morphology and clinical outcomes of embryos after in vitro fertilization are superior to those after...
TRANSCRIPT

FERTILITY AND STERILITY@
Copyright o 1997 American Smiety for Reproductive Medicine
Published by Elsevier Science Inc.
Vol. 68, No. 4, October 1997
Printed on acid-free paper in U. S. A.
Morphology and clinical outcomes of embryos after in vitro fertilization are superior to those after intracytoplasmic sperm injection
Itai Bar-Hava, M.D. Masha Brengauz, M.Sc. Jacob Ashkenazi, M.D. Dov Feldberg, M.D. Michal Shelef, M.Sc. Raoul Orvieto, M.D. Ariela Schwartz, M.Sc. Zion Ben-Rafael, M.D.*
Department of Obstetrics and Gynecology, Rabin Medical Center (Golda Campus), Petah-Tikva; and Suckler Faculty of Medicine,
Tel Aviv University, Tel Aviv, Israel
Objective: To compare embryos obtained after M? and intracytoplasmic sperm injection (ICSI) regarding morphology and the likelihood of achieving clinical pregnancy.
Design: Case-control study. Setting: An lVF unit controlling 1,310 cycles in 1996. Patient(s): Women having a total of 477 IVF and 475 ICSI consecutive cycles. Intervention(s): Ovarian stimulation, IVF-ET, or ICSI-ET for all couples. Main Outcome Measure(s): Number of grade-A embryos transferred, preclinical pregnancy
losses, and clinical pregnancy rates in IVF and ICSI cycles. Result(s): In comparison with the ICSI group, the IVF group showed significantly more
grade-A embryos available for transfer (mean, 2 2 1.6 versus 1.8 + 1.5), significantly fewer preclinical pregnancy losses (1.6% versus 4%), and significantly higher clinical pregnancy rates (25% versus 19.1%).
Conclusion(s): Embryos obtained after IVF are superior to those obtained after ICSI in relation to embryo morphology and the likelihood of achieving clinical pregnancy. (Fertil SteriP 1997;68:653-7. 0 1997 by American Society for Reproductive Medicine.)
Key Words: lVF, ICSI, embryo morphology, pregnancy
In recent years, intracytoplasmic sperm injection (ICSI) has gained tremendous popularity in assisted reproductive technology (ART) units throughout the world. The ICSI procedure is currently being used to assist in solving two main problems: severe male factor infertility and fertilization failure or low fer- tilization in previous standard M? procedures.
It is commonly believed that embryos obtained after ICSI are comparable (l), or even superior (2, 3), to those obtained after standard IVF’. However, because of the lack of natural selection of sperm and the circumvention of most of the known fertilization stages, concerns regarding the subsequent embryo
Received March 18, 1997; revised and accepted June 2, 1997. * Reprint requests: Zion Ben-Rafael, M.D., Department of Ob-
stetrics and Gynecology, Rabin Medical Center, Beilinson Cam- pus, Petah Tikva 49100, Israel (FAX: 972-3-9211660).
0015-0282/97/$17.00 PI1 SOO15-0282(97)00265-3
quality and pregnancy outcome have been ex- pressed. The aim of this study was to compare IW and ICSI embryos in terms of embryo morphology, preimplantation pregnancy losses, and clinical preg- nancy rates (PRs).
MAmRIALS AND METHODS
The ICSI procedure was performed initially in our department in June 1994. Since then, 7,150 M2 ova have been injected in our laboratory. All consecu- tively seen patients who reached the stage of ET between January 1, 1996 and December 22, 1996 were included in this study. Exclusion criteria in- cluded the following: cases in which both ICSI and standard IW were applied on sibling oocytes during the same cycle and both kinds of embryos were transferred; cycles in which sperm were obtained by electroejaculation or epididymal or testicular aspira-
653

tion; cycles in which donor oocytes were used or fro- zen-thawed embryos were transferred; and cycles in which the embryos were transferred at the 2 pronu- clei (2PN) stage.
Intracytoplasmic sperm injection was performed whenever the couple fulfilled one of the following criteria: [ll poor semen characteristics (<5 x lo6 total motile sperm in the ejaculate before pro- cessing); or 121 <30% fertilization rate in a previous standard IVF cycle. Ovarian stimulation, oocyte re- covery, embryo culture procedures, and ET tech- niques were similar in the IVF and ICSI cycles. Follicular development was monitored by serial hor- mone and ultrasound (US) measurements. A lO,OOO- IU dose of hCG (Chorigon; Tevapharma, Petah Tikva, Israel) was injected when at least two follicles had reached a diameter of 18 mm, and follicular as- piration was conducted under transvaginal US guid- ance 34-36 hours later.
of <1 x lO?mL>. The pellet was then resuspended to 0.5 mL and subsequently centrifuged in a flushing medium (1070; Medicult) for 20 minutes at 300 X g in a discontinuous Percoll gradient (95%, 70%, and 50%). Thereafter, the pellet was recentrifuged twice with flushing medium, at a speed in accordance with the initial sperm count, and incubated with a me- dium layer of ~0.1 mL for up to 3 hours.
When ICSI was carried out after oocyte retrieval, the oocytes were exposed briefly to 80 IU/mL hyaluronidase in HEPES-buffered Earle’s balanced salt solution (Catalog no. 1011; Medicult, Copenha- gen, Denmark) and mechanically cleaned of their surrounding cumulus cells by aspiration through a glass pipette with an inner diameter of 200 pm. The denuded oocytes were washed five times in a flush- ing medium (Catalog no. 1084; Medicult) supple- mented with 10% synthetic serum substitute (Irvine Scientific, Irvine, CA). These procedures were all performed in a 3004 Petri dish (Falcon, Plymouth, United Kingdom) under paraffin oil (Catalog no. 1010; Medicult) in 100~yL droplets. All oocytes then were examined under an inverted microscope (La- bovert FS Leitz, Wetzlar, Germany) at a magnifica- tion of x400, and those in which a first polar body was present were selected for micromanipulation.
Oocyte incubation before and after the ICSI proce- dure (and also after standard IVF) took place in 0.7 mL P-l medium, supplemented with 10% synthetic serum substitute, in four well-shaped dishes (176740; Nunc, Reskilde, Denmark) in an ambient atmosphere of 5% COZ. The use of expired media was avoided; the shelf-life of the medium was well below 30 days. Glucose and phosphate-free medium has been used in our laboratory since December 1995 because we (unpublished data) as well as other in- vestigators (4) have demonstrated better-quality embryos under these conditions.
Sperm were injected in a Petri dish cover (1006; Falcon, Lincoln Park, NJ) in 4-PL droplets (flushing medium supplemented with 10% synthetic serum substitute), each containing an individual oocyte, covered with paraffin oil. One droplet of medium was exchanged with 10% polyvinylpyrrolidone (1089; Medicult), and approximately 100 sperm cells/pL were added. The microinjection procedure was per- formed using an inverted-phase microscope (Labo- vert FS Leitz) that was equipped with a differential interference contrast, a heated stage, and a set of Leitz M micromanipulators. An IM 6 microinjector was used (Nikon Europe B.V., Amsterdam, The Netherlands) equipped with injection and hold- ing micropipettes (Humagen Fertility Diagnostics, Charlottesville, VA).
The injection micropipette was lowered in the polyvinylpyrrolidone, and the best morphologically normal motile spermatozoon was chosen and immo- bilized by touching its tail near the midpiece with the injection micropipette. The immobilized sperma- tozoon was aspirated, tail first, into the injection pi- pette. After the oocyte was secured in position with the holding pipette (polar body at the 6-o’clock posi- tion), the injection pipette was introduced at the 3- o’clock position, through the zona pellucida and the oolemma, until it reached up to two thirds of the cytoplasm, and then was withdrawn to the center. Thereafter, some of the cytoplasm was aspirated to verify that the oolemma had been broken, and the spermatozoon then was injected slowly. In cases of standard IVF, up to five oocytes were inseminated with approximately 70,000 sperm cells/ml in each well.
The following morning, the oocytes were examined for evidence of fertilization. Embryo quality was graded before ET; embryos with equal-sized blasto- meres and < 10% fragmentation were defined as be- ing grade A. Cleaving embryos were selected for transfer or freezing on the basis of their morphologic score.
Semen samples were obtained by masturbation Embryos were replaced transcervically into the and collected before ovum collection. Sperm density uterus either 2 or 3 days after the day of insemina- and motility were evaluated by World Health Orga- tion with use of a Wallace catheter (Simcare Ltd., nization criteria (5). After complete liquefaction, the Lancing, West Sussex, United Kingdom). All em- sperm were washed once with flushing medium (at bryos were left in culture until the day of ET. A 300 X g for 5 minutes for a sperm count of >1 X preclinical (chemical) pregnancy loss was defined lO?mL and at 1,800 X g for 5 minutes for a count as one or more serum hCG concentrations of
654 Bar-Hava et al. ZVF embryos versus embryos after ZCSZ Fertility and Sterility@
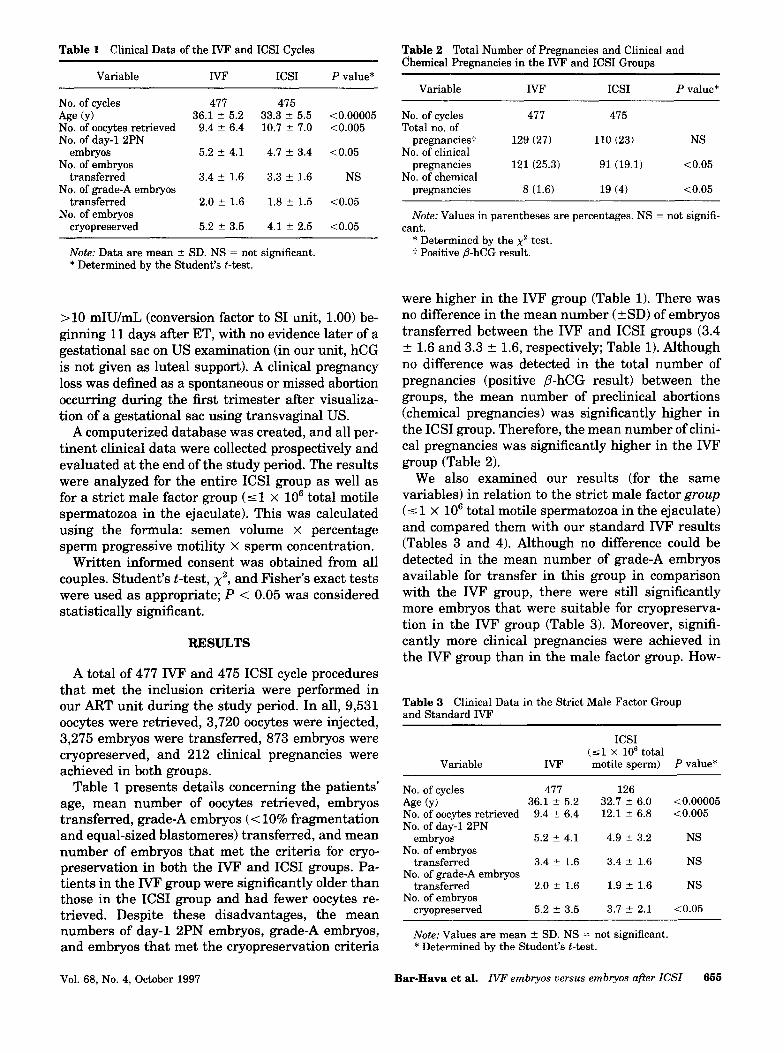
Table 1 Clinical Data of the IVF and ICSI Cycles
Variable IVF ICSI P value*
No. of cycles 477 415 Age (Y) 36.1 k 5.2 33.3 2 5.5 <0.00005 No. of oocytes retrieved 9.4 z 6.4 10.7 2 7.0 <0.005 No. of day-l 2PN
embryos No. of embryos
5.2 ? 4.1 4.7 ? 3.4 co.05
transferred No. of grade-A embryos
3.4 2 1.6 3.3 ? 1.6 NS
transferred No. of embryos
2.0 t 1.6 1.8 t 1.5 <0.05
cryopreserved 5.2 2 3.5 4.1 2 2.5 co.05
Note: Data are mean 2 SD. NS = not significant. * Determined by the Student’s t-test.
>lO mIU/mL (conversion factor to SI unit, 1.00) be- ginning 11 days after ET, with no evidence later of a gestational sac on US examination (in our unit, hCG is not given as luteal support). A clinical pregnancy loss was defined as a spontaneous or missed abortion occurring during the first trimester after visualiza- tion of a gestational sac using transvaginal US.
A computerized database was created, and all per- tinent clinical data were collected prospectively and evaluated at the end of the study period. The results were analyzed for the entire ICSI group as well as for a strict male factor group (51 X lo6 total motile spermatozoa in the ejaculate). This was calculated using the formula: semen volume x percentage sperm progressive motility X sperm concentration.
Written informed consent was obtained from all couples. Student’s t-test, x2, and Fisher’s exact tests were used as appropriate; P < 0.05 was considered statistically significant.
REBULTS
A total of 477 IVF and 475 ICSI cycle procedures that met the inclusion criteria were performed in our ART unit during the study period. In all, 9,531 oocytes were retrieved, 3,720 oocytes were injected, 3,275 embryos were transferred, 873 embryos were cryopreserved, and 212 clinical pregnancies were achieved in both groups.
Table 1 presents details concerning the patients’ age, mean number of oocytes retrieved, embryos transferred, grade-A embryos (< 10% fragmentation and equal-sized blastomeres) transferred, and mean number of embryos that met the criteria for cryo- preservation in both the IVF and ICSI groups. Pa- tients in the IVF group were significantly older than those in the ICSI group and had fewer oocytes re- trieved. Despite these disadvantages, the mean numbers of day-l 2PN embryos, grade-A embryos, and embryos that met the cryopreservation criteria
Table 2 Total Number of Pregnancies and Clinical and Chemical Pregnancies in the IVF and ICSI Groups
Variable IVF ICSI P value*
No. of cycles Total no. of
pregnancies? No. of clinical
pregnancies No. of chemical
pregnancies
477 475
129 (27) 110 (23) NS
121 (25.3) 91 (19.1) <0.05
8 (1.6) 19 (4) <0.05
Note: Values in parentheses are percentages. NS = not signifi- cant.
* Determined by the x2 test. t Positive P-hCG result.
were higher in the IVF group (Table 1). There was no difference in the mean number ( t SD) of embryos transferred between the IVF and ICSI groups (3.4 f- 1.6 and 3.3 + 1.6, respectively; Table 1). Although no difference was detected in the total number of pregnancies (positive P-hCG result) between the groups, the mean number of preclinical abortions (chemical pregnancies) was significantly higher in the ICSI group. Therefore, the mean number of clini- cal pregnancies was significantly higher in the IVF group (Table 2).
We also examined our results (for the same variables) in relation to the strict male factor group (5 1 x lo6 total motile spermatozoa in the ejaculate) and compared them with our standard IVF results (Tables 3 and 4). Although no difference could be detected in the mean number of grade-A embryos available for transfer in this group in comparison with the IVF group, there were still significantly more embryos that were suitable for cryopreserva- tion in the IVF group (Table 3). Moreover, signifi- cantly more clinical pregnancies were achieved in the IVF group than in the male factor group. How-
Table 3 Clinical Data in the Strict Male Factor Group and Standard IW
Variable IVF
ICSI (51 X lo6 total motile sperm) P value*
No. of cycles 477 126 Age (y) 36.1 2 5.2 32.7 k 6.0 <0.00005 No. of oocytes retrieved 9.4 k 6.4 12.1 -t 6.8 <0.005 No. of day-l 2PN
embryos 5.2 ? 4.1 4.9 5 3.2 NS No. of embryos
transferred 3.4 -+ 1.6 3.4 5 1.6 NS No. of grade-A embryos
transferred 2.0 2 1.6 1.9 2 1.6 NS No. of embryos
cryopreserved 5.2 k 3.5 3.7 k 2.1 co.05
Note: Values are mean 2 SD. NS = not significant. * Determined by the Student’s t-test.
Vol. 68, No. 4, October 1997 Bar-Hava et al. ZVF embryos versus embryos after ZCSZ 655

Table 4 Pregnancy Results in the IVF Group in Comparison With the Strict Male Factor ICSI Group
Variable
ICSI (51 X lo6 total
IVF motile sperm) P value*
No. of cycles Total no. of
pregnancies (%I No. of clinical
pregnancies (%) No. of chemical
pregnancies (o/o)
477 126
129 (27) 23 (18.2) <0.05
121 (25.3) 20 (15.8) <0.05
8 (1.6) 3 (2.3) NS
Note: NS = not significant. * Determined by the x2 or Fisher’s exact test, as appropriate.
ever, unlike the general ICSI group, no difference in the chemical PR was detected between the IVF and the male factor group (Table 4).
DISCUSSION
In this study, higher clinical PRs were achieved using IVF embryos than with ICSI embryos. This result was detected despite the significantly older age of the female partner and the initially fewer oocytes in the M? group. We believe that these findings may be attributed to a higher number of good-quality (grade-A) embryos available for trans- fer, which resulted in a lower incidence of preclinical pregnancy loss (chemical pregnancies) in this group.
Although an earlier report demonstrated that sperm microinjection does not increase the incidence of chromosomally abnormal embryos (El), it is well known that the frequency of chromosomal abnor- malities is high in preimplantation embryos and
Intracytoplasmic sperm injection is a powerful tool
that most abnormal embryos are lost before preg-
to overcome fertilization failure (1). Indeed, Palermo et al. (6) achieved a high PR using ICSI in a group
nancy is recognized clinically (9). Further, these oo-
of patients with total fertilization failure after con- ventional IVF. It is important to note that the semen
cytes are exposed to hyaluronidase, intense light,
characteristics in all of these patients were com- pletely normal (7). It is possible, therefore, that the
and fluctuations in temperature and are subjected
higher rate of preclinical (chemical) pregnancies found in the ICSI group in our study (compared with
to the creation of an artificial breach in the zona
the standard IVF group) may indicate a high inci- dence of abnormal embryos resulting from the
pellucida and oolemma. This opening may increase
“forced fertilization” of the ICSI procedure.
the risk of introducing toxins and debris into the perivitelline space and ooplasm, all of which may affect oocyte quality.
Our findings are discordant with a recently pub- lished study (10) in which differences were not found in the preclinical pregnancy loss rates between ICSI and IVF’ patient groups. We have no sound explana- tion for these differences, but it may be interesting to note that their reported figures of preclinical losses of 26% and 28% per cycle for ICSI and IVF, respectively, are substantially different from ours (4% and 1.6% per transfer, respectively).
There is no doubt that embryo quality may be af- fected by a traumatic injection that causes excessive disruption of the cytosol. Therefore, after completing our learning curve (June-December 1994), we paid special attention to correctly placing the oocyte be- fore injection in a position of orientation by ob- serving the polar body position and identifying the area of polar granularity, which is the assumed loca- tion of germinal vesicle breakdown. It should be noted that a 62% fertilization rate per injected egg was achieved in our laboratory during the study pe- riod, a figure that is similar to the 64.5% reported by the group from Cornell Medical Center (1). We believe, therefore, that it is highly unlikely that faulty technique would explain the findings of the current study.
We are well aware that our PRs may seem lower than those reported by other centers. It should be remembered, however, that we run a public service for the main health maintenance organization in Israel, and practically every woman in Israel is covered by medical insurance. This ensures no pa- tient selection whatsoever, and almost every woman (ages 20-49 years) can seek treatment with no up- per limit for the number of cycles. We assume that this is the main reason for the relatively lower PRs and that these factors similarly affected the IVF and ICSI groups.
The ICSI procedure is currently performed for two main indications: severe male factor infertility and low fertilization rate (<30%) in previous standard IVF treatments. Therefore, it may be postulated that the paternal or maternal factors that led to this type of infertility have a deleterious influence on the de- veloping ICSI embryo, resulting in reduced embryo quality and poorer outcome in comparison with stan- dard IVF with its “natural” selection mechanisms. Indeed, in contrast to other studies (2, 31, we de- tected a deleterious effect of the ICSI procedure (or of the causes that led to the necessity to perform ICSI) on the quality of the developing embryos. Sig- nificantly more grade-A (<lo% fragmentation) em-
It may be postulated that selection of embryos on day 3 may change the current study findings. Unfor- tunately, we are unable to verify this because of our small sample size; most of our embryos (85%) were transferred on day 2.
656 Bar-Hava et al. IVF embryos versus embryos af?er ICSI Fertility and Sterility@

bryos were available for transfer in the IVF group compared with the ICSI group (a total of 987 versus 870 grade-A embryos in the IVF versus the ICSI group, respectively; P < 0.05).
These findings also may suggest that the sperm provides a major contribution to, and has an influ- ence on, the fate of the developing embryo. Further- more, a greater number of embryos were available for cryopreservation in the IVF group, a difference that also was evident in comparison with the ICSI group for the strict male factor indication (5 1 x lo6 total motile sperm in the ejaculate). These findings are even more remarkable considering that signifi- cantly more oocytes were initially available in the ICSI group (Table 1).
It is interesting to note that no statistically sig- nificant differences were found in the number of grade-A embryos available for transfer when ICSI for strict male factor was compared with standard M? (Table 3). This may reflect the adverse influence of the maternal component on the developing ICSI embryos in cases in which ICSI was conducted be- cause of previously low fertilization in standard IVF procedures.
In a recent publication, De Sutter et al. (11) dem- onstrated a similar fertilization rate for “ideal” oo- cytes and for those containing a refractile body, a defect that is invariably associated with fertilization failure in standard IVF. When summarizing their study, they stated, “Eventually all oocytes can be fertilized by ICSI,” implying that ICSI may “force” the production of some embryos. The results of the current study are all in agreement with this concept, namely fewer grade-A embryos available for trans- fer, higher preimplantation abortion rate, and lower clinical PR in the ICSI group.
We believe that the strengths of this study are its consecutive, prospective nature and the large num- ber of cycles (n = 952). Furthermore, it is well known that in infertility treatments the age of the female partner is the single most important prognostic fac- tor in achieving pregnancy. Therefore, the results of this study are emphasized further by the fact that the women in the IVF group were significantly older than those in the ICSI group (36.2 t 5.2 versus 33.3 + 5.5 years, respectively; P < 0.0005).
Although several investigators (1,3,12) have spec- ulated that, in the near future, ICSI will be the pro- cedure of choice for all couples who need ART, we believe that our findings cast doubt on this state-
ment. Furthermore, although several studies have demonstrated that the health of children born after ICSI is similar to that of children born after other ART methods, there is still concern about the possi- ble long-term outcomes of bypassing most of the nat- ural fertilization stages and the possible transfer of genetic disorders using the ICSI procedure. The cur- rent study demonstrates that, if the option exists, it is preferable to use IVF rather than ICSI embryos.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
REFERENCES
Palermo GD, Cohen J, Rosenwaks Z. Intracytoplasmic sperm injection: a powerful tool to overcome fertilization failure. Fertil Steril 1996;65:899-908. Yang D, Shahata MA, Al-Bader M, Al-Natsha SD, Al- Flamerzia M, Al-Shawaf T. Intracytoplasmic sperm injection improving embryo quality: comparison of the sibling oocytes of non-male-factor couples. J Assist Reprod Genet 1996; 13: 351-5. Oehninger S, Kruger TF, Simon T, Jones D, Mayer J, Lan- zendorf S, et al. A comparative analysis of embryo implanta- tion potential in patients with severe teratozoospermia un- dergoing in-vitro fertilization with a high insemination concentration or intracytoplasmic sperm injection. Hum Re- prod 1996; 11:1086-9. Conaghan J, Handyside AH, Winston RML, Leese HJ. Effects of pyruvate and glucose on the development of human preim- plantation embryos in vitro. J Reprod Fertil 1993;99:87-95. World Health Organization. Laboratory manual for the ex- amination of human semen and sperm-cervical mucus inter- action. 3rd ed. New York: Cambridge University Press, 1993. Palermo GD, Cohen J, Alikani M, Adler A, Rosenwaks Z. Intracytoplasmic sperm injection: a novel treatment for all forms of male factor infertility. Fertil Steril 1995;63:1231- 40. Palermo G, Joris H, Derde MP, Camus M, Devroey P, Steir- teghem A. Sperm characteristics and outcome of human as- sisted fertilization by subzonal insemination and intracy- toplasmic sperm injection. Fertil Steril 1993;59:826-35. Lola I, Lacham 0, Jansen RPS, Turner M, Trounson A. Chro- mosomal analysis of human oocytes fertilized by microinjec- tion of spermatozoa into the perivitelline space. Hum Reprod 1990;5:575-7. Burgoyne PS, Holland D, Stephens R. Incidence of numerical chromosome abnormalities in human pregnancy estimated from induced and spontaneous abortion data. Hum Reprod 1991;6:555-65. Coulam CB, Opsahl MS, Sherins RJ, Thorsell LP, Dorfmann A, Krysa L, et al. Comparison of pregnancy loss patterns after intracytoplasmic sperm injection and other assisted repro- ductive technologies. Fertil Steril 1996;65:1157-62. De Sutter P, Dozortsev D, Qian C, Khont M. Oocyte morphol- ogy does not correlate with fertilization rate and embryo qual- ity after intracytoplasmic sperm injection. Hum Reprod 1996;11:595-7. Hall J, Fishel S, Green S. Intracytoplasmic sperm injection versus high insemination concentration in cases of very se- vere teratozoospermia. Hum Reprod 1995; 10:493-6.
Vol. 68, No. 4, October 1997 Bar-Hava et al. IVF embryos versus embryos after ICSI 657