neurodegeneration · glutathione pharmacokinetics •glutathione itself would need to be...
TRANSCRIPT
Neurodegeneration Eric Marsden ND
Lesson Outcomes
• Understand the role environment in aging and neurodegenerative diseases like: • Parkinson’s Disease • Alzheimer's Disease • Senile dementias
• Understand how to implement IV Therapeutics in the care of patients with neurodegenerative disorders using: • Glutathione • Alpha Lipoic Acid • Phosphatidylcholine
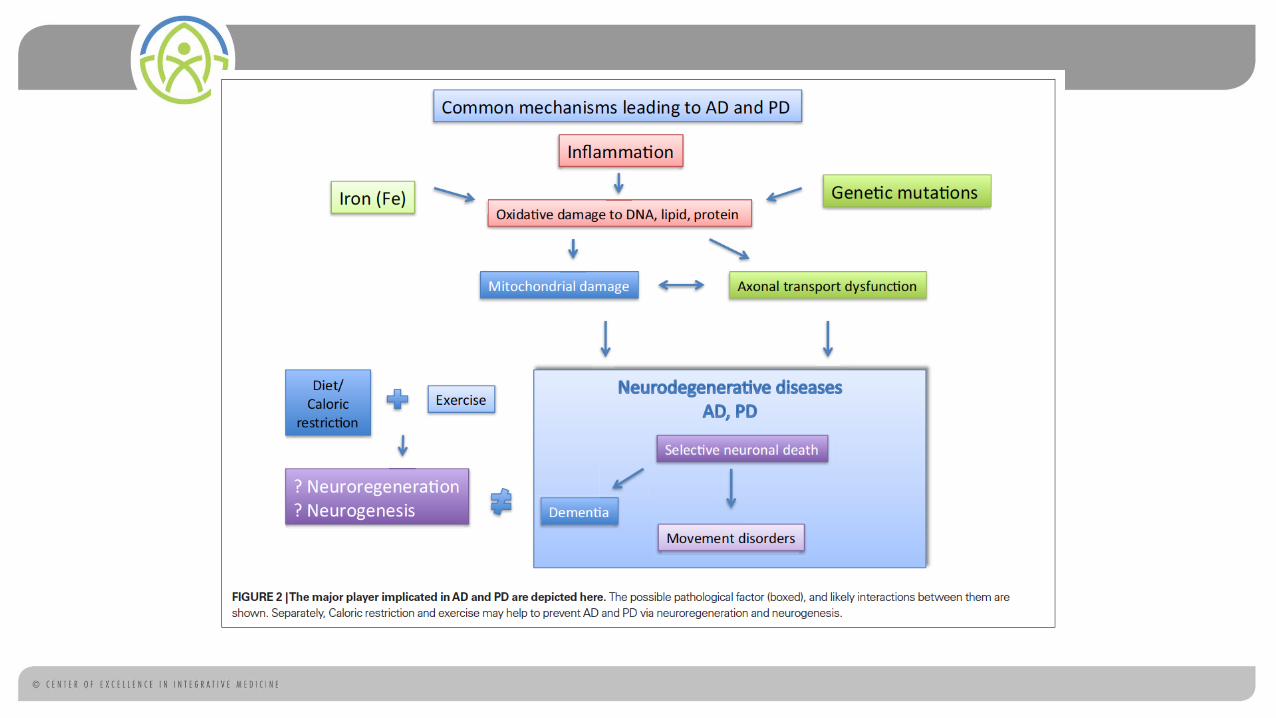
Role of Environment in Neurodegenerative Disorders (NDDs) • Multiple studies have pointed to the role of transition metals like Iron,
copper and manganese along with the toxic metals like mercury and lead in NDDs
• The strongest association is lead
• Past exposure to chlorinated pesticides is also significantly associated with NDDs
• These environmental contaminants have a common effect at increasing ROS in the brain and reducing glutathione levels
Diagnostics Important in Determining Potential Environmental Factors • Random and provoked assessments for determination of heavy metal
exposure and accumulation
• Toxic profiles for chlorinated pesticides may be insufficient to identify impacts as some are not persistent or expressed in serum in low level chronic exposure situations • Detailed exposure history is necessary
Glutathione
Glutathione in NDD (Parkinson’s Disease, Alzheimer’s, ALS) • The role of ROS in NDDs is well documented along with a resulting
reduction in mitochondrial glutathione
• This is a hallmark of almost all NDDs
• All of the previously mentioned environmental factors in NDDs exert their effect through this mechanism
• Conventional therapeutics are primarily aimed at increasing neuropeptides but not at the actual degenerative trends

Glutathione’s role in PD
Glutathione Pharmacokinetics
• Glutathione itself would need to be administered at a loading dose of 1.69 g/kg in order to have a significant effect on acute ROS injury if it was not further metabolized
• Glutathione given to healthy subjects is rapidly metabolized (1/2 life ~10 minutes) to cysteine and methionine with each of these having a further half life of 30 minutes
• Each of these constituents can reduce ROS intracellularly
• Glutathione along with cysteine and methionine are capable of passing the blood brain barrier
Ramifications of glutathione pharmacokinetics • For the purposes of NDDs where therapeutic agents have restricted
active transport mechanisms for BBB • Glutathione must be given in high doses
• Repeatedly over a short period of time
• Pre-existing factors causing ROS elevation must be removed

Glutathione Infusions and Parkinson’s Disease
• Sechi et. al. serial cases in 9 with PD
• Glutathione given 600 mg BID via infusion daily for 30 days
• Some patients maintained symptom free or substantially improved status after 3 months

Glutathione in Parkinson’s Disease RCT (Pilot trial) • Hauser, et. al. RCT double blind
placebo controlled n = 21
• Patients given 1,400 mg glutathione or placebo 3x/week for 4 weeks
• No statistical significance observed
Necessary Glutathione Cofactors (PRE-LOAD)
• IV • Vitamin C
• Vitamins - B1, B2, B6, B12,
• Minerals - selenium, magnesium and zinc
• Alpha lipoic acid (not part of the preload)
• Oral: • Vitamin E, folate

Glutathione Therapy For NDDs
• Preload:
• Vitamin C 7.5 g
• Calcium Chloride 500 mg
• Magnesium Chloride 1,000 mg
• Zinc Sulfate 25 mg
• Selenium` 200 mcg
• B Complex 100 2 mL
• Dexapanthenol 500 mg
• Pyridoxine 200 mg
• Sodium Bicarbonate 8.4% 10 mL
• Sterile Water 250 mL
• Administered prior to glutathione infusion
• Glutathione 1,000 – 4,000 mg
• 0.9% Sodium Chloride 50-100 mL
• Delivered over 10-20 minutes
• Compounded on demand if possible
• 2-3 times per week for 4-6 weeks then weekly for maintenance
Alpha Lipoic Acid
Rationale for PT use
• While the majority of its use has been by oral administration ALA’s effectiveness is often limited by insufficient absorption and rapid excretion.
• This limits the serum concentration below levels necessary to achieve responses in certain clinical situations like chemotherapeutic induced polyneuropathies and progressive diabetic neuropathies.
• Intravenous administration of alpha lipoic acid has been most prevalent in Germany where it has been used for over 30 years. Its primary clinical indication was as a treatment for diabetic neuropathy and other peripheral neuropathies.
Anti-Oxidant Effects
• ALA has two distinct ways to act as a free radical scavenger.
• What makes ALA a unique anti-oxidant is its amphophyllic nature - It can act as an antioxidant both within the cell cytosol and lipid membrane
• The second ROS quenching mechanism ALA exhibits is the ability to recycle other anti-oxidants. DHLA is the key form responsible for this effect. Vitamin C and glutathione are two key cellular anti-oxidants that can be recycled by DHLA
Insulin Potentiation
• Binding of insulin to receptors leads to enzymatic phosphorylation of tyrosine residues.
• This leads to several downstream processes resulting in eventual translocation of glucose receptors (GLUT 4) to the cell membrane leading to increased uptake of sugar into the cell.
• ALA has been shown to increase translocation of GLUT4 to membrane complex thereby acting as an insulin mimetic.
Heavy Metal Detoxification
• Many toxic metals present in the body are naturally removed through hepatobiliary excretion complexed with non-protein thiols like glutathione.
• ALA has a known enhancement of glutathione and other thiol compounds.
• Preclinical studies in rats showed that ALA not only stimulated increases in non-protein thiols in the blood, but also stimulated the excretion of glutathione in bile.
• This led to a substantially increased excretion in a dose dependent manner of Mercury and Cadmium
• In-vitro data also suggest that ALA/DHLA can limit ROS generation by Iron and Copper and lead to reduced accumulation of these metals in animals

Neuroprotection
• ALA has been well studied in diabetic neuropathic syndromes and has also hade limited trials in chemotherapy-induced neuropathies.
• In both of these conditions nerve dysfunction is caused by ROS generation leading to alterations in endoneural blood flow and nerve conduction
• ALA has been show improve both of these factors in animal trials
ALA Impact in NDDs
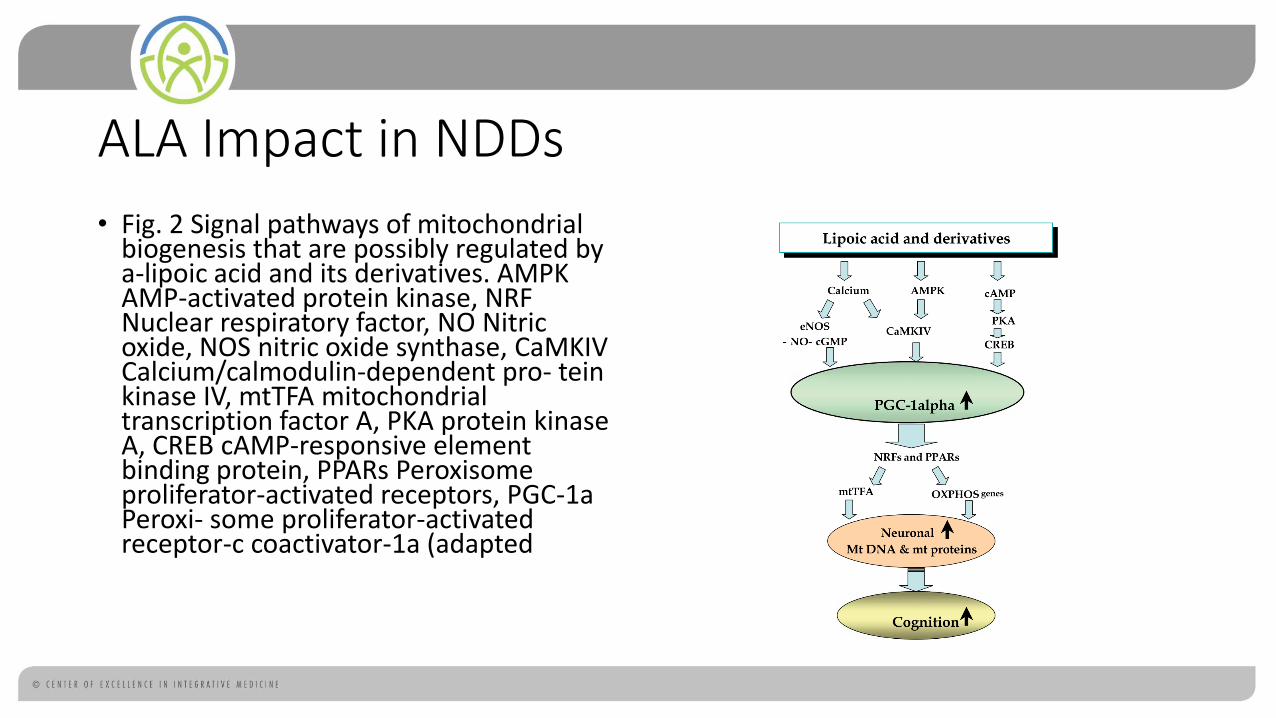
• Fig. 2 Signal pathways of mitochondrial biogenesis that are possibly regulated by a-lipoic acid and its derivatives. AMPK AMP-activated protein kinase, NRF Nuclear respiratory factor, NO Nitric oxide, NOS nitric oxide synthase, CaMKIV Calcium/calmodulin-dependent pro- tein kinase IV, mtTFA mitochondrial transcription factor A, PKA protein kinase A, CREB cAMP-responsive element binding protein, PPARs Peroxisome proliferator-activated receptors, PGC-1a Peroxi- some proliferator-activated receptor-c coactivator-1a (adapted

Proven Clinical Indications of IV Use
• Diabetic Poly-Neuropathy
• Chemotherapy Induced Neuropathy
Dosage
• ALA is administered in doses ranging from 300 - 600 mg infused slowly over 60-90 minutes
• ALA is light sensitive and must be run without exposure to light • Compound in low light room
• Cover IV bag
• Foil over administration set or use opaque line
Contraindications/Interactions
• ALA has no effects on cytochrome series enzymes in the liver and on renal clearance and therefore has no known effect on drug metabolism.
• As a result of ALA’s blood sugar lowering effects caution should be used when administering to medicated diabetic patients as it may potentiate hypoglycemic episodes.
Side Effects
• Gastrointestinal symptoms • nausea, vomiting and diarrhoea
• Skin reactions (urticaria, generalized pruritis)
• Headaches
• Hot flashes/Chills
• Rare cases of slowly progressing anaphylactoid reactions
• 1 case of serious allergic reaction with laryngospasm
• Most reactions occurred when administered doses exceeded 600 mg
Treatment of ADRs
• Ultimately there are no persistent toxic effects that have been observed at clinically relevant dosing of ALA.
• As mentioned in prior slide most ADRs are dose related and can be prevented by careful dose escalation or reduction of dosage in cases of intolerance.
• For allergic type reactions the obvious approach would be careful patient screening to evaluate potential patients with allergic tendencies where caution should be exercised.
• If allergic reactions occur the appropriate anti-allergic therapy should be prescribed depending on the severity of the reaction and further treatment with ALA should be avoided.
Lipoic Acid Therapy
• Racemic Alpha Lipoic Acid 150 – 600 mg • escalating to 600 mg in 150 increments
• If R+ ALA, 75-300 mg, escalating in 75 mg increments
• 0.9% sodium Chloride 100 mL
• Run over 60 minutes in a light protected bag and line
• Can be done 1-3 times per week
• Can be done concurrently after glutathione

Phosphatidyl Choline

Phosphatidylcholine (PTC) and NDD
• Oxidation of PTC has been shown to be a pathological marker in a variety of NDDs
• In addition, several NDDs also show aberrations in phospholipid metabolism
• Another postulated cofactor in NDD (especially) dementia is circulatory abnormalities
• For all of these reasons PTC has been used in treatment and research for NDD

Structure of bioactive cholines
Phosphatidyl Choline CDP Citicoline

Rationale for PT use
• Oral administration of phosphatidylcholine is insufficient to lead to direct changes in atherosclerotic plaques.
• Phosphatidylcholine (PC) enters the small intestine in the bile, diet or supplementation. It is hydrolized in the intestinal lumen by phospholipase to lysolecithin which is taken up by the intestinal lumen.
• Studies in animals suggest that a small portion of oral PC can be taken up intact but the remainder is partially or completely degraded.

Pharmacodynamics of CDP-Choline
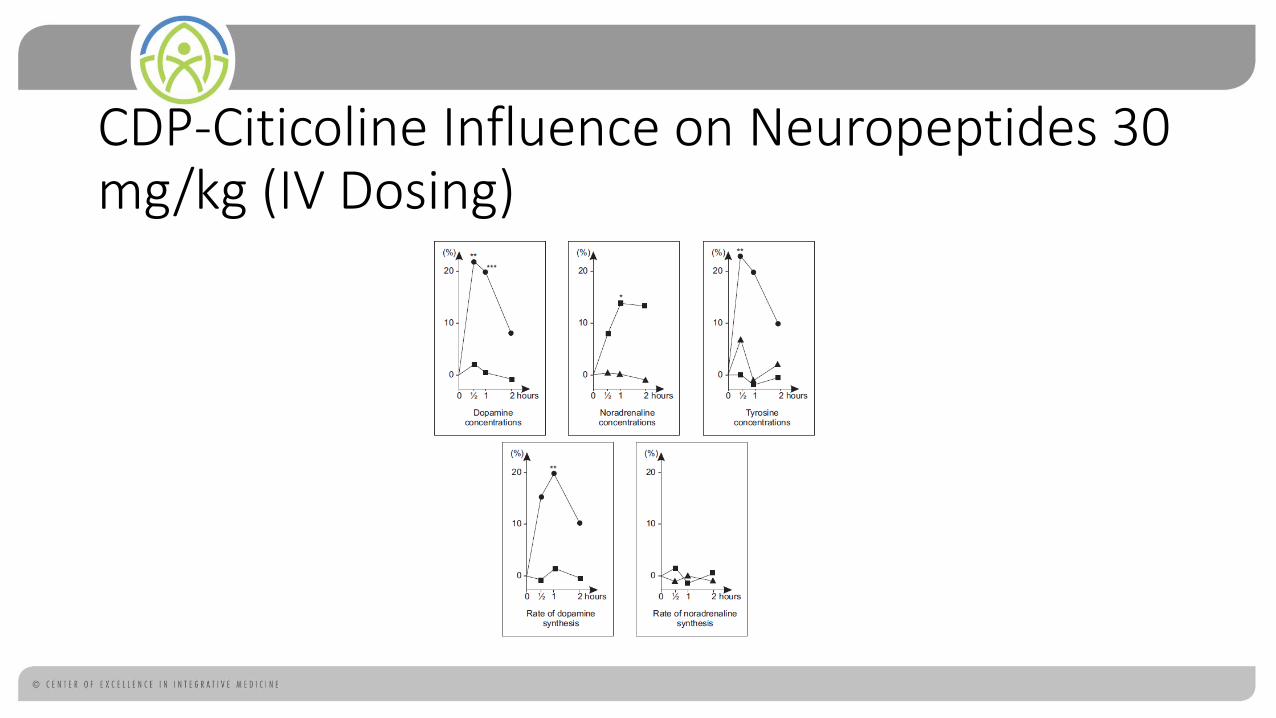
CDP-Citicoline Influence on Neuropeptides 30 mg/kg (IV Dosing)
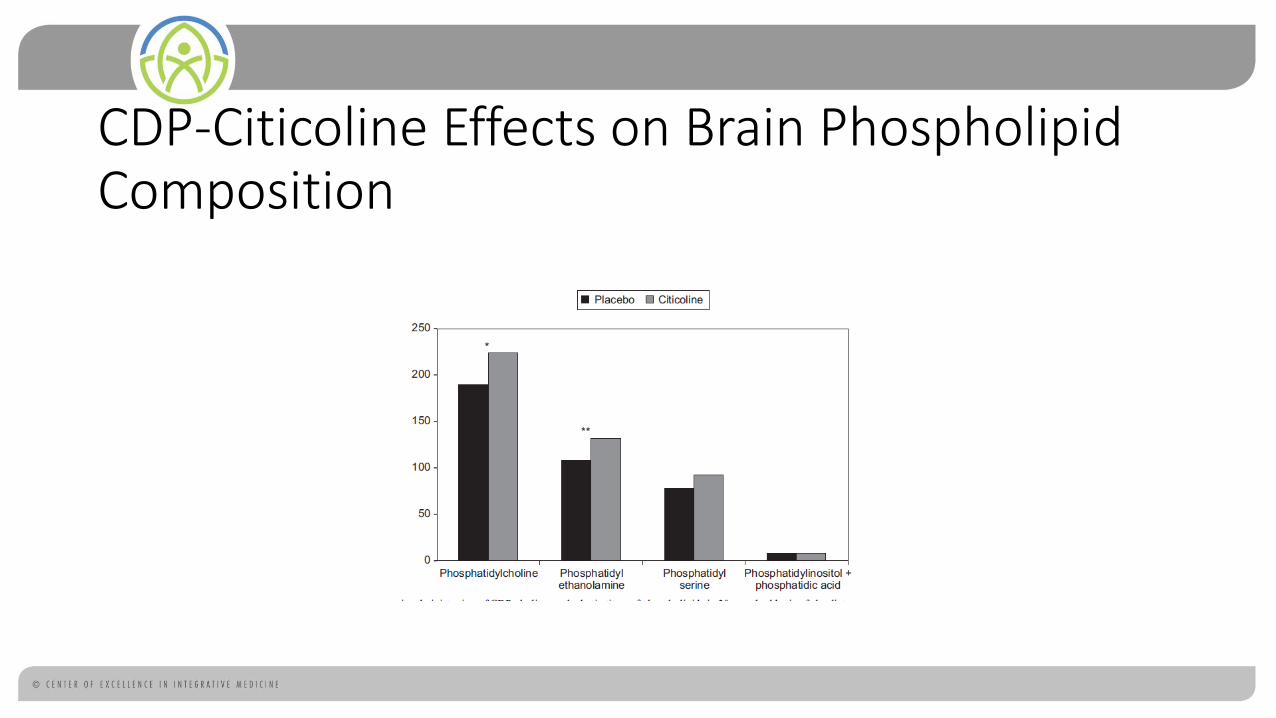
CDP-Citicoline Effects on Brain Phospholipid Composition
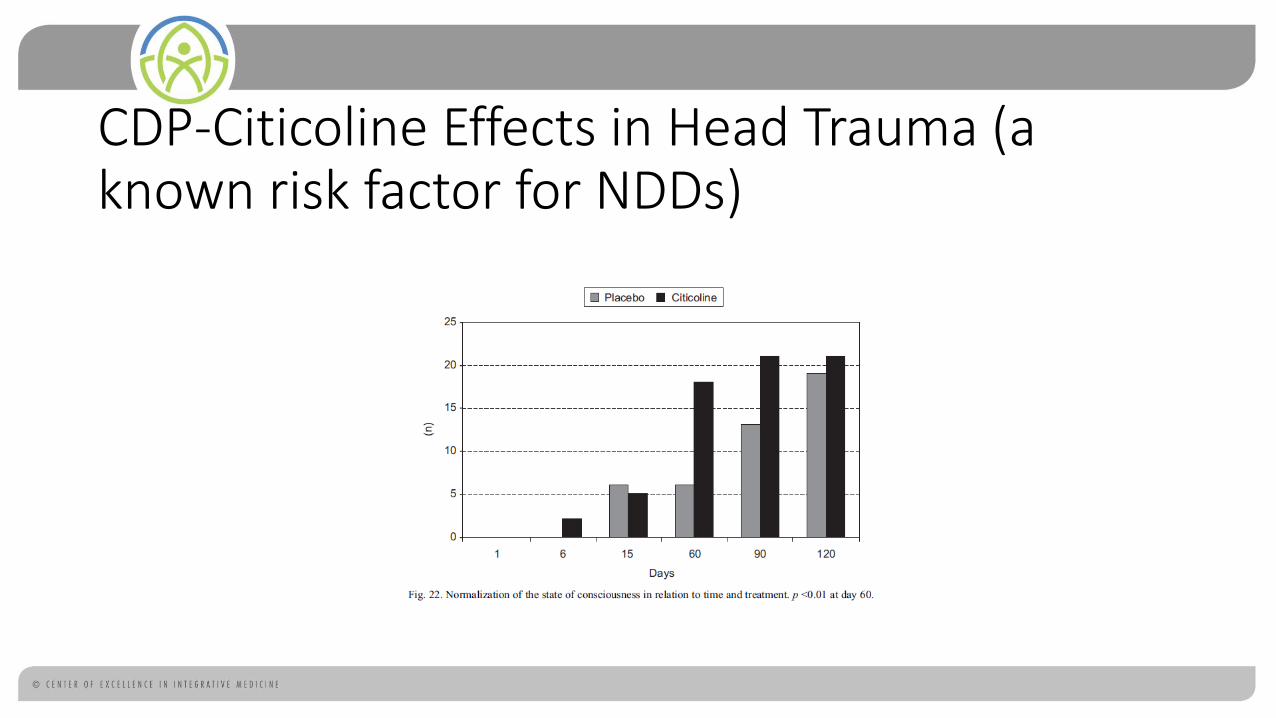
CDP-Citicoline Effects in Head Trauma (a known risk factor for NDDs)

CDP-Citicoline and Cerebral Ischemia Patients with Hemiplegia
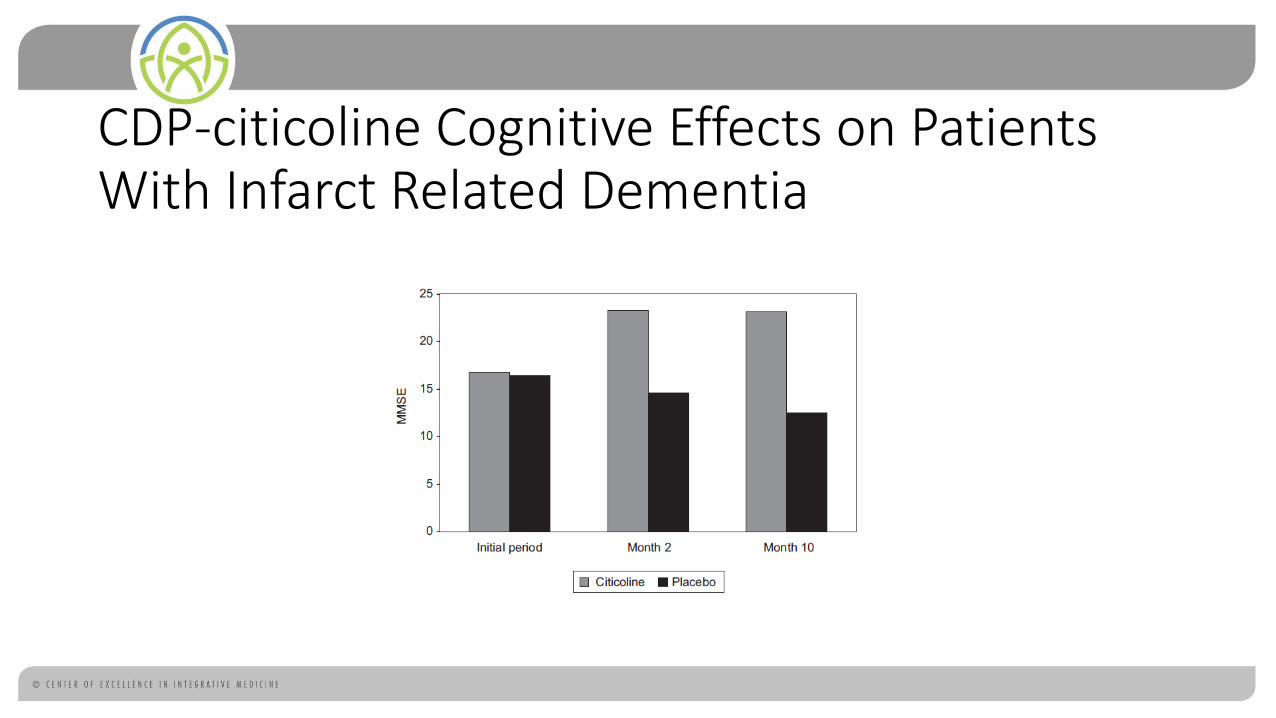
CDP-citicoline Cognitive Effects on Patients With Infarct Related Dementia
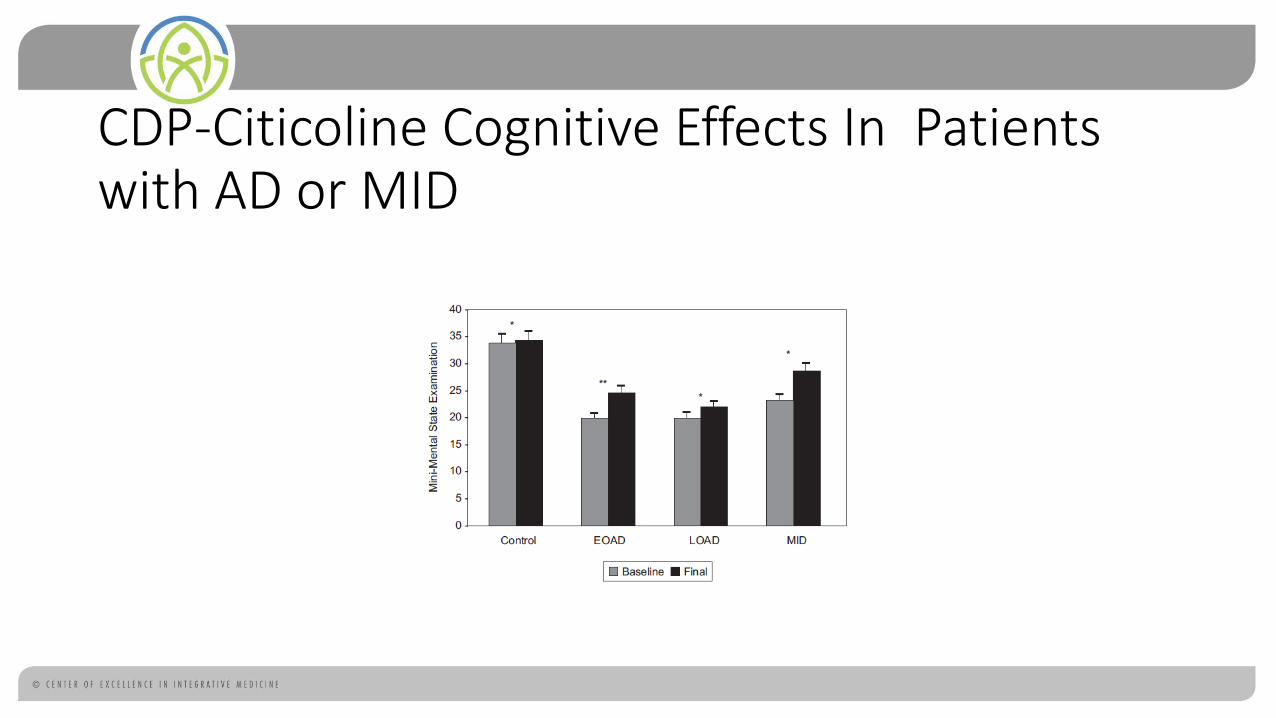
CDP-Citicoline Cognitive Effects In Patients with AD or MID
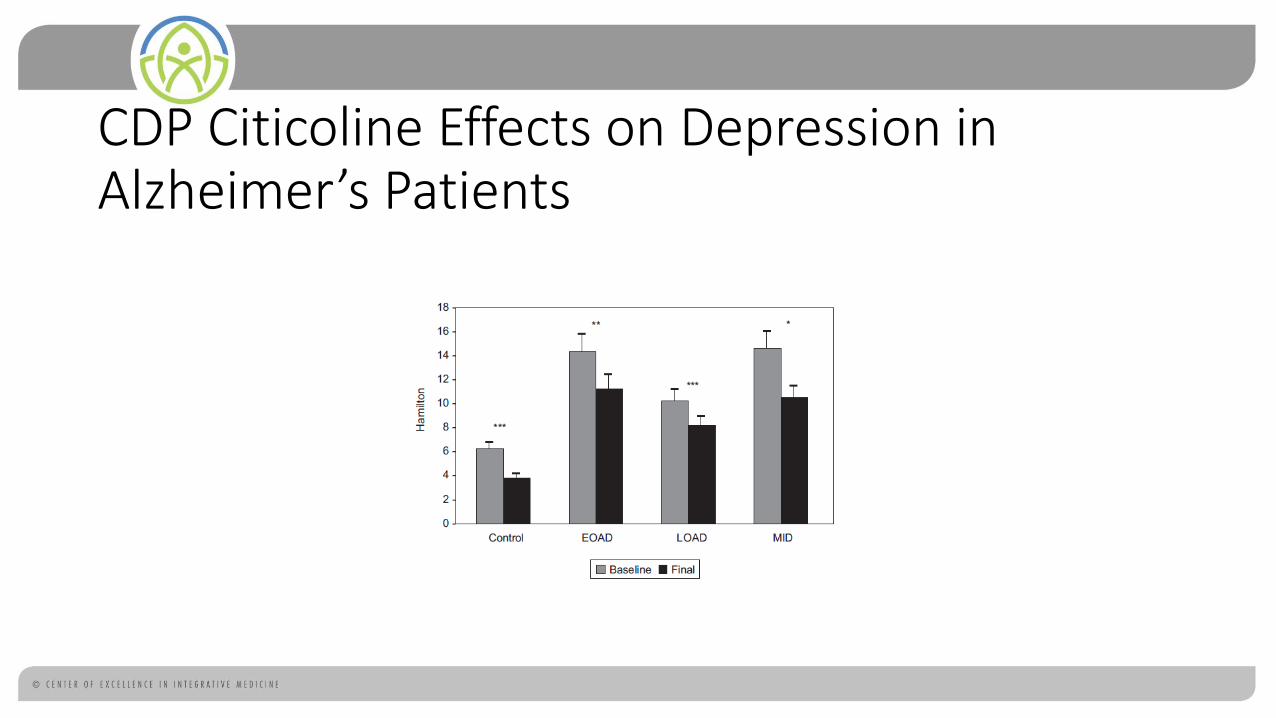
CDP Citicoline Effects on Depression in Alzheimer’s Patients
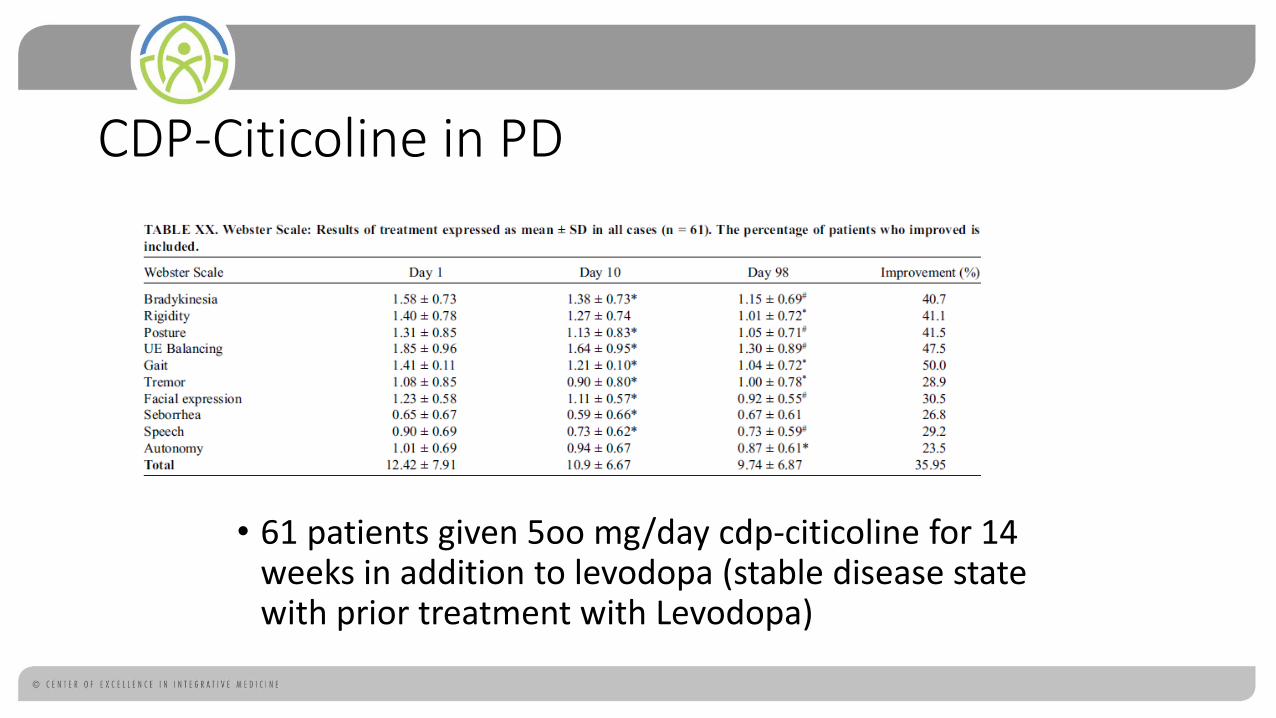
CDP-Citicoline in PD
• 61 patients given 5oo mg/day cdp-citicoline for 14 weeks in addition to levodopa (stable disease state with prior treatment with Levodopa)
1,2-dilinoleoylphosphatidylcholine EPL (Plaquex™) in NDD • Research has shown EPL has shown:
• Improvement in lipid levels
• Reduced Lipid Peroxidation
• Improvement in Endothelial Dysfunction
• Reduction in coagulability
• From this we can surmise a strong potential for activity in NDD
Implications of PTC in NDD for Infusion Therapy • Strong role for PTC infusion in early treatment of risk factors
associated with NDD: • Head Trauma
• Cerebral Infarct
• Early treatment with Infusions of PTC followed by oral maintenance therapy
Dosage
• Generally given 1,000-2,500 mg
• Recommended starting with 1,000 mg and increasing by 500 mg per treatment until 2,500 mg or tolerance is reached (phlebitis)
• Used only in 250 mL D5W
• PC is infused slowly over 90-120 minutes
• Usually 10-20 treatments are given
• Can be given 1- 5 times per week
• Use only BD catheters (may react with others)
Contraindications
• Known hypersensitivity to any of the ingredients in the formulation.
• Treatment protocols from manufacturer must be followed exactly to avoid thrombophlebitis and formula must be mixed only with indicated solution (ie. 5% dextrose).
• Patients with antiphospholipid-antibody syndrome need to be cautious in using this therapy.
• Those with malabsorption issues can develop diarrhea or steatorrhea.
• PC is incompatible with almost every intravenous admixture ingredient and should always be administered in a dextrose solution on its own
•
Side Effects of PC
Common
• Phlebitis/Thrombophlebitis (very common)
• Gastrointestinal effects: • Nausea/vomiting • Diarrhea
Rare
• Transient elevated transaminases
• Rash
• Fever/chills

Preventing Phlebitis
• Avoidance of Thrombophelbitis can be achieved in most patients by proper infusion equipment and technique. PC should only be administered slowly through an angiocatheter that is mean to deliver lipids. Insertion site selection is important and only patent large veins should be used. If patients experience pain at the insertion site, the infusion should be stopped and move to another site before a phlebitis occurs.

Putting It Together Simplified Treatment Strategies For NDDs
IV Treatment Protocol
Treatments should be done on separate days
• Treatment 1 (1-5 times per week): • Glutathione Pre-load Formula
• IV Glutathione 1,000 mg – 4,000 mg
• IV ALA 300-600 mg Racemic or 150-300 mg R+
• Treatment 2 (1-2 times per week): • PTC 1,000 – 2,500 mg
• Treatments 1 and 2 should be done on different days

Oral Supportive Therapies
• Acetyl-L-Carnitine - 1,000 mg bid
• DHA – 1,000 mg QD
• Vitamin E mixed tocopherol tocotrienols
• ALA 300-600 mg bid (1/2 dose if R+ALA)
• CoQ10 400 bid-tid
• He Shou Wu (polygonium multiflorum) 1-3 g per day
• Curcumin
• Consider Ketogenic diet

Got Questions?
• See you in the Facebook group!