mhealth mali - peter winch
TRANSCRIPT
Developing an mHealthintervention to improve maternal health in Sélingué Health District,
Mali
Peter Winch

Partners
JHSPH, International Health
University of Bamako/USTTB, Faculty of Medicine and Dentistry, Department of Public Health
– http://santepublique.fmpos.org/
– www.usttb.edu.ml/
ANTIM: Malian National Agency for Telemedicine and Medical Informatics
– www.antim.sante.gov.ml
Funding: NIH Fogarty International Center2

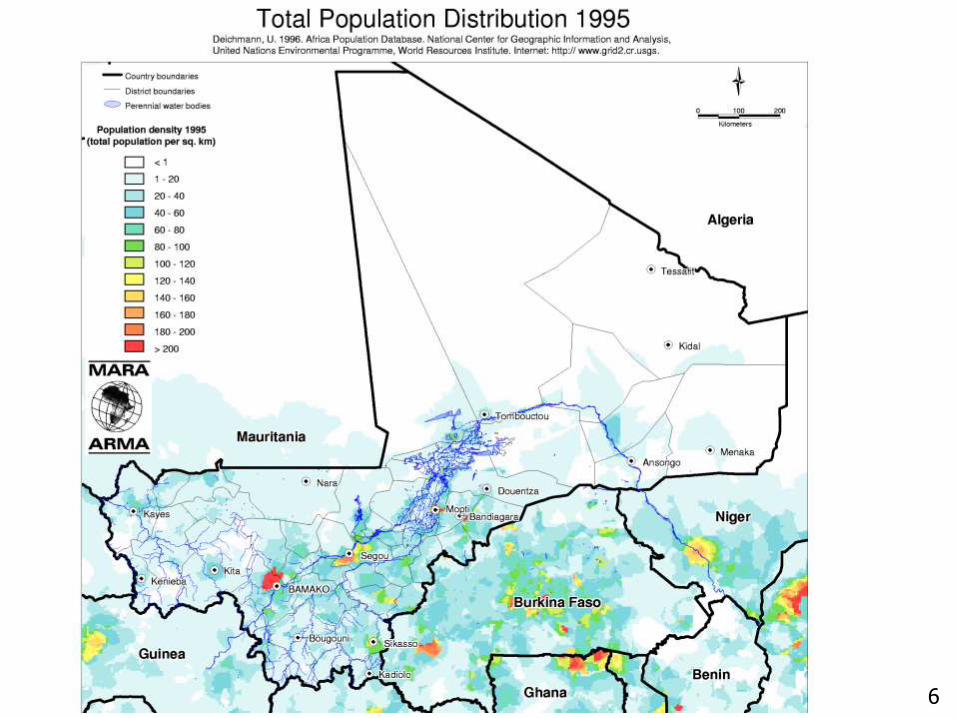
Mali, West Africa
3

4

Major conflict in northern Mali in 2012-2013
On-going skirmishes and attacks in 2015
5
6

Urban Rural TOTAL
Literacy in women 15-49
47.4% 11.8% 20.6%
Total Fertility Rate 5.0 6.5 6.1
Made at least one antenatal care visit
93.2% 69.3% 74.2%
Birth in health facility 91.4% 46.4% 55.0%
<5 Mortality Rate 64 113 95
Neonatal Mortality Rate 27 38 34
7
Indicators from DHS 2012-2013
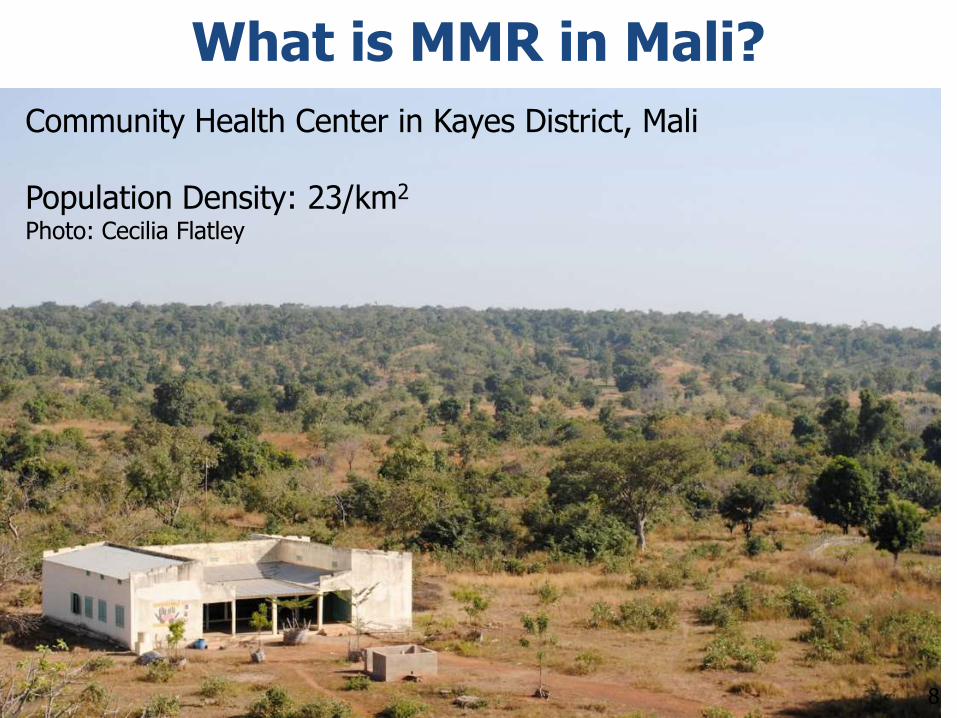
What is MMR in Mali?
Community Health Center in Kayes District, Mali
Population Density: 23/km2
Photo: Cecilia Flatley
8

Sisterhood method: 4 questionsSource - http://en.wikipedia.org/wiki/Sisterhood_method
Question 1: How many sisters have you ever had, born to the same mother, who ever reached the age 15 (or who were ever married), including those who are now dead? (cutoff age used varies in different studies)
Question 2: How many of your sisters who reached the age of 15 are alive now?
Question 3: How many of these sisters are dead?
Question 4: How many of your sisters who are dead died during a pregnancy or during childbirth, or during the six weeks after the end of a pregnancy?
9

What is maternal mortality ratio / MMR by Sisterhood method?
DHS 2012-2013: 368/100,000 live births - National
– 97,578 years of exposure
– 95% CI: 259-478
– 32% of deaths in women 15-49 years
Aa I et al. High maternal mortality estimated by the sisterhood method in a rural area of Mali. BMC Pregnancy Childbirth 2011, 11:56. – Kita District, Kayes Region
– 2,039 respondents reported 4,628 sisters
– MMR 3,131/100,000 live births (95% CI 2,967-
3,296), time reference around 1999, lifetime risk 20%
– Villages as far as 60km from nearest Health Center
10

Factors contributing to high MMR
Low population densities, dispersed populations
Non-functional transport and referral systems
Low quality of care in health facilities
Shortage of skilled providers
Maternal anemia – DHS 2012-2013
– Pregnant = 59.3%
– Lactating = 51.3%
– Neither = 49.6%
High TFR, low contraceptive prevalence
11
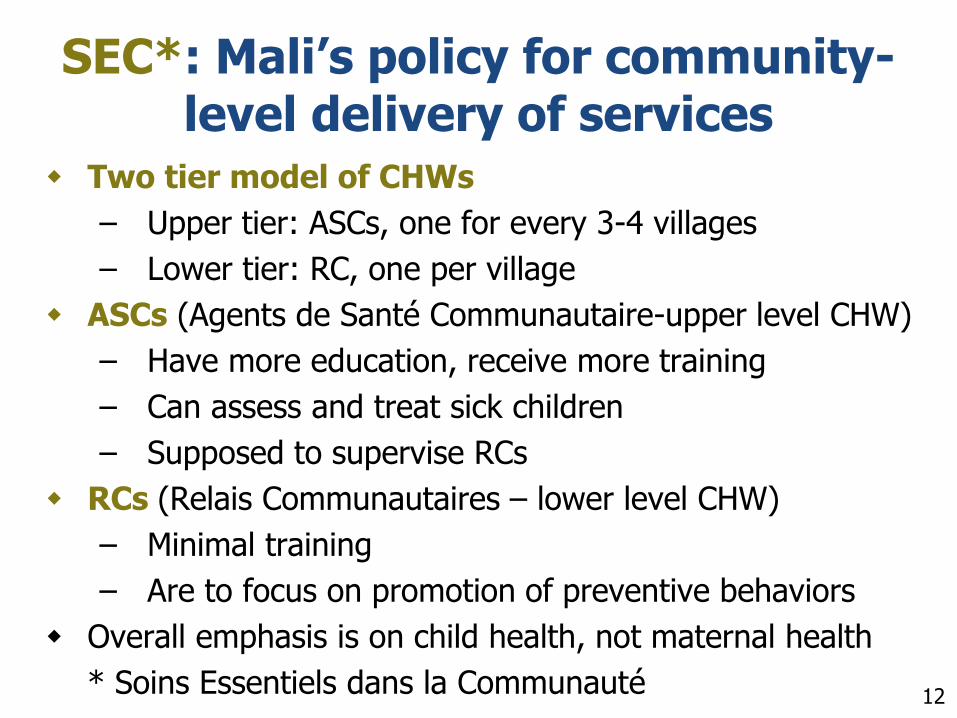
SEC*: Mali’s policy for community-level delivery of services
Two tier model of CHWs
– Upper tier: ASCs, one for every 3-4 villages
– Lower tier: RC, one per village
ASCs (Agents de Santé Communautaire-upper level CHW)
– Have more education, receive more training
– Can assess and treat sick children
– Supposed to supervise RCs
RCs (Relais Communautaires – lower level CHW)
– Minimal training
– Are to focus on promotion of preventive behaviors
Overall emphasis is on child health, not maternal health
* Soins Essentiels dans la Communauté 12

SEC: Mali’s policy for community-level delivery of services
In our current NIH R21, we started with equal emphasis on maternal and child health
After initial site visits and consultations with partners
– We are now looking to developing the maternal health components of the SEC
– Emphasis on antenatal care, birth planning and emergency transport
– mHealth playing a supportive role
13

Study site: SélinguéHealth District
South-west of Bamako
On both sides of Lake Sélingué
One District Hospital where C-sections performed
Seven community health centers
"Lac Sélingué" by Olivier EPRON - Own work. Licensed under CC BY 2.5 via Wikimedia Commons -
14

Sikasso Region
Lake Sélingué
15
Vision for intervention
Focus on:
– Provision of services to women during antenatal and intrapartum periods
– Improving communication between different community-level providers
– Link community-level providers to health facilities
Key role for ASC in communication, this role currently undeveloped
16

Role of ASC
17
Assessment and treatment of sick children
Coordination and communication of health system at community level

ASC
RC RC RC RC
Auxiliary Nurse-
Midwives
Women and their families
Improved communication with community-based providers
18
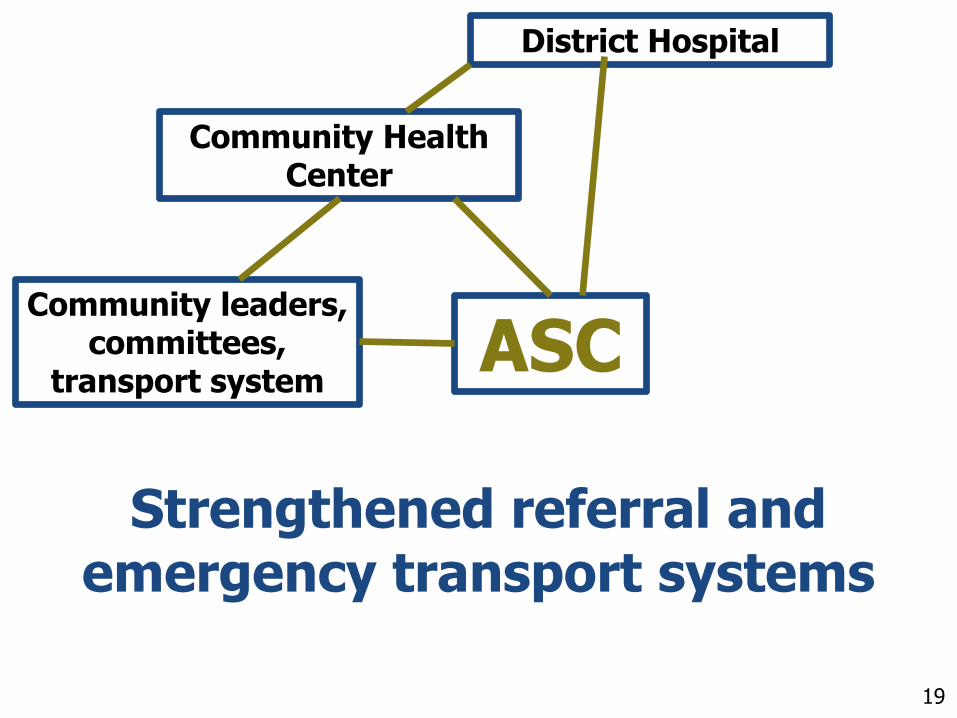
ASCCommunity leaders,
committees, transport system
Community Health Center
District Hospital
Strengthened referral and emergency transport systems
19

ASC
RC RC RC RC
Auxiliary Nurse-
Midwives
Community leaders, committees,
transport system
Community Health Center
District Hospital
Women and their families20

Tracking of pregnant women (1) Build upon Mali’s SNISI platform for
mHealth interventions, operated by ANTIM
ASC and others to enter women into tracking system as early as possible in pregnancy
Receipt of key interventions tracked, e.g.
– Antenatal care attendance
– SP tablets*: 1/month starting Month 4
– Tetanus toxoid vaccination
– Blood pressure measurement* Sulfadoxine-Pyramethamine intermittent preventive treatment for malaria 21

Tracking of pregnant women (2)
If a pregnant woman misses or is late for a key intervention
– ASC is notified: ASC visits woman, or ASC calls RC to visit woman
ASC or RC call or visit women weekly late in pregnancy
– Remind woman and family of emergency transport system
– Advise early use of system22
Emergency transport system
Currently three (or more) types
– Community-based
– Health center-based
– District hospital-based / ambulance
No formal linkage or communication between the different systems
Many calls go directly to ambulance driver at District Hospital, who does triage
We are examining lessons learned from existing systems e.g. Diangounté Camara 23

Tracking of pregnant women (3)
Analysis of outcomes in monthly meetings at Health Centers and District Hospital
– Time from first contact with system to arrival at Health Center or District Hospital
– Antenatal care interventions: SP, tetanus toxoid, blood pressure monitoring etc.
24

Next steps
Current:
– Develop intervention content
– Define mHealth platform & technology
June 2015: Baseline survey
July 2015-May 2016: Pilot test of intervention components for feasibility, acceptability
June 2016: Final survey
25