methyl methacrylate concentrations in tissues adjacent to bone cement
TRANSCRIPT

Methyl methacrylate concentrations in tissues adjacent to bone cement
William Petty Department of Orthopaedic Surgery, J. Hillis Miller Health Center, University of Florida, Gainesville, Florida 32610
The amount of methyl methacrylate mono- mer present in bone tissue immediately ad- jacent to implanted bone cement that has polymerized in vivo has been determined. Poly(methy1 methacrylate) was implanted into the distal femoral condyle of the dog and allowed to polymerize. At various times following polymerization, samples were removed and sections adjacent to the cement were cut and subjected to homoge- nization followed by liquid gas chromato- graphic determination of the amount of
methyl methacrylate monomer present. The highest concentration of methyl meth- acrylate monomer present in bone tissue was 0.140% in the 1000 pm of bone tissue adja- cent to bone cement immediately after polymerization of the cement. The concen- tration was very similar (O.r37%) 1 hr after cement polymerization, but dropped off rapidly following that with no free methyl methacrylate monomer present in bone tis- sue adjacent to cement after 4 hr following cement polymerization.
INTRODUCTION
The use of poly(methy1 methacrylate) bone cement has achieved clinical acceptance in neurosurgical, dental, and orthopaedic operative procedures. It has gained wide acceptance in orthopaedic surgery because of the excellent results obtained when artificial joints are mechanically secured in bone with bone ~ e m e n t . ~ , ~ , ~ Two major complications of the use of bone cement include loosening of the cement mass at the bone cement interface and i n f e ~ t i o n . ~ , ' ~ Both these complications often necessitate major revision surgery or removal of the prosthesis and cement. It is known that necrosis occurs in bone tissues surrounding implanted bone cement; this tissue necrosis may contribute to loosening and infection. Surgical insult, including dissection of soft tissues from bone and bone reaming resulting in decreased vascularity to the bone, heat of polymerization, and chemical toxicity of methyl methacrylate monomer have all been proposed as possible causes of the tissue necrosis.2,6,8,10,11J3,23,26 Various studies have been performed in vifro to determine the effects of methyl methacrylate monomer on mammalian cells and proteins as well as its effect on Other experiments have been designed to simulate in vivo polymerization of cement by in vifro methods in an attempt to gain some information regarding how much methyl methacrylate monomer is present
Journal of Biomedical Materials Research, Vol. 14,427-434 1980 0 1980 John Wiley & Sons, Inc. 0021-93041 80/0014-0427$01.00
428 PETTY
in tissues adjacent to bone cement that polymerizes in 7 ~ i v 0 . ~ , ~ ~ , ~ ~ In the study reported here, the amount of methyl methacrylate monomer present in tissues immediately adjacent to bone cement that has polymerized in vim has been determined.
MATERIALS AND METHODS
Liquid gas chromatographic techniques were used to determine methyl- methacrylate concentration in tissues adjacent to poly(methy1 methyacrylate) following in vim polymerization in the femoral condyle of the dog.
Surgical technique
Sixteen to twenty kilogram dogs were obtained from the University of Florida Health Sciences Animal Farm and carefully evaluated for infectious disease or other illness prior to experiments. They were housed at the animal farm and fed standard laboratory chow and water as desired. All surgery was performed in the surgical suite of the University of Florida Health Sciences Animal Quarters. After induction of suitable general anesthesia and sterile preparation and draping of the operative area, a 3-cm incision was made cen- tered over the lateral portion of the distal femur and dissection carried to bone. A specially constructed punch was used to remove a 5 sq. mm piece of bone
I II
0 - lOP0" ','/ i i ; 1000 -2000#' ' ,, 2000 - 3 O C O / 3"00-40"1)/
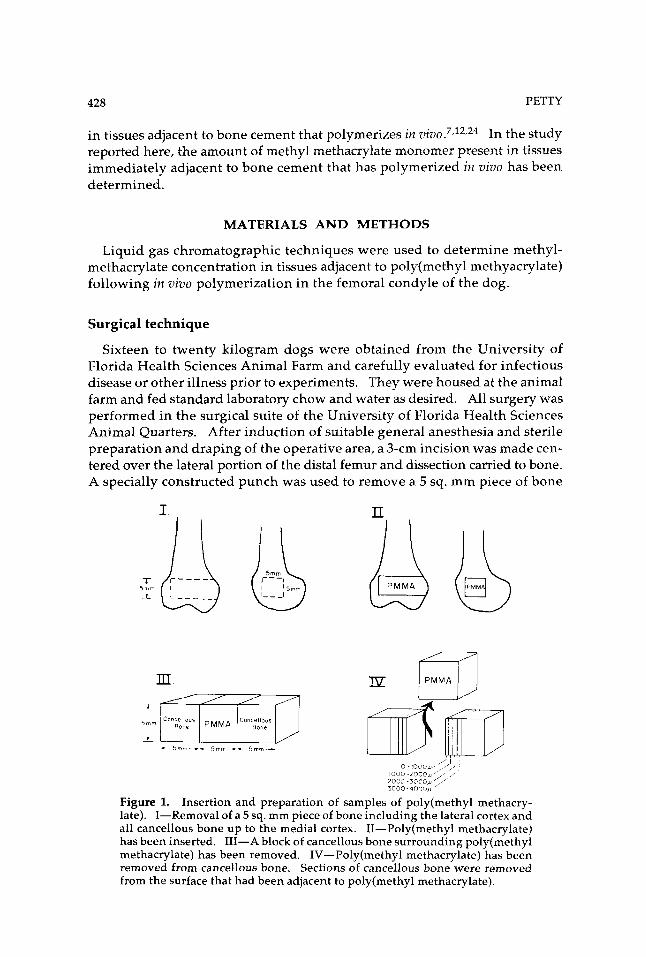
Figure 1. Insertion and preparation of samples of poly(methy1 methacry- late). I-Removal of a 5 sq. mm piece of bone including the lateral cortex and all cancellous bone up to the medial cortex. 11-Poly( methyl methacrylate) has been inserted. 111-A block of cancellous bone surrounding poly(methy1 methacrylate) has been removed. IV-Poly(methy1 methacrylate) has been removed from cancellous bone. Sections of cancellous bone were removed from the surface that had been adjacent to poly(methy1 methacrylate).

METHYL METHACRYLATE CONCENTRATION 429
which included the lateral cortex and cancellous bone to, but not through, the medical cortex (Fig. 1). Surgical Simplex-I' was mixed and at the end of 4 min of stirring at 60 beats per minute, the dough was placed in the defect in the femur. The defect was filled completely but forceful packing was avoided to allow easier removal from the adjacent cancellous bone. The poly(methy1 methacry late) was allowed to polymerize and the wound closed.
Collection and preparation of samples
Samples were collected at 0, 1,2,4, 6, and 8 hr following in vivo polymer- ization of poly(methy1 methacrylate). With the animal under general anes- thesia, the distal femur was removed and immediately frozen in liquid nitro- gen. Using a band saw and milling machine, all cortices surrounding the poly(methy1 methacrylate) and cancellous bone were removed. The specimen was then cut into a small segment 5 X 5 X 15 mm, which consisted of a central cube of poly(methy1 methacrylate), volume 5 cubic mm, covered at each end by a volume of 5 cubic mm of cancellous bone (Fig. 1). The poly(methy1 methacrylate) was removed from the bone, and the bone specimens were mounted on a manually operated heavy-duty microtome with a stainless-steel blade. Bone specimens were held in a clamp attached to a micrometer for measurement of section thickness. Sections 1000-pm thick were removed with the microtome, dimensions were confirmed with a hand micrometer, and the specimens were placed in 1 ml of normal saline solution in a small glass tube which was sealed. Beginning at the surface of bone that had been adjacent to the poly(methy1 methacrylate), four sections 1000-pm thick were cut (Fig. 1). The specimens, in saline, were homogenized to prepare them for deter- mination of methyl methacrylate by liquid gas chromatography. Methyl methacrylate is known to have low solubility in water or saline on the order of 1.5% with some variability, depending on the t empera t~ re .~ No concen- tration measured in these experiments approached this maximum solubility; all concentrations measured were on the order of one-tenth or less the known solubility of methyl methacrylate in water. Preparation of the specimens was complete within 30 min of removal from the animal.
Evaluation of samples
Immediately after homogenization, methyl methacrylate monomer was evaluated by liquid gas chromatography in a Hewlett Packard 402 gas chro- matograph. A whole glass column, 2 m X 1 cm packed with 20% polyethylene glycol with chromasorb W 60/80 mesh was used with nitrogen gas. The in- jection port temperature was 150°C and the sample volume was 10 pl. Quantification was by a standard graph using the peak height method. A series of reference solutions containing known amounts of methyl methac- rylate monomer, ranging from 1 to 10 pl per 10 ml normal saline solution, were evaluated. Evaluation of these solutions revealed that concentrations of methyl methacrylate monomer as low as 50 parts per 1,000,000 (0.00005%) could

430 PETTY
be reliably detected by this technique. For determination of the amount of methyl methacrylate contained in the experimental samples, a reference so- lution containing 10 pl of methyl methacrylate monomer per 10 ml normal saline solution was utilized as standard. A glass wool filter was placed in the glass column to absorb any cellular elements and thereby avoid interference with the chromatographic determinations.
The actual volume of tissue in each sample and the concentration of methyl methacrylate in the sample were known, so appropriate calculations yielded the methyl methacrylate monomer concentration per volume of tissue at varying distances from the mass of poly(methy1 methacrylate).
Quadruplicate samples were evaluated in all experiments; and the arithmetic mean, standard deviation of the mean, and standard error of the mean were determined. The significance of differences was evaluated by student’s t - test.
RESULTS
Methyl methacrylate was measured in cancellous bone tissue adjacent to implanted poly(methy1 methacrylate) at distances from 0 to 1000,1000 to 2000, 2000 to 3000, and 3000 to 4000 pm at times following polymerization of cement from 0 to 8 hr (Fig. 2). The mean concentration of methyl methacrylate found within 1000 pm of bone cement immediately after implantation was 0.140%. The concentration was similar (0.137%) 1 hr after cement implantation. With increasing distance form the implanted cement, there was a decreasing con- centration of methyl methacrylate so that immediately after and 1 hr after implantation the concentration was 0.004 and 0.020%, respectively, at a distance of 3000-4000 pl from the cement. By 2 hr following implantation, the mean concentration within 1000 pm of the cement was 0.027% and had dropped to
3 0.20, m
2000 - 3090 rnacmnr
3000 4000mrrrm “;ir 0 1 2 3 4 5 6
s
Time(hours )
Figure 2. Methyl methacrylate monomer present in cancellous bone tissue at various distances from the cement mass 0 to 6 hr following polymerization of poly(methy1 methacrylate) in viva

METHYL METHACRYLATE CONCENTRATION 431
0.015% at 4 hr. By 4 hr, there was no detectable methyl methacrylate beyond 1000 p1 from the cement; and by 6 hr, no methyl methacrylate was detectable in any of the areas tested including the 1000 pm area immediately adjacent ot the cement mass.
DISCUSSION
It is known that methyl methacrylate is released during polymerization, and it has been suggested that it may be slowly leached out of the polymerized material into the surrounding tissues for some time following implantat i~n.~ Though it is a toxic substance in high enough concentration, recent studies indicate that the amount of methyl methacrylate released into the systemic circulation does not cause significant systemic t o x i ~ i t y . ~ , ~ ~ , ' ~
The concentration of methyl methacrylate monomer in tissue adjacent to implanted cement has not been determined previously. It has been suggested that the monomer may not be carried away rapidly due to the low solubility of methyl methacrylate and the vascular trauma in the bed of implanta- tion.lJ0
The experiments reported here reveal that concentrations of methyl meth- acrylate in cancellous bone adjacent to cement are low, and that they are sus- tained for only a brief period of time. Immediately following and 1 hr fol- lowing in vivo polymerization of poly(methy1 methacrylate), there was a concentration of methyl methacrylate in the tissue adjacent to cement in the same range as the concentration found in previous experiments to have sig- nificant inhibitory effects on: the antibacterial activity that normal human serum has against Staphylococcus epiderrnidis, the activity of complement, pha- gocytosis and bacterial killing by polymorphonuclear leucocytes, and the cellular responses of human peripheral blood lymphocytes. By 2 hr following implantation the tissue concentrations of methyl methacrylate had dropped to a level found to have slight inhibitory activity only to complement activity and perhaps lymphocyte responses. Four hours following poly(methy1 methacrylate) polymerization, the concentration of methyl methacrylate in the tissue had dropped so low that the concentration was not high enough to effect any of the inhibition of immune mechanisms that was demonstrated in previous in vitro s t ~ d i e s . l ~ - ~ ~
It is probable that the concentrations of methyl methacrylate found in tissues adjacent to implanted cement in the clinical situation are somewhat higher than the concentrations found in the studies reported here for three reasons: (1) Some of the methyl methacrylate may have evaporated between the time of removal of the specimen from the animal and the time of methyl methac- rylate determination, but this time never exceeded 30 min. In experiments in our laboratory, the loss of methyl methacrylate monomer from open con- tainers of methyl methacrylate solutions, ranging from 0.039 to 1.25% in both human serum and saline solutions occurred in a nearly linear fashion with loss of less than 5% at 30 min, 50% at 12 hr, and 75% at 24 hr. Thus, it is unlikely that substantial amounts of methyl methacrylate were lost from the specimens

432 PETTY
during ~repara t i0n . l~ (2) In order to allow easy removal of the polymerized cement, significant pressure at the time of implantation was avoided, to avoid interdigitation of the cement with the cancellous bone. This, no doubt, sig- nificantly reduced the surface area of cement in contact with tissue, and Linder has demonstrated that surface area is an important determinant for the amount of monomer released from cement during polymerization.12 (3) The smallest distance for which these experiments determined the concentration of methyl methacrylate was 1000 pm of bone tissue. Since the concentration increased progressively from the 3000 to 4000 micrometer section to the 0 to 1000 pm section, it appears probable that the concentration in the first 100 pm from the cement, for example, would be higher than the concentration measured which was an average concentration for the entire first 1000 pm. However, in ex- periments conducted 6 and 8 hr following polymerization of cement, no methyl methacrylate was detected in tissues adjacent to the cement by the chromatographic method used in these experiments which detects methyl methacrylate in a concentration as low as 50 parts per 1,000,000 or 0.00005%. Therefore, even though concentration of monomer may be somewhat higher in the clinical situation than the values reported here, it is unlikely that there are significant amounts of monomer present in tissue for more than a few hours following polymerization. This is in agreement with the in uitro studies of both Linder et al. and Schoenfeld et al. who demonstrated that most free monomer that was released into aqueous medium was released within a few minutes of p01ymerization.l~~~~ Willert et al. reported that in vitro polymer- ization of poly(methy1 methacrylate) in bone marrow resulted in higher tissue concentrations of monomer (1-2.5% for fat and 0.12-0.5% for red blood cells) than found in the experiments reported here. The experiments of Willert et al. were performed in semiliquid bone marrow which was separated into three phases: (1) fat; (2) a mixture of fat, bone elements, and blood cells; and (3) blood cells. This material would be expected to contain considerably more fatty material than was present in the tissues examined in the experiments reported here, or in the cancellous bone in the metaphyseal region, or along the inner cortex of the bone in which poly(methy1 methacrylate) is implanted in the clinical situation. In addition, the experiments reported by Willert et al. were performed in vifro in a sealed container which prevented any loss of methyl methacrylate, while the experiments reported here were performed in vivo allowing the possibility of monomer dissipation due to metabolism of the methyl methacrylate and removal by the vascular system. These differ- ences may explain the different concentrations found in the studies by Willert et al. and those reported here.26
The studies reported here indicate that methyl methacrylate monomer is present in tissue adjacent to implanted cement in sufficient concentration to have an adverse effect on human cells and'proteins. However, this concen- tration is maintained probably for no more than 4 hr and possibly for no more than 2 hr following implantation. Even though there is significant vascular trauma when a site in bone is prepared for an implantation and methyl methacrylate solubility is low, vascular supply surrounding the implant bed

METHYL METHACRYLATE CONCENTRATION 433
Foundation.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
possibly combined with some metabolism of methyl methacrylate are sufficient to cause rapid dissipation of methyl methacrylate monomer following poly- (methyl methacrylate) implantation.
This work was supported in part by a grant from the Orthopaedic Research and Education
M. Brookes and S. C. Gallannaugh, ”Circulatory Depression in Bone After Acrylic Implantation,” Clin. Orthop., 107,274-276 (1975). J. Charnley, Acrylic Cement in Orthopaedic Surgery, Williams and Wilkins, Baltimore, 1970. J. Charnley, “The Long-term Results of Low-friction Arthroplasty of the Hip as a Primary Intervention,” J. Bone J. Surg., 54B, 61-76 (1972). F. R. Convery, D. R. Gunn, J. D. Hughes, and W. E. Martin, “The Relative Safety of Polymethylmethacrylate,” J. Bone Jt . Surg., 57A, 57-64 (1975). M. B. Coventry, R. D. Beckenbaugh, D. R. Nolan, and D. M. Ilstrup, ”2,012 Total Hip Arthroplasties: A Study of Postoperative Course and Early Complications,” J. Bone It. Surg., 56A, 273-284 (1974). R. Feith, Side Effects of Acrylic Cement Implanted into Bone, Drukkenij Brak- kenstein, Nijegen, 1975. S. S. Haas, G. M. Braver, and G. Dickson, “A Characterization of Polym- ethylmethacrylate Bone Cement,” J. Bone It. Surg., 57A, 381-391 (1975). C. D. Jeffries, A. J. C. Lee, and R. S. M. Ling, ”Thermal Aspects of Self- curing Polymethylmethacrylate,” ]. Bone Jt . Surg., 57B, 511-518 (1975). H. F. Mark, Kirk-Othmer Encyclopedia of Chemical Technology, 2nd ed., Wiley, New York, 1967, p. 341. L. Linder, ”Reaction of Bone to the Acute Chemical Trauma of Bone Ce- ment,” J. Bone lt. Surg., 59A, 82 (1977). L. Linder, “Tissue Reaction to Methylmethacrylate Monomer,” Acta. Or- thop. Scand., 47,3 (1976). L. Linder, L. Harthon, and L. Kullberg, ”Monomer Leakage from Poly- merizing Acrylic Bone Cement,” Clin. Orthop., 119,242 (1976). L. Linder and M. Romanus, ”Acute Local Tissue Effects of Polymerizing Acrylic Bone Cement.” Clin. Orthop., 115,303-312 (1976). R. E. McLaughlin, C. A. DiFazio, M. Hakala, B. Abbott, J. A. MacPhail, W. P. Mack, and D. E. Sweet, “Blood Clearance and Acute Pulmonary Toxicity of Methylmethacrylate in Dogs After Simulated Arthroplasty and Intra- venous Injection,” J. Bone J. Surg., 55A, 1621-1628 (1973). J, Modig, C. Busch, and S. Olerud, “The Importance of Intervascular Coagulation, Fat Embolism, and Acrylic Monomers for Respiratory and Circulatory Dysfunctions During Intramedullary Endoprosthetic Surgery,” Proceedings of the Orthopaedic Research Society, in J. Bone It. Surg., 57A, 583 (1975). D. R. Nolan, R. H.Fitzgerald, R. D. Beckenbaugh, and M. B. Coventry, Complications of Total Hip Arthroplasty Treated by Reoperation,” I . Bone Jt . Surg., 57A, 977-981 (1975). R. S. Panush and W. Petty, “The Effect of Methylmethacrylate on Normal Human Peripheral Blood Lymphocytes,” Clin. Orthop., 134, 356-363 (1978). W. Petty, and J, R. Caldwell, “The Effect of Methylmethacrylate on Com- plement Activity,” Clin. Orthop., 128,354-360 (1977). W. Petty, ”The Effect of Methylmethacrylate on the Bacterial Inhibiting Properties of Normal Human Serum,” Clin. Orthop., 132, 266-278 (1978). W. Petty, “The Effect of Methylmethacrylate on Chemotaxis of Polymor- phonuclear Leucocytes,“ J. Bone Jt . Surg., 60A, 492-498 (1978).

434 PETTY
21. W. Petty, "The Effect of Methylmethactylate on Phagocytosis and Bacterial Killing by Human Polymorphonuclear Leucocytes," J. Bone Jf . Surg., 60A, 752-757 (1978). W. Petty, "Influence of Methylmethacrylate on Quantitative Gel Diffusion Assay," J. Biomed. Mat. Res., 13,645-656 (1979). F. W. Reckling, "The Measurement of the Bone-Cement Interface Tem- perature During Total Joint Replacement Procedures." Trans. Orthop. Res. Sac., 1,59 (1976). C. M. Schoenfeld, G. J. Conard, and E. P. Lautenschlager, "Monomer Re- lease from Methacrylate Bone Cements During Simulated In V i m Poly- merization," J. Biomed. Muter. Res., 13, 135-147 (1979). A. B. Welch, "Effect of Simplex Liquid Methyl Methacrylate Monomer on Cells, J. Biorned. Muter. Res., 12,775-790 (1978). H. G. Willert, H. A. Frech, and A. Bechtel, Biomedical Application of Polymer, H. P. Gregor, Ed., Plenum, New York, 1975.
22.
23.
24.
25.
26.
Received October 15,1979 Accepted January 30,1980