open reduction and internal fixation of a severely displaced midshaft clavicle fracture
TRANSCRIPT

Open Reduction and
Internal Fixation of a Severely Displaced
Midshaft Clavicle Fracture
I M A G E S
Author: Magdalena Gonzalez, PA-C, MMS, Hollywood, Fla
Section Editor: Sally Bragg, RN, MSN, CCRC
Magdalena Gonzalez is Physician Assistant, Division of TraumaServices, Memorial Regional Hospital, Hollywood, Fla.
For correspondence, write: Sally Bragg, RN, MSN, CCRC, Centerfor Bioterrorism and All-hazards Preparedness, Nova SoutheasternUniversity, 3434 S University Drive, Fort Lauderdale-Davie, FL 33328;E-mail: [email protected].
J Emerg Nurs 2007;33:152-3.
0099-1767/$32.00
Copyright n 2007 by the Emergency Nurses Association.
doi: 10.1016/j.jen.2007.01.006
152
istorically, clavicle fractures have been treated
Hnonoperatively and with good functional out-
comes via a figure of eight brace or sling. Surgical
interventions are reserved for clavicle fractures associated
with neurovascular injuries; glenoid/scapula fractures re-
sulting in a ‘‘f loating arm’’; severe displaced fracture; or
open clavicle fractures. Complications of clavicle fractures
may include pnuemothorax, hemothorax, and injury to the
brachial plexus or subclavian vessels.1 Because of renewed
interest and patient dissatisfaction related to prolonged re-
covery periods, recent advances have been made in the fix-
ation of clavicle fractures with placement of locking plates
or intramedullary rods.
A 39-year-old female patient was seen after a storage
shelf fell onto the right side of her body. Initial work-
up revealed a severely displaced grade I midshaft clavicle
fracture (Figure 1). The patient’s upper right extremity neuro-
vascular status remained, and she underwent an open re-
duction and internal fixation (Figure 2). Postoperatively,
the patient was transferred to a rehabilitation unit follow-
ing an uneventful hospital course and early physical therapy.
A recent paper presented at the American Academy of
Orthopedic Surgeons concluded that patients who under-
went open reduction and internal fixation of severely dis-
placed clavicle fractures had statistically significant clinical
and functional improvement compared with patients who
were treated without surgical intervention and in a con-
servative manner.2 Another study concluded that acute ver-
sus delayed fixation showed similar restoration of objective
muscle strength but demonstrated significant loss in mus-
cle endurance in patients with delayed fixation.3
JOURNAL OF EMERGENCY NURSING 33:2 April 2007
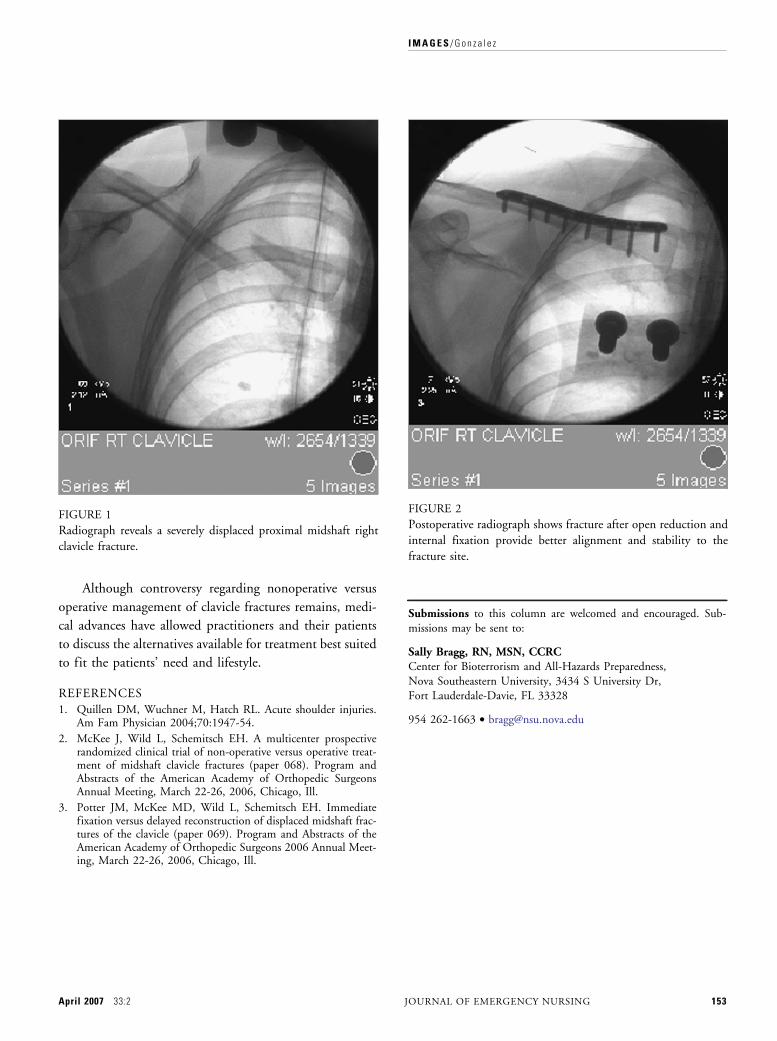
FIGURE 2
Postoperative radiograph shows fracture after open reduction and
internal fixation provide better alignment and stability to the
fracture site.
FIGURE 1
Radiograph reveals a severely displaced proximal midshaft rightclavicle fracture.
I M A G E S / G o n z a l e z
Although controversy regarding nonoperative versus
operative management of clavicle fractures remains, medi-
cal advances have allowed practitioners and their patients
to discuss the alternatives available for treatment best suited
to fit the patients’ need and lifestyle.
REFERENCES
1. Quillen DM, Wuchner M, Hatch RL. Acute shoulder injuries.Am Fam Physician 2004;70:1947-54.
2. McKee J, Wild L, Schemitsch EH. A multicenter prospectiverandomized clinical trial of non-operative versus operative treat-ment of midshaft clavicle fractures (paper 068). Program andAbstracts of the American Academy of Orthopedic SurgeonsAnnual Meeting, March 22-26, 2006, Chicago, Ill.
3. Potter JM, McKee MD, Wild L, Schemitsch EH. Immediatefixation versus delayed reconstruction of displaced midshaft frac-tures of the clavicle (paper 069). Program and Abstracts of theAmerican Academy of Orthopedic Surgeons 2006 Annual Meet-ing, March 22-26, 2006, Chicago, Ill.
April 2007 33:2
Submissions to this column are welcomed and encouraged. Sub-missions may be sent to:
Sally Bragg, RN, MSN, CCRCCenter for Bioterrorism and All-Hazards Preparedness,Nova Southeastern University, 3434 S University Dr,Fort Lauderdale-Davie, FL 33328
954 262-1663 . [email protected]
JOURNAL OF EMERGENCY NURSING 153