medvet drug protocols
TRANSCRIPT
MedVet Drug Protocols
Introduction The following are best practice protocols for drug dilutions commonly used in our hospitals. These are provided for a quick, accessible reference as you prescribe and deliver injectable medications to patients.
The protocol information includes alternative drug names, indications, dosages, tips for reconstitution/dilution, administration recommendations, compatibility notes, contraindications, adverse effects, storage, and additional comments.
If you have questions about a protocol or suggestions for additional drugs, please email [email protected].
Acetylcysteine ......................................................................................................................... 05 Alfaxalone ................................................................................................................................ 07
Amikacin .................................................................................................................................. 08 Aminocaproic Acid ................................................................................................................... 09 Amiodarone (Nexterone) ........................................................................................................ 10 Amphotericin B ........................................................................................................................ 11
Ampicillin & Sulbactam ........................................................................................................... 12 Ampicillin ................................................................................................................................. 13 10% Calcium Gluconate ........................................................................................................... 14 Cefazolin .................................................................................................................................. 15
Cefotaxime Sodium ................................................................................................................. 16 Ceftazidime .............................................................................................................................. 17 Ceftriaxone .............................................................................................................................. 18 Clindamycin ............................................................................................................................. 19 Dexmedetomidine ................................................................................................................... 20
Diazepam ................................................................................................................................. 21 Diltiazem .................................................................................................................................. 22 Dobutamine ............................................................................................................................. 23 Dopamine ................................................................................................................................ 24
Doxycycline .............................................................................................................................. 25 Enrofloxacin ............................................................................................................................. 27 Epinephrine ............................................................................................................................. 28 Erythromycin ........................................................................................................................... 29
Esmolol .................................................................................................................................... 30 Fentanyl ................................................................................................................................... 31 Fomepizole .............................................................................................................................. 32 Furosemide .............................................................................................................................. 33 Glucagon .................................................................................................................................. 35
Heparin (Unfractionated) ........................................................................................................ 36
Table of Contents
Hydromorphone ...................................................................................................................... 37
Ketamine ................................................................................................................................. 38
Levetiracetam .......................................................................................................................... 39
Lidocaine ................................................................................................................................. 40
Lipid Emulsion (Ile) .................................................................................................................. 41
Magnesium Sulfate .................................................................................................................. 42
Mannitol .................................................................................................................................. 44
Meropenem ............................................................................................................................. 45
Metoclopramide ...................................................................................................................... 46
Metronidazole ......................................................................................................................... 47
Midazolam ............................................................................................................................... 48
Naloxone ................................................................................................................................. 49
Nitroprusside ........................................................................................................................... 50
Norepinephrine ....................................................................................................................... 51
Oxymorphone .......................................................................................................................... 53
Pantoprazol ............................................................................................................................. 54
Piperacillin-Tazobactam .......................................................................................................... 55
Procainamide ........................................................................................................................... 56
Propofol ................................................................................................................................... 57
Pyridostigmine Bromide .......................................................................................................... 59
Simbadol (Buprenorphine) ...................................................................................................... 60
Vasopressin ............................................................................................................................. 61
Table of Contents
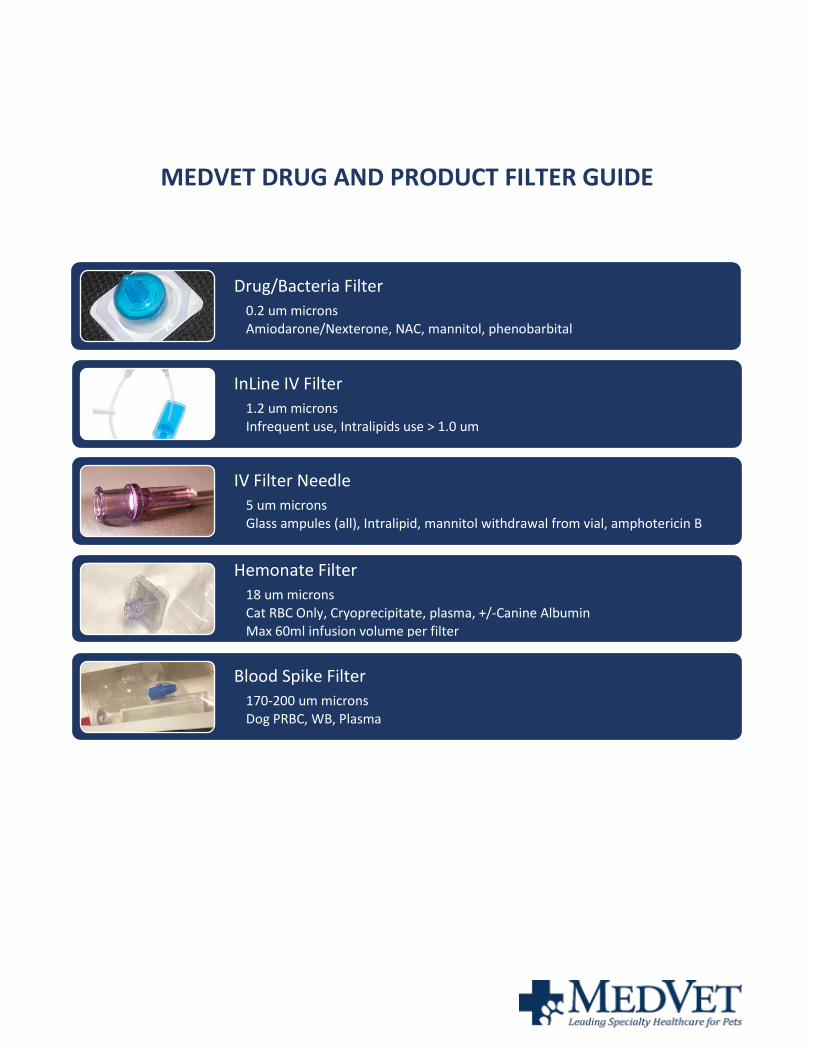
Drug/Bacteria Filter
0.2 um microns Amiodarone/Nexterone, NAC, mannitol, phenobarbital
InLine IV Filter
1.2 um microns Infrequent use, Intralipids use > 1.0 um
IV Filter Needle
5 um microns Glass ampules (all), Intralipid, mannitol withdrawal from vial, amphotericin B
Hemonate Filter
18 um microns Cat RBC Only, Cryoprecipitate, plasma, +/-Canine Albumin Max 60ml infusion volume per filter
Blood Spike Filter
170-200 um microns Dog PRBC, WB, Plasma
MEDVET DRUG AND PRODUCT FILTER GUIDE
5 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Other Names N-acetylcysteine, NAC, Mucomyst
Indications Used to prevent methemoglobinemia and hepatic necrosis in the treatment of acetaminophen toxicity (especially in cats), used for its hepatic protective effects in acute liver failure.
Less commonly used for free radical scavenging and nebulized to help break up mucous in the lungs.
Dosage Dogs/cats: 140mg/kg loading dose IV, then 70mg/kg IV or PO q6-8h – total dosing regimen depends on toxicity/disease – minimum recommend 7, may be up to 17 (PO dosing may be difficult as not very palatable)
Cats: 100mg/kg IV q6hr (less bioavailable PO) *
NAC Inhalation solution (for respiratory use): Dogs/cats: 50 ml/hr-nebulized for 30-60 minutes every 12 hours (watch for bronchospasm)
Supplied as Acetylcysteine/Mucomyst Respiratory (Inhalation) Sol: 10% (100mg/ml), 20% (200mg/ml)
Although Inhalation NAC is NOT labeled for IV administration, it can be safely given IV once diluted to 5% by using a bacteriostatic filter (0.2 µm=micron filter). DO NOT USE HEMONATE FILTER - pores are too large to filter bacteria.
Acetadote/Acetylcysteine Intravenous Inj Sol: 200mg/ml (No filter needed)
Acetylcysteine/Mucomyst/Mucosal Acetylcysteine Oral Sol: 10% (100mg/ml)
DO NOT GIVE IV EVEN WITH FILTER!!!
Reconstitution/Dilution • Most commonly available=Inhalation N-Acetylcysteine 20% (200 mg/ml)
• Dilution required: Dilute to 5% with D5W (Final concentration: 50mg/ml)
• Example: 1ml of 20% solution (200mg) should be added to 3ml D5W= 4ml of 50 mg/ml
• Acetylcysteine 20% is usually diluted to a concentration of 5% (final concentration of 50mg/ml) This concentration can be obtained by adding 1 part injection (20%) to 3 parts of diluent.
• Acetylcysteine is compatible with dextrose 5% (D5W), Sodium Chloride 0.45% injection (half-normal saline).
• D5W most common
Acetylcysteine
6 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Administration Administration IV: 20% IV or Inhalation solution MUST be diluted to 5% with D5W. Inhalation solution MUST be used with a bacteriostatic membrane filter (0.2 µm=micron filter-NOT HEMONATE) during IV administration. Give IV injections slowly over 20-60 minutes.
FILTER: USE A 0.2-micron membrane filter
Oral solution (Mucomyst): DO NOT USE IV-The 10% or 20% solution should be diluted to a 5% solution (50 mg/ml) with D5W to increase palatability and minimize vomiting.
Use diluted solutions within 1 hour of preparation.
For acetaminophen toxicity: Ideally give IV, if you must give PO then give first PRIOR to charcoal, serial PO doses should be spaced from activated charcoal administration by 2-3 hours.
Compatibility Incompatible with amphotericin, ampicillin, erythromycin, tetracycline, and trypsin
Compatible with Dextrose 5% (D5W), 0.45% Sodium Chloride
Contraindications Caution in animals with bronchospastic diseases
Adverse Effects Hypersensitivity, allergic reactions noted if administered without a filter
Storage
• Unopened vials can be stored at room temperature until expiration. Once opened, must be refrigerated, and discarded within 96 hours.
• Inhalation NAC: Once opened, must be refrigerated, and discarded within 96 hours.
• Do not need to discard if discolored or light purple if within 96 hours.
• Products labeled for IV use should be discarded after 24 hours.
• If kept in oral syringes for ORAL USE – 600 mg/3mL (20%) is stable for 6 months – DO NOT USE FOR IV; Use diluted oral solutions within 1 hour of preparation.
Notes The bottles are labeled as “NOT FOR INJECTION” however, this solution has been found to be safe to administer IV to dogs and cats when diluted to 5% and given via a 0.2-micron filter.
*Cat dosing may need to be higher- (PK from Buur. Am J Vet Res 2013 Feb;74(2):290-3)
Please address any corrections, questions, or suggestions to: [email protected].
Acetylcysteine
7 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Alfaxalon
Other Names Alfaxan multidose
Indications Anesthetic Heavy sedation
Dosage Dogs: Bolus Induction of anesthesia: 1-3 mg/kg IVSedation:1-3mg/kg IM/SQCRI: 0.05-0.15 mg/kg/min
Cats: Induction of anesthesia: 1-3 mg/kg IVSedation:1-3 mg/kg IM/SQCRI: 0.05-0.15mg/kg/min
Supplied as Alfaxalone 10 mg/mL
Dilution Dilution not required for CRI administration unless necessary for accurate volume via syringe pump (>1ml/hr)
Administration IV or IM or SQ
Compatibility Limited compatibility information has been studied; however, it has been mixed safely with many drugs for premedication/sedation such as ketamine, midazolam, various opioids, and dexmedetomidine. Drugs should not be mixed until immediately before administration.
Contraindications Always be cautious of the respiratory depressive effects of this drug, even when administered IM/SQ. Large doses and even more modest doses used in combination with other sedatives can cause significant respiratory depression and even apnea in some patients. All patients receiving this drug should be closely monitored after administration. Not advisable to use this as an induction agent prior to splenectomy.
Adverse Effects Respiratory depression and apnea. Tachycardia is observed in some patients, especially those with preexisting hypovolemia. Splenic engorgement.
Storage Schedule IV controlled drug - must be stored in a lockbox. Store at room temperature. Once punctured each bottle is good for 56 days.
Notes Not recommended as a sole agent for sedation as it provides poor muscle relaxation and can lead to myoclonus, muscle fasciculations, and an overall poor quality of sedation. Instead, it should be combined with one to two other agents such as a benzodiazepine/opioid or either on alone. When mixed in the same syringe with midazolam the solution will turn cloudy. This is thought to be due to interaction of the two preservatives and does not appear to have an effect on either drugs’ efficacy. Can be used safely in kittens from 4 weeks of age and puppies from 10 weeks. Shown to be safe for use in canine C-section.
Please address any corrections, questions, or suggestions to: [email protected].
8 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Amikacin
Other Names Amikin, Amiglyde-V
Indications An injectable antimicrobial drug for treatment of susceptible gram-negative, aerobic infections.
Dosage 10-30mg/kg IV or SC once daily.
Renal function should be considered on a case-by-case basis and dose adjusted accordingly.
Supplied as Veterinary labeled product – 50 mg/mL in 50 mL vials – may not be available
Human labeled product – 50 mg/mL and 250 mg/mL in 2 mL and 4 mL vials
Dilution Amikacin is supplied as a 250mg/ml concentration. Dilute 1:50 to a final concentration of 5mg/ml.
Administration IV: Give over 30-60 minutes Can be given SQ and IM as well
Compatibility Compatible with 0.45% and 0.9% saline, 5% dextrose (D5W), LRS and Normosol.
Incompatible with many other drugs including fluid additives. If drugs are added to the IVF, the IVF should be stopped during administration
Contraindications Use caution in neonatal & geriatric patients, those with preexisting renal disease, fever, sepsis and dehydrated patients.ly in patients with hepatic dysfunction or respiratory depression
Adverse Effects Nephrotoxicity, ototoxicity, neuromuscular blockade. Cats may be more sensitive to toxic effects.
Storage Unopened vials can be stored at room temperature until expiration. Once diluted, must be refrigerated, and discarded after 24 hours. Solutions may become pale yellow over time, but this does not indicate a loss of potency.
Notes Use caution with other nephrotoxic drugs (3rd gen cephalosporins, amphotericin B, NSAIDS). Monitoring for development of proteinuria or urine casts is recommended.
Please address any corrections, questions, or suggestions to: [email protected].
9 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Aminocaproic Acid
Please address any corrections, questions, or suggestions to: [email protected].
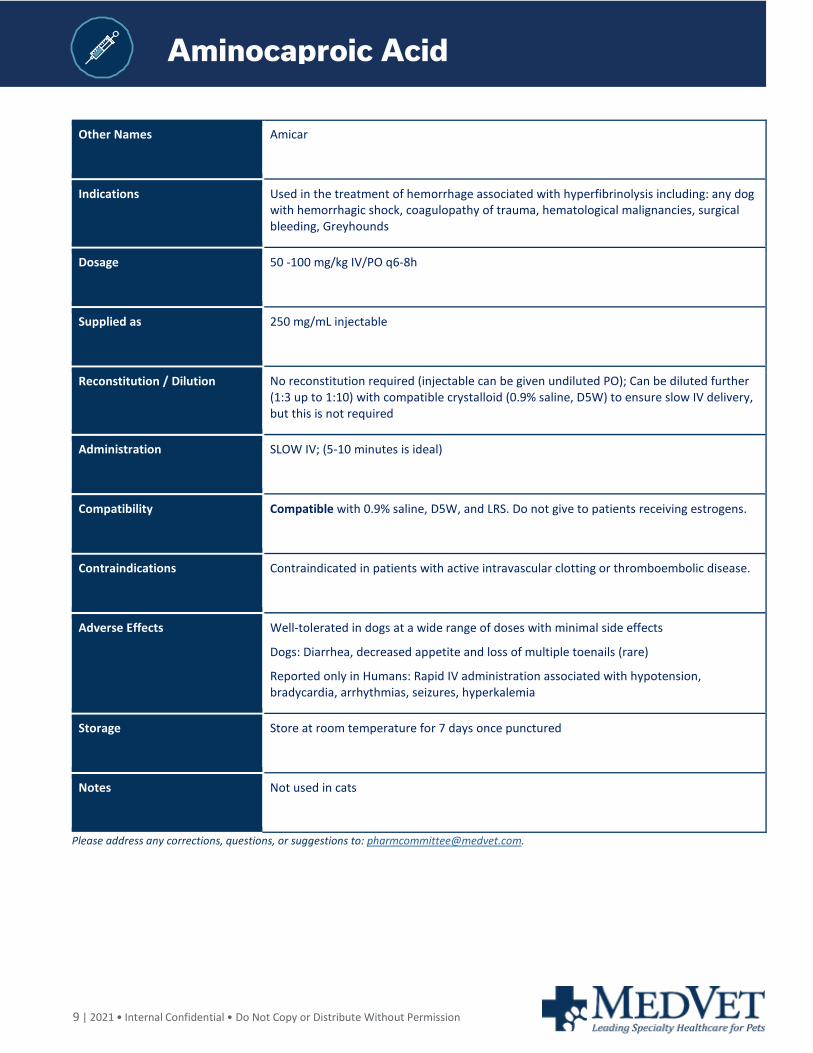
Other Names Amicar
Indications Used in the treatment of hemorrhage associated with hyperfibrinolysis including: any dog with hemorrhagic shock, coagulopathy of trauma, hematological malignancies, surgical bleeding, Greyhounds
Dosage 50 -100 mg/kg IV/PO q6-8h
Supplied as 250 mg/mL injectable
Reconstitution / Dilution No reconstitution required (injectable can be given undiluted PO); Can be diluted further (1:3 up to 1:10) with compatible crystalloid (0.9% saline, D5W) to ensure slow IV delivery, but this is not required
Administration SLOW IV; (5-10 minutes is ideal)
Compatibility Compatible with 0.9% saline, D5W, and LRS. Do not give to patients receiving estrogens.
Contraindications Contraindicated in patients with active intravascular clotting or thromboembolic disease.
Adverse Effects Well-tolerated in dogs at a wide range of doses with minimal side effects
Dogs: Diarrhea, decreased appetite and loss of multiple toenails (rare)
Reported only in Humans: Rapid IV administration associated with hypotension, bradycardia, arrhythmias, seizures, hyperkalemia
Storage Store at room temperature for 7 days once punctured
Notes Not used in cats
10 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Amiodarone (Nexterone)
Amiodarone (Nexterone)
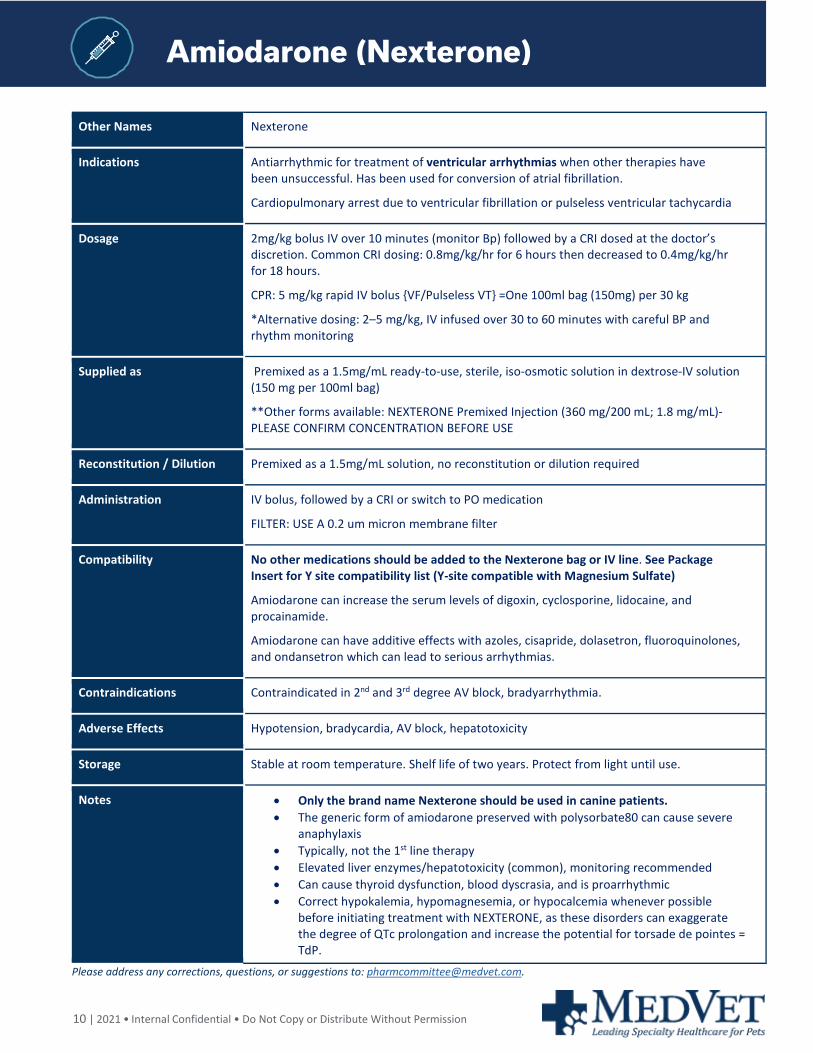
Other Names Nexterone
Indications Antiarrhythmic for treatment of ventricular arrhythmias when other therapies have been unsuccessful. Has been used for conversion of atrial fibrillation.
Cardiopulmonary arrest due to ventricular fibrillation or pulseless ventricular tachycardia
Dosage 2mg/kg bolus IV over 10 minutes (monitor Bp) followed by a CRI dosed at the doctor’s discretion. Common CRI dosing: 0.8mg/kg/hr for 6 hours then decreased to 0.4mg/kg/hr for 18 hours.
CPR: 5 mg/kg rapid IV bolus {VF/Pulseless VT} =One 100ml bag (150mg) per 30 kg
*Alternative dosing: 2–5 mg/kg, IV infused over 30 to 60 minutes with careful BP and rhythm monitoring
Supplied as Premixed as a 1.5mg/mL ready-to-use, sterile, iso-osmotic solution in dextrose-IV solution (150 mg per 100ml bag)
**Other forms available: NEXTERONE Premixed Injection (360 mg/200 mL; 1.8 mg/mL)-PLEASE CONFIRM CONCENTRATION BEFORE USE
Reconstitution / Dilution Premixed as a 1.5mg/mL solution, no reconstitution or dilution required
Administration IV bolus, followed by a CRI or switch to PO medication
FILTER: USE A 0.2 um micron membrane filter
Compatibility No other medications should be added to the Nexterone bag or IV line. See Package Insert for Y site compatibility list (Y-site compatible with Magnesium Sulfate)
Amiodarone can increase the serum levels of digoxin, cyclosporine, lidocaine, and procainamide.
Amiodarone can have additive effects with azoles, cisapride, dolasetron, fluoroquinolones, and ondansetron which can lead to serious arrhythmias.
Contraindications Contraindicated in 2nd and 3rd degree AV block, bradyarrhythmia.
Adverse Effects Hypotension, bradycardia, AV block, hepatotoxicity
Storage Stable at room temperature. Shelf life of two years. Protect from light until use.
Notes • Only the brand name Nexterone should be used in canine patients. • The generic form of amiodarone preserved with polysorbate80 can cause severe
anaphylaxis • Typically, not the 1st line therapy • Elevated liver enzymes/hepatotoxicity (common), monitoring recommended • Can cause thyroid dysfunction, blood dyscrasia, and is proarrhythmic • Correct hypokalemia, hypomagnesemia, or hypocalcemia whenever possible
before initiating treatment with NEXTERONE, as these disorders can exaggerate the degree of QTc prolongation and increase the potential for torsade de pointes = TdP.
Please address any corrections, questions, or suggestions to: [email protected].
11 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Amphotericin B
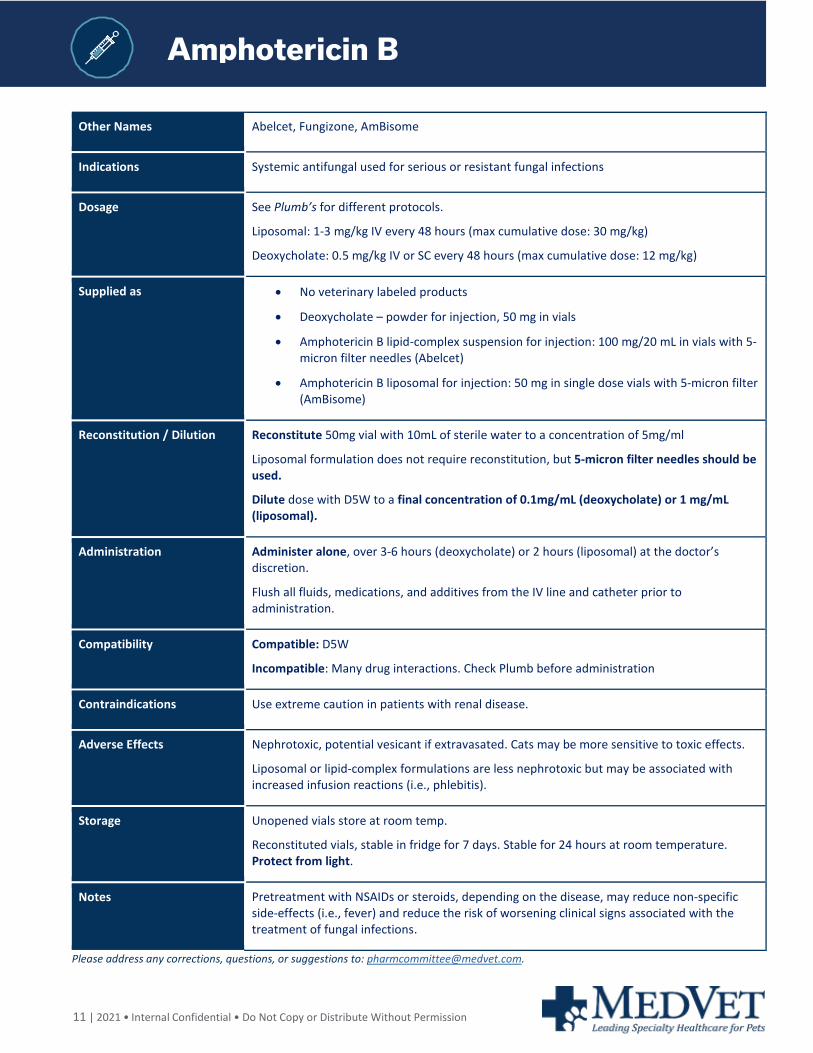
Other Names Abelcet, Fungizone, AmBisome
Indications Systemic antifungal used for serious or resistant fungal infections
Dosage See Plumb’s for different protocols.
Liposomal: 1-3 mg/kg IV every 48 hours (max cumulative dose: 30 mg/kg)
Deoxycholate: 0.5 mg/kg IV or SC every 48 hours (max cumulative dose: 12 mg/kg)
Supplied as • No veterinary labeled products
• Deoxycholate – powder for injection, 50 mg in vials
• Amphotericin B lipid-complex suspension for injection: 100 mg/20 mL in vials with 5-micron filter needles (Abelcet)
• Amphotericin B liposomal for injection: 50 mg in single dose vials with 5-micron filter (AmBisome)
Reconstitution / Dilution Reconstitute 50mg vial with 10mL of sterile water to a concentration of 5mg/ml
Liposomal formulation does not require reconstitution, but 5-micron filter needles should be used.
Dilute dose with D5W to a final concentration of 0.1mg/mL (deoxycholate) or 1 mg/mL (liposomal).
Administration Administer alone, over 3-6 hours (deoxycholate) or 2 hours (liposomal) at the doctor’s discretion.
Flush all fluids, medications, and additives from the IV line and catheter prior to administration.
Compatibility Compatible: D5W
Incompatible: Many drug interactions. Check Plumb before administration
Contraindications Use extreme caution in patients with renal disease.
Adverse Effects Nephrotoxic, potential vesicant if extravasated. Cats may be more sensitive to toxic effects.
Liposomal or lipid-complex formulations are less nephrotoxic but may be associated with increased infusion reactions (i.e., phlebitis).
Storage Unopened vials store at room temp.
Reconstituted vials, stable in fridge for 7 days. Stable for 24 hours at room temperature. Protect from light.
Notes Pretreatment with NSAIDs or steroids, depending on the disease, may reduce non-specific side-effects (i.e., fever) and reduce the risk of worsening clinical signs associated with the treatment of fungal infections.
Please address any corrections, questions, or suggestions to: [email protected].
12 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Ampicillin & Sulbactam
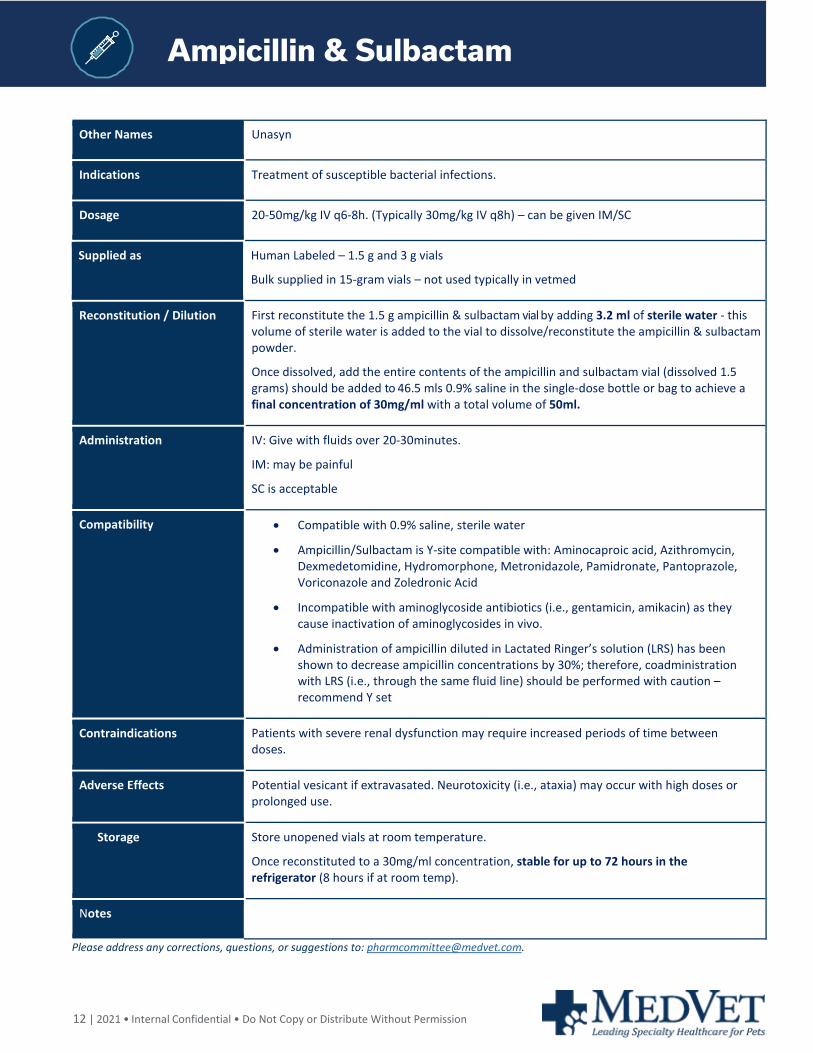
Other Names Unasyn
Indications Treatment of susceptible bacterial infections.
Dosage 20-50mg/kg IV q6-8h. (Typically 30mg/kg IV q8h) – can be given IM/SC
Supplied as Human Labeled – 1.5 g and 3 g vials
Bulk supplied in 15-gram vials – not used typically in vetmed
Reconstitution / Dilution First reconstitute the 1.5 g ampicillin & sulbactam vial by adding 3.2 ml of sterile water - this volume of sterile water is added to the vial to dissolve/reconstitute the ampicillin & sulbactam powder.
Once dissolved, add the entire contents of the ampicillin and sulbactam vial (dissolved 1.5 grams) should be added to 46.5 mls 0.9% saline in the single-dose bottle or bag to achieve a final concentration of 30mg/ml with a total volume of 50ml.
Administration IV: Give with fluids over 20-30minutes.
IM: may be painful
SC is acceptable
Compatibility • Compatible with 0.9% saline, sterile water
• Ampicillin/Sulbactam is Y-site compatible with: Aminocaproic acid, Azithromycin, Dexmedetomidine, Hydromorphone, Metronidazole, Pamidronate, Pantoprazole, Voriconazole and Zoledronic Acid
• Incompatible with aminoglycoside antibiotics (i.e., gentamicin, amikacin) as they cause inactivation of aminoglycosides in vivo.
• Administration of ampicillin diluted in Lactated Ringer’s solution (LRS) has been shown to decrease ampicillin concentrations by 30%; therefore, coadministration with LRS (i.e., through the same fluid line) should be performed with caution – recommend Y set
Contraindications Patients with severe renal dysfunction may require increased periods of time between doses.
Adverse Effects Potential vesicant if extravasated. Neurotoxicity (i.e., ataxia) may occur with high doses or prolonged use.
Storage Store unopened vials at room temperature.
Once reconstituted to a 30mg/ml concentration, stable for up to 72 hours in the refrigerator (8 hours if at room temp).
Notes
Please address any corrections, questions, or suggestions to: [email protected].
13 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Ampicillin
Other Names Ampicillin Sodium, Ampicillin Trihydrate, Polyflex
Indications Bactericidal antibiotic with same spectrum as amoxicillin (ineffective against bacteria that produce beta-lactamase)
Dosage 5-30mg/kg IV q8-12 hours Adjunctive antibiotic therapy for sepsis or susceptible systemic infections: (extra-label):
Ampicillin Sodium 20-50mg/kg every 6-8 hours.
Supplied as Ampicillin powder in multiple sizes: 250 mg, 500 mg, 1 gram, 2-gram vials
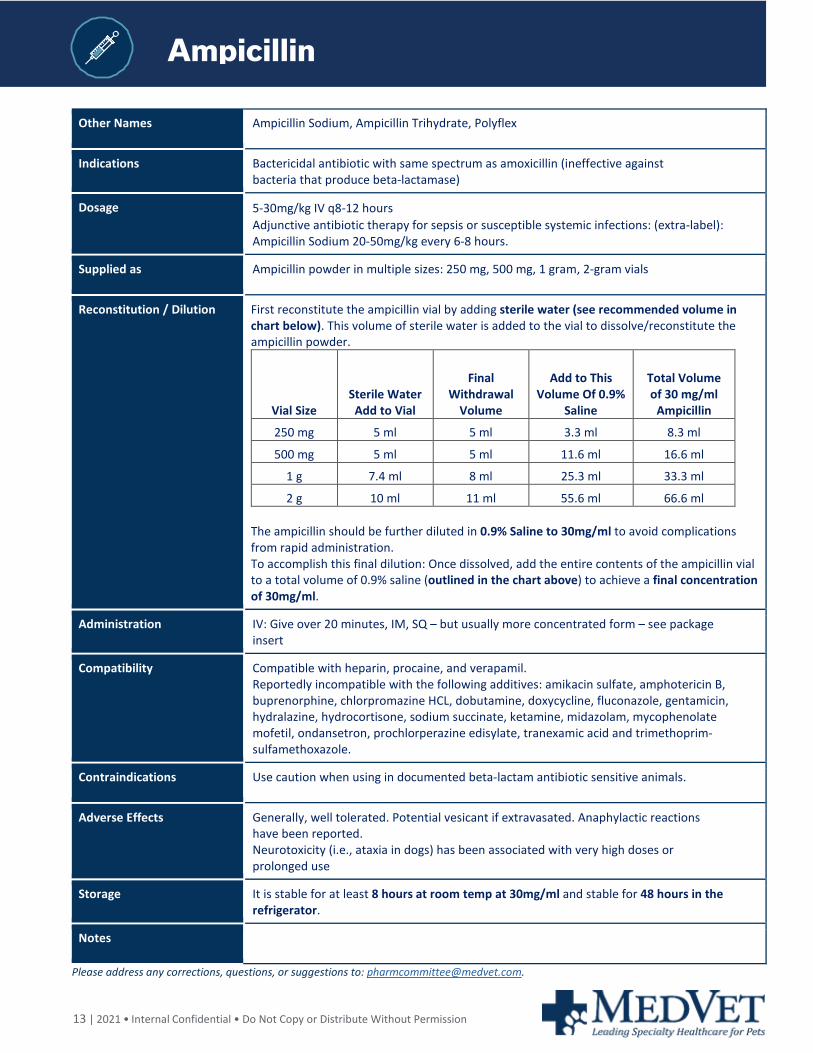
Reconstitution / Dilution First reconstitute the ampicillin vial by adding sterile water (see recommended volume in chart below). This volume of sterile water is added to the vial to dissolve/reconstitute the ampicillin powder.
Vial Size Sterile Water Add to Vial
Final Withdrawal
Volume
Add to This Volume Of 0.9%
Saline
Total Volume of 30 mg/ml
Ampicillin
250 mg 5 ml 5 ml 3.3 ml 8.3 ml
500 mg 5 ml 5 ml 11.6 ml 16.6 ml
1 g 7.4 ml 8 ml 25.3 ml 33.3 ml
2 g 10 ml 11 ml 55.6 ml 66.6 ml The ampicillin should be further diluted in 0.9% Saline to 30mg/ml to avoid complications from rapid administration. To accomplish this final dilution: Once dissolved, add the entire contents of the ampicillin vial to a total volume of 0.9% saline (outlined in the chart above) to achieve a final concentration of 30mg/ml.
Administration IV: Give over 20 minutes, IM, SQ – but usually more concentrated form – see package insert
Compatibility Compatible with heparin, procaine, and verapamil. Reportedly incompatible with the following additives: amikacin sulfate, amphotericin B, buprenorphine, chlorpromazine HCL, dobutamine, doxycycline, fluconazole, gentamicin, hydralazine, hydrocortisone, sodium succinate, ketamine, midazolam, mycophenolate mofetil, ondansetron, prochlorperazine edisylate, tranexamic acid and trimethoprim-sulfamethoxazole.
Contraindications Use caution when using in documented beta-lactam antibiotic sensitive animals.
Adverse Effects Generally, well tolerated. Potential vesicant if extravasated. Anaphylactic reactions have been reported. Neurotoxicity (i.e., ataxia in dogs) has been associated with very high doses or prolonged use
Storage It is stable for at least 8 hours at room temp at 30mg/ml and stable for 48 hours in the refrigerator.
Notes
Please address any corrections, questions, or suggestions to: [email protected].

14 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
10% Calcium Gluconate
Other Names Calcium salt (form of elemental calcium)
Indications Treatment of severe ionized hypocalcemia, acute hyperkalemia (most commonly in urinary obstructed “blocked” cats), calcium channel and beta-blocker overdose/toxicosis, eclampsia, hypoparathyroidism (PTH deficiency)-hypocalcemia with hyperphosphatemia.
Dosage Emergent: 0.5-1.5 mL/kg slow IV over 10-30min (10% Calcium gluconate) Administer while monitoring continuous ECG +/- BP monitoring 10% solution provides 50-150 mg/kg CaGluconate; equivalent 5-15 mg/kg elemental calcium For subacute therapy: CRI 10-30 mg/kg/hr CaGluconate=1-3mg/kg/hr Elemental Calcium (Diluted to 1%)
Supplied as 10% Calcium gluconate (100 mg/ml of calcium gluconate; 9.3 mg elemental calcium/ml) 1ml= 100mg of calcium gluconate; 1ml=9.3mg of elemental calcium (0.46 mEq/ml)
Dilution No dilution needed as a bolus in emergent settings For CRI, dilute 1:10 for a final concentration of 1% (10mg/mL)
Administration No dilution required for IV administration in emergent settings, however rapid administration can cause cardiac arrest Commonly diluted 1:3 or greater with 0.9% NaCl to ensure slow IV bolus (Example: 1ml of 10% calcium gluconate added to 3ml of 0.9% NaCl= 4ml total volume) For CRI, dilute 10% calcium gluconate (100mg/ml) to a final concentration of 1% =10mg/mL Example: Add 6 ml (600mg) to 54 ml of 0.9%NaCl= 60ml total volume, Conc: 10mg/ml Subcutaneous dosing generally not recommended
Compatibility Compatible with 0.9% saline, LRS, and D5W. *Given high risk of precipitation of calcium salts, ideally avoid giving with any other fluids/medications when possible. Compatible with erythromycin, heparin, lidocaine, norepinephrine, phenobarbital, KCl, verapamil, B vitamins. Incompatible with lipid emulsions, amphotericin, dobutamine, and metoclopramide.
Contraindications Contraindicated in patients with ventricular fibrillation and hypercalcemia. Caution in patients with cardiac and renal disease or those receiving digoxin.
Adverse Effects Rapid IV infusions can cause hypotension, cardiac arrhythmias, and cardiac arrest. SEVERE VESICANT POTENTIAL IF EXTRAVASATED. If extravasation occurs, stop infusion, leave catheter in place, and contact doctor. IV catheter can be sued to suction out any remaining extravasated calcium gluconate and possibly to dilute by infusing/ further infiltrating the affected area with 0.9% saline SQ injections cause severe skin necrosis and life-threatening abscesses
Storage Store at room temperature. Avoid freezing.
Notes Dosing parenteral calcium can be confusing and potentially dangerous. Depending on the reference, dosages can be listed by mL/kg, mEq/kg, mmol/kg, or mg/kg. These may be for the calcium salt being used OR for elemental calcium. Calcium chloride 10% injection contains approximately 3X more elemental calcium per mL as calcium gluconate 10%. Not interchangeable with calcium borogluconate 23% for veterinary use. Note higher concentration (230mg/ml; 20.7mg (1.06 meq) - do not administer on a per ml basis as outlined above
Please address any corrections, questions, or suggestions to: [email protected].
15 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Cefazolin
Other Names Cefazolin Sodium, Ancef, Kefzol, Zolicef
Indications 1st generation parenteral Cephalosporin used for surgical prophylaxis and for a variety of systemic infections
Dosage 8-30 mg/kg
Supplied as Cefazolin Sodium Powder for injection: 500 mg, 1 g, 2g, 10g, 20g, in vials
Cefazolin Sodium for injection: 1 g in 4% dextrose and 2 g in 3% dextrose, 50 mL plastic containers
Reconstitution / Dilution Add 10 ml of sterile water to 1 gram vial for a final concentration of 100mg/ml
Administration IV, IM, SQ q 6-8h
Give over 3-5 minutes IV.
If IM, give in large muscle mass.
Compatibility Compatible with: D5W, 0.45% and 0.9% saline, LRS
Compatible when given together at Y-site: Amiodarone, Atracurium, Calcium Gluconate, Famotidine, Cyclophosphamide, Dexmedetomidine, Diltiazem, Doxorubicin, Heparin, Hetastarch, Insulin, Lidocaine, Magnesium Sulfate, Midazolam, Metronidazole, Morphine, Propofol, Ranitidine, Vecuronium, Verapamil, and Vitamin-B Complex.
Incompatible with: Amikacin Sulfate, Calcium Chloride/Gluconate, Cimetidine, Erythromycin, Lidocaine, Pentobarbital Sodium, Polymyxin B Sulfate, Tetracycline, and Vitamin-B Complex.
Contraindications Use caution with other nephrotoxic drugs (NSAIDs, aminoglycosides, amphotericin). Reduce dose in patients with severe renal disease
Adverse Effects Patients with diminished renal function may require more intense renal monitoring.
Storage Stable for 24 hours a room temperature after reconstitution; 10 days if refrigerated (5◦
Celsius/41◦ F). Protect from light.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
16 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Cefotaxime Sodium
Other Names Claforan
Indications 3rd generation Cephalosporin useful treatment against gram positive and gram-negative bacteria
Dosage 25-50 mg/kg IV, IM, or SQ
Supplied as Cefotaxime Sodium powder for injection: 500 mg, 1 g, 2g, 10 g in vials
Reconstitution / Dilution Add 10mLs sterile water to 1g vial for a final concentration of 100mg/mL
Administration IV: Give over 15-20 minutes IM or SQ
Compatibility All commonly used IV fluids and the following drugs are compatible: clindamycin, metronidazole, and verapamil.
Use caution with other nephrotoxic drugs (aminoglycosides, NSAIDs, amphotericin)
Contraindications Use caution when using in patients who are documented hypersensitive to other beta-lactam antibiotics,
Patients in renal failure may need dose reduction.
Adverse Effects Soreness at injection site, overdose may cause seizure
Storage Protect from light. Once reconstituted, must be refrigerated, and discarded within 14 hours.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
17 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Ceftazidim
Other Names Ceptaz, Fortaz, Tazicef
Indications 3rd generation Cephalosporin used in the treatment of susceptible gram-negative bacterial infections
Dosage 25-50mg/kg IV q8-12 hours
Supplied as Ceftazidime powder for injection: 500 mg, 1, 2, g, 6 g in 20 mL and 100 ML vials
Reconstitution / Dilution Typically supplied as a 1g powder.
Reconstitute with 10mLs of sterile water for a final concentration of 100 mg/ml
Administration IV: Give over 20 minutes
IM, SQ: Painful on injection, can add lidocaine to dilution
Compatibility Compatible with 0.9% saline, 5% Dextrose (D5W), 5% Dextrose and 0.45% Sodium Chloride, and LRS.
Contraindications Prior allergic reaction to cephalosporins
Adverse Effects Vomiting and diarrhea have been reported in dogs given Ceftazidime SQ. Pain at injection site if given IM or SQ.
Storage Stable for 24 hours at room temperature. Stable for 7 days if refrigerated.
Notes Use caution with other nephrotoxic drugs (aminoglycosides, amphotericin B, NSAIDS)
Please address any corrections, questions, or suggestions to: [email protected].
18 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Ceftriaxon
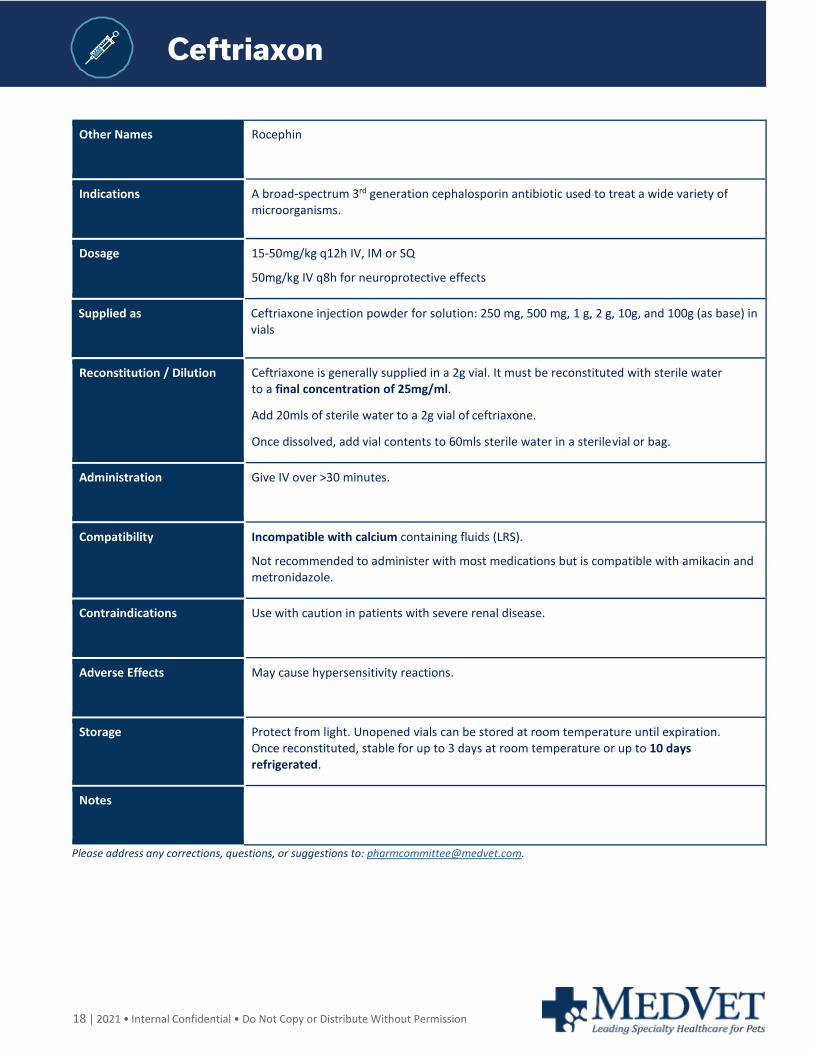
Other Names Rocephin
Indications A broad-spectrum 3rd generation cephalosporin antibiotic used to treat a wide variety of microorganisms.
Dosage 15-50mg/kg q12h IV, IM or SQ
50mg/kg IV q8h for neuroprotective effects
Supplied as Ceftriaxone injection powder for solution: 250 mg, 500 mg, 1 g, 2 g, 10g, and 100g (as base) in vials
Reconstitution / Dilution Ceftriaxone is generally supplied in a 2g vial. It must be reconstituted with sterile water to a final concentration of 25mg/ml.
Add 20mls of sterile water to a 2g vial of ceftriaxone.
Once dissolved, add vial contents to 60mls sterile water in a sterile vial or bag.
Administration Give IV over >30 minutes.
Compatibility Incompatible with calcium containing fluids (LRS).
Not recommended to administer with most medications but is compatible with amikacin and metronidazole.
Contraindications Use with caution in patients with severe renal disease.
Adverse Effects May cause hypersensitivity reactions.
Storage Protect from light. Unopened vials can be stored at room temperature until expiration. Once reconstituted, stable for up to 3 days at room temperature or up to 10 days refrigerated.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
19 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Clindamycin
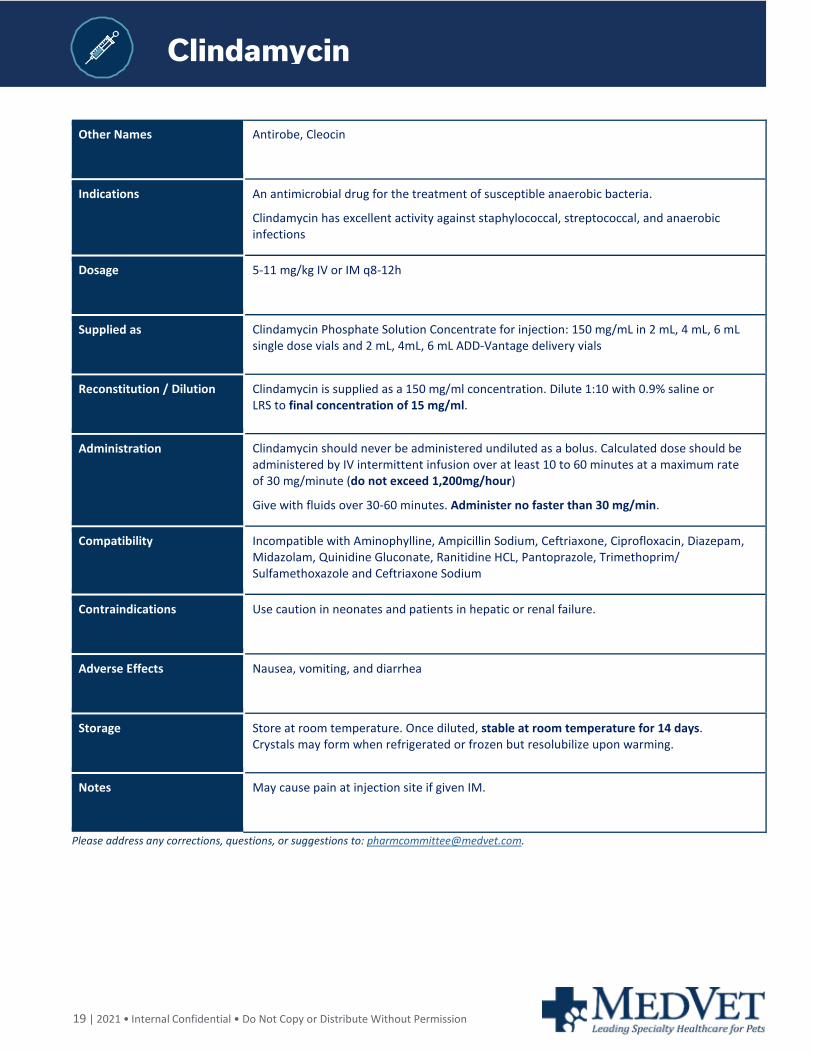
Other Names Antirobe, Cleocin
Indications An antimicrobial drug for the treatment of susceptible anaerobic bacteria.
Clindamycin has excellent activity against staphylococcal, streptococcal, and anaerobic infections
Dosage 5-11 mg/kg IV or IM q8-12h
Supplied as Clindamycin Phosphate Solution Concentrate for injection: 150 mg/mL in 2 mL, 4 mL, 6 mL single dose vials and 2 mL, 4mL, 6 mL ADD-Vantage delivery vials
Reconstitution / Dilution Clindamycin is supplied as a 150 mg/ml concentration. Dilute 1:10 with 0.9% saline or LRS to final concentration of 15 mg/ml.
Administration Clindamycin should never be administered undiluted as a bolus. Calculated dose should be administered by IV intermittent infusion over at least 10 to 60 minutes at a maximum rate of 30 mg/minute (do not exceed 1,200mg/hour)
Give with fluids over 30-60 minutes. Administer no faster than 30 mg/min.
Compatibility Incompatible with Aminophylline, Ampicillin Sodium, Ceftriaxone, Ciprofloxacin, Diazepam, Midazolam, Quinidine Gluconate, Ranitidine HCL, Pantoprazole, Trimethoprim/ Sulfamethoxazole and Ceftriaxone Sodium
Contraindications Use caution in neonates and patients in hepatic or renal failure.
Adverse Effects Nausea, vomiting, and diarrhea
Storage Store at room temperature. Once diluted, stable at room temperature for 14 days. Crystals may form when refrigerated or frozen but resolubilize upon warming.
Notes May cause pain at injection site if given IM.
Please address any corrections, questions, or suggestions to: [email protected].
20 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Dexmedetomidin
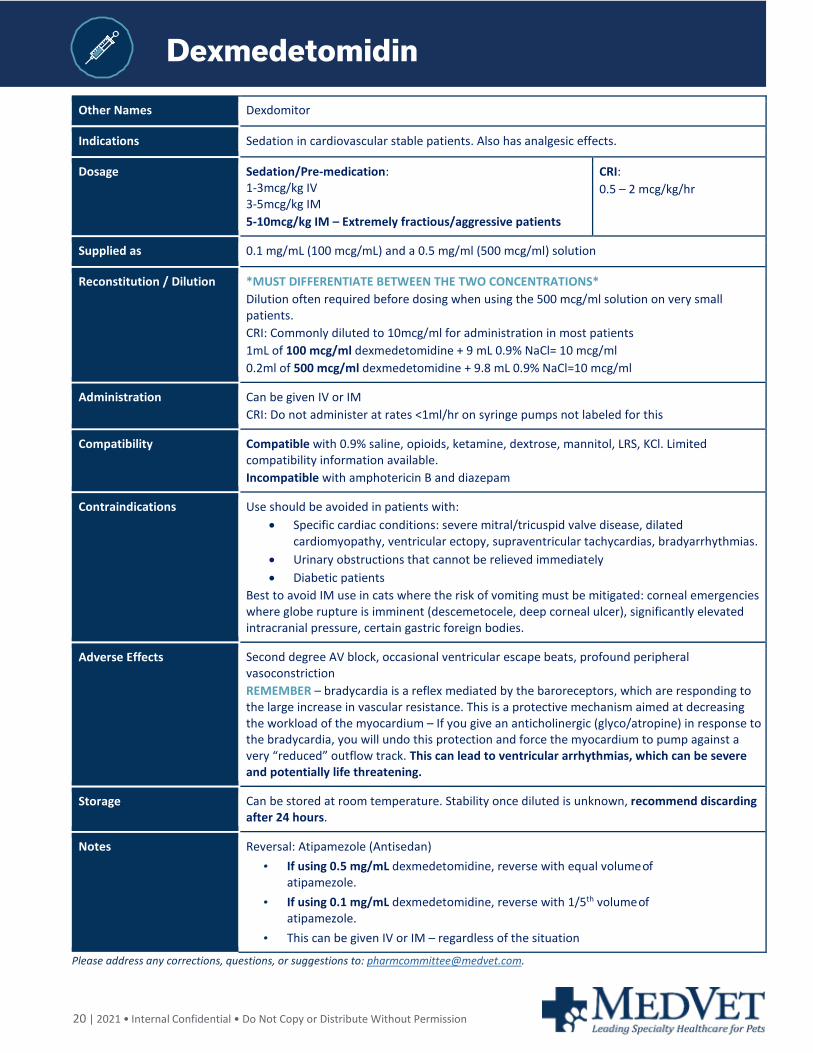
Other Names Dexdomitor
Indications Sedation in cardiovascular stable patients. Also has analgesic effects.
Dosage Sedation/Pre-medication: 1-3mcg/kg IV 3-5mcg/kg IM 5-10mcg/kg IM – Extremely fractious/aggressive patients
CRI: 0.5 – 2 mcg/kg/hr
Supplied as 0.1 mg/mL (100 mcg/mL) and a 0.5 mg/ml (500 mcg/ml) solution
Reconstitution / Dilution *MUST DIFFERENTIATE BETWEEN THE TWO CONCENTRATIONS* Dilution often required before dosing when using the 500 mcg/ml solution on very small patients. CRI: Commonly diluted to 10mcg/ml for administration in most patients 1mL of 100 mcg/ml dexmedetomidine + 9 mL 0.9% NaCl= 10 mcg/ml 0.2ml of 500 mcg/ml dexmedetomidine + 9.8 mL 0.9% NaCl=10 mcg/ml
Administration Can be given IV or IM CRI: Do not administer at rates <1ml/hr on syringe pumps not labeled for this
Compatibility Compatible with 0.9% saline, opioids, ketamine, dextrose, mannitol, LRS, KCl. Limited compatibility information available. Incompatible with amphotericin B and diazepam
Contraindications Use should be avoided in patients with: • Specific cardiac conditions: severe mitral/tricuspid valve disease, dilated
cardiomyopathy, ventricular ectopy, supraventricular tachycardias, bradyarrhythmias. • Urinary obstructions that cannot be relieved immediately • Diabetic patients
Best to avoid IM use in cats where the risk of vomiting must be mitigated: corneal emergencies where globe rupture is imminent (descemetocele, deep corneal ulcer), significantly elevated intracranial pressure, certain gastric foreign bodies.
Adverse Effects Second degree AV block, occasional ventricular escape beats, profound peripheral vasoconstriction REMEMBER – bradycardia is a reflex mediated by the baroreceptors, which are responding to the large increase in vascular resistance. This is a protective mechanism aimed at decreasing the workload of the myocardium – If you give an anticholinergic (glyco/atropine) in response to the bradycardia, you will undo this protection and force the myocardium to pump against a very “reduced” outflow track. This can lead to ventricular arrhythmias, which can be severe and potentially life threatening.
Storage Can be stored at room temperature. Stability once diluted is unknown, recommend discarding after 24 hours.
Notes Reversal: Atipamezole (Antisedan) • If using 0.5 mg/mL dexmedetomidine, reverse with equal volume of
atipamezole. • If using 0.1 mg/mL dexmedetomidine, reverse with 1/5th volume of
atipamezole. • This can be given IV or IM – regardless of the situation
Please address any corrections, questions, or suggestions to: [email protected].
21 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Diazepam
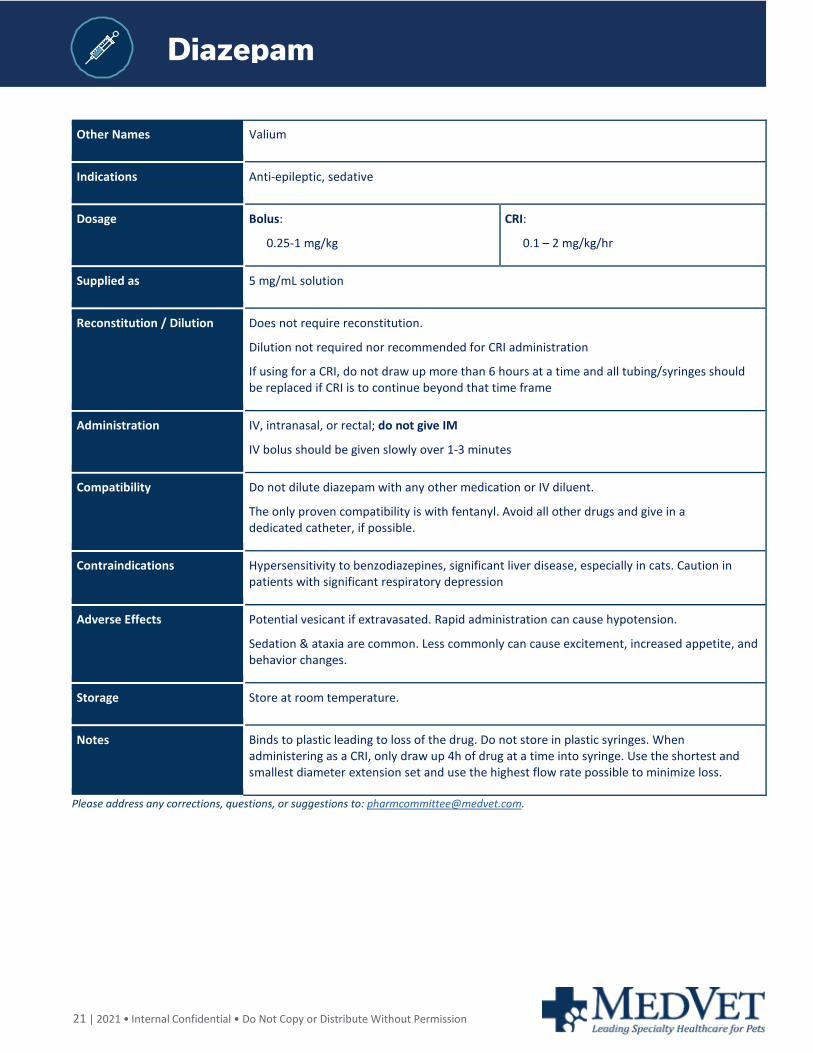
Other Names Valium
Indications Anti-epileptic, sedative
Dosage Bolus:
0.25-1 mg/kg
CRI:
0.1 – 2 mg/kg/hr
Supplied as 5 mg/mL solution
Reconstitution / Dilution Does not require reconstitution.
Dilution not required nor recommended for CRI administration
If using for a CRI, do not draw up more than 6 hours at a time and all tubing/syringes should be replaced if CRI is to continue beyond that time frame
Administration IV, intranasal, or rectal; do not give IM
IV bolus should be given slowly over 1-3 minutes
Compatibility Do not dilute diazepam with any other medication or IV diluent.
The only proven compatibility is with fentanyl. Avoid all other drugs and give in a dedicated catheter, if possible.
Contraindications Hypersensitivity to benzodiazepines, significant liver disease, especially in cats. Caution in patients with significant respiratory depression
Adverse Effects Potential vesicant if extravasated. Rapid administration can cause hypotension.
Sedation & ataxia are common. Less commonly can cause excitement, increased appetite, and behavior changes.
Storage Store at room temperature.
Notes Binds to plastic leading to loss of the drug. Do not store in plastic syringes. When administering as a CRI, only draw up 4h of drug at a time into syringe. Use the shortest and smallest diameter extension set and use the highest flow rate possible to minimize loss.
Please address any corrections, questions, or suggestions to: [email protected].
22 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Diltiazem
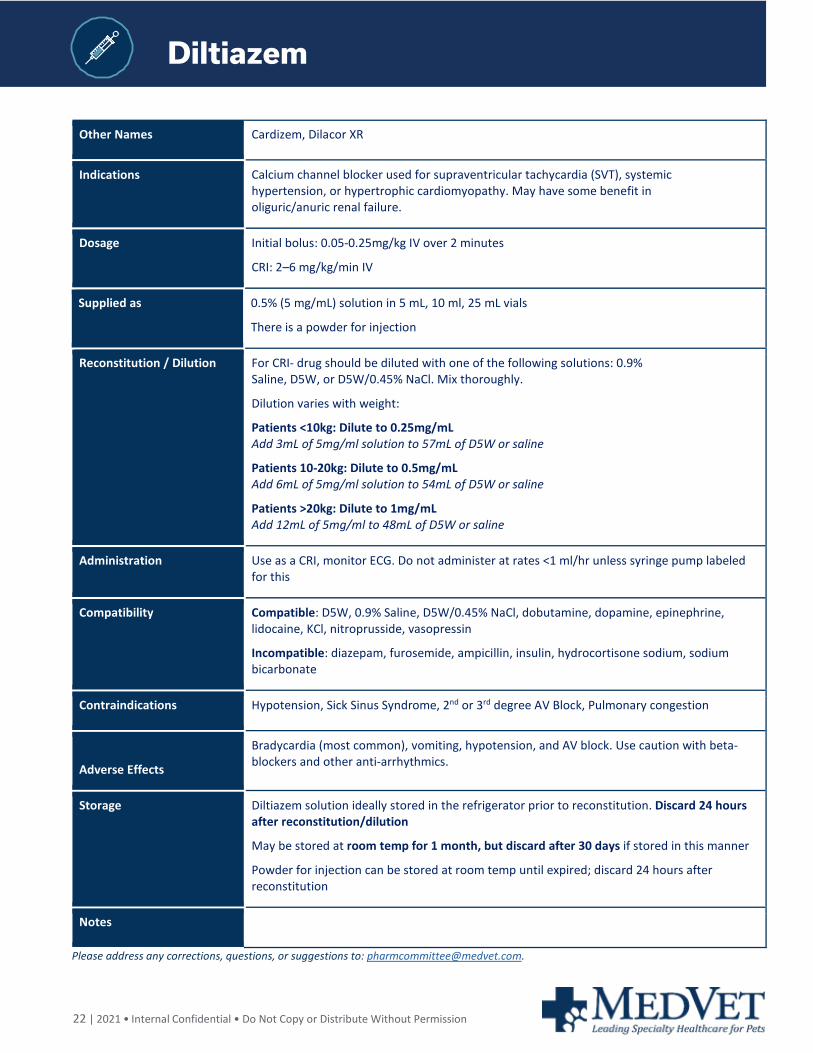
Other Names Cardizem, Dilacor XR
Indications Calcium channel blocker used for supraventricular tachycardia (SVT), systemic hypertension, or hypertrophic cardiomyopathy. May have some benefit in oliguric/anuric renal failure.
Dosage Initial bolus: 0.05-0.25mg/kg IV over 2 minutes
CRI: 2–6 mg/kg/min IV
Supplied as 0.5% (5 mg/mL) solution in 5 mL, 10 ml, 25 mL vials
There is a powder for injection
Reconstitution / Dilution For CRI- drug should be diluted with one of the following solutions: 0.9% Saline, D5W, or D5W/0.45% NaCl. Mix thoroughly.
Dilution varies with weight:
Patients <10kg: Dilute to 0.25mg/mL Add 3mL of 5mg/ml solution to 57mL of D5W or saline
Patients 10-20kg: Dilute to 0.5mg/mL Add 6mL of 5mg/ml solution to 54mL of D5W or saline
Patients >20kg: Dilute to 1mg/mL Add 12mL of 5mg/ml to 48mL of D5W or saline
Administration Use as a CRI, monitor ECG. Do not administer at rates <1 ml/hr unless syringe pump labeled for this
Compatibility Compatible: D5W, 0.9% Saline, D5W/0.45% NaCl, dobutamine, dopamine, epinephrine, lidocaine, KCl, nitroprusside, vasopressin
Incompatible: diazepam, furosemide, ampicillin, insulin, hydrocortisone sodium, sodium bicarbonate
Contraindications Hypotension, Sick Sinus Syndrome, 2nd or 3rd degree AV Block, Pulmonary congestion
Adverse Effects
Bradycardia (most common), vomiting, hypotension, and AV block. Use caution with beta-blockers and other anti-arrhythmics.
Storage Diltiazem solution ideally stored in the refrigerator prior to reconstitution. Discard 24 hours after reconstitution/dilution
May be stored at room temp for 1 month, but discard after 30 days if stored in this manner
Powder for injection can be stored at room temp until expired; discard 24 hours after reconstitution
Notes
Please address any corrections, questions, or suggestions to: [email protected].
23 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Dobutamine
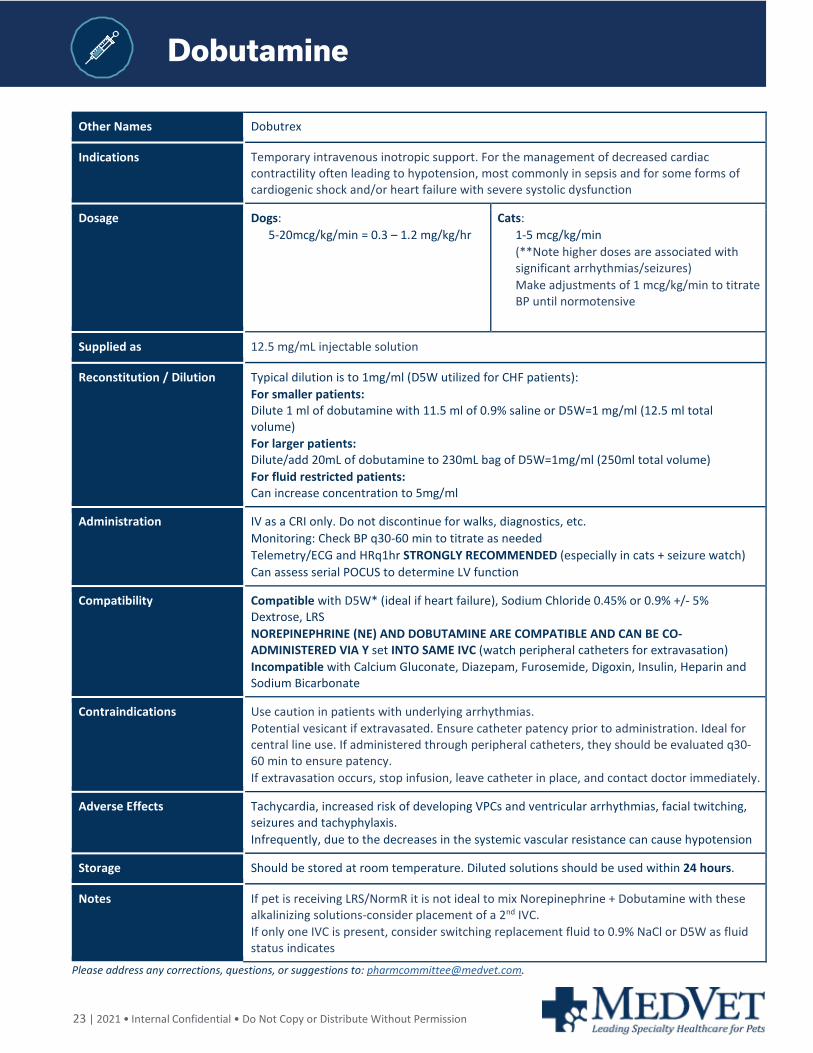
Other Names Dobutrex
Indications Temporary intravenous inotropic support. For the management of decreased cardiac contractility often leading to hypotension, most commonly in sepsis and for some forms of cardiogenic shock and/or heart failure with severe systolic dysfunction
Dosage Dogs: 5-20mcg/kg/min = 0.3 – 1.2 mg/kg/hr
Cats: 1-5 mcg/kg/min (**Note higher doses are associated with significant arrhythmias/seizures) Make adjustments of 1 mcg/kg/min to titrate BP until normotensive
Supplied as 12.5 mg/mL injectable solution
Reconstitution / Dilution Typical dilution is to 1mg/ml (D5W utilized for CHF patients): For smaller patients: Dilute 1 ml of dobutamine with 11.5 ml of 0.9% saline or D5W=1 mg/ml (12.5 ml total volume) For larger patients: Dilute/add 20mL of dobutamine to 230mL bag of D5W=1mg/ml (250ml total volume) For fluid restricted patients: Can increase concentration to 5mg/ml
Administration IV as a CRI only. Do not discontinue for walks, diagnostics, etc. Monitoring: Check BP q30-60 min to titrate as needed Telemetry/ECG and HRq1hr STRONGLY RECOMMENDED (especially in cats + seizure watch) Can assess serial POCUS to determine LV function
Compatibility Compatible with D5W* (ideal if heart failure), Sodium Chloride 0.45% or 0.9% +/- 5% Dextrose, LRS NOREPINEPHRINE (NE) AND DOBUTAMINE ARE COMPATIBLE AND CAN BE CO-ADMINISTERED VIA Y set INTO SAME IVC (watch peripheral catheters for extravasation) Incompatible with Calcium Gluconate, Diazepam, Furosemide, Digoxin, Insulin, Heparin and Sodium Bicarbonate
Contraindications Use caution in patients with underlying arrhythmias. Potential vesicant if extravasated. Ensure catheter patency prior to administration. Ideal for central line use. If administered through peripheral catheters, they should be evaluated q30-60 min to ensure patency. If extravasation occurs, stop infusion, leave catheter in place, and contact doctor immediately.
Adverse Effects Tachycardia, increased risk of developing VPCs and ventricular arrhythmias, facial twitching, seizures and tachyphylaxis. Infrequently, due to the decreases in the systemic vascular resistance can cause hypotension
Storage Should be stored at room temperature. Diluted solutions should be used within 24 hours.
Notes If pet is receiving LRS/NormR it is not ideal to mix Norepinephrine + Dobutamine with these alkalinizing solutions-consider placement of a 2nd IVC. If only one IVC is present, consider switching replacement fluid to 0.9% NaCl or D5W as fluid status indicates
Please address any corrections, questions, or suggestions to: [email protected].
24 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Dopamine
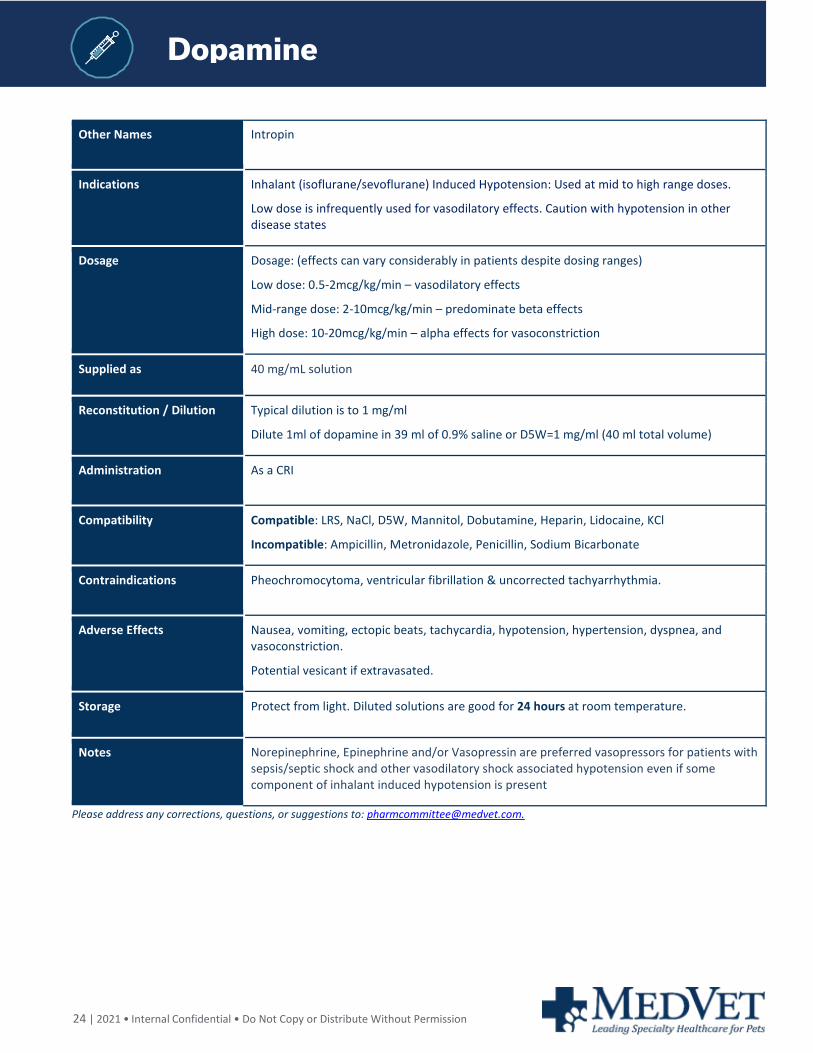
Other Names Intropin
Indications Inhalant (isoflurane/sevoflurane) Induced Hypotension: Used at mid to high range doses.
Low dose is infrequently used for vasodilatory effects. Caution with hypotension in other disease states
Dosage Dosage: (effects can vary considerably in patients despite dosing ranges)
Low dose: 0.5-2mcg/kg/min – vasodilatory effects
Mid-range dose: 2-10mcg/kg/min – predominate beta effects
High dose: 10-20mcg/kg/min – alpha effects for vasoconstriction
Supplied as 40 mg/mL solution
Reconstitution / Dilution Typical dilution is to 1 mg/ml
Dilute 1ml of dopamine in 39 ml of 0.9% saline or D5W=1 mg/ml (40 ml total volume)
Administration As a CRI
Compatibility Compatible: LRS, NaCl, D5W, Mannitol, Dobutamine, Heparin, Lidocaine, KCl
Incompatible: Ampicillin, Metronidazole, Penicillin, Sodium Bicarbonate
Contraindications Pheochromocytoma, ventricular fibrillation & uncorrected tachyarrhythmia.
Adverse Effects Nausea, vomiting, ectopic beats, tachycardia, hypotension, hypertension, dyspnea, and vasoconstriction.
Potential vesicant if extravasated.
Storage Protect from light. Diluted solutions are good for 24 hours at room temperature.
Notes Norepinephrine, Epinephrine and/or Vasopressin are preferred vasopressors for patients with sepsis/septic shock and other vasodilatory shock associated hypotension even if some component of inhalant induced hypotension is present
Please address any corrections, questions, or suggestions to: [email protected].
25 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Doxycyclin
Doxycyclin
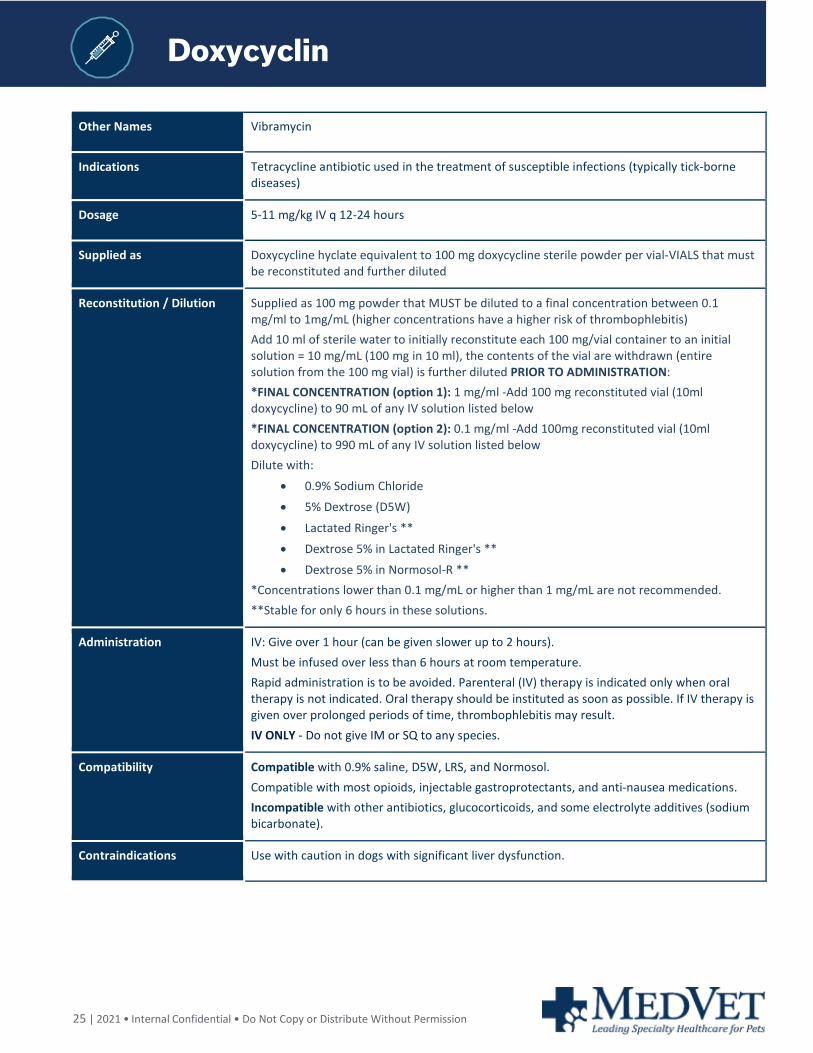
Other Names Vibramycin
Indications Tetracycline antibiotic used in the treatment of susceptible infections (typically tick-borne diseases)
Dosage 5-11 mg/kg IV q 12-24 hours
Supplied as Doxycycline hyclate equivalent to 100 mg doxycycline sterile powder per vial-VIALS that must be reconstituted and further diluted
Reconstitution / Dilution Supplied as 100 mg powder that MUST be diluted to a final concentration between 0.1 mg/ml to 1mg/mL (higher concentrations have a higher risk of thrombophlebitis) Add 10 ml of sterile water to initially reconstitute each 100 mg/vial container to an initial solution = 10 mg/mL (100 mg in 10 ml), the contents of the vial are withdrawn (entire solution from the 100 mg vial) is further diluted PRIOR TO ADMINISTRATION: *FINAL CONCENTRATION (option 1): 1 mg/ml -Add 100 mg reconstituted vial (10ml doxycycline) to 90 mL of any IV solution listed below *FINAL CONCENTRATION (option 2): 0.1 mg/ml -Add 100mg reconstituted vial (10ml doxycycline) to 990 mL of any IV solution listed below Dilute with:
• 0.9% Sodium Chloride • 5% Dextrose (D5W)
• Lactated Ringer's ** • Dextrose 5% in Lactated Ringer's ** • Dextrose 5% in Normosol-R **
*Concentrations lower than 0.1 mg/mL or higher than 1 mg/mL are not recommended. **Stable for only 6 hours in these solutions.
Administration IV: Give over 1 hour (can be given slower up to 2 hours). Must be infused over less than 6 hours at room temperature. Rapid administration is to be avoided. Parenteral (IV) therapy is indicated only when oral therapy is not indicated. Oral therapy should be instituted as soon as possible. If IV therapy is given over prolonged periods of time, thrombophlebitis may result. IV ONLY - Do not give IM or SQ to any species.
Compatibility Compatible with 0.9% saline, D5W, LRS, and Normosol. Compatible with most opioids, injectable gastroprotectants, and anti-nausea medications. Incompatible with other antibiotics, glucocorticoids, and some electrolyte additives (sodium bicarbonate).
Contraindications Use with caution in dogs with significant liver dysfunction.
26 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Doxycyclin
Adverse Effects Severe thrombophlebitis risk (DO NOT GIVE CONCENTRATED SOLUTIONS). Severe vesicant potential if extravasated. Ensure catheter patency prior to administration. Check IVC frequently during administration. If extravasation occurs, stop infusion, leave catheter in place, and contact doctor. Nausea, vomiting, and diarrhea are most common. Acute hepatopathies can occur. Transient weakness, collapse, and cardiac arrhythmias may be observed secondary to rapid IV infusion.
Storage Doxycycline is stable for 48 hours in solution when diluted with 0.9% Sodium Chloride, or 5% Dextrose, to concentrations between 1 mg/mL and 0.1 mg/mL and stored at 25° C (room temperature). Doxycycline in these solutions is stable under fluorescent light for 48 hours but must be protected from direct sunlight during storage and infusion. Reconstituted solutions (1 to 0.1 mg/mL) may be stored up to 72 hours prior to start of infusion if refrigerated and protected from sunlight and artificial light. Infusion must then be completed within 12 hours. Solutions must be used within these time periods or discarded. If diluted with LRS or LRS+5% dextrose: these solutions must be used within 6 hours after reconstitution/dilution to ensure adequate stability and should not be stored. Solutions of doxycycline for injection, at a concentration of 10 mg/mL in Sterile Water for Injection, when frozen immediately after reconstitution are stable for eight weeks when stored at –20° C. If the product is warmed, care should be taken to avoid heating it after the thawing is complete. Once thawed the solution should not be refrozen.
Notes Closely monitor IVC before, during, and after IV doxycycline. Switch to oral as quickly as possible. For dogs with the MDR1 gene mutation (i.e., Collies): doxycycline is pumped from cells by p-glycoprotein, but no dose alterations are required
Please address any corrections, questions, or suggestions to: [email protected].
27 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Enrofloxacin
Other Names Baytril, Enroflox
Indications Fluoroquinolone antibiotic used for treatment of a variety of susceptible bacterial infections (not effective against anaerobes).
Dosage 5-20 mg/kg IV, IM, SC, or PO q24h
Max dose in cats is 5 mg/kg/day PO or IM. IV administration in cats is not recommended.
Supplied as Small animal 22.7 mg/mL; 100 mg/mL large animal version not recommended
Reconstitution / Dilution Supplied in a 22.7mg/ml concentration. Dilute 1:10 with 0.9% saline.
Use of large animal 100 mg/ml formulation is discouraged in small animals.
Administration IV: Give alone over 30-60 minutes.
Compatibility Compatible with 0.9% saline
Incompatible with any fluid containing Mg++ and Ca++ including Plasmalyte, Norm-R, and LRS. Enro will precipitate with these electrolytes causing microprecipitates to develop in the lungs.
Incompatible with many drugs – see Plumb
May increase the nephrotoxicity of cyclosporine.
Contraindications Relatively contraindicated in dogs ages 2-8 months as it causes cartilage damage although this is typically with higher doses for >7-10 days – assess risk vs benefit in younger patient.
Doses > 5 mg/kg/day can cause permanent blindness in cats.
Caution in patients with seizure disorders, severe renal or hepatic dysfunction.
Adverse Effects GI: Vomiting, anorexia, diarrhea
Neuro: ataxia, seizures, lethargy, vocalization, and aggression.
Rapid infusions can cause hypotension, arrhythmias, vomiting, and mast cell degranulation.
Storage
Store at room temperature. Protect from light. Do not freeze.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
28 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Epinephrine
Other Names Adrenalin
Indications CPR, anaphylaxis (early), vasodilatory/septic shock, increase inotropy/cardiac contractility
Dosage CPR: Low dose: 0.01 mg/kg IV High Dose: 0.1mg/kg IV (no longer recommended, can consider with prolonged CPR > 15min) Vasodilatory shock (anaphylaxis): 0.01 mg/kg IM or IV (can repeat IM if IV access unavailable) 0.05 mcg/kg/min- 0.2 mcg/kg/min for Beta1 effects 0.2 mcg/kg/min - 1 mcg/kg/min for both alpha and beta effects
Supplied as 1 mg/ml (1:1000) solution (does come as other dilutions so double check bottle)
Reconstitution / Dilution Further dilution not required for CPR and IV bolus administration. For CRI: PERIPHERAL IV CATHETER-MAX CONCENTRATION - 40 micrograms/ml (0.04 mg/ml) QUICK CRI: 2 mg of Epinephrine (at 1mg/ml=2ml) in 48ml of 0.9% NaCl or D5W=50 ml total volume CENTRAL/PICC CATHETER-MAX CONCENTRATION - 80 micrograms/ml (0.08 mg/ml) QUICK CRI: 4 mg Epinephrine (at 1mg/ml=4ml) in 46ml of 0.9% NaCl or D5W=50ml total volume FULL RANGE: 0.05 to 0.5 mcg/kg/min (MAX 1 mcg/kg/min for post-arrest and severe anaphylaxis only)
Administration IV or IM (can be given SC but uncommon route due to patient perfusion/timing issues) Can be administered safely through a peripheral IV catheter for long term CRI use with minimal extravasation risk
Compatibility Compatible: D5W, 0.45% or 0.9% saline Y site compatible: norepinephrine, dobutamine, vasopressin Ideally should NOT be administered/diluted with LRS/NormR/PlasmalyteA as mixing epinephrine with these alkalinizing* solutions alter pH and may affect drug stability If only one IVC is present, consider switching replacement fluid to 0.9% NaCl for long term use Incompatible: hypertonic saline, aminophylline, and sodium bicarbonate*
Contraindications Use extreme caution in patients with cardiac arrhythmias
Adverse Effects Excitability, vomiting, hypertension, arrhythmias Ideally use central line; Can lead to local tissue necrosis in peripheral vein if extravasation occurs
Storage Protect from light
Notes Do not use the injection if it is pink, brown, or contains a precipitate
Please address any corrections, questions, or suggestions to: [email protected].
29 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Erythromycin
Other Names Gallimycin
Indications Macrolide antibiotic also used as a prokinetic agent.
Dosage Prokinetic: 0.5 – 1mg/kg PO or IV q8
Antibiotic: 10-20mg/kg PO q8
Supplied as Erythromycin lactobionate lyophilized powder for injection solution: 500 mg vial
Reconstitution / Dilution For IV use (only): Reconstitute 500 mg vial with 1 0mls of sterile water for a concentration of 50 mg/mL. Dilute 1 mL of the 50 mg/mL solution into 50mL of 0.9% saline for a final concentration of 1 mg/mL
Administration IV, IM, PO Prokinetic effect is achieved after oral administration. Give with fluids over 30 minutes.
Compatibility Compatible with 0.9% saline, LRS, and Norm-R. Most products use sterile water for reconstitution – see package insert for details. Incompatible with many other drugs, do not co-administer with other drugs without referencing a compatibility chart.
Contraindications • Patients with hepatic dysfunction.
• Patients with previously diagnosed or increased risk of cardiac arrhythmias.
• Erythromycin can affect the metabolism of many drugs via P450 inhibition. Consult a compatibility chart and consider therapeutic drug monitoring if indicated.
• Oral bioavailability is low for treating systemic infection and associated with GI side-effects due to prokinetic effects.
See Plumb’s for further details about the possible interactions
Adverse Effects When used as a prokinetic agent, it can occasionally increase clinical signs of intestinal distress as it will cause emptying of larger food particles into the intestine than is normal – generally not a problem for patient receiving liquefied diets. Can cause sloughing if extravasated. Prolonged QT interval may increase the risk of cardiac arrhythmias.
Storage Once reconstituted, stable for 24 hours at room temperature, and 2 weeks in the refrigerator. Protect from light.
Notes Erythromycin lactobionate is for IV use only Erythromycin ethyl succinate is for IM use only
Please address any corrections, questions, or suggestions to: [email protected].
30 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Esmolol
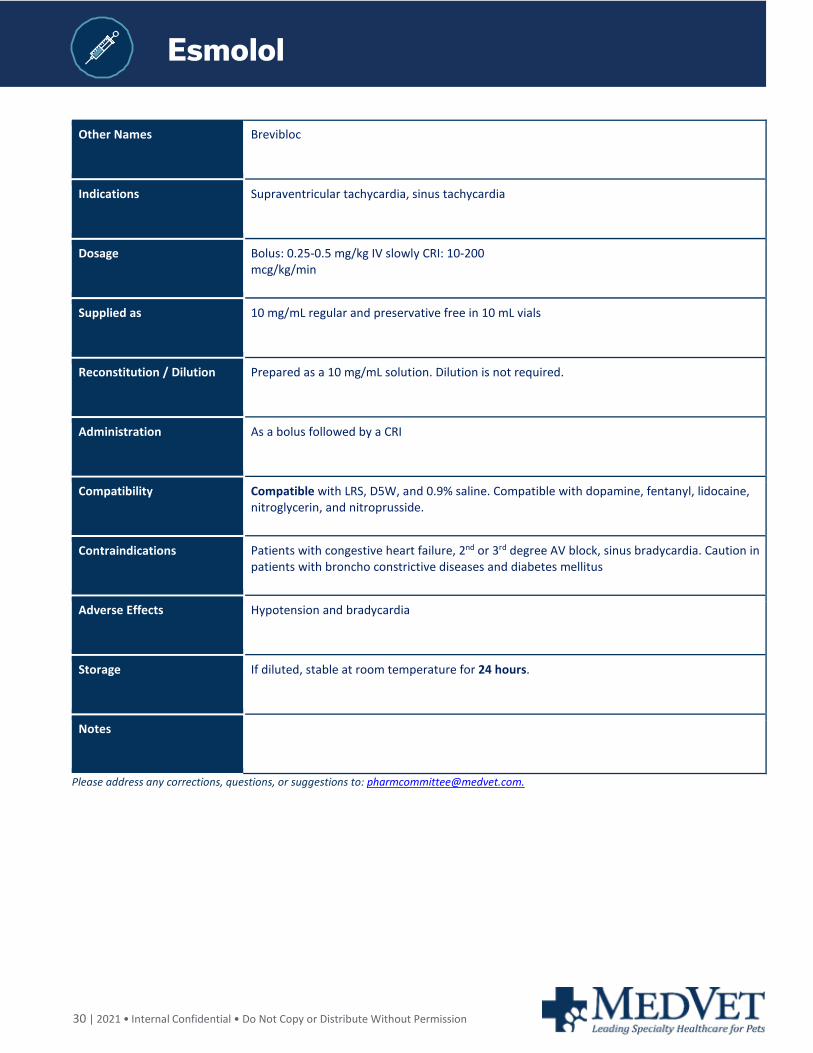
Other Names Brevibloc
Indications Supraventricular tachycardia, sinus tachycardia
Dosage Bolus: 0.25-0.5 mg/kg IV slowly CRI: 10-200 mcg/kg/min
Supplied as 10 mg/mL regular and preservative free in 10 mL vials
Reconstitution / Dilution Prepared as a 10 mg/mL solution. Dilution is not required.
Administration As a bolus followed by a CRI
Compatibility Compatible with LRS, D5W, and 0.9% saline. Compatible with dopamine, fentanyl, lidocaine, nitroglycerin, and nitroprusside.
Contraindications Patients with congestive heart failure, 2nd or 3rd degree AV block, sinus bradycardia. Caution in patients with broncho constrictive diseases and diabetes mellitus
Adverse Effects Hypotension and bradycardia
Storage If diluted, stable at room temperature for 24 hours.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
31 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Fentany
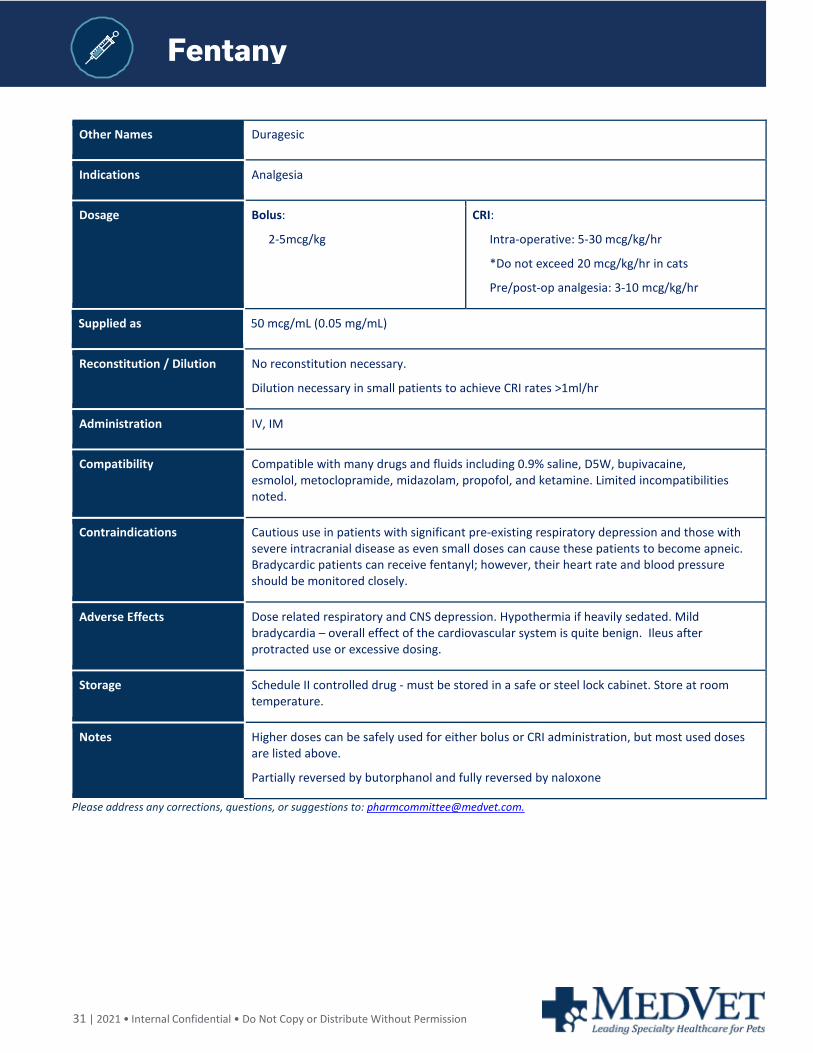
Other Names Duragesic
Indications Analgesia
Dosage Bolus:
2-5mcg/kg
CRI:
Intra-operative: 5-30 mcg/kg/hr
*Do not exceed 20 mcg/kg/hr in cats
Pre/post-op analgesia: 3-10 mcg/kg/hr
Supplied as 50 mcg/mL (0.05 mg/mL)
Reconstitution / Dilution No reconstitution necessary.
Dilution necessary in small patients to achieve CRI rates >1ml/hr
Administration IV, IM
Compatibility Compatible with many drugs and fluids including 0.9% saline, D5W, bupivacaine, esmolol, metoclopramide, midazolam, propofol, and ketamine. Limited incompatibilities noted.
Contraindications Cautious use in patients with significant pre-existing respiratory depression and those with severe intracranial disease as even small doses can cause these patients to become apneic. Bradycardic patients can receive fentanyl; however, their heart rate and blood pressure should be monitored closely.
Adverse Effects Dose related respiratory and CNS depression. Hypothermia if heavily sedated. Mild bradycardia – overall effect of the cardiovascular system is quite benign. Ileus after protracted use or excessive dosing.
Storage Schedule II controlled drug - must be stored in a safe or steel lock cabinet. Store at room temperature.
Notes Higher doses can be safely used for either bolus or CRI administration, but most used doses are listed above.
Partially reversed by butorphanol and fully reversed by naloxone
Please address any corrections, questions, or suggestions to: [email protected].
32 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Fomepizol
Fomepizol
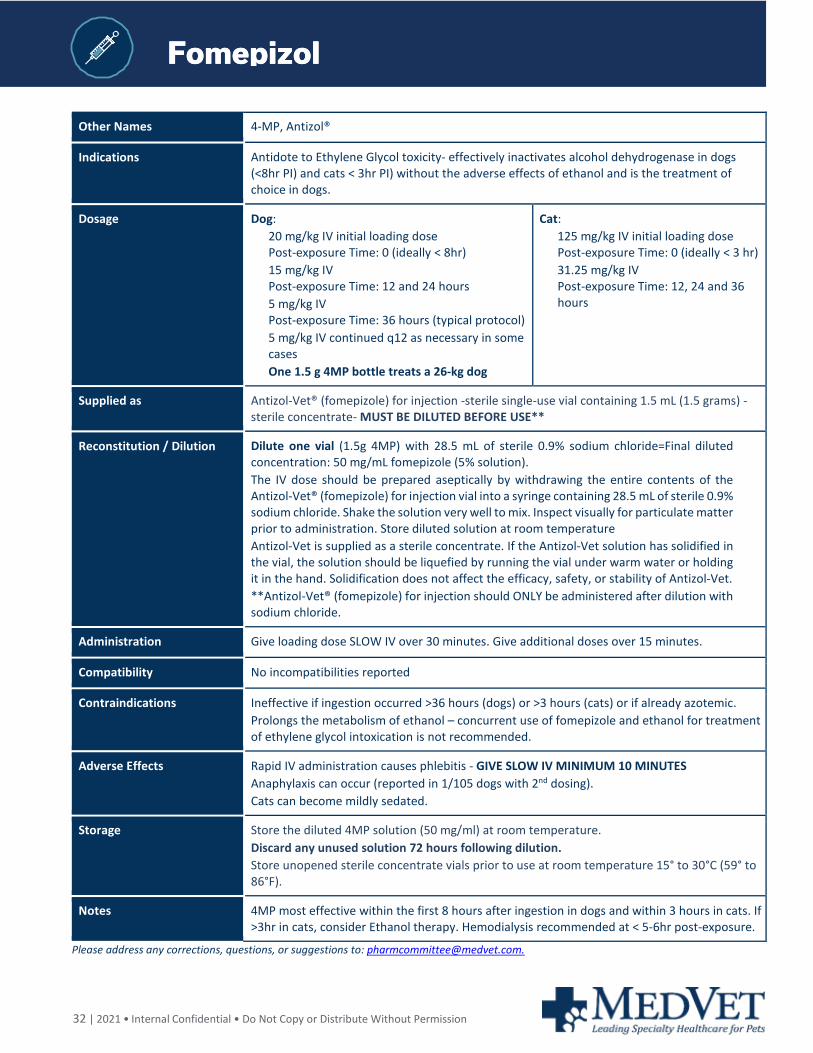
Other Names 4-MP, Antizol®
Indications Antidote to Ethylene Glycol toxicity- effectively inactivates alcohol dehydrogenase in dogs (<8hr PI) and cats < 3hr PI) without the adverse effects of ethanol and is the treatment of choice in dogs.
Dosage Dog: 20 mg/kg IV initial loading dose Post-exposure Time: 0 (ideally < 8hr) 15 mg/kg IV Post-exposure Time: 12 and 24 hours 5 mg/kg IV Post-exposure Time: 36 hours (typical protocol) 5 mg/kg IV continued q12 as necessary in some cases One 1.5 g 4MP bottle treats a 26-kg dog
Cat: 125 mg/kg IV initial loading dose Post-exposure Time: 0 (ideally < 3 hr) 31.25 mg/kg IV Post-exposure Time: 12, 24 and 36 hours
Supplied as Antizol-Vet® (fomepizole) for injection -sterile single-use vial containing 1.5 mL (1.5 grams) - sterile concentrate- MUST BE DILUTED BEFORE USE**
Reconstitution / Dilution Dilute one vial (1.5g 4MP) with 28.5 mL of sterile 0.9% sodium chloride=Final diluted concentration: 50 mg/mL fomepizole (5% solution). The IV dose should be prepared aseptically by withdrawing the entire contents of the Antizol-Vet® (fomepizole) for injection vial into a syringe containing 28.5 mL of sterile 0.9% sodium chloride. Shake the solution very well to mix. Inspect visually for particulate matter prior to administration. Store diluted solution at room temperature Antizol-Vet is supplied as a sterile concentrate. If the Antizol-Vet solution has solidified in the vial, the solution should be liquefied by running the vial under warm water or holding it in the hand. Solidification does not affect the efficacy, safety, or stability of Antizol-Vet. **Antizol-Vet® (fomepizole) for injection should ONLY be administered after dilution with sodium chloride.
Administration Give loading dose SLOW IV over 30 minutes. Give additional doses over 15 minutes.
Compatibility No incompatibilities reported
Contraindications Ineffective if ingestion occurred >36 hours (dogs) or >3 hours (cats) or if already azotemic. Prolongs the metabolism of ethanol – concurrent use of fomepizole and ethanol for treatment of ethylene glycol intoxication is not recommended.
Adverse Effects Rapid IV administration causes phlebitis - GIVE SLOW IV MINIMUM 10 MINUTES Anaphylaxis can occur (reported in 1/105 dogs with 2nd dosing). Cats can become mildly sedated.
Storage Store the diluted 4MP solution (50 mg/ml) at room temperature. Discard any unused solution 72 hours following dilution. Store unopened sterile concentrate vials prior to use at room temperature 15° to 30°C (59° to 86°F).
Notes 4MP most effective within the first 8 hours after ingestion in dogs and within 3 hours in cats. If >3hr in cats, consider Ethanol therapy. Hemodialysis recommended at < 5-6hr post-exposure.
Please address any corrections, questions, or suggestions to: [email protected].
33 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Furosemide
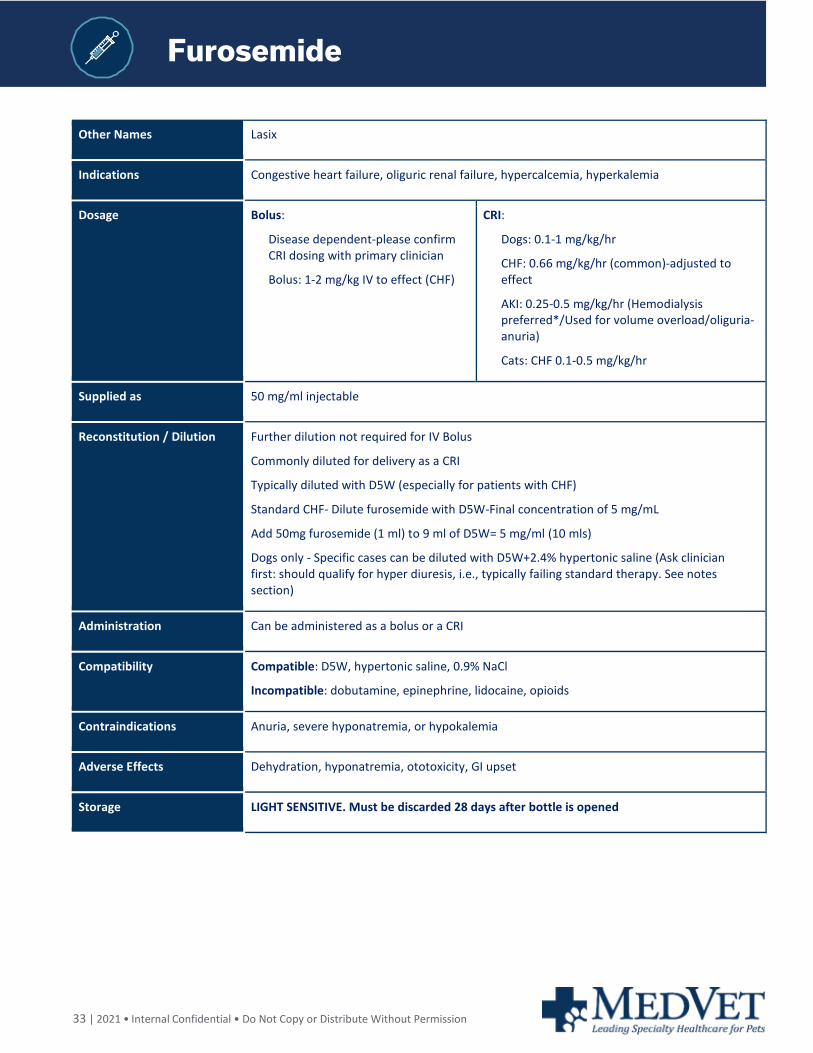
Other Names Lasix
Indications Congestive heart failure, oliguric renal failure, hypercalcemia, hyperkalemia
Dosage Bolus:
Disease dependent-please confirm CRI dosing with primary clinician
Bolus: 1-2 mg/kg IV to effect (CHF)
CRI:
Dogs: 0.1-1 mg/kg/hr
CHF: 0.66 mg/kg/hr (common)-adjusted to effect
AKI: 0.25-0.5 mg/kg/hr (Hemodialysis preferred*/Used for volume overload/oliguria-anuria)
Cats: CHF 0.1-0.5 mg/kg/hr
Supplied as 50 mg/ml injectable
Reconstitution / Dilution Further dilution not required for IV Bolus
Commonly diluted for delivery as a CRI
Typically diluted with D5W (especially for patients with CHF)
Standard CHF- Dilute furosemide with D5W-Final concentration of 5 mg/mL
Add 50mg furosemide (1 ml) to 9 ml of D5W= 5 mg/ml (10 mls)
Dogs only - Specific cases can be diluted with D5W+2.4% hypertonic saline (Ask clinician first: should qualify for hyper diuresis, i.e., typically failing standard therapy. See notes section)
Administration Can be administered as a bolus or a CRI
Compatibility Compatible: D5W, hypertonic saline, 0.9% NaCl
Incompatible: dobutamine, epinephrine, lidocaine, opioids
Contraindications Anuria, severe hyponatremia, or hypokalemia
Adverse Effects Dehydration, hyponatremia, ototoxicity, GI upset
Storage LIGHT SENSITIVE. Must be discarded 28 days after bottle is opened
34 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Furosemide
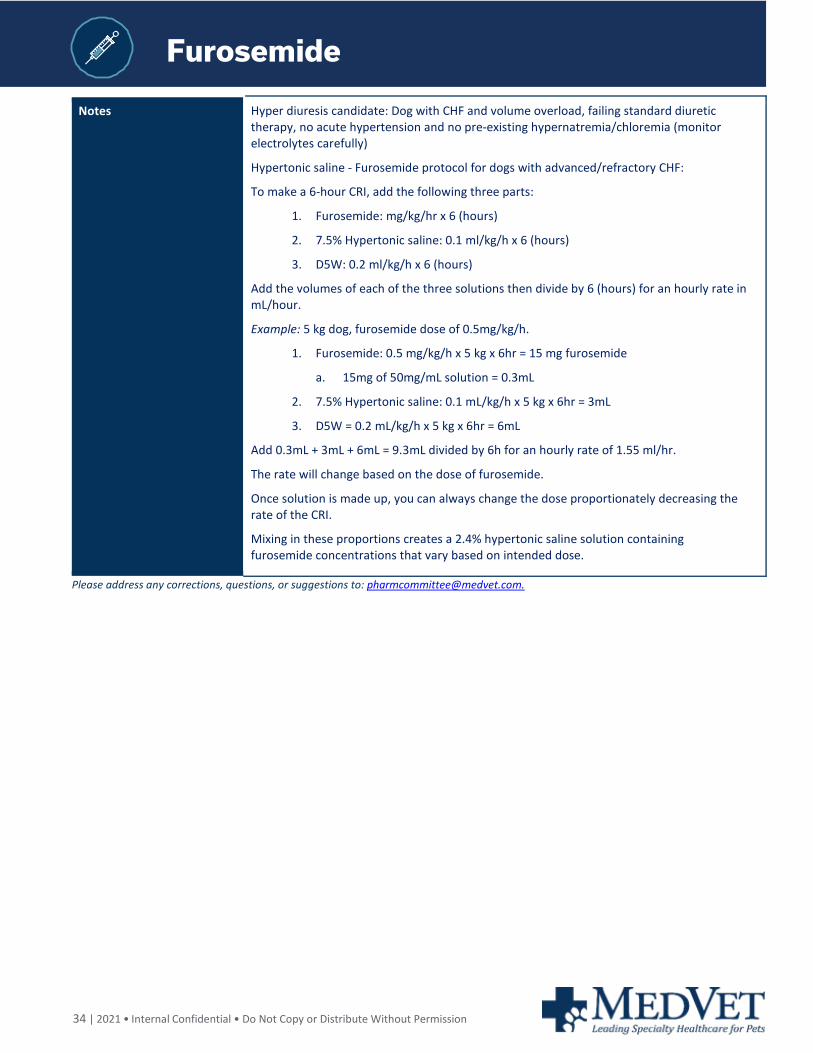
Notes Hyper diuresis candidate: Dog with CHF and volume overload, failing standard diuretic therapy, no acute hypertension and no pre-existing hypernatremia/chloremia (monitor electrolytes carefully)
Hypertonic saline - Furosemide protocol for dogs with advanced/refractory CHF:
To make a 6-hour CRI, add the following three parts:
1. Furosemide: mg/kg/hr x 6 (hours)
2. 7.5% Hypertonic saline: 0.1 ml/kg/h x 6 (hours)
3. D5W: 0.2 ml/kg/h x 6 (hours)
Add the volumes of each of the three solutions then divide by 6 (hours) for an hourly rate in mL/hour.
Example: 5 kg dog, furosemide dose of 0.5mg/kg/h.
1. Furosemide: 0.5 mg/kg/h x 5 kg x 6hr = 15 mg furosemide
a. 15mg of 50mg/mL solution = 0.3mL
2. 7.5% Hypertonic saline: 0.1 mL/kg/h x 5 kg x 6hr = 3mL
3. D5W = 0.2 mL/kg/h x 5 kg x 6hr = 6mL
Add 0.3mL + 3mL + 6mL = 9.3mL divided by 6h for an hourly rate of 1.55 ml/hr.
The rate will change based on the dose of furosemide.
Once solution is made up, you can always change the dose proportionately decreasing the rate of the CRI.
Mixing in these proportions creates a 2.4% hypertonic saline solution containing furosemide concentrations that vary based on intended dose.
Please address any corrections, questions, or suggestions to: [email protected].
35 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Glucagon
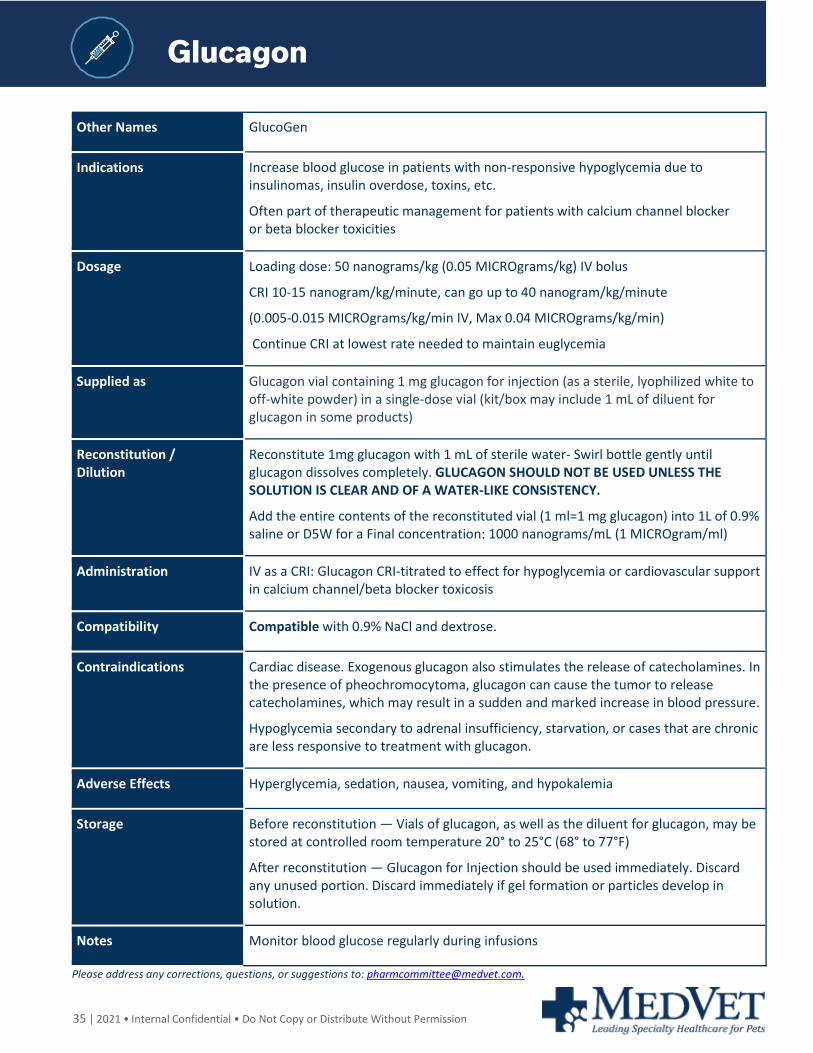
Other Names GlucoGen
Indications Increase blood glucose in patients with non-responsive hypoglycemia due to insulinomas, insulin overdose, toxins, etc.
Often part of therapeutic management for patients with calcium channel blocker or beta blocker toxicities
Dosage Loading dose: 50 nanograms/kg (0.05 MICROgrams/kg) IV bolus
CRI 10-15 nanogram/kg/minute, can go up to 40 nanogram/kg/minute
(0.005-0.015 MICROgrams/kg/min IV, Max 0.04 MICROgrams/kg/min)
Continue CRI at lowest rate needed to maintain euglycemia
Supplied as Glucagon vial containing 1 mg glucagon for injection (as a sterile, lyophilized white to off-white powder) in a single-dose vial (kit/box may include 1 mL of diluent for glucagon in some products)
Reconstitution / Dilution
Reconstitute 1mg glucagon with 1 mL of sterile water- Swirl bottle gently until glucagon dissolves completely. GLUCAGON SHOULD NOT BE USED UNLESS THE SOLUTION IS CLEAR AND OF A WATER-LIKE CONSISTENCY.
Add the entire contents of the reconstituted vial (1 ml=1 mg glucagon) into 1L of 0.9% saline or D5W for a Final concentration: 1000 nanograms/mL (1 MICROgram/ml)
Administration IV as a CRI: Glucagon CRI-titrated to effect for hypoglycemia or cardiovascular support in calcium channel/beta blocker toxicosis
Compatibility Compatible with 0.9% NaCl and dextrose.
Contraindications Cardiac disease. Exogenous glucagon also stimulates the release of catecholamines. In the presence of pheochromocytoma, glucagon can cause the tumor to release catecholamines, which may result in a sudden and marked increase in blood pressure.
Hypoglycemia secondary to adrenal insufficiency, starvation, or cases that are chronic are less responsive to treatment with glucagon.
Adverse Effects Hyperglycemia, sedation, nausea, vomiting, and hypokalemia
Storage Before reconstitution — Vials of glucagon, as well as the diluent for glucagon, may be stored at controlled room temperature 20° to 25°C (68° to 77°F)
After reconstitution — Glucagon for Injection should be used immediately. Discard any unused portion. Discard immediately if gel formation or particles develop in solution.
Notes Monitor blood glucose regularly during infusions
Please address any corrections, questions, or suggestions to: [email protected].

36 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Heparin (unfractionated)
Other Names Unfractionated heparin, UHF
Indications Anticoagulant used to prevent thromboembolic disease
Dosage Bolus: 150-300 units/kg SQ or IV CRI: 50-100 units/kg/hr
Supplied as 1000 Unit/mL solution (**PLEASE CHECK CONCENTRATION AS CAN VARY WITH PRODUCT)
Reconstitution / Dilution Dilution is not required but can be utilized to obtain appropriate volumes. Heparinized FLUSH = Final concentration 2 UNITS/ml Used for arterial/central and PICC line flush Add 2000 Units (1000 U/ml=2 ml) to 1 Liter 0.9% NaCl (0.5 mL (500 Units) per 250 mL bag). For blood collection/HemoSavr Autotransfusion=Final concentration 30 UNITS/ml 7500 U (1000 U/ml-7.5ml) in 25 0ml 0.9% NaCl=30 Units/ml 90 U (1000 U/ml-0.09ml) per 3 ml saline flush=30 Units/ml Ratio of blood collection to DILUTED heparin (30 U/ml) 1 5ml diluted heparin to 100ml blood collected 1ml diluted heparin to 7 ml blood collected **This equals 5 units of Heparin per ml of collected blood Heparin is not a preservative and does not enable storage of blood for later use - IF heparin is used as anticoagulant for blood collection it should be transfused immediately after collection.
Administration IV or SQ only, do not administer IM
Compatibility Compatible: 0.9% saline, LRS, lipids, calcium gluconate, clindamycin, dopamine, lidocaine, metronidazole, norepinephrine, KCl, and sodium bicarb. Incompatible (questionable): Dextrose solutions, ampicillin, and dobutamine.
Contraindications Thrombocytopenia, hemorrhage, coagulopathy
Adverse Effects Hemorrhage and thrombocytopenia (reported in humans). Hypersensitivity reactions can occur.
Storage Store at room temperature.
Notes Monitor PT/PTT, AntiXa activity, PCV/TS, platelet count Patients with renal disease will require higher doses as it is renally excreted. Studies have confirmed that critically ill patients and those with IMHA have non-linear and unpredictable responses to standard dosing schemes-ideally AntiXa activity should be monitored and used to titrate heparin CRI to effect for individual patient dosing. If this cannot be performed other anticoagulant therapy should be substituted.
Please address any corrections, questions, or suggestions to: [email protected].
37 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Hydromorphone
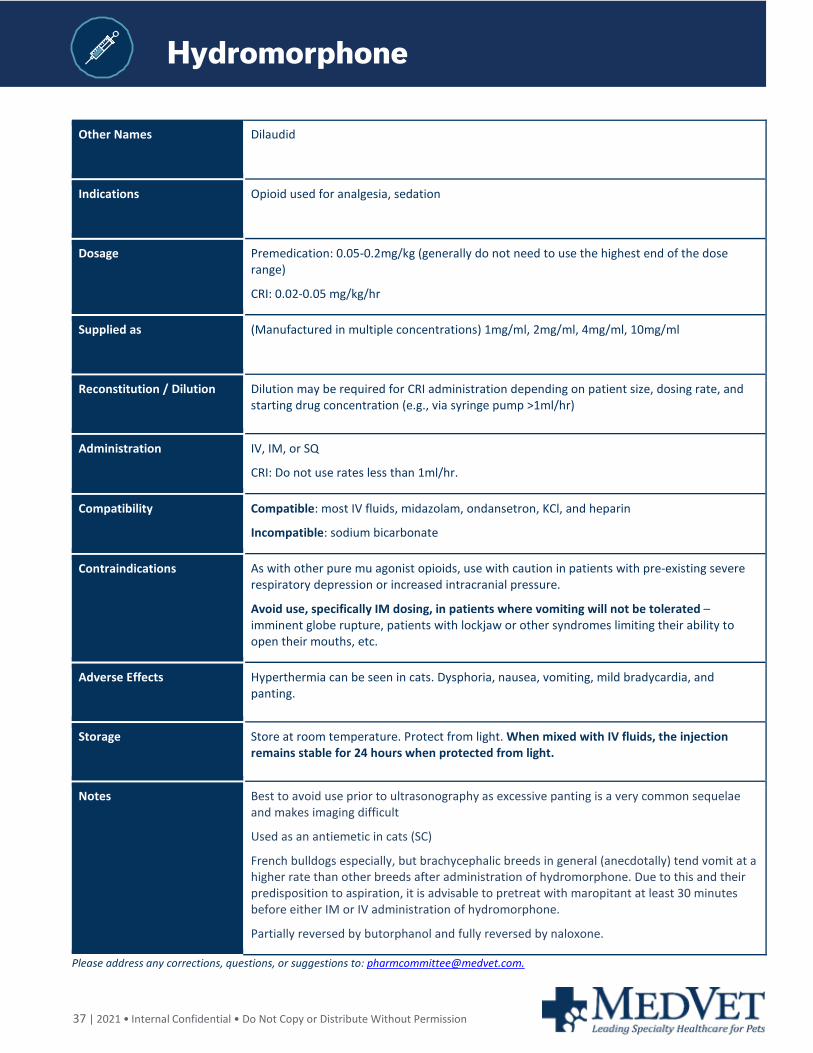
Other Names Dilaudid
Indications Opioid used for analgesia, sedation
Dosage Premedication: 0.05-0.2mg/kg (generally do not need to use the highest end of the dose range)
CRI: 0.02-0.05 mg/kg/hr
Supplied as (Manufactured in multiple concentrations) 1mg/ml, 2mg/ml, 4mg/ml, 10mg/ml
Reconstitution / Dilution Dilution may be required for CRI administration depending on patient size, dosing rate, and starting drug concentration (e.g., via syringe pump >1ml/hr)
Administration IV, IM, or SQ
CRI: Do not use rates less than 1ml/hr.
Compatibility Compatible: most IV fluids, midazolam, ondansetron, KCl, and heparin
Incompatible: sodium bicarbonate
Contraindications As with other pure mu agonist opioids, use with caution in patients with pre-existing severe respiratory depression or increased intracranial pressure.
Avoid use, specifically IM dosing, in patients where vomiting will not be tolerated – imminent globe rupture, patients with lockjaw or other syndromes limiting their ability to open their mouths, etc.
Adverse Effects Hyperthermia can be seen in cats. Dysphoria, nausea, vomiting, mild bradycardia, and panting.
Storage Store at room temperature. Protect from light. When mixed with IV fluids, the injection remains stable for 24 hours when protected from light.
Notes Best to avoid use prior to ultrasonography as excessive panting is a very common sequelae and makes imaging difficult
Used as an antiemetic in cats (SC)
French bulldogs especially, but brachycephalic breeds in general (anecdotally) tend vomit at a higher rate than other breeds after administration of hydromorphone. Due to this and their predisposition to aspiration, it is advisable to pretreat with maropitant at least 30 minutes before either IM or IV administration of hydromorphone.
Partially reversed by butorphanol and fully reversed by naloxone.
Please address any corrections, questions, or suggestions to: [email protected].
38 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Ketamin
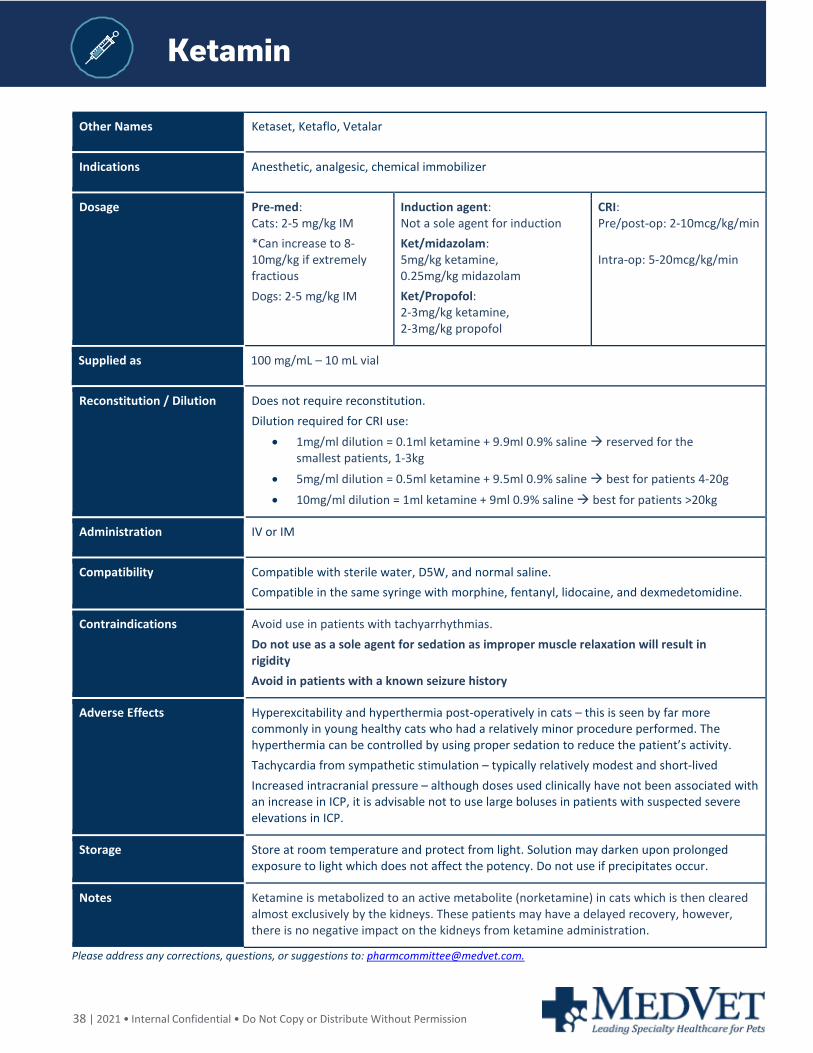
Other Names Ketaset, Ketaflo, Vetalar
Indications Anesthetic, analgesic, chemical immobilizer
Dosage Pre-med: Cats: 2-5 mg/kg IM *Can increase to 8-10mg/kg if extremely fractious Dogs: 2-5 mg/kg IM
Induction agent: Not a sole agent for induction Ket/midazolam: 5mg/kg ketamine, 0.25mg/kg midazolam Ket/Propofol: 2-3mg/kg ketamine, 2-3mg/kg propofol
CRI: Pre/post-op: 2-10mcg/kg/min Intra-op: 5-20mcg/kg/min
Supplied as 100 mg/mL – 10 mL vial
Reconstitution / Dilution Does not require reconstitution. Dilution required for CRI use:
• 1mg/ml dilution = 0.1ml ketamine + 9.9ml 0.9% saline reserved for the smallest patients, 1-3kg
• 5mg/ml dilution = 0.5ml ketamine + 9.5ml 0.9% saline best for patients 4-20g • 10mg/ml dilution = 1ml ketamine + 9ml 0.9% saline best for patients >20kg
Administration IV or IM
Compatibility Compatible with sterile water, D5W, and normal saline. Compatible in the same syringe with morphine, fentanyl, lidocaine, and dexmedetomidine.
Contraindications Avoid use in patients with tachyarrhythmias. Do not use as a sole agent for sedation as improper muscle relaxation will result in rigidity Avoid in patients with a known seizure history
Adverse Effects Hyperexcitability and hyperthermia post-operatively in cats – this is seen by far more commonly in young healthy cats who had a relatively minor procedure performed. The hyperthermia can be controlled by using proper sedation to reduce the patient’s activity. Tachycardia from sympathetic stimulation – typically relatively modest and short-lived Increased intracranial pressure – although doses used clinically have not been associated with an increase in ICP, it is advisable not to use large boluses in patients with suspected severe elevations in ICP.
Storage Store at room temperature and protect from light. Solution may darken upon prolonged exposure to light which does not affect the potency. Do not use if precipitates occur.
Notes Ketamine is metabolized to an active metabolite (norketamine) in cats which is then cleared almost exclusively by the kidneys. These patients may have a delayed recovery, however, there is no negative impact on the kidneys from ketamine administration.
Please address any corrections, questions, or suggestions to: [email protected].
39 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Levetiracetam
Other Names Keppra
Indications Seizure control
Dosage Loading dose: 40-60 mg/kg IV
Maintenance dose: 20-30 mg/kg IV q8h
Can be given IM, SC
Supplied as Levetiracetam concentrate for injection: 100 mg/mL in 5 mL single use vials (other sizes available but not typically used)
Reconstitution / Dilution No dilution needed in emergent situations but still need to give slowly
Can be diluted 1:10 to a final concentration of 10mg/mL to prevent phlebitis and burning on administration
Administration Give slowly over at least 5-15 minutes if undiluted – reported anaphylactoid events with rapid administration
If diluted, give over 15 minutes.
Compatibility Limited information available
Contraindications Appears to be well tolerated in dogs and cats.
Adverse Effects Sedation in dogs, lethargy, and decreased appetite in cats.
Storage Store at room temperature for 24 hours once diluted. Does not require refrigeration.
Notes Charged per vial – do not confuse with the 100 mg/mL oral solution that is charged by mL
Please address any corrections, questions, or suggestions to: [email protected].
40 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Lidocaine
Other Names Xylocaine
Indications Local anesthetic agent, treatment of ventricular tachycardia, and as an adjunct to analgesic therapy.
Dosage Antiarrhythmic: Dogs: 50-100 mcg/kg/min
Analgesic: Dogs: 50 mcg/kg/min
In dogs, an initial bolus of 2 mg/kg is generally administered to reach adequate plasma levels. In cats a bolus of 0.25 mg/kg is typically recommended to treat ventricular arrhythmias, however, some consider other antiarrhythmics (procainamide) to be first line in treatment in this species.
Local/regional: 1-2 mg/kg (can be diluted to desired volume with saline depending on block being performed)
Supplied as 2% (20 mg/mL) solution
Reconstitution Does not require dilution BUT dilution is needed in small patients for CRI administration
Administration Administer bolus over 1-2 minutes. When used as a CRI for anti-arrhythmic effects, do not discontinue for diagnostics, walks, etc.
Compatibility Compatible with 0.9% saline, 0.45% saline, D5W, LRS, Plasmalyte, and Normosol
Compatible with ketamine, opioid injection formulations, dexmedetomidine, dobutamine, and metoclopramide.
Incompatible with dopamine, isoproterenol, norepinephrine, ampicillin, and cefazolin.
Contraindications VERY cautious use, if at all, in cats. Cardiac and neurotoxicity occur at significantly lower levels than in dogs.
Careful use in bradycardic patients or patients with high grade AV block. Do not use in patients in 3rd degree AV block.
Lower doses suggested in patients with known MDR-1 mutation and those with severe hepatic dysfunction.
Adverse Effects Monitor for signs of toxicity:
• GI: nausea, salivation, vomiting, ileus
• Neurologic: ataxia, nystagmus, depression, seizures
• Cardiac: bradycardia
Caution in cats
Storage Stored at room temperature
Notes Short duration of action (<10 minutes), if CRI is discontinued for >10 minutes an additional loading dose may be needed.
Please address any corrections, questions, or suggestions to: [email protected].

41 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Intravenous Lipid Emulsion
Other Names Fat Emulsion, Intralipid® (20%), Liposyn (20%), Intravenous Lipid Emulsion
Indications Primarily used to manage certain toxins/drug overdoses with known response to ILE
Parenteral calorie and fatty acid source
Dosage 1.5 ml/kg bolus IV over 1-3 minutes, then give as a CRI at 0.25 ml/kg/min for MAX 60 min (equivalent to 15ml/kg given over an hour-ideally utilizing a syringe or IV pump)
Can be repeated 4-6 hours if serum is NOT lipemic and clinical signs require additional doses
Supplied as Intralipid 20% lipid emulsion, Liposyn is supplied in other concentrations - use 20% only
Reconstitution When used for the management of intoxications no dilution or reconstitution required (ensure only 20% lipid emulsion product is used)
The creation of TPN/PPN solutions and mixing of other constituents with lipid emulsions should not performed without proper equipment/training.
Administration Administer alone through a dedicated and patent IV catheter.
Use aseptic technique and monitor catheter closely as extravasation may lead to irritation or possible abscess.
Unlike TPN/ PPN, can be administered in a peripheral line
Compatibility Use caution when administering other lipid-soluble drugs as ILE will decrease their effectiveness, particularly lidocaine and calcium channel blockers.
Contraindications Use caution in neonates; generally safe
Adverse Effects Potential vesicant if extravasated.
Fat overload syndrome (very rare): pulmonary changes, GI effects, somnolence, pancreatitis, hypercoagulability, and hypersensitivity.
Storage Unopened bottles/bags should be stored at room temperature and not allowed to freeze. Unused amounts can be stored in the refrigerator and discarded 24 hours after opening. A new bag or vial must be used every 24 hours.
Notes Filter not required for administration.
Please address any corrections, questions, or suggestions to: [email protected].
42 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Magnesium Sulfate
Magnesium Sulfate
Other Names MgSO4
Indications • Ventricular arrhythmias (severe V-tach, torsade de pointes)
• Pheochromocytoma peri-op management
• Ionized hypomagnesemia (common in DKA patients)
• Adjunct for refractory hypokalemia/hypocalcemia management
• Adjunct to eclampsia induced seizures
• Adjunct severe generalized tetanus
• Magnesium sulfate’s characteristics make it a useful drug in several emergent conditions: It is a NMDA receptor antagonist, vasodilator, antiarrhythmic, inhibitor of catecholamine release and of acetylcholine in the terminal motor plate.
Dosage ER LOADING DOSE: 20-40 mg/kg IV bolus [0.15-0.3 mEq/kg] (given over 5-60min per DVM)
Arrhythmia/Rapid CRI: 1.25-5 mg/kg/hr [0.01-0.04 mEq/kg/hr]
Pheochromocytoma/Hypertension: 40mg/kg IV bolus followed by 15 mg/kg/hr
*Please Note dosing differences – often listed as mg vs mEq
Supplied as 50% solution (500 mg/mL) which is equal to 4mEq/mL.
Reconstitution / Dilution Magnesium sulfate injection (supplied as 50%) MUST be diluted to a concentration of 20% or LESS prior to IV infusion. Typically administered as a CRI diluted to 2.5-12.5% concentration (25-125 mg/ml)
Can dilute with either 0.9% saline or D5W
12.5% solution (125 mg/ml)-Add 15ml MgSO4 at 500mg/ml (50%) to 45 ml of 0.9% Saline for a total volume of 60ml-FINAL CONCENTRATION-125 mg/ml (1 mEq/ml)
- or -
2.5% solution (25 mg/ml)-Add 3ml MgSO4 at 500 mg/ml (50%) to 57 ml of 0.9% Saline for a total volume of 60ml-FINAL CONCENTRATION-25 mg/ml (0.2 mEq/ml)
Administration For emergent situations often given as a loading bolus followed by a CRI
Compatibility Compatible: D5W and 0.9% saline, metoclopramide, verapamil, ampicillin, cefazolin, doxycycline, esmolol, heparin, KCl.
Incompatible: IV lipids, dobutamine, sodium bicarbonate, LRS or any calcium or lactate containing fluid
Magnesium sulfate in solution may result in a precipitate formation when mixed with solutions containing: Calcium, Clindamycin, Hydrocortisone Sodium Succinate, Polymyxin B Sulfate
Contraindications Do not use with AV heart block. Magnesium sulfate should be given very cautiously in the presence of serious impairment of renal function since it is excreted almost entirely by the kidneys.

43 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Magnesium Sulfate
Adverse Effects Hypotension, bradycardia, severe muscle weakness=respiratory depression, loss patellar reflex, CNS depression, coma, fatal arrhythmias
The central and peripheral effects of magnesium poisoning are antagonized to some extent by IV administration of calcium.
Storage Do not refrigerate.
Notes
At higher doses requires very close monitoring as can lead to serious respiratory depression, bradycardia, hypotension-ICU monitoring, continuous telemetry, serial BP, patellar reflex tendon assessments q2-6hr, serial electrolytes (including ionized calcium, K, Phos, Mg), daily CREA+/- urine output monitoring.
Overdosage: Magnesium intoxication is manifested by a sharp drop in blood pressure and respiratory paralysis. Disappearance of the patellar reflex is a useful clinical sign to detect the onset of magnesium intoxication. In the event of overdosage, manual ventilation must be provided until a calcium gluconate can be injected IV to antagonize the effects of magnesium.
Important Conversions: Magnesium sulfate:
10% solution (100 mg/ml) =0.8 mEq/ml
12.5% solution (125mg/ml) =1 mEq/ml
1mEq Mg = 0.5 mmol M g= 12.3mg Magnesium
1 g MgSO4 = 8.12 mEq Mg
1 mmol/L = 2.46 mg/dL
Please address any corrections, questions, or suggestions to: [email protected].
44 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Mannitol
Other Names Mannitol (Osmitrol)
Indications Osmotic diuretic
An osmotic diuretic used primarily to manage increased ICP (intracerebral pressures); less commonly for oliguric acute kidney injury and to reduce intraocular pressure (IOP)
Dosage 0.25-2* grams/kg IV (*higher doses typically reserved for ICP cases as this can cause AKI)
Supplied as Mannitol 20% (200 mg/ml=0.2 grams/ml) solution (unless opening a new vial for a patient this medication is not considered to be sterile)
Reconstitution / Dilution No reconstitution or dilution needed.
Doses should be withdrawn from the vial using a 5-micron filter needle due the risk of crystallization.
A 0.22 micron in-line or membrane (Bacteriostatic) filter must be used during administration for all mannitol parenteral solutions.
Doses are prescribed in grams/kg please make sure you are administering the correct number of grams vs. milligrams per kg.
Administration IV: Over 20-30 minutes. Must use a filter – 0.2 um micron filter.
Compatibility Incompatible with whole blood products, NaCl, KCl, and strongly acidic or alkaline solutions.
Contraindications Do not give to patients receiving sotalol or oliguric volume overloaded patients (dialysis referral ideal).
Hypovolemia, severe dehydration, anuria secondary to renal disease, or pulmonary edema.
Adverse Effects Fluid and electrolyte imbalances (hyperosmolarity), nausea, vomiting, and fluid overload (pulmonary edema, CHF)
SEVERE VESICANT POTENTIAL IF EXTRAVASATED. Ensure catheter patency prior to administration.
If extravasation occurs, stop infusion, leave catheter in place, and contact doctor.
Storage Store at controlled room temperature between 15° and 30°C (59° and 86°F)
When stored at room temperature crystallization may occur.
To avoid crystallization, bottles can be kept in a warm water bath (set at 38C/100F).
Notes This solution his HYPERosmolar and contains 1098 mOsmols/Liter
Crystals of mannitol may form in a 20% saturated solution of mannitol. Dissolve the crystals by warming in hot water or autoclaving for 15 minutes. Cool to body temperature before administering. This is a single dose vial that contains no preservatives. Use entire contents when first opened, re-sterilize by autoclaving and/or use a 0.2 um micron bacteriostatic membrane filter
Close monitoring of electrolytes, fluid volume status, acid-base status and urine output is recommended, HR and BP monitoring may also be considered.
Please address any corrections, questions, or suggestions to: [email protected].
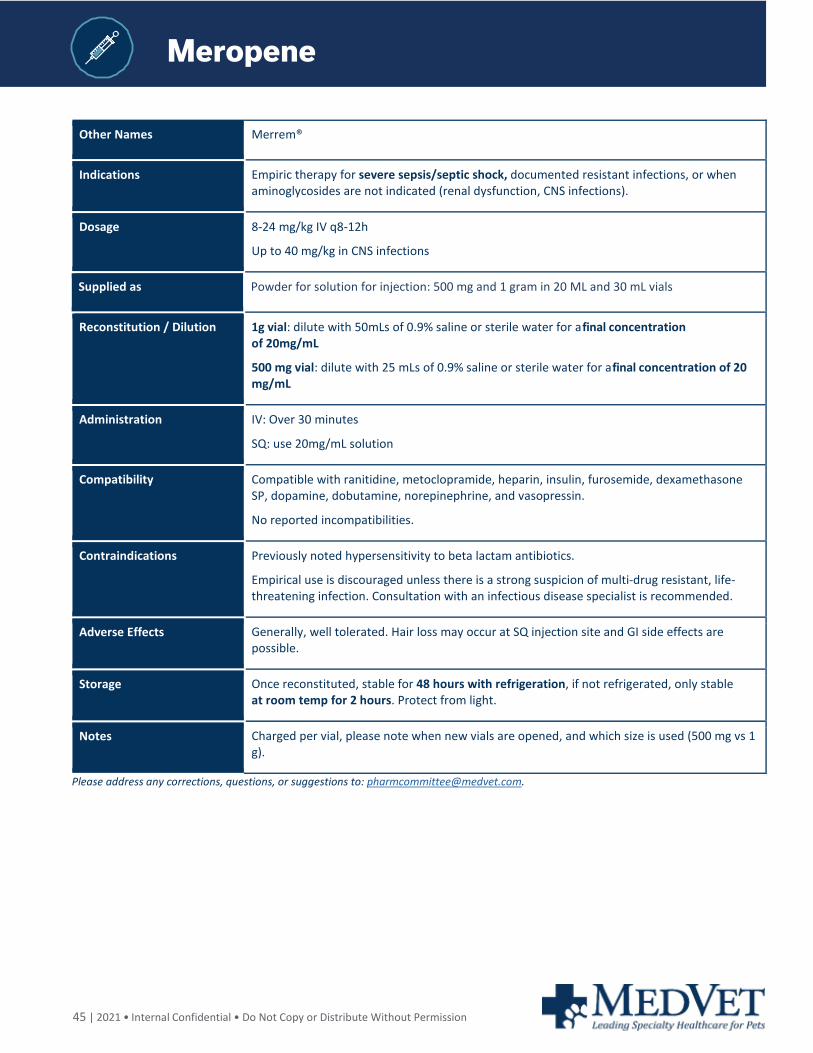
45 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Meropene
Other Names Merrem®
Indications Empiric therapy for severe sepsis/septic shock, documented resistant infections, or when aminoglycosides are not indicated (renal dysfunction, CNS infections).
Dosage 8-24 mg/kg IV q8-12h
Up to 40 mg/kg in CNS infections
Supplied as Powder for solution for injection: 500 mg and 1 gram in 20 ML and 30 mL vials
Reconstitution / Dilution 1g vial: dilute with 50mLs of 0.9% saline or sterile water for a final concentration of 20mg/mL
500 mg vial: dilute with 25 mLs of 0.9% saline or sterile water for a final concentration of 20 mg/mL
Administration IV: Over 30 minutes
SQ: use 20mg/mL solution
Compatibility Compatible with ranitidine, metoclopramide, heparin, insulin, furosemide, dexamethasone SP, dopamine, dobutamine, norepinephrine, and vasopressin.
No reported incompatibilities.
Contraindications Previously noted hypersensitivity to beta lactam antibiotics.
Empirical use is discouraged unless there is a strong suspicion of multi-drug resistant, life-threatening infection. Consultation with an infectious disease specialist is recommended.
Adverse Effects Generally, well tolerated. Hair loss may occur at SQ injection site and GI side effects are possible.
Storage Once reconstituted, stable for 48 hours with refrigeration, if not refrigerated, only stable at room temp for 2 hours. Protect from light.
Notes Charged per vial, please note when new vials are opened, and which size is used (500 mg vs 1 g).
Please address any corrections, questions, or suggestions to: [email protected].
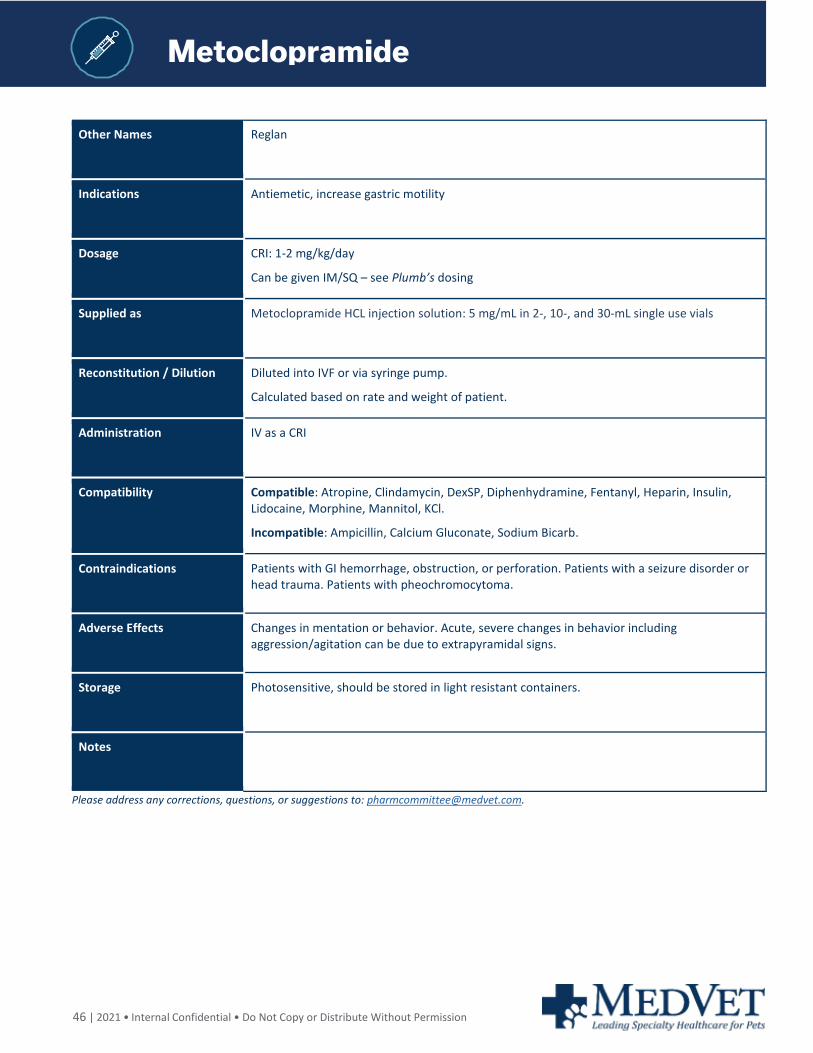
46 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Metoclopramide
Other Names Reglan
Indications Antiemetic, increase gastric motility
Dosage CRI: 1-2 mg/kg/day
Can be given IM/SQ – see Plumb’s dosing
Supplied as Metoclopramide HCL injection solution: 5 mg/mL in 2-, 10-, and 30-mL single use vials
Reconstitution / Dilution Diluted into IVF or via syringe pump.
Calculated based on rate and weight of patient.
Administration IV as a CRI
Compatibility Compatible: Atropine, Clindamycin, DexSP, Diphenhydramine, Fentanyl, Heparin, Insulin, Lidocaine, Morphine, Mannitol, KCl.
Incompatible: Ampicillin, Calcium Gluconate, Sodium Bicarb.
Contraindications Patients with GI hemorrhage, obstruction, or perforation. Patients with a seizure disorder or head trauma. Patients with pheochromocytoma.
Adverse Effects Changes in mentation or behavior. Acute, severe changes in behavior including aggression/agitation can be due to extrapyramidal signs.
Storage Photosensitive, should be stored in light resistant containers.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
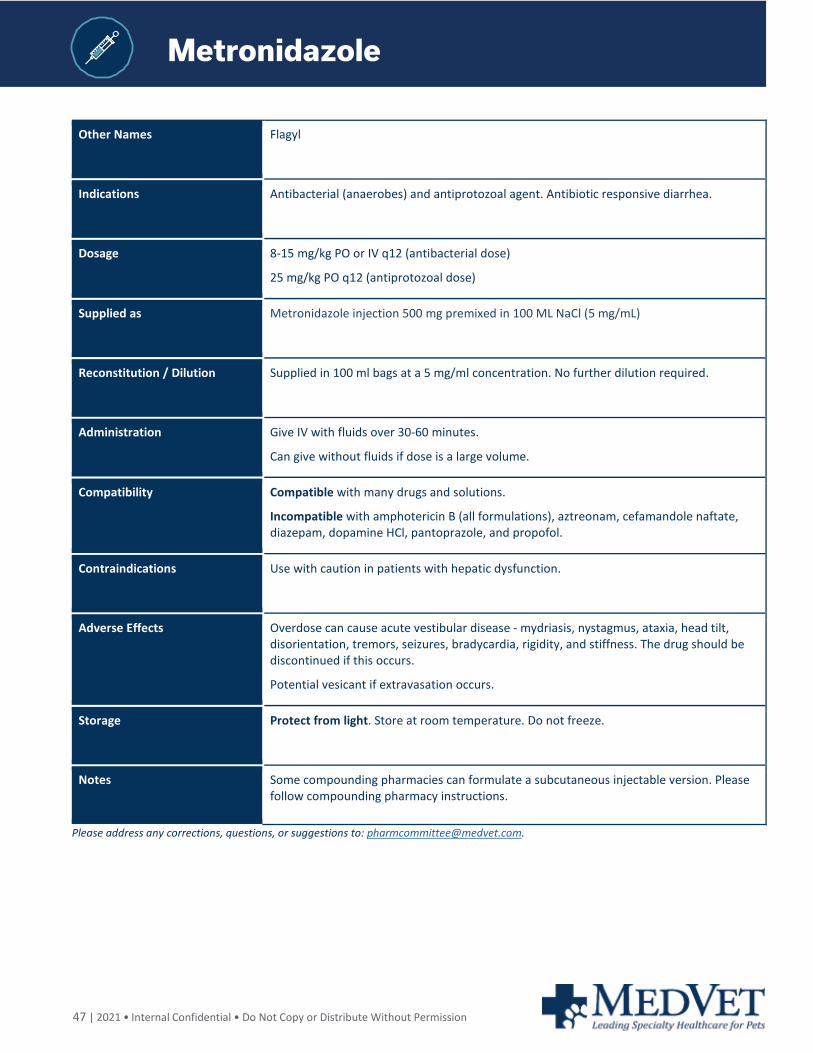
47 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Metronidazole
Other Names Flagyl
Indications Antibacterial (anaerobes) and antiprotozoal agent. Antibiotic responsive diarrhea.
Dosage 8-15 mg/kg PO or IV q12 (antibacterial dose)
25 mg/kg PO q12 (antiprotozoal dose)
Supplied as Metronidazole injection 500 mg premixed in 100 ML NaCl (5 mg/mL)
Reconstitution / Dilution Supplied in 100 ml bags at a 5 mg/ml concentration. No further dilution required.
Administration Give IV with fluids over 30-60 minutes.
Can give without fluids if dose is a large volume.
Compatibility Compatible with many drugs and solutions.
Incompatible with amphotericin B (all formulations), aztreonam, cefamandole naftate, diazepam, dopamine HCl, pantoprazole, and propofol.
Contraindications Use with caution in patients with hepatic dysfunction.
Adverse Effects Overdose can cause acute vestibular disease - mydriasis, nystagmus, ataxia, head tilt, disorientation, tremors, seizures, bradycardia, rigidity, and stiffness. The drug should be discontinued if this occurs.
Potential vesicant if extravasation occurs.
Storage Protect from light. Store at room temperature. Do not freeze.
Notes Some compounding pharmacies can formulate a subcutaneous injectable version. Please follow compounding pharmacy instructions.
Please address any corrections, questions, or suggestions to: [email protected].
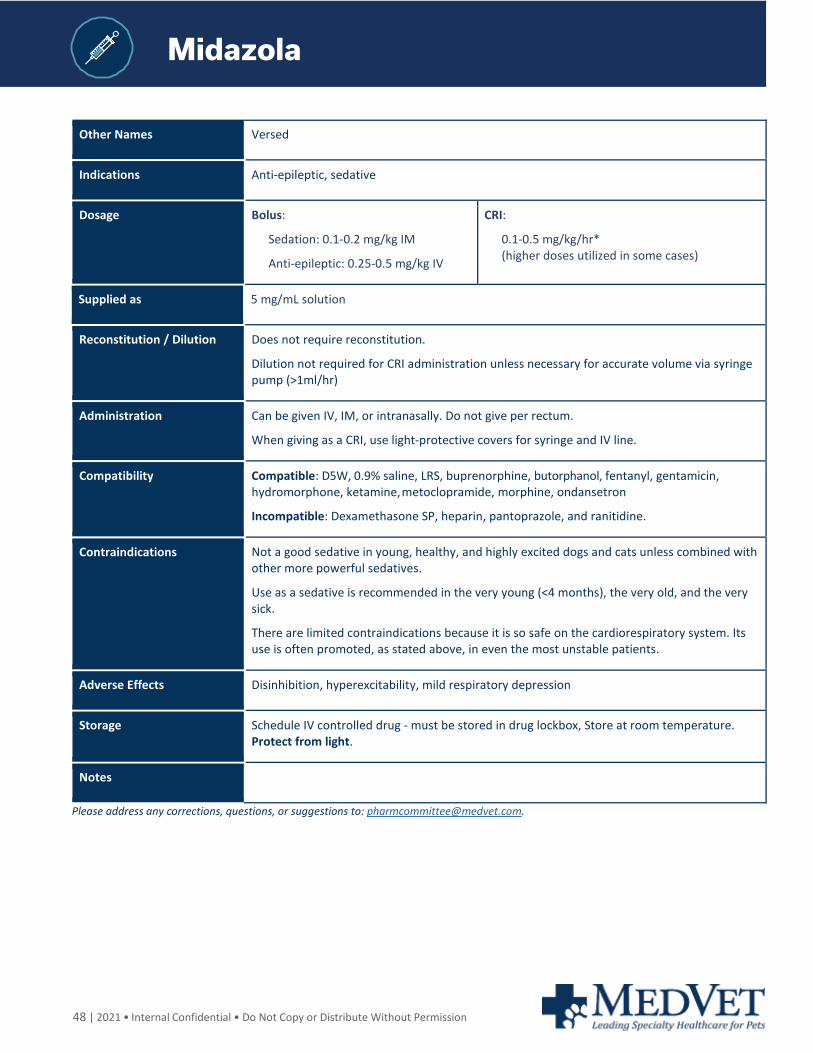
48 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Midazola
Other Names Versed
Indications Anti-epileptic, sedative
Dosage Bolus:
Sedation: 0.1-0.2 mg/kg IM
Anti-epileptic: 0.25-0.5 mg/kg IV
CRI:
0.1-0.5 mg/kg/hr* (higher doses utilized in some cases)
Supplied as 5 mg/mL solution
Reconstitution / Dilution Does not require reconstitution.
Dilution not required for CRI administration unless necessary for accurate volume via syringe pump (>1ml/hr)
Administration Can be given IV, IM, or intranasally. Do not give per rectum.
When giving as a CRI, use light-protective covers for syringe and IV line.
Compatibility Compatible: D5W, 0.9% saline, LRS, buprenorphine, butorphanol, fentanyl, gentamicin, hydromorphone, ketamine, metoclopramide, morphine, ondansetron
Incompatible: Dexamethasone SP, heparin, pantoprazole, and ranitidine.
Contraindications Not a good sedative in young, healthy, and highly excited dogs and cats unless combined with other more powerful sedatives.
Use as a sedative is recommended in the very young (<4 months), the very old, and the very sick.
There are limited contraindications because it is so safe on the cardiorespiratory system. Its use is often promoted, as stated above, in even the most unstable patients.
Adverse Effects Disinhibition, hyperexcitability, mild respiratory depression
Storage Schedule IV controlled drug - must be stored in drug lockbox, Store at room temperature. Protect from light.
Notes
Please address any corrections, questions, or suggestions to: [email protected].
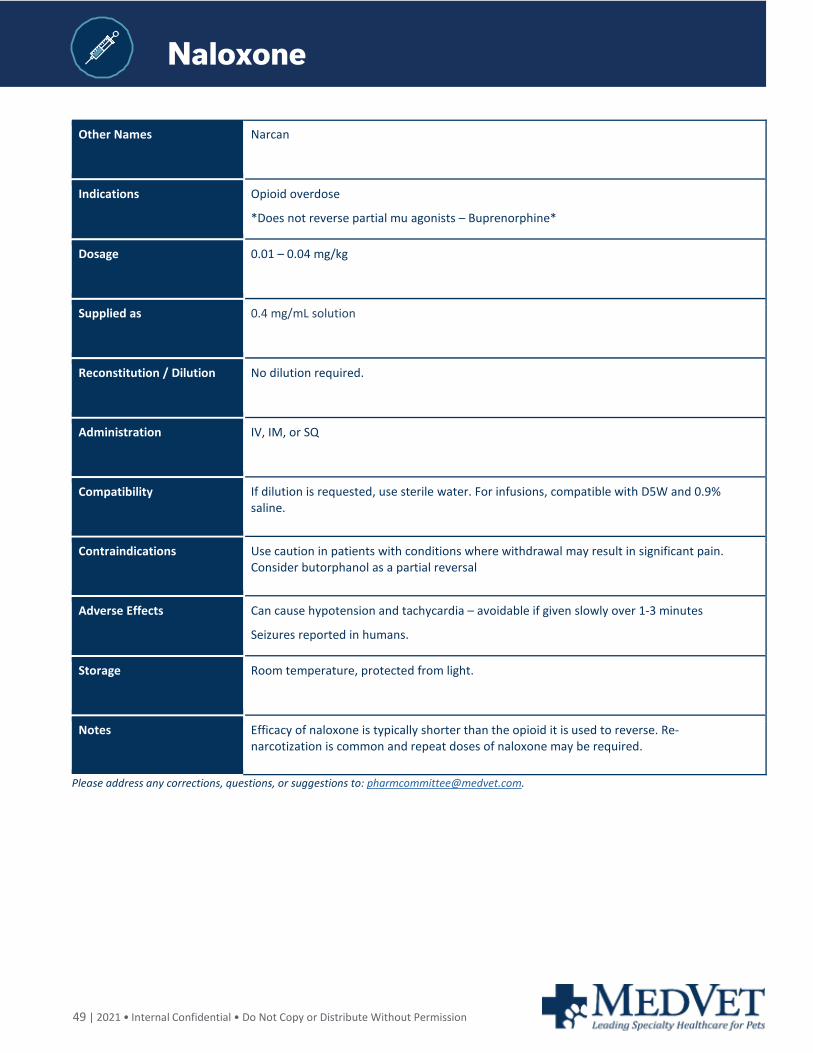
49 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Naloxone
Other Names Narcan
Indications Opioid overdose
*Does not reverse partial mu agonists – Buprenorphine*
Dosage 0.01 – 0.04 mg/kg
Supplied as 0.4 mg/mL solution
Reconstitution / Dilution No dilution required.
Administration IV, IM, or SQ
Compatibility If dilution is requested, use sterile water. For infusions, compatible with D5W and 0.9% saline.
Contraindications Use caution in patients with conditions where withdrawal may result in significant pain. Consider butorphanol as a partial reversal
Adverse Effects Can cause hypotension and tachycardia – avoidable if given slowly over 1-3 minutes
Seizures reported in humans.
Storage Room temperature, protected from light.
Notes Efficacy of naloxone is typically shorter than the opioid it is used to reverse. Re-narcotization is common and repeat doses of naloxone may be required.
Please address any corrections, questions, or suggestions to: [email protected].
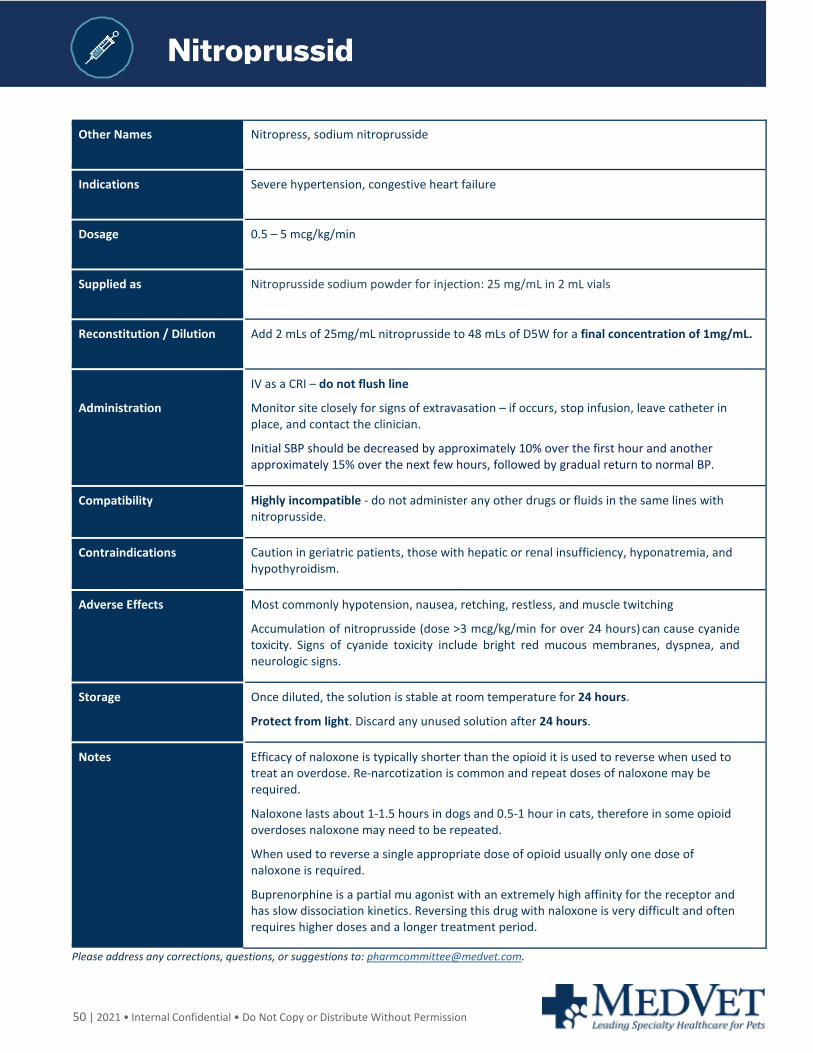
50 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Nitroprussid
Other Names Nitropress, sodium nitroprusside
Indications Severe hypertension, congestive heart failure
Dosage 0.5 – 5 mcg/kg/min
Supplied as Nitroprusside sodium powder for injection: 25 mg/mL in 2 mL vials
Reconstitution / Dilution Add 2 mLs of 25mg/mL nitroprusside to 48 mLs of D5W for a final concentration of 1mg/mL.
Administration
IV as a CRI – do not flush line
Monitor site closely for signs of extravasation – if occurs, stop infusion, leave catheter in place, and contact the clinician.
Initial SBP should be decreased by approximately 10% over the first hour and another approximately 15% over the next few hours, followed by gradual return to normal BP.
Compatibility Highly incompatible - do not administer any other drugs or fluids in the same lines with nitroprusside.
Contraindications Caution in geriatric patients, those with hepatic or renal insufficiency, hyponatremia, and hypothyroidism.
Adverse Effects Most commonly hypotension, nausea, retching, restless, and muscle twitching
Accumulation of nitroprusside (dose >3 mcg/kg/min for over 24 hours) can cause cyanide toxicity. Signs of cyanide toxicity include bright red mucous membranes, dyspnea, and neurologic signs.
Storage Once diluted, the solution is stable at room temperature for 24 hours.
Protect from light. Discard any unused solution after 24 hours.
Notes Efficacy of naloxone is typically shorter than the opioid it is used to reverse when used to treat an overdose. Re-narcotization is common and repeat doses of naloxone may be required.
Naloxone lasts about 1-1.5 hours in dogs and 0.5-1 hour in cats, therefore in some opioid overdoses naloxone may need to be repeated.
When used to reverse a single appropriate dose of opioid usually only one dose of naloxone is required.
Buprenorphine is a partial mu agonist with an extremely high affinity for the receptor and has slow dissociation kinetics. Reversing this drug with naloxone is very difficult and often requires higher doses and a longer treatment period.
Please address any corrections, questions, or suggestions to: [email protected].
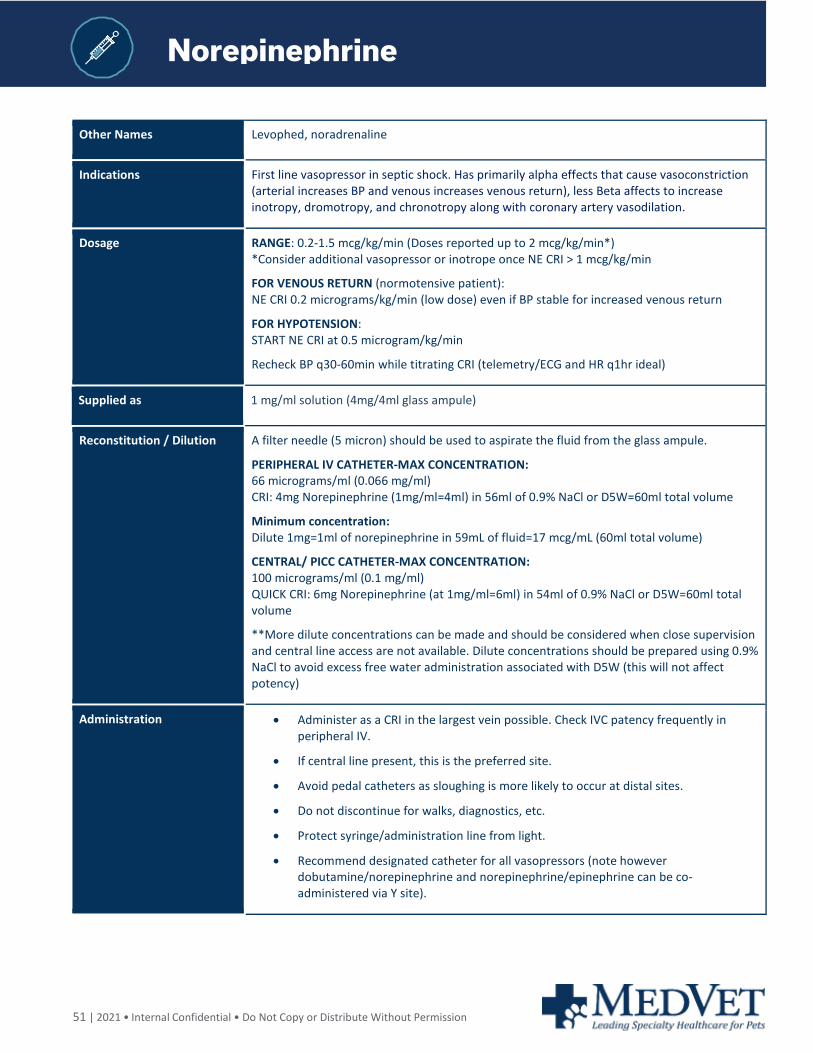
51 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Norepinephrine
Norepinephrine
Norepinephrine
Other Names Levophed, noradrenaline
Indications First line vasopressor in septic shock. Has primarily alpha effects that cause vasoconstriction (arterial increases BP and venous increases venous return), less Beta affects to increase inotropy, dromotropy, and chronotropy along with coronary artery vasodilation.
Dosage RANGE: 0.2-1.5 mcg/kg/min (Doses reported up to 2 mcg/kg/min*) *Consider additional vasopressor or inotrope once NE CRI > 1 mcg/kg/min
FOR VENOUS RETURN (normotensive patient): NE CRI 0.2 micrograms/kg/min (low dose) even if BP stable for increased venous return
FOR HYPOTENSION: START NE CRI at 0.5 microgram/kg/min
Recheck BP q30-60min while titrating CRI (telemetry/ECG and HR q1hr ideal)
Supplied as 1 mg/ml solution (4mg/4ml glass ampule)
Reconstitution / Dilution A filter needle (5 micron) should be used to aspirate the fluid from the glass ampule.
PERIPHERAL IV CATHETER-MAX CONCENTRATION: 66 micrograms/ml (0.066 mg/ml) CRI: 4mg Norepinephrine (1mg/ml=4ml) in 56ml of 0.9% NaCl or D5W=60ml total volume
Minimum concentration: Dilute 1mg=1ml of norepinephrine in 59mL of fluid=17 mcg/mL (60ml total volume)
CENTRAL/ PICC CATHETER-MAX CONCENTRATION: 100 micrograms/ml (0.1 mg/ml) QUICK CRI: 6mg Norepinephrine (at 1mg/ml=6ml) in 54ml of 0.9% NaCl or D5W=60ml total volume
**More dilute concentrations can be made and should be considered when close supervision and central line access are not available. Dilute concentrations should be prepared using 0.9% NaCl to avoid excess free water administration associated with D5W (this will not affect potency)
Administration • Administer as a CRI in the largest vein possible. Check IVC patency frequently in peripheral IV.
• If central line present, this is the preferred site.
• Avoid pedal catheters as sloughing is more likely to occur at distal sites.
• Do not discontinue for walks, diagnostics, etc.
• Protect syringe/administration line from light.
• Recommend designated catheter for all vasopressors (note however dobutamine/norepinephrine and norepinephrine/epinephrine can be co-administered via Y site).
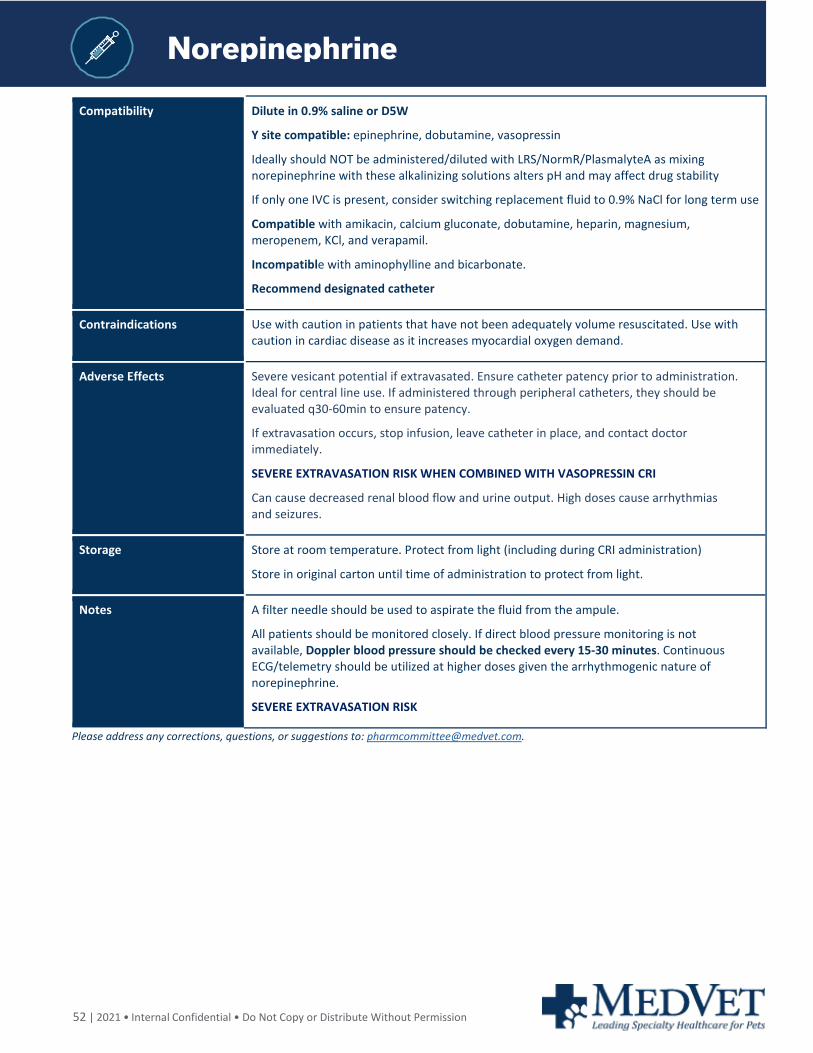
52 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Norepinephrine
Compatibility Dilute in 0.9% saline or D5W
Y site compatible: epinephrine, dobutamine, vasopressin
Ideally should NOT be administered/diluted with LRS/NormR/PlasmalyteA as mixing norepinephrine with these alkalinizing solutions alters pH and may affect drug stability
If only one IVC is present, consider switching replacement fluid to 0.9% NaCl for long term use
Compatible with amikacin, calcium gluconate, dobutamine, heparin, magnesium, meropenem, KCl, and verapamil.
Incompatible with aminophylline and bicarbonate.
Recommend designated catheter
Contraindications Use with caution in patients that have not been adequately volume resuscitated. Use with caution in cardiac disease as it increases myocardial oxygen demand.
Adverse Effects Severe vesicant potential if extravasated. Ensure catheter patency prior to administration. Ideal for central line use. If administered through peripheral catheters, they should be evaluated q30-60min to ensure patency.
If extravasation occurs, stop infusion, leave catheter in place, and contact doctor immediately.
SEVERE EXTRAVASATION RISK WHEN COMBINED WITH VASOPRESSIN CRI
Can cause decreased renal blood flow and urine output. High doses cause arrhythmias and seizures.
Storage Store at room temperature. Protect from light (including during CRI administration)
Store in original carton until time of administration to protect from light.
Notes A filter needle should be used to aspirate the fluid from the ampule.
All patients should be monitored closely. If direct blood pressure monitoring is not available, Doppler blood pressure should be checked every 15-30 minutes. Continuous ECG/telemetry should be utilized at higher doses given the arrhythmogenic nature of norepinephrine.
SEVERE EXTRAVASATION RISK
Please address any corrections, questions, or suggestions to: [email protected].
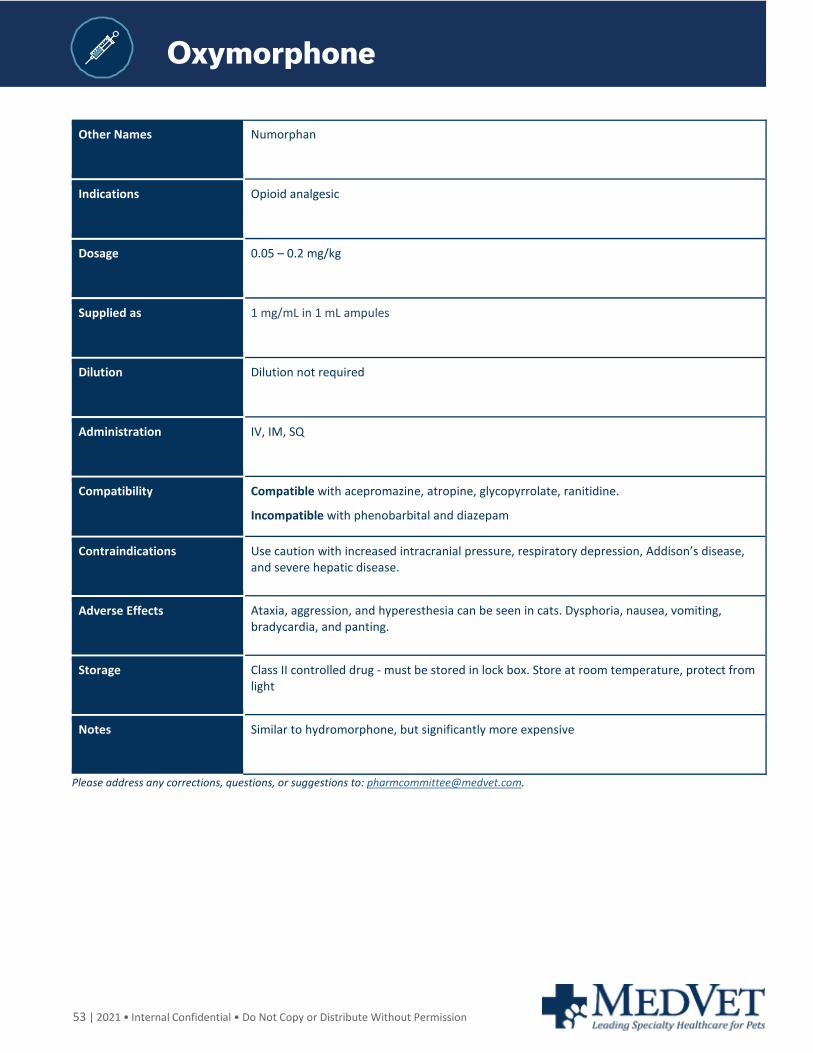
53 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Oxymorphone
Other Names Numorphan
Indications Opioid analgesic
Dosage 0.05 – 0.2 mg/kg
Supplied as 1 mg/mL in 1 mL ampules
Dilution Dilution not required
Administration IV, IM, SQ
Compatibility Compatible with acepromazine, atropine, glycopyrrolate, ranitidine.
Incompatible with phenobarbital and diazepam
Contraindications Use caution with increased intracranial pressure, respiratory depression, Addison’s disease, and severe hepatic disease.
Adverse Effects Ataxia, aggression, and hyperesthesia can be seen in cats. Dysphoria, nausea, vomiting, bradycardia, and panting.
Storage Class II controlled drug - must be stored in lock box. Store at room temperature, protect from light
Notes Similar to hydromorphone, but significantly more expensive
Please address any corrections, questions, or suggestions to: [email protected].
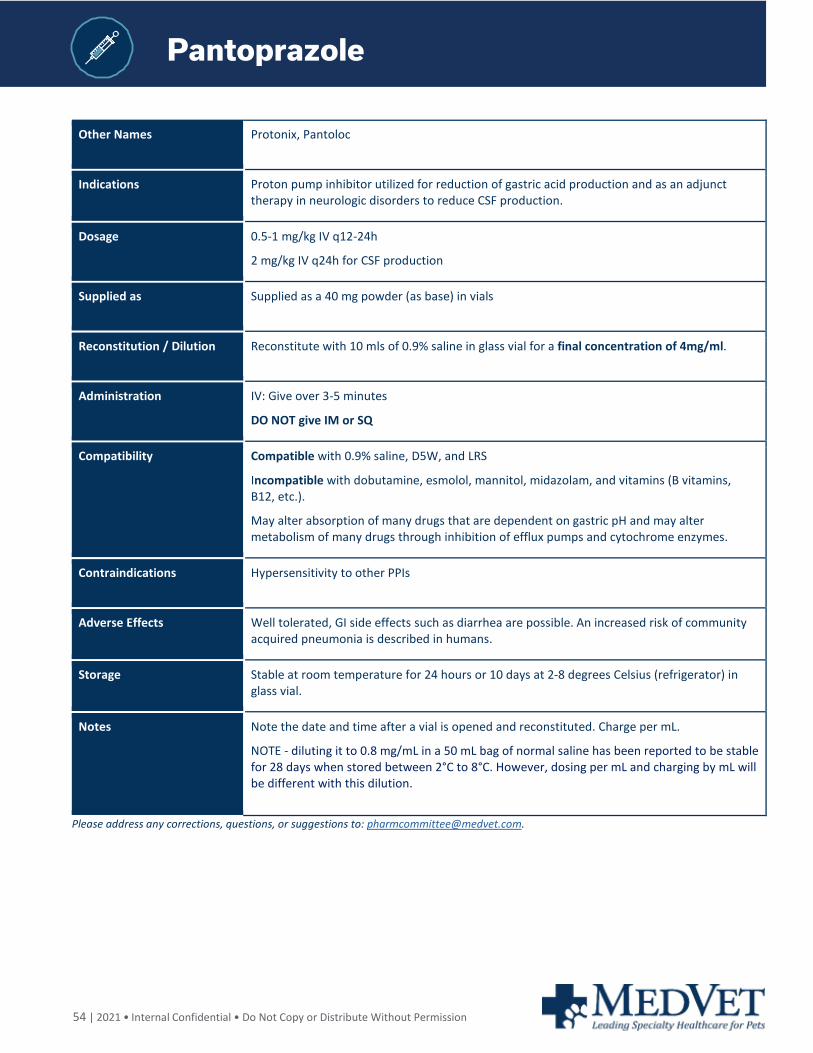
54 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Pantoprazole
Other Names Protonix, Pantoloc
Indications Proton pump inhibitor utilized for reduction of gastric acid production and as an adjunct therapy in neurologic disorders to reduce CSF production.
Dosage 0.5-1 mg/kg IV q12-24h
2 mg/kg IV q24h for CSF production
Supplied as Supplied as a 40 mg powder (as base) in vials
Reconstitution / Dilution Reconstitute with 10 mls of 0.9% saline in glass vial for a final concentration of 4mg/ml.
Administration IV: Give over 3-5 minutes
DO NOT give IM or SQ
Compatibility Compatible with 0.9% saline, D5W, and LRS
Incompatible with dobutamine, esmolol, mannitol, midazolam, and vitamins (B vitamins, B12, etc.).
May alter absorption of many drugs that are dependent on gastric pH and may alter metabolism of many drugs through inhibition of efflux pumps and cytochrome enzymes.
Contraindications Hypersensitivity to other PPIs
Adverse Effects Well tolerated, GI side effects such as diarrhea are possible. An increased risk of community acquired pneumonia is described in humans.
Storage Stable at room temperature for 24 hours or 10 days at 2-8 degrees Celsius (refrigerator) in glass vial.
Notes Note the date and time after a vial is opened and reconstituted. Charge per mL.
NOTE - diluting it to 0.8 mg/mL in a 50 mL bag of normal saline has been reported to be stable for 28 days when stored between 2°C to 8°C. However, dosing per mL and charging by mL will be different with this dilution.
Please address any corrections, questions, or suggestions to: [email protected].
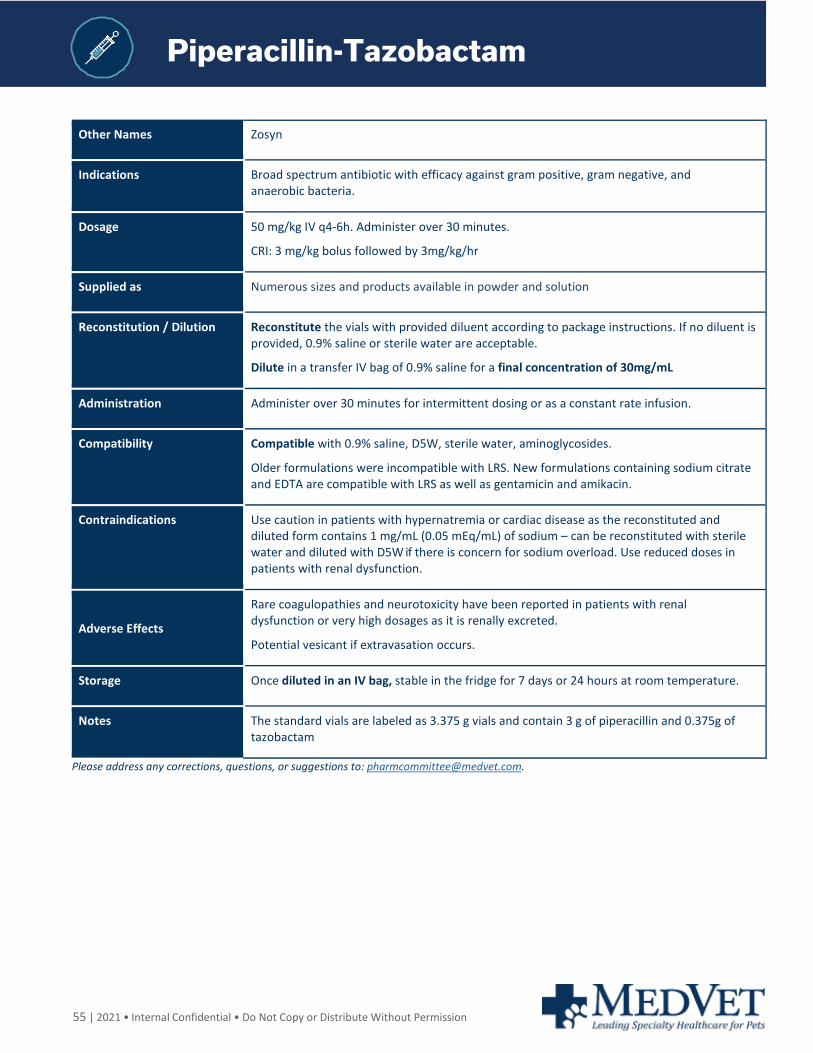
55 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Piperacillin-Tazobactam
Other Names Zosyn
Indications Broad spectrum antibiotic with efficacy against gram positive, gram negative, and anaerobic bacteria.
Dosage 50 mg/kg IV q4-6h. Administer over 30 minutes.
CRI: 3 mg/kg bolus followed by 3mg/kg/hr
Supplied as Numerous sizes and products available in powder and solution
Reconstitution / Dilution Reconstitute the vials with provided diluent according to package instructions. If no diluent is provided, 0.9% saline or sterile water are acceptable.
Dilute in a transfer IV bag of 0.9% saline for a final concentration of 30mg/mL
Administration Administer over 30 minutes for intermittent dosing or as a constant rate infusion.
Compatibility Compatible with 0.9% saline, D5W, sterile water, aminoglycosides.
Older formulations were incompatible with LRS. New formulations containing sodium citrate and EDTA are compatible with LRS as well as gentamicin and amikacin.
Contraindications Use caution in patients with hypernatremia or cardiac disease as the reconstituted and diluted form contains 1 mg/mL (0.05 mEq/mL) of sodium – can be reconstituted with sterile water and diluted with D5W if there is concern for sodium overload. Use reduced doses in patients with renal dysfunction.
Adverse Effects
Rare coagulopathies and neurotoxicity have been reported in patients with renal dysfunction or very high dosages as it is renally excreted.
Potential vesicant if extravasation occurs.
Storage Once diluted in an IV bag, stable in the fridge for 7 days or 24 hours at room temperature.
Notes The standard vials are labeled as 3.375 g vials and contain 3 g of piperacillin and 0.375g of tazobactam
Please address any corrections, questions, or suggestions to: [email protected].
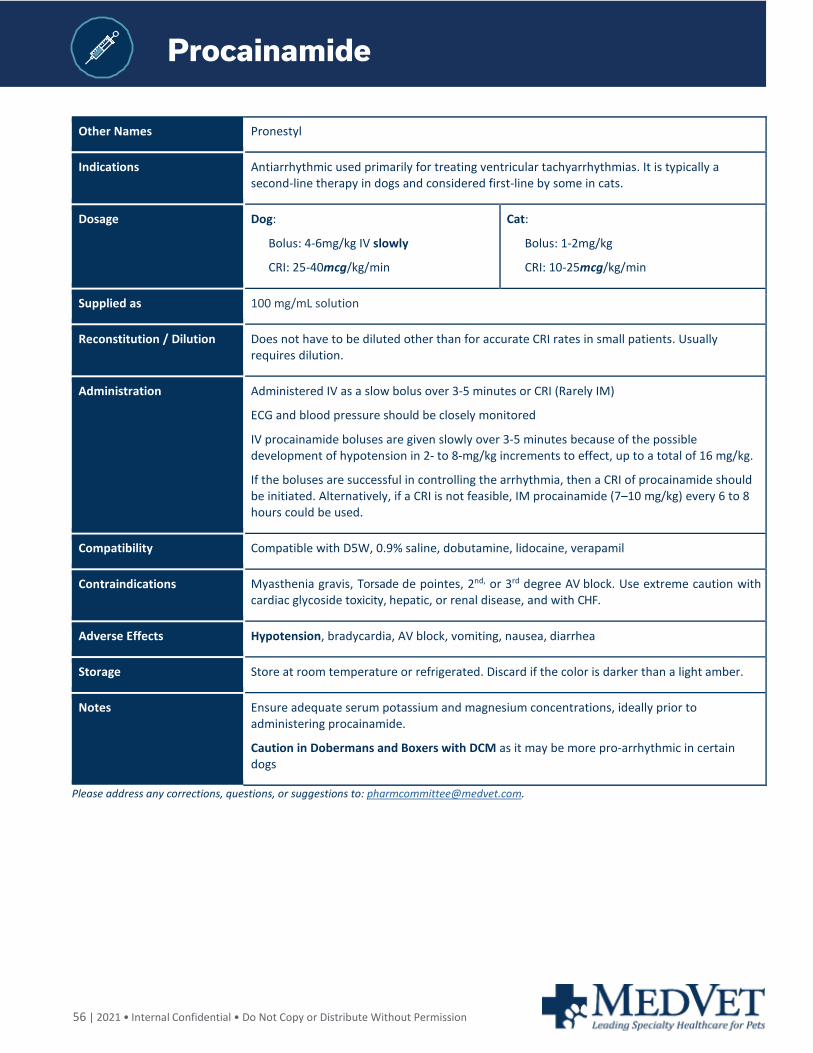
56 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Procainamide
Other Names Pronestyl
Indications Antiarrhythmic used primarily for treating ventricular tachyarrhythmias. It is typically a second-line therapy in dogs and considered first-line by some in cats.
Dosage Dog:
Bolus: 4-6mg/kg IV slowly
CRI: 25-40mcg/kg/min
Cat:
Bolus: 1-2mg/kg
CRI: 10-25mcg/kg/min
Supplied as 100 mg/mL solution
Reconstitution / Dilution Does not have to be diluted other than for accurate CRI rates in small patients. Usually requires dilution.
Administration Administered IV as a slow bolus over 3-5 minutes or CRI (Rarely IM)
ECG and blood pressure should be closely monitored
IV procainamide boluses are given slowly over 3-5 minutes because of the possible development of hypotension in 2- to 8-mg/kg increments to effect, up to a total of 16 mg/kg.
If the boluses are successful in controlling the arrhythmia, then a CRI of procainamide should be initiated. Alternatively, if a CRI is not feasible, IM procainamide (7–10 mg/kg) every 6 to 8 hours could be used.
Compatibility Compatible with D5W, 0.9% saline, dobutamine, lidocaine, verapamil
Contraindications Myasthenia gravis, Torsade de pointes, 2nd, or 3rd degree AV block. Use extreme caution with cardiac glycoside toxicity, hepatic, or renal disease, and with CHF.
Adverse Effects Hypotension, bradycardia, AV block, vomiting, nausea, diarrhea
Storage Store at room temperature or refrigerated. Discard if the color is darker than a light amber.
Notes Ensure adequate serum potassium and magnesium concentrations, ideally prior to administering procainamide.
Caution in Dobermans and Boxers with DCM as it may be more pro-arrhythmic in certain dogs
Please address any corrections, questions, or suggestions to: [email protected].
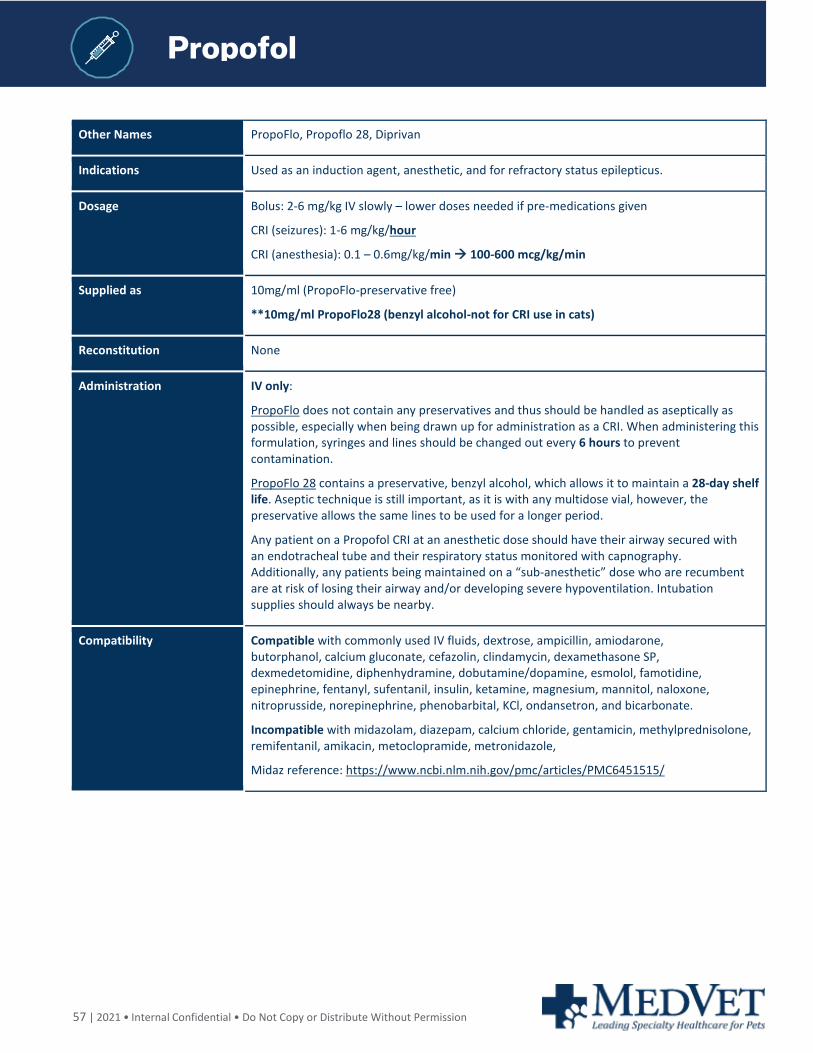
57 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Propofol
Other Names PropoFlo, Propoflo 28, Diprivan
Indications Used as an induction agent, anesthetic, and for refractory status epilepticus.
Dosage Bolus: 2-6 mg/kg IV slowly – lower doses needed if pre-medications given
CRI (seizures): 1-6 mg/kg/hour
CRI (anesthesia): 0.1 – 0.6mg/kg/min 100-600 mcg/kg/min
Supplied as 10mg/ml (PropoFlo-preservative free)
**10mg/ml PropoFlo28 (benzyl alcohol-not for CRI use in cats)
Reconstitution None
Administration IV only:
PropoFlo does not contain any preservatives and thus should be handled as aseptically as possible, especially when being drawn up for administration as a CRI. When administering this formulation, syringes and lines should be changed out every 6 hours to prevent contamination.
PropoFlo 28 contains a preservative, benzyl alcohol, which allows it to maintain a 28-day shelf life. Aseptic technique is still important, as it is with any multidose vial, however, the preservative allows the same lines to be used for a longer period.
Any patient on a Propofol CRI at an anesthetic dose should have their airway secured with an endotracheal tube and their respiratory status monitored with capnography. Additionally, any patients being maintained on a “sub-anesthetic” dose who are recumbent are at risk of losing their airway and/or developing severe hypoventilation. Intubation supplies should always be nearby.
Compatibility Compatible with commonly used IV fluids, dextrose, ampicillin, amiodarone, butorphanol, calcium gluconate, cefazolin, clindamycin, dexamethasone SP, dexmedetomidine, diphenhydramine, dobutamine/dopamine, esmolol, famotidine, epinephrine, fentanyl, sufentanil, insulin, ketamine, magnesium, mannitol, naloxone, nitroprusside, norepinephrine, phenobarbital, KCl, ondansetron, and bicarbonate.
Incompatible with midazolam, diazepam, calcium chloride, gentamicin, methylprednisolone, remifentanil, amikacin, metoclopramide, metronidazole,
Midaz reference: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6451515/

58 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Propofol
Contraindications Avoid in neonatal patients as Propofol causes vasodilation and blunts the baroreceptor-mediated increase in heart rate to compensate.
Avoid in patients with severe cardiac disease where negative inotropy cannot be tolerated – DCM, severe mitral/tricuspid degeneration.
Do not use as an induction agent in patients prior to splenectomy.
Avoid in patients where apnea cannot be tolerated – patients with known pulmonary bullae, difficult intubation risk, etc.
Notes: The PropoFlo 28 formulation is not labeled for use in cats due to the preservative, benzyl alcohol, which can have toxic effects. Cats lack adequate glucuronic acid conjugation, which results in a decreased rate of metabolism and cumulative toxic effects such as ataxia, hyperesthesia, fasciculations, blindness, aggression, convulsions, respiratory failure, and death. The original propofol without the benzyl alcohol is recommended for CRI use in cats.
Adverse Effects Potent respiratory depressant, bradycardia, hypotension, splenic engorgement, myoclonus.
Monitor ventilation/oxygenation closely. Hypotension occurs commonly at higher doses. Seizure-like clinical signs may occur during induction.
Storage Propoflo: 6 hours once opened
Propoflo 28: 28 days after initial puncture
Storage and Handling: Propoflo 28 - Multi-use vial at 10 mg/mL and is an emulsion. It is labeled for IV use in dogs. Shake the vial before opening. Date when the vial was opened so it can be discarded by 28 days if it has not been used. Refrigeration is not recommended
Notes Propoflo 28 is not labeled for cats because it contains the preservative benzyl alcohol, which may be toxic to cats. However, single use as an induction agent has been shown to be safe in healthy populations of cats.
Repeat use of preservative free Propofol in cats has been implicated as causing hemolytic anemia, however, this has been disproven in studies recently.
Please address any corrections, questions, or suggestions to: [email protected].
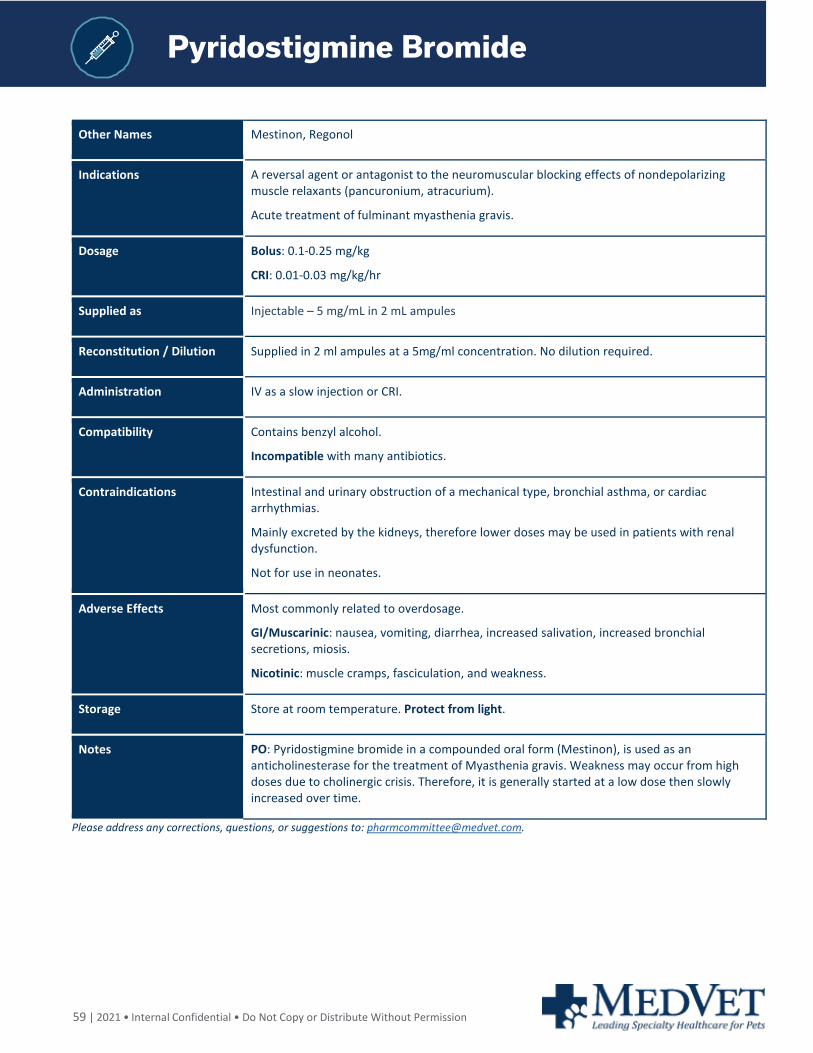
59 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Pyridostigmine Bromide
Other Names Mestinon, Regonol
Indications A reversal agent or antagonist to the neuromuscular blocking effects of nondepolarizing muscle relaxants (pancuronium, atracurium).
Acute treatment of fulminant myasthenia gravis.
Dosage Bolus: 0.1-0.25 mg/kg
CRI: 0.01-0.03 mg/kg/hr
Supplied as Injectable – 5 mg/mL in 2 mL ampules
Reconstitution / Dilution Supplied in 2 ml ampules at a 5mg/ml concentration. No dilution required.
Administration IV as a slow injection or CRI.
Compatibility Contains benzyl alcohol.
Incompatible with many antibiotics.
Contraindications Intestinal and urinary obstruction of a mechanical type, bronchial asthma, or cardiac arrhythmias.
Mainly excreted by the kidneys, therefore lower doses may be used in patients with renal dysfunction.
Not for use in neonates.
Adverse Effects Most commonly related to overdosage.
GI/Muscarinic: nausea, vomiting, diarrhea, increased salivation, increased bronchial secretions, miosis.
Nicotinic: muscle cramps, fasciculation, and weakness.
Storage Store at room temperature. Protect from light.
Notes PO: Pyridostigmine bromide in a compounded oral form (Mestinon), is used as an anticholinesterase for the treatment of Myasthenia gravis. Weakness may occur from high doses due to cholinergic crisis. Therefore, it is generally started at a low dose then slowly increased over time.
Please address any corrections, questions, or suggestions to: [email protected].
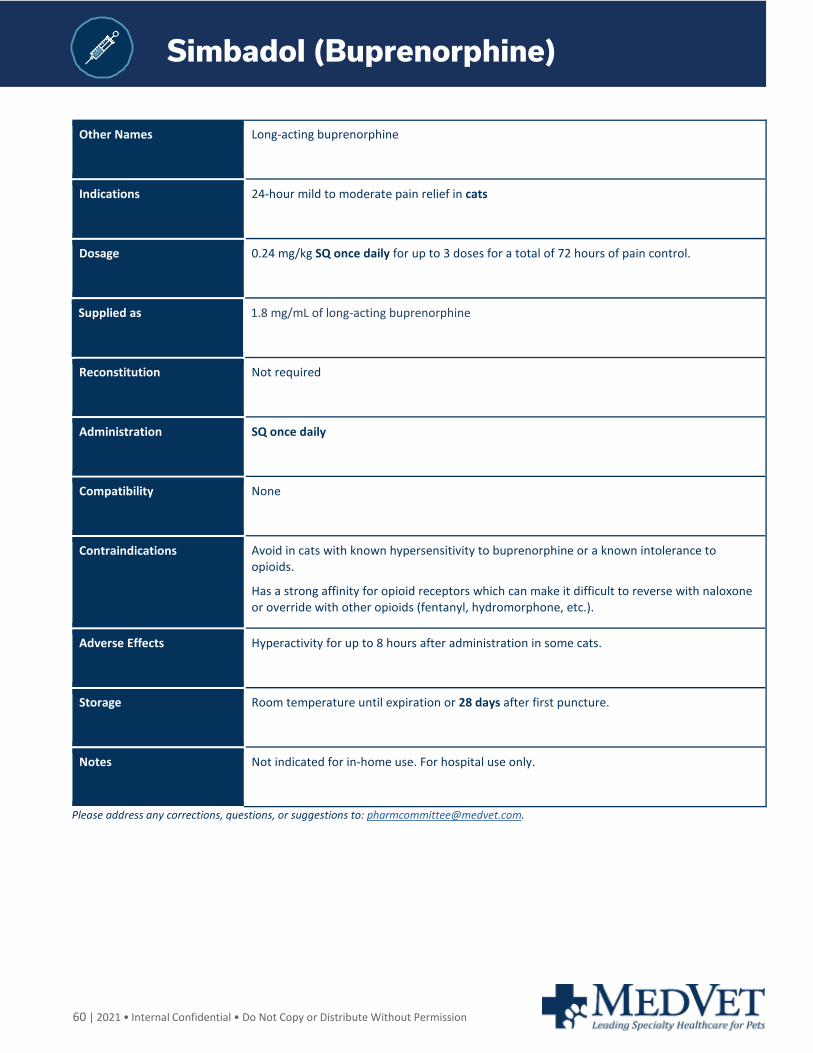
60 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Simbadol (Buprenorphine)
Other Names Long-acting buprenorphine
Indications 24-hour mild to moderate pain relief in cats
Dosage 0.24 mg/kg SQ once daily for up to 3 doses for a total of 72 hours of pain control.
Supplied as 1.8 mg/mL of long-acting buprenorphine
Reconstitution Not required
Administration SQ once daily
Compatibility None
Contraindications Avoid in cats with known hypersensitivity to buprenorphine or a known intolerance to opioids.
Has a strong affinity for opioid receptors which can make it difficult to reverse with naloxone or override with other opioids (fentanyl, hydromorphone, etc.).
Adverse Effects Hyperactivity for up to 8 hours after administration in some cats.
Storage Room temperature until expiration or 28 days after first puncture.
Notes Not indicated for in-home use. For hospital use only.
Please address any corrections, questions, or suggestions to: [email protected].
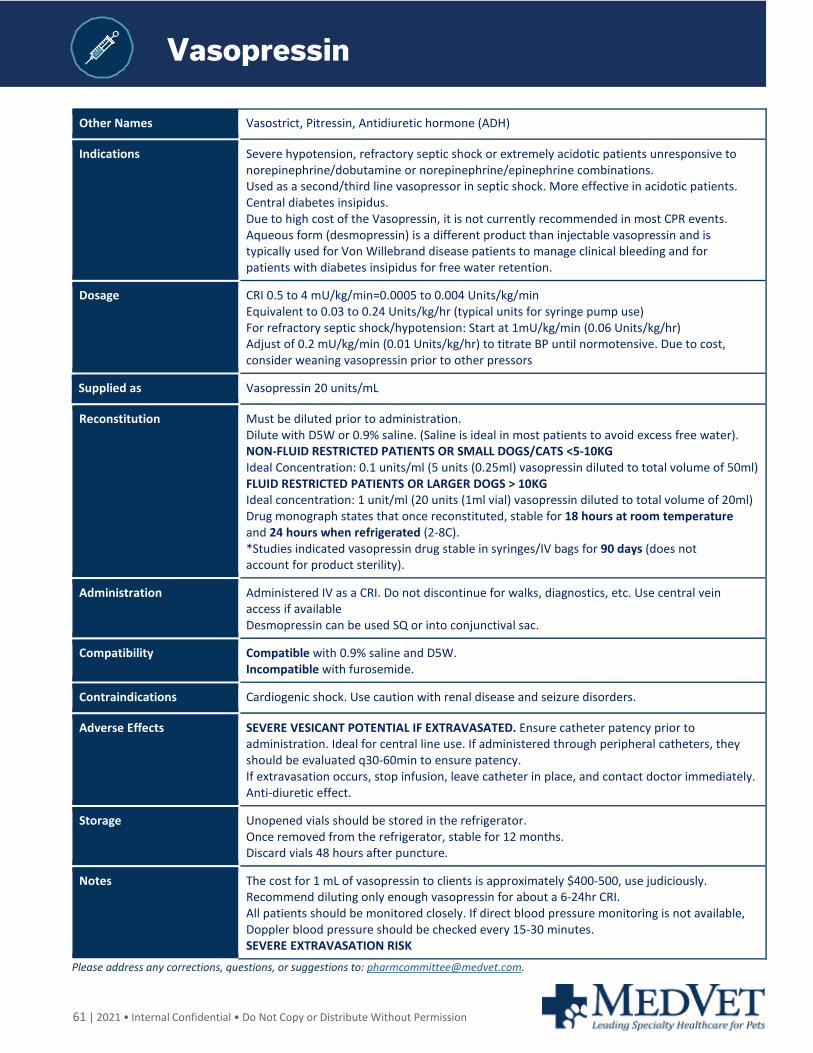
61 | 2021 • Internal Confidential • Do Not Copy or Distribute Without Permission
Vasopressin
Other Names Vasostrict, Pitressin, Antidiuretic hormone (ADH)
Indications Severe hypotension, refractory septic shock or extremely acidotic patients unresponsive to norepinephrine/dobutamine or norepinephrine/epinephrine combinations. Used as a second/third line vasopressor in septic shock. More effective in acidotic patients. Central diabetes insipidus. Due to high cost of the Vasopressin, it is not currently recommended in most CPR events. Aqueous form (desmopressin) is a different product than injectable vasopressin and is typically used for Von Willebrand disease patients to manage clinical bleeding and for patients with diabetes insipidus for free water retention.
Dosage CRI 0.5 to 4 mU/kg/min=0.0005 to 0.004 Units/kg/min Equivalent to 0.03 to 0.24 Units/kg/hr (typical units for syringe pump use) For refractory septic shock/hypotension: Start at 1mU/kg/min (0.06 Units/kg/hr) Adjust of 0.2 mU/kg/min (0.01 Units/kg/hr) to titrate BP until normotensive. Due to cost, consider weaning vasopressin prior to other pressors
Supplied as Vasopressin 20 units/mL
Reconstitution Must be diluted prior to administration. Dilute with D5W or 0.9% saline. (Saline is ideal in most patients to avoid excess free water). NON-FLUID RESTRICTED PATIENTS OR SMALL DOGS/CATS <5-10KG Ideal Concentration: 0.1 units/ml (5 units (0.25ml) vasopressin diluted to total volume of 50ml) FLUID RESTRICTED PATIENTS OR LARGER DOGS > 10KG Ideal concentration: 1 unit/ml (20 units (1ml vial) vasopressin diluted to total volume of 20ml) Drug monograph states that once reconstituted, stable for 18 hours at room temperature and 24 hours when refrigerated (2-8C). *Studies indicated vasopressin drug stable in syringes/IV bags for 90 days (does not account for product sterility).
Administration Administered IV as a CRI. Do not discontinue for walks, diagnostics, etc. Use central vein access if available Desmopressin can be used SQ or into conjunctival sac.
Compatibility Compatible with 0.9% saline and D5W. Incompatible with furosemide.
Contraindications Cardiogenic shock. Use caution with renal disease and seizure disorders.
Adverse Effects SEVERE VESICANT POTENTIAL IF EXTRAVASATED. Ensure catheter patency prior to administration. Ideal for central line use. If administered through peripheral catheters, they should be evaluated q30-60min to ensure patency. If extravasation occurs, stop infusion, leave catheter in place, and contact doctor immediately. Anti-diuretic effect.
Storage Unopened vials should be stored in the refrigerator. Once removed from the refrigerator, stable for 12 months. Discard vials 48 hours after puncture.
Notes The cost for 1 mL of vasopressin to clients is approximately $400-500, use judiciously. Recommend diluting only enough vasopressin for about a 6-24hr CRI. All patients should be monitored closely. If direct blood pressure monitoring is not available, Doppler blood pressure should be checked every 15-30 minutes. SEVERE EXTRAVASATION RISK
Please address any corrections, questions, or suggestions to: [email protected].