neuroimmunology in clinical practice€¦ · neuroimmunology in clinical practice / edited by...
TRANSCRIPT

Neuroimmunology inClinical Practice
Edited by Bernadette Kalman and Thomas H. Brannagan III


Neuroimmunology in Clinical Practice


Neuroimmunology inClinical Practice
Edited by Bernadette Kalman and Thomas H. Brannagan III
© 2008 by Blackwell Publishing Ltd
BLACKWELL PUBLISHING350 Main Street, Malden, MA 02148-5020, USA9600 Garsington Road, Oxford OX4 2DQ, UK550 Swanston Street, Carlton, Victoria 3053, Australia
The right of Bernadette Kalman and Thomas H. Brannagan III to be identified as the Authors of the Editorial Material in this Work has been asserted in accordance with the UK Copyright, Designs, and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright, Designs, and Patents Act 1988, without the prior permission of the publisher.
First published 2008 by Blackwell Publishing Ltd
1 2008
Library of Congress Cataloging-in-Publication Data
Neuroimmunology in clinical practice / edited by Bernadette Kalman and Thomas H. Brannagan III.p. ; cm.
Includes bibliographical references and index.ISBN-13: 978-1-4051-5840-4 (hardback : alk. paper)ISBN-10: 1-4051-5840-9 (hardback : alk. paper) 1. Neuroimmunology. 2. Nervous
system—Diseases—Immunological aspects. I. Kalman, Bernadette. II. Brannagan, Thomas H.[DNLM: 1. Autoimmune Diseases of the Nervous System—physiopathology. 2. Nervous
System—immunology. WL 140 N49152 2008]
RC346.5.N4785 2008616.8′0479—dc22
2007001113
A catalogue record for this title is available from the British Library.
Set in 10/12.5pt Photinaby Graphicraft Limited, Hong KongPrinted and bound in Singaporeby Fabulous Printers Pte Ltd
The publisher’s policy is to use permanent paper from mills that operate a sustainable forestry policy, and which has been manufactured from pulp processed using acid-free and elementarychlorine-free practices. Furthermore, the publisher ensures that the text paper and cover board used have met acceptable environmental accreditation standards.
For further information onBlackwell Publishing, visit our website:www.blackwellpublishing.com

Contents
Preface, viiForeword, viiiContributing authors, ix
Part I: Basic science introduction to clinical neuroimmunology, 1Editor: Bernadette Kalman
1 The basics of cellular and molecularimmunology, 3Amy E. Lovett-Racke, Anne R. Gocke, and Petra D. Cravens
2 Major components of myelin in themammalian central and peripheral nervous systems, 11Alexander Gow
Part II: Inflammatory demyelination in the central nervous system, 27Editor: Bernadette Kalman
3 Multiple sclerosis, 29
3.1 Epidemiology and genetics (Bernadette Kalman), 29
3.2 Immunopathogenesis (Thomas P. Leist), 35
3.3 Courses and diagnosis of MS (Bernadette Kalman), 38
3.4 Clinical features (Bernadette Kalman), 42
3.5 The pathology of MS: A quest for clinical correlation (William F. Hickey), 50
3.6 Cerebrospinal fluid (Mark S. Freedman), 54
3.7 Magnetic resonance imagingcharacteristics of MS (Jennifer L. Coxand Robert Zivadinov), 56
3.8 Treatment of MS (Sean Pittock), 63
4 Dévic’s disease, 83Bernadette Kalman
5 Acute disseminated encephalomyelitis and related conditions, 88Robert S. Rust
Part III: Autoimmune diseases of the peripheral nervous system and the muscle, 115Editor: Thomas H. Brannagan III
6 Guillain–Barré syndrome, 117Eduardo A. De Sousa and Thomas H.Brannagan III
7 Immune-mediated chronic demyelinatingpolyneuropathies, 123Thomas H. Brannagan III
8 Immune-mediated autonomic neuropathies, 139Louis H. Weimer and Mill Etienne
9 Autoimmune myasthenic syndromes:Myasthenia gravis and Lambert–Eatonmyasthenic syndrome, 153Andrew Sylvester and Armistead Williams
10 Polymyositis and dermatomyositis, 169S. Christine Kovacs
Part IV: Disorders of the central andperipheral nervous systems related to known or assumed system-immuneabnormalities, 179Editor: Bernadette Kalman
11 Neuro-Sjögren’s syndrome, 181Bernadette Kalman
vi CONTENTS
12 Neuro-Behçet’s syndrome, 185Bernadette Kalman
13 Steroid-responsive encephalopathy associated with Hashimoto’s thyroiditis, 189Bernadette Kalman
14 Rasmussen’s encephalitis, 191Bernadette Kalman
15 Susac’s syndrome, 197Bernadette Kalman
16 Cogan’s syndrome, 200Bernadette Kalman
17 Neurosarcoidosis, 203Bernadette Kalman
18 Anti-VGKC syndromes: Isaacs’ syndrome,Morvan’s syndrome, and autoimmune limbic encephalitis, 207Bernadette Kalman
19 Paraneoplastic neurological autoimmunity, 210Daniel H. Lachance and Vanda A. Lennon
20 Vasculitis and connective tissue diseases, 218David S. Younger and Adam P.J. Younger
21 Poststreptococcal movement disorders, 240Andrew J. Church and Gavin Giovannoni
22 Neurological manifestations of gluten sensitivity, 251Marios Hadjivassiliou
23 Anti-GAD associated neurological diseases, 256Marios Hadjivassiliou
Index, 259

Neurology, as many other fields in medicine, hasevolved into a framework of rapidly developing sub-specialties increasingly dependent on technology-driven advances in clinical and basic sciences.Neuroimmunology is a particularly dynamic sub-specialty with daily emergence of new informationin imaging, electrophysiology, clinical trials, molecularimmunology, neurosciences, and genetics, whichnecessitates frequent changes in clinical practice.The authors of this book recognize the difficult taskthat neurology residents and other young medicalprofessionals have to face when preparing for theirexams and practicing modern neuroimmunology.With the intention to alleviate this task, here we provide a comprehensive but concise description of
immune-mediated neurological disorders comple-mented with the most pertinent and up-to-date scientific data. We hope that not only residents, fellows, young neurologists, physician assistants,and nurses, but also scientists working in the area of neuroimmunology will find this volume useful.The editors invited coauthor experts who both teachand study specific aspects of neuroimmunology at academic medical centers. Non-author expertsincluding Drs. John O. Susac, Mark Keegan, ChristianG. Bien, Horst Urbach, Alexander G. Khandji, andFred D. Lublin generously contributed to severalchapters with their constructive comments andimages of rare disorders.
Preface

Foreword
Neuroimmunology in Clinical Practice provides a use-ful and comprehensive review of the field of clinicalneuroimmunology. In addition to presenting timelyupdates of such common conditions as multiple sclerosis, autoimmune neuropathies, myastheniagravis, and polymyositis, it highlights less familiarneuroimmunological entities such as anti-VGKCsyndromes, and gluten-induced neurological dys-function, which can go unrecognized in commonclinical practice. It provides a scientific background
for understanding the underlying pathophysiology,and guides the physician through the diagnosis andmanagement of patients with these conditions. Thebook is a welcome and timely addition to our libraryof neurological subspecialties.
Norman Latov, M.D., Ph.D.Professor of Neurology and NeuroscienceWeill Medical College of Cornell University

Contributing authors
Thomas H. Brannagan, III. M.D.Associate ProfessorDirector, Diabetic Neuropathy Research Center,Peripheral Neuropathy CenterDepartment of NeurologyWeill Medical College of Cornell University635 Madison Avenue, Suite 400New York, NY 10022, [email protected]
Andrew Church, Ph.D.FellowDepartment of NeuroinflammationNational Institute of NeurologyUniversity College of LondonQueen SquareLondon WC1N 3BG, United [email protected]
Jennifer L. Cox, Ph.D.Assistant ProfessorDepartment of NeurologySUNY School of Medicine and Biomedical SciencesThe Jacobs Neurological Institute100 High StreetBuffalo, NY 14203, [email protected].
Petra D. Cravens, Ph.D.Postdoctoral FellowDepartment of NeurologyUniversity of Texas Southwestern Medical Center5323 Harry Hines BlvdDallas, TX 75390-9036, [email protected]
Eduardo Adonias De Sousa, M.D.Assistant ProfessorDepartment of NeurologyThomas Jefferson University900 Walnut Street, Suite 200
Philadelphia, PA 19107, [email protected]
Mill Etienne, M.D.FellowDepartment of NeurologyCollege of Physicians and SurgeonsColumbia University710W 168th StreetNew York, NY 10032, [email protected]
Mark S. Freedman M.Sc., M.D., FAAN, FRCP(C)Professor of Medicine (Neurology)Director, Multiple Sclerosis Research UnitUniversity of OttawaThe Ottawa Hospital-General CampusBox 601, 501 Smyth RoadOttawa, ON K1H8L6, [email protected]
Gavin Giovannoni, M.D., Ph.D.Department of NeuroinflammationConsultant NeurologistNational Institute of NeurologyUniversity College of LondonQueen SquareLondon WC1N 3BG, United [email protected]
Alexander Gow, Ph.D.Associate ProfessorCenter for Molecular Medicine and GeneticsWayne State University School of Medicine3216 Scott Hall, 540 E Canfield AveDetroit, MI 48201, [email protected]
Anne R. Gocke, B.S.StudentDepartment of Neurology

x CONTRIBUTING AUTHORS
University of Texas Southwestern Medical Center5323 Harry Hines BlvdDallas, TX 75390-9036, [email protected]
Marios Hadjivassiliou, M.D.Consultant NeurologistDepartment of NeurologyThe Royal Hallamshire HospitalGlossop RoadSheffield S10 2JF, United [email protected]
William F. Hickey, M.D.Professor of Pathology and NeuropathologySenior Associate Dean for Academic AffairsDepartment of PathologyDartmouth-Hitchcock Medical CenterOne Medical Center DriveLebanon, NH 03756, [email protected]
Bernadette Kalman, M.D., Ph.D.Associate Professor of Neurology, Associate Chief of StaffVAMC and SUNY Upstate Medical University800 Irving Avenue, Research (151)Syracuse, NY 13210, [email protected]
S. Christine Kovacs, M.D.Assistant Clinical Professor of MedicineDivision of RheumatologyLehay Clinic41 Mall RoadBurlington, MA 01805, USATufts Medical SchoolBoston, [email protected]
Daniel H. Lachance, M.D.Assistant Professor of NeurologyConsultant, Neurology and NeuroimmunologyLaboratoryMayo Clinic College of MedicineRochester, MN 55905, USA200 First St. [email protected]
Thomas P. Leist, M.D., Ph.D.Associate ProfessorDirector of the Comprehensive MS Center and the
Division of NeuroimmunologyDepartment of NeurologyThomas Jefferson University900 Walnut Street, Suite 200Philadelphia, PA 19107, [email protected]
Vanda A. Lennon, M.D., Ph.D.Director, Neuroimmunology Laboratory, Professor of Immunology and NeurologyDirector, Autoimmune Neurology FellowshipProgramMayo Clinic College of Medicine200 First St. SWRochester, MN 55905, [email protected]
Amy Lovett-Racke, Ph.D.Assistant ProfessorDepartment of Molecular VirologyImmunology and Medical GeneticsOhio State University College of Medicine333 W. 10th Avenue2166D Graves HallColumbus, OH 43210, [email protected]
Sean J. Pittock, M.D.Assistant Professor of NeurologyCo-Director Neuroimmunology LaboratoryCo-Director Autoimmune Neurology FellowshipMayo Clinic College of Medicine200 First St. SWRochester, MN 55905-0001, [email protected]
Robert S. Rust Jr., M.D.Thomas E. Worall, Jr. Professor of Epileptology andNeurology and Professor of PediatricsDepartment of Neurology and PediatricsUniversity of VirginiaP.O. Box 800394Charlottesville, VA 22908, [email protected]
Andrew Sylvester, M.D.Attending NeurologistInternational Multiple SclerosisManagement Practice521 West 57th Street, Suite 400New York, NY 10019, [email protected]
Contributing authors xi
Louis H. Weimer, M.D.Associate Clinical ProfessorDepartment of NeurologyCollege of Physicians and SurgeonsColumbia University710W 168th street, R55New York, NY 10032, [email protected]
Armistead Williams, M.D.FellowInternational Multiple SclerosisManagement Practice521 West 57th Street, Suite 400.New York, NY 10019, [email protected]
Adam P.J. YoungerResearch AssistantEdgemont Science Scholar Program300 White Oak LaneScarsdale, NY 10583, USA
David S. Younger, M.D.Clinical Associate ProfessorDepartment of NeurologyNew York University School of MedicineSt. Vincent’s Catholic Medical CenterLenox Hill Hospital550 First AvenueNew York, NY 10016, [email protected]
Robert Zivadinov, M.D., Ph.D.Associate ProfessorDepartment of NeurologySUNY School of Medicine and Biomedical SciencesThe Jacobs Neurological Institute100 High StreetBuffalo, NY 14203, [email protected]


Part I
Basic science introduction to clinical neuroimmunology
Editor: Bernadette Kalman


The immune system is composed of cells, tissues, and vessels that collectively protect the body frompathogens. In some instances, the immune systemcan inadvertently cause tissue damage resulting inimmune-mediated diseases, and appears to be at leastpartially responsible for the pathology seen in multiplesclerosis (MS). The immune system provides defensesagainst pathogens in nonspecific mechanisms, termedinnate immunity, and pathogen-specific mechanisms,termed adaptive immunity. Innate immunity is composed of phagocytic cells that engulf and digestmicroorganisms, natural killer cells that nonspecific-ally kill infected cells, and physical barriers as a meansto eradicate pathogens. Adaptive immunity is com-posed of cells that specifically recognize componentsof pathogens and directly target a particular infectedcell. It is the adaptive immune response that is be-lieved to be responsible for targeting self-proteins inautoimmunity, but innate immunity plays a criticalrole in the events that initially condition the environ-ment that ultimately determines the phenotype ofthe cells of the adaptive immune response.
B lymphocytes and T lymphocytes are the key cells that provide adaptive immunity. B cells havemultiple functions, including antibody production,antigen presentation, and immune modulation viacytokine expression. The production of antibodies by B cells is the key feature of humoral immunity,which is critical to the defense against extracellularmicrobes. Cell-mediated immunity is primarily provided by T cells, which recognize antigens of intracellular pathogens displayed on the surface of infected cells. Together, B cells and T cells can usually eradicate an infection in a pathogen-specificmanner with minimal damage to the host, and further protect the host from future infections of thatpathogen by establishing immunological memory.
Humoral immunity
B cells express and secrete antibodies that are uniqueand specific for proteins. This provides humoral
immunity to the host, which was originally describedas a form of immunity that could be transferred fromimmunized to naive hosts via serum. All antibodies,which are also referred to as immunoglobulins ( Ig),have a common structure composed of two heavyand two light chains (Edelman et al., 1969). Theheavy chain is composed of four sequence domains,three of which are highly conserved and referred to as constant regions (CH) (Hilschman and Craig,1969). The fourth domain, the variable region (VH),has a unique sequence that provides the specificity ofthe antibody for its target protein. Two identicalheavy chains are linked by disulfide bonds betweenthe CH1 and CH2 domains as shown in Fig. 1.1. Inaddition, there are two light chains that are each com-posed of a single constant region (CL) and a singlevariable region (VL ). The light chain is connected to the heavy chain at CH1 and CL. The VH and VLregions form the antigen-binding site. The V regionsof both the heavy and light chains contain threeshort, highly diverse sequences called the hypervari-able or complementary-determining regions (CDR),
1
The basics of cellular and molecular immunology
Amy E. Lovett-Racke, Anne R. Gocke, and Petra D. Cravens
Lightchain
Heavychain
Complementary-determiningregions (CDR)
VH
CH1
CH2
CH3
FC region
VL
CL
Antigen-binding site
Fc receptorcomplementbinding site
Fig. 1.1 Antibodies are composed of two heavy and twolight chains that form an antigen-specific binding site.

4 AMY E. LOVETT-RACKE, ANNE R. GOCKE, AND PETRA D. CRAVENS
which encode the unique binding site for specificantigens (Wu and Kabat, 1970).
Antibodies are classified into five isotypes based onthe differences in the structure of their heavy chain C regions, IgA, IgD, IgE, IgG, and IgM. IgM and IgDserve as the antigen receptors for the activation ofnaive B cells. Antigen binding to membrane-boundIgM and IgD results in the secretion of IgM andexpression of other Ig isotypes. This process, termedisotype switching, results from a new CH chain beingproduced by the B cells, while the V regions remainunchanged and thus the specificity of the antibody isthe same (Kataoka et al., 1980). Both secreted IgM,which is typically found in a pentameric form, andIgG can utilize the complement system to mediatethe lysis of IgM- or IgG-coated targets. IgG can alsofacilitate the opsonization of microbes by promotingthe phagocytosis of IgG-coated targets by binding tothe FC (constant region framework of IgG) receptorson phagocytes (Leijh et al., 1981). IgA providesdefenses against microbes that enter through mucosalsurfaces such as the gastrointestinal and respiratorytracts. IgA is produced by mucosal lymphoid tissues,secreted through the epithelium, binds to pathogensin the lumen, and prevents the entry of pathogensinto the host (South et al., 1966). IgE is the antibodyisotype that mediates immediate hypersensitivityreactions, as well as defense against helminthic parasites. Mast cells and basophils express an IgEreceptor that interacts with antigen-bound IgE, re-sulting in degranulation of mast cells and basophils,and the expression of immediate hypersensitivityreactions (Schleimer et al., 1986). Eosinophils expressIgE receptors and can elicit antibody-dependent cell-mediated cytotoxicity (ADCC) of IgE-coated hel-minthes (Gounni et al., 1994). Thus, antibodies protectthe host by providing a very diverse set of antigen-specific antibodies with multiple isotypes to controlthe numerous pathogens that the host encounters.In addition, antigen-specific memory B cells areestablished following the initial infection with a particular pathogen. Memory B cells produce anti-bodies rapidly following re-exposure to a pathogen,protecting the host from a subsequent infection (Uhr and Finkelstein, 1963).
Monoclonal antibodies have provided a valuableresearch tool, as well as a mechanism to developantigen-specific therapeutic agents. Since each B cell produces an antibody with a unique specificity,immortalized B cells have been generated that canproduce an unlimited amount of an antibody specificfor an antigen of interest. Immortalized B cells are
generated by fusing B cells with a myeloma cell toform a hybridoma, and then selecting B cell clonesthat produce an antibody with the desired specificity.Because monoclonal antibodies can be generated for virtually any protein or peptide, and even forpolysaccharides and lipids, they have become a majortool in studying many molecules. Some of the in vitroresearch techniques, which utilize monoclonal anti-bodies, include ELISA, ELISPOT, western blot, flowcytometry, and immunohistochemistry. Monoclonalantibodies have also been utilized in vivo to studyparticular molecules, pathways, and the function ofa specific cell population. In vivo, monoclonal anti-bodies that induce complement or ADCC can be usedto deplete a particular cell population by targeting acell-surface molecule specific for that cell population.In addition, monoclonal antibodies administered in vivo can be used to physically block a particularmolecule, thus preventing the natural ligand frombinding and initiating a signal. It is these in vivoresearch strategies that have extended into the devel-opment of monoclonal antibodies as therapeuticagents. A monoclonal antibody specific for the adhesion molecule, VLA4, expressed on T cells wasdeveloped as a therapeutic agent for multiple sclerosis.The anti-VLA4 antibody prevented the binding ofVLA4 to VCAM on the vascular epithelium, physic-ally preventing the entry of T cells into the centralnervous system (CNS) (Yednock et al., 1992; Milleret al., 2003). Using an alternative strategy, a mono-clonal antibody specific for CD20, a molecule expressedspecifically by B cells, was developed to treat B cell malignancies (Maloney et al., 1997). Anti-CD20binds to B cells and elicits an immune-mediateddestruction of these cells. Thus, monoclonal anti-bodies have been an invaluable tool in both theunderstanding and treatment of diseases.
Cell-mediated immunity
T lymphocytes are the mediators of cell-mediatedimmunity. T cells recognize antigens in the con-text of major histocompatibility complex (MHC)molecules. The human MHC, often referred to ashuman leukocyte antigens (HLA), contains at least50 genes on chromosome 6. T cells recognize anti-gens bound to HLA class I molecules called HLA-A, -B, and -C; and HLA class II molecules called HLA-DR, -DP, and -DQ. Class I molecules are single-chainglycoproteins that pair with β2-microglobulin. Incontrast, class II molecules are heterodimeric, com-posed of α and β chains.
The basics of cellular and molecular immunology 5
MHC molecules bind peptides derived frommicrobes generated by two distinct processing path-ways (Morrison et al., 1986). Endogenous cytosolicproteins from intracellular viruses or tumors aredigested into peptides in proteosomes, transported tothe endoplasmic reticulum where they bind MHCclass I molecules, and presented on the cell surface(Braciale, 1992). Virtually all nucleated cells expressMHC class I molecules with one notable exceptionbeing neurons ( Joly, Mucke, and Oldstone, 1991). It is also important to note that cell-surface MHCmolecules always contain a peptide, usually a self-peptide, which is not recognized by autologous Tcells. Peptides presented by MHC class I moleculesare recognized by T cells that express the CD8molecule. CD8 binds to nonpolymorphic regions of the class I molecule and actively participates in transducing signals necessary for activation in coordination with the T-cell receptor (Emmrich,Strittmatter, and Eichmann, 1986).
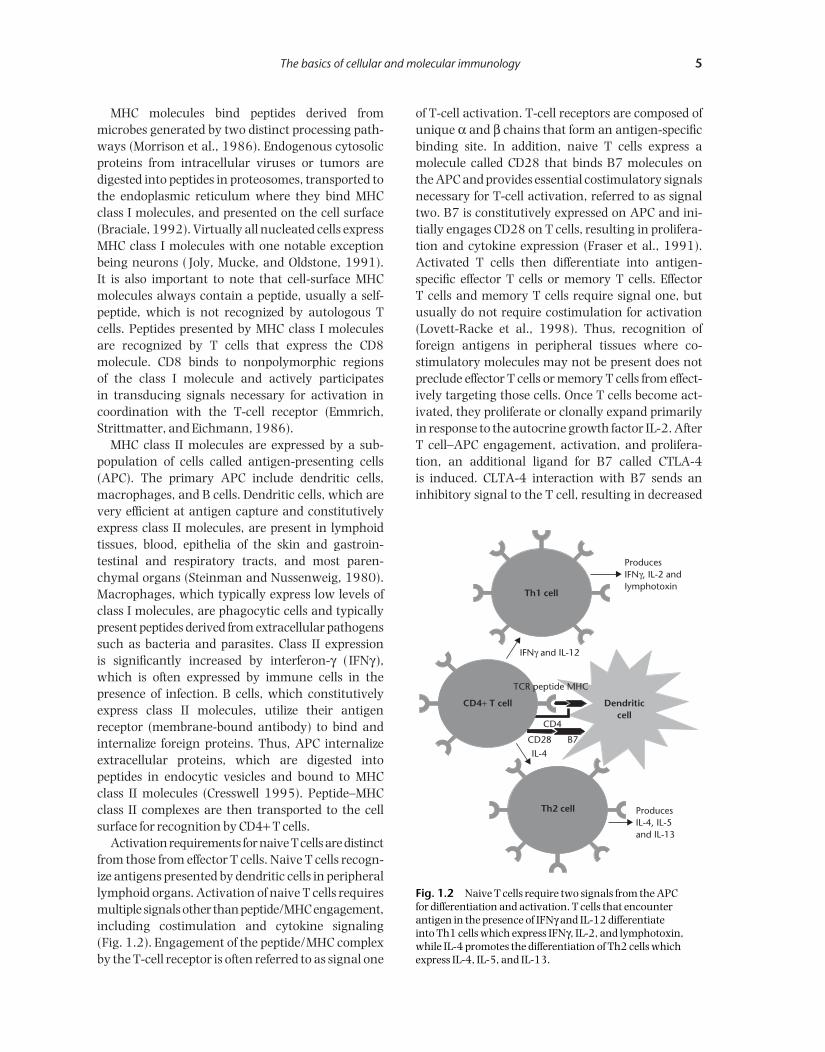
MHC class II molecules are expressed by a sub-population of cells called antigen-presenting cells(APC). The primary APC include dendritic cells,macrophages, and B cells. Dendritic cells, which arevery efficient at antigen capture and constitutivelyexpress class II molecules, are present in lymphoidtissues, blood, epithelia of the skin and gastroin-testinal and respiratory tracts, and most paren-chymal organs (Steinman and Nussenweig, 1980).Macrophages, which typically express low levels ofclass I molecules, are phagocytic cells and typicallypresent peptides derived from extracellular pathogenssuch as bacteria and parasites. Class II expression is significantly increased by interferon-γ ( IFNγ ),which is often expressed by immune cells in the presence of infection. B cells, which constitutivelyexpress class II molecules, utilize their antigen receptor (membrane-bound antibody) to bind andinternalize foreign proteins. Thus, APC internalizeextracellular proteins, which are digested into peptides in endocytic vesicles and bound to MHCclass II molecules (Cresswell 1995). Peptide–MHCclass II complexes are then transported to the cellsurface for recognition by CD4+ T cells.
Activation requirements for naive T cells are distinctfrom those from effector T cells. Naive T cells recogn-ize antigens presented by dendritic cells in peripherallymphoid organs. Activation of naive T cells requiresmultiple signals other than peptide/MHC engagement,including costimulation and cytokine signaling (Fig. 1.2). Engagement of the peptide/MHC complexby the T-cell receptor is often referred to as signal one
of T-cell activation. T-cell receptors are composed ofunique α and β chains that form an antigen-specificbinding site. In addition, naive T cells express amolecule called CD28 that binds B7 molecules on the APC and provides essential costimulatory signalsnecessary for T-cell activation, referred to as signaltwo. B7 is constitutively expressed on APC and ini-tially engages CD28 on T cells, resulting in prolifera-tion and cytokine expression (Fraser et al., 1991).Activated T cells then differentiate into antigen-specific effector T cells or memory T cells. Effector T cells and memory T cells require signal one, butusually do not require costimulation for activation(Lovett-Racke et al., 1998). Thus, recognition of foreign antigens in peripheral tissues where co-stimulatory molecules may not be present does notpreclude effector T cells or memory T cells from effect-ively targeting those cells. Once T cells become act-ivated, they proliferate or clonally expand primarilyin response to the autocrine growth factor IL-2. AfterT cell–APC engagement, activation, and prolifera-tion, an additional ligand for B7 called CTLA-4 is induced. CLTA-4 interaction with B7 sends aninhibitory signal to the T cell, resulting in decreased
ProducesIFNγ, IL-2 andIymphotoxin
ProducesIL-4, IL-5and IL-13
IL-4
CD4
CD28 B7
TCR peptide MHC
IFNγ and IL-12
Th2 cell
CD4+ T cell Dendriticcell
Th1 cell
Fig. 1.2 Naive T cells require two signals from the APC for differentiation and activation. T cells that encounterantigen in the presence of IFNγ and IL-12 differentiate into Th1 cells which express IFNγ, IL-2, and lymphotoxin,while IL-4 promotes the differentiation of Th2 cells whichexpress IL-4, IL-5, and IL-13.

6 AMY E. LOVETT-RACKE, ANNE R. GOCKE, AND PETRA D. CRAVENS
activation and return of the T cell to a resting state(Krummel and Allison, 1995).
The other critical factor in the differentiation ofnaive T cells is the cytokine milieu in which the naiveT cells are differentiated. CD4+ T cells are generallyclassified into T helper 1 (Th1) and T helper 2 (Th2)cells based on the cytokines that are expressed by the CD4+ T cells (Cherwinski et al., 1987) (Fig. 1.2).The cytokines expressed by CD4+ T cells are actuallydetermined by the cytokine present in the lymphoidtissue during the initial activation. IFNγ and IL-12,often expressed by APC and innate immune cells,direct the differentiation of Th1 cells, which subse-quently express IFNγ, IL-2, and lymphotoxin (Hsiehet al., 1993; Reynolds, Boom, and Abbas, 1987). Re-cognition of pathogens occurs partially through a set of evolutionarily conserved proteins, called toll-likereceptors (TLR), expressed by macrophages and othercells of the innate immune system. TLR recognizeconserved pathogen-associated molecular patters,generating proinflammatory signals that are criticalto the generation of an antigen-specific response.TLR signaling directly contributes to the cytokinesgenerated by the APC and therefore effects thecytokine milieu in which antigen-specific T cells dif-ferentiate. For example, TLR signaling that inducesthe expression of IFNγ and IL-12 would promote the development of Th1. Th1 cells express these pro-inflammatory cytokines, which are often associatedwith immune-mediated tissue damage. In contrast,IL-4 directs the differentiation of Th2 cells whichexpress IL-4, IL-5, IL-6, IL-10, and IL-13 (Swain et al.,1990). These anti-inflammatory cytokines expressedby Th2 cells can downregulate the effects of Th1cells. More recently, a small, yet distinct populationof CD4+ T cells that express IL-17 has been de-scribed. The requirement for the differentiation of thisT-cell population is still unclear, but it appears thatIL-23 plays a role in at least promoting the expansionof these T cells (Harrington et al., 2005; McKenzie,Kastelein, and Cua, 2006). CD4+ T cells primarilyprovide help to other immune cells by the cytokinesthat they express. For example, isotype switching ofIg genes is dependent on IL-4, which is primarilyexpressed by Th2 cells. Thus, B cells are very depend-ent on CD4+ T cells for antibody production.
Naive CD8+ T cells require the same three signals(T-cell receptor engagement, costimulation, andcytokine signaling) as CD4+ T cells for differentia-tion into cytotoxic T lymphocytes (CTL). Since mostnucleated cells express MHC class I molecules, CD8+T cells can differentiate in both the lymphoid tissue
and any peripheral tissue that express foreign ortumor antigens. CD4+ T cells often play a critical rolein CD8+ T-cell differentiation by producing cytokinesor activating APC via CD40–CD40L engagement,which subsequently stimulates CD8+ T cells. CD8+ Tcells mediate their effects by two primary mechanisms.CD8+ T cells can function as CTL in which cytoplasmicgranules containing perforin and granzymes arereleased by the CD8+ T cell upon T-cell receptorengagement resulting in the killing of the antigen-presenting cell (Masson and Tschopp, 1987). Inaddition, CD8+ T cells can produce cytokines, suchas IFNγ, lymphotoxin, and TNFα, which can activatephagocytes, increase inflammation, and alter the func-tion of other immune cells (Ramshaw et al., 1992).
Trafficking of lymphocytes is key to an effectiveimmune response. Chemokines play a central role in the recruitment of immune cells to the site of infection. Chemokines up-regulate expression ofadhesion molecules on the vascular endothelium,which are necessary for lymphocytes to enter tissueswhen directed by chemotactic signals. The CNS entryof activated lymphocytes, monocytes, and dendriticcells positive for distinct sets of chemokine receptorsis also controlled by a gradient of correspondingchemokines between the CNS and the peripheral circulation. The intervening blood–brain barrier is composed of cerebrovascular endothelial cells, pericytes, and astrocytic processes (Carlson et al.,2006). This multifunctional complex structure isinvolved in the regulation of cell trafficking and thedevelopment of CNS autoimmunity (see Chapter 3).
Lymphocyte maturation and immunogenetics
Lymphocytes arise from pluripotent stem cells in the bone marrow. Early lymphocyte maturation is dependent on rapid proliferation of lymphocyte progenitors promoted by IL-7 (Peschon et al., 1994).The generation of large numbers of immature lym-phocytes provides a sizable group of cells with a highlydiverse repertoire of antigen receptors necessary toprotect the host from diverse pathogens. The diverserepertoire of antigen receptors for both B and T cellsis generated by somatic recombination, also termedgenetic rearrangement (Okada and Alt, 1994).Human B cell receptor genes are located on three different chromosomes: the heavy chain locus is onchromosome 14; the κ light chain is on chromosome2; and the λ light chain is on chromosome 22. Eachlocus contains a set of V (variable) genes, J ( joining)genes, and C (constant) genes. In addition, the heavy

The basics of cellular and molecular immunology 7
gene locus contains D (diversity) genes. The numberof V, D, and J genes varies between loci and species.For example, the V region of the heavy chain ofhuman B cells contains approximately 45 genes,while the Vκ locus contains about 35 genes and theVλ locus contains about 30 genes. Although all cellshave these loci, these germline genes are not tran-scribed into messages that encode antigen receptors.In B cells, a gene from each V, (D), and J region isjoined by somatic recombination, involving double-strand DNA breaks within the V, (D), and J regions,and ligating these segments together such that a single V, (D), and J gene form a single exon capable ofbeing transcribed. This V–(D)–J gene codes for theantigen-binding site of antibodies. The diversity of B cell antigen receptors is created by the multiple V,(D), and J genes which can potentially combine, theadditions or deletions of nucleotides that can occurduring ligation of V, (D), and J genes; somatic muta-tions within recombined V–(D)–J segments that canoccur following B-cell activation; and antigen receptorediting in which a B cell may select a new light chainto pair with an existing heavy chain. Immature Bcells that express an antigen receptor then undergo aprocess of negative selection in the bone marrow inwhich B cells with antigen receptors specific for self-proteins are deleted or fail to mature (Grandien et al.,1994). These nonself-reactive B cells then migrateinto the periphery where they are capable of recog-nizing and responding to foreign proteins.
Maturation of T cells and development of the T-cellreceptor is quite similar to B cells. T-cell precursorsare derived from stem cells in the bone marrow or fetal liver and migrate to the thymus where thesethymocytes proliferate and undergo somatic recom-bination. The germline configuration of T-cell re-ceptor genes is similar to B-cell receptor genes. T-cellreceptors can form from the pairing of an α and βchain or a γ and δ chain, with αβ T-cell receptorsexpressing significantly more diversity and beingexpressed by the majority of T cells (Kronenberg et al.,1986). The α, δ locus is located on chromosome 14,the β locus is on chromosome 7, and the γ locus is onchromosome 7. The α and γ loci contain multiple Vand J genes, while the β and δ genes also include a set of D genes. The recombination of V–(D)–J geneswithin thymocytes results in a unique T-cell receptorgene for each T cell. The diversity of T-cell receptorsresults from combinatorial and junctional diver-sity similar to that observed in B cells, but somaticmutations and receptor editing have not been observedin T cells. Thymocytes with a T-cell receptor that
recognize self-MHC are stimulated to survive andthus positively selected (Pardoll and Carerra, 1992).Subsequently, thymocytes that have a T-cell receptorthat strongly recognizes self-peptides are programmedto die and thus negatively selected. Therefore, thehost’s T cells only recognize peptides in the context of self-MHC and potentially autoreactive T cells areeliminated in the thymus. Mature T cells exit the thymus and migrate to lymphoid tissues, where theyawait the encounter with antigen-laden APC.
Immune privilege, tolerance, andautoimmunity
There are several sites in the body, called immuno-logically privileged sites, in which normal immuneresponses are not typically elicited. Immune privilegewas originally described when tissue grafts placed in some areas of the body failed to elicit an immuneresponse and consequently were not rejected. Im-munologically privileged sites include the brain, eye,testis, and uterus. The brain has several features thatnormally protect it from immune-mediated damage(Steilein, 1993). First, there is limited lymphatic drain-age from the brain. Second, there is a blood–brainbarrier established by vascular endothelium cellsthat form tight junctions, preventing the transport ofmost cells and proteins into the brain. Third, there islimited expression of MHC molecules in the brain,reducing the possibility that T cells can become activated in the brain.
Interestingly, antigens sequestered in immunologic-ally privileged sites may be the target of autoimmunediseases. For example, experimental autoimmuneencephalomyelitis, a model for multiple sclerosis, isinduced by immunization with myelin proteins andthe disease can be transferred to naive recipients by transfer of myelin-specific T cells (Martin andMcFarland, 1995). In addition, both healthy indi-viduals and multiple sclerosis patients have myelin-specific T cells, but the activation state of these T cells is different (Lovett-Racke et al., 1998). Thus,it appears that autoreactive T cells are not com-pletely eliminated in the thymus during negativeselection. The failure to delete some autoreactive T cells may be due to low avidity T-cell receptors on these cells or minimal expression of some self-peptides in the thymus during T-cell maturation.
The realization that all individuals have T cellsthat recognize self-peptides has led to the discoverythat T-cell tolerance is critical to limiting autoim-mune disease. Central tolerance is the phenomenon

8 AMY E. LOVETT-RACKE, ANNE R. GOCKE, AND PETRA D. CRAVENS
described above in which self-reactive T cells aredeleted in the thymus during maturation. Peripheraltolerance is obtained through several mechanisms.Naive CD4+ T cells, which normally require both T-cell receptor-peptide/MHC engagement and costi-mulation for activation, can become anergic (unre-sponsive to antigen) if they engage peptide/MHC inthe absence of costimulation (Gimmi et al., 1993).Since peripheral antigen-presenting cells express few, if any, costimulatory molecules in the absenceof infection, autoreactive T cells may commonlyengage self-peptide/MHC complexes in the absenceof costimulation in the periphery, resulting in clonalanergy. T cells may also become tolerant in the peri-phery if the T cell expresses CTLA-4, the inhibitoryreceptor for B7, at the time of T-cell receptor engage-ment (Perez et al., 1997). Since CTLA-4 binds B7with a higher affinity, autoreactive T cells that expresslow levels of B7 may preferentially bind CTLA-4 andbecome anergic. It has recently been postulated thatregulatory T cells, defined as CD4+CD25+Foxp3+T cells, induce tolerance by blocking the functionand activation of effector T cells. Mutation in thehuman Foxp3 gene results in multisystem auto-immune disease, suggesting that the regulatory Tcells are critical for self-tolerance (Patel, 2001).
It is speculated that infections may play a criticalrole in the loss of self-tolerance and the onset ofautoimmunity. Infections can induce the expressionof costimulatory molecules on cells presenting self-proteins. Thus, peripheral antigen-presenting cells,once incapable of activating self-reactive T cells, maynow be capable of eliciting a destructive immuneresponse against self-tissues. This is supported by theobservation that mice with a transgenic T-cell recep-tor for myelin basic protein usually remain healthyin a pathogen-free environment, but frequentlydevelop spontaneous experimental autoimmuneencephalomyelitis in a conventional environment(Goverman et al., 1993). Another mechanism bywhich infections may trigger autoimmunity ismolecular mimicry (Fujinami and Oldstone, 1985).Pathogens induce the activation of T cells and B cellsthat may have antigen receptors that can cross-reactwith self-proteins. As a result, T cells and antibodiesoriginally expanded by recognition of a foreign protein may target and destroy self-tissues.
Summary
The immune system is designed to protect the hostfrom pathogens and tumors. The diversity of the
antibody and T-cell repertoire and the selection process that occurs during lymphocyte maturationensures that the immune system is capable of recog-nizing and responding to the vast array of potentialmicrobes with minimal damage to the host. How-ever, this does not preclude the possibility that somehosts harbor lymphocytes that may inadvertentlyrecognize self-proteins under some circumstances.Our increasing understanding of lymphocyte matura-tion, selection, activation, and tolerance will provideinsight into the understanding of immune-mediateddiseases and potential therapeutic interventions.
References
Braciale, T.J. 1992. Antigen processing for presenta-tion by MHC class I molecules. Curr Opin Immunol,4, 59–62.
Carlson, M.J., Doose, J.M., Melchior, B., Schmid, C.D.and Ploix, C.C. 2006. CNS immune privilege is not immune isolation. Immunol Rev, 213,48–65.
Cherwinski, H.M., Schumacher, J.H., Brown, K.D. andMosmann, T.R. 1987. Two types of mouse helper T cell clone. III. Further differences in lymphokinesynthesis between Th1 and Th2 clones revealed by RNA hybridization, functionally monospecificbioassays, and monoclonal antibodies. J Exp Med,166, 1229–44.
Cresswell, P. 1995. Assembly, transport and functionof MHC class II molecules. Ann Rev Immunol, 12,259–93.
Edelman, G.M., Cunningham, B.A., Gall, W.E., Gottlieb,P.D., Rutihauser, U. and Waxdal, M.J. 1969. Thecovalent structure of an entire gamma G immuno-globulin molecule. Proc Natl Acad Sci USA, 63,78–85.
Emmrich, F., Strittmatter, U. and Eichmann, K. 1986.Synergism in the activation of human CD8 T cells bycross-linking the T-cell receptor complex with theCD8 differentiation antigen. Proc Natl Acad Sci USA,83, 8298–302.
Fraser, J.D., Irving, B.A., Grabtree, G.R. and Weiss, A.1991. Regulation of interleukin-2 gene enhanceractivity by the T-cell accessory molecule CD28.Science, 251, 313–16.
Fujinami, R.S. and Oldstone, M.B. 1985. Amino acid homology between the encephalitogenic site of myelin basic protein and virus: Mechanism forautoimmunity. Science, 230, 1043–5.
Gimmi, C.D., Freeman, G.J., Gribben, J.G., Gray, G. andNadler, L.M. 1993. Human T-cell clonal anergy is induced by antigen presentation in the absence of B7 costimulation. Proc Natl Acad Sci USA, 90,6586–90.
Gounni, A.S., Lamkhioued, B., Ochiai, K. et al. 1984. High-affinity IgE receptor on eosinophils is
The basics of cellular and molecular immunology 9
involved in defense against parasites. Nature, 367,183–6.
Goverman, J., Woods, A., Larson, L., Weiner, L.P.,Hood, L. and Zaller, D.M. 1993. Transgenic mice that express a myelin basic protein-specific T cellreceptor develop spontaneous autoimmunity. Cell,72, 551–60.
Grandien, A., Modigliani, Y., Freitas, A., Andersson, J.and Coutinho, A. 1994. Mechanisms that controlantigen receptor variable region gene assembly.Semin Immunol, 6, 185–96.
Harrington, L.E., Hatton, R.D., Mangan, P.R. et al.2005. Interleukin 17-producing CD4+ effector Tcells develop via a lineage distinct from the T helpertype 1 and 2 lineages. Nat Immunol, 6, 1123–32.
Hilschman, N. and Craig, L.C. 1969. Amino acidsequence studies with Bence–Jones proteins. ProcNatl Acad Sci USA, 53, 1403–9.
Hsieh, C.S., Macatonia, S.E., Tripp, C.S., Wolf, S.F.,O’Garra, A. and Murphy, K.M. 1993. Developmentof TH1 CD4+ T cells through IL-12 produced byListeria-induced macrophages. Science, 260, 547–9.
Joly, E., Mucke, L. and Oldstone, M.B. 1991. Viral persistence in neurons explained by lack of major histocompatibility class I expression. Science, 253,1283–5.
Kataoka, T., Kawakawi, T., Takahashi, N. and Honjo, T. 1980. Rearrangement of the immuno-globulin γ1-chain gene and mechanism for heavy-chain class switch. Proc Natl Acad Sci USA, 77,919–23.
Kronenberg, M., Siu, G., Hood, L.E. and Shastri, N.1986. The molecular genetics of the T-cell antigenreceptor and T-cell antigen recognition. Annu RevImmunol, 4, 529–91.
Krummel, M.F. and Allison, J.P. 1995. CD28 andCTLA-4 have opposing effects on the response of T cells to stimulation. J Exp Med, 182, 459–65.
Leijh, P.C., van den Barselaar, M.T., Daha, M.R. and van Furth, R. 1981. Participation of immuno-globulins and complement components in the intracellular killing of Staphylococcus aureus andEscherichia coli by human granulocytes. Infect Immun,33, 714–24.
Lovett-Racke, A.E., Trotter, J.L., Lauber, J., Perrin, P.J.,June, C.H. and Racke, M.K. 1998. Myelin basic protein-reactive T cells are less dependent on CD28-mediated costimulation in multiple sclerosispatients: A marker of activation/memory T cells. J Clin Invest, 101, 725–30.
Maloney, D.G., Grillo-López, A.J., White, C.A. et al.1997. IDEC-C2B8 (Rituximab) anti-CD20 mono-clonal antibody therapy in patients with relapsed low-grade non-Hodgkin’s lymphoma. Blood, 90,2188–95.
Martin, R. and McFarland, H.F. 1995. Immunologicalaspects of experimental allergic encephalomyelitisand multiple sclerosis. Crit Rev Clin Lab Sci, 32,121–82.
Masson, D. and Tschopp, J. 1987. A family of serineesterases in lytic granules of cytolytic T lymphocytes.Cell, 49, 679–85.
McKenzie, B.S., Kastelein, R.A. and Cua, D.J. 2006.Understanding the IL-23-IL-17 immune pathway.Trends Immunol, 27, 17–23.
Miller, D.H., Khan, O.A., Sheremata, W.A. et al., andthe International Natalizumab Multiple SclerosisTrial Group. 2003. A controlled trial of Natalizumabfor relapsing multiple sclerosis. N Engl J Med, 348,15–23.
Morrison, L.A., Lukacher, A.E., Braciale, V.L., Fan, D.P.and Craciale, T.J. 1986. Differences in antigen presentation to MHC class 1 and class II-restrictedinfluenza virus-specific cytolytic T-lymphocyte clones.J Exp Med, 163, 903–21.
Okada, A. and Alt, F.W. 1994. Mechanisms that con-trol antigen receptor variable region gene assembly.Semin Immunol, 6, 185–96.
Pardoll, D. and Carerra, A. 1992. Thymic selection.Curr Opin Immunol, 4, 162–5.
Patel, D.D. 2001. Escape from tolerance in the humanX-linked autoimmunity-allergic disregulation syn-drome and the Scurfy mouse. J Clin Invest, 107,155–7.
Perez, V.L., van Parijs, L., Biuckians, A., Zheng, X.X.,Strom, T.B. and Abbas, A.K. 1997. Induction ofperipheral T cell tolerance in vivo requires CTLA-4engagement. Immunity, 6, 411–17.
Peschon, J.J., Morrissey, P.J., Grabstein, K.H. et al.1994. Early lymphocyte expansion is severelyimpaired in interleukin 7 receptor-deficient mice. J Exp Med, 180, 1955–60.
Ramshaw, I., Ruby, J., Ramsay, A., Ada, G. andKarupiah, G. 1992. Expression of cytokines byrecombinant vaccinia viruses: A model for studyingcytokines in viral infections in vivo. Immunol Rev,127, 157–82.
Reynolds, D.S., Boom, W.H. and Abbas, A.K. 1987.Inhibition of B lymphocyte activation by interferon-gamma. J Immunol, 139, 767–73.
Schleimer, R.P., MacGlashan, D.W., Petters, S.P.,Pinchard, R.N., Adkinson, N.F. and Lichtenstein,L.M. 1986. Characterization of inflammatory medi-ator release from purified human lung mast cells.Ann Rev Resp Dis, 133, 614–17.
South, M.A., Cooper, M.D., Wollheim, F.A., Hong, R.and Good, R.A. 1966. The IgA system. I. Studies ofthe transport and immunochemistry of IgA in thesaliva. J Exp Med, 123, 615–27.
Steinman, R.M. and Nussenweig, M.C. 1980. Dendriticcells: features and functions. Immunol Rev, 53,127–47.
Steilein, J.W. 1993. Immune privilege as the result oflocal tissue barriers and immunosuppressive micro-environments. Curr Opin Immunol, 5, 428–32.
Swain, S.L., Weinberg, A.D., English, M. and Huston, G.1990. IL-4 directs the development of Th2-likehelper effectors. J Immunol, 145, 3796–806.

10 AMY E. LOVETT-RACKE, ANNE R. GOCKE, AND PETRA D. CRAVENS
Uhr, J.W. and Finkelstein, M.S. 1963. Antibody forma-tion. IV. Formation of rapidly and slowly sediment-ing antibodies and immunological memory to bacteriophage phi-X 174. J Exp Med, 117, 457–77.
Wu, T.T. and Kabat, E.A. 1970. An analysis of thesequences of the variable regions of the Bence–Jones proteins and myeloma light chain and their
implications for antibody complementarity. J ExpMed, 132, 211–50.
Yednock, T.A., Cannon, C., Fritz, L.C., Sanchez-Madrid,F., Steinman, L. and Karin, N. 1992. Prevention ofexperimental autoimmune encephalomyelitis byantibodies against alpha 4 beta 1 integrin. Nature,356, 63–6.

Introduction
Insulation of large diameter axons by supporting glia in the nervous system is a feat of evolution thathas appeared independently at least three times(Waehneldt, 1990): in worms (Annelida), in crusta-ceans (Crustacea), and in terrestrial and some marinevertebrates (Gnathostomata). Although each of theseincarnations has yielded insulation with distinctmorphologies, the critical feature in each instance isa multilayered cellular sheath that confers high-speedneural transmission, enables large reductions inenergy expenditure, and allows for compaction ofthe nervous system. In vertebrates, this insulationtakes the form of the myelin sheath, which is a verystable lipid-rich membrane that is wrapped aroundsegments of larger diameter axons in the central nervous system (CNS) and peripheral nervous system(PNS) and some dendrites.
In its native state, the myelinated axon is oftendescriptively likened to link-sausage in lay terms; thesausage portions being analogous to myelin sheathsand the knots in between analogous to short bareregions of the axon, which are called nodes of Ranvier(sites of sodium channel clustering for neural trans-mission). However, myelin sheaths are not simplyblobs of fatty substance along the axon but, rather,are large specialized flattened membrane domainsthat are spirally wrapped around segments of axons,as illustrated in Fig. 2.1 for a CNS myelin sheath. Infurther contrast to the humble sausage, myelin sheathsare by no means amorphous or uniform membranesbut are highly organized and compartmentalized.
At the ultrastructural level, the vertebrate myelinsheath has a very distinct organization. A flattened,cytoplasm-containing membrane process from amyelinating cell contacts and expands radially andlongitudinally around an axon, loosely enveloping it in a manner analogous to rolling up a newspaper.The membrane then compacts to tighten around theaxon and extrude the cytoplasm. During this process,cytoplasmic membrane surfaces become juxtaposed
and appear to fuse together. In electron micrographs,these fused surfaces are darkly stained by lead saltsand the spiral line is known as the major dense line.The extracellular surfaces of the membrane alsobecome juxtaposed; however, these surfaces do notfuse but, rather, maintain a discrete distance to formthe minor dense line.
Myelinating oligodendrocytes and Schwann cells
Myelin sheaths elaborated by oligodendrocytes inthe CNS and Schwann cells in the PNS share similarorganizations and serve the same functions (Arroyoand Scherer, 2000). Typically, axons are small caliberin the CNS and myelin sheaths may reach 500 μmin length with 50–100 lamellae. In the PNS, myelinsheaths may be over 1000 μm in length and com-prise 200 or so lamellae. There is a linear relation-ship between the diameter of an axon and the size ofthe myelin sheath. In the CNS and PNS, axons mustexceed minimum diameters to be myelinated, whichare approximately 0.5 μm and 1 μm, respectively.
Several features distinguish CNS and PNS myelin:a Schwann cell establishes a one-to-one relation-ship around a segment of a single axon while mostoligodendrocytes synthesize and maintain multiplemyelin sheaths around a number of nearby axons,perhaps as many as 50; a Schwann cell synthesizes a collagenous basement membrane around the out-side of the cell to form a tube, oligodendrocytes donot; in the event of axonal transection in the PNS,axons usually regrow through the original basementmembrane tube and are reinvested by Schwann cells and remyelinated; in the CNS transected axonsgenerally do not regrow.
Major functions of myelin
A major function of the myelin sheath is to electric-ally insulate a segment of axon. In this regard, myelinis analogous to the coating around the outside of
2
Major components of myelin in the mammalian central and peripheral nervous systems
Alexander Gow
12 ALEXANDER GOW
copper wires in underground cables that supply asuburb with electricity. Shielding the conductivefiber (copper wire or axon) dramatically reduces current dissipation to the environment and isolatesthe signal from interfering with signals in other conductive fibers.
In similar fashion to an underground cable, electrical signals traveling along an axon (actionpotentials) must be boosted at regular distances to maintain signal strength and integrity. This isachieved for the underground cable using step-uptransformers at relay stations. In the axon, boostingthe signal is achieved at nodes of Ranvier betweenthe myelin sheaths. In these regions of an axon, voltage-sensitive sodium channels are clustered at
high density and open when they detect an approach-ing action potential. The current that flows into theaxon through these ion channels is greater than that flowing along the axon; thus, depolarization at nodes of Ranvier boosts the signal and propag-ates it toward the nerve terminal. After an actionpotential has passed through a region of the axon,ATPases in the axonal membrane must pump outthe sodium ions that entered through the channelsand repolarize the axon in preparation for the nextaction potential.
There are several advantages conferred on neuralcommunication by myelin that are pivotal to thesuccess of the insulated nervous system. First, myelinenables an electrical signal to travel along the axon
InnerLoop
TightJunctions
Axon JP Paranode
Cyt.
Node ofRanvier
AxoglialJunction
CompactMyelin
Axon
TightJunctions
Paranode
B C
A
Internode Paranode
Node ofRanvier
Node ofRanvier
JP JPAxon
ParanodalTight Junction
InternodalTight Junction
CompactMyelin
OuterLoop
ParanodalLoop
AxoglialJunction
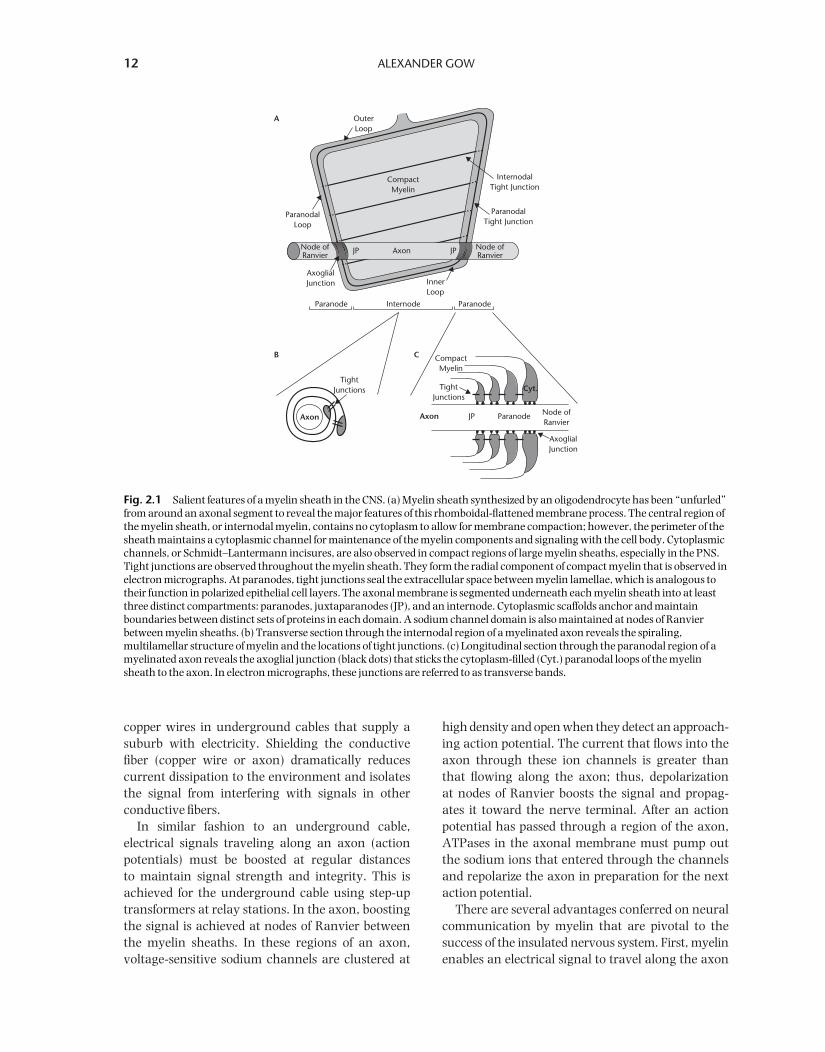
Fig. 2.1 Salient features of a myelin sheath in the CNS. (a) Myelin sheath synthesized by an oligodendrocyte has been “unfurled”from around an axonal segment to reveal the major features of this rhomboidal-flattened membrane process. The central region ofthe myelin sheath, or internodal myelin, contains no cytoplasm to allow for membrane compaction; however, the perimeter of thesheath maintains a cytoplasmic channel for maintenance of the myelin components and signaling with the cell body. Cytoplasmicchannels, or Schmidt–Lantermann incisures, are also observed in compact regions of large myelin sheaths, especially in the PNS.Tight junctions are observed throughout the myelin sheath. They form the radial component of compact myelin that is observed inelectron micrographs. At paranodes, tight junctions seal the extracellular space between myelin lamellae, which is analogous totheir function in polarized epithelial cell layers. The axonal membrane is segmented underneath each myelin sheath into at leastthree distinct compartments: paranodes, juxtaparanodes (JP), and an internode. Cytoplasmic scaffolds anchor and maintainboundaries between distinct sets of proteins in each domain. A sodium channel domain is also maintained at nodes of Ranvierbetween myelin sheaths. (b) Transverse section through the internodal region of a myelinated axon reveals the spiraling,multilamellar structure of myelin and the locations of tight junctions. (c) Longitudinal section through the paranodal region of amyelinated axon reveals the axoglial junction (black dots) that sticks the cytoplasm-filled (Cyt.) paranodal loops of the myelinsheath to the axon. In electron micrographs, these junctions are referred to as transverse bands.

Major components of myelin in the mammalian CNS and PNS 13
approximately 10 times faster than it would in anunmyelinated axon of similar size; thus, animals canrespond to their environment very rapidly. Further-more, axons can be of smaller diameter and still con-duct signals rapidly which enables miniaturizationof the nervous system or enhancement of its com-plexity by increasing the number of axons. Second,myelin dramatically reduces energy consumption.Membrane depolarization/repolarization is an energy-intensive process that, in an unmyelinated axon,occurs along its entire length as the action potentialmoves like a wave to the nerve terminal; however,myelin limits depolarization to nodes of Ranvier as theaction potential jumps from node to node (saltatoryconduction) and only small regions of the axon needto be repolarized.
Diseases of myelin
In neurodegenerative disease states myelin sheathscan be direct or indirect targets, which renders vulnerable the critical communication networks inthe CNS and between the nervous system and thebody. Certain regions of the myelin sheath are moresensitive to damage than others. The myelin paranodeis particularly sensitive because it compartmentalizesthe axonal membrane to cluster sodium channels at the node and potassium channels at the juxta-paranode, by means of the axoglial junction. Actionpotentials are slowed or may even fail to reach thenerve terminal (conduction block) if this compart-mentalization is compromised. In contrast, inter-nodal myelin is relatively resilient and can enablenear normal conduction velocity with only a frac-tion of the normal number of lamellae around eachsegment of the axon.
Although genetic diseases of myelin may damagespecific regions of myelin sheaths, diseases involvingthe immune system such as multiple sclerosis orGuillain–Barré syndrome usually damage large regionsof the nervous system containing hundreds or thous-ands of myelin sheaths and it is unlikely that thedestruction will be localized to specific regions of thesesheaths. Nonetheless, it is instructive to understandthat myelin repair will be ineffective unless myelinparanodes can reestablish compartmentalization.
In the event that axons are transected during thedisease process, the CNS and PNS respond very differ-ently. In the PNS, myelin sheaths around degener-ating axons are cleared by macrophages and the proximal axon stumps sprout neurites which growout to reinnervate their targets. In the CNS, axonal
regrowth is very limited and is potently inhibited by several components of myelin sheaths that particip-ate in the Nogo ligand–receptor complex.
To serve as a guide to molecular components ofthe myelinated axon, I describe general features ofthe major proteins and lipids that comprise myelinsheaths in the CNS and PNS as well as importantneuronal proteins with which the myelin proteinsinteract. In addition, I briefly touch on transcriptionalregulation of myelin genes and provide some discus-sion aimed at dispelling the notion of the myelinsheath as an immune-privileged compartment.
Internodal proteins
CD9
Located on the short arm of chromosome 12 inhumans (12p13) and on chromosome 6 in mice (6 F2), the CD9 gene yields a single transcript(Boucheix et al., 1991).
CD9 is a polytopic membrane glycoprotein withfour putative transmembrane domains and the aminoand carboxyl termini exposed to the cytoplasm. Thisprotein was initially recognized as an abundant pro-tein on the surface of developing B lymphocytes andplatelets but is not required for development of thesecell types. The protein is expressed by differentiatedSchwann cells and its gene is regulated by the pre-sence of axons in vitro and in vivo in similar fashion toother myelin genes (Banerjee and Patterson, 1995).CD9 is also expressed by oligodendrocytes and local-ized to myelin paranodes in the CNS (Ishibashi et al.,2004; Nakamura, Iwamoto, and Mekada, 1996).
CD9 has been associated with a number of functions. It is the receptor for pregnancy-specific glycoprotein-17 in mice (Waterhouse, Ha, andDveksler, 2002). CD9 functions in concert with CD81and integrin-α6β1 to regulate sperm–egg fusion (Le Naour et al., 2000; Miyado et al., 2000) and alsoappears to interact with this integrin in myelinatingcells. Female knockout mice exhibit reduced fertilityand both males and females exhibit mild paranodalpathology in the CNS and PNS where axoglial junc-tions of some paranodes are partially disrupted andimportant paranodal components including Casprand NF155 are mislocalized ( Ishibashi et al., 2004).
Myelin associated glycoprotein, MAG
Located on the long arm of chromosome 19 inhumans (19q13.1) and on chromosome 7 in mice

14 ALEXANDER GOW
(7 B1), MAG is alternatively spliced at the mutu-ally exclusive exons 2 and 12, which yield the protein isoforms S-MAG and L-MAG, respectively(Schachner and Bartsch, 2000).
MAG is a member of the immunoglobulin super-family (IgSF) and is one of the earliest proteins to beinserted into the myelin membrane during develop-ment. This glycoprotein is localized to the inner loopin mature myelin where it can interact with surfacelipids or proteins from the axon. One such interact-ing protein is the Nogo-66 receptor (NgR), which ispresent at the axolemma and in neurites. MAG is one of a number of myelin proteins that are involvedin suppressing axonal outgrowth in the CNS, pos-sibly through its interaction with the Nogo receptoron the surface of growth cones (Hunt, Coffin, andAnderson, 2002).
Deletion of the MAG gene in mice causes a subtlelate-onset phenotype in the CNS characterized bydelayed myelin sheath formation (Bartsch et al.,1997; Li et al., 1994; Li et al., 1998; Montag et al.,1994). The PNS is also abnormal in MAG-null micewith tomaculae forming in some myelin sheathsshortly after birth and increasing in frequency withage, which suggests that MAG may regulate axonalcaliber, at least in the PNS (Cai et al., 2002; Yin et al.,1998).
Myelin basic protein, MBP
Located on the long arm of chromosome 18 inhumans (18q23) and on chromosome 18 in mice(18 E2-E4), the MBP gene is alternatively spliced at exons 2, 5, and 6 and gives rise to five major isoforms (de Ferra et al., 1985; Newman, Kitamura,and Campagnoni, 1987; Takahashi et al., 1985). Inaddition, several promoters are known for MBP; thecanonical promoter used by myelinating oligoden-drocytes and two upstream promoters that give riseto multiple Golli-forms of MBP by alternative splicing(Campagnoni et al., 1993).
MBP is the second most abundant protein in CNSmyelin and comprises approximately 35% of totalprotein by weight (Braun, 1984). MBP is an extrinsicmembrane protein which is bound to the cyto-plasmic surfaces of the myelin membrane and may serve as an electrostatic adhesive to form the majordense line of compact myelin (Omlin et al., 1982).The protein has a high content of positive chargedamino acids and exhibits very little higher-orderedstructure even when purified under non-denaturingconditions (Gow and Smith, 1989) and binds very
strongly to the headgroups of negatively chargedlipids (Smith, 1992).
The absence of the MBP gene in naturally occur-ring mutant mice, shiverer and mld, causes severedisease from an early age which is characterized bywhole-body intention tremors and an inability tocompact CNS myelin to form the major dense line( Jacobs, 2005). MBP appears to play a similar role inPNS myelin (Martini et al., 1995a), although this is aminor role because of its low abundance and thepresence of the MPZ protein (Giese et al., 1992;Martini et al., 1995a).
The functions of Golli-MBP proteins have alsobeen characterized in some detail. These proteins are not only expressed by oligodendrocytes, but alsoby neurons and in lymphoid tissue during develop-ment and autoimmune disease (MacKenzie, Ghabriel,and Allt, 1984; Pribyl et al., 1993). These proteinsare localized to cell nuclei (Landry et al., 1996) and negatively regulate Ca2+-mediated signal trans-duction in T-lymphocytes (Feng et al., 2004) andoligodendrocytes ( Jacobs et al., 2005). Golli-nullmice have a subtle phenotype characterized by re-gional hypomyelination and delayed myelination in the CNS.
Myelin-associated oligodendrocyte basic protein, MOBP
Located on the short arm of chromosome 3 in humans(3p22.1) and on chromosome 9 in mice (9 F4), theMOBP gene yields at least five isoforms by altern-ative splicing, with all isoforms sharing a commonamino terminus (Holz et al., 1996; McCallion et al.,1999; Yamamoto et al., 1994).
MOBP isoforms are small soluble proteins expressedat high levels by oligodendrocytes that are incor-porated into compact myelin. Interestingly, one ofthe MOBP isoforms (MOBP155) includes tandemrepeats of a proline-rich domain, suggesting it mayinteract with other proteins (Yamamoto et al., 1994).The gene is not expressed by Schwann cells. Similarto MBP, MOBP has an unusually high proportion ofpositively charged amino acids in its primary struc-ture and is hypothesized to function at the majordense line (Yamamoto et al., 1994). Indeed, dele-tion of the MOBP gene in mice renders the myelinultrastructure less stable to organic solvents thanwild-type controls (Yamamoto et al., 1999). In addition, the organization of tight junctions in themutant myelin appears to be partially disrupted.However, this disruption does not cause a behavioral