monitoring clinical quality through indicators, metrics and dashboards national perspective
DESCRIPTION
Monitoring clinical quality through indicators, metrics and dashboards National perspective. Danny Keenan National Clinical Advisor Care Quality Commission. Quality metrics and indicators explained: what’s the difference between a metric and an indicator Discussion re Clinical Quality - PowerPoint PPT PresentationTRANSCRIPT

Monitoring clinical quality through indicators, metrics and dashboardsNational perspectiveDanny Keenan
National Clinical Advisor
Care Quality Commission

2
NHS Performance Framework; Implementation guidance April 2011Technical Guidance for the 2011/12Operating Framework; Jan 2011The NHS Outcomes Framework 2011/12
• Quality metrics and indicators explained: what’s the difference between a metric and an indicator
• Discussion re Clinical Quality
• Augmenting national indicators with local measurements of quality
• How the Care Quality Commission will monitor improvements in quality
• Using clinical dashboards to monitor improvement in quality indicators and metrics
3
Metric or indicator?
A metric is a measure
Patients in primary care have their blood pressure measured
An indicator is a way of using a metric for purposes of comparison: (Latin: indicare = to point out)
4
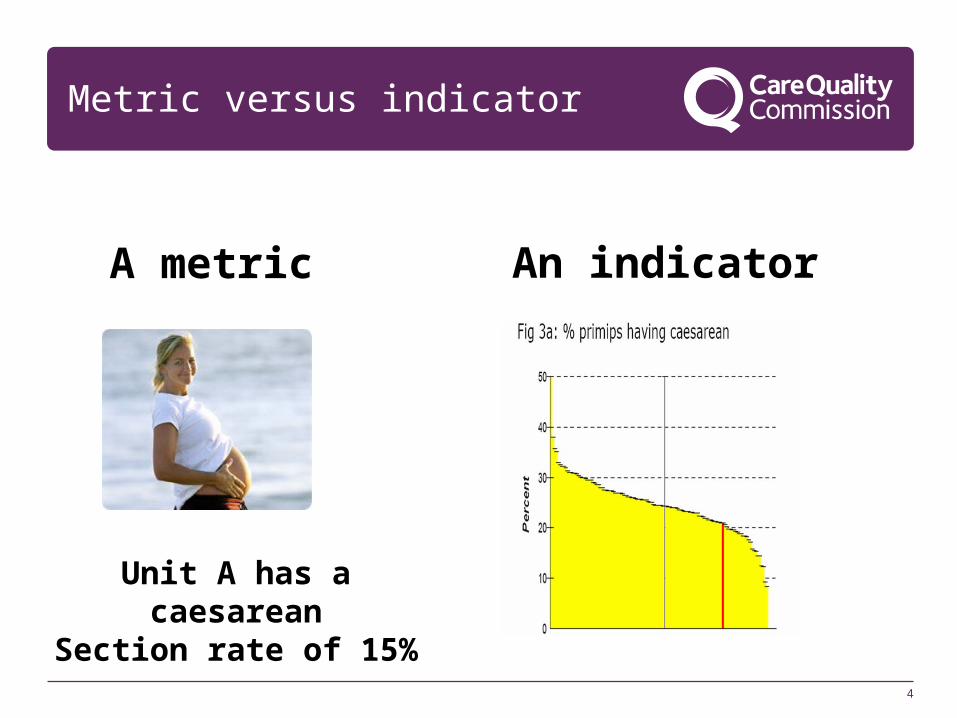
Metric versus indicator
Unit A has a caesareanSection rate of 15%
A metric An indicator

5
What is clinical quality?

6
Three domains of quality
Safety
Effectiveness
Patient experience

7
Outcomes and indicators for the first framework
Preventing people from dying prematurely
Enhancing the quality of life for people with long-term conditions
Helping people to recover from episodes of ill health or following injury
Ensuring people have a positive experience of care
Treating and caring for people in a safe environment and protecting them from avoidable harm
EFFECTIVNESS
PATIENT EXPERIENCE
SAFETY
Clin
ical qu
ality
The NHS Outcomes Framework 2011/12

8
Assessing quality
Measuring clinical quality:
• Structure- Refers to the inherent characteristics which are associated with higher
quality (e.g):• Procedure volumes• Advanced IT• Nurse staffing ratios• Stroke service
• Processes- Do you comply with evidence-based care guidance?
• Administration of aspirin and B blockers with acute coronary syndrome• Compliance with desirable practices such as frequent determination of
HbA1c in diabetics
• Outcomes- some general ones- some sector or condition specific

9
Example metrics for assessing quality
Inputs(Policies and inputs that ensure quality)
Process(Pathways and best-practices for quality)
Outcome(Ensuring that patients are better-off)
Safety (Ensuring that providers ‘do no harm’)
Clinical effectiveness (Evaluating clinical quality of care)
Patient experience(Ensuring good quality of non-clinical care)
• Health and safety regulations understood
• Ensure staff qualifications
• Systems and structures in place for setting standards and monitoring quality of care
• Systems and structures for monitoring
• Patient advocate in place
• Use of double identifiers in drug prescription process
• Breast cancer screening rates
• Thrombolysis rates
• Confidentiality• Waiting times• Access to
information • Customer
satisfaction training
• Rate of adverse events, serious untoward incidents
• Functional capability post routine surgery
• Survival rates for major surgery
• Patient satisfaction rates with services
• Number of complaints
Structure
10
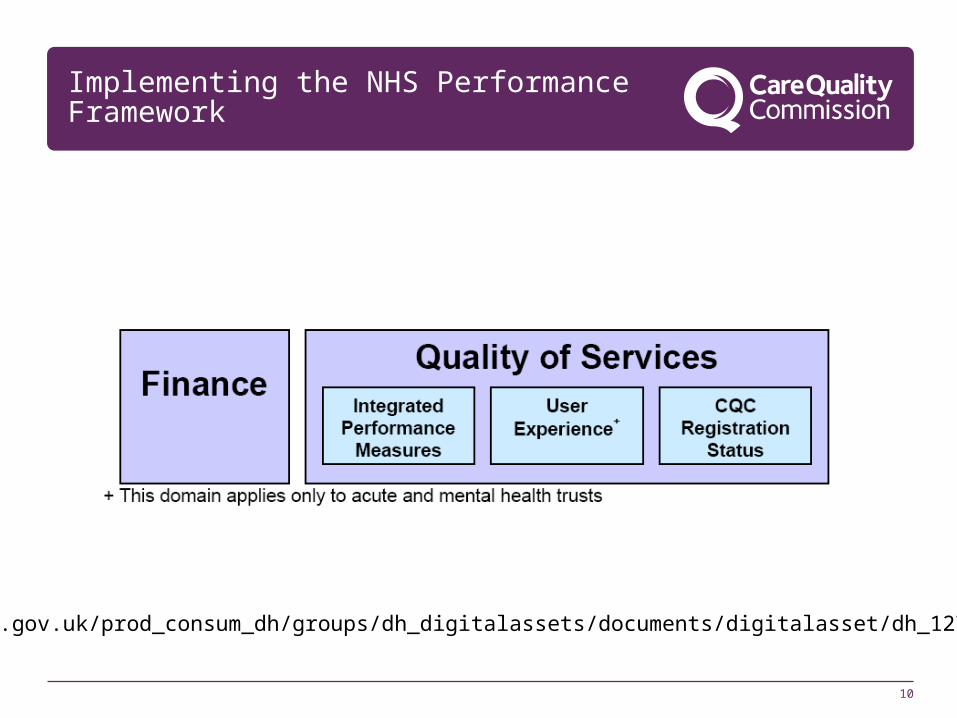
Implementing the NHS Performance Framework
www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_127007.pdf
11
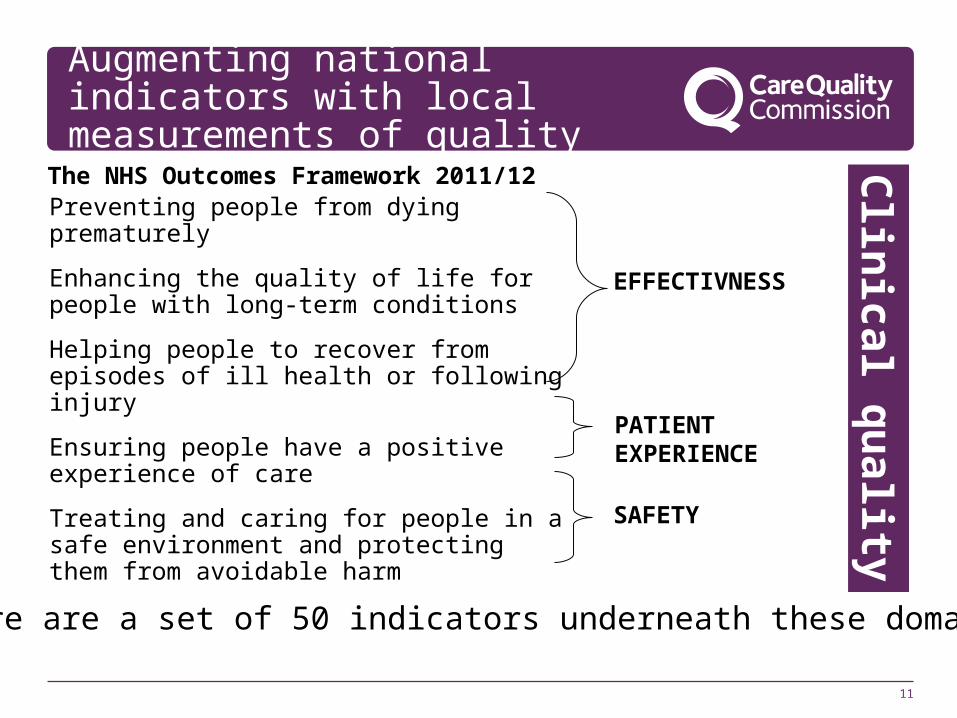
Augmenting national indicators with local measurements of quality
Preventing people from dying prematurely
Enhancing the quality of life for people with long-term conditions
Helping people to recover from episodes of ill health or following injury
Ensuring people have a positive experience of care
Treating and caring for people in a safe environment and protecting them from avoidable harm
EFFECTIVNESS
PATIENT EXPERIENCE
SAFETY
Clin
ical qu
ality
The NHS Outcomes Framework 2011/12
There are a set of 50 indicators underneath these domains

12
Augmenting national indicators with local measurements of quality
The Commissioning Outcomes Framework
Derived from the NICE Quality Standards, among other things.
There will always be room for local measures:
North West :
• Advancing Quality ---AQuA (Advancing Quality Alliance):- Heart Attack- Hip or knee replacement- Heart failure- Pneumonia- Coronary artery bypass surgery- Next iteration:
Mental health, including dementia COPD Diabetes
13
NHS Performance Guidance-Implementation Guidance. April 2011
Measuring for Quality Improvement launched the development of a menu of Assured Quality Indicators to enable local clinical teams to identify indicators that support their improvement work and allow benchmarking with other clinical teams.
Quality indicators from this Assured Menu will have a number of uses, including in commissioner contracts (particularly the Commissioning for Quality and Innovation (CQUIN) payment framework), publication of Quality Accounts, and information for the public through NHS Choices.
14
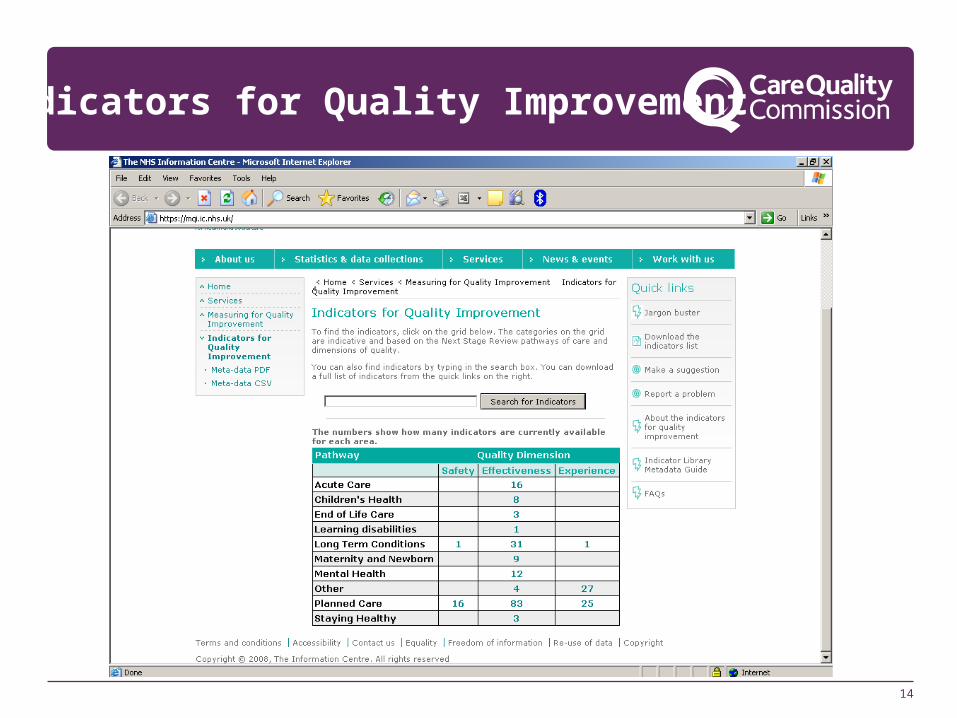
Indicators for Quality Improvement

15
How CQC will monitor improvements in quality
The essential standards of quality and safety

16
CQC and registration
CQC regulates under the Essential Standards of Quality and Safety
The essential standards are focused on outcomes - the experiences people have as a result of the care they receive
• Regulation 9; Outcome 4;Care and welfare of people who use services
People experience effective, safe and appropriate care, treatment and support that meets their needs and protects their rights.
• Regulation 10; Outcome 16;Assessing and monitoring the quality of service provision
People benefit from safe, quality care because effective decisions are made and because of the management of risks to people’s health, welfare and safety.
• Regulation 12; Outcome 8;Cleanliness and infection control
People experience care in a clean environment, and are protected from acquiring infections.

17
Quality and Risk Profile (QRP)

18
Quality Risk Profiles (QRP) are at the centre
Bring together information about a care provider so as to estimate risk and prompt front line regulatory activity
Act as a guide and aid CQC’s inspectors
Not a judgement (or a rating, or a league table) in themselves
Build over timeCapable of using both numeric (quantitative) and textual (qualitative) data
Essential tool to support monitoring of compliance
Help inform subsequent judgements and add to the knowledge base about a care provider
Rejects the use of a small number of numeric indicators to make judgements about service quality

19
…but builds on 10 years development
19
The philosophy draws on the work of Klein and Carter in the 1980s
The mathematical approaches have been being developed by CQC and its predecessors since the early 2000s and have substantial academic input
The qualitative analysis techniques allow us to treat textual information consistently draw on best practice in social research techniques
The approach draws on and addresses Bevan and Hood’s reflections of the “measurement frenzy” in public service reform in the 2000s
This approach is at the cutting edge of use of information, but we believe transferable between sectors

20
Updating and sharing of QRPs with providers
20
QRPs are updated regularly (monthly or more often depending upon data feeds)
The QRPs will be shared with Providers as they are updated so that we are all working from the same data
NHS trusts have had access to their QRP since September via a .pdf. This has been made available to commissioners, SHAs, Monitor and DH since October
This summer we will release an online service which will give access to data as live and which will have vastly increased functionality

21

22
How the Care Quality Commission will monitor improvements in quality

23
How CQC will monitor improvements in quality
Our main tool will be using Registration
and……….
Compliance with Registration
Previously we had the Annual Health Check…proved to be a blunt tool
Now that Registration has been in place, with Trusts, for a year compliance is becoming more important

24
Site visits
The aim of site visits is to gather evidence of compliance
They are short, focussed unannounced site visits, rather than set piece inspections that require the provider to spend a lot of time in preparation
Site visits are direct checks of compliance rather than assessing compliance through the assurance systems the organisation has in place.
Therefore site visits may include direct observation of care and spending time with people who use the service, their families and carers, unless not appropriate to do so. We may also talk to managers and staff. Experts by experience will join us on some site visits to help us engage with people who use services.
25
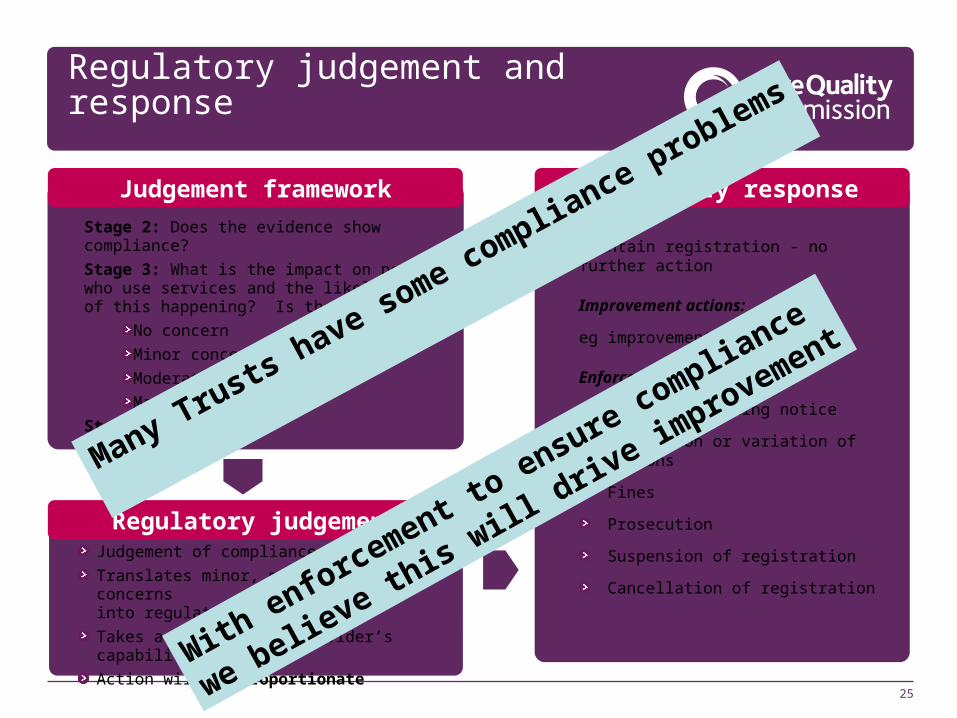
Judgement framework
Regulatory judgement and response
Stage 2: Does the evidence show compliance?
Stage 3: What is the impact on people who use services and the likelihood of this happening? Is there:
No concern
Minor concern
Moderate concern
Major concern
Stage 4: Validation
Regulatory response
Maintain registration - no further action
Improvement actions:
eg improvement letter
Enforcement actions:
Statutory warning notice
Imposition or variation of conditions
Fines
Prosecution
Suspension of registration
Cancellation of registration
Regulatory judgementJudgement of compliance or concerns
Translates minor, moderate or major concerns into regulatory judgement
Takes account of the provider’s capability to improve
Action will be proportionate
Many Trusts have some compliance problems
With enforcement to
ensure compliance
we believe this will d
rive im
provement

26
Using clinical dashboards to monitor improvement in quality indicators and metrics
This will be determined locally, bearing in mind that there will be requirements laid down by the Department (including QIPP local agenda); CQC and Monitor.So a dashboard will have these through it:
•Measures to reassure the Board/Managers that the service they provide is effective, safe and patient responsive•Measures negotiated with local commissioners•Measures suggested by clinicians and for use in revalidation•Measures suggested by patients, including patient outcomes and surveys

27
Using clinical dashboards to monitor improvement in quality indicators and metrics
Pitfalls:
• Avoid that which is easy to measure but not useful
• The adverse effects of any measure which is that the measured item improves at the expense of other important areas
• The burden of measurement
28
Local dashboards
Some overarching themes:• Process:
- Board Issues (Having a culture of quality and safety in an organisation and amongst staff)
- Quality of Records
- Information / HES quality/ NHS number
- Commitment to safety
- Issues relating to staff
• Sickness/stress, staff satisfaction, absence, training, vacancies
- Commitment to Audit and Service Improvement
- Commitment to Research
29
Local dashboards
Some overarching themes:• Outcomes:
- Mortality - Healthcare associated infections- Patients:
• Satisfaction, complaints- Prescribing, administration and reconciliation of medicines - Patient Safety First outcomes- Never events- National audits;
• Cardiac• Cancer
- HES based outcomes

31
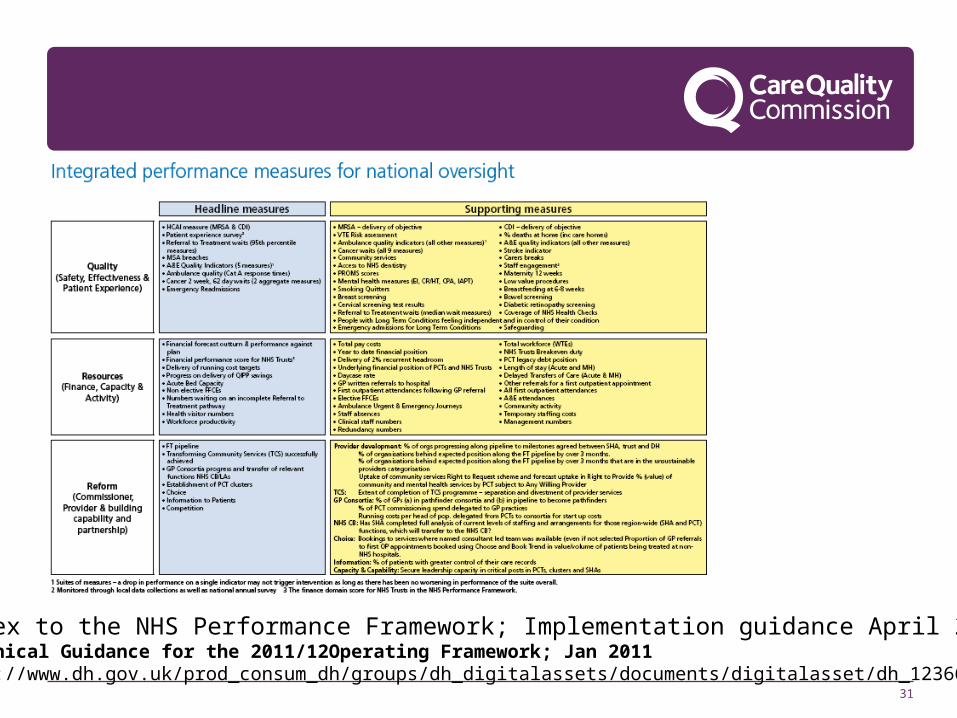
Annex to the NHS Performance Framework; Implementation guidance April 2011Technical Guidance for the 2011/12Operating Framework; Jan 2011http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_123660.pdf

32
Mental Health
www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_127007.pdf