original article follicular thyroid adenoma dominated … · surgical department of waldkrankenhaus...
TRANSCRIPT

Introduction Spindle cell lesions of the thyroid gland are quite rare. Besides rare miscellaneous benign and malignant primary mesenchymal tumors and tumor-like lesions [1], they encompass re-active spindle cell stromal proliferations (nodular fasciitis-like areas) in papillary thyroid carcinoma [2] and spindle cell variants of me-dullary [3], papillary [4] follicular [5,6] and anaplastic [7] carcinoma. Furthermore, spindle cell epithelial tumor with thymus-like elements (SETTLE) represents a rare but distinctive type of primary thyroid neoplasm with spindle cell morphology and significant metastatic potential [8]. In addition, a variety of rare mesenchymal tumors and tumor-like lesions may present in the thyroid [1]. However, the occurrence of ar-eas of bland-looking spindle cell metaplasia within benign thyroid nodules is quite uncom-mon and may be mistaken for a malignant or
metastatic neoplasm. Some earlier reports on “atypical” variants of follicular adenoma might have represented similar metaplastic lesions [9]. We encountered two unusual benign follicu-lar thyroid nodules (adenomas) that showed a predominance of spindle cells besides a minor follicular component and other unusual histo-logical features that we think merit brief de-scription. A thorough review of the available English literature revealed 14 well documented examples of this rare phenomenon [10-16]. The clinicopathological features of reported cases and our two cases are summarized in table 1 and discussed in more details in the discussion section. Case histories Case 1 In 2009, a 77-year-old woman presented to the
Int J Clin Exp Pathol 2012;5(2):143-151 www.ijcep.com /ISSN:1936-2625/IJCEP1202002
Original Article Follicular thyroid adenoma dominated by spindle cells: report of two unusual cases and literature review Abbas Agaimy1, Thomas Hahn2, Josef Schroeder3, Afaf Elhag4
1Institute of Pathology, University Hospital, 91054 Erlangen, Germany; 2Department of Surgery, Waldkrankenhaus, 91054 Erlangen, Germany; 3Institute of Pathology, University Hospital, 93053 Regensburg, Germany; 4Histopathol-ogy Department, Scarborough Hospital, North Yorkshire, YO12 6QL, UK. Received February 1, 2012; accepted February 9, 2012; Epub February 12, 2012; published February 28, 2012 Abstract: Primary spindle cell neoplasms of the thyroid gland are quite rare. They encompass a heterogeneous group of benign and malignant lesions of mesenchymal and epithelial origin. We herein describe two unusual follicular thy-roid adenomas dominated by spindle cells with occasional areas of colloid-forming follicular differentiation. The tu-mors affected a 77-year woman and a 70-year old man; both had a long-history of monoclonal gammopathy of un-known significance (MGUS). One tumor presented as a large cold thyroid nodule and the other was an autopsy find-ing. The tumors were predominantly composed of fibroblast-like spindled cells. One case showed prominent men-ingioma-like concentric perivascular arrangement and contained cytoplasmic melanin-like pigment. Stromal hyaliniza-tion was a prominent feature of both. By immunohistochemistry, the spindled cells expressed vimentin, pankeratin (KL1), thyroglobulin and TTF1 consistent with a follicular differentiation. They did not stain with calcitonin, CEA and other lineage-specific mesenchymal, neuroendocrine and melanocytic markers. There was no evidence of metastasis at autopsy (case 2) or at last follow-up 2 years after surgery (case 1). These cases demonstrate the diversity of follicu-lar thyroid neoplasms and the unusual occurrence of extensive spindle cell metaplasia. These uncommon lesions need to be distinguished from spindle cell medullary carcinoma, paucicellular spindle cell anaplastic carcinoma, spin-dle cell foci in papillary and follicular carcinoma, solitary fibrous tumor and other rare benign and malignant mesen-chymal lesions. Keywords: Spindle cell neoplasm, thyroid, follicular adenoma, TTF1, pigmented

Spindle thyroid adenoma
144 Int J Clin Exp Pathol 2012;5(2):143-151
surgical department of Waldkrankenhaus (Erlangen, Germany) with fatigue and difficulty with swallowing. Her medical history revealed a diagnosis of monoclonal gammopathy of un-known significance (MGUS; IgA-Kappa) since 2001 that did not necessitate medical treat-ment. She also has suffered from a chronic re-nal insufficiency (stage II; creatinine was 1.15 mg/dl). A bone marrow biopsy performed previ-ously confirmed the diagnosis of MGUS but there was no evidence of myeloma. Ultrasound examination of the abdominal organs revealed no pathological findings. A thorough clinical workup revealed no significant abnormal find-ings. Ultrasonographic evaluation of the thyroid gland showed a large non-homogenous nodule 6x4x3 cm in the caudal right lobe of the thyroid extending retrosternally and displacing the tra-chea to the left side. A radionucleotide scintigra-phy confirmed a cold nodule in the caudal right lobe. Based on suspicion of malignancy, the patient underwent bilateral thyroidectomy. She remained alive and well without evidence of recurrent disease or new neoplasms at last fol-low-up (2 years after surgery). Case 2 In 2011, a 70 years old male was admitted to the Accident and Emergency department of Scarborough Hospital/ UK after he collapsed at home. He died 5 hours later in the Intensive Care Unit. He had a history of hypertension, hy-percholesterolemia, left ventricular dysfunction, left nephrectomy for renal cell carcinoma in 2000 and inoperable prostatic carcinoma treated with chemotherapy in 2008. He was also diagnosed with MGUS in 2008. There was no evidence of myeloma. At Autopsy, the left thyroid lobe was largely oc-cupied by a 4x3 cm encapsulated tumor with dark tan cut-surface and extensive hemorrhage. The overlying thyroid capsule was intact and not infiltrated by the tumor. The right thyroid lobe looked normal. Material and methods Tissue specimens have been fixed in buffered formalin, embedded routinely and stained with Hematoxylin and Eosin for histological examina-tion. In addition, representative sections have been stained with Congo Red for amyloid, Prus-sian blue for hemosiderin pigment and Masson-Fontana to detect melanin pigment. Immunohis-
tochemistry was performed on 5 µm sections using a polymer Kit purchased from Zytomed (Zytomed systems Ltd., Berlin, Germany) accord-ing to the manufacturer’s instructions and the following antibodies: vimentin, pankeratin (KL-1), CK18, CK5, CD117, protein S100, epithelial membrane antigen (EMA), thyroglobulin, thyroid transcription factor-1 (TTF-1), polyclonal carci-noembryonic antigen (CEA), calcitonin, synapto-physin, chromogranin A, desmin, α-smooth mus-cle actin, CD34, CD31, CD99, GFAP, p53, Melan A, HMB45 and Ki67/Mib1. In Case 1, electron microscopy was performed on formalin-fixed paraffin-embedded tumor tissue as described previously [17]. Results Pathological findings: Case 1 The right lobe of the thyroid weighed 52 grams and measured 5.2 x3.1 x 1.2 cm. An encapsu-lated nodule 5.5 cm in maximum diameter was seen attached to the caudal part of the right lobe. The cut-surface of this nodule was dark brown (Figure 1A). The periphery of the nodule was separated from the thyroid parenchyma by a thin capsule. Thorough histological examina-tion (20 sections) showed a spindle cell prolif-eration with prominent and remarkably hyalin-ized blood vessels with evidence of thrombosis and recurrent bleeding (Figure 1B). There was a remarkable component of slender dendritic-like spindle cells that forms both organized fascicles and haphazardly arranged aggregates (Figure 1C), occasionally encasing blood vessels in an onion-skin pattern (Figure 1D). Several spindle cells contained granular dark pigment reminis-cent of melanin (Figure 1D). This pigment was Prussian blue negative and Masson-Fontana positive suggesting melanin pigment. Amid these spindle cell areas were scattered and aggregated colloid-filled thyroid follicles (Figure 1C). Prussian blue stain displayed significant stromal hemosiderin in the interstitium and within macrophages. Congo Red stain demon-strated no amyloid deposits. Cellular atypia, coagulative necrosis, infiltrative growth and mi-totic activity were absent. Immunohistochemis-try revealed diffuse and strong expression of vimentin, pankeratin (KL1) (Figure 1E), cy-tokeratin 18, thyroglobulin (Figure 1F) and TTF-1 (Figure 1G) in both spindle cells and en-trapped follicles. The spindle cells were nega-tive for all other markers listed above in the

Spindle thyroid adenoma
145 Int J Clin Exp Pathol 2012;5(2):143-151
method section. The proliferation index (Ki67/Mib-1) was below 1% (almost zero). The left lobe showed benign nodular goiter without evidence of pigmentation or a spindle cell component. Electron microscopy on formalin-fixed paraffin
embedded tumor tissue showed dense osmo-philic material present within the lysosomes of the spindle cells consistent with the pigment seen on H&E stained sections. Melanosomes or premelanosomes were not detected (Figure 2).
Figure 1. Pathological features of case 1. A: cross section showed varied coloration with black and light areas. B: prominent vascular thrombosis amid a spindle cell proliferation. C: compact aggregates of oval to spindled cells with intervening sclerosis and scattered colloid-containing follicles. D: onion skin pattern surrounding thick-walled vessels, note dark cytoplasmic pigment in some of the spindle cells. E: KL1 (pankeratin) highlighted spindle cells in a lamellar arrangement. F (thyroglobulin) and G (TTF-1) highlighted the onion-skin pattern around vessels.

Spindle thyroid adenoma
146 Int J Clin Exp Pathol 2012;5(2):143-151
Pathological findings: Case 2 The entire left thyroid lobe was processed for microscopic examination. It was almost com-pletely replaced by a encapsulated lesion com-posed mostly of spindle cells in fascicles, whorls and singly in addition to occasional solid nod-ules of cuboidal cells and scattered aggregates of follicular cells occasionally forming colloid (Figure 3A). The spindle cells were plump and slender with, mostly, vesicular nuclei, incon-spicuous nucleoli and eosinophilic cytoplasm. Bizarre, degenerative hyperchromatic spindle cells were seen in areas of extensive hyaliniza-tion (Figure 3B) but there were no mitoses or foci of necrosis. A few macro- and micro-follicles were present interspersed among the spindle cells. A remarkable feature was the presence of focal solid aggregates of spindle cells within a rich stromal vascularity closely mimicking a vas-cular lesion (Figure 3C, D) amid stromal hyalini-zation with focal calcifications. Examination of Congo Red-stained sections under polarized light demonstrated the presence of apple green birefringent deposits of amyloid in blood ves-sels’ wall. The background thyroid parenchyma showed no amyloid. There were no nuclear fea-tures of papillary carcinoma. Immunohistochem-istry showed almost identical findings as in case
1 with strong and diffuse staining for vimentin (Figure 3E), KL-1 and CK18 (Figure 3F) in the spindle cells and variable (less extensive than case 1) staining for thyroglobulin (20% tumor cells), TTF-1 (10%) and CK7 (10%). All other markers listed above were negative (Figure 3G). The proliferation index (Ki67/Mib-1) was well below 1%. The cause of death of the patient was cardiac amyloidosis which was part of sys-temic amyloidosis as illustrated by histopa-thological examination of other organs. Discussion Because of their rarity, spindle cell thyroid le-sions may be challenging. Careful exclusion of unusual and paucicellular spindle cell variants of common thyroid cancer is of utmost impor-tance for appropriate therapy and prognosis. Medullary carcinoma not uncommonly displays spindle cell morphology, infiltrates between thy-roid follicles and rarely shows melanin pigment [18]. However, unlike our cases, medullary car-cinoma usually shows higher cellularity, clear-cut malignant features and immunoreactivity with calcitonin and/or CEA [3]. Amyloid deposits in our case 2 were vascular (part of systemic amyloidosis) in contrast to the isolated stromal amyloid seen in medullary carcinoma.
Figure 2. Left: Electron microscopy in case 1 showed elongated cells with vesicular occasionally indented nuclei sur-rounded by abundant dense osmophilic intracytoplasmic material corresponding to the pigment seen on H&E stain. Right: At higher resolution, this pigment displayed amorphic structure with intervening degenerating organelles. No melanosomes or premelanosomes were seen.
Spindle thyroid adenoma
147 Int J Clin Exp Pathol 2012;5(2):143-151
Anaplastic carcinoma is an important considera-tion in elderly patients with spindle cell thyroid mass. While diagnosis of classical anaplastic carcinoma poses no diffculty, a rare paucicellu-lar spindle cell variant of anaplastic carcinoma has been described [7]. Although bland looking, this unusual variant displays similar permeation and plugging of arteries by tumor cells as seen
in conventional anaplastic carcinoma and the clinical course seems to be similarly aggressive. Spindle cell thyroid lesions may represent di-rect extension of neoplasms within adjacent cervical soft tissue, the proximal esophagus or the larynx [19]. These include in particular spin-dle cell carcinoma, desmoid fibromatosis and
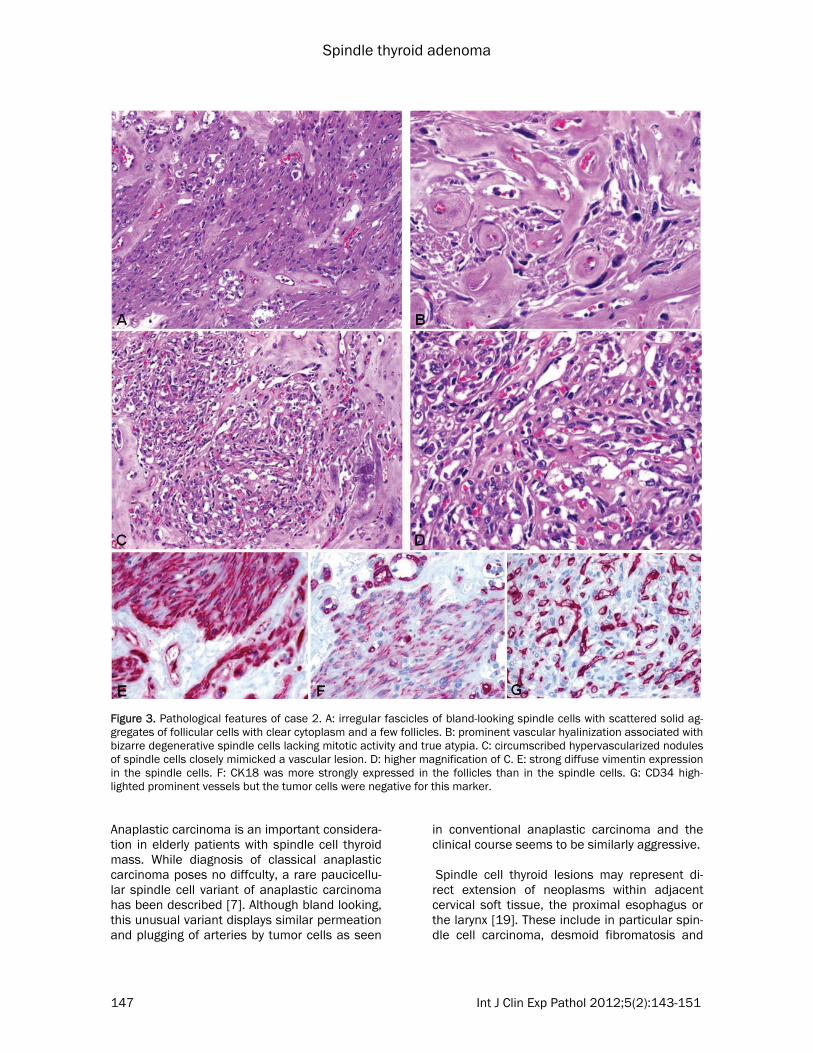
Figure 3. Pathological features of case 2. A: irregular fascicles of bland-looking spindle cells with scattered solid ag-gregates of follicular cells with clear cytoplasm and a few follicles. B: prominent vascular hyalinization associated with bizarre degenerative spindle cells lacking mitotic activity and true atypia. C: circumscribed hypervascularized nodules of spindle cells closely mimicked a vascular lesion. D: higher magnification of C. E: strong diffuse vimentin expression in the spindle cells. F: CK18 was more strongly expressed in the follicles than in the spindle cells. G: CD34 high-lighted prominent vessels but the tumor cells were negative for this marker.

Spindle thyroid adenoma
148 Int J Clin Exp Pathol 2012;5(2):143-151
rare miscellaneous sarcomas. Desmoid fibro-matosis may rarely arise within the thyroid gland and should be excluded by appropriate histo-logical features and staining for alpha-smooth muscle actin and nuclear staining with beta-catenin. Rare papillary carcinomas may be asso-ciated with an exuberant spindle cell mesenchy-mal fibroblastic/myofibroblastic proliferation forming short fascicles separated by edematous stroma, collagen and foci of hemorrhage [1, 2]. These spindle cells do not stain for keratins and thyroglobulin but instead show myofibroblastic or fibroblastic phenotypes [1, 2]. Metaplastic spindle cell foci have been rarely observed in papillary carcinoma and microinvasive follicular carcinoma [10,16]. These metaplastic foci occa-sionally show similar nuclear features as the basic neoplasm and they express marker of follicular cells and lack myofibroblastic differen-tiation. Thus, in such cases, the background follicular component should be carefully exam-ined for nuclear and architectural features of papillary carcinoma and excessive sectioning of the tumor capsule is necessary to exclude inva-sion as evidence of follicular carcinoma. A rare pure spindle cell follicular carcinoma has also been described but, by definition, this rare vari-ant shows clear-cut capsular and vascular inva-sion [5]. Fine needle aspiration (FNA)-associated nodule of the thyroid is another consideration [20]. Di-agnosis of this lesion is based on a recent his-tory of FNA and the characteristic florid fibro-/myofibroblastic reaction associated with eryth-rocyte extravasation and hemorrhages. SETTLE tumors are usually composed of lobules of spin-dle cells intermixed with tubulopapillary epithe-lial component. These rare neoplasms are defi-nitionally keratin positive but they lack follicular line of differentiation (thyroglobulin and TTF-1 negative) [8]. Riedel’s thyroiditis is character-ized by paucicellular highly collagenized tissue with variable but generally prominent plasma-cell rich inflammatory infiltrate and associated obliterative phlebitis without atypia. Rare sar-coma metastasis to multinodular goiter may result into similar histology as our cases and should be carefully excluded by history of sar-coma, malignant cytology and lack of follicular differentiation [21]. Including our cases, 16 well documented be-nign thyroid nodules with spindle cell metapla-sia/component have been reported (Table 1). They affected 10 women and 6 men at a mean
age of 55 yrs (range, 27-77). Histology of the epithelial component corresponded to follicular adenoma (n=10) and multinodular goiter (n=6). The size of the spindle cell foci ranged from 2 mm to several centimeters. They constituted from 1% to >95% of the background nodule. In a few cases, the lesion was so dominated by spindle cells that the follicular nature was diffi-cult to establish [10,13,16]. Histologically, the spindle cell areas showed either a nodular or diffuse pattern or a combination thereof. They uniformly expressed vimentin, pankeratin, thy-roglobulin and TTF-1 but did not stain for high molecular weight keratins, CD34, calcitonin, smooth muscle and myofibroblastic markers. The spindle cells in our case 1 and in the case reported by Magro et al [13] showed peculiar meningioma-like concentric whorls surrounding numerous thick-walled hyalinized blood vessels. Interestingly, all reports including our cases showed a Ki67 index of <1% indicating that these benign nodules containing metaplastic spindle cells are non-proliferative lesions. This finding is of great value in excluding malignant spindle cell lesions including primary and me-tastatic carcinomas and sarcomas. Our cases and previous reports are consistent with previ-ous observation that cells of papillary carci-noma and follicular adenoma may assume a fibroblast-like morphology in tissue cultures but maintain reactivity with cytokeratin, thyroglobu-lin, and vimentin suggesting epithelial-mesenchymal transition [22]. Two further findings in our cases merit short comments. The black discoloration of one case showed ultrastructural features consistent with black thyroid induced by long-term use of mino-cycline [23]. However, the pigmentation in our case was restricted to the tumor and absent in the background thyroid, thus representing the opposite situation as would be expected in mi-nocycline-induced pigmentation [23]. However, rare cases of black adenoma associated with minocycline therapy have been reported [24]. The pigment in black thyroid is positive with the Fontana-Masson stain, negative with iron stain and can be bleached with potassium permanga-nate suggesting a melanin-like pigment [24]. Electron microscopic examination failed to dem-onstrate melanosomes or premelanosomes [24], similar to our case. Our patient had no recent history of minocycline intake but informa-tion regarding the remote drug history was in-conclusive. A remarkable but unexplained ob-servation in our 2 cases is the concurrence of

Spindle thyroid adenoma
149 Int J Clin Exp Pathol 2012;5(2):143-151
Table 1. Clinicopathological features of reported benign thyroid follicular nodules with spindle cell metaplasia (n=16) No Author/ref. Age/
Sex Histological type
Size whole nodule cm
Size spindle cell areas cm
Spindle cell pattern
TTF1 TG CK Vimentin CD34/ SMA
Other findings/ diseases Follow-up
1 Vergilio et al [10]
71 M Follicular adenoma
NA 1 cm Diffuse (˃95%)
ND + ND ND ND No follow-up
2 Vergilio et al [10]
45 F Follicular adenoma
NA >3 cm (~95%)
diffuse ND + ND ND ND No follow-up
3 Vergilio et al [10]
33 F Follicular adenoma
NA NA (~95%) diffuse ND + - ND ND No follow-up
4 Aker et al [11]
27 F Follicular adenoma
4 cm ~90% Diffuse ND + Focal + + - Alive & well 15 months
5 Magro et al [12]
54 M Multinodular goiter
n.s. 1.5 cm Nodular n.s. + Focal + + - Bizarre hyperchromatic cells, No follow-up
6 Magro et al [13]
69 F Follicular adenoma
5 cm ~90% Nodular + + + + - Transitional meningioma-like pattern, 1 yr alive and well
7 Shikama et al [14]
60 F Follicular adenoma
3.2 cm ~50% Nodular + + - + - No follow-up
8 Hirokawa et al [15]
56 F Multinodular goiter
n.s. 2 cm Nodular + + + ND CD34- No follow-up
9 Hirokawa et al [15]
65 F Multinodular goiter
0.3 cm 50% Diffuse + + + ND CD34- Concurrent multifocal papillary carcinoma , no follow-up
10 Hirokawa et al [15]
50 M Multinodular goiter
5.7 cm n.s. Diffuse & nodular
+ + - ND CD34- No follow-up
11 Matoso et al [16]
43 F Multinodular goiter
n.s. 0.2-1.5 cm Nodular + + - + SMA- No follow-up
12 Matoso et al [16]
49 M Multinodular goiter
n.s. 0.2-1.5 cm Diffuse + + + + SMA- No follow-up
13 Matoso et al [16]
62 M Follicular adenoma
n.s. 0.2-1.5 cm Diffuse + + + + SMA- No follow-up
14 Matoso et al [16]
57 F Follicular adenoma
n.s. 0.2-1.5 cm Diffuse + + + + SMA- No follow-up
15 Current case 1
77 F Follicular adenoma
5.5 cm ~80% Diffuse + + + + - Monoclonal gammopathy since 8 yrs Alive and well at 2 yrs
16 Current case 2
70 M Follicular adenoma
Whole right lobe
>50% Diffuse & nodular
+ + + + - Bizarre hyperchromatic cells, Monoclonal gammopathy since 3 yrs. Autopsy case
NA, not available; ND, not done; n.s., not specified; ; CK, cytokeratin, SMA, smooth muscle actin.

Spindle thyroid adenoma
150 Int J Clin Exp Pathol 2012;5(2):143-151
the lesions with MGUS in both. Although this might be a mere coincidence, it is unusual and worth mentioning given the relative rarity of MGUS and the strictly rare occurrence of spin-dle cell follicular adenoma. Yativ et al found that anti-thyroglobulin antibodies were more fre-quent among patients with IgG gammopathy, although these patients had no clinical or bio-chemical evidence of thyroid disease [25]. An-other report described a patient with MGUS who subsequently developed thyrotoxicosis, pretibial myxedema and thyroid-associated ophthalmo-pathy [26]. The authors postulated that the MGUS could be the cause of the subsequently observed thyroid pathology [26]. In summary we described further two cases of spindle cell follicular adenoma of the thyroid expanding their morphological spectrum and depicting potential diagnostic pitfalls related to this rare findings. Address correspondence to: Abbas Agaimy, MD, Pathologisches Institut, Universitätsklinikum Erlangen, Krankenhausstraße 8-10, 91054 Erlangen, Germany/. Tel: +49-9131-85-22288, Fax: +49-9131-85-24745, E-mail: [email protected] References [1] Papi G, Corrado S, LiVolsi VA. Primary spindle
cell lesions of the thyroid gland; an overview. Am J Clin Pathol 2006;125 Suppl:S95-123.
[2] Chan JK, Carcangiu ML, Rosai J. Papillary carci-noma of thyroid with exuberant nodular fasciitis-like stroma. Report of three cases. Am J Clin Pathol 1991;95:309-14.
[3] Papotti M, Sambataro D, Pecchioni C, Bussolati G. The pathology of medullary carcinoma of the thyroid: Review of the literature and personal experience on 62 Cases. Endocr Pathol 1996;7:1-20.
[4] Brandwein-Gensler MS, Wang BY, Urken ML. Spindle cell transformation of papillary carci-noma: an aggressive entity distinct from anaplastic thyroid carcinoma. Arch Pathol Lab Med 2004;128:87-9.
[5] Giusiano-Courcambeck S, Denizot A, Secq V, De Micco C, Garcia S. Pure spindle cell follicular carcinoma of the thyroid. Thyroid 2008;18:1023-5.
[6] Mizukami Y, Nonomura A, Michigishi T, Noguchi M, Ishizaki T. Encapsulated follicular thyroid carcinoma exhibiting glandular and spindle cell components. A case report. Pathol Res Pract 1996;192:67-71.
[7] Wan SK, Chan JK, Tang SK. Paucicellular vari-ant of anaplastic thyroid carcinoma. A mimic of Reidel's thyroiditis. Am J Clin Pathol
1996;105:388-93. [8] Folpe AL, Lloyd RV, Bacchi CE, Rosai J. Spindle
epithelial tumor with thymus-like differentia-tion: a morphologic, immunohistochemical, and molecular genetic study of 11 cases. Am J Surg Pathol 2009;33:1179-86.
[9] Hazard JB, Kenyon R. Atypical adenoma of the thyroid. Arch Pathol 1954;58:554–563.
[10] Vergilio J, Baloch ZW, LiVolsi VA. Spindle cell metaplasia of the thyroid arising in association with papillary carcinoma and follicular ade-noma. Am J Clin Pathol 2002;117:199-204.
[11] Aker FV, Bas Y, Ozkara S, Peker O. Spindle cell metaplasia in follicular adenoma of the thyroid gland: case report and review of the literature. Endocr J 2004;51:457-61.
[12] Magro G, Torrisi A, Torrisi A. Atypical/bizarre spindle cell epithelial metaplasia in nodular goiter: a potential diagnostic pitfall. Virchows Arch 2005;446:91–92.
[13] Magro G, Benkova K, Michal M. Meningioma-like tumor of the thyroid: a previously unde-scribed variant of follicular adenoma. Virchows Arch 2005;446:677-9.
[14] Shikama Y, Mizukami H, Sakai T, Yagihashi N, Okamoto K, Yagihashi S. Spindle cell metaplasia arising in thyroid adenoma: characterization of its pathology and differential diagnosis. J Endocrinol Invest 2006;29:168-71.
[15] Hirokawa M, Haba R, Kushida Y, Bando K, Kuma S, Kihara M, Miyauchi A. Benign nodular goiter with spindle cell component. Pathol Int 2010;60:586-90.
[16] Matoso A, Easley SE, Mangray S, Jacob R, Delellis RA. Spindle cell foci in the thyroid gland: an immunohistochemical analysis. Appl Immunohistochem Mol Morphol 2011;19:400-7.
[17] Agaimy A, Wünsch PH, Schroeder J, Gaumann A, Dietmaier W, Hartmann A, Hofstaedter F, Mentzel T. Low-grade abdominopelvic sarcoma with myofibroblastic features (low-grade myofi-broblastic sarcoma): clinicopathological, immu-nohistochemical, molecular genetic and ultra-structural study of two cases with literature review. J Clin Pathol 2008;61:301-6.
[18] Beerman H, Rigaud C, Bogomoletz WV, Hollander H, Veldhuizen RW. Melanin production in black medullary thyroid carcinoma (MTC). Histopathology 1990;16:227-33.
[19] Nakhjavani M, Gharib H, Goellner JR, Heerden JA. Direct extension of malignant lesions to the thyroid gland from adjacent organs: report of 17 cases. Endocr Pract 1999;5:69-71.
[20] Baloch ZW, Wu H, LiVolsi VA. Post-fine-needle aspiration spindle cell nodules of the thyroid (PSCNT). Am J Clin Pathol 1999;111:70-4.
[21] Khadilkar UN, Lobo FD, Shahabuddin MD, Shetty A, Kini A. Sarcoma seeding to multinodu-lar goitre--a diagnostic dilemma. Cytopathology

Spindle thyroid adenoma
151 Int J Clin Exp Pathol 2012;5(2):143-151
1999;10:360-1. [22] Herrmann ME, Trevor KT. Epithelial-
mesenchymal transitions during cell culture of primary thyroid tumors? Genes Chromosomes Cancer 1993;6:239-242.
[23] Kang SW, Hong SW, Yeon PJ, Jeong JJ, Sung TY, Lee SC, Lee YS, Nam KH, Chung WY, Chang HS, Park CS. A case of black thyroid associated with hyalinizing trabecular tumor. Endocr J 2008;55:1109-12.
[24] Koren R, Bernheim J, Schachter P, Schwartz A, Siegal A, Gal R. Black thyroid adenoma. Clinical, histochemical, and ultrastructural features. Appl Immunohistochem Mol Morphol 2000;8:80-4.
[25] Yativ N, Buskila D, Blank M, Burek CL, Rose NR, Shoenfeld Y. The detection of antithyroglobulin activity in human serum monoclonal immu-noglobulins (monoclonal gammopathies). Immunol Res. 1993;12:330-7.
[26] Tonacchera M, Costagliola S, Cetani F, Ducobu J, Stordeur P, Vassart G, Ludgate M. Patient with monoclonal gammopathy, thyrotoxicosis, pretibial myxedema and thyroid-associated ophthalmopathy; demonstration of direct bind-ing of autoantibodies to the thyrotropin recep-tor. Eur J Endocrinol 1996;134:97-103.