review of oral iron chelators (deferiprone and deferasirox) for the
TRANSCRIPT

1
Review of Oral Iron Chelators (Deferiprone and Deferasirox)
for the Treatment of Iron Overload in Pediatric Patients
D. Adam Algren, MD Assistant Professor of Pediatrics and Emergency Medicine
Division of Pediatric Pharmacology and Medical Toxicology Departments of Pediatrics and Emergency Medicine
Children’s Mercy Hospitals and Clinics/Truman Medical Center University of Missouri-Kansas City School of Medicine

2
PROPOSAL The World Health Organization Model List of Essential Medicines and Model Formulary 2010 list deferoxamine (DFO) as the treatment of choice for both acute and chronic iron poisoning. The Model Formulary currently does not designate any orally administered agents for the chelation of iron. It is proposed that deferasirox be considered the oral chelator of choice in the treatment of chronic iron overload. Deferasirox is widely available recent evidence support that it is both safe and efficacious. INTRODUCTION Acute iron poisoning and chronic iron overload result in significant morbidity and mortality worldwide. Treatment of acute iron poisoning and chronic iron overload can be challenging and care providers are often confronted with management dilemmas. Oral iron supplements are commonly prescribed for patients with iron deficiency anemia. The wide availability of iron supplements and iron-containing multivitamins provide easy accessibility for both adults and children. The approach to treatment of acute iron toxicity involves providing adequate supportive care, optimizing hemodynamic status and antidotal therapy with IV deferoxamine, when indicated.1 Early following an acute ingestion gastrointestinal (GI) decontamination can be potentially beneficial. Multiple options exist including: syrup of ipecac, gastric lavage, and whole bowel irrigation (WBI). Although definitive evidence that GI decontamination decreases morbidity and mortality is lacking it is often considered to be beneficial. The decision to initiate GI decontamination should be made on an individual case basis. In addition to conventional GI decontamination other methods to prevent absorption have been investigated. Likewise, several small studies have investigated the use of other oral agent/chelators for the treatment of acute iron poisoning. Chronic iron overload associated with red cell disorders (i.e. sickle cell anemia and thalassemia) and other myelodysplastic syndromes affect a significantly larger number of individuals. The body does not have an efficient mechanism to excrete iron. Thus, in those patients requiring multiple transfusions iron accumulates and is deposited into multiple organ systems. The long term consequences of chronic iron overload include multiple organ dysfunction (heart, liver, and endocrine) and/or failure.2-5
Therefore. iron chelation is necessary to prevent organ failure and decrease mortality. Deferoxamine was the first iron chelator introduced into clinical practice. Although effective, there are significant challenges associated with its use that can result in non-compliance. Deferiprone and deferasirox, oral iron chelators, are increasingly available and evidence supports their use in the treatment of chronic iron overload. A perfect oral iron chelator does not exist; although, both deferiprone and deferasirox are effective they have differences including different pharmacokinetics and adverse effect profiles. These differences are both advantageous and/or problematic. These advantages and disadvantages will be reviewed and a recommendation for a chelator of choice will be made based on these considerations. This review will summarize the available evidence regarding:
3
a) Efficacy of deferoxamine in the treatment of chronic iron overload and the challenges associated with its use. b) Efficacy and safety of deferiprone c) Efficacy and safety of deferasirox d) Formulation, dosing recommendation, and cost comparison between deferiprone and deferasirox. LITERATURE REVIEW
The studies for this review were identified by performing a search of the PubMed using the search terms: “iron poisoning”, “iron toxicity”, “iron chelation”, “deferoxamine”, “deferiprone”, and “deferasirox”. The dates included 1966-2010. The Cochrane Database for Systematic Reviews was also searched and pertinent reviews were identified.6-8 The bibliographies of selected articles were also reviewed to identify any relevant studies not found by the original literature search. CURRENT LISTING WHO 2010 Model Formulary for Children: Deferoxamine. Acute Iron Poisoning. Neonate, Infant, Child. 15mg/kg/he reduced after 4-6 hours so that total dose does not exceed 80mg/kg in 24 hours. Maximum dose 6 grams/day. IM: 50mg/kg/dose every 6 hours. Maximum dose 6 grams/day. The preferred route is IV. Chronic Iron Overload: SC or IV infusion in an infant or child: 30mg/kg over 8-12 hours on 3-7 days/week. For established iron overload the dose is usually 20-50mg/kg daily. The dose should reflect the degree of iron overload. Use the lowest effect dose. Diagnosis of iron overload: 500mg IM. EFFICACY AND SAFETY ACUTE IRON POISONING- Several different methods to prevent iron absorption following acute ingestions have been investigated. GI decontamination involves removing the compound from the GI tract prior to its absorption or administering an agent that is capable of binding the compound so that it is not available for systemic absorption. Syrup of ipecac traditionally had been recommended to induce vomiting in order to facilitate removal of a substance from the GI tract. There is scant evidence to support or refute the use of ipecac and therefore a recent international position statement recommended against routine use of ipecac in the poisoned patient.9 The available evidence does suggest that efficacy decreases dramatically beyond 30-60 minutes following ingestion. The generalizability of these recommendations to developing nations is not clear. In locations with limited medical resources ipecac administration may be the best GI decontamination option due to the fact that it is not resource or labor intensive. Physical removal of iron from the stomach may also be accomplished by gastric lavage. There are no studies that specifically address its use in those with acute iron ingestions. A consensus position statement also does not endorse its routine use in poisoned patients.10 Available evidence suggests that it is most effective if performed within 1 hour. Performing gastric lavage with different lavage
4
solutions has also been investigated. Intuitively it would make sense that lavage solutions could complex with the iron to form insoluble iron compounds. Hypertonic phosphate solutions were not effective quickly abandoned due to morbidity from associated electrolyte abnormalities that it induced.11-14 Although there is some evidence to support the efficacy of magnesium hydroxide to prevent absorption of iron it is generally not recommended for several reasons.15-17 An un-realistically large volume would have to be administered and patients would be at risk for developing electrolyte abnormalities. Activated charcoal has become the method of choice among healthcare providers for GI decontamination. However, iron does not adsorb well to charcoal and therefore its use should be limited to those situations involving co-ingestants that charcoal is deemed necessary.18
Whole bowel irrigation consists of the administration of polyethylene glycol electrolyte solution to promote intestinal evacuation prior to systemic absorption. WBI should be considered in cases of significant iron ingestion as there are limited options for GI decontamination in iron poisoning.19 However, this procedure can be labor intensive as it requires the ingestion of a large amount of polyethylene glycol solution over a relatively brief time course. Although commonly recommended there is limited evidence to support its use. Several investigators have examined the utility of oral iron chelation in the setting of an acute iron overdose. Animal studies initially suggested that oral deferoxamine decreased iron absorption and could potentially be of benefit.20 Subsequent investigations failed to confirm decreased absorption in deferoxamine treated swine and dogs.21-23 The literature regarding the efficacy of oral DFO in humans is limited. A small volunteer study that assessed its ability to bind iron failed to demonstrate decreased absorption.24 However, another volunteer study that used a larger dose of DFO was able to show decreased iron absorption.25 Clinical experience with oral DFO in overdose patients is limited. Early studies examining the efficacy of DFO suggested that it likely does not prevent iron absorption and could in fact contribute to toxicity by facilitating production and absorption of the toxic metabolite ferrioxamine.22-23 The utility of other oral iron chelators for acute iron poisoning is unknown. A rat model administered oral deferiprone following administration of an LD50 dose of iron. Deferiprone decreased mortality in the treatment group, especially in those that received a follow up dose.26 There are no human studies addressing its use. CHRONIC IRON OVERLOAD Deferoxamine was introduced in the 1960’s and was the first iron chelator used for the treatment of chronic iron overload. Several of the studies addressed in this review have combined the use of DFO with an oral chelator. Although it is administered parenterally, a review of evidence supporting its use will provide background regarding chelation therapy for chronic iron overload. Even though there is significant clinical experience with DFO a majority of the literature is retrospective or observational. DFO is derived from Streptomyces pilosus and is administered parenterally given its poor oral bioavailability.27 DFO has a short half life and must be administered by intravenous (IV) or subcutaneous injections/infusions.28-29 IV and subcutaneous administration were shown to be more efficacious at improving iron excretion compared to intramuscular administration.30-32 An intermittent subcutaneous
5
injection schedule was shown to be as efficacious in promoting iron excretion as a continuous 12 hour subcutaneous injection.33 Increasing the dose of DFO administered generally results in higher iron excretion, especially in those with patients with more significant iron overload.34 Urinary excretion of iron increases within hours of administration. Different clinical parameters are used to assess body iron burden and response to therapy. Serum ferritin levels are the laboratory parameter most often used. In general, sustained ferritin levels greater than 2500 mcg/L are associated with organ toxicity and death.35 Most chelation regimens attempt to achieve the goal of lower ferritin below 2500 mcg/L. DFO has demonstrated efficacy in decreasing morbidity associated with iron overload. Other methods of determining body iron burdens include: liver biopsy and liver/cardiac magnetic resonance imaging.2 Deferoxamine has long term data to support its use as a chelation agent in chronic iron overload in both adult and children. Following the introduction of deferoxamine survival rates for thalassemia patients increased substantially within a decade.36 Morbidity from organ system toxicity as decreased significantly as well. Cardiac disease has been reversed in multiple trials. Thalassemia patients (mean ages 9-15 years old) treated with 12 hour subcutaneous deferoxamine infusions that resulted in well controlled serum ferritin levels had estimated 10 year survival of 100% without cardiac disease.35 Additional work demonstrated significant reduction in mortality and incidence of heart failure in thalassemia patients treated with DFO.37-
38 Long-term morbidity associated with other organ system dysfunction was prevented using a subcutaneous infusion regimen.39 Further studies also support the clinical equivalence of IV and intermittent subcutaneous DFO infusion.30,40-42 Additional trials support the use of 12 hour continuous subcutaneous infusions in pediatric patients.43-44 Other investigators have combined both intravenous and subcutaneous dosing to avoid daily DFO administration. This protocol was effective at lowering serum ferritin after 1 year of therapy and resulted in further reduction at the end of the second year of treatment.45 A 24 hour infusion regimen was successful in lowering ferritin levels and reversing cardiac complications; however mortality at the end of the follow up period was equivalent to that of intermittent DFO protocols.46 Deferoxamine is effective in reversing hepatic iron overload. Early trials in children demonstrated intermittent DFO infusions were effective in decreasing liver iron stores and prevent progression of hepatic fibrosis.47 Intensive chelation significantly reduced liver iron stores in four children within 52-83 months of DFO initiation.48 Active liver disease may necessitate adjustment of the DFO dose that is administered.49
The data to support deferoxamine use in other disorders associated with iron overload is limited. Deferoxamine appears capable of increasing iron excretion in sickle cell patients.50 Intermittent IV DFO infusions were effective in decreasing liver iron concentrations in two small cohorts of sickle cell anemia patients.51-52 While effective deferoxamine administration can result in systemic toxicity and it is resource and labor intensive. It those cases where it is administered intravenously it requires the patient to have semi-permanent intravenous access. Given its short half life it requires frequent administration, typically 5-7 days/week. Long term intravenous access is associated with complications.46 Subcutaneous administration avoids some risks associated with IV administration, but is more painful. Both routes of administration require prolonged infusion times affecting quality of life and risk non-compliance with therapy.53-54 Early and aggressive DFO
6
administration can adversely affect skeletal maturation and result in growth retardation.55 The cumbersome nature and complications associated with DFO therapy pushed investigators to identify oral agents that would suitable for long-term chelation in those with chronic iron overload. Deferiprone was initially introduced in Europe in the 1980’s and was the first oral chelator to be used for the treatment of iron overload (Table). It is a bidentate hydroxypyridone with a small molecular weight (139). Peak plasma levels occur within 1 hour. It forms a stable complex with iron that is then excreted in the urine.56 It is metabolized by glucuronidation in the liver and has a relatively short half-life of 47-134 minutes necessitating multiple daily dosing.57-58 Early animal data demonstrated good iron mobilization using deferiprone.59-60 The scientific data regarding deferiprone is derived mostly from observational, retrospective, or combination chelator studies. The lack of traditional safety and efficacy trials comparing deferiprone to deferoxamine has prevented approval in the United States; however it is used in Europe (under specific conditions) and other countries. Several decades of experience with deferiprone have been reported. Initial studies demonstrated comparable amounts of iron excretion when deferiprone was compared to deferoxamine.61-62 However, DFO appears to results in slightly higher net iron excretion as a result of fecal loss. Deferiprione results in more significant reduction in iron levels in those with a higher iron burden.63 It may not be as helpful for those less significant iron overload. However, this problem can be overcome by increasing the amount of deferiprone administered from 75 to 100 mg/kg/day.63 Multiple studies have examined the deferiprone’s ability to lower serum ferritin concentrations. These studies are mostly retrospective and observational and include both adult and pediatric patients. A majority of the trials followed patients for at least 1 year with several trails following patients for 3 or more years. The most common dose administered in the trails was 75 mg/kg/day. The number of subjects in each trial is small, typically numbering less than 40. However, several series with a larger number of subjects have been published. The effectiveness of deferiprone was reported by Cohen and colleagues in a 4 year observational trial.64 It included 187 patients with a mean age of 18 (range 10-41). Deferiprone was quite effective in lowering serum ferritin over the study period. In those patients with more severe iron overload the ferritin level dropped from 3661 ± 1862 mcg/L to 2630 ± 1708 mcg/L. Patients with lower initial ferritin levels had less dramatic results. There were 47 patients that discontinued therapy as a result of increasing ferritin levels. The reasons for decreased effectiveness in this subset of patients were not clear. They did not differ significantly from the study population except they were less likely to have undergone splenectomy.64 Goel and collegues examined their 3 year experience with deferiprone in 58 thalassemia patients (mean age 11.9 years).65 They demonstrated that those patients that entered the trial with higher mean serum ferritin concentrations (mean 4745 ± 1873 ng/ml) tended to have the best response to therapy. Deferiprone was not uniformally successful in lower ferritin concentrations as 17 patients finished in the study with higher concentrations A smaller study of 21 patients evaluated deferiprone in thalassemia patients.66 The mean age of patients was 22 (range 7.5-31 years). Follow up at 3 years demonstrated significant decreases in hepatic iron and serum ferritin concentrations. Although the mean serum ferritin decreased from 3975 ± 766 mcg/L to 2546 ± 381 mcg/L those patients with more severe iron overload were only able to achieve ferritin concentrations of 3273 ± 568 mcg/L.66 Similarly, the same authors examined deferiprone effectiveness in 18 patients treated for a mean of 4.6 years.67 The mean
7
age of the patients was 18.2 (range 10.5-23.7 years). Hepatic iron concentrations remained elevated in 7 of18 patients. Five of these patients had biopsy documented progression of liver fibrosis. Even though there was significant improvement in serum ferritin levels, 9 of17 patients had levels that remained greater than 2500 mcg/L.67 More recent trials have assessed the efficacy of deferiprone in young children. El Alfy and colleagues reviewed its use in 100 children (mean age 5.1 ± 2.4 years) with thalassemia or sickle cell disease.68 At the end of the 6 month treatment period there was a significant drop in mean serum ferritin levels from 2532 ± 1463 ng/L to 2176 ± 1144 ug/L (p<0.05). Similar results were reported in another trial of pediatric patients (median age 10.6 years).69 Mean serum ferritin levels decreased from a mean of 4,677 ± 1,130 ng/L at baseline to 3,363 ± 1,149 ng/L following a median treatment duration of 11.4 months (range 1.4-39.6 months). Preventing iron burden of organs such as the heart and liver is crucial in decreasing morbidity and mortality associated with chronic iron overload. Liver iron concentrations more than 15mg/gram dry weight are associated with increased mortality.39 Thus, several studies have examined deferiprone’s ability to lower liver iron concentrations in thallasemia patients.66-67,70-73 . These studies involve small numbers of patients followed for 1-5 years. Although deferiprone appears to be effective in lower serum iron concentrations in some patients a majority of the trials did not demonstrate significant improvement. Multiple studies have looked at combination therapy involving the use of deferiprone and deferoxamine.74-91 Although many of the studies suffer from methodological issues including small patient numbers, short-follow up, and/or other confounding variables they typically demonstrate the combining deferiprone with deferoxamine is associated with improved outcomes. Deferiprone is less effective in those with lower initial serum ferritin elevations. However, the use of this combination is often more efficacious than use of either as a single agent as the addistion of deferoxamine to deferiprone is synergestic. This is likely a result of deferiprone’s ability to enter cells and chelate intracellular iron.56 Deferoxamine can serve as adjunctive therapy in those patients with marginal responses to deferiprone.92
The largest trial comparing deferiprone monotherapy to combination therapy was recently published. Maggio and colleagues assessed efficacy of deferiprone versus combination therapy in a randomized trial involving 213 thalassemia patients (mean age 23 years).74 Patients were followed for 5 years. The results demonstrated that combination of deferiprone with subcutaneous deferoxamine was more effective in lower serum ferritin. The ferritin concentration in the combination group was 1369 ± 816 mcg/L versus 1588 ± 1217 mcg/L in the deferiprone group (p<0.05). There was not statistically significant differences in mortality or cost between the groups.74 Daar and Pathare reviewed use of deferiprone/deferoxamine combination therapy in 55 thalassemia patients (mean age 15 ± 5.8 years).75 Combination therapy was associated with a significant improvement in serum ferritin levels and echocardiographic paramaters over the mean follow up period of 22 months. Similar results were reported by Origa and collegues.76 They enrolled 79 patients (mean age 23 ± 5 years). Over the 12-24 month follow up period there was a statistically significant improvement in serum ferritin and cardiac function in combination deferiprone/deferoxamine group when compared to deferoxamine monotherapy. A recent Cochrane review addressed deferiprone use in thalassemia patients.6 The reviewers concluded that although there was significant heterogeneity in study data that they reviewed. Both deferiprone and deferoxamine resulted in iron excretion; however, there was little consistency regarding the effectiveness of these
8
chelators. Given that combination therapy appeared to result in greater iron excretion and that deferiprone was associated with a higher incidence of adverse effects the reviewers concluded that deferiprone should be reserved for those patients in whom deferoxamine therapy is contraindicated or inadequate.6
Deferiprone is associated with several adverse effects. The most concerning is agranulocytosis. In clinical trials neutropenia has been reported in up to 5% with agranulocytosis typically reported in < 1%. Patients that develop agranulocytosis typically do so during the first year of therapy, but it has been reported up to 19 months after deferiprone initiation.56,93 Combination therapy with deferoxamine and and/or an intact spleen place patients at higher risk.73 Neutropenia is typically reversible upon discontinuation of the drug, but can reoccur if deferiprone is reintroduced.94-95 It has yet to be elucidated if the neutropenia and agranulocytiosis is an idiosyncratic reaction or a dose-related direct myelotoxicty.56,93 Frequent monitoring of white blood cell counts is recommended.96 Consideration should be given to avoiding deferiprone in patients with myeloproliferative disorders. Gastrointestinal symptoms such as nausea, vomiting, and abdominal pain have been reported in up to 33% of patients.94,97 These are usually mild and typically do not result in drug discontinuation. Elevations of liver transaminases have been reported during deferiprone treatment. An early trial suggested that deferiprone was associated with progressive liver fibrosis.67 This was a small trial involving 19 patients of which 5 were considered to have progression of liver fibrosis. Subsequent trials involving larger numbers of patients have not demonstrated liver toxicity.94,98-100 Liver enzyme elevations tend to be mild and reversible. In a recent pediatric trial 12% of patients experienced a mild elevation in ALT.68 Only 1 patient had an elevation greater than twice the upper limit of normal at 3 and 6 months. Deferiprone was continued in all patients without incident. The contribution of deferiprone to worsening liver disease is often difficult to determine because of the natural progression associated with chronic iron overload. Other co-existing diseases, such as hepatitis, or other medications associated with hepatotoxicity contribute to the difficulty of assigning culpability to deferiprone. Arthralgias and arthritis have been associated with deferiprone. Although it has been reported to occur in 30-40% of patients in some studies large trials have reported a much lower incidence of 4%.56,64,101-2 Large joint, such as the knees, are more commonly affected. 50% of cases develop with the first year of therapy. Symptoms are typically mild and resolve with discontinuation. Deferasirox is the most recent oral chelator to be used for the management of chronic iron overload (Table). Unlike deferiprone, deferasirox was developed and studied under more rigorous scientific scrutiny. Although there is less long-term outcome data available, multiple studies have or are currently addressing its efficacy and safety. Iron chelation occurs when 2 molecules of deferasirox bind to 1 molecule of iron.103 Peak plasma concentrations occur within 1-2 hours of administration. It is highly protein bound (99%) and is metabolized by the liver with subsequent fecal excretion.104 The eliminations half life is 7-18 hours.105 This relatively long elimination facilitates once daily dosing. The tablets may be dissolved in water or juice without altering the bioavailability.96
Initial data suggests that deferasirox has the capacity to gain access to intracellular iron similar to deferiprone. Laboratory and animal studies confirm its ability to chelate cardiac iron.106-107 Recent data regarding deferasirox’s ability to treat cardiac iron overload initial human studies are promising. Multiple studies have
9
shown deferasirox is effective in decreasing cardiac iron burden; however, the results regarding if it is effective in removing cardiac iron in cases of severe iron overload are conflicting.108-110 More recently a large trial of 192 thalassemia patients investigated the efficacy of deferasirox in reducing cardiac iron overload as well as preventing cardiac iron accumulation.111 One third of the patients were less than 16 years old. The mean deferasirox dose administered over the 1 year treatment period was 32.6 mg/kg/day. A statistically significant decrease in cardiac iron, as demonstrated by cardiac magnetic resonance imaging, was observed. Deferasirox was also beneficial in preventing accumulation of cardiac iron.111 Deferasirox is effective in lowering serum ferritin levels and decreasing overall iron burden. An early trial that evaluated the dose-response relationship demonstrated that 20mg/kg/day effectively chelated iron. However, net iron excretion only occurred at a dose of 40 mg/kg/day.112 Yet, in another trial 20 mg/kg/day decreased liver iron concentrations in 71 adult thalassemia patients.113 A larger trial compared deferasirox (132 patients) to deferoxamine (63 patients) for the treatment of iron overload in patients with sickle cell anemia. The median age of the deferasirox treatment group was 15 years. At the end of 1 year deferasirox (10-30 mg/kg/day) was equivalent to deferoxamine in lowering liver iron concentrations.114 Likewise, Cappellini and colleagues assessed the efficacy of deferasirox versus deferoxamine in pediatric thalassemia patients.115 The mean age of the 296 patients that received deferasirox was 17 (± 9.4 years). The mean daily dose of deferasirox varied between 6.2mg and 28.2mg depending on baseline liver iron concentrations. Across all treatment groups noninferiority of deferasirox was not demonstrated. This was likely related to underdosing of deferasirox in a significant number of patients. Further analysis demonstrates that deferasirox was not inferior to deferoxamine in those patients that received 20-30mg/kg/day. At the higher 30mg/kg/day dose a decrease in serum ferritin and liver iron concentrations were observed.115 Taher and colleagues assessed the utility of deferasirox in heavily iron-overloaded thalassemia patients.116 This was a prospective trial that followed 237 patients (162 were between 2 and 16 years of age) for 1 year. A majority of patients completed the trial on 30 mg/kg/day. Deferasirox was effective and resulted in statistically significant decreases in liver iron concentrations and serum ferritin levels.116 Recently, the largest trial to date assessing deferasirox was published. It was a 1 year, prospective study of 1,744 patients with transfusion-associated iron overload.117 The mean age of all patients was 30.6 years (range 2-89 years). Similar to other trials the initial deferasirox dose varied and dose adjustments occurred throughout the trial. At the conclusion of the study 51% of patient were receiving greater than 30 mg/kg/day and 39.6% were receiving between 20-30 mg/kg/day. There was a statistically significant reduction in serum ferritin from baseline.117 Although a majority of deferasirox studies have enrolled thalassemia patients it has shown efficacy in treatment of other conditions associated with iron overload.114,118
A Cochrane review addressed the use deferasirox for the treatment of iron overload. In assessing its use in sickle cell anemia patients the reviewers concluded that deferasirox was as effective as deferoxamine in reducing iron overload.7 They cautioned however that long-term outcome data does not exist and further study is needed to assess its efficacy and safety. Although the same authors reviewed deferasirox use in patients with myelodysplastic syndromes they were not able to identify any trials that met their inclusion criteria.8 Additionally, a review of deferasirox for the treatment of thalassemia patients is currently in progress.
10
Deferasirox is generally well tolerated. Adverse effects associated with its use are for the most part mild and self-limiting. The development of adverse effects seems to be idiosyncratic and not dose dependent.119 Gastrointestinal symptoms, such as nausea, vomiting, and abdominal pain, as common and have been reported in up to 1/3 of patients.96,111,116,117,120 These symptoms are often mild, self-resolving, and typically do not necessitate discontinuing therapy. Skin rashs (maculopapular) are another common adverse effect that is reported in up to 10% of patients.114-117,121 Again, these rashes are mild and resolve with drug discontinuation. The most concerning adverse effect is acute renal insufficiency. This has been reported in up to 1/3 of patients in trials.111,113-116,121 Generally the elevations are mild and transient, however up to 10% of patients can have an increase greater than 33% above baseline117. These abnormalities almost always resolve following drug discontinuation. A significant number of pediatric patients have been included in deferasirox trials to date.114,115,121 The adverse effect profile in children is similar to that seen in adults. Likewise, no effects on growth and sexual development have been reported to date. FORMULATION, DOSING, COST Deferiprone is available as a 500mg tablet and an oral solution (100mg/0.4ml). The recommended dose is 75 mg/kg/day divided into 3 doses.122
Deferasirox is available in 125 mg, 250 mg, and 500 mg dissolvable oral tablets. The tablets are to be completely dissolved in water or juice and taken on an empty stomach.123 The recommended dose is 20-30 mg/kg/day given in a single daily dose. Subsequent dosing should be based on periodic serum ferritin monitoring. A cost comparison between deferiprone and deferasirox has to account for multiple variables including: drug cost, laboratory monitoring cost, cost associated with treating adverse effects and/or worsening of underlying disease as a result of non-compliance. A true, unbiased cost comparison between deferiprone and deferasirox has not been published. It has been estimated that the cost of treating a child with deferiprone could be twice the cost of deferoxamine. Whereas, the deferasirox could cost 2-3 times as much as deferoxamine.124 Thus a rough pricing order would be: deferasirox> deferiprone> deferoxamine. However, this could vary from country to country. Several recent reports suggest that deferasirox therapy is more cost effective than traditional deferoxamine therapy.125,126
11
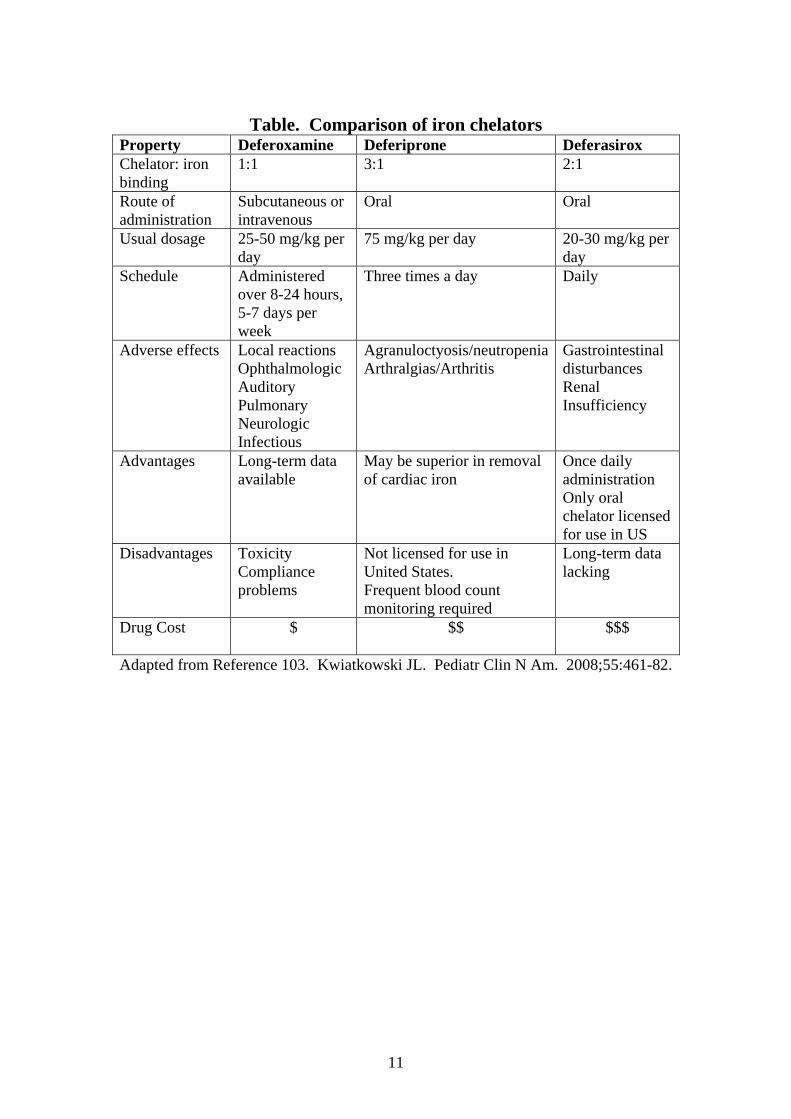
Table. Comparison of iron chelators
Property Deferoxamine Deferiprone Deferasirox Chelator: iron binding
1:1 3:1 2:1
Route of administration
Subcutaneous or intravenous
Oral Oral
Usual dosage 25-50 mg/kg per day
75 mg/kg per day 20-30 mg/kg per day
Schedule Administered over 8-24 hours, 5-7 days per week
Three times a day Daily
Adverse effects Local reactions Ophthalmologic Auditory Pulmonary Neurologic Infectious
Agranuloctyosis/neutropeniaArthralgias/Arthritis
Gastrointestinal disturbances Renal Insufficiency
Advantages Long-term data available
May be superior in removal of cardiac iron
Once daily administration Only oral chelator licensed for use in US
Disadvantages Toxicity Compliance problems
Not licensed for use in United States. Frequent blood count monitoring required
Long-term data lacking
Drug Cost
$ $$ $$$
Adapted from Reference 103. Kwiatkowski JL. Pediatr Clin N Am. 2008;55:461-82.

12
SUMMARY Acute iron poisoning continues to occur resulting in morbidity and mortality. Treatment of acute iron poisoning should focus on providing supportive care and administering deferoxamine parenterally. Oral iron chelators have not been widely studied in human, acute iron poisoning and are therefore not recommended. Worldwide many individuals with red cell disorders and myelodysplasia develop transfusion-associated chronic iron overload. Significant morbidity and mortality are associated with iron overload. Historically, deferoxamine was the only iron chelator available. Deferoxamine therapy is inconvenient, time-consuming, and associated with undesirable adverse effects resulting in non-compliance. Over the last couple of decades significant evidence has emerged supporting the use of the oral iron chelators deferiprone and deferasirox. Although both are effective at decreasing iron burden several characteristics favor deferasirox. The once daily dosing requirement for Deferasirox permits relative ease of administration and would be expected to positively contribute to treatment adherence. It also has a favorable adverse effect profile when compared to deferiprone which requires frequent blood count monitoring. Although more research and long-term follow up studies are needed for both oral chelators it is proposed that deferasirox be considered the oral chelator of choice in pediatric patients with transfusion-associated chronic iron overload.
13
REFERENCES 1. Madiwale T, Liebelt E. Iron: Not a Benign Therapeutic Drug. Curr Op Pediatr. 2006;18:174-9. 2. Cunningham MJ. Update on Thalassemia: Clinical Care and Complications. Hematol Oncol Clin North Am. 2010;24:215-27. 3. Toumba M, Sergis A, Kanaris C, Skordis N. Endocrine Complications in Patients with Thalassemia Major. Pediatr Endocrinol Rev. 2007;5:642-8. 4. Delvecchio M, Cavallo L. Growth and Endocrine Function in Thalassemia Major in Childhood and Adolescence. J Endocrinol Invest. 2010;33:61-8. 5. Hershko C. Pathogenesis and Management of Iron Toxicity in Thalassemia. Ann NY Acad Sci. 2010;1202:1-9. 6. Roberts D, Brunskill S, Doree C, Williams S, Howard J, Hyde C. Oral Deferiprone for Iron Chelation in People with Thalassemia. Cochrane Database Syst Rev. 2007;3:CD004839. 7. Meerpohl JJ, Antes G, Rücker G. Deferasirox for managing Transfusional Iron Overload in People with Sickle Cell Disease. Cochrane Database Syst Rev. 2010;4:CD007477. 8. Meerpohl JJ, Antes G, Rücker G. Deferasirox for Managing Iron Overload in People in People with Myelodysplastic Syndome. Cochrane Database Syst Rev. 2010;10:CD007461. 9. American Academy of Clinical Toxicology, European Association of Poison Control Centres and Clinical Toxicologists. Position Paper: Ipecac Syrup. J Toxicol Clin Toxicol. 2004;42:133-43. 10. American Academy of Clinical Toxicology, European Association of Poison Control Centres and Clinical Toxicologists. Position Paper: Gastric Lavage. J Toxicol Clin Toxicol. 2004;42:933-43. 11. Geffner ME, Opas LM. Phosphate Poisoning Complicating Treatment for Iron Ingestion. Am J Dis Child. 1980;134:509-10. 12. Bachrach L, Correa A, Levin R, Grossman M. Iron Poisoning: Complications of Hypertonic Phosphate Lavage Therapy. J Pediatr. 1979;94:147-9. 13. Dean BS, Krenzelok EP. In Vivo Effectiveness of Oral Complexation Agents in the Management of Iron Poisoning. J Toxicol Clin Toxicol. 1987;25:221-30. 14. Dean BS, Krenzelok EP. In Vivo Effectiveness of Oral Complexation Agents in the Management of Iron Poisoniong. J Toxicol Clin Toxicol. 1987;25:221-230.
14
15. Corby DG, McCullen AH, Chadwick EW, Decker WJ. Effect of Orally Administered Magnesium Hydroxide in Experimental Iron Intoxication. J Toxicol Clin Toxicol. 1985-1986;23:489-99. 16. Wallace KL, Curry SC, LoVecchio F, Raschke RA. Effect of Magnesium Hydroxide on Iron Absorption Following Simulated Mild Iron Overdose in Human Subjects. Acad Emerg Med. 1998;5:961-65. 17. Snyder BK, Clark RF. Effect of Magnesium Hydroxide Administration on Iron Absorption after a Supratherapeutic Dose of Ferrous Sulfate in Human Volunteers: A Randomized Controlled Trial. Ann Emerg Med. 1999;33:400-5. 18. American Academy of Clinical Toxicology, European Association of Poison Control Centres and Clinical Toxicologists. Position Paper: Single-Dose Activated Charcoal. Clin Toxicol. 2005;43:61-87. 19. American Academy of Clinical Toxicology, European Association of Poison Control Centres and Clinical Toxicologists. Position Paper: Whole Bowel Irrigation. J Toxicol Clin Toxicol. 2004;42:843-854. 20. Dean B, Oehme FW, Krenzelok E, Hines R. A Study of Iron Complexation in a Swine Model. Vet Hum Toxicol. 1988;30:313-5. 21. Dean BS, Oehme FW, Krenzelok EP, Griffith GR, Hines RH. Iron Complexation with Oral Deferoxamine . Vet Hum Toxicol. 1996;38:96-8. 22. Whitten CF, Gibson GW, Good MH, Goodwin JF, Brough AJ. Studies in Acute Iron Poisoning. I. Deferrioxamine in the Treatment of Acute Iron Poisoning: Clinical Observation, Experimental Studies, and Theoretical Considerations. Pediatrics. 1965;36:322-35. 23. Whitten CF, Chen Y, Gibson GW. Studies in Acute Iron Poisoning. II. Further Observations on Deferrioxamine in the Treatment of Acute Experimental Iron Poisoning. Pediatrics. 1966;38:102-110. 24. Jackson TW, Ling LJ, Washinton V. The Effect of Oral Deferoxamine on Iron Absorption in Humans. J Toxicol Clin Toxicol. 1995;33:325-9. 25. Gomez HF, McClafferty HH, Flory D, Brent J, Dart RC. Prevention of Gastrointestinal Iron Absorption by Chelation from an Orally Administered Premixed Dereroxamine/Charcoal Slurry. Ann Emerg Med. 1997;30:587-592. 26. Berkovitch M, Livne A, Lushkov G, et al. The Efficacy of Oral Deferiprone in Acute Iron Poisoning. Am J Emerg Med. 2000;18:36-40. 27. Bannerman RM, Callender ST, Williams DL. Effect of Desferrioxamine and D.T.P.A in Iron Overload. Br Med J. 1962;2:1573-1577. 28. Lee P, Mohammed N, Marshall L, et al. Intravenous Infusion Pharmacokinetics of Deferoxamine in Thalassaemic Patients. Drug Metab Disp. 1993;21:640-4.
15
29. Porter JB. Deferoxamine Pharmacokinetics. Semin Hematol. 2001;38:(1 Suppl 1):63-8. 30. Propper RD, Cooper B, Rufo RR, et al. Continuous Subcutaneous Administration of Deseroxamine in Patients with Iron Overload. N Engl J Med. 1977;297:418-23. 31. Propper RD, Shurin SB, Nathan DG. Reassessment of the use of Desferrioxamine in Iron Overload. N Engl J Med. 1976;294:1421-1423. 32. Hussain MA, Green N, Flynn DM, Hussein S, Hoffbrand AV. Subcutaneous Infusion and Intramuscular Injection of Desferrioxamine in Patients with Transfusional Iron Overload. Lancet. 1976;2:1278-80. 33. Borgna-Pignatti C, Cohen A. Evaluation of a New Method of Administration of the Iron Chelating Agent Deferoxamine. J Pediatr. 1997;130:86-88. 34. Smith RS. Iron Excretion in Thalassaemia Major After Administration of Chelating Agents. Br Med J. 1962;2:1577-80. 35. Olivieri NF, Nathan DG, MacMillan JH, et al. Survival in Medically Treated Patients with Homozygous B-Thalassemia. N Engl J Med. 1994;331:574-8. 36. Zurlo MG, De Stefano P, Borgna-Pignatti C, et al. Survival and Causes of Death in Thalassaemia Major. Lancet. 1989;2:27-30. 37. Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survival and Complications in Patients with Thalassemia Major Treated with Transfusion and Deferoxamine. Haematologica. 2004;89:1187-93. 38. Wolfe L, Oliveri N, Sallan D, et al. Prevention of Cardiac Disease by Subcutaneous Deferoxamine in Patients with Thalassemia Major. N Engl J Med. 1985;312:1600-3. 39. Brittenham GM, Griffith PM, Nienhuis AW, et al. Efficacy of Deferoxamine in Preventing Complications of Iron Overload in Patients with Thalassemia Major. N Engl J Med. 1994;331:567-73. 40. Cooper B, Bunn HF, Propper RD, Nathan DG, Rosenthal DS, Moloney WC. Treatment of Iron Overload in Adults with Continuous Parenteral Desferrioxamine. Am J Med. 1977;63:958-66. 41. Borgna-Pignatti C, Franchini M, Gandini G, Vassanelli A, De Gironcoli M, Aprili G. Subcutaneous Bolus Injection of Deferoxamine in Adult Patients Affected by Onco-hamatologic Diseases and Iron Overload. Haematologica. 1988;83:788-90. 42. Franchini M, Gandini G, de Gironcoli M, Vassanelli A, Borgna-Pignatti C, Aprili G. Safety and Efficacy of Subcutaneous Bolus Injection of Deferoxamine in Adult Patients with Iron Overload. Blood. 2000;95:2776-9.
16
43. Cossu P, Toccafondi C, Vardeu F, et al. Iron Overload and Desferrioxamine Chelation Therapy in Beta-thalassemia Intermedia. Eur J Pediatr. 1981;137:267-71. 44. Di Gregorio F, Romeo MA, Pizzarelli G, Aiello G, Russo G. An Alternative to Continuous Subcutaneous Infusion of Desferrioxamine in Thalassaemic Patients. Br J Haematol. 1997;98:601-2. 45. Wali YA, Taqi A, Deghaidi A. Study of Intermittent Intravenous Deferrioxamine High-dose Therapy in Heavily Iron-loaded Children with Beat-thalassemia Major Poorly Compliant to Subcutaneous Injections. Pediatr Hematol Oncol. 2004;21:453-60. 46. Davis BA, Porter JB. Long-term Outcomes of Continuous 24-hour Deferoxamine Infusions via Indwelling Intravenous Catheters in High-Risk Beta-Thalassemia. Blood. 2000;95:1229-36. 47. Barry M, Flynn DM, Letsky EA, Risdon RA. Long-term Chelation Therapy in Thalassaemia Major: Effect on Liver Iron Concentration, Liver Histology, and Clinical Progress. Br Med J. 1974;2:16-20. 48. Cohen A, Martin M, Schwartz E. Depletion of Excessive Liver Iron Stores with Desferrioxamine. Br J Haematol. 1984;58:369-73. 49. De Virgiliis S, Cossu P, Sanna G, et al. Iron Chelation in Transfusion-dependent Thalassemia with Chronic Hepatitis. Acta Haematol. 1982;67:49-56. 50. Cohen A, Schwartz E. Excretion of Iron in Response to Deferoxamine in Sickle Cell Anemia. J Pediatr. 1978;92:659-62. 51. Kalpatthi R, Peters B, Holloman D, et al. Safety and Efficacy of High Dose Intravenous Desferoxamine for Reduction of Iron Overload Due to Chronic Transfusion in Sickle Cell Patients. Blood. 2008;112:abst 1430. 52. Silliman CC, Peterson VM, Mellman DL, et al. Iron Chelation by Deferoxamine in Sickle Cell Patients with Severe Transfusion-induced Hemsiderosis: A Randomized, Double-blind Study of the Dose-response Relationship. J Lab Clin Med. 1993;122:48-54. 53. Aydinok Y, Erermis S, Bukusoglu N, et al. Psychosocial Implications of Thalassemia Major. Pediatr Int. 2005;47:84-9. 54. Delea TE, Edelsberg J, Sofrygin O, et al. Consequences and Costs of Noncompliance with Iron Chelation Therapy in Patients with Transfusion-dependent Thalassemia: a Literature Review. Transfusion. 2007;47:1919-29. 55. De Virgiliis S, Congia M, Frau F, et al. Deferoxamine-induced Growth Retardation in Patients with Thalassemia Major. J Pediatr. 1988;113:661-9. 56. Piga A, Roggero S, Salussolia I, Massano D, Serra M, Longo F. Deferiprone. Ann NY Acad Sci. 2010;1202:75-8.
17
57. Matsui D, et al. Relationship Between the Pharmacokinetics and Iron Excretion Pharmacodynamics of the New Oral Iron Chelator 1,2-dimethyl-3-hydroxypyrid-4-one in Patients with Thalassemia. Clin Pharmacol. 1991;50:294-98. 58. Kontoghiorghes GJ, Goddard JG, Bartlett AN, Sheppard L. Pharmacokinetic Studies in Human with the Oral Iron Chelator 1,2-dimethyl-3-hydroxypyrid-4-one. Clin Pharm Ther. 1990;48:255-61. 59. Gale GR, Litchenberg WH, Smith AB, Singh PK, Campbell RA, Jones MM. Comparative Iron Mobilizing Actions of Deferoxamine, 1,2 Dimethyl-3-hydroxypyrid-4-one, and Pyridoxal Isonicotinoyl Hydrazone in Iron Hydroxamate-loaded Mice. Res Commun Chem Pathol Pharmacol. 1991;73:299-313. 60. Bergeron RJ, Streiff RR, Wiegand J, Luchetta G, Creary EA, Peter HH. A Comparison of the Iron-chelating Properties of 1,2-dimethyl-3-hydroxypyrid-4-one, 1,2-diethyl-3-hydroxypyrid-4-one, and Deferoxamine. Blood. 1992;79:1882-90. 61. Olivieri NF, Koren G, Hermann C, et al. Comparison of Oral Iron Chelator L1 and Desferrioxamine in Iron-loaded Patients. Lancet. 1990;336:1275-9. 62. Collins AF, Fassos FF, Stobie S, et al. Iron-balance and Dose-response Studies of the Oral Iron Chelator 1,2-dimethyl-3-hydroxypyrid-4-1 (L1) in Iron-loaded Patients with Sickle Cell Disease. Blood. 1994;83:2329-2333. 63. Cappellini MD, Musallam KM, taher AT. Overview of Iron Chelation Therapy with Desferrioxamine and Deferiprone. Hemoglobin. 2009;33:S58-S69. 64. Cohen AR, Galanello R, Piga A, De Sanctis V, Tricta F. Safety and Effectiveness of Long-term Therapy with the Oral Iron Chelator Deferiprone. Blood. 2003;102:1583-7. 65. Goel H, Girish KM, Phadke SP. Long-term Efficacy of Oral Deferiprone in Management of Iron Overload in Beta Thalassemia Major. Hematology. 2008;13:77-82. 66. Olivieri NF, Brittenham GM, Matsui D, et al. Iron Chelation Therapy with Oral Deferiprone in Patients with Thalassemia Major. N Engl J Med. 1995;332:918-22. 67. Olivieri NF, Brittenham GM, McLaren CE, et al. Long-term Safety and Effectiveness of Iron-chelation Therapy with Deferiprone for Thalassemia Major. N Engl J Med. 1998;339:417-23. 68. El Alfy M, Sari TT, Lee CL, Tricta F, El-Beshlawy A. The Safety, Tolerability, and Efficacy of a Liquid Formulation of Deferiprone in Young Children with Transfusional Iron Overload. J Pediatr Hematol Oncol. In Press. 69. Won SC, Han DK, Seo JJ, et al. Efficacy and Safety of Deferipron (Ferriprox), an Oral Iron-chelating Agent, in Pediatric Patients. Korean J Hematol. 2010;45:58-61.
18
70. Al-Refaie FN, Wonke B, Hoffbrand AV, et al. Efficacy and Possible Adverse Effects of the Oral Iron Chelator 1,2-dimethyl-3-hydroxypyrid-4-1 (L1) in Thalassemia Major. Blood. 1992;80:593-99. 71. Mazza P, Amurri B, Lazzari G, et al. Oral Iron Chelating Therapy: a Single Center Interim Report on Deferipron (L1) in Thalasssemia. Haematologica. 1998;83:496-501. 72. Del Vecchio GC, Crollo E, Schettini F, et al. Factors Influencing Effectiveness of Deferiprone in a Thalassemia Major Setting. Acta Hematol. 2000;104:99-102. 73. Maggio A, D’Amico GD, Morabito A, et al. Deferiprone versus Deferoxamine in Patients with Thalassemia Major: a Randomized Clinical Trial. Blood Cell Mol Dis. 2002;28:196-208. 74. Maggio A, Vitrano A, Capra M, et al. Long-term Sequential Deferiprone-deeroxamine versus Deferiprone Alone for Thalassaemia Major Patients: a Randomized Clinical Trial. Br J Haematol. 2009;145:245-54. 75. Daar S, Pathare AV. Combined Therapy with Desferrioxamine and Deferiprone in Beta Thalassemia Major Patients with Transfusional Iron Overload. Ann Hematol. 2006;85:315-9. 76. Origa R, Bina P, Agus A. Combined Therapy with Deferiprone and Desferrioxamine in Thalassemia Major. Haematologia. 2005;90:1309-14. 77. Galanello R, Kattamis A, Piga A. A Prospective Randomized Controlled Trial on the Safety and Efficacy of Alternating Deferoxamine and Deferiprone in the Treatment of Iron Overload in Patients with Thalassemia. Haematologia. 2006;91:1241-1243. 78. Kolnagou A, Kleanthous, Kontoghiorghes GJ. Reduction of Body Iron Stores to Normal Range Levels in Thalassaemia by using a Deferiprone/deferoxamine Combination and their Maintenance thereafter by Deferiprone Monotherapy. Eur J Haematol. 2010;85:1-9. 79. Farmaki K, Tzoumari I, Pappa C, Chouliaras G, Berdoukas V. Normalisation of Total Body Iron load with Very Intensive Combination Chelation Resverses Cardiac and Endocrine Complications of Thalassaemia major. Br J Haematol. 2010;148:466-75. 80. Tsiapras D, Fragatou S, Farmaki K, et al. Effect of Combined Chelation Therapy with Deferipron and Deferoxamine of Left Ventricular Diastolic Function in Adult Beta-thalassemia Major Patients. Hemoglobin. 2010;34:210-20. 81. Tsironi M, Assimakopoulos G, Polonofi K, Rigaki K, Aessopos A. Effects of Combined Deferiprone and Deferoxamine Chelation Therapy on Iron Load Indices in Beta-thalassemia. Hemoglobin. 2008;32:29-34. 82. Christofordis A, Haritandi A, Tsatra I, Tsitourides I, Karyda S, Athanassiou-Metaxa M. Four-year Evaluation of Myocardial and Liver Iron Assessed
19
Prospectively with Serial MRI Scans in Young Patients with Beta-thalassemia Major: Comparison Between Different Chelation Regimens. Eur J Haematol. 2007;78:52-7. 83. D’Angelo E, Mirra N, Rocca A, Carnelli V. Combined Therapy with Desferrioxamine and Deferiprone: a New Protocol for Iron Chelation in Thalassemia. J Pediatr Hematol Oncol. 2004;26:451-3. 84. Alymara V, Bourantas D, Chaidos A, et al. Effectiveness and Safety of Combined Iron-chelation Therapy with Deferoxamine and Deferiprone. Hematol J. 2004;5:475-9. 85. Aydinok Y, Ulger Z, Nart D, et al. A Randomized Controlled 1-year Study of Daily Deferiprone Plus Twice Weekly Desferrioxamine Compared with Daily Deferiprone Monotherapy in Patients with Thalassemia Major. Haematologia. 2007;92:1599-606. 86. Kolnagou A, Economides C, Eracleous E, Kontoghiorghes GJ. Long Term Comparative Studies in Thalassemia Patients Treated with Deferoxamine or a Deferoxamine/deferiprone Combination. Identification of Effective Chelation Therapy Protocols. Hemoglobin. 2008;32:41-7. 87. Peng CT, Wu KH, Wu SF, et al. Deferiprone or Deferoxamine vs. Combination Therapy in Patients with Beta-thalassemia major: a Case Study in Taiwan. Hemoglobin. 2006;30:125-30. 88. Kattamis A, Ladis V, Berdousi H, et al. Iron Chelation Treatment with Combined Therapy with Deferiprone and Deferioxamine: a 12-month Trial. Blood Cells Mol Dis. 2006;36:21-5. 89. Lai ME, Grady RW, Vacquer S, et al. Increased Survival and Reversion of Iron-induced Cardiac Disease in Patients with Thalassemia Major receiving Intensive Combined Chelation Therapy as Compared to Desferoxamine Alone. Blood Cells Mol Dis. 2010;45:136-9. 90. Pepe A, Meloni A, Capra M. Deferasirox, Deferiprone and Desferrioxamine Treatment in Thalassemia Major Patients: Cardiac Iron and Function Comparison Determined by Quantitative Magnetic Resonance Imaging. Haematologica. 2010 Sep 30. In press. 91. Ricchi P, Ammirabile M, Spasiano A, et al. Combined Chelation Therapy in Thalassemia Major with Deferiprone and Desferrioxamine: a Reterospective Study. Eur J Haematol. 2010;85:36-42. 92. Galanello R, Agus A, Campus S, Danjou F, Giardina PJ, Grady RW. Combined Iron Chelation Thearpy. Ann NY Acad Sci. 2010;1202:79-86. 93. Hoffbrand AV, Cohen A, Hershko C. Role of Deferiprone in Chelation Therapy for Transfusional Iron Overload. Blood. 2003;102:17-24. 94. Ceci A, Baiardi P, Felisi M, et al. The Safety and Effectiveness of Deferiprone in a Large-scale 3-year Study in Italian Patients. Br J Haematol. 2002;118:330-6.
20
95. Al-Refaie FN, Wonke B, Hoffbrand AV. Deferiprone-associated Myelotoxicity. Eur J Haematol. 1994;53:298-301. 96. Cappellini MD, Piga A. Current Status in Iron Chelation in Hemoglobinopathies. Curr Mol Med. 2008;8:663-74. 97. Cohen AR, Galanello R, Piga A, DiPalma A, Vullo C, Tricta F. Safety Profile of the Oral Iron Chelator Deferiprone: a Multicenter Study. Br J Haematol. 2000;108:305-312. 98. Hoffbrand AV, Al-Refaie F, Davis B, et al. Long-term Trial of Deferiprone in 51 Transfusion-dependent Iron Overloaded Patients. Blood. 1998;91:295-300. 99. Wanless A, Sweeney G, Dhillon AP, et al. Lack of Progressive Hepatic Fibrosis During Long-term Therapy with Deferiprone in Subjects with Transfusion-dependent Beta-thalassemia. Blood. 2002;100:1566-9. 100. Tondury P, Zimmerman A, Nielsen P, et al. Liver Iron and Fibrosis during Long-term Treatment with Deferiprone in Swiss Thalassaemic Patients. Br J Haematol. 1998;101:413-5. 101. Al-Refaie FN, Hershko C, Hoffbrand AV, et al. Results of Long-term Deferiprone (L1) Therapy: a Report by the International Study Group on Oral Iron Chelators. Br J Haematol. 1995;91:224-9. 102. Ceci A, Baiardi P, Felisi M, et al. The Safety and Effectiveness of Deferiprone in a Large-scale 3-year Study in Italian Patients. Br J Haematol. 2002;118:330-6. 103. Kwiatkowski JL. Oral Iron Chelators. Pediatr Clin N Am. 2008;55:461-82. 104. Waldmeier F, Bruin GJ, Glaenzel U, et al. Pharmacokinetics, Metabolism, and Disposition of Deferasirox in Beta-thalassemic Patients with Transfusion-dependent Iron Overload who are at Pharmacokinetic Steady State. Drug Metab Dispos. 2010;38:808-16. 105. Lindsey WT, Olin BR. Deferasirox for Transfusion-related Iron Overload: A Clinical Review. Clin Ther. 2007;29:2154-66. 106. Glickstein H, El RB, Link G, et al. Action of Chelators in Iron-loaded Cardiac Cells. Accessibility to Intracellular Labile Iron and Functional Consequences. Blood. 2006;108:3195-203. 107. Wood JC, Otto-Duessel M, Gonzalez I, et al. Deferasirox and Deferiprone remove Cardiac Iron in the Iron-overloaded Gerbil. Trans Res. 2006;148:272-80. 108. Wood JC, Glynos T, Thompson A, et al. Follow-up Report on the 2-year Cardiac Data from a Deferasirox Monotherapy Trial. Am J Hematol. 2010;85:818-9. 109. Wood JC, Kang BP, Thompson A, et al. The Effect of Deferasirox on Cardiac Iron in Thalassemia Major: Impact of Total Body Iron Stores. Blood. 2010;116:537-43.
21
110. Pathare A, Taher A, Daar S. Deferasirox (Exjade) Significantly Improves Cardiac T2* in Heavily Iron-Overlaoded Patients with beta-Thalassemia Major. Ann Hematol. 2010;89:405-9. 111. Pennell DJ, Porter JB, Cappellini MD, et al. Efficacy of Deferasirox in Reducing and Preventing Cardiac Iron Overload in B-thalassemia. Blood. 2010;115:2364-71. 112. Nisbet-Brown E, Olivieri NF, Giardina PJ, et al. Effectiveness and Safety of ICL670 in Iron-loaded Patients with Thalassemia: a Randomised, Double-blind, Placebo-controlled, Dose-escalation Trial. Lancet. 2003;361:1597-602. 113. Piga A, Galanello R, Forni GL, et al. Randomized Phase II Trial of Deferasirox (Exjade, ICL 670), a Once-daily, Orally Administered Iron Chelator, in Comparison to Deferoxamine in Thalassemia Patients with Transfusional Iron Overload. Haematologia. 2006;91:873-80. 114. Vichinsky E, Onyekwere O, Porter J, et al. A Randomised Comparison of Deferasirox versus Deferoxamine for the Treatment of Transfusional Iron Overload in Sickle Cell Disease. Br J Haematol. 2006;136:501-8. 115. Cappellini MD, Cohen A, Piga A, et al. A Phase 3 Study of Deferasirox (ICL670), a Once-daily Oral Iron Chelator, in Patients with B-thalassemia. Blood. 2006;107:3455-62. 116. Taher A, El-Beshlawy A, Elalfy M, et al. Efficacy and Safety of Deferasirox, an Oral Iron Chelator, in Heavily Iron-Overloaded Patients with B-thalassemia: the ESCALATOR Study. Eur J Haematol. 2009;82:458-65. 117. Cappellini MD, Porter J, El-Beshlawy A, et al. Tailoring Iron Chelation by Iron intake and Serum Ferritin: the Prospective EPIC Study of Deferasirox in 1744 patients with Transfusion-dependent Anemia. Haematologica. 2010;95:557-66. 118. Gattermann N, Finelli C, Porta MD, et al. Deferasirox in Iron-overloaded Patients with Transfusion-dependent Myelodysplastic Syndromes: Results from a Large 1-year EPIC Study. Leuk Res. 2010;34:1143-50. 119. Taher A, Cappellini MD, Vichinsky E, et al. Efficacy and Safety of Deferasirox Dose of >30 mg/kg per d in Patients with Transfusion-dependent Anaemia and Iron Overload. Br J Haematol. 2009;147:752-9. 120. Porter JB. Deferasirox—Current Knowledge and Future Challenges. Ann NY Acad Sci. 2010;1202:87-93. 121. Galanello R, Piga A, Forni GL, et al. Phase II Clinical Evaluation of Deferasirox, a Once-daily Oral Chelating Agent, in Pediatric Patients with B-thalassemia major. Haematologia. 2006;91:1343-51.
22
122. Product Information: Ferriprox ® Apo Pharma. Ontario, Canada. Available at: http://www.ferriprox.com/aboutferriprox/default_intl.asp. Last accessed December 12, 2010. 123. Product Information: EXJADE ® . Novartis. East Hanover, New Jersey, US. Available at: http://www.us.exjade.com/patient/full-prescribing-information.jsp. Last accessed December 12, 2010. 124. Neufeld EJ. Oral Chelators Deferasirox and Deferiprone for Transfusional Iron Overload in Thalassemia Major: New Data, New Questions. Blood. 2006;107:3436-41. 125. Imran F, Phatak P. Pharmacoeconomic Benefits of Deferasirox in the Management of Iron Overload Syndomes. Expert Rev Pharmacoecon Outcomes Res. 2009;9:297-304. 126. Tolley K, Oliver N, Miranda E, Migliaccio-Walle K, Bozkaya D, Li Q. Cost Effectiveness of Deferasirox Compared to Desferrioxamine in the Treatment of Iron Overload in Lower-risk, Transfusion-dependent Myelodysplastic Syndrome Patients. J Med Econ. 2010;13:559-70.