nurs-ed-53 - strac
TRANSCRIPT

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 1 of 14
NURS-ED-53 Approval Date: 08/14
Title: Acute Coronary Syndrome (ACS) and Heart Alert
in the Emergency Department
Document Number: NURS-ED-53
Document Type: Policy, Procedure
Affected Departments: Emergency Department (ED), Catheterization Lab
(Cath Lab)
Review Bodies:
Position or Committee Date Review
Completed
BHS Regional Chest Pain Steering
Committee
(Owning body)
08/14
BHS Cardiovascular Service Line 09/14
BHS ED Service Line 08/14
Revision/(Review) Dates: (Dates that included only a review, but no content
revision, are in parentheses)
07/14
Effective Date: 08/14
SUMMARY OF ATTACHMENTS:
Associated Policies/Procedures: Nursing Care Protocols Guidelines for the Emergency
Department, NURS-ED-23
Patient Transfer, RM-EMTALA-01
Other Associated Document(s): Heart Alert Audit Tool, Attachment A
IMPACT Protocol, Attachment B
STEMI Walk-In/EMS Pathway, Attachment C
Transfer Process for MTB, Attachment D
Risk Stratification, Attachment E
ACS Clinical Pathways, Attachment F
Associated Form(s): EMS Prehospital ECG/Rhythm Strip, BHS-MR 90508802
Thrombolytic Orders for STEMI, BHS Orders Set #CA-CL08
CDU: Chest Pain Possible ACS, BHS-CD-CA03
AMI Admission Orders, CM-BH01
APPROVED BY:
Approval Body
(Position or Committee) Name Authentication Date
Quality & Patient Safety Steering
Committee
Meeting Minutes &
Digital Signatures
08/14
Medical Executive Board
Meeting Minutes 09/14

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 2 of 14
NURS-ED-53 Approval Date: 08/14
I. PURPOSE
To define and outline the process of an Emergency Department (ED) ACS and Heart Alert
patient from first medical contact to percutaneous coronary intervention (PCI).
II. DEFINITION(S)
A. Heart Alert
Heart Alert is the notification process that triggers a rapid chain of events leading to the
activation of the Cardiac Catheterization Lab (Cath Lab) team and the interventional
cardiologist on-call to the Cath Lab for acute treatment of a patient with symptoms of an
ST-segment elevation myocardial infarction (STEMI) or new left bundle branch block
(LBBB). The treating Cardiologist will determine the appropriate treatment of patients
with new or presumed new LBBB and possible Acute Coronary Syndrome. Heart Alert
is designed to shorten the door to PCI times (D2B) and heighten awareness using a
single paging system and calling Interventional Cardiology.
B. ST-segment Elevation Myocardial Infarction (STEMI)
STEMI is a clinical syndrome defined by characteristic symptoms of myocardial
ischemia in association with persistent electrocardiographic (ECG) diagnostic ST
elevation (at the J point in at least 2 contiguous leads of _2 mm (0.2 mV) in men or _1.5
mm (0.15 mV) in women in leads V2–V3 and/or of _1 mm (0.1 mV) in other contiguous
chest leads or the limb leads) and subsequent release of biomarkers of myocardial
necrosis. New or presumably new Left Bundle Branch Block (LBBB) has been
considered a STEMI equivalent (ACCF/AHA, 2013).
C. Percutaneous Coronary Intervention (PCI)
Percutaneous Coronary Intervention (PCI) is a non-surgical, minimally invasive
procedure that uses a catheter (a thin flexible tube) inserted into a blood vessel either in
the leg or arm to place a small structure called a stent to open up blood vessels in the
heart that have been narrowed by plaque buildup, a condition known as atherosclerosis.
D. Early Risk Assessment
For admitted patients, risk stratification is done after exclusion of STEMI/New LBBB
and other non-cardiac diagnoses.
Stratification is based on history, physical exam, ECG, lab and x-ray as determined by
the treating physician. A variety of tools such as TIMI, Braunwald, and Grace criteria
have been used to measure risk of mortality and recurrent cardiac events. However, in
the Emergency Department the decision to admit or discharge a patient should be based
on clinical judgment since these criteria have not been shown to be superior to physician
judgment. Risk stratification of admitted patients may guide additional therapies as an
inpatient.
E. First Medical Contact
The point at which the patient is either initially assessed by EMS or other medical
personnel in the pre-hospital setting or the patient arrives at the hospital’s emergency
department.

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 3 of 14
NURS-ED-53 Approval Date: 08/14
III. POLICY
The American College of Cardiology Foundation (ACCF) and the American Heart
Association (AHA) Task Force on Practice Guidelines recommend a Regional Systems of
STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals to enable rapid
recognition and timely reperfusion of patients with STEMI. System delays to reperfusion are
correlated with higher rates of mortality and morbidity.
The Southwest Regional Advisory Council (STRAC) formed a Regional Cardiac Systems
Committee in January 2008 to develop a cooperative and regional approach to STEMI care.
The Baptist Health System worked with other members of the healthcare community to
develop the HEART ALERT activation system to enable rapid recognition and timely
reperfusion of patients with STEMI.
IV. PROCEDURE
A. EMS Pre-hospital to Cath Lab
Patients arriving to the ED via EMS.
1. Pre-hospital Work Up
a. EMS completes a 12-lead ECG in the field to identify a STEMI or new LBBB.
2. ED Notification
a. After a STEMI or new LBBB is identified, the 12-lead ECG is transmitted to the
ED’s ECG receiving station where it is reviewed by the ED physician and/or ED
nurse.
b. If EMS is unable to transmit the ECG or the ECG receiving station is inoperable,
EMS will relay his/her findings to ED staff via the EMS phone or radio.
Additionally EMS will provide a detailed assessment of the 12-lead ECG to
include the computer derived interpretation and a description of the leads with
ST segment elevation.
3. Activation of Heart Alert
a. Based on the pre-hospital 12-Lead ECG and the EMS report of Heart Alert, the
ED Physician and/or ED nurse will activate a Heart Alert prior to the patient’s
arrival using a single paging system and calling Interventional Cardiology (see
below and STEMI Walk-In/EMS Pathway Flowchart (Attachment C)).
b. Initiating a BHS Heart Alert includes calling the on-call Interventionalist and
activating the Cath Lab team using a single page system. Nursing directors,
house officer, and administration will also be notified with paging system.
c. The pre-hospital ECG’s are mounted on BHS Pre-Hospital ECG/Rhythm Strip
mounting sheet. The pre-hospital ECG is given to the ED physician (goal less
than 10 minutes) who will generate a written record of their interpretation and
place in patient’s permanent medical record.
d. Reference to STEMI Walk-In/EMS Pathway Flowchart (Attachment C).
4. Patient Preparation
a. The ED staff will initiate the IMPACT protocol (Attachment B).

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 4 of 14
NURS-ED-53 Approval Date: 08/14
5. Transport to the Cath Lab
a. Once the Cath Lab team arrives the patient is transported to the Cath Lab by ED
personnel and/or Cath Lab team.
b. Verbal report providing pertinent information and the ED chart; medication
reconciliation, heart alert audit tool, original ECG, ED nursing documentation,
ED physician documentation is given to the Cath Lab team.
B. ED Walk-in to Cath Lab
Patients presenting to the ED with signs or symptoms of acute coronary syndrome, not
arriving by EMS.
1. Triage
a. The patient is initially greeted by a Registered Nurse or an employee who has
had annual formal training in ACS signs and symptoms.
2. ED Work-up
a. The triage nurse will ensure a 12-lead ECG is completed as soon as possible
upon identifying the chief complaint of Chest Pain or ACS symptoms. (Goal: less
than five minutes from time of arrival).
b. The ED Physician will review the ECG for evidence of STEMI and sign the
ECG. The triage nurse triages the patient based on standard Emergency Severity
Index (ESI) guidelines. (Goal: less than 10 minutes)
c. After the ECG is performed, patient will be transferred from triage to an
Emergency Department room if bed available. If no bed available chest pain
protocols will be initiated per BHS Nursing Care Protocols Guidelines for the
Emergency Department, NURS-ED-23.
3. Activation of Heart Alert
a. Based on the 12-lead ECG, the ED physician will activate a Heart Alert using a
single paging system and calling Interventional Cardiology for a STEMI or
presumed new LBBB.
b. Initiating a BHS Heart Alert includes calling the on-call Interventionalist and
activating the Cath Lab team using a single page system. Nursing directors,
house officer, and administration will also be notified with paging system.
4. Patient Preparation
a. The ED staff will initiate the IMPACT protocol (Attachment B).
5. Transport to the Cath Lab
a. Once the Cath Lab team arrives the patient is transported to the Cath Lab by ED
personnel and/or Cath Lab team.
b. Verbal report providing pertinent information and the ED chart; medication
reconciliation, heart alert audit tool, original ECG, ED nursing documentation,
ED physician documentation is given to the Cath Lab team.
6. Reference STEMI Walk-In/EMS Pathway Flowchart (Attachment C).

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 5 of 14
NURS-ED-53 Approval Date: 08/14
C. Thrombolytic Therapy
1. In some patients with identified STEMI the ED physician may decide the patient
would benefit from Thrombolytic therapy if PCI will be delayed. For example, a
patient in the first 120 minutes of symptoms where there will be greater than a 90
minute delay in PCI may do better if given thrombolytic. Refer to BHS
Thrombolytic Orders for STEMI.
D. Mission Trail Baptist Hospital Transfer Process
1. Mission Trails Baptist hospital does not perform heart catheterizations for acute
treatment. If the patient presents with STEMI or presumed new LBBB, a heart alert
is paged alerting Baptist Medical Center Cath Lab and the interventional cardiologist
is notified.
2. Following the BHS Patient Transfer Policy, RM-EMTALA-01, the patient is
transferred to Baptist Medical Center Cath Lab by EMS (Attachment D).
3. See Attachment D for transfer process flowchart.
E. Risk Stratification Guide
1. Risk stratification is done for admitted patients using the guide after exclusion of
STEMI/New LBBB and other non-cardiac diagnoses (Attachment E). Consider
utilization of the BHS Low Risk Chest Pain Orders (order number) for low risk
patients or BHS Admission Orders Acute MI (order number) for non-low risk
patients.
2. Patient’s being admitted will be admitted to a cardiac monitoring unit.
3. Nursing handoff per BHS Hand-Off Communication, RM-PS-04, with original ECG
accompanying the patient and an additional copy scanned into the medical record.
4. Reference BHS ACS Clinical Pathways flowchart (Attachment F).
V. REFERENCES
American Heart Association. (2013). ACCF/AHA practice guideline. Circulation, 127,
e663-e828. doi: 10.1161/CIR.0b013e31828478ac. Retrieved from:
http://circ.ahajournals.org/content/127/23/e663.full
Hess, E. (2012). Diagnostic accuracy of the TIMI risk score in patients with chest pain in the
emergency department: A meta-analysis. Canadian Medical Association Journal,
182(10), 1039-1044. doi: 10.1503/cmaj.092119
Manini, A., Dannemann, N., Brown D., Butler, J., Nagurney, J., et al. (2009). Limitations of
risk score models in patients with acute chest pain. American Journal of Emergency
Medicine, 27(1), 42-48. doi: 10.1016/j.ajem/2008.01.022
Meyer, M., Mooney, R., & Sekera, A. (2006). A critical pathway for patients with acute
chest pain and low risk for short-term adverse cardiac events: Role of outpatient
stress testing. Annals of Emergency Medicine, 47(5). doi:
10.1016/j.annemergmed.2005.10.010
Norekyl, T., Lindahl, B., Hasin, Y., McLean, S., Tubaro, M., & et al. (2012). Pre-hospital
treatment of STEMI patients: A scientific statement of the working group acute care
of the European society of cardiology. Acute Cardiology Care, 13, 56-67.

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 6 of 14
NURS-ED-53 Approval Date: 08/14
O’Gara, P., Kushner, F., Ascheim, D., Casey, D., Chung, M., & et al. (2013). 2013
ACCF/AHA Guideline for the management of ST-evelation myocardial infarction:
Executive summary. Journal of the American College of Cardiology, 61(4), 485-510.
doi: 10.1016/j.jacc.2012.11.018

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 7 of 14
NURS-ED-53 Approval Date: 08/14
Heart Alert Audit Tool
Attachment A

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 8 of 14
NURS-ED-53 Approval Date: 08/14
IMPACT Protocol
Attachment B
The IMPACT protocol was designed to expedite STEMI care in the ED while the Heart Alert team
is in route to the facility. IMPACT is an acronym for the following:
1. Identify and consent the patient (if applicable)
2. Medicate the patient. Communicate with the physician(s) regarding the patient’s
medication needs (example: ASA, pain medication, heparin, beta blockers, etc.). Remember,
the key is good communication
3. Pads. Use radiolucent defibrillator pads (white leads). Place one pad on the right back and
the other on the left side.
4. Access X 2. Please provide two (2) IV access points. Draw labs/cardiac biomarkers.
5. Clip (both sides of groin). Trim from the groin to just above the knee. Electric clipper only.
6. Transport on monitor with defibrillator/external pacing capability. Assist Cath Lab staff
with transporting the patient to the Cath lab and transferring the patient to the procedure
table. Assist with lead, BP monitor, O2, and SPO2 placement. When applicable, assist
family members to the waiting area.
Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 9 of 14
NURS-ED-53 Approval Date: 08/14
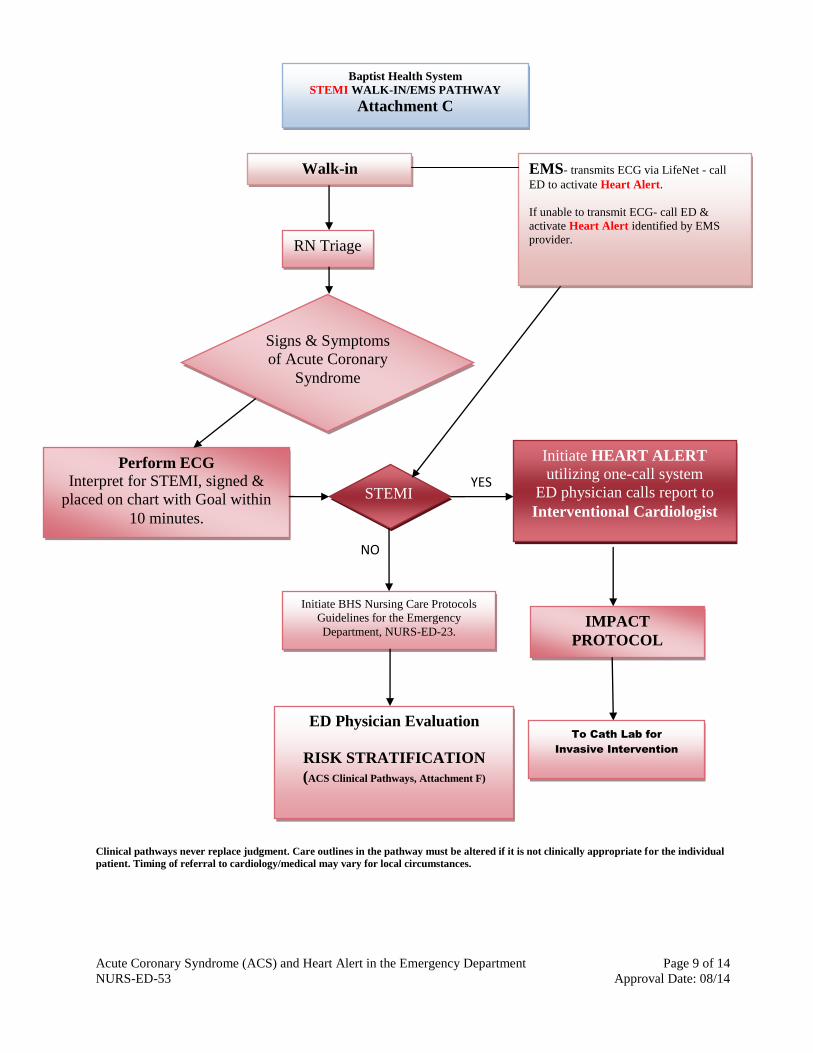
YES
NO
Clinical pathways never replace judgment. Care outlines in the pathway must be altered if it is not clinically appropriate for the individual
patient. Timing of referral to cardiology/medical may vary for local circumstances.
RN Triage
Signs & Symptoms
of Acute Coronary
Syndrome
Perform ECG
Interpret for STEMI, signed &
placed on chart with Goal within
10 minutes.
STEMI
Initiate BHS Nursing Care Protocols
Guidelines for the Emergency
Department, NURS-ED-23.
Initiate HEART ALERT
utilizing one-call system
ED physician calls report to
Interventional Cardiologist
IMPACT
PROTOCOL
To Cath Lab for
Invasive Intervention
ED Physician Evaluation
RISK STRATIFICATION
(ACS Clinical Pathways, Attachment F)
EMS- transmits ECG via LifeNet - call
ED to activate Heart Alert.
If unable to transmit ECG- call ED &
activate Heart Alert identified by EMS
provider.
Walk-in
Baptist Health System
STEMI WALK-IN/EMS PATHWAY
Attachment C

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 10 of 14
NURS-ED-53 Approval Date: 08/14
Transfer Process for Mission Trails Baptist
Attachment D
ED Physician decides Thrombolysis may be
preferable to transport in select patients
Thrombolysis Order Set

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 11 of 14
NURS-ED-53 Approval Date: 08/14
Risk Stratification
Attachment E
Risk Stratification for Likelihood of Acute Coronary Syndrome and
Short Term morbidity/mortality
For Admitted patients after exclusion of STEMI/New LBBB and other non-cardiac diagnoses.
Stratification based on history, physical exam, ECG, lab and x-ray as determined by the treating
physician. This is a guide, but not a substitute for clinical judgment, which in multiple studies has
been found to be equivalent or better than scoring tools.
High Risk any of the following (suggest use of appropriate ACS physician order set)
☐Known Medical history of Coronary Artery Disease, MI, or Revascularization.
☐Chest or Left arm pain similar to prior symptom of angina or MI
☐Elevated cardiac troponin
☐Hypotension OR pulmonary edema on presentation
☐New (or presumed new) ST deviation (≥0.5 mm)
☐New (or presumed new) T-wave inversion (>1mm or in multiple precordial leads)
☐New RBBB
☐Ventricular tachycardia
Moderate Risk (suggest use of appropriate ACS physician order set)
☐Chest or Left arm pain or discomfort as chief symptom (do not mark if clearly chest wall pain,
GERD or pleuritic in nature)
☐Diabetes
☐Extracardiac vascular disease (CVA, PVD, AAA)
☐Pathologic Q waves
☐Age >70
☐2-3 risk factors for CAD
Low Risk (suggest use of appropriate ACS physician order set)
☐Absence of STEMI/New LBBB, High Risk Criteria or Moderate risk

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 12 of 14
NURS-ED-53 Approval Date: 08/14
Baptist Health System ACS Clinical Pathways
Attachment F
Diagnosis STEMI Angioplasty STEMI Thrombolysis
Probable NSTEMI Possible ACS Non-ACS
Clinical Evaluation/Symptoms
Based on ED Physician evaluation
Consistent with ACS Consistent with ACS Consistent with ACS Consistent with ACS or atypical Not consistent with ACS
ECG (as indicated)
Completed in <5 MINUTES
ECG given to physician for interpretation. Goal within 10 minutes.
Physician records time and interpretation.
Findings:
ST Elevation/New LBBB
ECG given to physician for interpretation. Goal within 10 minutes.
Physician records time and interpretation.
Findings:
ST Elevation/New LBBB
ECG given to physician for interpretation. Goal within 10 minutes. Physician records time and interpretation. Findings: Absence of ST Elevation/New LBBB
ECG given to physician for interpretation. Goal within 10 minutes.
Physician records time and interpretation. Findings:
Absence of ST Elevation/New LBBB
ECG given to physician for interpretation. Goal within 10 minutes.
Physician records time and interpretation.
Findings:
Not consistent with ACS
TESTS Labs/ Cardiac Biomarkers, CXR
Findings: Initial labs not a determinant of diagnosis or disposition
Labs/ Cardiac Biomarkers, CXR
Findings: Initial labs not a determinant of diagnosis or disposition
Labs/ Cardiac Biomarkers, CXR
Findings:
(+) Cardiac Troponin
Labs/Cardiac Biomarkers, CXR
Screening for non-ACS etiology as indicated.
Stress Test as indicated
Findings: (-) Cardiac Troponin
Diagnostic tests determined by ED Physician Evaluation. Screening for non-ACS etiology as indicated.
Findings: (-) Cardiac Troponin if ordered

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 13 of 14
NURS-ED-53 Approval Date: 08/14
Diagnosis STEMI Angioplasty STEMI Thrombolysis
Probable NSTEMI Possible ACS Non-ACS
MEDICATIONS ASA chewed (unless contraindicated)
*See IMPACT Protocol #2
ASA chewed (unless contraindicated)
*See IMPACT Protocol #2
ASA chewed (unless contraindicated)
ASA chewed (unless contraindicated)
Medications determined by ED Physician Evaluation, as appropriate for determined etiology
DISPOSITION Activate HEART ALERT- CONTACT INTERVENTIONAL CARDIOLOGIST
Initiate IMPACT Protocol.
TRANSFER TO CATHERIZATION LAB
(MTB Only)- Follow MTB to BMC STEMI Transfer Process
Activate HEART ALERT- CONTACT INTERVENTIONAL CARDIOLOGIST
Initiate IMPACT Protocol.
TRANSFER TO CATHERIZATION LAB
(MTB Only)- Follow MTB to BMC STEMI Transfer Process
In the event of a significant delay in the availability of the Cath lab or interventional cardiologist, consider Thrombolysis. Follow Thrombolytic Policy.
Admit to Cardiac Monitoring Unit. Implement AMI Physician Order Set
Secondary Risk Stratification
Further risk stratification using Risk Stratification tool (Attachment E)
Discharged Instructions based on determined etiology including specific information that includes risk and lifestyle modifications as indicated. Follow-up instructions provided.
Moderate or High Risk
Place patient in Observation Status to Cardiac Monitored Unit, use appropriate ACS physician order set.
Low Risk
Place in Observation Status to Cardiac Monitored Unit, use appropriate ACS Physician order set. May consider discharge from Emergency Department with follow up plan. Discharge patients receive information that includes risk and lifestyle modifications and outpatient follow-up. If Stress Test not done during initial visit, discharge instructions should include a follow up plan with physician.

Acute Coronary Syndrome (ACS) and Heart Alert in the Emergency Department Page 14 of 14
NURS-ED-53 Approval Date: 08/14
1. (-) ECG means normal or unchanged from previous ECG
2. Non-STEMI Definition: Either one of the following criteria satisfies the diagnosis of an acute, evolving or recent MI:
a.) Rise and fall of biochemical markers for myocardial necrosis with at least one of the following: ischemic symptoms, development of pathologic Q waves on ECG, and ECG changes indicative of
ischemia (ST elevation or depression).
b.) Pathologic findings of AMI
3. Risk stratification tool for admitted patients only (Observation/Admit).
If the patient's condition changes, patient will be reassigned to the appropriate clinical pathway.
CLINICAL PATHWAYS NEVER REPLACE CLINICAL JUDGMENT. CARE OUTLINED IN THE PATHWAY MUST BE ALTERED IF IT IS NOT CLINICALLY APPROPRIATE FOR THE INDIVIDUAL PATIENT. TIMING OF THE
REFRERRAL TOO CARDIOLOGY/MEDICAL MAY VARY FOR LOCAL CIRCUMSTANCES.