palliative care needs of people with end-stage heart failure · palliative care needs of people...
TRANSCRIPT

PALLIATIVE CARE NEEDS OF PEOPLE WITH
END-STAGE HEART FAILURE
PALLIATIVE CARE PALLIATIVE CARE NEEDS OF PEOPLE WITH NEEDS OF PEOPLE WITH
ENDEND--STAGE STAGE HEART FAILUREHEART FAILURE
Nancy M. Albert PhD, CCNS, CCRN, CNAThe Cleveland Clinic Foundation
Cleveland, Ohio

OBJECTIVESOBJECTIVESOBJECTIVES• Provide overview of advanced HF
pathophysiology, modes of death, and treatment• Describe prognostic factors and issues of
determining prognosis• State current guidelines related to end-of-life• Discuss palliative care needs
Symptom managementDepression and anxietySkin breakdownPainSleepGI complaintsConversations

Hypertrophy, remodeling, apoptosis, ischemia, ↑ HR, ↓ HR variability, arrhythmias, fibrosis
Mortality
Hypertrophy, remodeling, apoptosis, ischemia, ↑ HR, ↓ HR variability, arrhythmias, fibrosis
Mortality
Norepinephrine-reduced baroreceptorsensitivity
Angiotensin II-aldosterone-vasopressin
NEUROENDOCRINE ACTIVATIONNEUROENDOCRINE ACTIVATIONNEUROENDOCRINE ACTIVATION
Cytokines

LV REMODELINGLV REMODELINGLV REMODELING
Normal HeartDilated
Cardiomyopathic Heart
↓ β-AR signal transduction, cytokines, RAAS↓ Bioenergetics
Altered Ca2+ handling architectureFetal gene induction
ApoptosisMortality
Mann & Bristow, Circulation 2005;111:2837.

Sudden Death59%
Other15%
HF26%
MERIT-HF: Mode of Deathby HF Severity
MERITMERIT--HF: Mode of DeathHF: Mode of Deathby HF Severityby HF Severity
HF12%
Other24%
Sudden Death64%
NYHA Class II NYHA Class IIISudden Death33%
Other11%
HF56%
NYHA Class IV
n=103 n=232 n=27
Number of Deaths
Patients with NYHA class II-IV HF (n=3991) were randomized to a target 200-mg once-daily dose of metoprolol succinate (n=1990) or placebo (n=2001) and followed for a mean of 1 year.
MERIT-HF Study Group. Lancet. 1999;353:2001-2007.

18%
21%
18%10%
19%
14% MetabolicProgressiveSCDUnwitnesed-SuddenOtherUnknown
Chronic HF: Mode of Death Single center, Disease Mgmt program studyChronic HF: Mode of Death Chronic HF: Mode of Death
Single center, Disease Mgmt program studySingle center, Disease Mgmt program study
Metabolic = Creatinine > 4.0 mg/dL in 1 month of death;Creatinine > 3.0 mg/dL before referral to hospice;Progressive hepatic failure
Progressive = NYHA FC IV symptoms without renal or hepatic failure
Other = Trauma, sepsis or other non-cardiac causesDerfler et al. AJGC 2004;13:299-306
N = 74 deaths

SYSTOLIC HF DeathBrigham & Women’s CM Clinic; EF ≤ 35%
SYSTOLIC HF DeathBrigham & Women’s CM Clinic; EF ≤ 35%
January 2000 - October 20, 2003• 160 deaths; 50% outpatients; 21% SCD
In 6 months before death:• 50% NYHA FC III-IV symptoms• Renal insufficiency and hyponatremia
were worse in months preceding death than at the time of death
• Creatinine: 3.2 vs. 2.3 mg/dL• Sodium: 128 vs. 135 mmol/L
P <.001
Teuteberg et al. J Cardiac Failure 2006;12:47

Reduce Mortality
β-BlockerACEIor ARB
AldosteroneAntagonist
CRT ±an ICD*
Hyd/ISDN*
*For select indicated patients.
ICD*
Treat ComorbiditiesAspirin*
Warfarin*Statin*
Enhance AdherenceEducation
Disease ManagementPerformance Improvement Systems
Evidence-Based Treatment Across the Continuum of LVD and HF
EvidenceEvidence--Based Treatment Across Based Treatment Across the Continuum of LVD and HFthe Continuum of LVD and HF
Hunt SA et al. Circulation 2005;112:1825-1852

Cohn J, et al. J Cardiac Failure. 2003;9:5(suppl):S87.
-4.9%(60%)
-11.2%(85%)
Major Opportunity
Dea
ths
at 2
yea
rs, %
24 month data from placebo arm of ValHeft
Heart Failure-Related Deaths: Impact of Contemporary Therapy
Heart FailureHeart Failure--Related Deaths: Related Deaths: Impact of Contemporary TherapyImpact of Contemporary Therapy
0
2
4
6
8
10
12
14
No ACEI or BB ACEI and BB
Pump FailureSudden Death

HF EtiologyIschemic: 100% Ischemic: 59%
Nonischemic: 41% Nonischemic: 100%Ischemic: 52%
Nonischemic: 48%
NYHA Class I/II/III(35%/35%/30%)
III/IV(87%/13%)
I/II/III(20%/60%/20%)
II/III(71%/29%)
LVEF ≤30% ≤35% ≤35% ≤35%No. Pts 1232 1520 458 2521Follow-Up 20 months 12 months 24 months 45 monthsHazard Ratio 0.69 0.64 0.66 0.77
19.8%
14.2%19.0%
12.0%14.1%
7.9%
28.8%
22.0%
0
5
10
15
20
25
30M
orta
lity,
%
MADIT II1 COMPANION2 DEFINITE3 SCD-HeFT4
Control TherapyP=.007
P=.065P=.004
P=.016
ICD Device Trials in HF & LVDICD Device Trials in HF & LVDICD Device Trials in HF & LVD
1Moss AJ, et al. N Engl J Med. 2002;346:877-883. 2Bristow MR, et al. N Engl J Med. 2004;350:2140-2150.3Kadish A, et al. N Engl J Med. 2004;350:2151-2158. 4Bardy GH, et al. N Engl J Med. 2005;352:225-237.

Control VolumeReduce Symptoms and Improve QOLSalt Restriction*
Diuretics*
Digoxin*
β-BlockerACEIor ARB
AldosteroneAntagonist
Treat Residual SymptomsCRT ±
an ICD* Hyd/ISDN*
*For select indicated patients.
ICD*
Improve Adherence and QOLEducation
Disease ManagementPerformance Improvement Systems
Evidence-Based Treatment in Advanced HF
EvidenceEvidence--Based Treatment Based Treatment in Advanced HFin Advanced HF
Hunt SA et al. Circulation 2005;112:1825-1852

4545
4040
3535
3030
2525
2020
1515
1010BaselineBaseline 1wk1wk 1mo1mo 3mo3mo offoff--
immedimmedoffoff--1wk1wk
offoff--4wk4wk
N=25N=25
Mitral RegurgitationMitral Regurgitation
Ejection fractionEjection fraction
%%
Yu, et al. Circulation 2002;105:438Yu, et al. Circulation 2002;105:438
††, significant diff. compared to 3 mo, significant diff. compared to 3 mo, significant diff. compared to baseline, significant diff. compared to baseline**
**** **
** **††
††††††
†† ††
** ****
**
**
**
Cardiac Resynchronization:Cardiac Resynchronization:Must be Must be ““ONON”” Continuously to Achieve EffectsContinuously to Achieve Effects

Cardiac Device in and active matters.
Renal function matters.
Home and Hospital care matters.

Prognosis Near Death: SupportPrognosis Near Death: Support1.0
0.8
0.6
0.4
0.2
0.0
6-M
onth
Sur
viva
l Est
imat
e
14 13 12 11 10 9 8 7 6 5 4 3 2 1
CHFCOPDCirrhosis
Days to DeathBock et al. New Horizons, 1997; 5:51

VARIABILITY in FC from I-IVVARIABILITY in FC from IVARIABILITY in FC from I--IVIV

VARIABLES ASSOCIATED with POOR PROGNOSTIC
VARIABLES ASSOCIATED with VARIABLES ASSOCIATED with POOR PROGNOSTICPOOR PROGNOSTIC
Serum Na < 136 mg/dL
Serum creatinine ≥2.0 mg/dL
Presence of CVA, COPD, Ca, dementia
Low BP w Acute Decomp. HF
Dyspnea Orthopnea Older age EF < 45 %
↓ In 6 min. walk test
Dependency with ADL’s
Frequent firing of ICD
NYHA FC IV ↑ Resp rate ↓ HRV
PND ↑ HR > 100 bpm
Syncope Atrial Fib
3 or more hospitalizations/yr ↑ serum BNP ↓ Peak VO2
Symptoms when on optimal medical Tx
Problem: We do not know which factors remain the
most important in mortality risk
after multivariate regression…need RESEARCH
Albert NM. Cardiovascular. In Keubler, Davis and Dea (Eds). Palliative Practices. An Interdisciplinary Approach . 2005

PROGNOSTIC MODELSPROGNOSTIC MODELSPROGNOSTIC MODELS• 280 patients w advanced HF from 16 US sites• Applied 4 prognostic models from literature• 148 deaths or transplantations occurred
Average follow-up was 31.2 months• Each model identified patients with different
prognosesLimited overall predictive powerMany component patient characteristics did not have independent prognostic significance
Frankel et al. J Cardiac Failure. 2006;12:430
PROGNOSTIC MODELSPROGNOSTIC MODELSPROGNOSTIC MODELS
• Most powerful prognostic factors within the 4 models:
Increasing ageIschemic cardiomyopathyHx of cardiomyopathyAnkle edemaDecreased peak oxygen consumptionAbsence of beta-blocker use
Frankel et al. J Cardiac Failure. 2006;12:430
Problem: Physician researchers focused on variables
associated with demographics, medical Hx,
drug tx’s but not social or psychological factors
known to affect outcomes …need RESEARCH

GUIDELINES on End-of-LifeGUIDELINES on EndGUIDELINES on End--ofof--LifeLifeACC/AHA (2005)1 HFSA (2006)2
Ongoing discussions w pt/family about prognosis
Ongoing discussions w pt/family about QOL and prognosis
Education about advance directives
Discuss and individualize advanced directives and resuscitation wishes
Ensure continuity of medical care from inpatient to ambulatory
Optimize pt status- medically and psychologically BEFORE discussing end-of-life Consider end-of-life if symptoms warrant:• Frequent hospitalizations• Chronic poor QOL• Need intermittent or chronic IV support• Considered for assist device
1. Hunt SA et al. Circulation 2005;112:1825-1852; 2. HFSA. J Cardiac Fail 2006;12:10-38.
Level C evidence

GUIDELINES on End-of-LifeGUIDELINES on EndGUIDELINES on End--ofof--LifeLifeACC/AHA (2005)1 HFSA (2006)2
Discuss inactivating ICD Give directions about clinical response if does not want resuscitation; Discuss inactivating ICD
Hospice components for symptom palliation include opiates, inotropes and IV diuretics
Individualize strategies for symptom management, limiting testing and interventions
Professionals working with HF pts should examine end-of-life processes and make improvements
Have pts reassess their wishes concerning Tx options as decisions may change over time
Aggressive procedures in the final days of life are not appropriate
Discuss the possibility of unexpected cardiac death. Consider hospice care in the home, hospital or special hospice unit
1. Hunt SA et al. Circulation 2005;112:1825-1852; 2. HFSA. J Cardiac Fail 2006;12:10-38.

Palliative Care Needs
at End of Life
Palliative Palliative Care Needs Care Needs
at End of Lifeat End of Life

Characteristics of patients with HFCharacteristics of patients with HFWomen Men P value
Age, mean 79 73 <0.001HTN % 72 61 0.02DM % 19 29 0.03Smoking % 35 68 <0.001Hyperlipidemia 16 20 NS≥ 3 comorbidities 22 31 0.04History MI 19 26 NSObesity (BMI ≥ 25) 49 62 0.04
Roger et al. JAMA 2004;292:344

43%
37%
12%8%
HospitalHomeSNFOther
Chronic HF: Place of DeathSingle center, Disease Mgmt program studyChronic HF: Place of DeathChronic HF: Place of DeathSingle center, Disease Mgmt program study
Derfler et al. AJGC 2004;13:299-306
N = 74; mean age 57.7 years

MAINSTAY: General Disease Management Rules
MAINSTAY: General Disease MAINSTAY: General Disease Management RulesManagement Rules
ADHERE Registry; All Enrolled Discharges from April 1, 2004 to March 31, 2005 with History of HF and LVEF Documented and < 0.40 (n = 29,759) SciosScios, Inc., Inc.
*Excludes patients with documented contraindications.
16
71
84
53
29
0102030405060708090
100
Patie
nts
Trea
ted
(%)
Chronic Outpatient HF Medication Prior to Hospitalization
ACE Inhibitor* ARB Beta-Blocker* Diuretic Digoxin
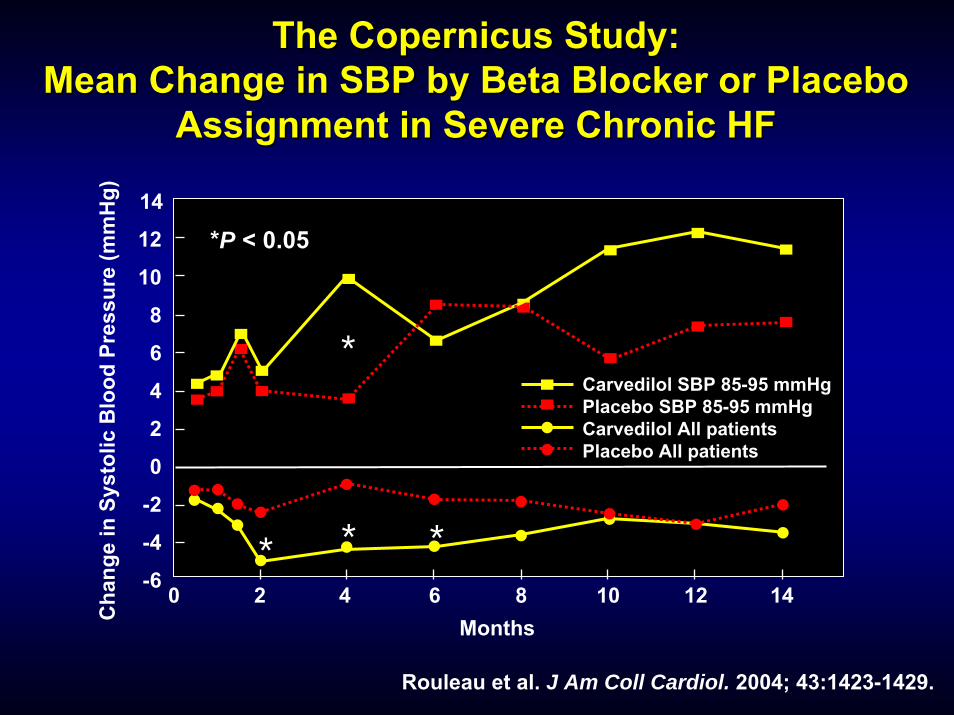
The Copernicus Study: The Copernicus Study: Mean Change in SBP by Beta Blocker or Placebo Mean Change in SBP by Beta Blocker or Placebo
Assignment in Severe Chronic HFAssignment in Severe Chronic HF
Rouleau et al. J Am Coll Cardiol. 2004; 43:1423-1429.
Cha
nge
in S
ysto
lic B
lood
Pre
ssur
e (m
mH
g)
*P < 0.05
Carvedilol SBP 85-95 mmHgPlacebo SBP 85-95 mmHgCarvedilol All patientsPlacebo All patients
Months
*
* * *4 6 8 10 12 140 2
-6
-4
-2
0
2
4
6
8
10
12
14

COPERNICUS: Morbidity and Mortality by Systolic Blood
Pressure Quintiles
COPERNICUS: Morbidity and COPERNICUS: Morbidity and Mortality by Systolic Blood Mortality by Systolic Blood
Pressure QuintilesPressure QuintilesBlood
Pressure(mm Hg)
Placebon (%)
Carvediloln (%)
Risk ReductionDeath or
Hospitalization
>125 478 (42) 475 (41) 40% 32%
Risk Reduction(Mortality)
85-95 62 (5) 70 (6) 23% 26%
96-105
106-115
116-125
39% 25%136 (12)128 (11)
244 (22) 224 (19)
221 (20) 251 (22)
35% 22%
39% 46%
Rouleau et al. J Am Coll Cardiol. 2004; 43:1423-1429.

GOAL: Lower impedance & slow progression of structural and functional disease
SBP in Advanced HFSBP in Advanced HFSBP in Advanced HFHealthy heart: SBP is a product of SV and the impedance to ejection (afterload)• Impedance does NOT affect SV, just pressureFailing heart: Impedance controls SV• Neurohormonal & vascular consequences of HF raise
impedanceSV becomes the measure of severity of LV dysfunction
HYPOTENSION is d/t reduced contractile function of the heart
Cohn JN. JACC. 2004;43:1430

MEDICATION Dosage/TimingMEDICATION Dosage/TimingMEDICATION Dosage/Timing• Drugs that peak at same time:
1 - 2 hoursLoop diureticsEplerenoneCaptoprilHydralazine/nitrate combo
Trandolapril
2 - 4 hoursMetolazoneCarvedilolBisoprololCandesartanFosinoprilQuinaprilValsartan
4 - 6 hoursHCTZRamiprilEnalaprilLisinopril (7 hrs)Metoprolol
succinate(6-12 hrs)
PERSISTENT SYMPTOMSPERSISTENT SYMPTOMSPERSISTENT SYMPTOMS• Symptomatic hypotension (orthostasis)• Increasing dyspnea• Worsening renal dysfunction• Hypoperfusion
Decreased urine outputCold, clammy skinMental obtundation, confusion, sleepyDizzy, lightheaded, weak, fatiguedTachycardiaNausea, anorexia, no appetite, bloating

MEDICATIONS for PERSISTENT SYMPTOMS
MEDICATIONS for PERSISTENT MEDICATIONS for PERSISTENT SYMPTOMSSYMPTOMS
• Are HF medication therapies optimized?Right drugs, right doses, right schedule?
• Continuous ambulatory IV inotropic supportMilrinone or dobutamine• May decrease survival • May improve QOL
Regularly obtain hemodynamic data to assess for need
• Nesiritide infusion is NOT supported

BAD PHARMACOLOGICAL BAD PHARMACOLOGICAL THERAPIESTHERAPIES
• Antidepressants that inhibit CNS neuron uptake of dopamine or norepinephrine
SSRI class OK • Drugs used in psychosis; bipolar mania• COX-2 inhibitor-NSAID’s (ALL!!) • Thiazolidinedione (TZD) Type II DM agents• Most antidysrhythmics
Exception: amiodarone

BAD BAD ““OTCOTC”” DRUGS/ THERAPIESDRUGS/ THERAPIES
•• Na+ based antacids Na+ based antacids (Rolaids)(Rolaids)
•• ASA (high dose)ASA (high dose)•• NSAIDNSAID’’ss•• Ginseng Ginseng
(germanium)(germanium)•• GinkgoGinkgo•• EchinaceaEchinacea•• Black licoriceBlack licorice•• DecongestantsDecongestants

Medication SummaryMedication SummaryMedication Summary• Follow “optimal HF drug” guidelines
Unless patient is unable to swallow or is obtunded
• Resist inclination to remove HF drugs if no contraindications
May worsen symptoms / increase suffering• Remove excess non-HF drugs and alternative
therapies• Assess potassium and creatinine if:
Aggressive diuresisAdding aldosterone inhibitor

Survival (%)
0 6Months After Re-Assessment at 4-6 wks
100
40
0
80
18
60
24
20
12
No Cong., n = 801-2 Cong., n = 403-5 Cong., n = 26
Clinical Evidence of Congestion 4 to 6 Clinical Evidence of Congestion 4 to 6 Weeks after Hospitalization & SurvivalWeeks after Hospitalization & Survival
Lucas et al., AHJ. 2000; 140:840
p < 0.0001p < 0.0001
Congestion CriteriaCongestion CriteriaOrthopneaOrthopneaJVDJVDWeight gain Weight gain >> 2 2 lbs in one weeklbs in one week↑↑diuretic dose on diuretic dose on visitvisitEdemaEdema

More than 50% of Patients Have Little or no Weight Loss During Hospitalization
Fonarow GC. Rev Cardiovasc Med. 2003; 4 (Suppl. 7): 21
7% 6%
13%
24%
33%
15%
3% 2%
0
5
10
15
20
25
30
35
Patie
nts
(%)
(<-20) (-20 to -15)(-15 to -10)(-10 to -5) (-5 to 0) (0 to 5) (5 to 10) (>10)
Change in Weight (lbs)

• Among pts. with severe heart failure 1PCWP 33 ± 6 mmHg, CI 1.8 ± 0.5, LVEF 0.18 ± 0.06CXR: 27% no congestion, 41% minimal congestion
• Among pts. with moderate to severe heart failure 2PCWP 30 ± 9 mmHg, CI 2.1 ± 0.8, LVEF 0.18 ± 0.06No rales: 84%, No edema: 80%, No JVP 50%, No orthopnea: 22%
• Hemodynamic congestion may not be recognized clinically (doesn’t translate into symptoms/signs until late) 1 Mahdyoon H et al. Am J Card. 2003; 63: 625
2 Stevenson LW et al. JAMA. 1989; 261: 884
Congestion Often Does not Translate in Signs/SymptomsCongestion Often Does not Congestion Often Does not
Translate in Signs/SymptomsTranslate in Signs/Symptoms

MANAGEMENTMANAGEMENTMANAGEMENTBreathlessness due to CongestionBreathlessness due to Congestion
Exertion At rest Terminal
•• Pharmaceutical and nonPharmaceutical and non--pharmaceutical measurespharmaceutical measures
Correct correctable causeCorrect correctable cause
NonNon-- drug drug TxTxSymptomatic drug Symptomatic drug TxTx

MedicationsDevices

↑ Distal Ca++Reabsorption
↓ Plasma Volume
↓ Uric AcidClearance
Complications of Diuretic Therapy in HFComplications of Diuretic Therapy in HFKaplan, N.M., Treatment of Hypertension: Drug Therapy in Clinical Hypertension (p. 203) in Clinical Hypertension, 6th. Ed. Baltimore: Williams & Wilkins 1994.
HypomagnesemiaHypomagnesemiaDiuretic TherapyDiuretic Therapy
↓ Cardiac Output
↓ Renal Reabsorption of Na (& Mg)
↓ Renal Blood Flow
HyponatremiaHyponatremia
↑ PRA
↓ GFR
↑ ProximalReabsorption
↑ Aldosterone
Kaliuresis
HypokalemiaHypokalemia
Glucose IntoleranceGlucose IntoleranceHypocalcemiaHypocalcemiaHyperuricemiaHyperuricemia
↓ CalciumClearance
Pre-renalAzotemiaPre-renalAzotemia
Neurohumoral Activation
Neurohumoral Activation
VT/VF
SCD
VT/VF
SCD
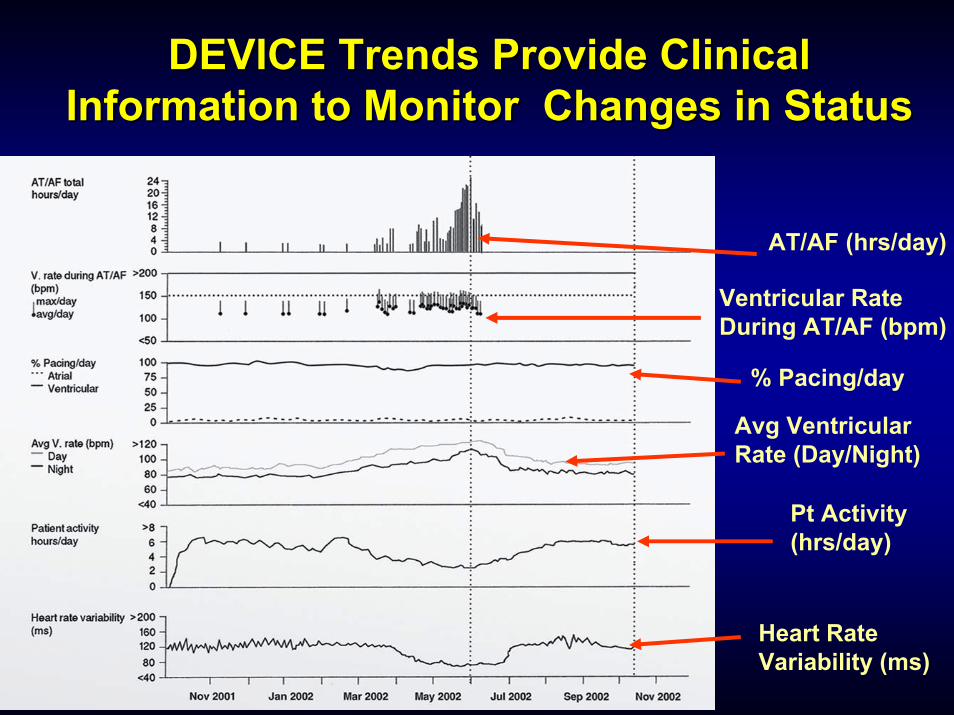
DEVICE Trends Provide Clinical DEVICE Trends Provide Clinical Information to Monitor Changes in StatusInformation to Monitor Changes in Status
AT/AF (hrs/day)
Ventricular Rate During AT/AF (bpm)
Avg Ventricular Rate (Day/Night)
Pt Activity (hrs/day)
Heart Rate Variability (ms)
% Pacing/day

Impedance
“Wetter” Lungs
DEVICE Monitoring: IntraDEVICE Monitoring: Intra--Thoracic ImpedanceThoracic Impedance
“Dryer” Lungs

IntraIntra--Thoracic ImpedanceThoracic Impedance
MD Programmed Threshold
Reference impedance slowly adapts to daily impedance
Daily impedance is average of one day’s measurements
Accumulation of difference between daily and reference impedance

DIET and FLUIDSDIET and FLUIDSDIET and FLUIDS• Low sodium diet
Educate• Restaurants• Relatives homes
Monitor• Fluids
EducateTricks to decrease thirst• Suck on hard
candy, frozen grapes, cold washcloth…

IF CONGESTION INCREASESIF CONGESTION INCREASESIF CONGESTION INCREASES• Carefully assess adherence to current diuretic regime
Especially related to when taken during day• Increase loop diuretic dose or frequency; give IV• Change loop diuretic agent to one with different
absorption (i.e., furosemide to torsemide)• Add a thiazide diuretic• Topical or oral nitrate at night (if not on during daytime)
May improve sleep / decrease awakenings• Carefully assess adherence to diet and fluid regime and
tighten modifications• Initiate or tighten fluid restriction

Congestion SummaryCongestion SummaryCongestion Summary• Use loop diuretics to control symptoms
Add metolazone p.r.n. but beware of erratic absorption
• Overdiuresis causes increased fatigue and symptoms that mimic worsening HF
• Use low sodium diet 1600 mg sodium/day
• Use fluid restrictionLess than 8 cups/day

DEPRESSIONand
ANXIETY

DEPRESSIONDEPRESSION
05
1015202530
Fatigue Breathlessness Chest Pain0
1020304050607080
KCCQ Physical KCCQ Total SF36 PhysicalroleHAM-D
r 0.33** 0.33 0.32* 0.41** 0.57*** 0.37* * P < 0.05; ** P < 0.01; ***P < 0.001
Effects on health status at 6 months• 139 ambulatory patients with HF in primary care• Mean age 75 ± 9.7 yrs Major depression
Minor depressionNo depression
Sullivan et al. AJGC 2004;13:252-260
Multidimensional Assessment of Fatigue

DEPRESSION and ANXIETYDEPRESSION and ANXIETYDEPRESSION and ANXIETY• Predictors of anxiety and depression in a
consecutive series of 227 hospitalized HF patients; mean age, 77.1 ± 7.9 yrs
Yu et al. J Psychosomatic Research 2004;57:573-581.
Hierarchal regression model with all 4 factorsR2, 0.49
Variables BetaPoor perceived emotional-informational support
0.34
Higher levels of fatigue 0.40Poorer health perception 0.21Not living with family 0.10
• Assess mood, morale and coping skills• Counseling
Support groups (church, community, neighbor, or healthcare initiated)Caretaker classes
• Help patient to retain a sense of control of their disease processes
• Treat depression with serotonin reuptake inhibitors, as needed
• Treat anxiety with short acting and longer acting anxiolytics, as needed
DEPRESSION and ANXIETYDEPRESSION and ANXIETYDEPRESSION and ANXIETY
SKIN BREAKDOWNSKIN BREAKDOWNSKIN BREAKDOWN• Can occur from edema or venous stasis• Can be painful• Treatment:
Assess cause and correct when possibleElastic stockings or elastic wrapsExercise and active ROM exercisesConsult with skin care/wound experts as needed

PAINPAINPAIN• Systematic review of pain in HF
9 descriptive studies; 5 specifically on HF23-75% of patients with HF reported painFactors related to pain:• Anxiety• Depression• Self rating of poor QOL• Dyspnea• More dependencies in ADL’s
Symptom of pain is NOT well understood• PAIN-HF study underway
Godfrey et al. J Cardiac Fail 2006;12:307-313.

PAIN RELIEFPAIN RELIEFPAIN RELIEF• Clinical practice guidelines by ACC/AHA:
No recommendations on pain assessmentNo recommendations on ongoing monitoring1 recommendation on management: “opiates”• No details on opiate therapy
• Palliative care medicine providers are the experts; we defer to you!!

SLEEPSLEEPSLEEP
• Sleep related breathing disorders are prevalent at end-of-life:
OrthopneaParoxysmal nocturnal dyspneaObstructive sleep apneaCentral sleep apneaCheyne stokes respirationsDaytime sleepiness

SLEEPSLEEPSLEEP• Management:
Elevate HOBOral or topical nitrate at nightCPAP for obstructive sleep apneaDiuresis/fluid removal for central sleep apneaOxygen at night? • Does not improve daytime sleepiness• Does not improve health related QOL

CPAP in Central Sleep ApneaCPAP in Central Sleep ApneaCPAP in Central Sleep Apnea
Bradley et al. NEJM 2005;353:2025-33.
0
1.00
80
60
40
20
Tran
spla
ntat
ion-
free
Su
rviv
al (%
)
Time from Enrollment (mo)0 12 24 36 48 60
CPAP group (32 events)Control group (32 events) P = 0.54

CPAP in Central Sleep ApneaCPAP in Central Sleep ApneaCPAP in Central Sleep Apnea
00
10
20
50Ep
isod
es o
f Apn
ea a
nd
Hyp
opne
a(n
o. p
er h
r of s
leep
)
30
40
3 24
P < 0.001 CPAP groupControl group
Bradley et al. NEJM 2005;353:2025-33.
Time from Randomization (mo)

CPAP in Central Sleep ApneaCPAP in Central Sleep ApneaCPAP in Central Sleep Apnea
Bradley et al. NEJM 2005;353:2025-33.
00
LVEF
(%)
24Time from Randomization (mo)
P < 0.007 CPAP groupControl group
15
20
25
30
35
63
Also improved in CPAP group:Mean and minimal oxygen saturation

GI COMPLAINTSGI COMPLAINTSGI COMPLAINTS• Nausea and loss of appetite
Caused by congestion in liver and stomach• Avoid fluid overload
Caused by low cardiac output• Assess for hypoperfusion; treat
• Digoxin toxicityUse low dose (0.125 mg/day)
• Screen for toxicity, as needed• Constipation
Fluid status and morphine• Avoid OTC pre-packaged enemas (Na+ based)• Stool softeners and laxatives OK
END-OF-LIFE CONVERSATIONSENDEND--OFOF--LIFE CONVERSATIONSLIFE CONVERSATIONS
TOPICS• Unfavorable prognosis & treatment failure• Treatment choices and family responses• Advance care planning• Concerns about one’s ability to cope• Life goals and other life-closure issues• Anticipatory mourning• The meaning of illness and the suffering it
creates

ENHANCING CONVERSATIONS• Interpersonal communication skills• Patient centered care
Mutual participation relationships• Informed choice• Patient autonomy
• Need to understand the meaning of illness for the patient
ENDEND--OFOF--LIFE CONVERSATIONSLIFE CONVERSATIONS

Preferences for Death vs. Conditions:Preferences for Death vs. Conditions:Patient Would Rather Die ThanPatient Would Rather Die Than
Spend All of the Time In:Spend All of the Time In:9090
8080
7070
6060
5050
4040
3030
2020
1010
00 6 mos. 6 mos. -- 3 mos.3 mos. 3 mos. 3 mos. -- 1 mo.1 mo. 1 mo. 1 mo. -- 3 days3 daysn=97n=97 n=109n=109 n=107n=107
VentilatorVentilator Feeding tubeFeeding tube Nursing homeNursing home
Levenson et al. JAGS, 2000; 48:5101.
Perc
ent

Levenson et al. JAGS, 2000; 48:5101.
Preferences for Death vs. Symptoms:Preferences for Death vs. Symptoms:Patient Would Rather Die ThanPatient Would Rather Die Than
Spend All of the Time In:Spend All of the Time In:9090
8080
7070
6060
5050
4040
3030
2020
1010
00 6 mos. 6 mos. -- 3 mos.3 mos. 3 mos. 3 mos. -- 1 mo.1 mo. 1 mo. 1 mo. -- 3 days3 daysn=97n=97 n=109n=109 n=107n=107
Perc
ent
PainPain ConfusionConfusion ComaComa

Levenson et al. JAGS, 2000; 48:5101.
Preferences for Care OverPreferences for Care OverThe Last 6 Months of LifeThe Last 6 Months of Life
8080
6060
4040
2020
00 6 mos. 6 mos. -- 3 mos.3 mos. 3 mos. 3 mos. -- 1 mo.1 mo. 1 mo. 1 mo. -- 3 days3 days
Perc
ent
n=217n=217n=222n=222
Comfort CareComfort CareDNRDNR
n=200n=200n=207n=207
n=155n=155n=159n=159
Prefers comfort care, P=.069Prefers comfort care, P=.069Prefers DNR, P=.017Prefers DNR, P=.017

• Balancing therapies:
AggressivePalliative
•Promoting:QOLA gooddeath
