low level
*phenols not to
be used on toys
Laundry Sorting, washing and disinfecting as per procedures
outlined in Health ’s Infection Control Guidelines- Hand
washing, Cleaning, Disinfection and Sterilization in Health
Care
After each
use.____
When blood / body fluids spills occur on any of the above surfaces or objects, refer to your Nursing Procedures for
specific cleaning and disinfection instructions.
Please consult with your Nurse in Charge or Environmental Health Officer.
During an outbreak, thorough environmental cleaning and disinfection with a disinfectant that has demonstrated
effectiveness against the specific organism is required. Increasing the disinfectant level may also be required.
Please consult with your Nurse in Charge or Environmental Health Officer.
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998Environmental Services Training Guide - 2016

Environmental Control
Environmental cleaning in Health Care Facilities – one of most important steps in breaking chain of infection.
• Janitor training: see Environmental Training Guide for Cleaning Basics
Appendix 6 - Guidelines

Environmental Control
• Routine cleaning – removes visible debris and foreign material– Water, detergents and mechanical action
• Additional cleaning and disinfection– Especially for high touch surfaces– Effective pre-cleaning– Correct use of disinfectants:
• Concentration• Contact time• Correct amount

Environmental Control
Appendix 6: Infection Prevention and Control Guidelines, 2016; Environmental Services Training Guide
Environmental Control
• Nursing Best Practices:– Management of medications, biologicals, lab
specimens, sharps• TDG
• Sharps management
• Vaccine management
– Waste management
– Food Safety
– Pest control

Environmental Control
• Best Practices away from Health Centre
– Nursing bags
– Supplies
– Aseptic field creation
• Barriers
• Hand hygiene
– Records management

Best Practices – “Sharps”
• Single Use
• Never recap needles
• Approved sharps containers
• TDG guidelines during transport
• Designated space for biohazardous waste bag/box

Best Practices: Laboratory Specimens
• PCRA: appropriate PPE for collection of specimens
• Ensure proper labelling and completion of requisition
• Transport patient specimens as per TDG guidelineshttp://www.provlab.ab.ca/guide-to-services.pdf

Best Practices: Waste Disposal
Most waste can go in “regular” garbage• General office waste• Used PPE; dialysis waste• Non-sharp medical
supplies
Extra precautions:• Bag BBF contaminated
bandages/dressings first→ “regular” garbage
• All sharps: (e.g. lancets, needles, scalpel blades)
→ Sharps containers
• Blood, blood products, expired biologicals→ Sharps container → Biohazardous disposal→ DDC (some vaccines)

Best Practices: Personal Care Supplies
• Single use preferred
• Do not share
• Minimize handling
• Only take what is required into home
• Ensure proper cleaning
Routine Practices and Additional Precautions for Health Care Workers. PHAC, 1998

Best Practices: Pest Exposure
• If providing care in home with suspect/known infestation: (i.e. bed bugs, head lice, mice, etc.)
– Use PPE based on PCRA
– End of day visit
– Limit supplies in home
– Create “clean or aseptic” field
– Appropriate teaching

APPLYING THESE PRINCIPLES
Point of Care Risk Assessment & Personal Protective Equipment in Health Care Workers
No Yes
Assess patient, environment, and interaction
Contact with patient
or environment
expected?
No PPE required
Hand hygiene
Splash or spray of
blood/body fluids
anticipated?
Facial protection
Contact with mucous
membranes, non-intact skin,
body fluids, secretions, or
soiled surfaces anticipated?
Hand hygiene before
leaving patient
environment
Put on gloves;
Put on a gown if soiling
of clothes is likely
Airborne Exposure*
potential?
Yes
No
No
Yes
Routine Practices
Yes
No
N95 Mask
*Airborne Exposure can include:
Infectious TB
Measles
some foot care practices
Methotrexate
spill.

WOUND MANAGEMENT

Using Chain of Infection
• Agent: see lab work to confirm organism
– MRSA, C. diphtheriae, Streptococcal organism (Group A or B), etc.
• Reservoir: blood, wound, other
• Exit/Entry: direct contact, respiratory, indirect contact
• Host: self care, household factors, susceptibility

Agent
• MRSA: clinical or screening specimen– Check drug sensitivity on lab results – right Rx?
– Mitigate risk for transmission: • Client and family education
• HCW PCRA: appropriate PPE, follow wound protocols
– Prevention measures: • appropriate use of antibiotics
• hand hygiene
• appropriate cleansing and dressing techniques
– Decolonization? • seldom of benefit in a home setting.
Infectious Agent

Agent
• Corynebacterium Diphtheriae – may be 2nd or third organism on lab results– Site of specimen collection, Characteristics of site.
• Superficial? Mucky? Membranous? Other?
– Will need confirmation re toxigenic or not.• Follow wound management protocols
• PCRA: Routine practices, especially hand washing.
– Prevention: • immunization – diphtheria part of primary
immunizations and part of adult booster (Td, dTap).
Infectious Agent
Agent
• Streptococcal Organisms:– Group A: streptococcus pyogenes.
• only of public health concern if deemed invasive (Specimen from normally sterile site or body fluid.)
– Strept. sore throat, impetigo, erysipelas, scarlet fever, puerperal fever, rheumatic fever, septicemia, cellulitis, mastoiditis, otitis media, pneumonia, wound infections, necrotizing fasciitis, toxic shock-like syndrome.
• Frequently in wound specimens along with MRSA
– Management: • PCRA - focus on hand washing, appropriate PPE• wound management protocols, appropriate treatment based
on manifestation• Client and family education
Infectious Agent

Agent
• Streptococcal Organisms:
– Group B: streptococcus agalactiae
• Public health concern if mother is carrier because of risk to babe.– Sepsis, pneumonia, meningitis, osteomyelitis, septic arthritis
• All women are screened during pregnancy:– antibiotics offered based on lab results during intrapartum
period.
Infectious Agent

Lab Reports
• Key factors:
– Organism(s) identified
– Site of specimen
– Date collected
– Sensitivity results
– Lab notes
Infectious Agent

RN Roles and Responsibility
• PCRA for all interactions– Gloves? Gown? Mask?
• Wound Management:– Monitor clinical status: update MD/NP of wound
status if not healing appropriately• Ordering HCP also receives copies of labs – and will be aware
of Sensitivity results
• Follow best practices: cleansing , dressing techniques
– Collect specimen if warranted
• Appropriate client and family education
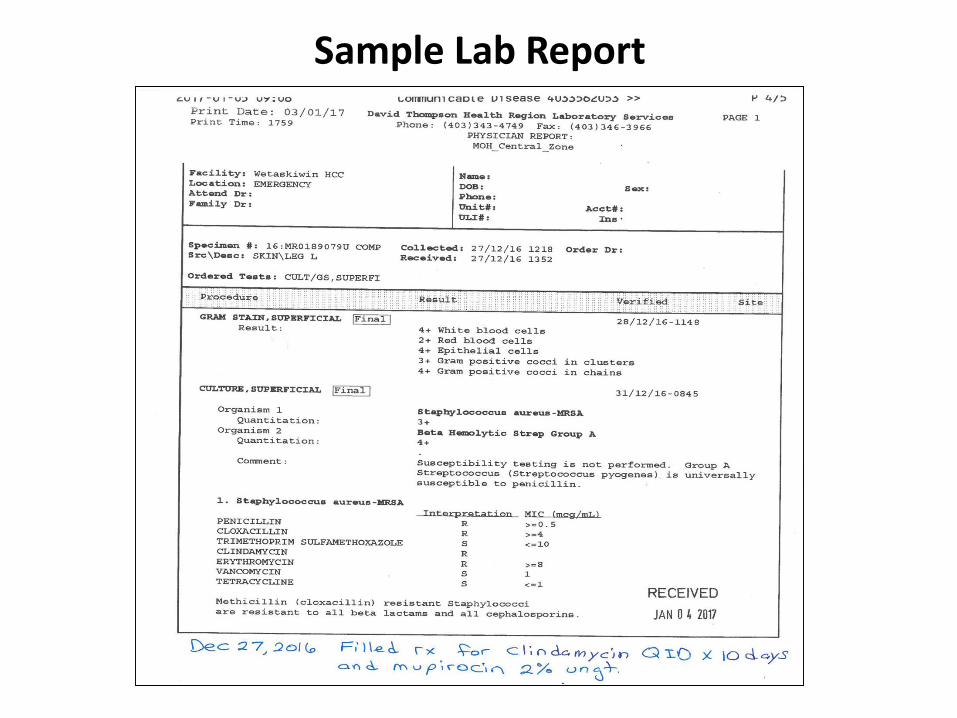
Sample Lab Report

Sample Lab Report

Sample Lab Report

Sample Lab Report

“ROUTINE” CONTACTS

Routine Contacts
Examples include:
• Monitoring for therapeutic interventions– BP, VS, blood glucose
• Post-natal home visits
• Well child clinics
• Dental clinics
Additional Factors:
• Extended family present

Routine Contacts
• Using PCRA:
– Will there be contact with BBF?
• No: hand hygiene
• Yes: gloves may be warranted; masks may be warranted
• Using Chain of Infection:
– Host factors (symptoms, immune status)
• E.g. Respiratory symptoms – offer mask to individual; limit contact with others

PERSONAL CARE
Personal Care
Examples include:
• Baths
• Pericare
• Oral hygiene

Personal Care
• Using PCRA:
– Will there be contact with BBF?
• No: hand hygiene
• Yes: gloves
– Is there be potential for spraying/splashing?
• No: hand hygiene
• Yes: gloves, possibly gowns, possibly eye protection

SPECIMEN COLLECTION

Specimen Collection
• Using PCRA/Chain of Infection:
– Suspected /known organism?
• i.e. Measles, TB, MRSA– May need mask
– Type of specimen required
• i.e. Sputum, Blood, Swab (NP, wound, throat)– May need mask, gloves

Specimen Collection
• Do not need a physician’s order to collect specimens:
– Wounds
– CDC related
• Work with local lab re appropriate specimens and lab requisitions.
– Guide to Services

INJECTIONS OR TESTING

Injections or Testing
Examples include:
• Intramuscular or subcutaneous injections
– Vaccines
– Treatments: B12, methotrexate
• Intradermal tests
• Glucose tests

Injections or Testing
• Using PCRA:
– Exposure to BBF?
• No: hand hygiene – Other measures: clean site before injection, sharps
management
– Other risks?
• PPE based on assessment

Education of Clients/Families
• Base specific teaching on:
– applying what is relevant from the Chain of Infection
– Incorporating Infection Prevention and Control basics.

Our Responsibility
• Routine practices are the foundation for prevention and control
• You are the important link in all prevention activities.

The Chain of Infection can be Broken
Source: Nunavut Health – Chain of Infection
References
• Public Health Agency of Canada – Routine Practices and Additional Precautions for Health Care Workers– Hand washing, Cleaning and Disinfection– http://www.phac-aspc.gc.ca/nois-sinp/guide/pubs-eng.php
• Alberta Health– Hand Hygiene– Infection Prevention and Control Standards– http://www.health.alberta.ca/newsroom/pub-infection-
prevention.html
• Alberta Health Services– Many resources– http://www.albertahealthservices.ca/6410.asp
Resources
• FNIHB AB Region – :
– OneHealth “CDC Resources”
• Infection Control Guidelines: Community Health
• Reprocessing Reusable Medical and Dental Equipment: Policy and Procedures
– FNIHB Regional Dental Infection Prevention and Control Standards Manual

Resources
• Alberta Health, Public Health Notifiable Disease Management Guidelines
• Alberta Health Services, Infection Control in Community Setting

FNIHB Regional Contacts
• Key Regional contact:
– Ruth Richardson: 780-495-5439 [email protected]
• Other contacts:
– Nursing Practice Standards and Guidance:
• Home Care Advisor
• Wound Management Consultant
• Regional Nursing Team
– Environmental Health Officers