mesure de la crf comme indicateur du recrutement...
TRANSCRIPT

Laurent Brochard Toronto
Laurent Brochard Toronto
Synchronie Patient-Ventilateur

Conflicts of interest
• Our clinical research laboratory has received research grants for clinical research projects from the following companies: – Covidien (PAV+)
– Dräger (SmartCare)
– General Electric (FRC)
– Philips (NIV-sleep)
– Fisher Paykel (High flow)
– To the Hospital: Maquet (NAVA)

Dose of support? D
ysfu
nct
ion
Quantity of Ventilatory Support
Respiratory Distress
VILI VALI VIDD
Normal
Patient-Ventilator Asynchrony
Patient-Ventilator
Asynchrony

ICU ventilators
Servo I
Engström Galileo
Evita 4
Extend
Avea
PB 840

Pes
Paw
Good Synchrony: Paw follows Pes
time

Clinical consequences of asynchronies?
•Dynamic hyperinflation
•Excessive or insufficient ventilatory assistance
•2)
•1)
•3) •Sedation
•4)
•5) •Errors in assessing weaning readiness
•6) •Prolonged duration of ventilation
•Sleep fragmentation
•7) •Respiratory sequelae...

ICM 2006

Multivariable model : mechanical ventilation duration for the group of patients with asynchrony index>10% was 10 days, 95% CI
(4.1; 25.0) compared to 4 days, 95% CI (2.7; 5.6) for the group of patients with ITI <10% (p .0004).
De Wit CCM 2009


Blanch L et al. ICM 2015

Assistance in excess
• Apneas
• Ineffective Efforts or Missed Cycles

Pressure support ventilation

Pressure support ventilation

1 min Parthasarathy. AJRCCM 2002;166:1423
C4-A1
O3-A2
ROC
LOC
Chin
Leg
VT
RC
AB SpO2
EKG
Assist-Control Pressure Support Arousal

2002

Assist-Control, PEEP 10 cmH2O
Triggering asynchrony Chao et al., Chest 1997; 112: 1592-1599
Assist-control, ø PEEP

-2
0
2
4
6
0 2 4 6 8
Wasted Effort: Ineffective breath
Esophageal
Pressure
(cmH2O)
0
5
10
15
20
25
Airway
Pressure
(cmH2O)
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8Pressure drop
Flow increase
Time (s)
Flow
(L/s)
Intrinsic
PEEP
Ineffective triggering
Start of patient’s effort
Start of ventilator insufflation

-0,6
-0,4
-0,2
0
0,2
0,4
0,6
0,8
0 2 4 6 8 10 12
-10
-5
0
5
0 2 4 6 8 10 12
0
5
10
15
20
25
0 2 4 6 8 10 12
Weak effort
Flow
(L/min)
Airway
Pressure
(cmH2O)
Esophageal
Pressure
(cmH2O)

-1
-0.5
0
0.5
1
0 3 6 9 12
0
10
20
30
40
0 3 6 9 12
Time (s)
-1
-0,5
0
0,5
1
1,5
0 3 6 9 12 15
0
10
20
30
0 3 6 9 12 15
Airway
Pressure
Flow
PSV
ACV
Flow
Airway
Pressure


Delayed
triggering Delayed cycling
Ineffective Triggering



Patient Respiratory Rate (min-1)

0
5
10
15
20
25
0 1 2 3
0
5
10
15
20
25
0 1 2
0
5
10
15
20
25
0 1 2 3
0
5
10
15
20
25
0 1 2
Airway Pressure (cmH2O)
Baseline PS-ZEEP
Baseline PS-PEEP
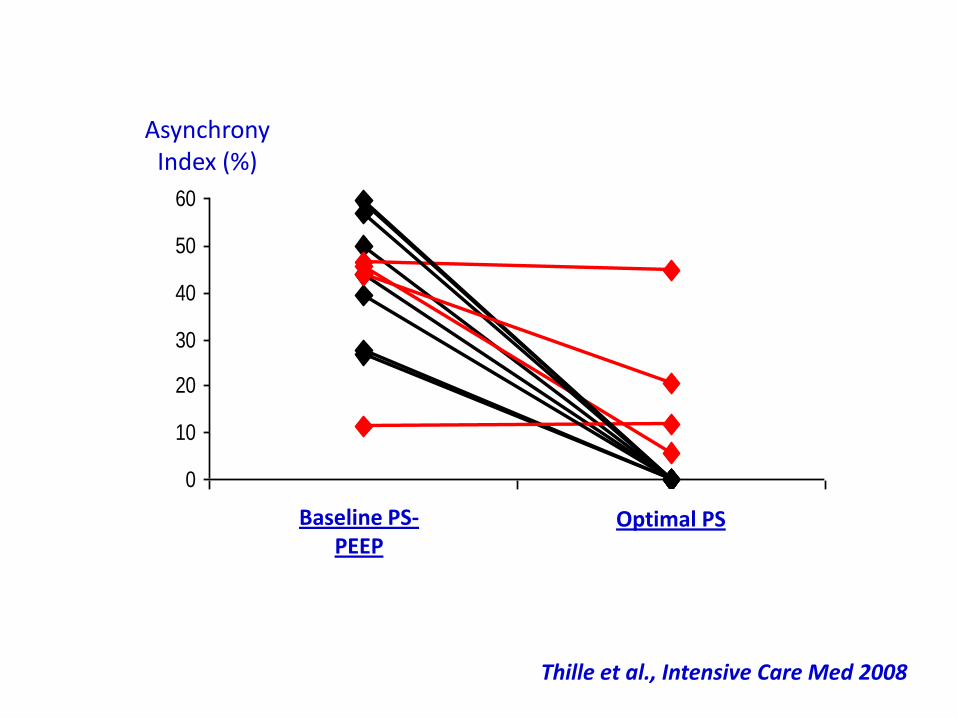
Optimal PS Optimal Ti
Time (s)
Intensive Care Med 2008

Thille et al., Intensive Care Med 2008
0
10
20
30
40
50
60
PS basal PS optimal
Asynchrony Index (%)
Baseline PS-PEEP
Optimal PS
Thille et al., Intensive Care Med 2008

Baseline PS Optimal PS
PS (cmH2O) 20.0 [19.5-20.0] 13.0 [12.0-14.0]
RR ventilator 16.1 [12.4-17.2] 22.4 [22.0-31.3] *
RR patient 26.5 [23.1-31.9] 29.4 [24.6-34.5]
Ti Ventilator (s) 1.3 [1.0-1.8] 0.8 [0.8-1.0] *
PTP (cmH2O.s/min) 61 [58-81] 82 [61-106]
VT (ml) 571 [487-638] 349 [336-368] *
VT (ml/kg, IBW) 10.2 [7.2-11.5] 5.9 [4.9-6.7] *
Reducing tidal volume to reduce patient-ventilator asynchrony
Thille et al., Intensive Care Med 2008

(Hidden) Assistance in excess
• Auto triggering

Short cycle and distortion of flow signal
No airway pressure drop at the beginning of the cycle
No effort
When to suspect
auto-triggering ?
During controlled ventilation:
• RR > adjusted RR
• Respiratory alkalosis
During assisted ventilation:
• Sudden increase or persistently
high respiratory rate
•Absence of an airway pressure
drop at beginning of the cycle
• PSV: short cycle with a flow
signal distortion
• ACV: abrupt airway pressure
increase
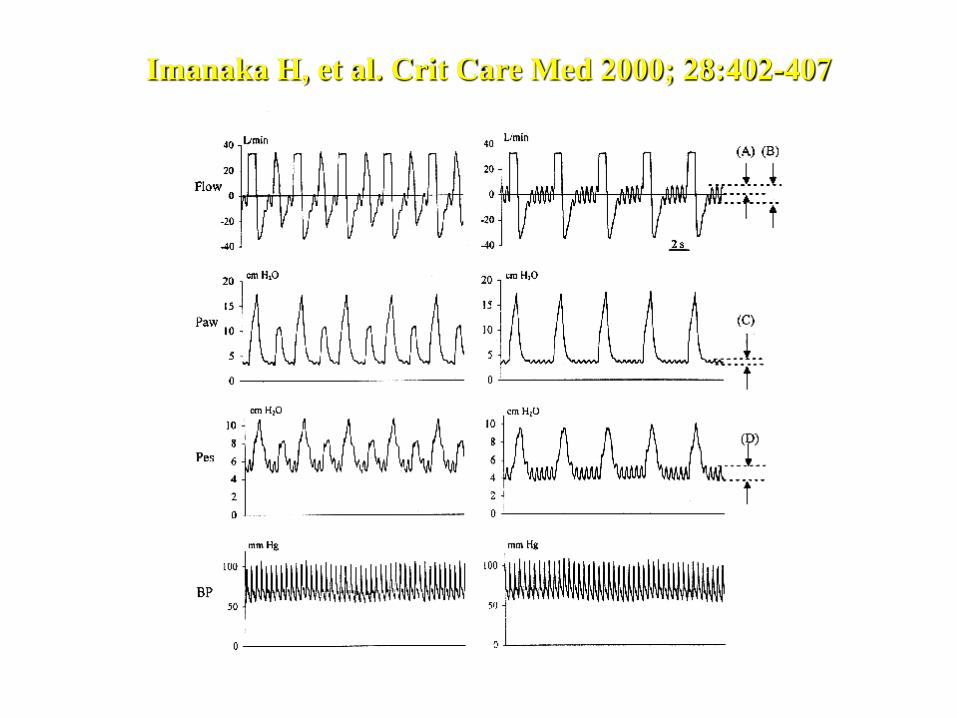
Imanaka H, et al. Crit Care Med 2000; 28:402-407

Insufficient Assistance
• Double triggering, breath stacking and short cycles

-5
0
5
10
0 2 4 6 8 10
-5
0
5
10
0 1 2 3
0
5
10
15
20
0 1 2 3
-0,8
-0,4
0
0,4
0,8
1,2
0 1 2 3
-0.8
-0.4
0
0.4
0.8
1.2
0 2 4 6 8 10
0
5
10
15
20
25
30
0 2 4 6 8 10
Flow
(L/min)
Airway
Pressure
(cmH2O)
Esophageal
Pressure
(cmH2O)
Beginning of patient’s effort
End of patient’s effort
Double Triggering
Continuation of
patient’s effort
A B
Under Assistance

ACV

KALLET et al., Critical Care Med 2006; 34:8-14
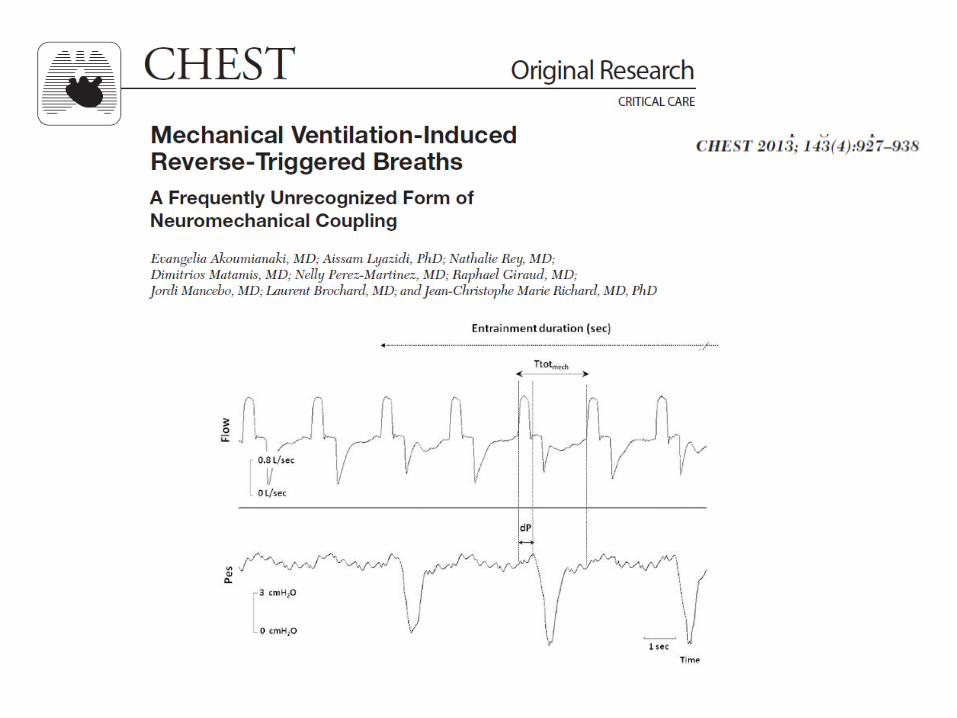
Excessive Sedation?
• Respiratory Entrainement or Reverse Triggering

A
EAdi (µV)
Paw (cm H2O)
Flow (L/sec)
Respiratory Entrainment
Akoumianaki E et al Chest 2012

Paw (cm H2O)
Flow (L/sec)
EAdi (µV)
Accidental observation…

Flow
Paw
Pes
VT
Clinical consequences: VT increase

Clinical consequences: double cycle

Tool: screen and ventilator waveforms
Education and Training
Automated Monitoring
Excessive Assistance : apneas, ineffective efforts
Insufficient Assistance : Short Insufflation & double cycles
Reverse triggering
Autotriggering
Patient Ventilator dys or a-synchrony