mucormicosis (zygomicosis)
TRANSCRIPT

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 1/21
Official reprint from UpToDatewww.uptodate.com ©2015 UpToDate
Author
Gary M Cox, MD
Section Editor
Carol A Kauffman, MD
Deputy Editor
Anna R Thorner, MD
Mucormycosis (zygomycosis)
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Jul 2015. | This topic last updated: Jul 27, 2015.
INTRODUCTION — Mucormycosis is manifested by a variety of different syndromes in humans, particularly in
immunocompromised patients and those with diabetes mellitus [1]. Devastating rhino-orbital-cerebral and pulmonary
infections are the most common syndromes caused by these fungi.
There is some controversy over the terminology used to refer to infections due to this group of fungi. The term
"mucormycosis" was used for years and then was supplanted by "zygomycosis" for several decades. Based on
molecular studies, "mucormycosis" is currently again the appropriate term [1-4].
The microbiology, clinical manifestations, diagnosis, and therapy of mucormycosis will be reviewed here. Several
specific syndromes that can be caused by these fungi are discussed separately. (See "Fungal rhinosinusitis" and
"Non-access-related infections in chronic dialysis patients".)
MYCOLOGY — The genera in the order Mucorales cause most human infection. These organisms are ubiquitous in
nature and can be found on decaying vegetation and in the soil. These fungi grow rapidly and release large numbers of
spores that can become airborne. Because the agents of mucormycosis are common in the environment, they are
relatively frequent contaminants in the clinical microbiology laboratory; all humans have ample exposure to these fungi
during day-to-day activities. The fact that mucormycosis is a rare human infection reflects the effectiveness of the
intact human immune system. This is further supported by the finding that almost all human infections due to the agents
of mucormycosis occur in the presence of some underlying compromising condition.
The genera most commonly found in human infections are Rhizopus, Mucor , and Rhizomucor ; Cunninghamella,
Absidia, Saksenaea, and Apophysomyces are genera that are less commonly implicated in infection [5].
The hyphae of the Mucorales are distinct and allow for a presumptive identification from clinical specimens. The
hyphae are broad (5 to 15 micron diameter), irregularly branched, and have rare septations (picture 1). This is in
contrast to the hyphae of ascomycetous molds, such as Aspergillus, which are narrower (2 to 5 micron diameter),
exhibit regular branching, and have many septations.
The lack of regular septations may contribute to the fragile nature of the hyphae and the difficulty of growing the
agents of mucormycosis from clinical specimens. Grinding clinical specimens can cause excessive damage to the
hyphae. Thus, finely mincing tissues is preferred for culturing tissue samples that may contain molds.
PATHOGENESIS — Rhizopus organisms have an enzyme, ketone reductase, that allows them to thrive in high
glucose, acidic conditions. Serum from healthy individuals inhibits growth of Rhizopus, whereas serum from individuals
in diabetic ketoacidosis stimulates growth [6].
Rhino-orbital-cerebral and pulmonary mucormycosis are acquired by the inhalation of spores. In healthy individuals,
cilia transport these spores to the pharynx and they are cleared through the gastrointestinal tract. In susceptible
individuals, infection usually begins in the nasal turbinates or the alveoli [7]. The agents of mucormycosis are
angioinvasive; thus, infarction of infected tissues is a hallmark of invasive disease [8].
Deferoxamine and iron overload — Deferoxamine, which chelates both iron and aluminum, increases the risk of
mucormycosis by enhancing growth and pathogenicity [7,9-11]. The deferoxamine-iron chelate, called feroxamine, is a
siderophore for the species Rhizopus, increasing iron uptake by the fungus, which stimulates fungal growth and leads
to tissue invasion [8,12].
®
®
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0
7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 2/21
Iron overload itself may predispose to mucormycosis in the absence of deferoxamine therapy [13]. In addition,
individuals with diabetic ketoacidosis have elevated concentrations of free iron in their serum, which supports the
growth of Rhizopus oryzae at an acidic, but not at an alkaline, pH [14,15].
Deferoxamine was once used commonly as an aluminum chelator in patients with renal failure; however, aluminum
excess is rarely seen today. Currently, patients at risk for deferoxamine-associated mucormycosis are those who have
received multiple blood transfusions and are treated with this chelating agent for iron overload. The majority of patients
with deferoxamine-associated infection present with disseminated disease that is rapidly fatal, with a mortality rate that
approaches 90 percent [11]. (See "Aluminum toxicity in chronic kidney disease", section on 'Adverse effects of deferoxamine'.)
In contrast with deferoxamine, other iron chelating agents, such as deferasirox and deferiprone, do not act as
siderophores and therefore do not increase the risk of mucormycosis. To the contrary, studies in mice with
mucormycosis found that these agents might actually be beneficial (eg, improve survival and reduce the tissue fungal
burden) [16,17]. The use of deferasirox for the treatment of mucormycosis has not been adequately studied in
humans. (See 'Deferasirox' below.)
RISK FACTORS — Almost all patients with invasive mucormycosis have some underlying disease that both
predisposes to the infection and influences the clinical presentation. The most common underlying diseases are
[5,18-29]:
EPIDEMIOLOGY — The incidence of mucormycosis is difficult to estimate since it is not a reportable disease and the
risk varies widely in different populations. A review of 929 cases of mucormycosis that were reported between 1940
and 2003 noted that diabetes mellitus was the most common risk factor, found in 36 percent of cases, followed by
hematologic malignancies (17 percent) and solid organ or hematopoietic cell transplantation (12 percent) [5]. In some
patients, mucormycosis was the diabetes-defining illness. In a later study of 101 patients diagnosed with
mucormycosis between 2005 and 2007 in France, hematologic malignancy was the most common risk factor,
occurring in 50 percent of patients, followed by diabetes in 23 percent and trauma in 18 percent of cases [35].
Malignancy and hematopoietic cell transplantation — Among patients with malignancy, hematologic malignanciesare much more frequently associated with mucormycosis than solid tumors [5,25-27]. However, even in patients with
hematologic malignancies, mucormycosis appears to occur in less than 1 percent of patients [36]. Among
hematopoietic cell transplant (HCT) recipients, the reported incidence has ranged from 0.1 to 2 percent, with the
highest incidence in patients with graft-versus-host disease [31].
Reports from several countries have noted an increase in mucormycosis in patients with hematologic malignancies
[1,30,37]. Most of these patients had undergone HCT, many had graft-versus-host disease, and almost all were on
voriconazole for prophylaxis or treatment [1,30]. A case-control study in a population of patients with hematologic
malignancies compared patients with mucormycosis to those who had no fungal infection; voriconazole prophylaxis was
an independent risk factor for mucormycosis (odds ratio 10.4, 95% CI 2.1-39) [27].
Diabetes mellitus, particularly with ketoacidosis●
Treatment with glucocorticoids [25]●
Hematologic malignancies [1,27,30]●
Hematopoietic stem cell transplantation [5,25,31]●
Solid organ transplantation [31-34]●
Treatment with deferoxamine [9-11,13] (see 'Deferoxamine and iron overload' above and "Chelation therapy for
thalassemia and other iron overload states")
●
Iron overload [13]●
AIDS●
Injection drug use●
Trauma/burns [35]●
Malnutrition●
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 3/21
Although the possible causes of the increase in mucormycosis in patients with hematologic malignancies continue to be
debated, reasons that have been proposed include selection of the agents of mucormycosis caused by voriconazole
use, increasing use and intensity of immunosuppressive agents, and a decrease in invasive aspergillosis-related
mortality following HCT, resulting in the emergence of rare fungi during the late posttransplant period [38].
Solid organ transplantation — In a multicenter prospective study of invasive fungal infections in transplant recipients
in the United States between 2001 and 2006, the 12-month cumulative incidence of mucormycosis was less than 1
percent among solid organ transplant recipients; only 2 percent of invasive fungal infections in such patients were
caused by the agents of mucormycosis [31,39]. Among solid organ transplant recipients, risk factors for mucormycosisinclude renal transplantation [32], renal failure, diabetes, and prior voriconazole or caspofungin use [34].
Diabetes — As noted above, diabetes is a common predisposing condition [5]. The number of reported cases of
mucormycosis in diabetic patients in the United States has declined since the 1990s, a trend that has not been noted in
France [37] or in developing countries [28,40]. One hypothesis that has been suggested to explain the decline in the
United States is the widespread use of statins, which have inhibitory activity in vitro against a wide range of the agents
of mucormycosis [28].
Healthcare-associated — Healthcare-associated cases of mucormycosis have been reported. In a study of 169
healthcare-associated cases of mucormycosis in Europe between 1970 and 2008, the major underlying diseases were
solid organ transplantation (in 24 percent), diabetes mellitus (in 22 percent), and severe prematurity (in 21 percent)
[41]. Skin was the most common site of infection (in 57 percent), followed by the gastrointestinal tract (15 percent).Portals of entry included surgery, catheters (especially intravascular catheters), and adhesive tape. Outbreaks and
clusters have been associated with adhesive bandages, wooden tongue depressors, adjacent building construction,
and hospital linens [41-43]. Fatal gastrointestinal mucormycosis has also been reported in a premature neonate who
received a probiotic that was contaminated with Rhizopus oryzae; probiotics were being given in an attempt to prevent
necrotizing enterocolitis [44]. (See "Prevention of necrotizing enterocolitis in newborns", section on 'Probiotics' .)
Natural disaster-associated — Cases of mucormycosis have occurred following a tornado, a tsunami, and a volcanic
eruption [45-49]. As an example, in 2011, an outbreak of necrotizing soft tissue infections causes by Apophysomyces
trapeziformis occurred in patients with traumatic injuries resulting from a tornado in Joplin, Missouri, in the United
States [45]. A total of 18 suspected cases were identified, of which 13 were confirmed. Two patients had diabetes
and none were immunocompromised. Ten patients required intensive care unit admission and five died.
In a case-control study of patients injured during the tornado in Joplin, Missouri, the 13 patients with confirmed
infection each had a median of five wounds (range one to seven); 11 patients (85 percent) had ≥1 fracture, nine
patients (69 percent) had blunt trauma, and five patients (38 percent) had penetrating trauma [48]. All case patients
had been located in the zone that sustained the most severe damage during the tornado. On multivariate analysis,
infection was associated with penetrating trauma (adjusted odds ratio [aOR] 8.8, 95% CI 1.1-69.2) and an increased
number of wounds (aOR 2.0 for each additional wound; 95% CI 1.2-3.2). Whole genome sequencing showed that the
Apophysomyces trapeziformis isolates represented four separate strains.
Combat-associated — Invasive fungal infections, including mucormycosis, have been reported in United States
military personnel who sustained blast injuries during combat in Afghanistan [50]. Between June 2009 and through
December 2010, a total of 37 cases were identified, including 20 proven cases (with histopathologic evidence of angioinvasion), 4 probable cases (with histopathologic evidence of nonvascular tissue invasion), and 13 possible cases
(with a positive fungal culture, but without histopathologic evidence). All injuries occurred secondary to explosive blasts,
and most injuries occurred during foot patrol (in 34 patients; 92 percent). All patients had extremity injuries and 29
patients (78 percent) had lower extremity amputation either at the time of the injury or during the first surgery following
the injury. Thirty-six patients (97 percent) required large-volume blood transfusion.
Mold isolates were recovered from the wounds of 31 patients (83 percent); the most commonly detected fungi
belonged to the order Mucorales (in 16 patients), Aspergillus spp (in 16 patients), and Fusarium spp (in 9 patients)
[50]. Multiple mold species were isolated from 28 percent of infected wounds. Frequent debridements or amputation
revisions were required and three deaths were thought to be related to the infection (8 percent).
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 4/21
CLINICAL PRESENTATION — Mucormycosis is characterized by infarction and necrosis of host tissues that results
from invasion of the vasculature by hyphae [29]. The pace is usually fast, but there are rare descriptions of infections
with an indolent course [51,52].
Rhino-orbital-cerebral mucormycosis — The most common clinical presentation of mucormycosis is rhino-orbital-
cerebral infection, which is presumed to start with inhalation of spores into the paranasal sinuses of a susceptible host.
Hyperglycemia, usually with an associated metabolic acidosis, is the most common underlying condition [5]. A review
of 179 cases of rhino-orbital-cerebral mucormycosis found that 126 (70 percent) of the patients had diabetes mellitus
and that most had ketoacidosis at the time of presentation [18]. There are rare reports of rhino-orbital-cerebralmucormycosis in the absence of any apparent risk factors [18,52-55].
The infection usually presents as acute sinusitis with fever, nasal congestion, purulent nasal discharge, headache, and
sinus pain. All of the sinuses become involved, and spread to contiguous structures, such as the palate, orbit, and
brain, usually progresses rapidly. However, there have been some reports of rhino-orbital-cerebral mucormycosis with
an indolent course [51].
The hallmarks of spread beyond the sinuses are tissue necrosis of the palate resulting in palatal eschars, destruction
of the turbinates, perinasal swelling, and erythema and cyanosis of the facial skin overlying the involved sinuses. A
black eschar, which results from necrosis of tissues after vascular invasion by the fungus, may be visible in the nasal
mucosa or the palate [56].
Signs of orbital involvement include periorbital edema, proptosis, and blindness. Facial numbness is frequent and
results from infarction of sensory branches of the fifth cranial nerve. Spread of the infection from the ethmoid sinus to
the frontal lobe results in obtundation. Spread from the sphenoid sinuses to the adjacent cavernous sinus can result in
cranial nerve palsies, thrombosis of the sinus, and involvement of the carotid artery. Hematogenous spread to other
organs is rare unless the patient has an underlying hematologic malignancy with neutropenia.
A review of 208 cases of rhino-orbital-cerebral mucormycosis published in the literature between 1970 and 1993 found
the following frequency of symptoms and signs [57]:
Rhino-orbital-cerebral mucormycosis is most commonly caused by Rhizopus oryzae.
Pulmonary mucormycosis — Pulmonary mucormycosis is a rapidly progressive infection that occurs after inhalation
of spores into the bronchioles and alveoli (image 1). Pneumonia with infarction and necrosis results, and the infection
can spread to contiguous structures, such as the mediastinum and heart [58,59], or disseminate hematogenously to
other organs [60,61].
Most patients have fever with hemoptysis that can sometimes be massive [60,61]. The most common underlying
conditions have been hematologic malignancies, treatment with glucocorticoids or deferoxamine, and solid organ
transplantation; pulmonary infection is less common than rhino-orbital-cerebral infection in diabetics [19,60-65]. In a
series of 24 patients with mucormycosis and hematologic malignancy, 71 percent had pulmonary involvement and only
one had rhino-orbital-cerebral involvement; 7 of 12 patients who underwent autopsy had disseminated disease in
addition to pulmonary infection [25].
Gastrointestinal mucormycosis — Although unusual, mucormycosis of the gastrointestinal tract may occur as the
result of ingestion of spores. One review of 87 cases found that the stomach was the most common site (58 percent),
followed by the colon (32 percent) [66]. The ileum and esophagus were rare sites of involvement.
Fever – 44 percent●
Nasal ulceration or necrosis – 38 percent●
Periorbital or facial swelling – 34 percent●
Decreased vision – 30 percent●
Ophthalmoplegia – 29 percent●
Sinusitis – 26 percent●
Headache – 25 percent●
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 5/21
The underlying diseases of patients with gastrointestinal mucormycosis have been diabetes mellitus, solid organ
transplantation, treatment with glucocorticoids, and prematurity and/or malnutrition in infants [20,66-69]. Patients
present with abdominal pain and hematemesis. The gastrointestinal lesions are necrotic ulcers that can lead to
perforation and peritonitis [20]. Bowel infarctions and hemorrhagic shock can result from gastrointestinal mucormycosis
[70], and the prognosis for all patients is poor.
Cutaneous mucormycosis — Infection of the skin and soft tissues with the agents of mucormycosis usually results
from inoculation of the spores into the dermis. Thus, cutaneous mucormycosis is almost always associated with
trauma or wounds. The entry of the fungi into the dermis can result from seemingly innocuous insults, such as the entrysite for an intravenous catheter, spider bites, and insulin injection sites [21,22,71-75]. Infection has also been
associated with contaminated traumatic wounds, dressings and splints, burns, and surgical sites
[21,22,41,45,46,48,50,71-75].
When infection is associated with relatively minor breaks in the skin, the host usually has some underlying disease,
such as diabetes mellitus, organ transplantation, neutropenia, or severe prematurity. Infections associated with major
trauma or contaminated dressings have been found in otherwise immunocompetent patients [5,75].
Healthcare-associated, natural disaster–associated, and combat-associated cases of mucormycosis are discussed
above. (See 'Healthcare-associated' above and 'Natural disaster-associated' above and 'Combat-associated' above.)
Cutaneous mucormycosis usually appears as a single, painful, indurated area of cellulitis that develops into an
ecthyma-like lesion. Patients who have suffered trauma with an open wound that was contaminated with spores can
develop rapidly progressive tissue necrosis reflecting the presence of ischemic infarction [21,22,46,48,50,72,74,75].
Dissemination and deep tissue involvement are unusual complications of cutaneous mucormycosis [73,75].
Renal mucormycosis — Isolated involvement of the kidneys with mucormycosis has been reported and is presumed
to occur via seeding of the kidneys during an episode of fungemia. Almost all patients with isolated renal mucormycosis
have risk factors for fungemia, including an intravenous catheter, intravenous drug use, or AIDS [23,24,76-78].
Patients with renal mucormycosis usually present with flank pain and fever. Involvement can be either unilateral or
bilateral.
Isolated CNS involvement — Central nervous system (CNS) mucormycosis typically arises from an adjacent
paranasal sinus infection. However, there have been more than 30 cases of isolated CNS mucormycosis described in
the literature [24,79-81]. Infection was thought to result from seeding of the brain during an episode of fungemia,
analogous to renal involvement. Over two-thirds of the patients with isolated CNS mucormycosis have been
intravenous drug users who presumably have injected material contaminated with fungi directly into the bloodstream.
Some of the patients with isolated CNS mucormycosis had HIV infection in addition to drug use. However, it is not clear
whether HIV infection is an independent risk factor [24,80,82].
Most of the patients presented with lethargy and focal neurologic deficits, with the vast majority having involvement of
the basal ganglia [79-81]. Isolated involvement of the frontal lobe has also been described [79].
Disseminated disease — Disseminated mucormycosis is rare and occurs most commonly in severely
immunocompromised patients, burn patients, premature infants, and individuals who have received deferoxamine [1,5].
In the series of 929 cases of mucormycosis described above, disseminated disease was present in 40 to 50 percent
of patients with cerebral or pulmonary mucormycosis [5]. The mortality rate in patients with disseminated
mucormycosis was 96 percent.
DIAGNOSIS — The diagnosis of mucormycosis relies upon the identification of organisms in tissue by histopathology
with culture confirmation. However, culture often yields no growth, and histopathologic identification of an organism with
a structure typical of Mucorales may provide the only evidence of infection. A clinician must think of this entity in the
appropriate clinical setting and pursue invasive testing in order to establish a diagnosis as early as possible.
Investigational studies have demonstrated the feasibility of using polymerase chain reaction (PCR)-based techniques
on histologic specimens [83-85]. In one study of patients with proven mucormycosis, among 12 cases that were
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 6/21
positive by culture, 10 were also positive by PCR and sequencing was concordant with culture results to the genus
level in 9 [84]. Among 15 culture-negative cases, PCR was positive and sequencing allowed genus identification in 12.
The PCR-based technique used in this study appears promising for establishing the diagnosis of mucormycosis when
cultures are negative.
Rhino-orbital-cerebral infection — The presence of mucormycosis should be suspected in high-risk patients,
especially those who have diabetes and metabolic acidosis and who present with sinusitis, altered mentation, and/or
infarcted tissue in the nose or palate.
Endoscopic evaluation of the sinuses should be performed to look for tissue necrosis and to obtain specimens. The
specimens should be inspected for characteristic broad, nonseptate hyphae with right-angle branching using calcofluor
white and methenamine silver stains. The presence of the characteristic hyphae in a clinical specimen provides a
presumptive diagnosis that should prompt further evaluation (picture 1). However, the absence of hyphae should not
dissuade clinicians from the diagnosis of mucormycosis when the clinical picture is highly suggestive.
Further evaluation includes imaging of the head with either computed tomography (CT) or magnetic resonance imaging
(MRI) to gauge sinus involvement and to evaluate contiguous structures such as the eyes and brain [86].
Pulmonary infection — The diagnosis of pulmonary mucormycosis is difficult since the presentation does not differ
from pneumonia due to other angioinvasive molds. Chest radiographs or CT scans may demonstrate focal
consolidation, masses, pleural effusions, or multiple nodules [62,87]. A halo sign (ground glass attenuation surrounding
a nodule) is characteristic of angioinvasive fungi, but a reversed halo sign, a focal area of ground glass attenuation
surrounded by a ring of consolidation, has also been reported [ 88-90]. Mucormycosis appears to be the most common
condition to cause the reversed halo sign in immunocompromised hosts [89]. In a retrospective study that included 189
patients with proven or probable fungal pneumonia, the reversed halo sign was seen in 7 of 37 patients with
mucormycosis (19 percent), 1 of 132 patients with invasive aspergillosis (<1 percent), and none of 20 patients with
fusariosis [88]. Radiographic evidence of infarction with cavitary lesions and an air crescent sign is unusual [62]. In a
series of 45 cases, the following radiographic features were independent predictors of mucormycosis and helped to
differentiate it from aspergillosis: concomitant sinusitis, >10 pulmonary nodules on CT scan, pleural effusion, and prior
voriconazole prophylaxis [87].
Sputum or bronchoalveolar lavage (BAL) specimens can show the characteristic broad nonseptate hyphae, which is
often the first indicator of mucormycosis [63]. However, in one case series, only 25 percent of sputum or BAL
specimens were positive premortem [25]. Hyphae can also be demonstrated on lung biopsy (picture 1).
Other syndromes — The diagnosis of gastrointestinal mucormycosis can be made with endoscopic biopsy of the
lesions that show the characteristic hyphae. For isolated renal involvement, percutaneous biopsy or nephrectomy can
establish a diagnosis [23]. Urine cultures are almost always sterile. Imaging of the kidneys with ultrasound or CT can
demonstrate enhancement and small foci suggestive of abscesses.
In isolated central nervous system (CNS) involvement, CT scan usually shows poorly enhancing lesions; cerebrospinal
fluid cultures are negative. Diagnosis can be made with biopsy or resection of the involved areas.
TREATMENT
Approach to treatment — Treatment of mucormycosis involves a combination of surgical debridement of involved
tissues and antifungal therapy [2]. Elimination of predisposing factors for infection, such as hyperglycemia, metabolic
acidosis, deferoxamine administration, immunosuppressive drugs, and neutropenia, is also critical.
Intravenous (IV) amphotericin B (lipid formulation) is the drug of choice for initial therapy [91]. Posaconazole is used as
step-down therapy for patients who have responded to amphotericin B; in most cases, the extended-release tablet
formulation can be used. Posaconazole can also be used as salvage therapy for patients who don't respond to or
cannot tolerate amphotericin B; for salvage therapy, the decision to use oral or intravenous posaconazole depends on
how ill the patient is, whether an initial course of amphotericin B was able to be administered, and whether the patient
has a functioning gastrointestinal (GI) tract. Isavuconazole, available in both an IV and an oral formulation, can be used
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 7/21
if the patient cannot tolerate posaconazole.
Surgery — Aggressive surgical debridement of involved tissues should be undertaken as soon as the diagnosis of
rhino-orbital-cerebral mucormycosis is suspected. The debridement to remove all necrotic tissue will often be
disfiguring, requiring removal of the palate, nasal cartilages, and the orbit. There are reports of patients with early
pulmonary infection who were cured with lobectomies [60,61,92]. However, many patients present with multilobar
involvement that precludes surgical resection.
Antifungal drugs — Early initiation of antifungal therapy improves the outcome of infection with mucormycosis. This
was illustrated in a retrospective study of 70 patients with hematologic malignancy who had mucormycosis in which
delayed amphotericin B therapy (starting treatment ≥6 days after diagnosis) resulted in an almost twofold increase in
mortality at 12 weeks after diagnosis (83 versus 49 percent) [93].
Initial therapy — As noted above, amphotericin B is the drug of choice for initial therapy; most clinicians use a lipid
formulation of amphotericin B (rather than amphotericin B deoxycholate) in order to deliver a high dose with less
nephrotoxicity. The usual starting dose is 5 mg/kg daily of liposomal amphotericin B or amphotericin B lipid complex,
and many clinicians will increase the dose up as high as 10 mg/kg daily in an attempt to control this infection. The total
dosage of lipid amphotericin B that should be administered has not been studied.
There have been apparent cures of isolated renal mucormycosis using amphotericin B deoxycholate alone [ 23,76] or
combined with nephrectomy [23]. In severe cases in which there is little residual renal function, nephrectomy with a
short course of amphotericin B deoxycholate (1 mg/kg daily for one to two weeks) appears to be a reasonable course
of action.
Step-down therapy — Posaconazole and isavuconazole are broad-spectrum oral azoles that are active in vitro
against the agents of mucormycosis [94-96]. For patients who have responded to a lipid formulation of amphotericin B,
posaconazole can be used for oral step-down therapy. Isavuconazole is an alternative for patients who cannot take
posaconazole. We continue amphotericin B until the patient has shown signs of improvement; this usually takes several
weeks.
When switching to oral posaconazole, we favor the use of posaconazole delayed-release tablets (300 mg every 12
hours on the first day, then 300 mg once daily) taken with food if possible [ 97]. We do not use the oral suspension of
posaconazole since it is not highly bioavailable and requires fatty food for absorption. A serum trough concentration of posaconazole should be checked after one week of therapy; we suggest a goal trough concentration of at least 0.7
mcg/mL, but higher levels are preferred for treatment of this serious infection (see "Pharmacology of azoles", section
on 'Posaconazole'). The data supporting the use of posaconazole for mucormycosis are discussed below. (See
'Salvage therapy' below.)
When using isavuconazole, loading doses are necessary for the first 48 hours. Loading doses of 200 mg (ie, two
capsules) of oral isavuconazole (equivalent to 372 mg of the prodrug isavuconazonium sulfate) should be given every 8
hours for six doses, followed by 200 mg orally once daily starting 12 to 24 hours after the last loading dose [98]. An IV
formulation of isavuconazole is also available. (See "Pharmacology of azoles", section on 'Isavuconazole'.)
Isavuconazole has not been studied in randomized trials, but it has been evaluated in an open-label non-comparative
study that included 37 patients with proven or probable mucormycosis [98]. Patients were treated with isavuconazoleIV or orally. Median treatment duration was 102 days for patients with primary mucormycosis, 33 days for those with
refractory mucormycosis, and 85 days for those with intolerance to other antifungal therapy. All-cause mortality
through day 42 was 38 percent, and overall success rate at the end of treatment was 31 percent. These data suggest
that isavuconazole has some clinical efficacy in treating mucormycosis, although how it compares to amphotericin B or
posaconazole is unknown.
Salvage therapy — We use posaconazole as salvage therapy for patients who do not respond to or cannot
tolerate amphotericin B [97]. The IV formulation should be used in patients who have to be switched from amphotericin
B before they have had a favorable response and in patients who have an inability to absorb oral medications.
Posaconazole (both IV and oral formulations) is given as a loading dose of 300 mg every 12 hours on the first day,
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 8/21
followed by a maintenance dose of 300 mg every 24 hours thereafter. The IV formulation should be avoided in patients
with moderate or severe renal impairment (CrCl <50 mL/min) due to the potential for accumulation of the betadex
sulfobutyl ether sodium (SBECD) vehicle, unless an assessment of the possible benefits and risks to the patient
justifies its use. If it is used in patients with renal impairment, serum creatinine should be monitored closely, and, if
increases occur, consideration should be given to changing to the extended-release tablet formulation of posaconazole
or to IV or oral isavuconazole. In patients who are able to take medications orally, we use posaconazole delayed-
release tablets, usually given with food, rather than the oral suspension because bioavailability with the tablets is much
better and it is easier for patients to take.
Isavuconazole is an alternative to posaconazole in patients who are intolerant of posaconazole or who cannot achieve
a therapeutic serum level of posaconazole. Because the IV formulation of isavuconazole is highly water soluble and
does not contain the SBECD vehicle, there are no known concerns about administering the IV formulation to patients
with renal impairment. Isavuconazole should be given as a loading dose of 200 mg (equivalent to 372 mg of the
prodrug isavuconazonium sulfate) IV or orally every 8 hours for the first six doses followed by 200 mg IV or orally
every 24 hours thereafter.
The clinical efficacy of the oral suspension of posaconazole was shown in a salvage study that enrolled 91 patients
who had failed or could not tolerate standard therapy [99]. Posaconazole led to complete or partial response in 60
percent of patients; 21 percent had stable disease. Although there are limitations to this salvage study, this series
supports a potential role for oral posaconazole for the treatment of mucormycosis refractory to standard therapy.
Duration of therapy — As noted above, patients can be switched from a lipid formulation of amphotericin B to
delayed-release posaconazole tablets for oral step-down therapy once a favorable clinical response has been
achieved, which usually takes several weeks.
Therapy should continue until there is clinical resolution of the signs and symptoms of infection, as well as resolution of
radiographic signs of active disease; therapy should also continue until reversal of underlying immunosuppression has
been achieved, when feasible [100]. Therapy often extends for months.
Other possible adjunctive therapies
Antifungals — Although the echinocandins (eg, caspofungin) have no in vitro activity against the agents of
mucormycosis [101-103], Rhizopus oryzae, the most common cause of mucormycosis, expresses the target enzymefor echinocandins, suggesting that these agents may have clinical utility [104]. In a retrospective study of 21 patients
with rhino-orbital mucormycosis and 20 patients with rhino-orbital-cerebral mucormycosis, all six patients who received
combination therapy with amphotericin B and an echinocandin had successful outcomes, defined as surviving and not
requiring hospice care, compared with only 14 of 31 patients who received amphotericin B monotherapy [105]. The
benefit of combination therapy was most pronounced among patients with cerebral involvement; all four patients who
received combination therapy survived compared with 4 of 16 patients who received amphotericin B monotherapy.
However, there are several limitations to the above observations. In addition to the limited number of patients, all
underwent surgical debridement, making it difficult to assess the impact of antifungal therapy on outcomes. The
patients who received an echinocandin were seen more recently than most of those who were treated with
amphotericin B alone. In addition, the patients were predominantly nonneutropenic. This may have influenced the
response to antifungal therapy because modulation of the host neutrophil response is postulated to occur when
echinocandins are used to treat infections with filamentous fungi [106,107].
At this time, larger studies are needed to establish whether combination therapy is beneficial [108]. We do not
recommend using the combination of a polyene and an echinocandin for the treatment of mucormycosis.
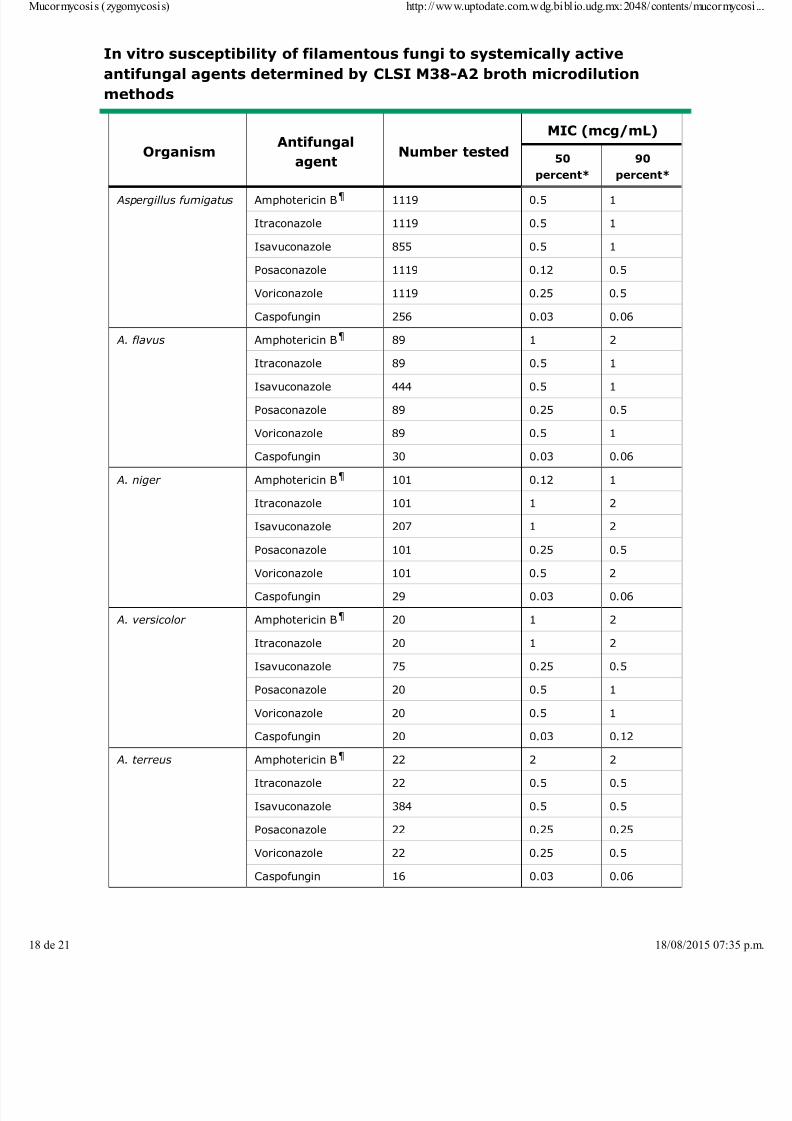
Other antifungal agents, including voriconazole, fluconazole, and flucytosine, are not effective against the Mucorales
(table 1) [94].
Deferasirox — In contrast with the iron chelator, deferoxamine, which increases the risk of mucormycosis, the oral
iron chelating agent, deferasirox, showed a possible benefit when used to treat mucormycosis in murine models. (See
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 9/21
'Deferoxamine and iron overload' above.)
The possible utility of deferasirox as an adjunctive therapy for mucormycosis has been evaluated in small studies, with
mixed results. In an open-label study of deferasirox in combination with antifungal therapy, seven of eight patients
survived [109]. In a small trial, 20 patients with proven or probable mucormycosis were randomly assigned to receive
either liposomal amphotericin B plus either deferasirox or placebo for the first 14 days of therapy [110]. Death at 90
days after therapy was initiated was significantly more frequent in those who received deferasirox than in those who
received placebo (82 versus 22 percent). Reported adverse events were similar between the groups. One possible
reason for the worse outcomes in the patients who received deferasirox is that more patients with hematologicmalignancy, neutropenia, and/or pulmonary involvement received this agent; all of these conditions are associated with
poor outcomes. Further study is necessary to determine the possible benefits or harms of deferasirox.
Hyperbaric oxygen — Hyperbaric oxygen has been used in some patients with mucormycosis, but the benefit of
this therapy has not been established [57,111,112].
OUTCOMES — Despite early diagnosis and aggressive combined surgical and medical therapy, the prognosis for
recovery from mucormycosis is poor (table 1). An exception is cutaneous involvement, which rarely disseminates.
Independent risk factors for mortality include disseminated infection, renal failure, and infection with Cunninghamella
species, while the use of surgery and administration of any antifungal agent were associated with a better outcome
[5].
Rhino-orbital-cerebral infection — A review of 208 patients with rhino-orbital-cerebral infection showed that the
most significant factors associated with death were delayed diagnosis, the presence of hemiparesis/hemiplegia,
bilateral sinus involvement, leukemia, renal disease, and treatment with deferoxamine [57]. Overall mortality from rhino-
orbital-cerebral mucormycosis ranges from 25 to 62 percent, with the best prognosis in patients with infection confined
to the sinuses [5]. The prognosis is especially poor for patients with brain, cavernous sinus, or carotid involvement,
although some patients with these complications have been cured of the infection [ 113-115].
Pulmonary mucormycosis — The outcome in patients with pulmonary mucormycosis is worse than for patients with
rhino-orbital-cerebral involvement, with mortality rates as high as 87 percent [5,32,60]. This may be in part due to the
underlying conditions and to the inability to widely excise the involved tissues. Widely disseminated mucormycosis
carries a mortality rate of 90 to 100 percent [5].
SUMMARY AND RECOMMENDATIONS
Mucormycosis is manifested by a variety of syndromes, particularly in immunocompromised patients and those
with diabetes mellitus. Devastating rhino-orbital-cerebral and pulmonary infections are the major syndromes
caused by these fungi. (See 'Introduction' above.)
●
Organisms in the order Mucorales are ubiquitous in nature and can be found on decaying vegetation and in the
soil. The genera most commonly found in human infections are Rhizopus, Mucor , and Rhizomucor ;
Cunninghamella, Saksenaea, and Apophysomyces are less commonly implicated in infection. (See 'Mycology'
above.)
●
Deferoxamine, which chelates both iron and aluminum, increases the risk of mucormycosis by enhancing growthand pathogenicity. The deferoxamine-iron chelate, called feroxamine, is a siderophore for the species Rhizopus,
increasing iron uptake by the fungus, which stimulates fungal growth and leads to tissue invasion. (See
'Deferoxamine and iron overload' above.)
●
Mucormycosis is characterized by infarction and necrosis of host tissues that results from invasion of the
vasculature by hyphae. The most common clinical presentation of mucormycosis is rhino-orbital-cerebral
infection, which is presumed to start with inhalation of spores into the paranasal sinuses of a susceptible host.
(See 'Clinical presentation' above and 'Rhino-orbital-cerebral mucormycosis' above.)
●
Pulmonary mucormycosis is a rapidly progressive infection that occurs after inhalation of spores into the
bronchioles and alveoli. Pneumonia with infarction and necrosis results, and the infection can spread to
●
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0
7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 10/21
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
Kauffman CA, Malani AN. Zygomycosis: an emerging fungal infection with new options for management. Curr
Infect Dis Rep 2007; 9:435.
1.
Spellberg B, Walsh TJ, Kontoyiannis DP, et al. Recent advances in the management of mucormycosis: from2.
contiguous structures, such as the mediastinum and heart, or disseminate hematogenously to other organs.
Mucormycosis can also cause gastrointestinal, cutaneous, renal, and disseminated disease. (See 'Pulmonary
mucormycosis' above and 'Clinical presentation' above.)
The diagnosis of mucormycosis relies upon the identification of organisms in tissue by histopathology with culture
confirmation. However, culture often yields no growth, and histopathologic identification of an organism with a
structure typical of Mucorales may provide the only evidence of infection. A clinician must think of this entity in the
appropriate clinical setting and pursue invasive testing in order to establish a diagnosis as early as possible. (See
'Diagnosis' above.)
●
Treatment of mucormycosis involves a combination of surgical debridement of involved tissues and antifungal
therapy. Aggressive surgical debridement of involved tissues should be undertaken as soon as the diagnosis of
rhino-orbital-cerebral mucormycosis is suspected. Elimination of predisposing factors for infection, such as
hyperglycemia, metabolic acidosis, deferoxamine administration, and neutropenia, is also critical. (See
'Treatment' above and 'Surgery' above.)
●
The drug of choice for initial therapy of mucormycosis is a lipid formulation of amphotericin B. The usual starting
dose is 5 mg/kg daily of liposomal amphotericin B or amphotericin B lipid complex, and many clinicians will
increase the dose up as high as 10 mg/kg daily in an attempt to control this infection. (See 'Initial therapy' above.)
●
For patients who have responded to a lipid formulation of amphotericin B, posaconazole can be used for oral
step-down therapy. Isavuconazole is an alternative for patients who cannot take posaconazole. We continue
amphotericin B until the patient has shown signs of improvement; this usually takes several weeks. When
switching to oral posaconazole, we favor the use of posaconazole delayed-release tablets (300 mg every 12
hours on the first day, then 300 mg once daily) taken with food. We do not use the oral suspension of
posaconazole since it is not highly bioavailable and requires fatty food for absorption. Loading doses of 200 mg
(ie, two capsules) of oral isavuconazole (equivalent to 372 mg of isavuconazonium sulfate) should be given every
8 hours for six doses, followed by 200 mg orally once daily starting 12 to 24 hours after the last loading dose.
(See 'Step-down therapy' above.)
●
We use intravenous (IV) posaconazole as salvage therapy for patients who do not respond to or cannot tolerate
amphotericin B. IV posaconazole should be given as a loading dose of 300 mg IV every 12 hours on the first day,
followed by a maintenance dose of 300 mg every 24 hours thereafter. The IV formulation should be avoided in
patients with moderate or severe renal impairment (CrCl <50 mL/min) due to the potential for accumulation of the
cyclodextrin vehicle. In patients who are able to take medications orally, we use posaconazole delayed-release
tablets. The dose is 300 mg every 12 hours on the first day and then 300 mg once daily thereafter, taken with
food if possible. Isavuconazole is an alternative to posaconazole. Isavuconazole should be given as a loading
dose of 200 mg (equivalent to 372 mg of the prodrug isavuconazonium sulfate) IV or orally every 8 hours for the
first six doses followed by 200 mg IV or orally every 24 hours thereafter. (See 'Salvage therapy' above.)
●
Overall mortality from rhino-orbital-cerebral mucormycosis ranges from 25 to 62 percent, with the best prognosis
in patients with infection confined to the sinuses. The prognosis is especially poor for patients with brain,
cavernous sinus, or carotid involvement, although some patients with these complications have been cured of the
infection. The outcome in patients with pulmonary mucormycosis is worse than for patients with rhino-orbital-cerebral involvement, with mortality rates as high as 87 percent. (See 'Outcomes' above.)
●
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 11/21
bench to bedside. Clin Infect Dis 2009; 48:1743.
Hibbett DS, Binder M, Bischoff JF, et al. A higher-level phylogenetic classification of the Fungi. Mycol Res 2007;
111:509.
3.
Kwon-Chung KJ. Taxonomy of fungi causing mucormycosis and entomophthoramycosis (zygomycosis) and
nomenclature of the disease: molecular mycologic perspectives. Clin Infect Dis 2012; 54 Suppl 1:S8.
4.
Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929
reported cases. Clin Infect Dis 2005; 41:634.
5.
GALE GR, WELCH AM. Studies of opportunistic fungi. I. Inhibition of Rhizopus oryzae by human serum. Am J
Med Sci 1961; 241:604.
6.
Ferguson BJ. Mucormycosis of the nose and paranasal sinuses. Otolaryngol Clin North Am 2000; 33:349.7.
Greenberg RN, Scott LJ, Vaughn HH, Ribes JA. Zygomycosis (mucormycosis): emerging clinical importance and
new treatments. Curr Opin Infect Dis 2004; 17:517.
8.
Boelaert JR, Van Cutsem J, de Locht M, et al. Deferoxamine augments growth and pathogenicity of Rhizopus,
while hydroxypyridinone chelators have no effect. Kidney Int 1994; 45:667.
9.
de Locht M, Boelaert JR, Schneider YJ. Iron uptake from ferrioxamine and from ferrirhizoferrin by germinating
spores of Rhizopus microsporus. Biochem Pharmacol 1994; 47:1843.
10.
Boelaert JR, Fenves AZ, Coburn JW. Deferoxamine therapy and mucormycosis in dialysis patients: report of an
international registry. Am J Kidney Dis 1991; 18:660.
11.
Boelaert JR, de Locht M, Van Cutsem J, et al. Mucormycosis during deferoxamine therapy is a siderophore-mediated infection. In vitro and in vivo animal studies. J Clin Invest 1993; 91:1979.
12.
Maertens J, Demuynck H, Verbeken EK, et al. Mucormycosis in allogeneic bone marrow transplant recipients:
report of five cases and review of the role of iron overload in the pathogenesis. Bone Marrow Transplant 1999;
24:307.
13.
Ibrahim AS, Spellberg B, Walsh TJ, Kontoyiannis DP. Pathogenesis of mucormycosis. Clin Infect Dis 2012; 54
Suppl 1:S16.
14.
Artis WM, Fountain JA, Delcher HK, Jones HE. A mechanism of susceptibility to mucormycosis in diabetic
ketoacidosis: transferrin and iron availability. Diabetes 1982; 31:1109.
15.
Ibrahim AS, Edwards JE Jr, Fu Y, Spellberg B. Deferiprone iron chelation as a novel therapy for experimental
mucormycosis. J Antimicrob Chemother 2006; 58:1070.
16.
Ibrahim AS, Gebermariam T, Fu Y, et al. The iron chelator deferasirox protects mice from mucormycosis throughiron starvation. J Clin Invest 2007; 117:2649.
17.
McNulty JS. Rhinocerebral mucormycosis: predisposing factors. Laryngoscope 1982; 92:1140.18.
Lee FY, Mossad SB, Adal KA. Pulmonary mucormycosis: the last 30 years. Arch Intern Med 1999; 159:1301.19.
Ismail MH, Hodkinson HJ, Setzen G, et al. Gastric mucormycosis. Trop Gastroenterol 1990; 11:103.20.
Adam RD, Hunter G, DiTomasso J, Comerci G Jr. Mucormycosis: emerging prominence of cutaneous infections.
Clin Infect Dis 1994; 19:67.
21.
Cocanour CS, Miller-Crotchett P, Reed RL 2nd, et al. Mucormycosis in trauma patients. J Trauma 1992; 32:12.22.
Levy E, Bia MJ. Isolated renal mucormycosis: case report and review. J Am Soc Nephrol 1995; 5:2014.23.
Nagy-Agren SE, Chu P, Smith GJ, et al. Zygomycosis (mucormycosis) and HIV infection: report of three cases
and review. J Acquir Immune Defic Syndr Hum Retrovirol 1995; 10:441.
24.
Kontoyiannis DP, Wessel VC, Bodey GP, Rolston KV. Zygomycosis in the 1990s in a tertiary-care cancer center.
Clin Infect Dis 2000; 30:851.
25.
Marr KA, Carter RA, Crippa F, et al. Epidemiology and outcome of mould infections in hematopoietic stem cell
transplant recipients. Clin Infect Dis 2002; 34:909.
26.
Kontoyiannis DP, Lionakis MS, Lewis RE, et al. Zygomycosis in a tertiary-care cancer center in the era of
Aspergillus-active antifungal therapy: a case-control observational study of 27 recent cases. J Infect Dis 2005;
191:1350.
27.
Kontoyiannis DP. Decrease in the number of reported cases of zygomycosis among patients with diabetes
mellitus: a hypothesis. Clin Infect Dis 2007; 44:1089.
28.
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0
7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 12/21
Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect
Dis 2012; 54 Suppl 1:S23.
29.
Trifilio SM, Bennett CL, Yarnold PR, et al. Breakthrough zygomycosis after voriconazole administration among
patients with hematologic malignancies who receive hematopoietic stem-cell transplants or intensive
chemotherapy. Bone Marrow Transplant 2007; 39:425.
30.
Lanternier F, Sun HY, Ribaud P, et al. Mucormycosis in organ and stem cell transplant recipients. Clin Infect Dis
2012; 54:1629.
31.
Almyroudis NG, Sutton DA, Linden P, et al. Zygomycosis in solid organ transplant recipients in a tertiary
transplant center and review of the literature. Am J Transplant 2006; 6:2365.
32.
Aslani J, Eizadi M, Kardavani B, et al. Mucormycosis after kidney transplantations: report of seven cases. Scand
J Infect Dis 2007; 39:703.
33.
Singh N, Aguado JM, Bonatti H, et al. Zygomycosis in solid organ transplant recipients: a prospective, matched
case-control study to assess risks for disease and outcome. J Infect Dis 2009; 200:1002.
34.
Lanternier F, Dannaoui E, Morizot G, et al. A global analysis of mucormycosis in France: the RetroZygo Study
(2005-2007). Clin Infect Dis 2012; 54 Suppl 1:S35.
35.
Cornely OA, Maertens J, Winston DJ, et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients
with neutropenia. N Engl J Med 2007; 356:348.
36.
Bitar D, Van Cauteren D, Lanternier F, et al. Increasing incidence of zygomycosis (mucormycosis), France,
1997-2006. Emerg Infect Dis 2009; 15:1395.
37.
Nucci M, Marr KA. Emerging fungal diseases. Clin Infect Dis 2005; 41:521.38.
Park BJ, Pappas PG, Wannemuehler KA, et al. Invasive non-Aspergillus mold infections in transplant recipients,
United States, 2001-2006. Emerg Infect Dis 2011; 17:1855.
39.
Chakrabarti A, Das A, Mandal J, et al. The rising trend of invasive zygomycosis in patients with uncontrolled
diabetes mellitus. Med Mycol 2006; 44:335.
40.
Rammaert B, Lanternier F, Zahar JR, et al. Healthcare-associated mucormycosis. Clin Infect Dis 2012; 54 Suppl
1:S44.
41.
Duffy J, Harris J, Gade L, et al. Mucormycosis outbreak associated with hospital linens. Pediatr Infect Dis J
2014; 33:472.
42.
Kanamori H, Rutala WA, Sickbert-Bennett EE, Weber DJ. Review of Fungal Outbreaks and Infection Prevention
in Healthcare Settings During Construction and Renovation. Clin Infect Dis 2015; 61:433.
43.
Vallabhaneni S, Walker TA, Lockhart SR, et al. Notes from the field: Fatal gastrointestinal mucormycosis in a
premature infant associated with a contaminated dietary supplement--Connecticut, 2014. MMWR Morb Mortal
Wkly Rep 2015; 64:155.
44.
Notes from the field: fatal fungal soft-tissue infections after a tornado --- Joplin, Missouri, 2011. MMWR Morb
Mortal Wkly Rep 2011; 60:992.
45.
Andresen D, Donaldson A, Choo L, et al. Multifocal cutaneous mucormycosis complicating polymicrobial wound
infections in a tsunami survivor from Sri Lanka. Lancet 2005; 365:876.
46.
Patiño JF, Castro D, Valencia A, Morales P. Necrotizing soft tissue lesions after a volcanic cataclysm. World J
Surg 1991; 15:240.
47.
Neblett Fanfair R, Benedict K, Bos J, et al. Necrotizing cutaneous mucormycosis after a tornado in Joplin,
Missouri, in 2011. N Engl J Med 2012; 367:2214.
48.
Benedict K, Park BJ. Invasive fungal infections after natural disasters. Emerg Infect Dis 2014; 20:349.49.
Warkentien T, Rodriguez C, Lloyd B, et al. Invasive mold infections following combat-related injuries. Clin Infect
Dis 2012; 55:1441.
50.
Harril WC, Stewart MG, Lee AG, Cernoch P. Chronic rhinocerebral mucormycosis. Laryngoscope 1996;
106:1292.
51.
Xia ZK, Wang WL, Yang RY. Slowly progressive cutaneous, rhinofacial, and pulmonary mucormycosis caused by
Mucor irregularis in an immunocompetent woman. Clin Infect Dis 2013; 56:993.
52.
Radner AB, Witt MD, Edwards JE Jr. Acute invasive rhinocerebral zygomycosis in an otherwise healthy patient:
case report and review. Clin Infect Dis 1995; 20:163.
53.
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 13/21
Del Valle Zapico A, Rubio Suárez A, Mellado Encinas P, et al. Mucormycosis of the sphenoid sinus in an
otherwise healthy patient. Case report and literature review. J Laryngol Otol 1996; 110:471.
54.
Elinav H, Zimhony O, Cohen MJ, et al. Rhinocerebral mucormycosis in patients without predisposing medical
conditions: a review of the literature. Clin Microbiol Infect 2009; 15:693.
55.
Rajagopalan S. Serious infections in elderly patients with diabetes mellitus. Clin Infect Dis 2005; 40:990.56.
Yohai RA, Bullock JD, Aziz AA, Markert RJ. Survival factors in rhino-orbital-cerebral mucormycosis. Surv
Ophthalmol 1994; 39:3.
57.
Connor BA, Anderson RJ, Smith JW. Mucor mediastinitis. Chest 1979; 75:525.58.
Helenglass G, Elliott JA, Lucie NP. An unusual presentation of opportunistic mucormycosis. Br Med J (Clin Res
Ed) 1981; 282:108.
59.
Tedder M, Spratt JA, Anstadt MP, et al. Pulmonary mucormycosis: results of medical and surgical therapy. Ann
Thorac Surg 1994; 57:1044.
60.
Brown RB, Johnson JH, Kessinger JM, Sealy WC. Bronchovascular mucormycosis in the diabetic: an urgent
surgical problem. Ann Thorac Surg 1992; 53:854.
61.
Murphy RA, Miller WT Jr. Pulmonary mucormycosis. Semin Roentgenol 1996; 31:83.62.
al-Abbadi MA, Russo K, Wilkinson EJ. Pulmonary mucormycosis diagnosed by bronchoalveolar lavage: a case
report and review of the literature. Pediatr Pulmonol 1997; 23:222.
63.
Latif S, Saffarian N, Bellovich K, Provenzano R. Pulmonary mucormycosis in diabetic renal allograft recipients.
Am J Kidney Dis 1997; 29:461.
64.
Chavanet P, Lefranc T, Bonnin A, et al. Unusual cause of pharyngeal ulcerations in AIDS. Lancet 1990; 336:383.65.
Agha FP, Lee HH, Boland CR, Bradley SF. Mucormycoma of the colon: early diagnosis and successful
management. AJR Am J Roentgenol 1985; 145:739.
66.
Martinez EJ, Cancio MR, Sinnott JT 4th, et al. Nonfatal gastric mucormycosis in a renal transplant recipient.
South Med J 1997; 90:341.
67.
Cheng VC, Chan JF, Ngan AH, et al. Outbreak of intestinal infection due to Rhizopus microsporus. J Clin
Microbiol 2009; 47:2834.
68.
Corey KE, Gupta NK, Agarwal S, Xiao HD. Case records of the Massachusetts General Hospital. Case
32-2013. A 55-year-old woman with autoimmune hepatitis, cirrhosis, anorexia, and abdominal pain. N Engl J Med
2013; 369:1545.
69.
Hosseini M, Lee J. Gastrointestinal mucormycosis mimicking ischemic colitis in a patient with systemic lupus
erythematosus. Am J Gastroenterol 1998; 93:1360.
70.
Linder N, Keller N, Huri C, et al. Primary cutaneous mucormycosis in a premature infant: case report and review
of the literature. Am J Perinatol 1998; 15:35.
71.
Chakrabarti A, Kumar P, Padhye AA, et al. Primary cutaneous zygomycosis due to Saksenaea vasiformis and
Apophysomyces elegans. Clin Infect Dis 1997; 24:580.
72.
Wirth F, Perry R, Eskenazi A, et al. Cutaneous mucormycosis with subsequent visceral dissemination in a child
with neutropenia: a case report and review of the pediatric literature. J Am Acad Dermatol 1997; 36:336.
73.
Weinberg WG, Wade BH, Cierny G 3rd, et al. Invasive infection due to Apophysomyces elegans in
immunocompetent hosts. Clin Infect Dis 1993; 17:881.
74.
Arnáiz-García ME, Alonso-Peña D, González-Vela Mdel C, et al. Cutaneous mucormycosis: report of five casesand review of the literature. J Plast Reconstr Aesthet Surg 2009; 62:e434.75.
Weng DE, Wilson WH, Little R, Walsh TJ. Successful medical management of isolated renal zygomycosis: case
report and review. Clin Infect Dis 1998; 26:601.
76.
Langston C, Roberts DA, Porter GA, Bennett WM. Renal phycomycosis. J Urol 1973; 109:941.77.
Melnick JZ, Latimer J, Lee El, Henrich WL. Systemic mucormycosis complicating acute renal failure: case report
and review of the literature. Ren Fail 1995; 17:619.
78.
Siddiqi SU, Freedman JD. Isolated central nervous system mucormycosis. South Med J 1994; 87:997.79.
Hopkins RJ, Rothman M, Fiore A, Goldblum SE. Cerebral mucormycosis associated with intravenous drug use:
three case reports and review. Clin Infect Dis 1994; 19:1133.
80.
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 14/21
Stave GM, Heimberger T, Kerkering TM. Zygomycosis of the basal ganglia in intravenous drug users. Am J Med
1989; 86:115.
81.
Sanchez MR, Ponge-Wilson I, Moy JA, Rosenthal S. Zygomycosis and HIV infection. J Am Acad Dermatol 1994;
30:904.
82.
Machouart M, Larché J, Burton K, et al. Genetic identification of the main opportunistic Mucorales by
PCR-restriction fragment length polymorphism. J Clin Microbiol 2006; 44:805.
83.
Hammond SP, Bialek R, Milner DA, et al. Molecular methods to improve diagnosis and identification of
mucormycosis. J Clin Microbiol 2011; 49:2151.
84.
Walsh TJ, Gamaletsou MN, McGinnis MR, et al. Early clinical and laboratory diagnosis of invasive pulmonary,
extrapulmonary, and disseminated mucormycosis (zygomycosis). Clin Infect Dis 2012; 54 Suppl 1:S55.
85.
Saltoğlu N, Taşova Y, Zorludemir S, Dündar IH. Rhinocerebral zygomycosis treated with liposomal amphotericin
B and surgery. Mycoses 1998; 41:45.
86.
Chamilos G, Marom EM, Lewis RE, et al. Predictors of pulmonary zygomycosis versus invasive pulmonary
aspergillosis in patients with cancer. Clin Infect Dis 2005; 41:60.
87.
Wahba H, Truong MT, Lei X, et al. Reversed halo sign in invasive pulmonary fungal infections. Clin Infect Dis
2008; 46:1733.
88.
Georgiadou SP, Sipsas NV, Marom EM, Kontoyiannis DP. The diagnostic value of halo and reversed halo signs
for invasive mold infections in compromised hosts. Clin Infect Dis 2011; 52:1144.
89.
Legouge C, Caillot D, Chrétien ML, et al. The reversed halo sign: pathognomonic pattern of pulmonarymucormycosis in leukemic patients with neutropenia? Clin Infect Dis 2014; 58:672.90.
McCarthy M, Rosengart A, Schuetz AN, et al. Mold infections of the central nervous system. N Engl J Med 2014;
371:150.
91.
Gonzalez CE, Couriel DR, Walsh TJ. Disseminated zygomycosis in a neutropenic patient: successful treatment
with amphotericin B lipid complex and granulocyte colony-stimulating factor. Clin Infect Dis 1997; 24:192.
92.
Chamilos G, Lewis RE, Kontoyiannis DP. Delaying amphotericin B-based frontline therapy significantly increases
mortality among patients with hematologic malignancy who have zygomycosis. Clin Infect Dis 2008; 47:503.
93.
Spanakis EK, Aperis G, Mylonakis E. New agents for the treatment of fungal infections: clinical efficacy and
gaps in coverage. Clin Infect Dis 2006; 43:1060.
94.
Sun QN, Fothergill AW, McCarthy DI, et al. In vitro activities of posaconazole, itraconazole, voriconazole,
amphotericin B, and fluconazole against 37 clinical isolates of zygomycetes. Antimicrob Agents Chemother 2002;46:1581.
95.
Thompson GR 3rd, Wiederhold NP. Isavuconazole: a comprehensive review of spectrum of activity of a new
triazole. Mycopathologia 2010; 170:291.
96.
Noxafil (posaconazole). Highlights of prescribing information. https://www.merck.com/product/usa/pi_circulars
/n/noxafil/noxafil_pi.pdf (Accessed on March 18, 2014).
97.
CRESEMBA (isavuconazonium sulfate). Highlights of prescribing information. http://www.accessdata.fda.gov
/drugsatfda_docs/label/2015/207500Orig1s000lbl.pdf (Accessed on March 09, 2015).
98.
van Burik JA, Hare RS, Solomon HF, et al. Posaconazole is effective as salvage therapy in zygomycosis: a
retrospective summary of 91 cases. Clin Infect Dis 2006; 42:e61.
99.
Kontoyiannis DP, Lewis RE. How I treat mucormycosis. Blood 2011; 118:1216.100.
Espinel-Ingroff A. Comparison of In vitro activities of the new triazole SCH56592 and the echinocandins MK-0991(L-743,872) and LY303366 against opportunistic filamentous and dimorphic fungi and yeasts. J Clin Microbiol
1998; 36:2950.
101.
Pfaller MA, Marco F, Messer SA, Jones RN. In vitro activity of two echinocandin derivatives, LY303366 and
MK-0991 (L-743,792), against clinical isolates of Aspergillus, Fusarium, Rhizopus, and other filamentous fungi.
Diagn Microbiol Infect Dis 1998; 30:251.
102.
Del Poeta M, Schell WA, Perfect JR. In vitro antifungal activity of pneumocandin L-743,872 against a variety of
clinically important molds. Antimicrob Agents Chemother 1997; 41:1835.
103.
Ibrahim AS, Bowman JC, Avanessian V, et al. Caspofungin inhibits Rhizopus oryzae 1,3-beta-D-glucan synthase,
lowers burden in brain measured by quantitative PCR, and improves survival at a low but not a high dose during
murine disseminated zygomycosis. Antimicrob Agents Chemother 2005; 49:721.
104.
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 15/21
Reed C, Bryant R, Ibrahim AS, et al. Combination polyene-caspofungin treatment of rhino-orbital-cerebral
mucormycosis. Clin Infect Dis 2008; 47:364.
105.
Walsh TJ, Kontoyiannis DP. Editorial commentary: what is the role of combination therapy in management of
zygomycosis? Clin Infect Dis 2008; 47:372.
106.
Lamaris GA, Lewis RE, Chamilos G, et al. Caspofungin-mediated beta-glucan unmasking and enhancement of
human polymorphonuclear neutrophil activity against Aspergillus and non-Aspergillus hyphae. J Infect Dis 2008;
198:186.
107.
Spellberg B, Ibrahim A, Roilides E, et al. Combination therapy for mucormycosis: why, what, and how? Clin
Infect Dis 2012; 54 Suppl 1:S73.
108.
Spellberg B, Andes D, Perez M, et al. Safety and outcomes of open-label deferasirox iron chelation therapy for
mucormycosis. Antimicrob Agents Chemother 2009; 53:3122.
109.
Spellberg B, Ibrahim AS, Chin-Hong PV, et al. The Deferasirox-AmBisome Therapy for Mucormycosis (DEFEAT
Mucor) study: a randomized, double-blinded, placebo-controlled trial. J Antimicrob Chemother 2012; 67:715.
110.
Ferguson BJ, Mitchell TG, Moon R, et al. Adjunctive hyperbaric oxygen for treatment of rhinocerebral
mucormycosis. Rev Infect Dis 1988; 10:551.
111.
Bentur Y, Shupak A, Ramon Y, et al. Hyperbaric oxygen therapy for cutaneous/soft-tissue zygomycosis
complicating diabetes mellitus. Plast Reconstr Surg 1998; 102:822.
112.
Strasser MD, Kennedy RJ, Adam RD. Rhinocerebral mucormycosis. Therapy with amphotericin B lipid complex.
Arch Intern Med 1996; 156:337.
113.
Weprin BE, Hall WA, Goodman J, Adams GL. Long-term survival in rhinocerebral mucormycosis. Case report. J
Neurosurg 1998; 88:570.
114.
Shah PD, Peters KR, Reuman PD. Recovery from rhinocerebral mucormycosis with carotid artery occlusion: a
pediatric case and review of the literature. Pediatr Infect Dis J 1997; 16:68.
115.
Topic 2465 Version 28.0
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 16/21
GRAPHICS
Rhizopus arrhizus hyphae in lung tissue
Hyphae in lung tissue, hematoxylin and eosin stain.
Courtesy of www.doctorfungus.org. Copyright ©2007.
Graphic 66476 Version 2.0
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 17/21
Pulmonary mucormycosis in a lung transplant
recipient
(A) Computed tomography (CT) scan of lung showing pulmonary nodule
and (B) fine needle aspiration of right lower lobe of lung showing
aseptate hyphae (Papanicolaou stain, x400).
Reproduced with permission from: Silveira FP, Husain S. Fungal infections in
lung transplant recipients. Curr Opin Pulm Med 2008; 14:211. Copyright ©
2008 Lippincott Williams & Wilkins.
Graphic 71447 Version 14.0
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0
7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 18/21
In vitro susceptibility of filamentous fungi to systemically active
antifungal agents determined by CLSI M38-A2 broth microdilution
methods
OrganismAntifungal
agentNumber tested
MIC (mcg/mL)
50
percent*
90
percent*
Aspergillus fumigatus Amphotericin B 1119 0.5 1
Itraconazole 1119 0.5 1
Isavuconazole 855 0.5 1
Posaconazole 1119 0.12 0.5
Voriconazole 1119 0.25 0.5
Caspofungin 256 0.03 0.06
A. flavus Amphotericin B 89 1 2
Itraconazole 89 0.5 1
Isavuconazole 444 0.5 1
Posaconazole 89 0.25 0.5
Voriconazole 89 0.5 1
Caspofungin 30 0.03 0.06
A. niger Amphotericin B 101 0.12 1
Itraconazole 101 1 2
Isavuconazole 207 1 2
Posaconazole 101 0.25 0.5
Voriconazole 101 0.5 2
Caspofungin 29 0.03 0.06
A. versicolor Amphotericin B 20 1 2
Itraconazole 20 1 2
Isavuconazole 75 0.25 0.5
Posaconazole 20 0.5 1
Voriconazole 20 0.5 1
Caspofungin 20 0.03 0.12
A. terreus Amphotericin B 22 2 2
Itraconazole 22 0.5 0.5
Isavuconazole 384 0.5 0.5
Posaconazole 22 0.25 0.25
Voriconazole 22 0.25 0.5
Caspofungin 16 0.03 0.06
¶
¶
¶
¶
¶
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 19/21
Fusarium spp Amphotericin B 67 8 32
Itraconazole 67 16 32
Isavuconazole 20 16 >16
Posaconazole 67 16 32
Voriconazole 67 16 32
Caspofungin 13 >8 >8
Scedosporium
apiospermum
Amphotericin B 26 2 8
Itraconazole 26 1 32
Isavuconazole 16 4 4
Posaconazole 26 0.25 1
Voriconazole 13 0.12 0.25
Micafungin 36 >16 >16
S. prolificans Amphotericin B 80 16 32
Itraconazole 80 64 64
Isavuconazole 6 16 -
Posaconazole 80 16 32
Voriconazole 55 4 4
Micafungin 17 >32 >32
Mucorales Amphotericin B 86 0.25 2
Itraconazole 86 1 32
Isavuconazole 45 2 16
Posaconazole 86 0.5 4
Voriconazole 86 16 128
CLSI: Clinical and Laboratory Standards Institute; MIC: minimum inhibitory concentration.
* 50 percent and 90 percent; MIC encompassing 50 percent and 90 percent of isolates tested, respectively.
¶ Amphotericin B MICs determined by Etest.
Data from:
Sabatelli F, Patel R, Mann PA, et al. In vitro activities of posaconazole, fluconazole, itraconazole,
voriconazole, and amphotericin B against a large collection of clinically important molds and yeasts.
Antimicrob Agents Chemother 2006; 50:2009.
1.
Diekema DJ, Messer SA, Hollis RJ, et al. Activities of caspofungin, itraconazole, posaconazole,
ravuconazole, voriconazole, and amphotericin B against 448 recent clinical isolates of filamentousfungi. J Clin Microbiol 2003; 41:3623.
2.
Pfaller MA, Messer SA, Boyken L, et al. In vitro survey of triazole cross-resistance among more than
700 clinical isolates of Aspergillus species. J Clin Microbiol 2008; 46:2568.
3.
Cortez KJ, Roilides E, Quiroz-Telles F, et al. Infections caused by Scedosporium spp. Clin Microbiol
Rev 2008; 21:157.
4.
Espinel-Ingroff A, Chowdhary A, Gonzalez GM, et al. Multicenter study of isavuconazole MIC
distributions and epidemiological cutoff values for Aspergillus spp. for the CLSI M38-A2 broth
microdilution method. Antimicrob Agents Chemother 2013; 57:3823.
5.
Guinea J, Pelaez T, Recio S, et al. In vitro antifungal activities of isavuconazole (BAL4815),
voriconazole, and fluconazole against 1,007 isolates of zygomycete, Candida, Aspergillus, Fusarium,
6.
¶
¶
¶
¶
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 20/21
and Scedosporium species. Antimicrob Agents Chemother 2008; 52: 1396.
Graphic 82439 Version 8.0
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco
21 18/08/2015 0

7/23/2019 Mucormicosis (zygomicosis)
http://slidepdf.com/reader/full/mucormicosis-zygomicosis 21/21
Disclosures: Gary M Cox, MD Nothing to disclose. Carol A Kauffman, MD Nothing to disclose. Anna R Thorner, MD Nothing to disclose.
Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through amulti-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content isrequired of all authors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Disclosures
rmycosis (zygomycosis) http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/muco