neuroimmunology - ecourse2.ccu.edu.tw
TRANSCRIPT

CHAPTER
13
Neuroimmunology
Michael R. Swenson
The immune system is that collection of tissues and organs devoted to the defenseof self, an action usually directed against infectious pathogens: parasites, fungi,viruses, and bacteria. Antigens are the distinguishing characteristics of pathogens,
usually foreign molecules, used by the immune system as a target for identifi cation of an invader and for direction of attack. The immune system can be functionally dividedinto two subsystems: innate immunity and adaptive immunity. The innate immune sys-tem is nondiscriminating, reacting to antigen at fi rst encounter and mounting a fi rstline of defense. Skin, membranes, mucus, cilia, and soluble factors such as complementare components of the innate system. The phagocytes are its cellular elements. Theyscavenge for invaders and act as antigen-presenting cells. The adaptive immune systemis the standing army of immunity. Its forces divide into lymphocytes, which engage in the operations of command and control, and the antibodies, which perform the basicwork of the immune system. The lymphocytes identify distinguishing components of the antigen, develop a response specifi c to the pathogen, mobilize and direct forces, and remember and anticipate recurrent antigenic challenges. T lymphocytes occur in two major types: CD8 cells and CD4 cells. CD8 lymphocytes recognize antigenic frag-ments (epitopes) complexed with major histocompatibility complex (MHC) class I andexpressed from within other cells. Virally infected cells express MHC class I, calling in the CD8 lymphocyte for killing the infected cell. CD4 cells become actively involvedin activation and control of the immune response, reacting to MHC class II–epitopecomplexes expressed on the surfaces of antigen-presenting scavenger cells. The anti-gen-presenting cell serves a reconnaissance function, capturing invaders and bringing in antigen fragments for recognition and initiation of action by the CD4 lymphocytes.Activated CD4 cells release cytokines to stimulate B cells; activated B cells proliferate and differentiate to become plasma cells; plasma cells manufacture and secrete antibod-ies, which are the soluble form of the B-cell receptor. Antibodies in the immune systemtake the form of immunoglobulin molecules. Antibodies recognize intact antigen. Theycan bind and directly neutralize antigen, or they can opsonize antigen for phagocytosis. Antibodies also may act by sensitizing target cells to initiate the infl ammatory response or by activating complement to mediate cell lysis.
© Springer Science+Business Media LLC 2009R. N. Rosenberg (ed.), Atlas of Clinical Neurology
Current Medicine Group LLC, part of

518 Atlas of Clinical Neurology
Innate immune system Adaptive immune system
Mucous membranes,bronchi, gut
Tonsils, adenoids
Thymus
Spleen
Peyer's patcheson small intestine
Bone marrow
Lymph nodes andlymphatic vessels
Skin
Phagocytic cells,lungs, liver, spleen Figure 13-1. Gross anatomy of the immune system. Immune
reactions to infection must occur at widely scattered sites, sothe lymph nodes, spleen, adenoids, tonsils, and other lymphoid tissues of the immune system are diffusely arranged. T cellsoriginate in the thymus and B cells in the bone marrow. Oncematured, T cells and B cells migrate to lymph organs, where they process antigen, reacting to nonself components. The thymus, a bilobed lymphoid organ in the anterior mediasti-num, is the proving ground for maturing T cells. Self-toleranceis learned by maturing T cells in the thymus. T cells, B cells, and immunoglobulins are the reactive components for adap-tive immunity. They are capable of specifi c antigen recognitionfollowed by activation and proliferation of the componentsneeded to mount an attack on invaders. The adaptive immunesystem also has memory, reacting more quickly and more force-fully with repeated antigenic challenge. The innate immune system, acting nonselectively and without memory, is composedof skin, mucous membranes, and phagocytic cells. These com-ponents react to any antigen. Phagocytes, however, participate in adaptive immunity by presenting antigen to lymphocytes.
Direct neutralization
Opsonization
Fc receptor
Cell lysisMAC
Complementfixation activationof membrane attackcomplex G
Phagocyte Figure 13-2. Mechanisms of antibody function. Antibodies, through their Fab regions, bind to antigen, either free in solu-tion or on cell surfaces. Antibody can directly neutralize anti-gen, but more commonly it acts by cross-linking antigen to host cells of the immune system that have surface receptors for theFc portion. Some antigen–antibody complexes activate the classic complement cascade, resulting in, among other actions, the formation of membrane attack complex (MAC) that destroys cell membrane and lyses cells.
ANATOMY AND FUNCTION OF THE IMMUNE SYSTEM

Neuroimmunology 519
Antigen
Peptide–T-cell epitope
B7-CD28
T
T
T
B
Plasma cell productionof antibody molecules
TCRMHC
Activated T cellsLymphokinestimulation ofB cells
B-cell proliferationand transformationto plasma cells
PPPPPPPPPP
PP
T
AAPC
APAPC
Figure 13-3. Lymphocyte activation and antibody production. Antigen-pre-senting cells (APCs) are found in manyorgans, including lymph nodes, thymus,spleen, liver, lung, and gut. APCs performreconnaissance activity, scavenging for antigens. Antigen is phagocytosed and broken into short (10- to 20-amino acid)peptide fragments. These peptides are used by the immune system as the dis-tinguishing and identifying characteristicof the antigen, called the T-cell epitope, for T-cell signaling. The peptides are complexed with major histocompatibility complex (MHC) class II and expressed on the APC surface. The APC seeks out and docks on a helper T cell bearing a com-patible receptor, the T-cell receptor (TCR).The “handshake” between APC and T cell–MHC–peptide–TCR is called the trimolecular complex (TMC). The TMCstimulates the T cell when appropriateco-stimulatory signals are present (eg, B7-CD28). The stimulated T cells proliferate and secrete cytokines called interleukins(eg, IL-2, IL-4). These cytokines activate othergglymphocytes, including B lymphocytes, forantibody production.
–
–
B7-CD28
ThTh
TTh
TCRMHC
APC
Blood–brainbarrier
NoNoNo
NoNo
YYes
Yes
TsB
1
Anti-idiotypicantibody
Self-tolerantT cell
5
32
4
ThThymymusus
Recognizeself?
React toself?
Clonal deletion
Figure 13-4. Mechanisms of self-tolerance. In dedication to the defense of self, the immune system has been required to defi ne“self,” a defi nition that occurs at the cellular and molecular levels. Tolerance relies on the talent of self-recognition that B cells and T cells probably acquire during maturation. Lymphocytesunable to recognize self or lacking the willingness to tolerateself are deleted or rendered anergic by mechanisms still not fullyunderstood. These mechanisms are sequestration, lack of anti-gen presentation, clonal energy, clonal deletion, and suppressorcells. In sequestration (1) some tissue proteins (eg, myelin basic ggprotein, lens of the eye) are anatomically isolated from exposureto lymphocytes; anatomic barriers (eg, the blood–brain barrier)ggpreclude contact with helper T cells. The development of T-cell tolerance is also blocked, so a later breakdown of sequestra-tion can lead to lymphocyte activation and the development of autoimmune disease. In lack of antigen presentation (2), sometissues contain cells lacking the capability of antigen-presentingcells (APCs)—cells unable to express major histocompatibility complex (MHC). Neurons, for example, cannot express MHC. Inclonal anergy (3), T-cell activation requires a secondary co-stimu-latory signal received by the CD28 complex. If a T cell confronts an antigen on a cell that lacks a functional B7 protein, the T cell becomes inactivated or tolerant. In clonal deletion (4), duringmaturation, T cells must demonstrate recognition of self and tolerance of self. This takes place in the thymus (Th). T-cell linesfailing to pass these tests are deleted or inactivated. Suppressor cells (5) (Ts) and other cells have been proposed to induce self-tolerance. For development of tolerance, Ts cells may be activatedby binding to anti-idiotypic antibodies. TCR—T-cell receptor.

520 Atlas of Clinical Neurology
Non–organ-specific diseases
Organ-specific diseases
Thyroid Hashimoto's thyroiditis Primary myxedema Thyrotoxicosis
Stomach Pernicious anemia
DermatomyositisSkinMuscle (? vasculitis)
Systemic lupuserythematosus
SkinKidneyJoints
Adrenal Addison's disease
Pancreas Insulin-dependent diabetes mellitus
Figure 13-5. Types of autoimmunity. Autoimmunity occurswhen the protective mechanisms of self-tolerance fail or arebypassed; pathologic reactions against self-antigens may result. Anti-self antibodies and self-reacting cells disrupt tissues andcause organ damage, or autoimmune disease. The spectrumof autoimmune disease spans two major categories. In organ-specific disorders, typified by thyroiditis and myasthenia gravis, attack is directed against a single antigen in a single organ or tissue. Non–organ-specific diseases target widespread self-anti-gens such as nucleic acids in systemic lupus erythematosus.Organ damage is widely disseminated owing to the ubiquitousdistribution of the antigen, and immune complex depositionmay cause remote systemic injury. The organ-specific diseasesoccur together with greater than expected likelihood. Forexample, 5% to 10% of patients with myasthenia gravis also haveantibody-mediated thyroid disease [1]. Disease clustering alsooccurs at the other end of the spectrum, with frequent overlapbetween, for example, dermatomyositis and other rheumato-logic syndromes [2].
T-T-cecellllepititype
TT celllTT TTTT
TT lllTT ceellTT llTT ll BB cellll
PlPlasssmmmaaaamccececeelllllll
AAPCC
MMMMHHHHCCCC TCTCCRR
Molecular mimicryand cross-antigenicity
Activationof T cells
Proliferationof B cells
Antibodies
Self
Microbe
Figure 13-6. Mechanisms of autoimmunity. The causes of a breakdown of self-tolerance are not fully understood, but proposed mechanisms include the following: 1) In molecularmimicry, cell surface antigens of some microbial pathogensresemble self-proteins. Presumably, the forces of evolution have selected those pathogens that are cloaked in such a camou-flage. When the immune system recognizes these pathogens, self-proteins are attacked by “friendly fire” (a case of mistaken identity). The connection between “strep throat” and rheumatic heart diseases is one of the simplest examples of such cross-antigenicity. 2) Activation of tolerant T cells may be due to abypass of the normal controls of autoreactivity. Self-antigens may, for example, lose their tolerated status when bound todrugs (eg, procainamide). 3) Cells of self-tissue may be inducedto express major histocompatibility complex (MHC) when stimulated with -interferon. 4) Excessive cytokine release dur-ing infections or inflammations may awaken self-tolerant T cells,a theory in line with flare-ups of autoimmune disease observedafter viral infections [3]. APC—antigen-presenting cell;TCR—T-cell receptor.

Neuroimmunology 521
Migratingactivated
CD4+ T cell
Antigen-presentingcell
Braininterstitium
Blood
Oligodendrocyte
Myelin
MULTIPLE SCLEROSIS
Figure 13-7. Pathogenesis of multiple sclerosis (MS). A poten-tially disabling infl ammatory central nervous system disease, MS affects about 250,000 Americans, mostly young adults, often during the most productive years of life. A strong regional variation of prevalence, demonstrating a steep gradient fromsouth to north, suggests an environmental exposure, perhaps achildhood virus with re-exposure to a secondary factor dur-ing adulthood, that triggers a complex autoimmune response.Infl ammatory lesions aggregate around venules, mostly inwhite-matter regions, suggesting that the blood–brain barrier (BBB) is breached and that serum antimyelin factors gain access to antigenic targets on myelin sheaths. Disruption of motor andsensory transmission in heavily myelinated pathways of thebrain, brainstem, cerebellum, and spinal cord causes a diverse spectrum of neurologic symptoms and disabilities. The widelyscattered regions of injury, combined with an unpredictable relapsing and remitting time course, make accurate diagnosis a challenge, especially in the early years of the disease.
Presumably, activated helper T cells (CD4+) induced by somesystemic factor breach the BBB into the central nervous system and demonstrate specifi city for peptide subunits of myelin.Secretion of -interferon leads to release of tumor necrosis fac-tor and other cytokines that damage myelin and contribute to myelin phagocytosis. Gadolinium-enhanced MRI scanning ofbrain, cerebellum, brainstem, and spinal cord allows detection of MS lesions with remarkable sensitivity. The diagnosis of MS,once reliant on a demonstration of a typical clinical pattern ofattacks (disseminated in time and space), is made much easier by these techniques.
Revolutionary discoveries in the treatment of MS are justbreaking. The two available -interferons and copolymer 1 haveeach been shown to reduce annual attack rates by about 30%. Corticosteroids, methotrexate, cyclophosphamide, and other general immunosuppressant methods are still under study, withsome encouraging results. Antigen-specifi c therapies, or “sil-ver bullet” methods, rely on recognition of antigenic peptides(epitopes) or their specifi c lymphocyte receptors. Once theseare identifi ed, methods are envisioned that would interfere with cellular signaling and enable an intervention that would inhibit the immune response to the specifi c target antigens in MS. Because these antigens are still unknown, these methodsremain investigational but are the source of much hope.
Autoreactive T cells in the circulation, presumably stimulatedby an environmental challenge, breach the BBB and migrate into the central nervous system, accompanied by other recruitedlymphocytes. Transmigration across the BBB begins by adhesionto the vascular endothelium in a region of infl ammation. Adhe-sion molecules, such as 4 integrins or very late antigen-4, areexpressed on the activated T cell. Likewise, counterreceptors, such as vascular cell adhesion molecules (VCAM), are present on the endothelial cells of the vessel wall, presumably expressed in regions of disease activity. These provide docking sites where the
T-cell adhesion molecules bind, bringing the activated T cells to a stop. In addition, endothelial components, such as degradative enzymes, matrix metalloproteinases, and chemokines allow theinfl ux of T cells into the central nervous system.
Natalizumab (Tysabri, Biogen Idec, Cambridge, MA and Elan Corp., Dublin, Ireland) was fi rst approved for treatment of MS in 2004 and was withdrawn after two case of progressive multi-focal leukoencephalopathy resulted in patient deaths. Reintro-duced in 2006, the drug now carries enhanced safety warnings and must be given in accordance with a risk management plan(TOUCH Prescribing Program). The clinical effect of natalizumabin MS may be mediated by blockade of the molecular bind-ing between 4 1-integrin on T cells with VCAM-1 on vascular endothelium. Disruption of this docking mechanism preventstransmigration of leukocytes across endothelium into regions of infl ammation. Data from an animal model of MS show reduced leukocyte migration into the brain and reduced plaque formationafter treatment with natalizumab.
Macrophages and microglial cells are activated directly andby cytokine release. Self-reactivity against some lamellar com-ponent may result in myelin attack and destruction.
The regulatory effects of cytokines play a signifi cant role inthe development of experimental allergic encephalitis and, pre-sumably, MS. Putative cytokines involved in the process include -interleukins, interferon, and tumor necrosis factor. Subsets of
these substances engage in a complex interplay of cell signalingthat leads to directed attack and myelin damage [4].

522 Atlas of Clinical Neurology
Figure 13-8. MRI showing optic neuritisin a patient with multiple sclerosis (MS).Optic neuritis, internuclear ophthalmo-plegia, and various patterns of nystagmusare the most common ophthalmologic declarations of MS. Optic neuritis causesrelatively acute impairment of vision,progressing over hours to days, reaching a nadir in about 1 week. During the acute phase, orbital pain, brow pain, and painwith eye movement occur. Depression of vision affects the whole fi eld of one eye,sometimes both [5]. The disc is sparedwith retrobulbar neuritis: “The patient sees nothing—neither does the doctor.” Optic neuritis is the presenting featurein 25% of MS cases and occurs at somestage of the illness in 73%. Conversely,50% to 75% of patients with isolated opticneuritis later develop defi nite MS within 12 to 15 years [6]. Bilateral optic neuri-tis, occurring acutely in the company of transverse myelitis, is termed neuromy-elitis optica or Devic’s disease. This formof MS attack occurs most often in youngpeople and carries a poorer prognosis [7].
A 00 100100 200200
10 VN 75 N 145
P 100
Stimulation
Figure 13-9. Central scotoma and pattern-reversal visual evoked potentials in optic neu-ritis. A and B, Optic neuritis typically causes a central or centrocecal scotoma, usually involving the central 20°. Diminished acuity, color desaturation, and reduced contrast sensitivity are detectable. Pattern-reversal visual evoked potentials show delayed latency and reduced amplitude with stimulation of the affected eye. Abnormal visual evoked potentials are nonspecifi c but are useful in detecting asymptomatic lesions of the optic nerve. Abnormal visual evoked potentials may be detected in up to 20% of patients withdefi nite multiple sclerosis who do not provide a history of optic neuritis.
50 100 150
50 100 150
Eye patch
Visual evoked potential in eye with optic neuritis
Eye patch
Visual evoked potential in normal eye
Central scotoma due to left optic neuritis
10 V
10 V
N 75
P 100
0
B

Neuroimmunology 523
Cerebrospinal Fluid Abnormalitiesin Multiple Sclerosis
Quantitation of IgG synthesis rate
IgG index (IgG CSF/IgG serum) / (alb CSF/alb serum)
CSF electrophoresis demonstrating oligoclonal bands
Myelin basic protein
Leukocyte count
Figure 13-10. Cerebrospinal fl uid (CSF) abnormalities in the diagnosis of multiple sclerosis (MS). Clinical criteria for the diagnosis of MS typically include objective neurologic signs of central nervous system dysfunction at two distinct sites on two ormore occasions in a patient between the ages of 10 and 50 years. The diagnosis should be made in the absence of other neuro-logic disease. MRI has greatly enhanced the diagnostic yield and is required in most suspected cases. Spinal fl uid testing is still a useful adjunctive test and is an important supporting labora-tory test in the criteria proposed by Poser et al. [8]. About 70% ofpatients with clinically confi rmed MS have an elevated intrathe-cal rate of immunoglobulin synthesis. This can be determined directly, or it can be expressed as an index that allows compensa-tion for the serum levels and ratios of IgG to albumin (alb). IgGindices of greater than 0.7 are abnormal, and ratios greater than 1.7 indicate a high probability of MS [9]. Agarose gel electropho-resis of CSF demonstrates migration of -globulins in discretepopulations—the so-called oligoclonal bands. Oligoclonal bandpatterns appear early in patients with MS and tend to remain constant over the course of the disease. They are not abolishedby treatment. Other infl ammatory diseases, including subacutesclerosing panencephalitis, aseptic meningitis, Guillain-Barré syn-drome, and other encephalitides, may also generate bands. The
Figure 13-11. Periventricular plaques. Theutility of MRI is seen most dramatically in images of the brain of patients with mul-tiple sclerosis (MS). The periventricular white matter is typically involved, dem-onstrating multiple lesions with charac-teristically prominent T1 prolongation (A)and high T2-weighted signal density (B). Elliptical lesions deep in the white matter directed toward the ventricular marginappear in the corona radiata and tendto point toward the ventricular margin,a morphology known as Dawson’s fi n-ger [11]. Subependymal lesions may benodular or confl uent. Subcortical–cortical junction lesions and callosal lesions dis-tinguish MS from vascular diseases. BrainMRI fi ndings are abnormal in more than 95% of patients with MS [12]. BA
A B
Figure 13-12. MRI scans showing multiple sclerosis (MS) of the optic nerve, brain-stem, and spinal cord. A and B, Accurate visualization of the intraorbital portion ofthe optic nerve (arrows) can demonstrate unilateral optic neuritis. Fat-saturationsequences enhance the signal contrast between optic nerve and orbital fat.
Continued on the next page
presence of oligoclonal bands in patients with early or isolatedattacks suggests a higher risk of subsequent progression [10]. High-resolution techniques and isoelectric focusing techniquesadd sensitivity to the determination of oligoclonal bands. Immu-nofi xation techniques, though not widely available, can be usedto make the test very specifi c. High levels of myelin basic protein are seen in the spinal fl uid during acute attacks; levels tend to belower in progressive disease and revert to normal during remis-sions. The test is not widely available. Leukocytes are often foundduring acute attacks, refl ecting the infl ammatory nature of MS.Cell counts are usually less than 50/mm3, but in rapidly progres-sive cases or more severe attacks, the count can exceed 100. Lymphocytes are predominant, usually T cells.

524 Atlas of Clinical Neurology
Figure 13-12. (Continued) C, Focal brainstem and cerebellarpeduncular foci, especially the middle cerebellar peduncle (bra-chium pontis), are common sites of involvement in MS. These lesions are usually symptomatic in the acute phase, often cor-relating with internuclear ophthalmoplegia or other brainstem signs. Comi et al. [13] found brainstem lesions by MRI scanning of 50 patients with clinical signs of brainstem involvement. Seventy-four percent of these lesions correlated with clinical findings. Dand E, Transverse myelitis may involve thoracic or cervical seg-ments and may overlap in appearance with spinal astrocytoma,even with contrast-enhanced techniques. McDonald and Miller[14] identified 139 lesions in 74% of 59 patients, more commonlyin the cervical segments. Spinal cord atrophy, found in 40%, cor-related more with clinical disability than did discrete cord lesions. Curiously, the burden of plaque detectable by MRI typically goes far beyond the clinical signs and symptoms. The burden of
disease increases about 10% per year [15,16], and a high rate ofMRI activity correlates with poor prognosis [17]. Although theMRI findings should not stand alone to establish a diagnosis ofMS, cases of a single clinical attack may be considered as clini-cally probable MS if new lesions can be shown to develop on serial scans. Fazekas’ criteria specify the finding of a periventricu-lar lesion, an infratentorial lesion, and a lesion 6 mm or greater in diameter. These criteria are 89% specific for the diagnosisof MS [18]. Filippi et al. [19] studied 100 patients with MS who had undergone neuropsychologic testing to evaluate cognitive impairment. Atrophy of the corpus callosum and dilation of theventricles correlated significantly with lower mean scores on neu-ropsychologic testing. Widening of the cortical sulci and higherlesion scores correlated inversely with performance intelligencequotient (IQ) and total IQ, suggesting that MRI pathology corre-lates with cognitive dysfunction in patients with MS.
C D E

Neuroimmunology 525
Current Therapies for Multiple SclerosisFDA-approved Therapies Non–FDA-approved Therapies
Interferon -1b (Betaseron, Bayer Healthcare Pharmaceuticals, Richmond, CA)
Corticosteroids
May lengthen the intervals between attacks [23]
Approved for relapsing or remitting MS Commonly used for treatment of acute attacks, but proof of effect still lackingResults in a 30% reduction in attack rate [20]
Results in an 80% reduction in plaque burden seen on MRI scans Numerous side effects with long-term use
Minimal side effects [21] Cyclophosphamide
Injection site irritation Monthly pulse therapy
Flu-like symptoms Useful in younger patients [24]
Long-term benefits unclear Canadian Cooperative Study Group [25] found disappointing results
Every-other-day dosing Methotrexate
Interferon -1a (Avonex, Biogen Idec, Cambridge, MA) Demonstrated effect in patients with chronic-progressive MS [26]
Effective in relapsing or remitting MS Natalizumab (Tysabri, Biogen Idec, Cambridge, MA, and Elan Corp., Dublin, Ireland)About a 30% reduction in attack rate [22]
Slower progression of disability Monoclonal antibody against adhesion molecules
Minimal side effects Slight risk of PML
Flu-like symptoms Approved in 2004; withdrawn 2005 due to PML
Weekly dosing Reintroduced in 2006 with box warning
Glatiramer (previously copolymer-1, Copaxone, Teva Pharmaceuticals, Petach Tikva, Israel)
Monthly infusions through TOUCH program
~68% reduction in relapse rate [32]
Results in a 29% reduction in annual relapse rate ~40% reduction in disability progression
Improvement of disability scores Anaphylaxis in < 1%
Daily injections but few side effects and minimal site reaction Increased risk of infections
Mitoxantrone (Novantrone, EMD Sorono, Rockland, MA, and OSI Phamaceuticals, Melville, NY; Immunex, Amgen, Thousand Oaks, CA)
UTI, pneumonia, herpes, gastroenteritis
IV immunoglobulin
Results in a > 60% reduction in annual relapse rate Reduced exacerbation rate
EDSS reduced by half Slow disease progression
Reduced rate of new MRI lesions Very small clinical trials [33]
IV infusion every 3 mo Plasmapheresis
Cumulative cardiotoxicity limits the duration of treatment Minimal clinical trial evidence
Dramatic improvement reported but remains unsubstantiated [34]
Other therapies
2-Chlorodeoxyadenosine (Leustatin, Ortho Biotech, Raritan, NJ) B-cell tolerogens
Induces lymphocyte apoptosis Monoclonal antibodies
Clinical and MRI scan improvement in chronic-progressive MS [27] Natalizumab
Isoprinosine [28] Symptomatic treatment
Total lymphoid irradiation [29–31] Antispasticity therapy
Antigen-specific therapies 4-AP; 3,4-DAP
T-cell tolerogens Rehabilitative techniques
Figure 13-13. Current therapies for multiple sclerosis (MS). Theapprovals of -interferons [35], glatiramer [36], and mitoxan-trone [37] for clinical use signaled the beginning of a new era intherapy for MS. The challenge is in deciding which treatments,single drugs, or combinations are the most efficacious. 4-AP—4-
aminopyridine; 3,4-DAP—3,4-diaminopyridine; EDSS—ExpandedDisability Status Score; FDA—Food and Drug Administration;IV—intravenous; PML—progressive multifocal leukoencepha-lopathy; UTI—urinary tract infection.

526 Atlas of Clinical Neurology
ANTIBODY-ASSOCIATED CENTRAL NERVOUS SYSTEM DISORDERS
Central Nervous System Paraneoplastic SyndromesSyndrome Putative antigen Associated antibody
Paraneoplastic cerebellar degeneration Ovarian or breast cancer Anti-Yo, type 1, PCA-1, APCA
Paraneoplastic encephalomyelitis or limbic encephalitis Small cell lung cancer Anti-Hu, type IIa, ANNA-1
Paraneoplastic sensory ganglioneuritis Small cell lung cancer Anti-Hu
Opsoclonus Neuroblastoma, retinoblastoma, or breast cancer Anti-Ri, type IIb, ANNA-2
Paraneoplastic retinal degeneration Small cell lung cancer Antiretinal antibody
Figure 13-14. Central nervous system (CNS) paraneoplastic syndromes. Cerebellar degeneration is the most familiar para-neoplastic syndrome. This syndrome manifests with pancerebel-lar dysfunction, including oculomotor nystagmus, dysarthria,and wide-based ataxic gait. Anti-Yo antibody is directed against Purkinje cells. Less commonly, anti-Hu antibody or an atypicalantibody is found. Seventy-seven percent of patients with parane-oplastic encephalomyelitis or limbic encephalitis have an under-lying small cell lung cancer [38]. Symptoms reflect the regionof involvement: lower-extremity weakness with myelitis, bulbar palsy with brainstem encephalitis, and memory loss and cogni-tive impairment with limbic encephalitis. Paraneoplastic sensoryganglioneuritis is a frequent accompaniment. The correlation is high with anti-Hu antibody. Anti-Hu cross-reacts with neuronal protein components in the CNS and the dorsal root ganglia. Aswith other paraneoplastic syndromes, symptoms may precede
detection of tumor by many months. The opsoclonus syndromesare rare paraneoplastic disorders characterized by rapid arrhyth-mic conjugate square wave gaze jerks, often accompanied bymyoclonic jerks of appendicular musculature. Ataxia, dysarthria, myoclonus, vertigo, and encephalopathy are other signs associ-ated with this relapsing and remitting syndrome, usually related to the antineuronal antibody of type II (anti-Ri or type IIb). Ras-mussen’s encephalitis, Bickerstaff’s encephalitis, and “stiff-man”syndrome are other inflammatory CNS disorders with reported antibody association. Paraneoplastic retinal degeneration causes painless visual loss, most commonly in association with small celllung cancer [39]. Autoreactive antigens against retinal cell compo-nents have been found, most frequently identified with photo-receptor cells. Immunosuppressive agents may be helpful [40]. ANNA—antineuronal nuclear antibody; APCA—anti-Purkinje cellantibody; PCA—Purkinje cell antibody.
PARANEOPLASTIC SYNDROMES

Neuroimmunology 527
*Alternatively, some clinicians choose to request Western blot analysis first.
Noo sYYes
No
NNo
No YeYesYeYes
YeYes NoNYes
NoNo YeYess
Noo
YeYessYes
Known systemic cancer?
Signs suggest paraneoplastic syndrome?
Typical paraneoplastic syndrome?
Antineoplastic therapyRe-evaluate
Intensive follow-upRepeat malignancy work-up
Supportive care, PT, ST, OT, symptom treatment
Consider immunosuppression1. Plasma exchange2. Steroids
Is paraneoplastic syndrome progressing?
Cancer detected? Cancer detected?
Work-up for rest of differential diagnosis
Re-evaluate
Western blot to confirm pattern*
Signs explained by cancer?
Treat appropriatelyRe-evaluate
Subacute neurologic deficitsParaneoplastic disorder considered
Rule out metastases and otherdirect effects of cancer,
includes MRI, CSF cytology
Initial cancer screening,includes screening labs,
neuroimaging CSF analysis
Immunohistologic screening for antineuronal antibodiesIdentify pattern
PCD Hodgkin’sSCLC
OMS SCLCNeuroblastoma
Syndrome: Suspect
Atypicalpattern
Anti-Ri
Cancereg: lung
BreastcancerSCLC
Anti-Hu
SCLC
anti-Yo
Ovarian, othergynecologiccancer, breast cancer
Pattern: Suspect
–
– +
+
Figure 13-15. Algorithm for the evaluation of central nervous system (CNS) paraneo-plastic syndromes. Detection of antibod-ies associated with disorders of the CNShas led to the discovery that these diseas-es are often acquired through association with tumors and viruses. Some antibodytests are now used as diagnostic markersin the clinic. The mediation of these dis-eases by antibody suggests opportunities for treatment by a variety of immunosup-pressant methods.
The paraneoplastic syndromes occurrarely in patients with known cancer but may be the heralding symptom and may be the most disabling and potentially treatable aspect of the disorder (abouthalf of patients develop neurologicsymptoms preceding the diagnosis of systemic cancer).
Paraneoplastic syndromes often occurwhen the causative cancer is relativelysmall, opening greater opportunity foreffective treatment. The paraneoplasticsyndromes are also important to considerbecause they frequently cause symptoms that are mistaken for metastatic disease or for the adverse effects of chemothera-py or malnutrition.
The theory that these disorders are autoimmune in pathogenesis implies that tumor antigens or viral antigens cross-react with antigenically similar molecular components of neurons or other CNSstructures. The role of antineuronalantibodies (Hu, Ri, Yo) is still debated.Antibody titer may be high in the pres-ence of minimal disease and present inthe absence of disease [41], and para-neoplastic syndromes may occur withoutmeasurable antibody titer. Stated moresimply, antibody testing is neither specifi cnor sensitive for the presence of paraneo-plastic disease. The evidence for cross-antigenicity between tumor (or virus) intarget neurons is still compelling, bothclinically and in the laboratory. Treatmentof paraneoplastic CNS disorders relieson an aggressive search for underlying malignancy to interrupt tumor progres-sion early. Tumor removal may also cureor ease the treatment of paraneoplasticsyndromes. Because antibody-mediatedattack against tumor may be part of anantineoplastic defense, immunosuppres-sant therapy before tumor removal might
accelerate tumor growth and disinhibit metastasis formation. Many of these syn-dromes occur even in the absence of tumor or may continue after tumor removal, soimmunosuppressant techniques or plasma exchange may be warranted [42]. Brashear[43] recommends concurrent plasmapheresis with high-dose steroids after clinical response and antibody titer determination. CSF—cerebrospinal fl uid; OMS—opsoclo-nus myoclonus syndrome; OT—occupational therapy; PCD—paraneoplastic cerebellar degeneration; PT—physical therapy; SCLC—small cell lung cancer; ST—speech thera-py. (Adapted from Brashear [43].)

528 Atlas of Clinical Neurology
VIRAL SYNDROMES
Antibody-Associated Central Nervous System Viral SyndromesSyndrome Putative antigen Associated antibody
Stiff-man syndrome (Moersch-Woltman syndrome) Unknown Anti-GAD
Rasmussen’s encephalitis Possibly cytomegalovirus or herpes simplex virus Possibly GluR3
Bickerstaff’s encephalitis Possibly cytomegalovirus Possibly anti-GQ1b
Possibly ALS Unknown Possibly anti-VGCC
Figure 13-16. Antibody-associated central nervous system viral syn-dromes. “Stiff-man” syndrome (SMS) is a rare disorder characterizedby rigidity and continuous electromyographic motor activity affect-ing axial musculature. Paroxysmal autonomic dysfunction has been reported to cause sudden death. The painful axial stiffening is oftentriggered by startling noises, touch, emotion, or attempted voluntarymovements. The frequent association with insulin-dependent diabe-tes and autoimmune thyroid disorders, identifi cation of associated antibodies to glutamic acid decarboxylase (anti-GAD), and reports ofsuccessful reversal with immunosuppressant methods all suggest an immune-mediated cause of SMS [44,45].
Reportedly, SMS is caused by an antibody-mediated attackagainst inhibitory glutamatergic inhibitory interneurons. Rare cases have been associated with breast cancer [46]. Treatmentof idiopathic cases has been successful with plasmapheresis, corticosteroids, and intravenous immunoglobulin.
A chronic infl ammatory encephalopathy, often unilateral and associated with hemiparesis and intractable focal epilepsy, is known as Rasmussen’s encephalitis [47]. Children and young teens are affected. Viral associations (herpes simplex virus types
1 and 2, cytomegalovirus) and detection of serum antibody to glutamate receptor 3 (GluR3) indicate an autoimmune cause[48]. Antiviral agents and immunosuppressants have been tried with some success. Bickerstaff’s encephalitis is a similar infl am-matory disease of the brainstem, also associated with cytomega-lovirus and with detectable amounts of anti-GQ1b antibody.
Sporadic amyotrophic lateral sclerosis (ALS) has been mim-icked in guinea pig models of autoimmune motor neurondisease. Clinical observations suggest an autoimmune-mediated cause of ALS based on the following evidence: 1) 3% to 5% of patients have other autoimmune disorders (eg, thyroid disease); 2) immunoglobulin monoclonal spikes occur with three to fi ve times the prevalence in ALS; 3) immune complex deposition can be seen at the neuromuscular junction and in kidneys; and 4) paraproteinemias are more common. Smith et al. [47] have shown increased intracellular Ca2+ concentrations and postulateimmune-mediated disruption of voltage-gated calcium-channel (VGCC) function, perhaps leading to apoptotic motor neuroncell death. Attempts to treat ALS with immunosuppressantmedication, however, have been futile.
Infl ammatory Demyelinating Nerve DiseaseSyndrome Putative antigen Associated antibody
Acute infl ammatory demyelinating polyradiculoneuropathy (Guillain-Barré syndrome) Campylobacter jejuni viruses Possily anti-GM1
Chronic infl ammatory demyelinating polyradiculoneuropathy Unknown Possibly cell mediated
Neuropathies in diabetes mellitus Unknown Unknown
Vasculitic neuropathies Unknown Unknown
Figure 13-17. Infl ammatory demyelinating nerve disease. Theinfl ammatory demyelinating polyradiculopathies occur in acute,chronic, and chronic relapsing forms (AIDP, CIDP, CRIP, respec-tively). AIDP leads to arrefl exic weakness. Respiratory failure occurs in 20% of cases and leaves 15% of patients with signifi -cant neurologic residual impairments. Because conventional immunosuppressant methods (eg, corticosteroids) have failedto show benefi t, positive therapeutic trials of plasmapheresis and intravenous immunoglobulin (IVIg) have been greetedeagerly. The large studies of plasmapheresis for AIDP, reported in the early 1980s, showed an impact on respirator time andtime to independent ambulation, cutting each about in half when treatment was given during the fi rst weeks of the disease. IVIg has also been proved benefi cial.
CIDP is a different syndrome, evolving insidiously over weeks or months and progressing slowly. Weakness is usually symmet-ric, involving proximal and distal muscles. Refl exes are lost ordepressed. Respiratory failure is rare. Nerve conduction studies show reduced velocities and scattered regions of conductionblock [49]. A wide array of treatment options are available for
CIDP, including corticosteroids, azathioprine, and cyclosporineA. Plasma exchange is also useful, but the benefi ts of therapyfade after 10 to 14 days, so maintenance with concomitant steroid therapy is required [50]. Long-term plasma exchangetherapy has obvious drawbacks in terms of expense, vascular access, and complications.
Dyck et al. [51] have shown that weekly IVIg is equal in effect to plasma exchange and may be the preferable therapy in termsof availability and lower rate of complications.
Krendel [52] reported successful treatment of neuropathiesin some diabetic patients using immunosuppressant methods(IVIg, prednisone, cyclophosphamide, pheresis, or azathio-prine) alone or in various combinations. Diabetic patients with CIDP-like illness were insulin dependent only, suggesting acommon underlying immunopathogenesis.
Vasculitic neuropathies manifest as mononeuritis multiplex orpolyneuropathy with equal likelihood, either as part of a systemicvasculitis or in isolation, without other organ involvement [53,54]. Circulating immune complex deposits, infl ammation, and cell-mediated mechanisms of injury to nerve have been postulated.
AUTOIMMUNE PERIPHERAL NERVOUS SYSTEM

Neuroimmunology 529
ACUTE INFLAMMATORY DEMYELINATING POLYNEUROPATHY
A
000 3030 6060 9090
Days since randomization120120 150150 180180
0.25
0.50
0.75
1.00
Pro
po
rtio
n n
ot
reac
hin
g e
nd
po
int
Plasma exchange
Immunoglobulin
Figure 13-18. Acute infl ammatory demyelinating polyneuropa-thy. Kaplan-Meier curves demonstrate a comparison of intra-venous immunoglobulin (IVIg) with plasma exchange in theDutch trial [55]. A total of 147 patients were randomly assigned to receive either (A) IVIg in fi ve daily doses of 0.4 g/kg/d or (B)plasma exchange of 200 to 250 mL/kg in fi ve sessions over 7 to 14days (albumin replacement). Thirty-four percent of the patientson plasma exchange improved one functional grade by 28 days, compared with 53% of those treated with IVIg. The median
time to improve one grade was 41 days with plasma exchange but only 27 days with IVIg therapy. Other measures included a shorter hospital stay by 14 days, shorter intubation time by 7days, greater safety, and fewer complications in the IVIg group. Relapse rates were higher with IVIg treatment. Nonetheless,the wide availability of IVIg and the ease of administration have made this technique a welcome therapeutic option, espe-cially in smaller hospitals and in outlying areas where plasmaexchange is unavailable. (Adapted from Parry [49].)
B
000 3030 6060 9090 120120 150150 180180
0.25
0.50
0.75
1.00
Pro
po
rtio
n n
ot
reac
hin
g e
nd
po
int
Plasma exchange
Immunoglobulin
Days since randomization

530 Atlas of Clinical Neurology
Inflammatory demyelinating neuropathy
Chronic
Corticosteroids
Patient requires further therapy?
Four or more infusions needed per year?
Initiate IVIgConsider lower dose for subsequent courses
Initiatesupportive
care
Initiate supportivecare
Continue prednisone (60 mg/d) for 2 mo
Continue with IVIgtherapy, monitor
Desirable response? Side-effect profile acceptable?
Favorable response?
Continue with cyclosporine
Taper dose and continue prednisone Initiate azathioprine or cyclosporine
NoNo YeYess
NNo YeYes
NoNo YeYess
YeYess
YYes
NoNo
YeYess NoNo
YYes NNo
YeYess NoNo
NoN
Consider:• Duration of illness: < or > 6 mo?• Severity of paralysis and rapidity of course• Age of patient
Acute (Guillain-Barré syndrome)
Patient a candidate for IVIg?
Substantial improvement instrength by day 8?
Begin IVIg*(2 g/kg)on days 1, 2, 3, 5, and 8
Continue withsupportive care
Continueplasmapheresis
If patientrelapses, consider
repeat IVIg
Evaluate degree of disability
Significant disability?
Multifocal motor neuropathy
Supportive careIVIg
Continueintermittent IVIg
Consider IV pulsedcyclophosphamide
Are 4 or more courses of IVIg/y required?
Consider three factors together:• Duration of symptoms: < or > 2 wk?• Severity of paralysis: Is patient ambulatory?• Rapidity of progression
*Plasmapheresis may be used as an alternative therapy if following the same logic tree.
Figure 13-19. Suggested clinical algorithm for treatment ofinfl ammatory demyelinating polyradiculoneuropathy [49]. This algorithm favors early use of intravenous immuno-
globulin (IVIg). In centers where plasma exchange is easilyavailable, either option could be exercised. (Adapted fromParry [49].)
INFLAMMATORY DEMYELINATING POLYRADICULONEUROPATHY

Neuroimmunology 531
Other Antibody-Mediated DisordersSyndrome Putative antigen Associated antibody
Multifocal motor neuropathy Unknown Anti-GM1
Anti-MAG–associated neuropathy Unknown Anti-MAG
Isaacs’ syndrome (acquired neuromyotonia) Unknown Nerve K+ channels
Figure 13-20. Other antibody-mediated disorders. Autoimmunity to gangliosides (glycoproteins and glycolipid compo-nents of cell membranes) may underlie two or more peripheral neuropathies. Inmultifocal motor neuropathy, a focal ormultifocal, predominantly distal motor impairment develops in a step-wise or gradually progressive fashion with mini-mal sensory expression. Nerve conduc-tion testing reveals localizable regionsof conduction block when involved sitesare accessible; conduction block may be too proximal or too distal to detect. High antibody titers to GM1 ganglioside are seen in about half of these patients. Recovery may be dramatic, even inchronic cases [56].
Sensorimotor neuropathy associatedwith a monoclonal paraprotein is recog-nized. Antibodies against myelin-associ-ated glycoprotein (MAG) are thought
GLYCOCONJUGATES
Extracellular
MAG
Glycosphingolipids
SGPG
–––––––
– –––––
Gal
Gal
GlcNAc
Glc
Gal
Gal
GlcNAc
Glc
NeuNAcSO3
GlcUA
GM1
Membrane bilayer
Cell cytoplasm
––––
– –––
Figure 13-21. Cell surface glycocon-jugates implicated as potential targetantigens in immune-mediated neu-ropathy. Glycolipids, glycoproteins, and proteoglycans contain complex oligo-saccharide moieties exposed on theoutside of cell membranes. These cell surface glycoconjugates are exposed tobecome foci of an immune attack and have been implicated as potential targetantigens in immune-mediated neuropa-thy. The myelin-associated glycoprotein(MAG) may be involved in myelin layeradhesion or in the interaction betweenSchwann cells and the axolemma.
Sulfate-3-glucuronyl paragloboside(SGPG) is a glycolipid that shares structur-al features with MAG and that is implicat-ed in neuronal function. SGPG may alsobe antigenic.
GM1 is presumably the antigenattacked in multifocal motor neuropathyas well as in some forms of Guillain-Barrésyndrome. Labeled anti-GM1 antibod-
OTHER ANTIBODY-MEDIATED DISORDERS
to account for a monoclonal spike and are considered the causative agent target-ing myelin and leading to demyelination of motor and sensory nerve fi bers. Plasma exchange, steroids, cyclophosphamide, and intravenous immunoglobulin have beentried with varying success. Parry and Swenson [57] favor plasmapheresis followed by cyclophosphamide and chlorambucil.
Acquired myotonia, known as Isaacs’ syndrome, is characterized by muscle activ-ity causing visible myokymia. This excessive muscle activity is of peripheral nerve origin. Electromyographically, bursts of multiple, single-unit discharges occur in highfrequency. Transfer of disease to mice by injection with affected patients’ immuno-globulin suggests an autoimmune cause. Antibodies to peripheral nerve potassium channels may be the pathophysiologic explanation. Treatment with plasma exchange has been of benefi t in a few patients [58,59]. Occurrence of Isaacs’ syndrome withchronic infl ammatory demyelinating polyradiculopathy with other neuropathies andin association with malignancies has been reported [60].
ies have been shown to bind preferentially to the nodes of Ranvier, perhaps blocking sodium-channel function. This would also explain the rapid reversibility of multifo-cal motor neuropathy with immunotherapeutic methods [61,62]. Gal—galactose;Glc—glucose; GlcNAc—N-acetylglucosamine; GlcUA—glucuronic acid; NeuNAc—N-acetylneuraminic acid (sialic acid). (Adapted from Quarles [62]; courtesy of Richard H.Quarles, PhD, National Institute of Neurological Disorders and Stroke.)

532 Atlas of Clinical Neurology
NEUROMUSCULAR JUNCTION
Neuromuscular JunctionSyndrome Putative antigen Associated antibody
Myasthenia gravis Possibly thymus Anti-AChR
Lambert-Eaton myasthenic syndrome Small cell lung cancer Anti-VGCC
Figure 13-22. Neuromuscular junction. Few neurologic studieshave yielded so clear a connection of pathophysiology with disease as have the disorders of the neuromuscular junction, especially myasthenia gravis and Lambert-Eaton myasthenic syndrome (LEMS). The acetylcholine receptor (AChR) is attacked by autoantibody, uncoupling the activation of muscle fibers from incoming nerve impulses. The results are painless fati-gability and weakness of skeletal musculature, the identifyingsymptoms of myasthenia gravis. Sensation, autonomic function, reflexes, and cognitive powers remain intact; myasthenia gravisspecifically affects only skeletal muscle [63].
Anti–AChR receptor antibodies are of IgG subtype, mostly binding to the main immunogenic region of the AChR -subunit,causing cross-linking of adjacent receptors, accelerated receptor turnover, and complement-mediated injury to the postsynapticjunction. Cross-antigenicity with thymic components, with or without thymoma, presumably plays a role in the disease devel-opment and explains the improvement seen in some patientsafter thymus removal. Diagnosis relies on antibody serology, repetitive nerve stimulation studies, and single-fiber electromy-ography. Careful and cautious management is mandated by theclinical instability and potential for rapid deterioration of respira-tory power in patients with generalized disease. Anticholinesterase
medication (eg, pyridostigmine) is the mainstay of therapy, withggadditional use of prednisone, azathioprine, cyclosporine, plasma exchange, and intravenous immunoglobulin, depending onseverity and degree of disability [64].
LEMS differs from myasthenia gravis in that patients usu-ally have more constant degrees of weakness, accompaniedby autonomic features such as dry mouth, impotence, andconstipation. Proximal muscle weakness may be reversed bybrief exercise. Antibodies to presynaptic voltage-gated calcium channels (VGCC), also of IgG subtype, impair calcium influxduring nerve terminal depolarization, inhibiting release of acetylcholine [65,66].
Most patients with LEMS have an underlying small cell lung cancer, but cases accompanying autoimmune disease are not uncommon. Diagnosis relies on recognition of the clinicalsyndrome and demonstration of marked enhancement of com-pound motor action potential amplitude (> 200%) after brief exercise. Treatment is directed at the underlying lung cancer orimmunosuppressant medication in nonneoplastic cases. Immu-nosuppression should be used cautiously if an underlying can-cer cannot be excluded because suppression of tumor growth by LEMS antibody could be reversed, creating a potential for rapid tumor growth. Pyridostigmine is useful in some cases [67].
MYASTHENIA GRAVIS
Clinical Groups in Myasthenia GravisEarly onset (55%) Thymoma (10%) Late onset (20%) Seronegativity (15%)
Weakness Generalized Generalized Generalized or ocular Ocular or generalized
Age at onset < 40 y Any > 40 y Any
Sex incidence M < F M = F M > F M > F
Antiacetylcholine receptors High Intermediate Low Absent
Thymus Hyperplasia Thymoma Normal Normal
HLA associations (whites) B8, DR3 B7, DR2
Figure 13-23. Clinical groups in myasthenia gravis. Patients with myasthenia gravis can be categorized into four groupsrelating to age at onset, presence of thymoma, and presence or absence of antibody. Myasthenia gravis has been calleda disease of young women and old men, but cases with thy-moma occur at any age without sex predilection. Seronegative
patients are more commonly mildly affected, but generalizedand severe weakness can occur in the absence of detectable antibodies. Passive transfer of disease to mice suggests that the antibody in these cases is simply not detectable by current methods [68,69]. HLA—human leukocyte antigen. (Adapted from Newsom-Davis [70].)

Neuroimmunology 533
A B
Acetylcholine
Acetylcholine receptors
Diminished number ofacetylcholine receptors
Junctional fold
Muscle cellmembrane
Disruptedjunctional folds
Acetylcholinesterase
Cholinereuptakereuptak
NeNervveeteteteerrmrminininalalal
CoaCoatedtedvesicleve ii
MitMitochochondddo iriorion
Figure 13-24. Neuromuscular junction in myasthenia gravis. A, The normal neuromuscular junction releases acetylcholine frompresynaptic vesicles that bind to acetylcholine receptors at theapices of postsynaptic junctional folds. Bound acetylcholinereceptors allow sodium infl ux, which causes depolarization of postsynaptic membranes. Acetylcholine is degraded by ace-tylcholinesterase, located deep within the postsynaptic crypts. B, Acetylcholine receptor antibodies bind to acetylcholinereceptors, causing accelerated endocytosis and degradation of
receptors, blockade of acetylcholine binding sites, and comple-ment-mediated damage to the postsynaptic membrane. The density of acetylcholine receptors is reduced, and the remain-ing receptors are blockaded by the presence of bound anti-body. Postsynaptic junctional folds are fl attened, damaged, and disorganized by this complement-mediated attack. The reduced population of receptor disallows suffi cient membrane depo-larization to originate a propagating muscle membrane action potential. (Adapted from Lindstrom [69].)
A2 ms
5 mV–
+
B2 ms
1 mV–
+
1 s
1 mV–
+
Figure 13-25. Neurophysiologic testing in myasthenia gravis(MG). A, Repetitive nerve conduction testing in a normal subjectdemonstrates a constant compound motor action potential(CMAP) amplitude with repetitive nerve stimulation at slow andrapid rates. B, In a patient with symptomatic myasthenia gravis,
the amplitude of the CMAP decrements at low rates of 2 to 5 Hz,showing greatest change between the fi rst and second responses.This decrement may correct with administration of intravenous edro-phonium (Tensilon; Hoffmann-LaRoche, Nutley, NJ), a short-actingacetylcholinesterase inhibitor.
Continued on the next page

534 Atlas of Clinical Neurology
C
Restedmuscle
Exercisetime
Time after exercise3 s
30 s
30 s
10 s
2 min 10 min
LEMS
MG
N 5 mV
10 ms
–
+
5 mV
10 ms
–
+
5 mV
7 ms
–
+
D
2 mV
0.5 ms
21 3
Neighboringmusclefibers
Motor axonterminalbranches
Single-fiberneedle
To EMGpreamplifier
Figure 13-25. (Continued) C, Comparison of repetitive nerve stimulation in normalsubjects (N), patients with MG, and patientswith Lambert-Eaton myasthenic syndrome(LEMS). The decrementing seen in symp-tomatic MG can be repaired by 30 secondsof exercise, but increasing decrementationthen occurs after about 2 minutes. In LEMS,the initial CMAP is of very low amplitude,increasing by greater than 200% after brief, 10-second exercise. After a few minutes, the amplitude again is low.
D, Use of a special single-fi ber needleallows the recording of action potentialsfrom individual muscle fi bers. Trigger-ing on one muscle cell action potential,the potential from a neighboring fi berof the same motor unit is also capturedand appears time-locked with the fi rst as a pair on the oscilloscope. (1) The fi rst potential is held steady on the screenby the instrument; the second fi res with variable timing, a phenomenon calledjitter. The jitter is increased in MG (2), andblocking of the second potential occurswhen the neuromuscular junction fails (3) (arrows). EMG—electromyograph. (Adapted from Muscle Nerve [71].)

Neuroimmunology 535
Patient with myasthenia gravis
Delay thymectomyuntil puberty; use
immunosuppressivetherapy (AZA, CSA,prednisone, IVIg,plasma exchange)
if necessary
Gradually taperimmunotherapy
Response to thymectomy?
Thymectomy
Add alternative treatment (AZA, CSA, IVIg)
NoNoYeY s
Continuepyridostigmine
Use immuno-suppressivecautiously
(intermittentprednisone)
NNoYYes
Add plasmaexchange
Switch to alternate-day prednisone
NNoNoNo YeYess
Continue plasmaexchange: consider IVIg
YeYes
Yes NoNN
Grade IVLife-threatening crisis
Grade IIISevere generalized disease
Trial of pyridostigmineTrial ofpyridostigmine
Begin daily prednisonePlasma exchange,
corticosteroids
Are additionaltherapies needed?
Patient between ages ofpuberty and 60 years?
Is patient respondingto prednisone?Response to treatment?
Grade IFocal disease
Grade IIGeneralized disease
Figure 13-26. Clinical algorithm for the treatment of myasthenia gravis. Treatment strategies in myasthenia gravis include the useof pharmacologic agents directed at the function of the neuro-muscular junction, immunosuppressant and immunomodulat-
ing techniques, and surgical thymectomy. AZA—azathioprine; CSA—cyclosporine; IVIg—intravenous immunoglobulin.(Adapted from Mendell [72].)

536 Atlas of Clinical Neurology
LAMBERT-EATON SYNDROME
Continue to treatwith pyridostigmine
Reassess tumor status on regular basis
Response to treatment?
Response to treatment?
Continue yearlyscreen for cancer
No tumor foundTumor found and treated
Treat LES with pyridostigmine(or 3,4-diaminopyridine
if available)
Search for malignancy
Combined treatmentwith plasmapheresis,
prednisone,azathioprine
Patient with LES
YYeess NoNo
Taper immunosuppression
Consider other immunosuppression
YYes NoNoFigure 13-27. Clinical algorithm for the treatment of Lambert-Eaton syndrome (LES). The management of LES assumes thepresence of an underlying malignancy, although 30% of patientsmay have no tumor found. Pharmacologic treatment is a secondstep. Immunosuppressive treatment should be used only when tumor is absent. (Adapted from Mendell [72].)
INFLAMMATORY MYOPATHIES
Diagnostic Criteria for Infl ammatory MyopathiesPolymyositis Dermatomyositis Inclusion body myositis
Criterion Defi nite Probable* Defi nite Mild or early Defi nite
Muscle strength Myopathic muscle weakness†
Myopathicmuscle weakness†
Myopathic muscleweakness†
Seemingly normalstrength‡
Myopathic muscle weakness with early involvement ofdistal muscles†
Electromyo-graphic fi ndings
Myopathic Myopathic Myopathic Myopathic or nonspecifi c
Myopathic with mixed potentials
Muscle enzymes Elevated (up to 50-fold)
Elevated(up to 50-fold)
Elevated (up to 50-fold)or normal
Elevated (up to 10-fold)or normal
Elevated (up to 10-fold)or normal
Muscle biopsy fi ndings
Diagnostic for this type of infl ammatorymyopathy
Nonspecifi c myopathywithout signs of primary infl ammation
Diagnostic Nonspecifi c or diagnostic
Diagnostic
Rash or calcinosis Absent Absent Present Present Absent
*An adequate trial of prednisone or other immunosuppressive drugs is warranted in probable cases. If, in retrospect, the disease is unresponsive to therapy,another muscle biopsy should be considered to exclude other diseases or possible evolution to inclusion body myositis.
†Myopathic muscle weakness, affecting proximal muscles more than distal ones and sparing eye and facial muscles, is characterized by a subacute onset (weeks tomonths) and rapid progression in patients who have no family history of neuromuscular disease, no endocrinopathy, no exposure to myotoxic drugs or toxins, and no biochemical muscle disease (excluded on the basis of muscle biopsy fi ndings).
‡Although strength is seemingly normal, patients often have new onset of easy fatigue, myalgia, and reduced endurance. Careful m‡ uscle testing may reveal mild muscle weakness.
Figure 13-28. Diagnostic criteria for infl ammatory myopathy.The autoimmune nature of acquired infl ammatory muscle dis-ease is generally accepted, and both cellular and humeral fac-tors are involved. Cellular attack directed against muscle fi bercomponents mediates the muscle invasion and phagocytosis
that are seen in polymyositis (PM) [24,73]. Dermatomyositis (DM), by contrast, appears to be mediated by an autoantibody or immune complex response directed against a component of the vascular endothelium.
Continued on the next page

Neuroimmunology 537Figure 13-28. (Continued) Damage to muscle and other tissues results from disruption of endothelial cells and capillaries, a theory in line with the appearance of perifascicular atrophy in muscle biopsy.
The skin manifestations of DM set it apart. Psoriatic rash overthe knuckles (Gottron’s sign), forehead and malar rash, periorbital discoloration, nail signs, and subcutaneous calcifications are dis-tinctive, but these may be noticed only in retrospect after biopsydiagnosis. Proximal painless muscle weakness in PM is unaccom-panied by other unique clinical features, so diagnosis relies on biopsy and the exclusion of other causes of muscle inflammation.Inclusion body myositis (IBM) is clinically and histologically distinctfrom PM and DM. The inflammatory myopathy in IBM may only be a secondary response to an underlying myopathic process [2,74].
Later age at onset and mixed proximal and distal weaknesscharacterize IBM. Finger flexors and ankle dorsiflexors arecharacteristically involved. The muscle biopsy in IBM shows rimmed vacuoles within muscle fibers accompanied by endomysial inflammation [75].
No proof of therapeutic efficacy has been achieved in PM, DM, or IBM for any pharmacologic or procedural method. Prednisone is first line for PM and DM, but refractory cases call for the use of methotrexate, azathioprine, cyclophosphamide, irradiation (lym-phoid or total body), plasmapheresis, and high-dose intravenousimmunoglobulin. Objective clinical measures such as an expanded Medical Research Council scale, and not creatine kinase levels,should be used to drive the therapeutic decision-making process.
The diagnosis of inflammatory myopathy relies on 1) demonstra-tion of muscle weakness, usually proximal, in the absence of severe sensory loss; 2) elevated muscle enzymes; 3) electromyography demonstrating brief, small, polyphasic motor units in association with fibrillations, positive waves, and complex repetitive discharges;4) muscle biopsy with characteristic features. DM shows accompa-nying features of rash and calcinosis. Distal weakness and mixedfeatures on electromyography typify IBM. Care should be taken toexclude infectious processes, toxic myopathies, and other systemic diseases when making these diagnoses. (Adapted from(( Dalakas [76].)
Age Groups Affected by and Conditions or Factors Associated With Inflammatory Myopathies
Characteristic Dermatomyositis Polymyositis Inclusion body myositis
Age at onset of disease Adulthood and childhood > 18 years of age > 50 years of age
Associated condition or factor
Connective tissue disease Yes, with scleroderma and mixed connective tissue disease
Yes Yes, in up to 15% of cases
Overlap syndrome Yes, with scleroderma and mixed connective tissue disease
No No
Systemic autoimmune diseases* Infrequently Frequently Infrequently
Malignant conditions Probably No No
Viruses Unproved Yes, with HIV, HTLV-1; possibly other viral or postviral conditions
Unproved
Parasites and bacteria No Yes† No
Drug-induced myotoxicity‡ Yes Yes No
Familial association No No Yes, in some cases
*The most commonly associated systemic autoimmune diseases are Crohn’s disease, vasculitis, sarcoidosis, primary biliary cirrhosis, adult celiac disease, chronic graft-versus-host disease, discoid lupus, ankylosing spondylitis, Behçet’s syndrome, myasthenia gravis, acne fulminans, dermatitis herpetiformis, psoriasis, Hashimoto’s disease, granulomatous diseases, agammaglobulinemia, monoclonal gammopathy, hypereosinophilic syndrome, Lyme disease, Kawasaki disease,autoimmune thrombocytopenia, hypergammaglobulinemic purpura, hereditary complement deficiency, and IgA deficiency.
†Includes parasitic (protozoa, cestodes, and nematodes), tropical, and bacterial myositis.‡Drugs include penicillamine (for dermatomyositis and polymyositis), zidovudine (for polymyositis), and contaminated tryptophan (for a dermatomyositis-likeillness). Other myotoxic drugs may cause myopathy but not inflammatory myopathy.
Figure 13-29. Age groups affected by and conditions or factors associated with inflammatorymyopathies. HTLV—human T-cell lymphotropic virus. (Adapted from Dalakas [76].)
Figure 13-30. Micrograph showing nonnecrotic muscle fiberssurrounded and invaded by mononuclear cells in polymyositis. (From [77]; courtesy of Andrew G. Engel, MD, Mayo Clinic,fRochester, MN.)

538 Atlas of Clinical Neurology
A B
MHC I+musclefiber
MHC I+
CD3+
CD8+
MHC II+T cellFigure 13-31. Representation of the typi-
cal histologic changes observed in infl am-matory myopathies. A, Dermatomyositis.Muscle fi bers are shown in pink, blood vessels in red. Note atrophic fi bers at thelower edge of the fascicle (perifascicu-lar atrophy). Clusters of capillaries andvenules stain positively for complementmembrane attack complex (MAC), and MAC-positive vessels are marked withblack arrowheads. The capillary density issignifi cantly reduced. B, Polymyositis orinclusion body myositis. T cells surround
Figure 13-33. Blue-purple discoloration, the heliotrope rash,appearing on the upper eyelids and in the periorbital regionin a patient with infl ammatory myopathy (A). The forehead
and malar areas are affected by a nonraised red rash (B). (FromGriggs et al. [80]; with permission.)
BBBBBA
and focally invade a nonnecrotic muscle fi ber. All invaded muscle fi bers, and somethat are noninvaded, show surface reactivity for major histocompatibility complexclass I (MHC I). (Adapted from Hohlfeld et al. [78].)
Figure 13-32. Micrograph showing immunolocalization of comple-ment membrane attack complex (MAC) with red rhodamine fl uo-rescence in a patient with dermatomyositis. Numerous capillariesare immunoreactive for MAC. The large MAC-positive profi le at the upper right is a necrotic muscle fi ber. Complement activationand MAC deposition occur nonspecifi cally when a muscle fi berundergoes necrosis from any cause. (From Hohlfeld [79]; courtesy ofAndrew G. Engel, MD, Mayo Clinic, Rochester, MN.)

Neuroimmunology 539
AAAAAAAAAAAAAAAAAA BBBBBBBBBBBBBBBBBBBB
Figure 13-34. Gottron’s sign in dermato-myositis, which is seen in some patients with infl ammatory myopathies. A , A raised,violaceous, scaly eruption with a psoriatic appearance overlies the extensor surfacesof the knuckles. Similar lesions appear over the extensor surfaces of the elbows and other joints. B , The same patient after treat-ment with intravenous immunoglobulin. (From Dalakas et al. [81]; with permission.)
Suspected inflammatory myopathy
Dermatomyositis
Satisfactory objective benefit found?
Patient responding toAZA at 3–6 months?
Continue AZA andlow-dose prednisone
Initiate high-doseIVIg
Add AZA (3 mg/kg);accelerate tapering
of prednisone
Continueprednisone at lowest possible
maintenance dose
NoNoYesYes
Noo YesYes
NoNoYesYes
YYeses
NooN
NNo
High-dose prednisoneHigh-dose IVIg for 3 months
Objective response noted?
IBM
Patient showing objective response?
Continuetreatment
and monitor
Repeat infusion ofIVIg every 6–8 weeks
Consider adding prednisone withazathioprine or methotrexate
No NoNoYessYees
Objective improvement present?
Taper prednisone dose gradually
Re-evaluate muscle strength
Patient responding to IVIg?
Considercyclosporine or
cyclophosphamide
Repeat infusion ofIVIg every 6–8 weeks;
maintain low-doseprednisone every
other day
NoNoYesYes
Re-evaluate at 8 weeks
Initiate trial of high-dose IVIg
Consider trial of cyclosporine,
methotrexate, orcyclophosphamide
High-dose prednisone 80–100 mg/d for 4 weeksfollowed by tapering to every other day
Re-evaluate; challengeoriginal diagnosis;
consider IBM or otherdisease; consider
repeat muscle biopsy
Patient responding after 3 months (whileprednisone at 80–100 mg every other day)?
Polymyositis
Figure 13-35. Clinical algorithm for the treatment of infl ammatory myopathies. AZA—azathioprine; IBM—inclusion body myositis; IVIg—intravenous immunoglobulin. (Adapted from( Dalakas [76].)
540 Atlas of Clinical Neurology
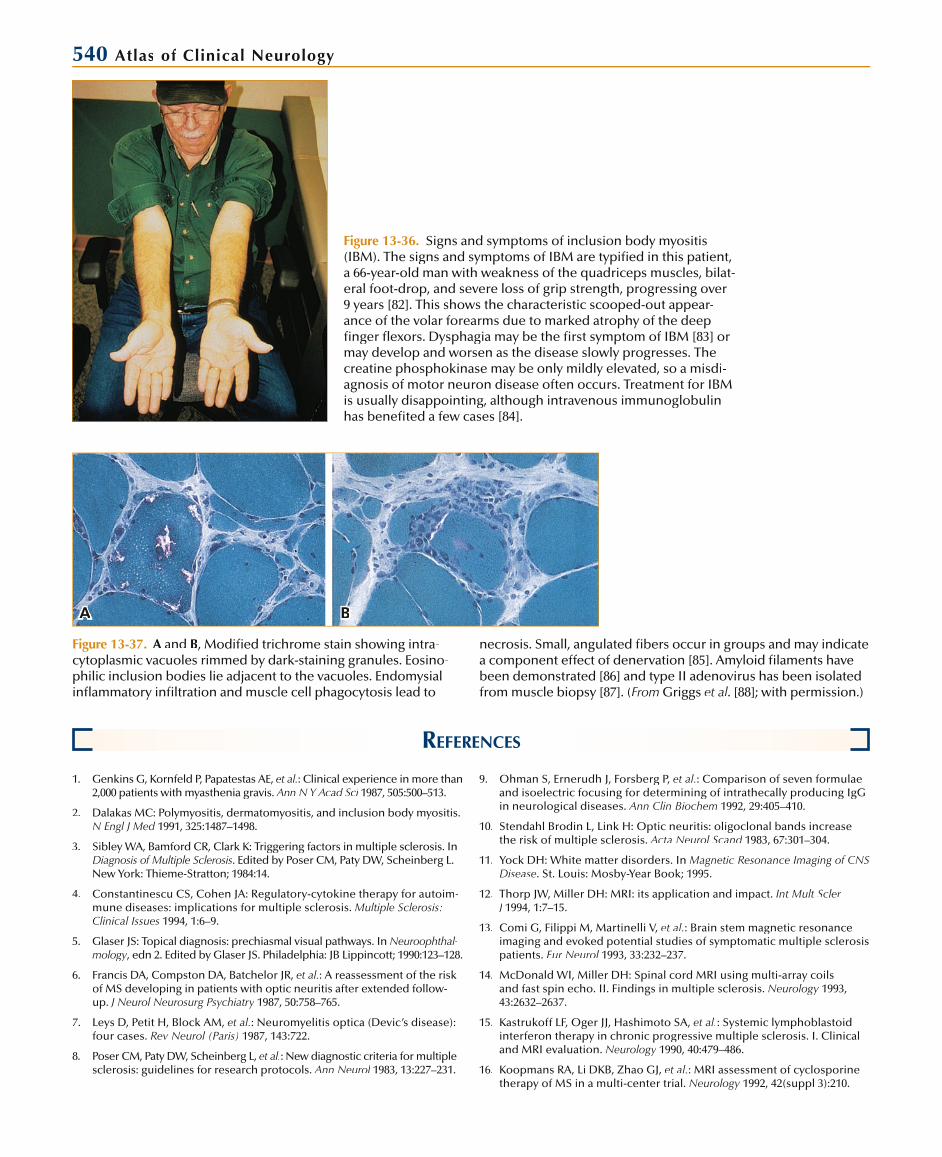
Figure 13-36. Signs and symptoms of inclusion body myositis (IBM). The signs and symptoms of IBM are typified in this patient, a 66-year-old man with weakness of the quadriceps muscles, bilat-eral foot-drop, and severe loss of grip strength, progressing over9 years [82]. This shows the characteristic scooped-out appear-ance of the volar forearms due to marked atrophy of the deep finger flexors. Dysphagia may be the first symptom of IBM [83] ormay develop and worsen as the disease slowly progresses. Thecreatine phosphokinase may be only mildly elevated, so a misdi-agnosis of motor neuron disease often occurs. Treatment for IBMis usually disappointing, although intravenous immunoglobulinhas benefited a few cases [84].
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA BBBBBBB
REFERENCES 1. Genkins G, Kornfeld P, Papatestas AE, et al.: Clinical experience in more than
2,000 patients with myasthenia gravis. Ann N Y Acad Sci 1987, 505:500–513. i
2. Dalakas MC: Polymyositis, dermatomyositis, and inclusion body myositis. N Engl J Med 1991, 325:1487–1498.
3. Sibley WA, Bamford CR, Clark K: Triggering factors in multiple sclerosis. In Diagnosis of Multiple Sclerosis. Edited by Poser CM, Paty DW, Scheinberg L. New York: Thieme-Stratton; 1984:14.
4. Constantinescu CS, Cohen JA: Regulatory-cytokine therapy for autoim-mune diseases: implications for multiple sclerosis. Multiple Sclerosis:Clinical Issues 1994, 1:6–9.
5. Glaser JS: Topical diagnosis: prechiasmal visual pathways. In Neuroophthal-llmology, edn 2. Edited by Glaser JS. Philadelphia: JB Lippincott; 1990:123–128.yy
6. Francis DA, Compston DA, Batchelor JR, et al.: A reassessment of the riskof MS developing in patients with optic neuritis after extended follow-up. J Neurol Neurosurg Psychiatry 1987, 50:758–765. y
7. Leys D, Petit H, Block AM, et al.: Neuromyelitis optica (Devic’s disease): four cases. Rev Neurol (Paris) 1987, 143:722.
8. Poser CM, Paty DW, Scheinberg L, et al.: New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann Neurol 1983, 13:227–231. l
9. Ohman S, Ernerudh J, Forsberg P, et al.: Comparison of seven formulaeand isoelectric focusing for determining of intrathecally producing IgGin neurological diseases. Ann Clin Biochem 1992, 29:405–410.
10. Stendahl Brodin L, Link H: Optic neuritis: oligoclonal bands increase the risk of multiple sclerosis. Acta Neurol Scand 1983, 67:301–304. d
11. Yock DH: White matter disorders. In Magnetic Resonance Imaging of CNS Disease. St. Louis: Mosby-Year Book; 1995.
12. Thorp JW, Miller DH: MRI: its application and impact. Int Mult Scler J 1994, 1:7–15.J
13. Comi G, Filippi M, Martinelli V, et al.: Brain stem magnetic resonance imaging and evoked potential studies of symptomatic multiple sclerosis patients. Eur Neurol 1993, 33:232–237. l
14. McDonald WI, Miller DH: Spinal cord MRI using multi-array coils and fast spin echo. II. Findings in multiple sclerosis. Neurology 1993,y43:2632–2637.
15. Kastrukoff LF, Oger JJ, Hashimoto SA, et al.: Systemic lymphoblastoidinterferon therapy in chronic progressive multiple sclerosis. I. Clinical and MRI evaluation. Neurology 1990, 40:479–486.y
16. Koopmans RA, Li DKB, Zhao GJ, et al.: MRI assessment of cyclosporinetherapy of MS in a multi-center trial. Neurology 1992, 42(suppl 3):210. y
Figure 13-37. A andA B, Modified trichrome stain showing intra-cytoplasmic vacuoles rimmed by dark-staining granules. Eosino-philic inclusion bodies lie adjacent to the vacuoles. Endomysial inflammatory infiltration and muscle cell phagocytosis lead to
necrosis. Small, angulated fibers occur in groups and may indicatea component effect of denervation [85]. Amyloid filaments have been demonstrated [86] and type II adenovirus has been isolatedfrom muscle biopsy [87]. (From Griggs et al. [88]; with permission.)

Neuroimmunology 54117. Thompson AJ, Miller D, Youl B, et al.: Serial gadolinium-enhanced MRI
in relapsing/remitting multiple sclerosis of varying disease duration. Neurology 1992, 42:60–63. y
18. Offenbacher H, Fazekas F, Schmidt R, et al.: Assessment of MRI criteria for a diagnosis of MS. Neurology 1993, 43:905–909.y
19. Filippi M, Martinelli V, Sirabian G, et al.: Brain magnetic resonanceimaging correlates of cognitive impairment in multiple sclerosis. J Neurol Sci 1993, 115(suppl):S66–S73. i
20. IFNB Multiple Sclerosis Study Group: Interferon -1b is effective in relapsing-remitting multiple sclerosis. I. Clinical results of a multicenter, randomized, double-blind, placebo controlled trial. Neurology 1993, y43:655–661.
21. Paty DW, Li DKB, UBC MS/MRI Study Group, IFNB Multiple Sclerosis Study Group: Interferon -1b is effective in relapsing-remitting multiplesclerosis. II. MRI analysis results of a multicenter, randomized, double-blind, placebo controlled trial. Neurology 1993, 43:662–667.y
22. Wolinsky JS: Copolymer 1: a most reasonable alternative therapy forearly relapsing-remitting multiple sclerosis with mild disability. Neurology1995, 45:1245–1247.
23. Beck RW, Cleary PA, Anderson MM, et al.: A randomized controlled trial of corticosteroids in the treatment of acute optic neuritis. N Engl J Med1992, 326:581–588.
24. Weiner HL, Mackin GA, Orav EJ, et al.: Intermittent cyclophosphamide pulse therapy in progressive multiple sclerosis: final report of theNortheast Cooperative Multiple Sclerosis Treatment Group. Neurology1993, 43:910–918.
25. Canadian Cooperative Multiple Sclerosis Study Group: The CanadianCooperative Trial of cyclophosphamide and plasma exchange in pro-gressive multiple sclerosis. Lancet 1991, 337:441–446. t
26. Goodkin DE, Rudick RA, Medendorp SV, et al.: Low dose oral weeklymethotrexate (MTX) significantly reduces the frequency of progression of impairment in patients with chronic progressive multiple sclerosis(CPMS). Neurology 1994, 44:A357.y
27. Sipe JC, Romine JS, Koziol JA, et al.: Cladribine in treatment of chronicprogressive multiple sclerosis. Lancet 1994, 344:9–13.t
28. Milligan NM, Miller DH, Compston DAS: A placebo-controlled trialof isoprinosine in patients with multiple sclerosis. J Neurol Neurosurg Psychiatry 1994, 57:164–168. y
29. Wiles CM, Omar L, Swan AV, et al.: Total lymphoid irradiation in multiple sclerosis. J Neurol Neurosurg Psychiatry 1994, 57:154–163.y
30. Miller A, Lider O, Roberts AB, et al.: Suppressor T cells generated byoral tolerization to myelin basic proteins suppress both in vitro and in vivo immune responses by the release of transforming growth factorafter antigen specific triggering. Proc Natl Acad Sci U S A 1992, 89:421.
31. Weiner HL, Mackin GE, Matsui M, et al.: Double-blind pilot trial of oraltolerization with myelin antigens in multiple sclerosis. Science 1993,259:1321–1324.
32. Polman CH, O’Connor PW, Havrdova E, et al.: A randomized, pla-cebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med 2006, 354:899–910.d
33. Achiron A, Pras E, Gilad R, et al.: Open controlled therapeutic trial ofintravenous immunoglobulin in relapsing-remitting multiple sclerosis.Arch Neurol 1992, 49:1233–1236. l
34. Rodriguez M, Karnes WE, Bartleson JD, et al.: Plasmapheresis in acute episodes of fulminant CNS inflammatory demyelination. Neurology1993, 43:1100–1104.
35. IFNB Multiple Sclerosis Study Group and the University of BritishColumbia MS/MRI Analysis Group: Interferon -1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. Neurology 1995, 45:1277–1285. y
36. Johnson KP, Brooks BR, Cohen JA, et al., and the Copolymer 1 MultipleSclerosis Study Group: Copolymer 1 reduces relapse rate and improves disability in relapsing-remitting multiple sclerosis: results of a phaseIII multicenter, double-blind, placebo controlled trial. Neurology 1995, y45:1268–1276.
37. Noseworthy JH, Hopkins MB, Vandervoort MK, et al.: An open trial evaluation of mitoxantrone in the treatment of progressive MS.Neurology 1993, 43:1401–1406.y
38. Graus F, Dalmau JO: Management of paraneoplastic neurologicalsyndromes. In Neurological Complications of Cancer. Edited by Wiley RO. New York: Marcel Dekker; 1995:167–198.
39. Posner JB: Paraneoplastic syndromes. In Neurological Complications of Cancer. Edited by Posner JB. Philadelphia: FA Davis; 1995:353–384.
40. Jacobson DM, Thirkill CL, Tipping SJ: A clinical triad to diagnose para-neoplastic retinopathy. Ann Neurol 1990, 28:162–167.l
41. Dropcho EJ: Autoimmune central nervous system paraneoplastic disor-ders: mechanisms, diagnosis and therapeutic options. Ann Neurol 1995, l37(suppl 1):S102–S113.
42. Greenlees J, Brashear HR: Remote effects of carcinoma. In Current Therapy in Neurologic Disease. Edited by Johnson RT, Griffin JW. St. Louis: Mosby-Year Book; 1995:167–198.
43. Brashear HR: Antibody testing: finding the inside track to early diagno-sis of CNS paraneoplastic syndromes. Adv Neuroimmunol 1995, 2:3–11. l
44. Meinck HM, Ricker K, Hulser PJ, et al.: Stiff-man’s syndrome: neurophys-iological findings in 8 patients. J Neurol 1995, 242:134–142.l
45. Meinck H, Ricker K, Hulser PJ, et al.: Stiff-man’s syndrome: clinical and laboratory findings in 8 patients. J Neurol 1994, 241:157–166.l
46. Folli F, Solimena M, Cofiell R, et al.: Autoantibodies to a 128-kd synaptic protein in 3 women with stiff-man syndrome and breast cancer. N Engl J Med 1993, 328:546–551.d
47. Smith RG, Engelhardt JI, Tajti J, et al.: Experimental immune-mediated motor neuron diseases: models for human ALS. Brain Res Bull 1993,l30:373–380.
48. Rogers SW, Andrews PI, Gahring LC, et al.: Autoantibodies to glutamate receptor 3 in Rasmussen’s encephalitis. Science 1994, 265:648–651.
49. Parry GJ: Inflammatory demyelinating polyneuropathies: new perspectivesin treatment. Adv Neuroimmunol 1994, 1:9–15. l
50. Dyck PJ, Daube J, O’Brien P, et al.: Plasma exchange in chronic inflamma-tory demyelinating polyradiculoneuropathy. N Engl J Med 1986, 314:461–465. d
51. Dyck PJ, Litchy WJ, Kratz KM, et al.: A plasma exchange versus immune globulin infusion trial in chronic inflammatory demyelinating polyra-diculoneuropathy. Ann Neurol 1994, 36:838–845. l
52. Krendel DA: Successful treatment of neuropathies in patients with diabetes mellitus. Arch Neurol 1995, 52:1053–1061.l
53. Kissel JT, Mendel JR: Vasculitic neuropathy. Neurol Clin 1992, 10:761–781.
54. Olney RK: Neuropathies in connective tissue disease. Muscle Nerve1992, 15:531–542.
55. van der Meche FGA, Schmitz PIM, and the Dutch Guillain-Barré StudyGroup: A randomized trial comparing intravenous immune globulin and plasma exchange in Guillain-Barré syndrome. N Engl J Med 1992,d326:1123–1129.
56. Hayes MT: Analyzing new strategies to diagnose and treat autoimmuneneuropathies. Adv Neuroimmunol 1995, 2:10–17.l
57. Parry G, Swenson MR: When is antibody testing useful and what therapy is effective in immune-mediated neuropathies? Adv Neuroim-munol 1995, 2:18–22. l
58. Odabasi Z, Joy JL, Claussen GC, et al.: Isaacs’ syndrome associated with chronic inflammatory demyelinating polyneuropathy. Muscle Nerve1996, 19:210–215.
59. Newsom-Davis J, Mills KR: Immunological associations of acquiredneuromyotonia (Isaacs’ syndrome): report of five cases and literaturereview. Brain 1993, 116 (part III):453–469.
60. Sinha S, Newsom-Davis J, Mills K, et al.: Autoimmune aetiology for acquired neuromyotonia (Isaacs’ syndrome). Lancet 1991, 338:75–77. t
61. Quarles RH, Colman DR, Salzer JL, et al.: Myelin associated glycoprotein: structure-function relationships and involvement in neurological diseases.In Myelin: Biology and Chemistry. Edited by Martenson RE. Boca Raton,FL: CRC Press; 1992:413–448.

542 Atlas of Clinical Neurology
62. Quarles RH: Antibody mediated neuropathies: exploring the pathogenic mechanisms. Adv Neuroimmunol 1995, 2:3–9.l
63. Drachman DB: Myasthenia gravis. N Engl J Med 1994, 330:1797–1810. d
64. Grob D, Arsura EL, Brunner NG, Namba T: The course of myasthenia gravis and therapies affecting outcome. Ann N Y Acad Sci 1987, 505:472–479.i
65. Engel AG: Review of evidence for loss of motor nerve terminal calcium channels in Lambert-Eaton myasthenic syndrome. Ann N Y Acad Sci1991, 635:246–258.
66. O’Neill JH, Murray NM, Newsom-Davis J: The Lambert-Eaton myasthenic syndrome: a review of 50 cases. Brain 1988, 111:577–596.
67. Chalk CH, Murray NM, Newsom-Davis J: Response of the Lambert-Eatonmyasthenic syndrome to treatment of associated small cell lung carcinoma. Neurology 1990, 40:1552–1556. y
68. Soliven BC, Lange DJ, Penn AS, et al.: Seronegative myasthenia gravis. Neurology 1988, 38:514–517.y
69. Lindstrom JM: Pathophysiology of myasthenia gravis: the mechanisms behind the disease. Adv Neuroimmunol 1994, 1:3–8. l
70. Newsom-Davis J: Myasthenia gravis: the Lambert-Eaton myasthenic syn-drome and acquired myotonia. In Diagnostic and Therapeutic Approachesto Myasthenia Gravis. Proceedings of the Annual Meeting of the Myas-thenia Gravis Foundation of America, Salt Lake City, Utah, April 28, 1995.
71. Section II: Illustrations of selected waveforms. Muscle Nerve 1987,10(8S):G24–G52.
72. Mendell J: Neuromuscular junction disorders: a guide to diagnosis andtreatment. Adv Neuroimmunol 1994, 1:9–16.l
73. Hohlfeld R, Engel AG, Kunio I, et al.: Polymyositis mediated by T celllymphocytes that express the gamma delta receptor. N Engl J Med 1991,d324:877–881.
74. Barohn RJ, Amato AA, Sahenk Z, et al.: Inclusion body myositis: expla-nation for poor response to immunosuppressive therapy. Neurology1995, 45:1302–1304.
75. Lotz BP, Engel AG, Nishino H, et al.: Inclusion body myositis. Brain1989, 112:727–742.
76. Dalakas MC: Polymyositis, dermatomyositis, and inclusion-body myositis.N Engl J Med 1991, 325:1487–1498.d
77. Cover photo from Adv Neuroimmunol 1995, 2(1). l
78. Hohlfeld R, Engel AG, Kunio I, et al.: The immunobiology of muscle. Immunol Today 1994, 15:269–274. y
79. Hohlfeld R: New concepts in the immunobiology of inflammatorymyopathy. Adv Neuroimmunol 1995, 2:4–8. l
80. Griggs R, Mendell J, Miller R: Inflammatory myopathy. In Evaluation and Treatment of Myopathy. Philadelphia: FA Davis; 1995.
81. Dalakas MC, Illa I, Dambrosia JM, et al.: A controlled trial of high-doseintravenous immune globulin infusions as treatment for dermatomyosi-tis. N Engl J Med 1993, 329:1993–1999.d
82. Shaibani A, Harati Y: Idiopathic inflammatory myopathies: polymyositis, dermatomyositis, inclusion body myositis. In Neuro-Immunology for the Clinician. Edited by Rolak LA, Harati Y. Boston: Butterworth-Heinemann; 1997:301–316.
83. Riminton DS, Chambers ST, Darkin PJ, et al.: Inclusion body myositispresenting solely as dysphagia. Neurology 1993, 43:1241. y
84. Dalakas MC, Dambrosia JM, Sekul EA, et al.: Inclusion body myositis:the efficacy of high-dose intravenous immunoglobulin (IVIg) in patients with inclusion body myositis. Neurology 1995, 45(suppl 4):A208. y
85. Pruitt JN, Showalter CJ, Engel AG, et al.: Sporadic inclusion body myositis:counts of different types of abnormal fibers. Ann Neurol 1996, 39:139.l
86. Mendell JR, Sahenk Z, Gales T, Paul L: Amyloid filaments in inclusionbody myositis: novel findings provide insight into nature of filaments.Arch Neurol 1991, 48:1229–1234. l
87. Mikol J, Felten-Papaiconomou A, Ferchal F, et al.: Inclusion-body myo-sitis: clinicopathological studies and isolation of an adenovirus type 2from muscle biopsy specimen. Ann Neurol 1982, 11:576–581. l
88. Griggs RC, Mendell JR, Miller RG: Evaluation and Treatment of Myopathies. Philadelphia: FA Davis; 1995:172.