module3-lec
DESCRIPTION
reviewTRANSCRIPT
Review
• Ketone Bodies – produced in liver from acetyl CoA as an alternative fuel source for peripheral tissues • Acetoacetate and 3-hydroxybutyrate
• Synthesized from 2 acetyl CoA
• Rate limiting step: HMG CoA synthase in liver mitochondria
• Extrahepatic tissues convert ketone bodies to acetyl CoA for TCA cycle
• Too many ketones – leads to ketoacidosis

Review
• Phospholipids • Amphipathic molecules used in cell membranes, bile
and lung surfactant
• Glycolipids • Carbohydrate and lipid • Found in cell membranes, particularly nerve cells, on
external side of membrane • Antigenic
• Eicosanoids: Prostaglandins and Friends • Elicit wide range of responses and have many important
roles in the body • Like hormones only the are produced by most tissues in
very small amounts and act locally

Cholesterol and Lipoproteins – Lecture Objectives • Identify cholesterol
• Structure
• Synthesis and use/disposal
• Regulation of cholesterol homeostasis
• Understand the role of the 4 different lipoproteins in transport of lipids • Structure of lipoproteins
• Metabolism of lipoproteins

Cholesterol
• Most abundant sterol in the body
• Functions: 1. Component of cell membranes. 2. Precursor of bile acids, steroid hormones,
and vitamin D
• Continuous supply of cholesterol is required for all cells.
• Liver play a major role in regulating cholesterol homeostasis
• Medical Relevance: Cholesterol levels are a risk factor for atherosclerosis and coronary artery disease

Structure of Cholesterol
• Cholesterol is very hydrophobic.
• Consists of: • 4 rings (“steroid nucleus”). • Hydrocarbon tail attached to the D
ring at C17. • Hydroxyl at C3 of A ring • Double bound in B ring between C5
and C6
• Cholesteryl Esters • Cholesterol attached to a fatty acid at
C-3 • More hydrophobic than cholesterol
Synthesis of Cholesterol
• Synthesized by all tissues in humans • Liver, intestine, adrenal cortex and reproductive tissues
make the largest contributions to the body’s cholesterol
• All carbon atoms come from acetyl CoA
• NADPH provides reducing equivalents
• Regulatory mechanisms are in place to balance cholesterol synthesis and cholesterol excretion
• Imbalance leads to: • Increase in body cholesterol: results in coronary artery
disease. • Increased secretion of cholesterol in bile: results in
cholesterol gallstone disease.

Synthesis of Cholesterol
• Step 1: Synthesis of HMG CoA • Same as for ketone body synthesis • Occurs in cytosol
2 acetyl CoA acetoacetyl CoA + acetyl CoA HMG CoA
• Liver cells contain 2 forms of HMG CoA synthase:
1. Cytosolic enzyme cholesterol synthesis
2. Mitochondrial enzyme ketone body synthesis

Synthesis of Cholesterol
• Step 2: Synthesis of Mevalonate
HMG CoA Melvonate
• Catalyzed by HMG CoA reductase
• Uses 2 NADPH as reducing agent
• CoA is released making the reaction irreversible

Cholesterol Synthesis

Regulation of Cholesterol Synthesis • HMG CoA reductase: Major control point for
cholesterol biosynthesis
1. Sterol-dependent regulation of gene expression • When cholesterol levels are low, HMG CoA reductase
expression is increased
2. Sterol-accelerated degradation of enzyme • When cholesterol levels are high, HMG CoA is degraded
faster (removed from the cell)
3. Sterol-independent (de)phosphorylation

Regulation of Cholesterol Synthesis 4. Hormonal Regulation
• Insulin increases amount of reductase expressed
• Glucagon decreases the amount of expressed
5. Inhibition by drugs • Statin drugs are structural analogs
of HMG CoA
• Act as competitive inhibitors of HMG CoA reductase
• Used to decrease plasma cholesterol levels
Degradation of Cholesterol
• Ring structure of cholesterol cannot be metabolized to CO2 and H2O in humans
• Intact sterol ring is eliminated from the body by:
1. Conversion to bile acids/salts which are extcreted in the feces
2. Secretion of cholesterol into the bile which is transported to the intestine
3. Modification of cholesterol by intestinal bacteria

Synthesis of Bile Acids
• Synthesized by liver
• Synthesis starts with cholesterol • Hydroxyl groups are introduced
at positions 7 and 12
• Carboxylic acid group added to ‘side-chain’

Synthesis of Conjugated Bile Salts
• Before they leave the liver bile acids are converted to conjugated bile salts • Conjugated (attached) to either
glycine or taurine
• Bile salts are more effective detergents than bile acids

Action of Intestinal Flora on Bile Salts • Bacteria in the intestine can deconjugate bile salts
• Remove glycine and taurine
• Bacteria can also remove a hydroxyl group from bile acids
• Leads to excretion in fecal matter

Enterohepatic Circulation
• Bile acids secreted into the intestine are effectively re-absorbed and reused

Bile Salt Deficiency • Cholesterol gallstone disease.
• Occurs when more cholesterol enters the bile than can be solubilized by bile salts
• Cholesterol precipitates (solidifies) in the gall bladder, initiating cholelithiasis
• Causes:
a) Malabsorption of bile acids from intestine
b) Obstruction of biliary tract
c) Severe hepatic dysfunction
d) Increased biliary cholesterol excretion
• Treatment
a) Surgical removal of gall bladder
b) Supplements with bile acids

Lipoproteins
• Lipoproteins are complexes of lipids and apolipoproteins found in the blood and plasma
• Four main classes 1. Chylomicrons (CM) 2. Very Low Density Lipoproteins (VLDL) 3. Low Density Lipoproteins (LDL) 4. High Density Lipoproteins (HDL)
• Functions 1. Maintain lipids in soluble form in blood 2. Deliver lipids to tissues
• Medical Relevance:
• Dietary condition or genetic defects in cholesterol metabolism lead to plaque formation and result in atherosclerosis.

Composition of Lipoproteins • Lipoproteins have:
• A core of tracylglycerol and cholesteryl esters
• A shell of cholesterol, phospholipids and apolipoproteins
• Lipoproteins particles keep lipids soluble in the blood.
• TAG and cholesterol obtained from diet or de novo synthesis are packaged into an inner core and carried by the particle in the blood
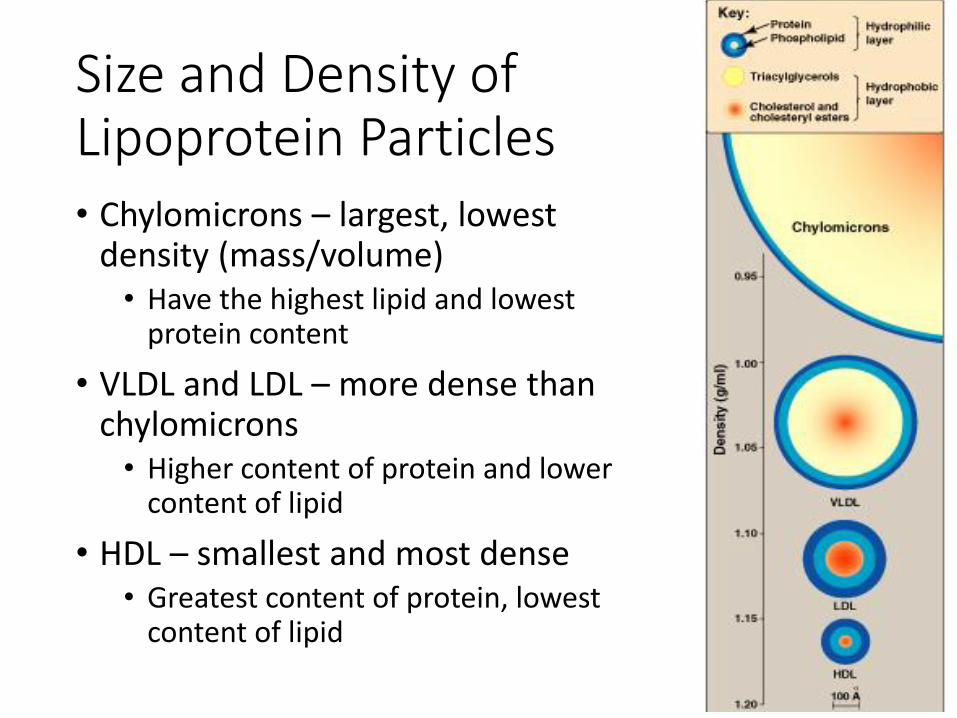
Size and Density of Lipoprotein Particles • Chylomicrons – largest, lowest
density (mass/volume) • Have the highest lipid and lowest
protein content
• VLDL and LDL – more dense than chylomicrons • Higher content of protein and lower
content of lipid
• HDL – smallest and most dense • Greatest content of protein, lowest
content of lipid

Composition of Plasma Lipoproteins • Chylomicrons – mostly TAG
• VLDL – mostly TAG
• LDL – very rich in cholesterol and cholesteryl esters
• HDL – acceptor of free cholesterol. Very rich in phospholipids and apolipoproteins

Apolipoproteins
• Protein component of lipoproteins
• Functions:
1. Structural components of lipoproteins
2. Recognition sites for cell-surface receptors
3. Activators or coenzymes for lipoprotein metabolic enzymes

Metabolism of Chylomicrons
• Assembled in the intestinal mucosal cells • Carry dietary TAG and cholesterol from small intestine to
other tissues
• Contain apolipoprotein B-48 (apo B-48) • In bloodstream, the receive apo CII and apo E from HDL
• Degradation of TAG by lipoprotein lipase • In capillaries of adipose tissue, hear and muscle, TAG
degrades into FA and glycerol
• Apo C-II activates lipoprotein lipase
• Free Fas are either stored or used for energy

Metabolism of Chylomicrons

Metabolism of VLDL
• VLDL produced in liver
• Carry de novo TAG and cholesterol from the liver to the tissues.
• Contain apo B-100 • Receive apo C-II and apo E from HDL in the blood
• TAGs degraded by the enzyme lipoprotein lipase

Metabolism of VLDL

Modification of Circulating VLDL • Some TAGs are transferred from
VLDL to HDL in exchange for cholesteryl esters from HDL to VLDL
• The loss of TAG by both TAG degradation and CE transfer converts VLDL to LDL in the blood

Metabolism of LDL
• Very rich in cholesterol and cholesteryl esters • Carrier of bad cholesterol
• Synthesized in the blood from VLDL
• Carry cholesterol to the peripheral tissues
• Contain apo B-100
• Removed from blood by cellular uptake and degradation • LDL receptors recognize apo B-100, and LDL is endocytosed • LDL degradation releases cholesterol, aminoacids, FAs and
phospholipids • LDL receptors are recycled to the cell surface

Derived Cholesterol Affects on Cellular Cholesterol • When cholesterol is over-
supplied:
1. High cholesterol inhibit HMG CoA reductase, resulting in decreased cholesterol synthesis
2. High cholesterol reduces the number of LDL receptors = less uptake
3. Storage of cholesterol as cholesteryl esters

When LDL is oxidized:
a) Chemically modified LDL is
taken up by macrophage
scavenger receptors.
b) Unlike LDL receptor, the
scavenger receptor is not down-
regulated in response to
increased intracellular
cholesterol levels.
c) Accumulation of cholesteryl
esters in macrophages results in
their transformation into ‘foam’
cells. Leads to formation of
atherosclerotic plaques.

Metabolism of HDL
• HDL is secreted into blood from liver and intestine
• Small protein-rich particles that contain relatively little cholesterol and cholesteryl esters
• Act as a reservoir for apolipoproteins (apo A, apo C-II and apo E).
• HDL takes up free cholesterol

Metabolism of HDL
• Cholesterol taken up by HDL is esterified by enzyme phosphatidylcholine-cholesterol acyl transferase (PCAT) • Apo A1 activates PCAT
• Reverse cholesterol transport: • Transfer of cholesterol from the peripheral tissues to
HDL, and from HDL to liver
• Key step in cholesterol homeostasis
• HDL is the good carrier of cholesterol

Lipoprotein Related Disease
• 2 primary disorders of lipoprotein metabolism
1. Familial hypercholesterolemia • LDL receptor deficiency
• Decreased cellular LDL uptake
• Increased blood LDL and cholesterol levels
• Accelerates progress to atherosclerosis
2. Lipoprotein lipase or apo C-II deficiency • Dramatic accumulation of chylomicrons in the blood
• Corresponding increase in blood TAG concentrations
• Leads to pancreatitis