observational study comparing long-term safety and efficacy of deferasirox with desferrioxamine...
TRANSCRIPT

Observational study comparing long-term safety and efficacyof Deferasirox with Desferrioxamine therapy in chelation-naıve children with transfusional iron overloadYesim Aydinok1, Sule Unal2, Yesim Oymak3, Canan Vergin3, Zeynep D. Turker4, Dilek Yildiz1,Akif Yesilipek4
1Department of Pediatric Hematology, Ege University Faculty of Medicine, Izmir; 2Department of Pediatrics, Antakya State Hospital, Antakya;3Department of Pediatric Hematology, Behcet Uz Children’s Hospital, Izmir; 4Department of Pediatric Hematology, Akdeniz University Faculty of
Medicine, Antalya, Turkey
Transfusion-dependent children with congenital blood
disorders rapidly develop potentially damaging levels of
iron overload in the body during early childhood (1).
Excess iron from transfusions initially invades the liver
but later spreads to the heart and endocrine organs lead-
ing to organ failures if not controlled and eliminated by
chelation therapy (2). The implementation of iron chela-
tion therapy in the late 1970s has resulted in a significant
decline in early cardiac deaths and endocrine complica-
tions of iron overload in patients with thalassemia major
(TM) (3). Growth deceleration and pubertal failure are
the earliest consequences of iron toxicity resulting from
pituitary iron deposition and may be prevented by main-
taining body iron at safe levels at all times.
Principles of chelation practice in infancy and child-
hood have been determined based on experience with
Desferrioxamine (DFO), the first chelator available.
Intensive chelation therapy starting at or close to the
time when a transfusion program was initiated to prevent
iron toxicity resulted in chelator toxicity such as
impaired growth and skeletal changes (4). In conse-
quence of this observation, chelation therapy has been
Abstract
Objectives: An observational study was conducted to explore postmarketing safety and efficacy of Defer-
asirox (DFX) in comparison with conventional Desferrioxamine (DFO) in chelation-naıve children with trans-
fusional iron overload. Methods: Transfusion-dependent children (aged £5 yr) who had serum ferritin
above 1000 lg ⁄ L and had been prescribed either first-line DFX or DFO for at least 12 months to maintain
serum ferritin between 500 and 1000 lg ⁄ L were included. Initial DFX dose was 20 mg ⁄ kg ⁄ d for 7 d a
week, and DFO dose was 25–35 mg ⁄ kg ⁄ d subcutaneously, given for 5 d a week. Dose adjustments were
based on serum ferritin changes and safety markers. The primary efficacy endpoint was change in serum
ferritin from baseline. The effect of transfusional iron loading rate (ILR) and different doses of chelators on
serum ferritin was also assessed. Results: A total of 111 patients were observed for a median of 2.29 yr
on DFX (n = 71) and 2.75 yr on DFO (n = 40). Absolute change in serum ferritin from baseline to the last
available observation was not significant with DFX (91 lg ⁄ L, P = 0.5) but significantly higher with DFO
(385 lg ⁄ L, P < 0.005). ILR and DFX doses had a major impact on serum ferritin changes in DFX cohort.
The height- and weight-standard deviation scores did not differ significantly in both cohorts during the
study. Fluctuations in liver enzymes and non-progressive increase in serum creatinine were the most
common adverse events (DFX; 9.8%, 18.0% and DFO; 5.0%, 7.5%, respectively). Conclusion: DFX is well
tolerable and at least as effective as DFO to maintain safe serum ferritin levels and normal growth
progression in chelation-naıve children.
Key words thalassemia major; iron overload; iron chelation; Desferrioxamine; Deferasirox
Correspondence Yesim Aydinok, Department of Pediatric Hematology, Ege University Faculty of Medicine, 35100 Bornova, Izmir,
Turkey. Tel: +90 532 3962746; Fax: +90 232 3438090; e-mail: [email protected]
Accepted for publication 8 February 2012 doi:10.1111/j.1600-0609.2012.01769.x
ORIGINAL ARTICLE
European Journal of Haematology 88 (431–438)
ª 2012 John Wiley & Sons A/S 431

initiated after 10–20 red cell transfusions once serum fer-
ritin exceeds 1000 lg ⁄L, and this recommendation has
also been applied to the other chelators. Chelation ther-
apy is administered to maintain serum ferritin levels
between 500 and 1000 lg ⁄L (1).
Although Deferasirox (DFX) was approved by FDA
for the treatment of patients with transfusional iron
overload who were older than 2 yr of age as first-line
therapy, it is important to assess postmarketing long-
term efficacy and safety of DFX in this group of small
children. This study aimed to explore whether DFX
therapy provides acceptable chelation and tolerability
compared with DFO in chelation-naıve children with
transfusional iron overload up to 5 yr.
Design and methods
This multicenter observational study was conducted in
four thalassemia centers in Turkey. Permission for retro-
spective review of medical records according to the
Declaration of Helsinki was approved by the IRB
Committee of Ege University Faculty of Medicine
(number: 11-11.1 ⁄ 62).
Inclusion and exclusion criteria
Transfusion-dependent (more than eight transfusions
annually) male and female children (aged £5 yr) who
were in need for chelation therapy based on serum ferri-
tin levels (‡1000 lg ⁄L) after 2003 and have been pre-
scribed either DFX or DFO as first-line therapy and
received either chelator for at least 12 months were
recruited into the study. Patients whose first-line chelator
has been switched to another chelating agent or stopped
for any reason (e.g., stem cell transplantation) were with-
drawn from the study.
Treatment and study design
This study is an observational study in which chelation-
naıve patients were initiated either DFX or DFO treat-
ment by their hematologists’ judgment based on family
interview and availability of either chelators. Initial DFX
dose was 20 mg ⁄kg ⁄d, once daily, 7 d ⁄wk in accordance
with the DFX-prescribing information. Dose titration of
DFX has been performed based on serum ferritin levels
and safety markers in steps of 5–10 mg ⁄kg ⁄d (in the
range of 0–40 mg ⁄kg ⁄d). DFO has been prescribed at
25–35 mg ⁄kg ⁄d as 8–12 h subcutaneous infusion, 5 d a
week in accordance with the guidelines for DFO dosing
in children (1). DFO doses were adjusted based on serum
ferritin levels and by considering safety markers up to
50 mg ⁄kg ⁄d.
The primary efficacy endpoint was the change in
serum ferritin from baseline. Serum ferritin levels were
evaluated monthly. Absolute change in serum ferritin
levels from baseline to final measurement for each sub-
ject was taken into consideration. The mean serum ferri-
tin levels at each completed chelation year were taken as
the average of available measurements during 1-yr per-
iod. Change in serum ferritin levels from baseline to each
chelation year for each subject was also evaluated. Safety
was evaluated by continuous monitoring for adverse
events as well as by laboratory assessments for hepatic
and renal toxicity and physical examination. Pediatric
growth was assessed by monitoring changes in height
and weight at 3-monthly intervals, expressed as height-
and weight-standard deviation scores (h-SDS and
w-SDS, respectively) at yearly intervals. h-SDS of
patients was calculated against the median height relative
to age for a non-thalassemia population, and median
change in h-SDS from baseline to each chelation year
was evaluated. The iron loading rate (ILR) as mg ⁄kg ⁄dwas calculated in each chelation year from transfusional
volumes of six consecutive transfusions and corrected for
hematocrit to obtain pure red blood cell (RBC) volume
that was multiplied by 1.08 (mg iron ⁄mL pure RBC) and
then divided by the days between the first and the last
transfusion and kg b.w. of patients. The corresponding
mean hemoglobin values (g ⁄dL) per chelation year were
also calculated.
Statistical analysis
Statistical analysis was performed using spss 13.0 for
Windows (SPSS Inc., Chicago, IL, USA). For continuous
variables, descriptive statistics were obtained, and com-
parisons were made using corresponding nonparametric
approaches (Mann–Whitney U-test, Wilcoxon signed
ranks test) or the two-sided independent and paired sam-
ples t-test when appropriate. The data obtained from
each chelation year with either chelator were compared
whenever the number of patients per chelation year was
sufficient for comparison. The last available observation
data of the patients were compared with their baseline
values regardless of the duration of chelation. A P value
of <0.05 was considered significant.
Results
Baseline characteristics of patients
A total of 123 children met the eligibility criteria and
received either DFX or DFO. Although most of the
chelation-naıve patients were prescribed DFX after the
registration of DFX in Turkey in 2007, few patients
who have already been initiated first-line DFX chelation
Deferasirox in chelation naive children Aydinok et al.
432 ª 2012 John Wiley & Sons A/S
as subjects of a phase III study (CL670107) in 2003 or
as part of compassionate use program under the super-
vision of the Turkey Ministry of Health in 2004 were
also included. A total of 111 patients (n = 106 TM
and n = 5 sickle cell disease) whose medical records
were complete for data collection were included in this
observational study. Table 1 shows descriptive statistics
of the two groups. The median time from first transfu-
sion to first initiation of chelation was substantially
longer in the DFO group as compared to the DFX
group. In line with this observation, baseline median
serum ferritin, alanin aminotransferase (ALT), and
aspartate aminotransferase (AST) values were also
significantly higher in the DFO group. The median time
on both chelators was comparable with 2.75 yr (range
1.0–6.1 yr) for a total of 109.33 patient-years on DFO
and 2.29 yr (range 1.0–7.0) for a total of 183.25
patient-years on DFX. The number of patients per che-
lation period (‡1, 2, 3, 4, or 5 yr) was comparable
between the treatment groups for the first four
chelation years.
Transfusional iron loading rates, average meanhemoglobin, and exposure to treatment
The mean ILR averaged at ranges between 0.3 and
0.4 mg ⁄kg ⁄d and the mean hemoglobin values main-
tained at 8.7–8.8 g ⁄dL throughout the years in both
study groups and did also not vary significantly through-
out the years within each chelation group. However,
although the mean actual DFX dose was similar
throughout the years, a continuous and significant
increase in DFO doses was observed during the years
(P = 0.003) (Table 2).
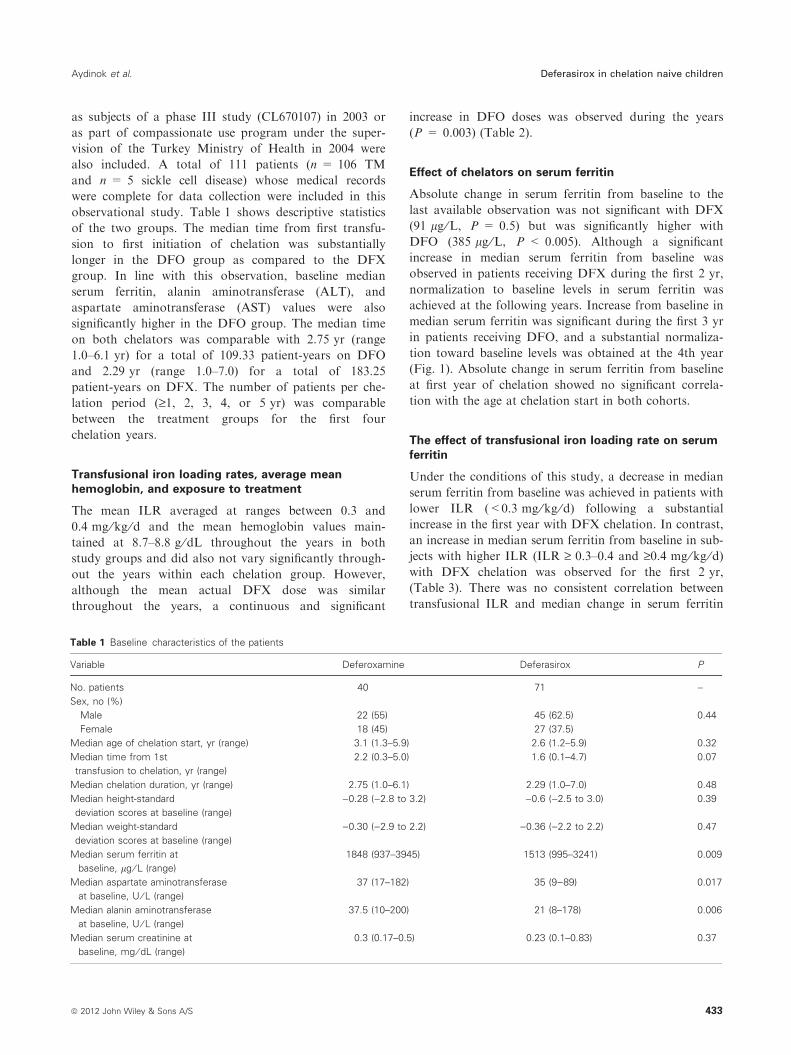
Effect of chelators on serum ferritin
Absolute change in serum ferritin from baseline to the
last available observation was not significant with DFX
(91 lg ⁄L, P = 0.5) but was significantly higher with
DFO (385 lg ⁄L, P < 0.005). Although a significant
increase in median serum ferritin from baseline was
observed in patients receiving DFX during the first 2 yr,
normalization to baseline levels in serum ferritin was
achieved at the following years. Increase from baseline in
median serum ferritin was significant during the first 3 yr
in patients receiving DFO, and a substantial normaliza-
tion toward baseline levels was obtained at the 4th year
(Fig. 1). Absolute change in serum ferritin from baseline
at first year of chelation showed no significant correla-
tion with the age at chelation start in both cohorts.
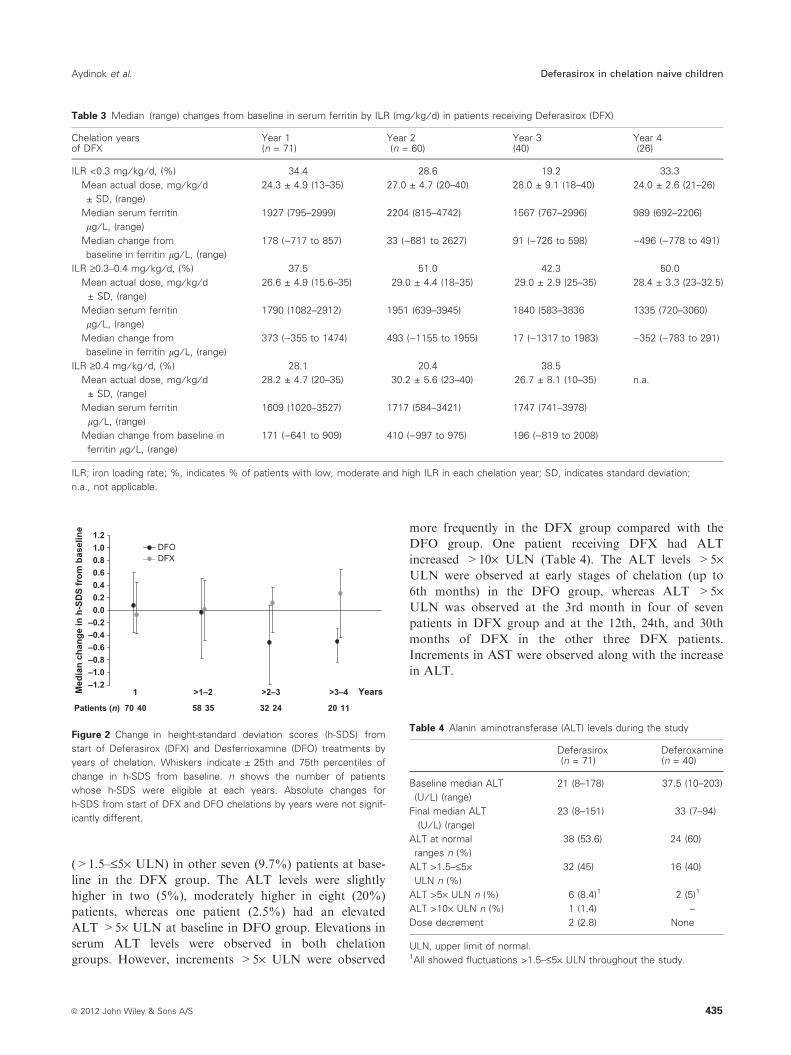
The effect of transfusional iron loading rate on serumferritin
Under the conditions of this study, a decrease in median
serum ferritin from baseline was achieved in patients with
lower ILR (<0.3 mg ⁄kg ⁄d) following a substantial
increase in the first year with DFX chelation. In contrast,
an increase in median serum ferritin from baseline in sub-
jects with higher ILR (ILR ‡ 0.3–0.4 and ‡0.4 mg ⁄kg ⁄d)with DFX chelation was observed for the first 2 yr,
(Table 3). There was no consistent correlation between
transfusional ILR and median change in serum ferritin
Table 1 Baseline characteristics of the patients
Variable Deferoxamine Deferasirox P
No. patients 40 71 –
Sex, no (%)
Male 22 (55) 45 (62.5) 0.44
Female 18 (45) 27 (37.5)
Median age of chelation start, yr (range) 3.1 (1.3–5.9) 2.6 (1.2–5.9) 0.32
Median time from 1st
transfusion to chelation, yr (range)
2.2 (0.3–5.0) 1.6 (0.1–4.7) 0.07
Median chelation duration, yr (range) 2.75 (1.0–6.1) 2.29 (1.0–7.0) 0.48
Median height-standard
deviation scores at baseline (range)
)0.28 ()2.8 to 3.2) )0.6 ()2.5 to 3.0) 0.39
Median weight-standard
deviation scores at baseline (range)
)0.30 ()2.9 to 2.2) )0.36 ()2.2 to 2.2) 0.47
Median serum ferritin at
baseline, lg ⁄ L (range)
1848 (937–3945) 1513 (995–3241) 0.009
Median aspartate aminotransferase
at baseline, U ⁄ L (range)
37 (17–182) 35 (9)89) 0.017
Median alanin aminotransferase
at baseline, U ⁄ L (range)
37.5 (10–200) 21 (8–178) 0.006
Median serum creatinine at
baseline, mg ⁄ dL (range)
0.3 (0.17–0.5) 0.23 (0.1–0.83) 0.37
Aydinok et al. Deferasirox in chelation naive children
ª 2012 John Wiley & Sons A/S 433
from baseline by years in patients receiving DFO chelation
(data not shown).
The effect of DFX doses on serum ferritin
All DFX doses resulted in a substantial increase in serum
ferritin from baseline at the first year. This effect was
highest at DFX doses higher than 30 mg ⁄kg ⁄d. It shouldbe noted that this group had the highest mean ILR com-
pared with those receiving lower DFX doses. In the fol-
lowing years, a small number of patients remained on
DFX doses of 20 mg ⁄kg ⁄d or below capable to maintain
iron balance. The mean ILR was the lowest in this group
compared with those receiving higher DFX doses. How-
ever, the patients receiving mean actual doses of DFX
above 30 mg ⁄kg ⁄d achieved higher reduction in serum
ferritin compared with the patients receiving DFX
between 20 and 30 mg ⁄kg ⁄d at the following years, and
mean ILR was comparable between the groups. Further,
6 of 71 patients (8.4%) on DFX showed an absolute
increase in serum ferritin above 1000 lg ⁄L from baseline
to the last available observation that ranged between 2.5
and 5 yr on DFX chelation. It has been observed that the
mean actual DFX doses had been increased from initiated
dose of 20–30 mg ⁄kg ⁄d in steps of 5–10 mg ⁄kg ⁄d by
investigator judgment in these patients with baseline
serum ferritin levels between 1096 and 1885 lg ⁄L (mean
1590 lg ⁄L). Although, 22 of 71 patients (30%) in DFX
cohort had received the mean DFX doses above
30 mg ⁄kg ⁄d at least one of the chelation years, it should
be noted that the highest DFX dose of 40 mg ⁄kg ⁄d was
administered to only four patients during the study years.
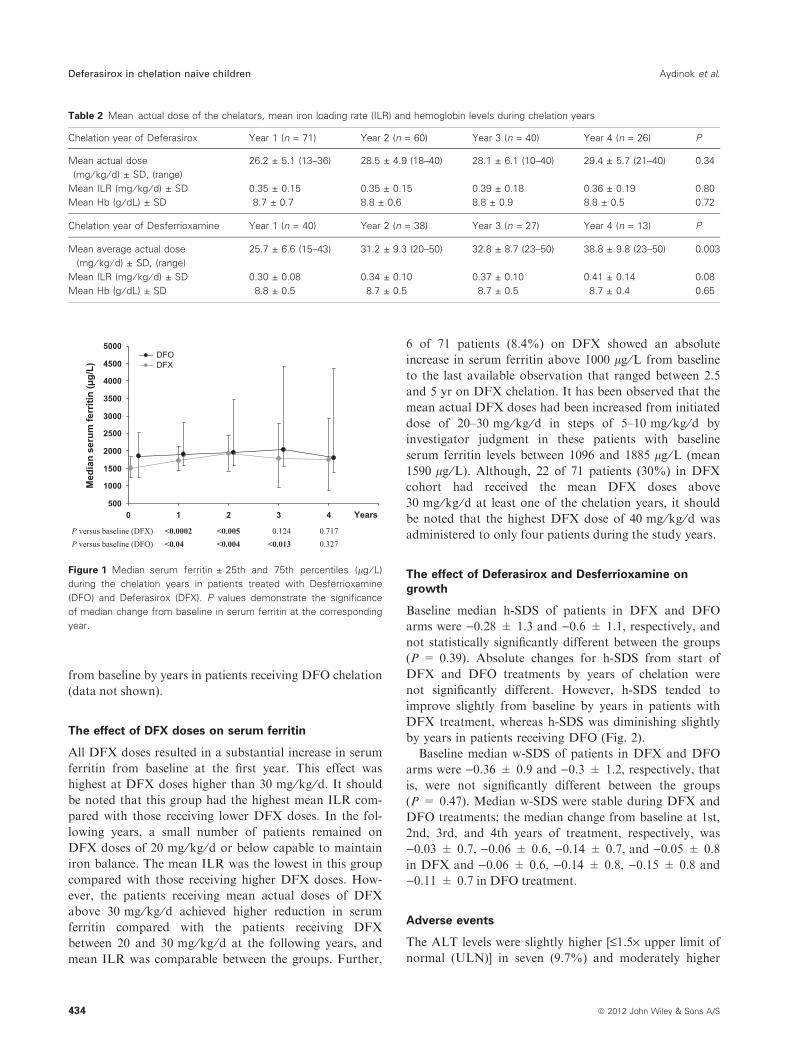
The effect of Deferasirox and Desferrioxamine ongrowth
Baseline median h-SDS of patients in DFX and DFO
arms were )0.28 ± 1.3 and )0.6 ± 1.1, respectively, and
not statistically significantly different between the groups
(P = 0.39). Absolute changes for h-SDS from start of
DFX and DFO treatments by years of chelation were
not significantly different. However, h-SDS tended to
improve slightly from baseline by years in patients with
DFX treatment, whereas h-SDS was diminishing slightly
by years in patients receiving DFO (Fig. 2).
Baseline median w-SDS of patients in DFX and DFO
arms were )0.36 ± 0.9 and )0.3 ± 1.2, respectively, that
is, were not significantly different between the groups
(P = 0.47). Median w-SDS were stable during DFX and
DFO treatments; the median change from baseline at 1st,
2nd, 3rd, and 4th years of treatment, respectively, was
)0.03 ± 0.7, )0.06 ± 0.6, )0.14 ± 0.7, and )0.05 ± 0.8
in DFX and )0.06 ± 0.6, )0.14 ± 0.8, )0.15 ± 0.8 and
)0.11 ± 0.7 in DFO treatment.
Adverse events
The ALT levels were slightly higher [£1.5· upper limit of
normal (ULN)] in seven (9.7%) and moderately higher
Table 2 Mean actual dose of the chelators, mean iron loading rate (ILR) and hemoglobin levels during chelation years
Chelation year of Deferasirox Year 1 (n = 71) Year 2 (n = 60) Year 3 (n = 40) Year 4 (n = 26) P
Mean actual dose
(mg ⁄ kg ⁄ d) ± SD, (range)
26.2 ± 5.1 (13–36) 28.5 ± 4.9 (18–40) 28.1 ± 6.1 (10–40) 29.4 ± 5.7 (21–40) 0.34
Mean ILR (mg ⁄ kg ⁄ d) ± SD 0.35 ± 0.15 0.35 ± 0.15 0.39 ± 0.18 0.36 ± 0.19 0.80
Mean Hb (g ⁄ dL) ± SD 8.7 ± 0.7 8.8 ± 0.6 8.8 ± 0.9 8.8 ± 0.5 0.72
Chelation year of Desferrioxamine Year 1 (n = 40) Year 2 (n = 38) Year 3 (n = 27) Year 4 (n = 13) P
Mean average actual dose
(mg ⁄ kg ⁄ d) ± SD, (range)
25.7 ± 6.6 (15–43) 31.2 ± 9.3 (20–50) 32.8 ± 8.7 (23–50) 38.8 ± 9.8 (23–50) 0.003
Mean ILR (mg ⁄ kg ⁄ d) ± SD 0.30 ± 0.08 0.34 ± 0.10 0.37 ± 0.10 0.41 ± 0.14 0.08
Mean Hb (g ⁄ dL) ± SD 8.8 ± 0.5 8.7 ± 0.5 8.7 ± 0.5 8.7 ± 0.4 0.65
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
0 1 2 3 4 Years
Med
ian
seru
m fe
rriti
n (µ
g/L)
DFODFX
P versus baseline (DFX)P versus baseline (DFO)
<0.0002 <0.005 0.124 0.717<0.04 <0.004 <0.013 0.327
Figure 1 Median serum ferritin ± 25th and 75th percentiles (lg ⁄ L)
during the chelation years in patients treated with Desferrioxamine
(DFO) and Deferasirox (DFX). P values demonstrate the significance
of median change from baseline in serum ferritin at the corresponding
year.
Deferasirox in chelation naive children Aydinok et al.
434 ª 2012 John Wiley & Sons A/S
(>1.5–£5· ULN) in other seven (9.7%) patients at base-
line in the DFX group. The ALT levels were slightly
higher in two (5%), moderately higher in eight (20%)
patients, whereas one patient (2.5%) had an elevated
ALT >5· ULN at baseline in DFO group. Elevations in
serum ALT levels were observed in both chelation
groups. However, increments >5· ULN were observed
more frequently in the DFX group compared with the
DFO group. One patient receiving DFX had ALT
increased >10· ULN (Table 4). The ALT levels >5·ULN were observed at early stages of chelation (up to
6th months) in the DFO group, whereas ALT >5·ULN was observed at the 3rd month in four of seven
patients in DFX group and at the 12th, 24th, and 30th
months of DFX in the other three DFX patients.
Increments in AST were observed along with the increase
in ALT.
Table 3 Median (range) changes from baseline in serum ferritin by ILR (mg ⁄ kg ⁄ d) in patients receiving Deferasirox (DFX)
Chelation yearsof DFX
Year 1(n = 71)
Year 2(n = 60)
Year 3(40)
Year 4(26)
ILR <0.3 mg ⁄ kg ⁄ d, (%) 34.4 28.6 19.2 33.3
Mean actual dose, mg ⁄ kg ⁄ d± SD, (range)
24.3 ± 4.9 (13–35) 27.0 ± 4.7 (20–40) 28.0 ± 9.1 (18–40) 24.0 ± 2.6 (21–26)
Median serum ferritin
lg ⁄ L, (range)
1927 (795–2999) 2204 (815–4742) 1567 (767–2996) 989 (692–2206)
Median change from
baseline in ferritin lg ⁄ L, (range)
178 ()717 to 857) 33 ()681 to 2627) 91 ()726 to 598) )496 ()778 to 491)
ILR ‡0.3–0.4 mg ⁄ kg ⁄ d, (%) 37.5 51.0 42.3 50.0
Mean actual dose, mg ⁄ kg ⁄ d± SD, (range)
26.6 ± 4.9 (15.6–35) 29.0 ± 4.4 (18–35) 29.0 ± 2.9 (25–35) 28.4 ± 3.3 (23–32.5)
Median serum ferritin
lg ⁄ L, (range)
1790 (1082–2912) 1951 (639–3945) 1840 (583–3836 1335 (720–3060)
Median change from
baseline in ferritin lg ⁄ L, (range)
373 ()355 to 1474) 493 ()1155 to 1955) 17 ()1317 to 1983) )352 ()783 to 291)
ILR ‡0.4 mg ⁄ kg ⁄ d, (%) 28.1 20.4 38.5
Mean actual dose, mg ⁄ kg ⁄ d± SD, (range)
28.2 ± 4.7 (20–35) 30.2 ± 5.6 (23–40) 26.7 ± 8.1 (10–35) n.a.
Median serum ferritin
lg ⁄ L, (range)
1609 (1020–3527) 1717 (584–3421) 1747 (741–3978)
Median change from baseline in
ferritin lg ⁄ L, (range)
171 ()641 to 909) 410 ()997 to 975) 196 ()819 to 2008)
ILR; iron loading rate; %, indicates % of patients with low, moderate and high ILR in each chelation year; SD, indicates standard deviation;
n.a., not applicable.
–1.2–1.0–0.8–0.6–0.4–0.2
0.00.20.40.60.81.01.2
YearsMed
ian
chan
ge in
h-S
DS
from
bas
elin
e
DFODFX
1 >1–2 >2–3
Patients (n) 70 40 58 35 32 24 20 11
>3–4
Figure 2 Change in height-standard deviation scores (h-SDS) from
start of Deferasirox (DFX) and Desferrioxamine (DFO) treatments by
years of chelation. Whiskers indicate ± 25th and 75th percentiles of
change in h-SDS from baseline. n shows the number of patients
whose h-SDS were eligible at each years. Absolute changes for
h-SDS from start of DFX and DFO chelations by years were not signif-
icantly different.
Table 4 Alanin aminotransferase (ALT) levels during the study
Deferasirox(n = 71)
Deferoxamine(n = 40)
Baseline median ALT
(U ⁄ L) (range)
21 (8–178) 37.5 (10–203)
Final median ALT
(U ⁄ L) (range)
23 (8–151) 33 (7–94)
ALT at normal
ranges n (%)
38 (53.6) 24 (60)
ALT >1.5–£5·ULN n (%)
32 (45) 16 (40)
ALT >5· ULN n (%) 6 (8.4)1 2 (5)1
ALT >10· ULN n (%) 1 (1.4) –
Dose decrement 2 (2.8) None
ULN, upper limit of normal.1All showed fluctuations >1.5–£5· ULN throughout the study.
Aydinok et al. Deferasirox in chelation naive children
ª 2012 John Wiley & Sons A/S 435
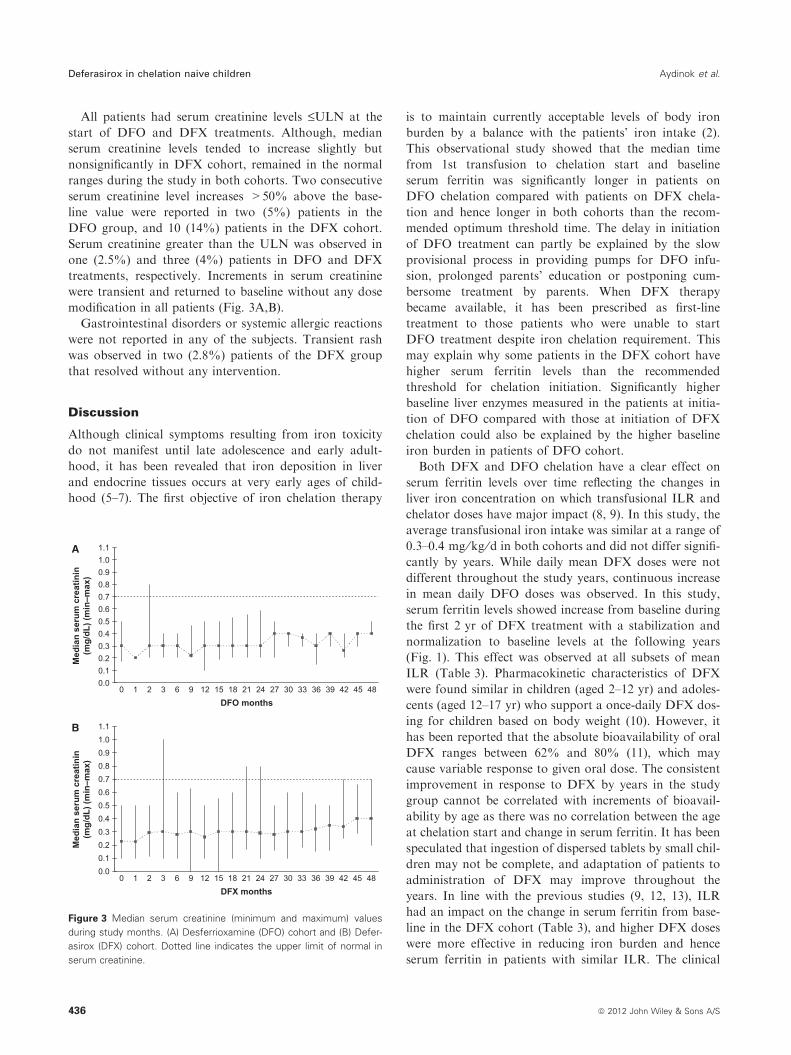
All patients had serum creatinine levels £ULN at the
start of DFO and DFX treatments. Although, median
serum creatinine levels tended to increase slightly but
nonsignificantly in DFX cohort, remained in the normal
ranges during the study in both cohorts. Two consecutive
serum creatinine level increases >50% above the base-
line value were reported in two (5%) patients in the
DFO group, and 10 (14%) patients in the DFX cohort.
Serum creatinine greater than the ULN was observed in
one (2.5%) and three (4%) patients in DFO and DFX
treatments, respectively. Increments in serum creatinine
were transient and returned to baseline without any dose
modification in all patients (Fig. 3A,B).
Gastrointestinal disorders or systemic allergic reactions
were not reported in any of the subjects. Transient rash
was observed in two (2.8%) patients of the DFX group
that resolved without any intervention.
Discussion
Although clinical symptoms resulting from iron toxicity
do not manifest until late adolescence and early adult-
hood, it has been revealed that iron deposition in liver
and endocrine tissues occurs at very early ages of child-
hood (5–7). The first objective of iron chelation therapy
is to maintain currently acceptable levels of body iron
burden by a balance with the patients’ iron intake (2).
This observational study showed that the median time
from 1st transfusion to chelation start and baseline
serum ferritin was significantly longer in patients on
DFO chelation compared with patients on DFX chela-
tion and hence longer in both cohorts than the recom-
mended optimum threshold time. The delay in initiation
of DFO treatment can partly be explained by the slow
provisional process in providing pumps for DFO infu-
sion, prolonged parents’ education or postponing cum-
bersome treatment by parents. When DFX therapy
became available, it has been prescribed as first-line
treatment to those patients who were unable to start
DFO treatment despite iron chelation requirement. This
may explain why some patients in the DFX cohort have
higher serum ferritin levels than the recommended
threshold for chelation initiation. Significantly higher
baseline liver enzymes measured in the patients at initia-
tion of DFO compared with those at initiation of DFX
chelation could also be explained by the higher baseline
iron burden in patients of DFO cohort.
Both DFX and DFO chelation have a clear effect on
serum ferritin levels over time reflecting the changes in
liver iron concentration on which transfusional ILR and
chelator doses have major impact (8, 9). In this study, the
average transfusional iron intake was similar at a range of
0.3–0.4 mg ⁄kg ⁄d in both cohorts and did not differ signifi-
cantly by years. While daily mean DFX doses were not
different throughout the study years, continuous increase
in mean daily DFO doses was observed. In this study,
serum ferritin levels showed increase from baseline during
the first 2 yr of DFX treatment with a stabilization and
normalization to baseline levels at the following years
(Fig. 1). This effect was observed at all subsets of mean
ILR (Table 3). Pharmacokinetic characteristics of DFX
were found similar in children (aged 2–12 yr) and adoles-
cents (aged 12–17 yr) who support a once-daily DFX dos-
ing for children based on body weight (10). However, it
has been reported that the absolute bioavailability of oral
DFX ranges between 62% and 80% (11), which may
cause variable response to given oral dose. The consistent
improvement in response to DFX by years in the study
group cannot be correlated with increments of bioavail-
ability by age as there was no correlation between the age
at chelation start and change in serum ferritin. It has been
speculated that ingestion of dispersed tablets by small chil-
dren may not be complete, and adaptation of patients to
administration of DFX may improve throughout the
years. In line with the previous studies (9, 12, 13), ILR
had an impact on the change in serum ferritin from base-
line in the DFX cohort (Table 3), and higher DFX doses
were more effective in reducing iron burden and hence
serum ferritin in patients with similar ILR. The clinical
A
0.00.10.20.30.40.50.60.70.80.91.01.1
DFO months
Med
ian
seru
m c
reat
inin
(mg/
dL) (
min
–max
)
B
0.00.10.20.30.40.50.60.70.80.91.01.1
0 1 2 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48
0 1 2 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48
DFX months
Med
ian
seru
m c
reat
inin
(mg/
dL) (
min
–max
)
Figure 3 Median serum creatinine (minimum and maximum) values
during study months. (A) Desferrioxamine (DFO) cohort and (B) Defer-
asirox (DFX) cohort. Dotted line indicates the upper limit of normal in
serum creatinine.
Deferasirox in chelation naive children Aydinok et al.
436 ª 2012 John Wiley & Sons A/S

studies confirmed the importance of timely dose adjust-
ments based on serum ferritin trends for achieving thera-
peutic target of maintenance or reduction in iron burden
in patients with transfusional iron overload (12–14). In
the current study, 8.4% of patients had an absolute
increase in serum ferritin values of more than 1000 lg ⁄Lcompared with baseline with an increasing trend despite
DFX dose adjustments up to 30 mg ⁄kg ⁄d, which was the
highest approved dose as a label indication at those times.
Clinical studies have indicated that some patients require
DFX doses of more than 30 mg ⁄kg ⁄d to achieve their
therapeutic goals (9, 15). It has been suggested that
patients who require dose escalation above 30 mg ⁄kg ⁄dwere heavily iron loaded, which was reflected by high
serum ferritin (>2500 lg ⁄L) at baseline (15). The current
study indicated that some patients may need higher DFX
doses, while they have relatively lower iron burden. DFO
infusions resulted in a significant increase in serum ferritin
from baseline for the first 3 yr with a substantial decrease
and stabilization at the 4th year. No consistency between
the ILR, the actual mean DFO doses and the change in
serum ferritin from baseline could be observed in this
cohort. One explanation for this evident lack of correla-
tion could lie in the variable compliance to DFO, which is
cumbersome to use.
Both chelation regimens were generally well tolerated,
and none of the patients in each cohort had to discontinue
chelation therapy because of adverse events. Although
gastrointestinal disturbances and skin rash were predomi-
nant side effects of DFX chelation in clinical studies (8,
13, 16), no patient has complained about clinically signifi-
cant gastrointestinal disturbances and only two patients
(2.8%) had temporary skin rash that spontaneously
resolved. Although gastrointestinal disorders with a sus-
pected relationship to DFX treatment were observed less
frequently in patients aged <16 yr (15.8%) than ‡16 yr
(29.1%) (17), the gastrointestinal tolerance in chelation-
naıve patients aged £5 yr has not been specifically
addressed in other clinical studies as it was confirmed in
this observation study. Although fluctuations in serum
ALT and AST levels were observed in both DFX and
DFO cohorts, only one patient with severe liver enzyme
elevations (ALT >10· ULN) was recorded in the DFX
group. None of the patients in both cohorts had progres-
sive increases in serum creatinine. In line with the previous
studies (15, 18), DFX doses above 30 mg ⁄kg ⁄d were not
associated with increase in the incidence and severity of
adverse events in chelation-naıve patients.
Pediatric patients aged £5 yr continued growth in both
cohorts. Further, it has been shown that linear growth
improved by years in patients receiving DFX. In con-
trast, the only study assessing long-term growth in pedi-
atric patients with TM revealed slightly reduced growth
in patients compared with a normal population at the
age <12 yr (13). In that study, the mean age and median
serum ferritin of patients at study start was higher com-
pared with our chelation-naıve patients.
Our study had some limitations. This study is not a
randomized study of DFO and DFX with the records of
all dispensed and returned study medications to deter-
mine the chelation compliance that may support a higher
compliance to the study drug than real-life administra-
tions. In that point of view, a randomized study is obvi-
ously needed to provide more robust efficacy comparison
of these chelation regimens in chelation-naıve patients.
However, an advantage of such a study may be that the
patients included are more likely to represent the general
compliance characteristics of disease population to chela-
tion therapy.
In conclusion, this is the first study to demonstrate
comparable tolerability and efficacy of DFX versus DFO
in chelation-naıve pediatric patients aged £5 yr with
transfusional iron overload. This observational postmar-
keting study confirmed that DFX is an effective first-line
regimen to maintain iron balance and normal growth
progression with an excellent tolerance at doses above
30 mg ⁄kg ⁄d in children aged £5 yr.
References
1. Maria-Domenica C, Alan C, Androulla E, Antonio P,
John P, Ali T, eds. Iron overload. In: Guidelines for the
Clinical Management of Thalassaemia, 2nd edn, Chapter
3. Nicosia-Cyprus: Published by Thalasaemia Interna-
tional Federation. 2007: 43–4.
2. Porter J. Optimizing iron chelation strategies in b-thalas-
saemia major. Blood Rev 2009;23:S3–7.
3. Borgna-Pignatti C, Rugolotto S, De Stefano P, et al.
Survival and complications in patients with thalassaemia
major treated with transfusion and deferoxamine. Haema-
tologica 2004;89:1187–93.
4. Olivieri NF, Koren G, Harris J, Khattak S, Freedman
MH, Templeton DM, Bailey JD, Reilly BJ. Growth fail-
ure and bony changes induced by deferoxamine. Am J
Pediatr Hematol Oncol 1992;14:48–56.
5. Angelucci E, Baronciani D, Lucarelli G, et al. Needle liver
biopsy in thalassaemia: analyses of diagnostic accuracy
and safety in 1184 consecutive biopsies. Br J Haematol
1994;89:757.
6. Wood JC, Noetzl L, Hyderi A, Joukar M, Coates T,
Mittelman S. Predicting pituitary iron and endocrine
dysfunction. Ann N Y Acad Sci 2010;1202:123–8.
7. Noetzli LJ, Papudesi J, Coates TD, Wood JC. Pancreatic
iron loading predicts cardiac iron loading in thalassemia
major. Blood 2009;144:4021–6.
8. Cappellini MD, Cohen A, Piga A, et al. A phase 3
study of deferasirox (ICL670), a once-daily oral iron
chelator, in patients with b-thalassemia. Blood
2006;9:3455–62.
Aydinok et al. Deferasirox in chelation naive children
ª 2012 John Wiley & Sons A/S 437

9. Cohen AR, Glimm E, Porter JB. Effect of transfusional
iron intake on response to chelation therapy in
b-thalassemia major. Blood 2008;111:583–7.
10. Galanello R, Piga A, Alberti D, Rouan MC, Bigler H,
Sechaud R. Safety, tolerability, and pharmacokinetics of
ICL670, a new orally active iron-chelating agent in
patients with transfusion-dependent iron overload due to
beta-thalassemia. J Clin Pharmacol 2003;43:565–72.
11. Se¢chaud R, Robeva A, Belleli R, Balez S. Absolute oral
bioavailability and disposition of deferasirox in healthy
human subjects. J Clin Pharmacol 2008;48:919–25.
12. Cappellini MD, Porter J, El-Beshlawy A, et al. Tailoring
iron chelation by iron intake and serum ferritin: the pro-
spective EPIC study of deferasirox in 1744 patients with
transfusion-dependent anemias. Haematologica
2010;95:557–66.
13. Cappellini MD, Bejaoui M, Agaoglu L, et al. Iron chela-
tion with deferasirox in adult and pediatric patients with
thalassemia major: efficacy and safety during 5 years’
follow-up. Blood 2011;4:884–93.
14. Taher A, El-Beshlawy A, Elalfy MS, et al. Efficacy and
safety of deferasirox, an oral iron chelator, in heavily
iron-overloaded patients with b-thalassaemia: the ESCA-
LATOR study. Eur J Haematol 2009;82:458–65.
15. Taher A, Cappellini MD, Vichinsky E, Galanello R, Piga
A, Lawniczek T, Clark J, Habr D, Porter JB. Efficacy and
safety of deferasirox doses of >30 mg ⁄kg per d in
patients with transfusion-dependent anaemia and iron
overload. Br J Haematol 2009;147:752–9.
16. Galanello R, Piga A, Forni GL, et al. Phase II clinical
evaluation of deferasirox, a once-daily oral chelating
agent, in pediatric patients with b-thalassemia major.
Haematologica 2006;91:1343–51.
17. Piga A, Galanello R, Forni GL, et al. Randomized phase
II trial of deferasirox (Exjade�, ICL670), a once-daily,
orally-administered iron chelator, in comparison to defe-
roxamine in thalassemia patients with transfusional iron
overload. Haematologica 2006;91:873–80.
18. Taher A, Elalfy MS, Al Zir K, Daar S, Al Jefri A, Habr
D, Kriemler-Krahn U, El-Ali A, Roubert B, El-Beshlawy
A. Importance of optimal dosing ‡30 mg ⁄ kg ⁄d during
deferasirox treatment: 2.7-yr follow-up from the ESCA-
LATOR study in patients with b-thalassaemia. Eur J
Haematol 2011;87:355–65.
Deferasirox in chelation naive children Aydinok et al.
438 ª 2012 John Wiley & Sons A/S