medical coding specialist - u.s. career institute
TRANSCRIPT

Medical CodingSpecialistInstruction Pack 2 Lessons 7-11
Explore the possibilities 0201604LB02A-14


Medical Coding Specialist
Instruction Pack 2
Lesson 7—Ethics and Legal IssuesLesson 8—Introduction to Anatomy Lesson 9—Anatomy: Landmarks
and DivisionsLesson 10—Cell and Tissue Anatomy
and PathologyLesson 11—Diagnostic Coding 101
No part of this document may be reproduced or transmitted in any form or by any means, electronic or mechanical, for any purpose, without the express written permission of U.S. Career Institute.
Copyright © 2013, Weston Distance Learning, Inc. All Rights Reserved. 0201604LB02A-14
AcknowledgmentsAuthorsKaty LittleBrenda Blomberg
Editorial StaffTrish BowenKimberly FieldsKathy DeVaultKelly BrownJoyce JeckewiczStephanie MacLeodCarrie Williams
Design/LayoutConnie HunsaderSandy PetersenD. Brent Hauseman
U.S. Career InstituteFort Collins, CO 80525
www.uscareerinstitute.edu

0201604LB02A-14 III
Table of Contents
Lesson 7: Ethics and Legal IssuesStep 1: Learning Objectives for Lesson 7...................................................................................................................... 1Step 2: Lesson Preview .................................................................................................................................................... 1Step 3: Confidentiality .................................................................................................................................................... 1
Guidelines for Confidentiality of Medical Records ..................................................................................... 2Guidelines for Faxing Medical Records ......................................................................................................... 2
Step 4: Medical Ethics ..................................................................................................................................................... 3Step 5: Health Insurance Portability and Accountability Act ...........................................................................................5
Covered Entities ................................................................................................................................................ 5Transaction and Code Sets Standards ............................................................................................................ 6Privacy Rule ....................................................................................................................................................... 7Security Rule ................................................................................................................................................... 10Unique Identifier Standard ............................................................................................................................ 11Breach of Privacy ............................................................................................................................................ 12Office for Civil Rights .................................................................................................................................... 13HIPAA Privacy & Security Rule Complaint Process ................................................................................. 13
Step 6: Practice Exercise 7-1 ......................................................................................................................................... 14Step 7: Review Practice Exercise 7-1 ........................................................................................................................... 15Step 8: Fraud and Abuse ............................................................................................................................................... 15
Preventing Fraud and Abuse ......................................................................................................................... 16Consequences of Committing Fraud ........................................................................................................... 16
Step 9: Liability Insurance ............................................................................................................................................ 17Insurance Audits ............................................................................................................................................. 17
Step 10: Recovery Audit Contractors .......................................................................................................................... 18Step 11: Legal Concerns ................................................................................................................................................ 18
Subpoenas ........................................................................................................................................................ 19Arbitration ....................................................................................................................................................... 19Medical Testimony ......................................................................................................................................... 19
Step 12: Practice Exercise 7-2 ...................................................................................................................................... 20Step 13: Review Practice Exercise 7-2 ......................................................................................................................... 20Step 14: Lesson Summary ............................................................................................................................................. 20Step 15: Quiz 7 ............................................................................................................................................................... 21
Endnotes .......................................................................................................................................................... 21

0201604LB02A-14
Medical Coding Specialist
IV
Lesson 8: Introduction to AnatomyStep 1: Learning Objectives for Lesson 8...................................................................................................................... 1Step 2: Lesson Preview .................................................................................................................................................... 1Step 3: Human Biology ................................................................................................................................................... 2
Anatomy ............................................................................................................................................................ 2Physiology.......................................................................................................................................................... 3
Step 4: Pathology ............................................................................................................................................................. 4How Anatomy, Physiology and Pathology Relate ........................................................................................ 5
Step 5: Practice Exercise 8-1 .......................................................................................................................................... 6Step 6: Review Practice Exercise 8-1 ............................................................................................................................. 6Step 7: Beginning Anatomy and Physiology Concepts .............................................................................................. 6
The Anatomic Position .................................................................................................................................... 7Planes and Sections of the Human Body ....................................................................................................... 8Transverse Planes and Sections ...................................................................................................................... 8Sagittal Planes and Sections ............................................................................................................................ 9Coronal Planes and Sections ........................................................................................................................... 9Planes and Sections ........................................................................................................................................ 10
Step 8: Practice Exercise 8-2 ......................................................................................................................................... 11Step 9: Review Practice Exercise 8-2 ........................................................................................................................... 11Step 10: Location Terms ............................................................................................................................................... 11Step 11: Pronounce New Terms ................................................................................................................................... 17Step 12: Write New Terms ............................................................................................................................................ 18Step 13: Meanings of New Terms ............................................................................................................................... 18Step 14: Organ and Organ Systems ............................................................................................................................. 18
Respiratory System ......................................................................................................................................... 19Circulatory/Cardiovascular System ............................................................................................................. 19Nervous System .............................................................................................................................................. 19Muscular System ............................................................................................................................................. 19Skeletal System ................................................................................................................................................ 19Integumentary System ................................................................................................................................... 20Endocrine System ........................................................................................................................................... 20Digestive System ............................................................................................................................................. 20Urinary System ............................................................................................................................................... 20Reproductive System ...................................................................................................................................... 20The Immune System ...................................................................................................................................... 20
Step 15: Practice Exercise 8-3 ...................................................................................................................................... 21Step 16: Review Practice Exercise 8-3 ......................................................................................................................... 21Step 17: Lesson Summary ............................................................................................................................................. 21Step 18: Quiz 8 ............................................................................................................................................................... 22

0201604LB02A-14
Table of Contents
V
Lesson 9: Anatomy: Landmarks and DivisionsStep 1: Learning Objectives for Lesson 9...................................................................................................................... 1Step 2: Lesson Preview .................................................................................................................................................... 1Step 3: Gross Anatomy .................................................................................................................................................... 1
Landmarks and Divisions ................................................................................................................................ 1Step 4: Pronounce New Terms ....................................................................................................................................... 5Step 5: Write New Terms ............................................................................................................................................... 5Step 6: Meanings of New Terms .................................................................................................................................... 5Step 7: Adjective Forms for Landmark Names ............................................................................................................ 6Step 8: Practice Exercise 9-1 .......................................................................................................................................... 7Step 9: Review Practice Exercise 9-1 ............................................................................................................................. 8Step 10: Divisions of the Abdomen ............................................................................................................................... 8
An Alternative Division of the Abdomen ..................................................................................................... 9Step 11: Practice Exercise 9-2 ...................................................................................................................................... 10Step 12: Review Practice Exercise 9-2 ......................................................................................................................... 11Step 13: Internal Landmarks: The Body Cavities ...................................................................................................... 11Step 14: Membranes That Line the Body Cavities .................................................................................................... 13
Epithelial Tissue Membranes ........................................................................................................................ 13Connective Tissue Membranes ..................................................................................................................... 14
Step 15: Retroperitoneal Organs .................................................................................................................................. 14Step 16: Pronounce New Terms ................................................................................................................................... 15Step 17: Write New Terms ............................................................................................................................................ 15Step 18: Meanings of New Terms ................................................................................................................................ 15Step 19: Organization of the Body .............................................................................................................................. 16Step 20: Practice Exercise 9-3 ...................................................................................................................................... 17Step 21: Review Practice Exercise 9-3 ......................................................................................................................... 17Step 22: Lesson Summary ............................................................................................................................................. 17Step 23: Quiz 9 ............................................................................................................................................................... 18Just for Fun ..................................................................................................................................................................... 18
Lesson 10: Cell and Tissue Anatomy and PathologyStep 1: Learning Objectives for Lesson 10 ................................................................................................................... 1Step 2: Lesson Preview .................................................................................................................................................... 1Step 3: Cell Components and Their Primary Functions ............................................................................................ 1
Cell Membrane.................................................................................................................................................. 2Cilia .................................................................................................................................................................... 3Flagella ............................................................................................................................................................... 3Villi ..................................................................................................................................................................... 3
Step 4: More Cell Components and Their Functions ................................................................................................. 3Cytoplasm .......................................................................................................................................................... 3
0201604LB02A-14
Medical Coding Specialist
VI
Step 5: The Nucleus ......................................................................................................................................................... 5DNA ................................................................................................................................................................... 5RNA .................................................................................................................................................................... 6Nucleoli .............................................................................................................................................................. 6
Step 6: Practice Exercise 10-1 ........................................................................................................................................ 6Step 7: Review Practice Exercise 10-1 ........................................................................................................................... 8Step 8: Pronounce New Terms ....................................................................................................................................... 8Step 9: Write New Terms ............................................................................................................................................... 8Step 10: Meanings of New Terms .................................................................................................................................. 9Step 11: Cell Pathology ................................................................................................................................................... 9Step 12: Etiologies ............................................................................................................................................................ 9
Developmental Abnormality ......................................................................................................................... 10Inflammatory Disease .................................................................................................................................... 10Hyperplasia and Neoplasia ............................................................................................................................ 10Metabolic Disease ........................................................................................................................................... 11Vascular Disease ............................................................................................................................................. 11Immunologic Disease..................................................................................................................................... 11Idiopathic Abnormality ................................................................................................................................. 11Iatrogenic Abnormality .................................................................................................................................. 11Nosocomial Disease ....................................................................................................................................... 12
Step 13: Cell Damage .................................................................................................................................................... 12Hypoxia and Anoxia ..................................................................................................................................... 12Toxic Agents ................................................................................................................................................... 12Microbial Infection ........................................................................................................................................ 13Allergic/Immune Reactions .......................................................................................................................... 13Metabolic and Genetic Disturbances .......................................................................................................... 13
Step 14: Practice Exercise 10-2 .................................................................................................................................... 14Step 15: Review Practice Exercise 10-2 ....................................................................................................................... 15Step 16: Cell Response ................................................................................................................................................. 15
Atrophy ........................................................................................................................................................... 16Hypertrophy ................................................................................................................................................... 16Hyperplasia ..................................................................................................................................................... 17Metaplasia ........................................................................................................................................................ 18Intracellular Accumulations ......................................................................................................................... 18Aging ............................................................................................................................................................... 18
Step 17: Practice Exercise 10-3 .................................................................................................................................... 18Step 18: Review Practice Exercise 10-3 ....................................................................................................................... 20Step 19: Tissue Response .............................................................................................................................................. 20
Inflammation .................................................................................................................................................. 21Repair ............................................................................................................................................................... 22Damage or Death ............................................................................................................................................ 23

0201604LB02A-14
Table of Contents
VII
Step 20: Pronounce New Terms ................................................................................................................................... 24Step 21: Write New Terms ............................................................................................................................................ 24Step 22: Meanings of New Terms ................................................................................................................................ 25Step 23: Practice Exercise 10-4 .................................................................................................................................... 25Step 24: Review Practice Exercise 10-4 ....................................................................................................................... 26Step 25: Lesson Summary ............................................................................................................................................. 27Step 26: Quiz 10 ............................................................................................................................................................. 27
Lesson 11: Diagnostic Coding 101Step 1: Learning Objectives for Lesson 11 ................................................................................................................... 1Step 2: Lesson Preview .................................................................................................................................................... 1Step 3: History of the International Classification of Diseases ........................................................................................1
The WHO .......................................................................................................................................................... 2ICD-10 ............................................................................................................................................................... 2
Step 4: Practice Exercise 11-1 ........................................................................................................................................ 3Step 5: Review Practice Exercise 11-1 ........................................................................................................................... 3Step 6: Contents of the ICD-10-CM ............................................................................................................................. 3
Conventions for the ICD-10-CM ..................................................................................................................... 4General Coding Guidelines ............................................................................................................................... 4Chapter-Specific Guidelines .............................................................................................................................. 4Alphabetic Index to Diseases ........................................................................................................................... 4Tabular List of Diseases and Injuries ............................................................................................................... 6
Step 7: Practice Exercise 11-2 ........................................................................................................................................ 7Step 8: Review Practice Exercise 11-2 ........................................................................................................................... 7Step 9: Lesson Summary ................................................................................................................................................. 8Step 10: Quiz 11 ............................................................................................................................................................... 8
Endnotes ............................................................................................................................................................ 8
Answer KeyLesson 7 ............................................................................................................................................................................ 1
Practice Exercise 7-1 ........................................................................................................................................ 1Practice Exercise 7-2 ........................................................................................................................................ 2
Lesson 8 ............................................................................................................................................................................ 3Practice Exercise 8-1 ........................................................................................................................................ 3Practice Exercise 8-2 ........................................................................................................................................ 4Practice Exercise 8-3 ........................................................................................................................................ 4
Lesson 9 ............................................................................................................................................................................ 5Practice Exercise 9-1 ........................................................................................................................................ 5Practice Exercise 9-2 ........................................................................................................................................ 6Practice Exercise 9-3 ........................................................................................................................................ 7
0201604LB02A-14
Medical Coding Specialist
VIII
Lesson 10 .......................................................................................................................................................................... 8Practice Exercise 10-1 ...................................................................................................................................... 8Practice Exercise 10-2 ...................................................................................................................................... 8Practice Exercise 10-3 ...................................................................................................................................... 9Practice Exercise 10-4 .................................................................................................................................... 10
Lesson 11 ........................................................................................................................................................................ 11Practice Exercise 11-1 .................................................................................................................................... 11Practice Exercise 11-2 .................................................................................................................................... 11
Lesson 7Ethics and Legal Issues
Step 1: Learning Objectives for Lesson 7When you have completed the instruction in this lesson, you will be trained to:
● Explain the importance of confidentiality in the healthcare profession.
● Describe the concept of ethics.
● Outline the main purposes of the federal HIPAA regulations.
● Explain fraud, and determine some common fraudulent situations that you must avoid.
● Explain the development of and need for Recovery Audit Contractors.
● Discuss the basic ideas surrounding liability and malpractice, including insurance coverage.
Step 2: Lesson PreviewLegal issues that affect medical coding specialists include confidentiality and ethics—concepts you need to keep in mind always. No matter how well you do your job, you must also be ethical. A big part of that code of ethics is ensuring that a patient’s private health information remains private.
Patients depend on workers in the healthcare field to protect their privacy from creditors, employers, insurers and others. If an employer learns of a potential employee’s family history of diabetes, would the employer refuse to hire the person? Would a life insurance company that learned of a client’s transfer to hospice care find a loophole to terminate coverage? Questions like these are certainly on the minds of many people today.
Step 3: ConfidentialityDo you remember the last time that you went to the doctor? Even if it was just a regular checkup, you wouldn’t want your doctor to discuss your appointment at dinner with his friends, would you? As a healthcare professional, you have access to many medical records. It is essential that you understand that these records are confidential.

0201604LB02A-07-14
Medical Coding Specialist
7-2
When something is confidential, it means that it is kept secret. Confidentiality goes hand in hand with ethics, which will be detailed shortly. You have learned a bit about medical records, and you’ve probably guessed that because of their sensitivity, these records are confidential. That means you can only release them to authorized persons. A medical facility must consider a wide range of factors to ensure confidentiality of patient records. These factors include:
● hiring trustworthy, responsible staff;
● ensuring information stored on computerized systems is secure and available only to authorized individuals; and
● having standardized, secured procedures in place for transferring patient information within the facility, between facilities and to outside individuals.
Guidelines for Confidentiality of Medical RecordsBeginning with the people it employs, a hospital, physician’s office or other healthcare facility must ensure that sensitive patient information is only accessible to reliable people. It’s important that all the policies and procedures that relate to confidentiality and release of all medical records be written down and available for reference.
Review the following security procedures that help ensure confidentiality of medical records and information:
● Employees are prohibited from working on records of acquaintances.
● New employees are required to sign confidentiality pledges before they can access confidential information, and a system must be in place to ensure that such statements are signed.
● Security procedures are in place for accessing medical record storage areas that aren’t under continuous supervision by authorized staff.
● All computerized patient information must only be accessible with a unique password, and information system users must not share their passwords.
● A written plan is developed to deal with suspected breaches of confidentiality.
● All physicians who use the computer system should agree, in writing, to keep their ID codes confidential and be responsible for authenticating their dictation.
Guidelines for Faxing Medical RecordsIn addition to following the guidelines previously mentioned, it is important to guard against unauthorized access to records in situations where a fax machine is used. Even if the information is sent to an authorized person, it is possible for someone else to receive the information. Procedures that help ensure the confidentiality of faxed medical records include the following:
● Always follow the rules set out by the provider or client with whom you are working. If there is a policy that prohibits sending records by fax, then do not do it. If there are no such restrictions, follow the next guideline.

0201604LB02A-07-14
Ethics and Legal Issues
7-3
● Always have an original release form on file before sending any patient records via fax. Do not accept a faxed copy of a patient release form; although the form appears to be signed, you have no way of knowing if that signature is valid because you are looking at a copy of the form and not the form itself.
● Send faxes only to a secure fax machine. This means you have to verify with the receiving person that the fax either will be picked up immediately or that the fax is in a secure area away from people who are not authorized to see what you are sending.
● Never send sensitive test information via fax. This includes HIV and pregnancy test results.
● Always use a fax cover sheet. The cover sheet must list your name, company name, telephone number, fax number and the number of pages sent.
Now that you have a better understanding of the sensitivity of medical records, let’s talk about being ethical.
Step 4: Medical EthicsMedical ethics include confidentiality, accuracy, integrity and completeness of medical records and the proper storage of these records. Medical ethics also involve guarding against fraud and misleading claims. Being ethical means that you strive to do what’s right and that you are dependable and trustworthy. As a healthcare professional, you will have access to confidential information regarding patients, physicians, insurance companies and government insurance programs. Handling this information correctly and appropriately establishes your credibility and level of professionalism. To work in the medical field, you must maintain your credibility and have a very high level of professionalism.
Most organizations have a code of ethics, which is a document that outlines specific ethical guidelines. This statement usually is posted where it easily can be read and lists specific behaviors and efforts that members or employees are expected to uphold. A code of ethics helps the employees of a company know what is expected of them but also helps patients or consumers relax and know that they are dealing with a credible, responsible office or business. Take a look at the sample code of ethics from the American Academy of Professional Coders that follows.

0201604LB02A-07-14
Medical Coding Specialist
7-4
Code of Ethical StandardsCommitment to ethical professional conduct is expected of every AAPC member. The specification of a Code of Ethics enables AAPC to clarify to current and future members, and to those served by members, the nature of the ethical responsibilities held in common by its members. This document establishes principles that define the ethical behavior of AAPC members. All AAPC members are required to adhere to the Code of Ethics and the Code of Ethics will serve as the basis for processing ethical complaints initiated against AAPC members.
AAPC members shall:
● Maintain and enhance the dignity, status, integrity, competence, and standards of our profession.
● Respect the privacy of others and honor confidentiality.
● Strive to achieve the highest quality, effectiveness and dignity in both the process and products of professional work.
● Advance the profession through continued professional development and education by acquiring and maintaining professional competence.
● Know and respect existing federal, state and local laws, regulations, certifications and licensing requirements applicable to professional work.
● Use only legal and ethical principles that reflect the profession’s core values and report activity that is perceived to violate this Code of Ethics to the AAPC Ethics Committee.
● Accurately represent the credential(s) earned and the status of AAPC membership.
● Avoid actions and circumstances that may appear to compromise good business judgment or create a conflict between personal and professional interests.
Adherence to these standards assures public confidence in the integrity and service of medical coding, auditing, compliance and practice management professionals who are AAPC members.
Failure to adhere to these standards, as determined by AAPC's Ethics Committee, may result in the loss of credentials and membership with AAPC.
Source: AAPC Code of Ethics: http://www.aapc.com/AboutUs/code-of-ethics.aspx 4 September 2013

0201604LB02A-07-14
Ethics and Legal Issues
7-5
Confidentiality and ethics go hand in hand with the Health Insurance Portability and Accountability Act which you’ll learn about next. You’ll learn who must abide by the act, the details of the act and how the act applies to you as a medical coding specialist.
Step 5: Health Insurance Portability and Accountability ActIn 1996, Congress enacted the Health Insurance Portability and Accountability Act (HIPAA). This bill has two main objectives. The first objective is portability, which is to ensure the continuation of health insurance coverage for workers and their families during times of job change or loss. The second, accountability, is to increase the effectiveness of the healthcare system while protecting health data integrity, confidentiality and availability, as well as preventing fraud and abuse.
The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted as part of the American Recovery and Reinvestment Act (ARRA) of 2009, was signed into law on February 17, 2009, to promote the adoption and meaningful use of health information technology.1 HIPAA (as modified by the HITECH Act of 2009) requires compliance to privacy standards and security in the maintenance and electronic exchange of administrative and financial healthcare information.
The different sections of HIPAA are known as titles. It is Title II, Subtitle F that is probably the most important to the healthcare professional. This part is called the Administrative Simplification Compliance Act. When healthcare professionals talk about HIPAA and being HIPAA compliant, they are usually referring to this section. The Administrative Simplification Compliance Act (ASCA) sets up nationally consistent regulations in four main areas:
● Transaction and Code Sets Standards
● Privacy Standards
● Security Standards
● Unique Identifier Standards
You’ll examine each of these standards in more detail and explain how it affects you, but first let’s look at who must follow HIPAA regulations.
Covered EntitiesThose that must follow HIPAA regulations are called covered entities. Covered entities include health plans, healthcare clearinghouses and healthcare providers who transmit any health information in electronic form. A healthcare professional who is a member of the covered entity’s workforce is also known as a covered entity.

0201604LB02A-07-14
Medical Coding Specialist
7-6
However, a healthcare professional who is, for example, an independent consultant providing coding services to a physician is not a covered entity, but a business associate. A business associate is a person that performs, or assists in the performance, of a function or activity involving the use or disclosure of individually identifiable health information. This includes claims processing or administration, data analysis, utilization review, quality assurance, billing, benefit management and practice management.2 The contract between a covered entity and a business associate must contain specific elements describing the permitted and required uses of protected health information. A sample business associate contract can be found at the Department of Health and Human Services Web site at www.hhs.gov/ocr/privacy/hipaa/understanding/coveredentities/contractprov.html.
Now that you know who must comply with HIPAA, let’s look at the rules that covered entities and their business associates must follow. Keep in mind that when covered entities are referred to, it’s assumed that business associates are included in the rule, as well, due to the contract between covered entities and business associates.
Transaction and Code Sets StandardsAccording to HIPAA, a transaction is an electronic exchange involving the transfer of information between two parties for a specific purpose.3 A transaction is electronic if it is transmitted with an electronic medium, which includes Internet, Extranet, leased lines, dial-up lines and private networks. Information physically moved from one location to another with storage media, such as magnetic tapes, disks or CDs, is also considered an electronic transaction. Telephone voice response or faxback systems are not electronic transactions, according to HIPAA.
Transaction and Code Sets Standards simply outline the format and codes used for electronic transmissions. At one time, there were about 400 formats for electronic health claims being used in the United States. This lack of standardization made it difficult and expensive to develop and maintain software to process claims. Today, it’s required that all covered entities doing business electronically use the same transactions and code sets. Let’s look at the standard code sets first.
Under HIPAA, specific code sets were adopted for diagnoses and procedures to be used in all healthcare transactions. These code sets include HCPCS (ancillary services/procedures), CPT (physician services/procedures), CDT (dental terminology), ICD-10-CM (diagnoses), ICD-10-PCS (hospital inpatient procedures) and NDC (National Drug Codes).
Now, let’s look at the standard transactions. You know about the CMS-1500 and UB-04 claim forms; however, when claim information is transmitted electronically, it’s not submitted in the same format as you see on the paper claim. Electronic data interchange (EDI) is the electronic transfer of information in a standard format between trading partners. Basically, EDI is the process of submitting a claim electronically in a standard format to an insurance company for reimbursement for the provider’s services.

0201604LB02A-07-14
Ethics and Legal Issues
7-7
Here is an example of a claim submitted to an insurance carrier for Robert Daly seen at the Medical Care Center:4
Header
Loop 100A – Submitter Name
Loop 1000B – Receiver Name
Loop 2000A – Service provider Name for Medical Care Center
Loop 2010BA – Subscriber (Patient) for Robert Daly
Wow! That looks like gibberish, doesn’t it? Luckily, it’s not your responsibility to understand, describe or maintain this information. You simply need to know that the claim information sent to an insurance carrier is not transmitted in the same format as the paper CMS-1500 or UB-04 claim forms but in a standard form that HIPAA requires.
Finally, it’s helpful to recognize the terminology associated with these electronic transactions. Since October 16, 2003, all healthcare businesses that submitted claims electronically have been required to use version 4010. In 2012, version 5010 replaced version 4010 with improvements, such as correcting technical issues, accommodating new business needs and eliminating inconsistencies in reporting requirements.
All of this technical information may seem overwhelming to you. However, keep in mind that it’s not the specifics that you need to know, but the big picture. There are standards in the healthcare industry. These standards define the codes you use, the forms you complete and how information is submitted electronically. You may hear the term 5010 in your work, and now you know that 5010 refers to the current standard version of electronic transmissions!
Privacy RuleThe HIPAA Privacy Rule establishes national standards to protect individuals’ medical records and other personal health information that applies to covered entities.5 The Privacy Rule addresses the use and disclosure of a patient’s protected health information. Protected Health Information (PHI) is individually identifiable health information, or information that can be used to identify an individual, that is held or transmitted by a covered entity or its business associate in any form, whether electronic, paper or oral.6 You’ll hear a lot about protected health information a lot in this section, as it’s the foundation of the privacy rule.

0201604LB02A-07-14
Medical Coding Specialist
7-8
HIPAA requires that covered entities provide patients a notice of privacy practices, which is a form that defines how the provider can use PHI. A notice of privacy practice in plain language that describes the following is necessary.7
● How the covered entity may use and disclose PHI about an individual.
● The individual’s rights with respect to the information and how the individual may exercise these rights, including how the individual may complain to the covered entity.
● The covered entity’s legal duties with respect to the information, including a statement that the covered entity is required by law to maintain the privacy of PHI.
● Whom individuals can contact for further information about the covered entity’s privacy policies.
In addition, the notice must include an effective date, and providers are required to provide the notice on a patient’s first visit.
The basic principal of the Privacy Rule is to define and limit the circumstances in which PHI may be used or disclosed by covered entities. This rule allows healthcare providers to obtain a consent, or written permission, to use or disclose a patient’s health information for treatment, payment and healthcare operations, often referred to as TPO. Written authorization is required for any use or disclosure of PHI that is not for TPO or not otherwise specified in the Privacy Rule.
Authorization to disclose information forms must contain:
● A specific description of the health information that will be used.
● The name or specific identification of the person or people to whom the healthcare facility may disclose the information.
● The name or specific identification of the person or people who are authorized to use the information.
● An expiration date that pertains to the individual or purpose of the disclosure of the health information.
● A statement of a person’s right to rescind the authorization in writing.
● A statement that outlines the exceptions to the right to rescind.
● A statement that outlines how a person may rescind the authorization right.
● A statement that the Privacy Rule would no longer protect health information that the recipient redisclosed, even if authorization disclosed it previously.
● The individual’s signature and the date.

0201604LB02A-07-14
Ethics and Legal Issues
7-9
The following results in an invalid authorization:
● The expiration date on the authorization to disclose information has passed.
● The authorization to disclose information form is not completely filled out.
● The authorization to disclose information form lacks one or more required elements.
● The authorization to disclose information form covers more than one request.
● The healthcare facility knows the patient or the patient’s legal representative has rescinded authorization.
● The healthcare facility knows that some or all of the information in the form is false.
There are only two instances in which the patient may not rescind authorization to disclose healthcare information: when the person or people to whom the healthcare facility disclosed the information have already taken action or when the authorization was given so that a patient could receive insurance coverage, and the insurance company contests a claim under the policy.
The Privacy Rules states that healthcare providers must make reasonable efforts to use, disclose and request the minimum necessary amount of PHI needed to accomplish the purpose of the authorization. Minimum necessary limits unnecessary or inappropriate access to and disclosure of PHI. Let’s look at an example to clarify this point.
A medical billing specialist that processes the billing for Weston Medical Clinic does not require the entire documentation (medical record) to submit a claim. The patient name and insurance information, as well as the medical codes, are needed to create a claim for the reimbursement process. Meanwhile, a medical transcriptionist does not need to know the patient’s insurance information; she just needs to know who the patient was, when the service was performed and what the provider did during the service.
So, aside from the previous example, how does the Privacy Rule affect you as a healthcare professional? Well, in the healthcare profession, you probably won’t be checking for consents or authorization, but you do need to protect the patient’s medical record. Look at the following scenario, and think about how the situation should have been handled differently.
Elizabeth does medical coding from home. Elizabeth’s home office is in the living room of her townhome. She begins her day by connecting to an EHR to pull the dictation that was transcribed the previous day. As she’s working on assigning codes, Elizabeth’s neighbor, Alice, knocks on the door. Elizabeth invites Alice in the living room for a cup of coffee. Forgetting to log off of the EHR, Elizabeth runs to the kitchen to make the coffee. While alone in the living room, Alice notices the name of a co-worker on the screen. Her curiosity gets the best of her, and Alice inches closer to read the details on the screen.
This is a violation of the Privacy Rule. It’s important that you keep the patient’s protected health information private. After all, consider how you would feel if you were the patient in this example!

0201604LB02A-07-14
Medical Coding Specialist
7-10
Security RuleWhile the Privacy Rule focuses on protected health information in general, the Security Rule deals with electronic protected health information (ePHI). The Security Rule establishes a national set of security standards for protecting health information that is held or transferred in electronic form. This rule does not apply to PHI transmitted orally or in writing.8 Prior to HIPAA, no formal security standards or requirements existed for protecting health information. As technology evolved, computers became standard in the healthcare profession, allowing medical information to become more mobile and efficient, but also increasing the potential security risk. Computer hackers and viruses can wreak havoc on computer systems; they can corrupt files, make information public and change critical data.
The Security Rule has two primary purposes:
● Require appropriate security safeguards to protect ePHI that may be at risk.
● Promote access and use of ePHI while protecting an individual’s health information.
Specifically, HIPAA notes: A covered entity must have in place appropriate administrative, technical and physical safeguards to protect the privacy of protected health information. This includes any intentional or unintentional use or disclosure of ePHI. HIPAA requires each covered entity to assess its own security needs and implement the measures that best meet those needs. Administrative, physical and technical concerns must be examined when these entities protect privacy. This doesn’t mean that every employee must now have top-secret clearance. Some changes can be simple. For example, a good security step is to ensure that unauthorized people cannot view computer monitors and faxed pages. Other security measures are more complicated, such as using proper electronic data encryption. Encryption means the electronic information is put into a coded form while transmitted. The encrypted electronic information cannot be understood without the appropriate decryption equipment. Take a look at the example that follows.
Patient: Alyssa TurnerMRN: 12345678DOB: 12-12-1962
Current Medications:Lipitor 20 mg dailyClonidine 0.17 mg q.h.s.Synthroid 1.7 mcg daily
Patient: Alyssa TurnerMRN: 12345678DOB: 12-12-1962
In your career as a healthcare professional, you will have access to protected health information. While electronic health records provide ease of access, you must have in place appropriate administrative, technical and physical safeguards to protect the privacy of protected health information. How will you do this? Passwords, key cards and encryption are a few ways.
Healthcare organizations must control access to their files. A small physician’s office might simply provide passwords for its personnel to meet this requirement. The medical coding specialist working from home could log onto the computer system to access coding information with her password, while the nurse practitioner at the office could renew prescriptions and view and modify health histories with her password.
0201604LB02A-07-14
Ethics and Legal Issues
7-11
In a large hospital, the access requirements have a more complex set of tools. Key cards might be used for personnel to access particular rooms that house information databases within the multi-building complex. A security officer might view daily printouts that detail who accessed certain files with their passwords. She also might require password changes every few months. The feature of the security standards may vary to ensure that compliance is economically feasible for organizations of every shape and size.
Using encryption software is a simple safeguard for the healthcare profession to ensure patient privacy. When PHI is encrypted, even if a hacker is able to gain access to medical records, he won’t be able to read or interpret the information. The patient’s privacy is protected because a key is required to unscramble the information.
Before you look at the final standard in the Administrative Simplification Compliance Act, which is the Unique Identifier Standard, let’s pause to review what you’ve learned.
Unique Identifier StandardThe Unique Identifier Standard establishes the implementation specifications for obtaining and using the standard unique health identifier for health care providers. At this time, there are two standards when it comes to unique identifier: the Employer Identification Number and the National Provider Identifier.
In 2002, HIPAA adopted the Employer Identification Number (EIN), which was issued by the Internal Revenue Service (IRS) to identify employers on standard transactions, which includes CMS-1500 and UB-04 claims, as well as all electronic transmissions of claims. The billing provider includes his EIN on the claim to be used for 1099 taxable income reporting purposes.
HIPAA mandated the adoption of a standard unique identifier for healthcare providers in 2007. The National Plan and Provider Enumeration System (NPPES) collects identifying information on healthcare providers and assigns each a unique National Provider Identifier (NPI). The NPI regulation seeks to eliminate multiple identifiers. At one time, insurance carriers, such as Medicare and Medicaid, assigned identifiers for providers to submit with claims. These identifiers were known as UPIN, OSCAR and PIN. The identifiers were not standardized, resulting in one provider having multiple identification and billing numbers. These legacy numbers complicated the claims submission processes and resulted in the assignment of the same identification number to different health care providers by different health plans.
According to CMS, the NPI is a 10-position, intelligence-free numeric identifier (10-digit number). This means that the numbers do not carry other information about healthcare providers, such as the state in which they live or their medical specialty. Once assigned, NPI is associated with the same provider forever; it will not change, regardless of job or location changes.
The use of standard identifiers is expected to ease the administrative challenges associated with all aspects of patient healthcare records. These challenges include documentation, maintenance and billing requirements. These standard identifiers will allow the various entities within the healthcare system to most effectively and efficiently perform their respective financial, clinical, preventive and research functions. To put it simply, a healthcare entity can devote more time to its own particular business and patients and less to general paper pushing when using an NPI.
Now that you have a better understanding of the standards associated with the Administrative Simplification Compliance Act, let’s look at what happens when patient privacy is breached, which means there was a violation or infraction of a standard.

0201604LB02A-07-14
Medical Coding Specialist
7-12
Breach of PrivacyWhat happens when there is an intentional or unintentional use or disclosure of ePHI? The HITECH Act requires covered entities to provide notification in the event of a breach of unsecured protected health information. Unsecured means the information hasn’t been encrypted. For instance, if a computer hacker gained access to patient information that hasn’t been encrypted, the practice would have to inform all patients and the Department of Health and Human Services (HHS) of that breach. In some cases, the practice is also required to notify the media. However, if the ePHI is encrypted, patients do not need to be notified.
Following are two examples of data breach notifications. The first is a notice from TRICARE posted to its Web site alerting the public of the breach. The second is a news article, also notifying the public of the breach, as required by HIPAA.
Letters are being mailed from Science Applications International Corporation (SAIC) to affected military clinic and hospital patients regarding a data breach involving personally identifiable and protected health information (PII/PHI). On Sept. 14, 2011, SAIC reported the loss of backup tapes containing electronic health care records used in the military health system (MHS) to capture patient data from 1992 through Sept. 7, 2011 in San Antonio area military treatment facilities (MTFs), including filling pharmacy prescriptions and other patients whose laboratory workups were processed in these same MTFs, even if the patients were receiving treatment elsewhere. The data may include Social Security numbers, addresses and phone numbers, and some personal health data such as clinical notes, laboratory tests and prescriptions. There is no financial data, such as credit card or bank account information, on the backup tapes.
Reference: http://www.tricare.mil/breach/
This breach affected nearly 5 million patients, making it the largest medical data breach since the HHS began tracking incidents in 2009.
On May 14, 2012 federal prosecutors charged one of the hospital’s medical technicians with violating the Health Insurance Portability and Accountability Act, or HIPAA. Prosecutors say that over a 17-month period Laurie Napper used her position at the hospital to gain access to patients’ names, addresses and Medicare numbers in order to sell their information.
Reference: http://www.kaiserhealthnews.org/Stories/2012/June/04/electronic-health-records-theft-hacking.aspx
The first case was an example of an unintentional breach of ePHI, while it was clearly an intentional violation in the second. Now, let’s look at the organization that has the right to enforce, audit, fine and charge covered entities for violations of HIPAA, such as those you just examined.

0201604LB02A-07-14
Ethics and Legal Issues
7-13
Office for Civil RightsHIPAA and HITECH are administered by the HHS in the Office of the Civil Rights (OCR). The OCR enforces the Privacy and Security Rules by investigating complaints and conducting compliance reviews, as well as performing education and outreach to foster compliance with the rules’ requirements. Since the compliance date in April 2003, HHS has received more than 71,849 HIPAA complaints. The OCR has resolved 91 percent of complaints received (more than 65,460). The OCR has investigated and resolved more than 16,708 cases by requiring changes in privacy practices and other corrective actions by the covered entities. Of the remaining complaints, 8,514 were investigated, and no violation was found; 40,238 complaints were resolved through closure of cases that were not eligible for enforcement because the entity wasn’t covered under the Privacy Rule, the complaint was not filed in a timely fashion or the incident described wasn’t in violation of the Privacy Rule.
HIPAA Privacy & Security Rule Complaint Process
Let’s look at those complaints that were resolved through investigation and enforcement. If the evidence indicates that the covered entity was not in compliance, the OCR will attempt to resolve the case with the covered entity by obtaining voluntary compliance, corrective action and/or a resolution agreement.9
A resolution agreement is a contract signed by HHS and a covered entity in which the covered entity agrees to perform certain obligations (e.g., staff training) and make reports to HHS, generally for a period of three years.10 The HHS monitors the covered entity during these three years to ensure that the entity is in compliance with the obligation.

0201604LB02A-07-14
Medical Coding Specialist
7-14
According to the OCR, most Privacy and Security Rule investigations are concluded to the satisfaction of the OCR. However, if the covered entity does not take action to resolve the matter in a way that is satisfactory, the OCR may decide to impose civil money penalties (CMPs) on the covered entity. Under the HITECH Act, mandatory penalties have been and will be imposed for willful neglect. According to HIPAA, willful neglect means conscious, intentional failure or reckless indifference to the obligation to comply with the administrative simplification provision violated. Civil money penalties for willful neglect can extend up to $250,000, with repeat or uncorrected violations extending up to $1.5 million.
You’ve learned a lot in this section! You studied the basics of HIPAA and the HITECH Act. You know the standards associated with the Administrative Simplification Compliance Act and understand how they apply to your career as a medical coding specialist. And you found that the OCR has the right to enforce, audit, fine and charge covered entities for violations of HIPAA.
The last section about the violations of HIPAA may have seemed a bit daunting, but it’s important to know that there will be ramifications for willful neglect. However, the key is remembering to act in an ethical manner and keep patient information private. As a medical coding specialist, you know not to share a chart note you’ve read earlier that day with your family during dinner. You understand that coding a chart of a close friend isn’t the best idea; it should be coded by someone else! And you would never share your neighbor’s billing troubles with another neighbor. These safeguards will keep you from breaking any of the rules you’ve just learned about! Now, let’s move on to fraud and abuse.
Step 6: Practice Exercise 7-1Determine the correct term(s) for each sentence, and write your answers on scratch paper.
1. The two main objectives of HIPAA are _____ and _____.
2. _____ are healthcare professionals who transmit any health information in electronic form.
3. The _____ addresses the use and disclosure of patients’ health information.
4. TPO stands for _____, payment and healthcare _____.
5. The Security Rule does not apply to PHI transmitted _____.
6. _____, is issued by the Internal Revenue Service (IRS) to identify employers on standard transactions.
7. The _____ is a 10-position, numeric identifier that does not carry other information about healthcare providers.
8. The term _____ refers to a violation or infraction of a standard.
9. When protected health information is unsecured it means the information hasn’t been _____.
10. A conscious, intentional failure or reckless indifference to the obligation to comply with the administrative simplification provision is _____.

0201604LB02A-07-14
Ethics and Legal Issues
7-15
Step 7: Review Practice Exercise 7-1Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 8: Fraud and AbuseOne of the government’s top priorities is to eliminate healthcare fraud. Unfortunately, investigations of fraud and abuse are on the rise. Fraud occurs when inaccurate information is used to wrongfully gain compensation. Fraud is a crime. In the medical field, this often can occur in the medical record itself. For example, a patient’s insurance coverage becomes effective June 15. The patient receives service from a provider on June 1. The medical record is altered to indicate the date of service as June 20 to allow the treatment to be covered by insurance. This is fraud.
To guard against fraud, you must do one simple thing: Be accurate. Don’t be tempted to change information on medical records if that information already is correct. If you do change correct information, you are committing fraud, and the consequences can be severe.
The U.S. General Accounting office estimates that $1 out of every $10 spent on Medicare and Medicaid is lost to fraud and abuse. With the increasing costs associated with health care, the reduction of fraud and abuse has become a point of focus for CMS.
Fraud examples:
● Billing for services or supplies that were not provided.
● Altering claims to obtain higher payments.
● Soliciting, offering or receiving a kickback, bribe or rebate.
● Provider providing services for fictitious patients.
● Using another person’s Medicare card to obtain medical care.
Abuse examples:
● Excessive charges for services or supplies.
● Claims for services that are not medically necessary.
● Breach of the Medicare participation or assignment agreements.
● Improper billing practices including billing Medicare when Medicare is not primary.
Fraud and abuse can be reported to the federal Office of Inspector General, OIG. This governing body then makes a decision as to the penalty. The penalty can be monetary, criminal, administrative or a combination of any of the three. The Office Inspector General is also responsible for notifying the state intermediaries of any new scams.

0201604LB02A-07-14
Medical Coding Specialist
7-16
As a healthcare professional, you need to be that you are not submitting claims for medically unnecessary services, that the Medicare patient is who she says she is and that you are using an appropriate fee schedule. Keep in mind you are human and may make a mistake from time to time. Medicare is not out to get you! They are looking for those who are purposely defrauding the system.
Preventing Fraud and AbuseThe Federal False Claims Act (FCA) was signed into law in 1863 by Abraham Lincoln and is the basis for prosecution of healthcare fraud and abuse claims. The FCA prohibits anyone from presenting a false or fraudulent claim to be paid by the government, using a false record or statement to conceal or avoid paying money to the government or conspiring to defraud the government.
The FCA was not originally intended to investigate healthcare providers, but in recent years, this has become increasingly necessary, as well as very costly. In 1986, Ronald Reagan signed amendments into law that significantly strengthened the government’s ability to successfully prosecute for fraud. Damages increased from double to triple, and the FCA was extended to include unintentional misconduct.
To prevent fraud and abuse, many healthcare providers have created corporate compliance plans. Compliance plans are formalizations of processes that identify, investigate and prevent violations in various healthcare services. In addition, the government has created model compliance plans for hospitals and clinics. These include structure, standards, oversight, education, monitoring and enforcement.
Insurance rates increase when an insurance company pays fraudulent claims. When codes are not correct, the insurance company will not pay the correct amount, which delays doctors’ payments and leads to increased healthcare costs. Thus, insurance companies often try to collect damages when they discover fraudulent claims.
Consequences of Committing FraudFraud is a crime and, therefore, punishable by law. If the fraud was intentional and systematic, and if the effects of the fraud were far-reaching, the justice system can impose harsh penalties, including jail time.
The criminal side of fraud is only half of the picture. There are also civil consequences to fraud. Fraud affects us every day. When insurance companies pay fraudulent claims, rates increase unnecessarily. Insurance companies often try to collect damages when they discover fraudulent claims. These damages include compensatory damages and punitive damages.
Compensatory damages are damages directly related to the fraud. For example, if a claim submitted to an insurance company with charges for $700 worth of procedures that were not performed, the civil courts might award the insurance company $700 in compensatory damages. Compensatory damages represent the compensation a plaintiff receives from a defendant for the actual damage caused (in our example, $700 in overcharges). The plaintiff is the person who files the claim and initiates a lawsuit, while the defendant is the person named in the claim or charged with the crime. However, if the insurance company feels the fraud was intentional or perhaps negligent, it might ask for punitive damages.

0201604LB02A-07-14
Ethics and Legal Issues
7-17
Punitive damages are damages awarded to the plaintiff to punish the defendant and, theoretically, deter the defendant from repeating the fraud in the future. Punitive damages can far exceed compensatory damages. In the $700 example above, a court might award punitive damages for five times that amount ($3,500) if the fraud was intentional. Punitive damages are awarded above and beyond any compensatory damages. That means our original $700 judgment has now swelled to $4,200! This is a high cost for a lapse in judgment. In addition, whoever committed the fraud is responsible for paying all damages.
Doctors and other healthcare professionals can be liable for damages in some situations, whether their actions were intentional or not. To help protect healthcare professionals, insurance companies offer a variety of liability insurance coverage.
Step 9: Liability InsuranceWhen you drive a car, you run the risk of being in an accident. Obviously, you don’t set out to intentionally hit another car, but accidents happen. To protect yourself and the other drivers on the road, you carry some form of automobile insurance. No doubt you’ve heard of people being awarded thousands of dollars by courts for damages suffered in accidents. If you have insurance, then your insurance company pays for these damages. (After all, that’s what insurance is for.) If you aren’t covered by insurance, then you pay the entire amount!
Doctors and other healthcare professionals can be covered by medical liability insurance. The physician you work with usually carries this insurance. In case there are damages suffered as a result of an accident or negligence, the insurance covers the doctor, the doctor’s staff and anyone the doctor contracts with for services relating to the practice. In the medical world, physicians are legally responsible for their actions, as well as the actions of their employees and anyone they contract with for services relating to their practice. This protects you, the medical coding specialist, as long as you stay within the scope of your duties, which means as long as you are doing the job you were hired to do. However, if you knowingly submit fraudulent claims or break the law in some other manner, you are liable, and insurance won’t cover you. Let’s look at two situations.
Example 1 While coding from a complex dictation, Julia accidentally transposes two numbers, causing an error that results in overpayment by the insurance company.
Example 2 Hillary works with Dr. Gregg. Dr. Gregg hands her his dictation and says, “Don’t use the surgical package code. I never do because I get more money if I code everything separately.” Hillary does as Dr. Gregg asks.
Which example represents fraud? The answer is Example 2. When Hillary knowingly goes along with Dr. Gregg, she is submitting codes she realizes are false. This should be reported, not complied with. How do insurance companies catch fraudulent claims? They conduct company-auditing procedures.
Insurance AuditsInsurance companies guard very closely against fraud. Even with safeguards, some fraudulent claims sneak through. However, through insurance audits, many of these claims are caught. An insurance audit is a thorough review by the insurance company of a claim and all related documentation. Auditors compare and search the records for inconsistencies and alterations.

0201604LB02A-07-14
Medical Coding Specialist
7-18
What triggers an insurance audit? Well, the insurance company might find the claim suspicious or notice that the doctor files an unusual number of similar claims. On the other hand, the patient might bring a questionable claim to the attention of the insurance company.
Many insurance companies encourage their clients to review medical records and bills to ensure that the procedures listed were performed and the diagnosis is accurate. If a patient has a question, the insurance company has a toll-free number to call for that purpose. If there is an overcharge on a claim that a patient notified the insurance company about, that patient usually gets some kind of cash reward from the insurance company. This encourages patients to review their records.
Step 10: Recovery Audit ContractorsAccording to the OIG, it is estimated that $16.4 billion in improper payments and error rates were made in 2000.11 The Medicare Modernization Act of 2003 created a three-year project to recover Medicare overpayments and identify underpayments. The three-year project focused on California, Florida, New York, South Carolina and Massachusetts. In March 2008, the program ended with more than $1.03 billion recovered from improper payments. Approximately 96 percent of the improper payments were overpayments collected from providers, and the remaining four percent were underpayments paid to providers.12
The Tax Relief and Health Care Act of 2006 expanded this project to all 50 states, creating a permanent and nationwide program by 2010. CMS contracted Recovery Audit Contractors (RACs) to recover overpayments. RACs are paid on a contingency fee basis, receiving a percentage of the improper payments they collect from providers.13 RACs may review the last three years of provider claims for the following types of services: hospital inpatient and outpatient, skilled nursing facility, physician, ambulance and laboratory, as well as durable medical equipment.
In 2011, CMS reported that it has collected more than $313 million in Medicare overpayments through its recovery audit program since October 2009.14 However, RAC decisions can be appealed. Look at the following report:
The Centers for Medicare & Medicaid Services (CMS) has released appeals data for Medicare fee-for-service Recovery Audit Contractors (RACs). For claims originating in fiscal year 2011 (Oct. 1, 2010-Sept. 30, 2011), providers appealed 56,620 repayment demands, over 6.25 percent of the 903,372 claims with overpayment determinations. Of these, 24,548 (43.4 percent) were decided in providers’ favor. Approximately 2.7 percent of all claims with overpayment determinations were overturned on appeal.
Reference: http://www.aapcps.com/news-articles/RAC-appeals-won.aspx
As with liability concerns, there are several legal concerns to consider when working with medical records. Let’s take a closer look.
Step 11: Legal ConcernsThe legal system in the United States is very complex. Attorneys study it for years and still may not understand everything there is to know about law. While you will study some of the basic concepts regarding medical records and the law, you should always consult an attorney if you have to deal with the legal system. By doing so, you receive expert advice from someone who knows the system. This section gives you an overview of some very basic concepts, which will enable you to effectively communicate with other medical professionals.

0201604LB02A-07-14
Ethics and Legal Issues
7-19
SubpoenasA subpoena is a legal document issued by the court requiring the person named on the subpoena to appear in court or to supply certain documents or both. A subpoena can authorize the legal release of confidential medical records.
A subpoena cannot be mailed. Instead, it is served personally by an authorized person. If you are served with a subpoena and fail to respond, you can be arrested and charged with a crime. A subpoena is a legal document and must never be ignored.
When you follow the directions contained in the subpoena, you have complied with it. To comply with a subpoena for medical records, you generally have a specified amount of time to produce the records. You make copies of the appropriate records, and supply the copies to whoever is named on the subpoena. Usually, this is an attorney.
If you receive a subpoena to testify, it means you must appear at the designated court on the assigned day and time. You cannot be late, and you cannot ignore the subpoena. Sometimes you are paid for your time, and the fee is included with the subpoena. Remember not to get angry with the person serving the subpoena. The server is usually neutral, not involved with the case at all and “just doing a job.”
When a subpoena is issued, it usually means someone is headed to court and needs the medical records for a case. Sometimes, however, disputes don’t end up in court. Instead, they may be heard in arbitration.
ArbitrationArbitration is an alternative to a court of law. In arbitration, two disputing parties meet with an arbitrator, or a person chosen to decide a dispute or settle differences. Each party tells its side of the situation, and the arbitrator issues a ruling. In binding arbitration, the ruling is final and must be obeyed. In nonbinding arbitration, the ruling is merely a suggestion from an objective person. Many contracts now specify that disputes must be settled in binding arbitration rather than in court. Arbitration is much less expensive and usually resolves problems faster than the court system.
Medical TestimonyIf arbitration is not an option, or if someone insists on going to court, then people may have to provide testimony. Testimony is the sworn statements of witnesses and experts given while on the witness stand in court. Witnesses give statements under an oath of truth, and people who lie during testimony can be charged with perjury, a serious crime.
In medical cases, doctors are sometimes called to testify. Often, doctors testify as expert witnesses—people who know about the circumstances surrounding a case, but not necessarily about the case itself. For example, imagine a trial involving physical evidence, such as DNA. The DNA is analyzed and the results brought to court. The side presenting the evidence might have an expert talk about DNA in general. That expert is someone who knows about DNA but has no other connection to the case. This person is an expert witness.
Now it’s time to review what you’ve learned about fraud and abuse with the following Practice Exercise.

0201604LB02A-07-14
Medical Coding Specialist
7-20
Step 12: Practice Exercise 7-2Determine the correct term(s) to complete each sentence, and write your answers on scratch paper.
1. As a healthcare professional, you cannot release any medical information unless it is to an authorized person because the information is _____.
2. Ethical guidelines are often spelled out in a document called a _____.
3. You should _____ fax sensitive test information.
4. Damages directly related to fraud are termed _____ damages.
5. The _____ prohibits anyone from presenting a false or fraudulent claim to be paid by the government.
6. Fraud includes inaccurate information that is used to wrongfully gain _____.
7. Fraud and abuse can be reported to the _____.
8. A(n) _____ is a thorough review by the insurance company of a claim and all related documentation.
9. _____ are paid on a contingency fee basis, receiving a percentage of the improper payments they collect from providers.
10. A(n) _____ can authorize the legal release of confidential medical records.
11. A(n) _____ is a person chosen to decide a dispute or settle differences.
12. When a person lies during testimony, he can be charged with _____.
Step 13: Review Practice Exercise 7-2Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 14: Lesson SummaryWe covered a lot of information in this lesson. Ethics and credibility are interwoven like threads in a rug. When you are in business, whether it is your own or someone else’s, you must always keep a strong code of ethics foremost in your mind. If you follow the principles of these ethics, you can relax and do your job. You have credibility. People can count on you.

0201604LB02A-07-14
Ethics and Legal Issues
7-21
Privacy and security are major concerns as more and more healthcare data is transmitted and maintained electronically. The Health Insurance Portability and Accountability Act is, in part, federal legislation that governs health information in electronic form. Here, legal and ethical issues are joined. As a medical coding specialist, you must be sure that you follow strict guidelines in protecting the confidentiality of the patient information entrusted to you. A signed patient consent, obtained by the physician, permits you to release information for purposes of treatment, payment and healthcare operations. You must not make any other release of information unless the patient has provided a signed authorization allowing such release.
Even the most ethical person can make a mistake. Mistakes can be covered by liability insurance carried by the physician with whom a person works. Fraud, however, is an intentional misrepresentation of facts. Fraud usually is committed to try to gain more money or some other undeserved benefit. Fraud is illegal. When illegal acts are committed or if two parties have a disagreement that cannot be settled, the legal system might come into play.
The legal system, as you’ve learned, settles disputes and upholds laws. Subpoenas are often used to present all the facts. A subpoena is a document that is served to a person who is in possession of vital information. This information might be in the form of medical records, or it might be in the form of expertise in the field. If you are in charge of records that are listed on a subpoena, you should make sure you are authorized to release the records to the appropriate party, and then you may do so.
Arbitration is used when two parties disagree and cannot settle their disagreement. Binding arbitration means the arbitrator’s decision is final and must be followed. In nonbinding arbitration, the decision of the arbitrator is treated as a suggestion. Finally, you learned that sometimes a physician has to go to court to provide medical testimony.
Now, let’s test your understanding of this lesson with a Quiz.
Step 15: Quiz 7Once you’ve mastered the course content, locate this Quiz in your Online Course or your Assignment Pack. Read and follow the instructions carefully.
Endnotes 1 HITECH Act Enforcement Interim Final Rule. U.S. Department of Health & Human Services. Web. 29 October 2013. 2 HIPAA.com. Web. 29 October 2013. 3 Transaction & Code Set Standards. CMS.gov. Web. 29 October 2013. 4 Data Standards Committee. Public Health Data Standards Consortium, 2013. Web. 29 October 2013. 5 The Privacy Rule. U.S. Department of Health & Human Services. Web. 29 October 2013. 6 The Privacy Rule. U.S. Department of Health & Human Services. Web. 29 October 2013. 7 Covered Entities. U.S. Department of Health & Human Services. Web. 29 October 2013. 8 Understanding Health Information Privacy. U.S. Department of Health & Human Services. Web. 29 October 2013. 9 HIPAA Enforcement. U.S. Department of Health & Human Services. Web. 29 October 2013.10 HIPAA Enforcement. U.S. Department of Health & Human Services. Web. 29 October 2013.11 Centers for Medicare & Medicaid Services’ Use of Medicare Fee-for-Service Error Rate Data To Identify and Focus on Error-Prone
Providers. Department of Health & Human Services, 7 Oct. 2010. Web. 14 March 2012.12 Recovery Audit Contractors (RAC). American Health Information Management Association. Web. 14 March 2012.13 Recovery Audit Contractors (RAC) Program. American Hospital Association. Web. 14 March 2012.14 CMS collects $162 million in overpayments in first three months of 2011. Modern Healthcare. Web. 14 March 2012.

0201604LB02A-07-14
Medical Coding Specialist
7-22

Lesson 8Introduction to Anatomy
Step 1: Learning Objectives for Lesson 8When you have completed the instruction in this lesson, you will be trained to:
● Explain the basic components of human biology.
● Describe the human body, including how it works and how it is put together.
● Define the terms used to locate parts of the body.
Step 2: Lesson PreviewToday, many people use anatomy daily in their professions. Athletic coaches must be well versed in anatomy, because their knowledge of muscles and bones helps their players achieve top performance and avoid injury. Doctors must know vast amounts of anatomy, from the top of the human head down to the little toe, and all of the nerves, blood vessels and organs in between. Healthcare professionals must know anatomy to understand the terms they see in their work. Your knowledge of medical terms, as well as anatomy, work together to make you competent in your future career.
You will be introduced to the basic components of human biology, including anatomy, physiology and pathology. Keep in mind that we do not expect you to memorize every term. The more familiar you are with your terminology, the quicker and easier it will be to complete some of your tasks as a healthcare professional. However, it is important you use your research tools. If you don’t remember a word while completing your lessons or while working, use your materials or flashterms to help.
Once you begin working, you will see many of these terms on a daily basis, and you will become very familiar with them. For now, complete your Practice Exercises and concentrate on reviewing your flashcards and listening to pronunciations when you have an opportunity. Don’t hesitate to research terms when needed. You will soon be confident in your skills!
In this lesson, you will see how anatomy affects our everyday lives. We’ll begin with an introduction to the science of life—biology. After you learn about basic human biology, we will move into the more specific science of anatomy, including physiology—the study of how the body works. Don’t worry! We will move at a comfortable pace, and we’ll carefully cover each detail you must know. Soon you will see how easy and fun anatomy can be.

0201604LB02A-08-14
Medical Coding Specialist
8-2
Step 3: Human BiologyFor the next several lessons, you will learn about the study of human living things. Because you are a human, you’ll learn a lot about yourself. In doing your Practice Exercises and studying your flashcards, you’ll grow in your understanding of the human body and the specialized terms doctors use to talk about the body.
Human biology is the study of how the body is put together and how it works in health and disease. As a medical coding specialist, you do not need to become an expert in biology. However, understanding the basics of biology gives you a good background for the terms doctors use, such as those you learned about in the medical terminology lessons!
Human biology in the healthy state covers two basic concepts: anatomy and physiology. Human biology in disease deals with pathology. On the next few pages of this lesson, you will find diagrams that show how these concepts are related.
We will discuss each of these topics in more detail. Remember, the idea is not to become an expert in biology, but to understand the context of the terms you might see in your daily work.
AnatomyAnatomy is the science of the structure of the body—the appearance and relationships of body parts. The two kinds of anatomy are gross anatomy and microscopic anatomy.
● Gross anatomy includes parts of the body that we can see with our eyes. It is also called macroscopic anatomy.
● Microscopic anatomy, or cell anatomy, includes parts of the body that are too small to be seen with the naked eye.
(Cell)
The two kinds of anatomy are gross anatomy and miscroscopic anatomy.
0201604LB02A-08-14
Introduction to Anatomy
8-3
Gross AnatomyGross anatomy focuses on presence and appearance of a body part. The study of the form of body parts is called morphology. The form of a body part includes its size, shape, color, contour and texture. For example, when a kidney is normal in size, shape, color, contour and texture, it has normal morphology.
A basketball player and a jockey both have the same anatomic structure; both have five fingers on each hand. However, there is a morphologic difference between them. For example, the hand of the basketball player is larger than the hand of the jockey.
Gross anatomy also deals with the location and position of the organs and body parts. For example, not only should the heart be in the chest, but it should be in the left side of the chest.
Facts About Gross AnatomyThe terms used to describe gross anatomy include:
♦ The names of the body parts
♦ Where the body parts are located
♦ How the locations of two body parts are related
Microscopic AnatomyMicroscopic anatomy is the science of the body’s individual cells and tissues. This study is done with a microscope. The microscopic study of cells is called cytology. The microscopic study of tissues is called histology.
Facts About Microscopic AnatomyThe terms used to describe microscopic anatomy include:
♦ The names of different cell parts and cell types
♦ The colors cells become when they are dyed for microscopic examination
♦ The ways cells are arranged in different types of tissue
PhysiologyPhysiology is the study of how the body works; it describes the function of the body and its organs, tissues and cells.
Each organ, cell or tissue has its own special physiologic function. For example, kidneys make urine, but they cannot think. The brain thinks, but it cannot make urine.
Physiology also can be divided into macroscopic physiology and microscopic physiology.
● Macroscopic physiology usually is called gross physiology.
● Microscopic physiology usually is called cell physiology.
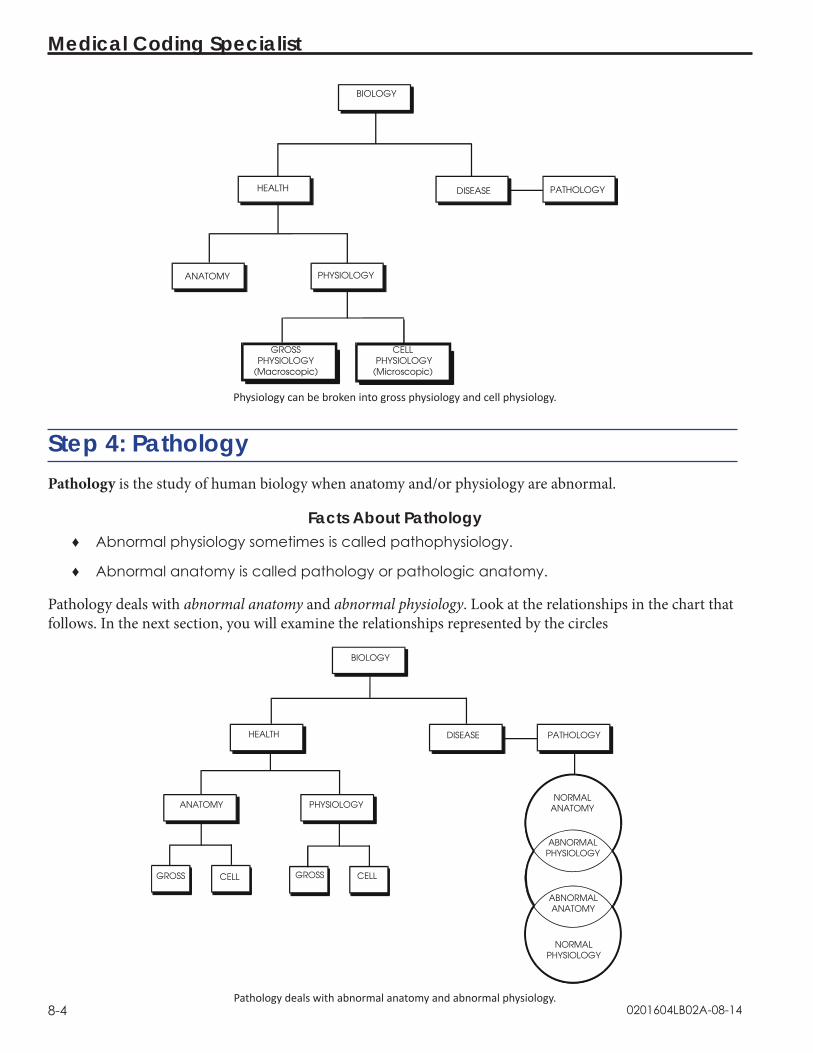
0201604LB02A-08-14
Medical Coding Specialist
8-4
Physiology can be broken into gross physiology and cell physiology.
Step 4: PathologyPathology is the study of human biology when anatomy and/or physiology are abnormal.
Facts About Pathology ♦ Abnormal physiology sometimes is called pathophysiology.
♦ Abnormal anatomy is called pathology or pathologic anatomy.
Pathology deals with abnormal anatomy and abnormal physiology. Look at the relationships in the chart that follows. In the next section, you will examine the relationships represented by the circles
BIOLOGY
HEALTH
PHYSIOLOGYANATOMY
Pathology deals with abnormal anatomy and abnormal physiology.

0201604LB02A-08-14
Introduction to Anatomy
8-5
How Anatomy, Physiology and Pathology RelateIn this section, you’ll examine normal anatomy and physiology.
Normal Anatomy/Abnormal PhysiologyA person can have abnormal physiology but normal anatomy. For example, a diabetic has abnormal physiology—the person cannot make insulin—but the diabetic may have normal anatomy. The insulin-making function is abnormal but the appearance and location of the organ that makes the insulin is normal.
Abnormal Anatomy/Normal PhysiologyA person can have abnormal anatomy but normal physiology. For instance, a healthy dwarf has abnormal anatomy but normal physiology. The anatomy is abnormal, but it functions normally.
Abnormal Anatomy/Abnormal PhysiologyWhen an anatomic abnormality lasts long enough, it may lead to a physiologic abnormality. For example, in early alcoholism, the liver changes by containing more fat and enlarging. These are anatomic abnormalities. The function is normal. If alcoholism continues long enough, the liver slowly stops functioning. This is a physiologic abnormality.
On the other hand, when a physiologic abnormality lasts long enough, it may lead to an anatomic abnormality. For example, at the start of a cold, you have sniffles and a loss of smell. These are physiologic abnormalities. The function of the nose is abnormal. The anatomy of the nose, its size and color, is normal. Later, you may have a swollen, red nose from the cold. Swelling and redness are pathologic changes in anatomy. Because swelling and redness are changes in size and color, they also can be called morphologic changes.
For most disease processes, anatomy and physiology both are abnormal by the time a diagnosis is made. For example, in the early stages of alcoholism, the liver functions well, and the liver function tests are normal. The diagnosis of alcoholic liver disease usually is not made. The patient feels fine and cannot believe that the liver is abnormal. When both the anatomy and physiology are pathologic, the patient feels sick, and the liver function tests are abnormal. So you can see that the diagnosis is not usually made until both the anatomy and physiology are pathologic.
Likewise, in the early stages of a cold, when you just have sniffles, you say, “I think I’m getting a cold.” When your nose is red, swollen, stuffy and runny, you say, “I have a cold.” Again, the diagnosis isn’t usually made until both anatomy and physiology are abnormal.
So even though diseases can be divided into anatomic pathology and pathophysiology, medicine often deals with both anatomic and physiologic pathology at the same time.

0201604LB02A-08-14
Medical Coding Specialist
8-6
Step 5: Practice Exercise 8-1 Determine the term(s) to complete each sentence, and write your answers on scratch paper.
1. Anatomy, physiology and pathology are included in the study of life called human _____.
2. The study of the form of an organ, such as size, shape or color, is called _____.
3. The science of the appearance and relationships of body parts is called _____.
4. The study of the function of body parts is called _____.
5. The study of disease is called _____.
6. The study of tissues is called _____.
7. The science of the appearance of cells and tissues is called _____.
8. To see a cell, you would use an instrument called a(n) _____.
9. Changes in the function of an organ are called _____ changes.
10. The disease changes you see in an organ are called _____ changes.
Step 6: Review Practice Exercise 8-1Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 7: Beginning Anatomy and Physiology ConceptsNow that you have a basic understanding of human biology, you are ready to move on to the more specific science of anatomy and physiology. Anatomy and physiology are two key components in the medical world. Remember:
● Anatomy refers to the structure of the body—the appearance and relationships of body parts, such as muscles, bones, organs and other systems.
● Physiology is the study of how these body parts work together to sustain life—the functions of the body and its organs, tissues and cells.
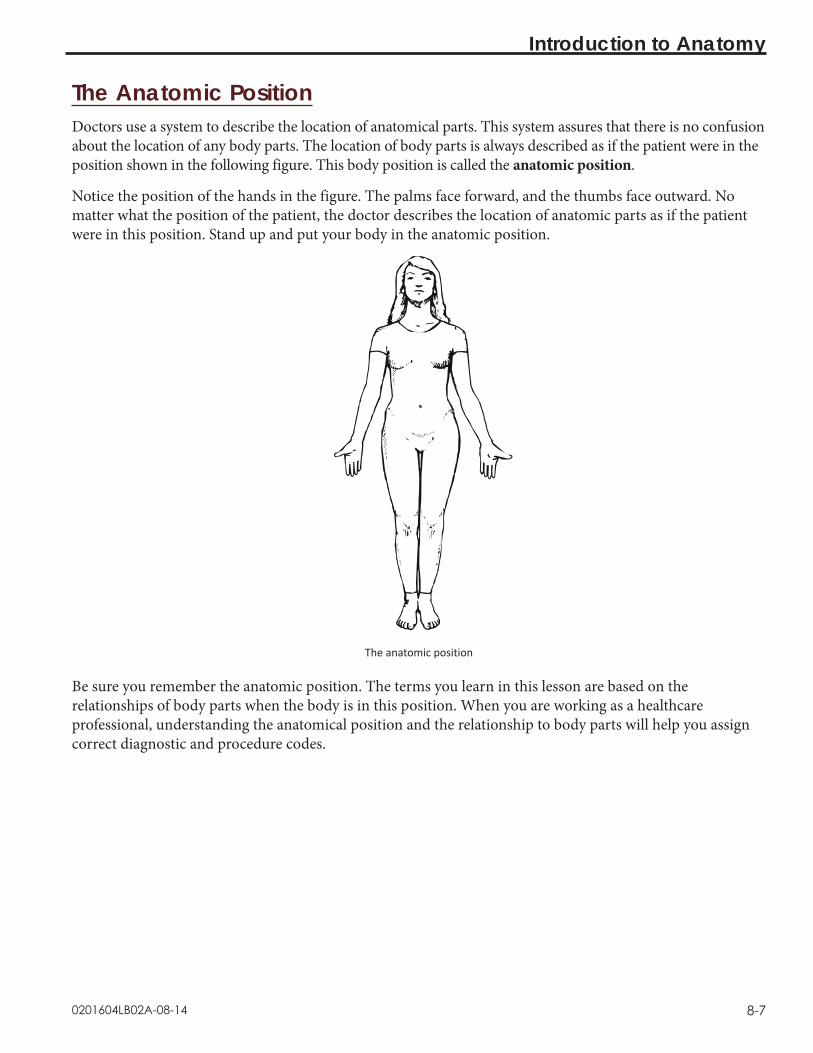
0201604LB02A-08-14
Introduction to Anatomy
8-7
The Anatomic PositionDoctors use a system to describe the location of anatomical parts. This system assures that there is no confusion about the location of any body parts. The location of body parts is always described as if the patient were in the position shown in the following figure. This body position is called the anatomic position.
Notice the position of the hands in the figure. The palms face forward, and the thumbs face outward. No matter what the position of the patient, the doctor describes the location of anatomic parts as if the patient were in this position. Stand up and put your body in the anatomic position.
The anatomic position
Be sure you remember the anatomic position. The terms you learn in this lesson are based on the relationships of body parts when the body is in this position. When you are working as a healthcare professional, understanding the anatomical position and the relationship to body parts will help you assign correct diagnostic and procedure codes.

0201604LB02A-08-14
Medical Coding Specialist
8-8
Planes and Sections of the Human BodyThe human body has three dimensions: height, width and depth.
Facts About Dividing the BodyThe body can be divided in three different ways:
♦ Superior and inferior (top and bottom) sections
♦ Right and left sections
♦ Anterior and posterior (front and back) sections
Dividing the body like this helps you understand where organs or parts are located. You can divide the body into these sections by making a mental “slice” or “cut.”
Transverse Planes and SectionsThe transverse or horizontal plane divides the body into superior (above) and inferior (below) sections. A transverse plane can be made anywhere in the body from the feet to the head.
● A transverse plane made at the neck divides the body into superior and inferior sections. The head is superior to the plane. The chest, arms, abdomen and legs lie inferior to the plane.
● A transverse plane made at the waist also divides the body into superior and inferior portions. The head, chest and arms are superior to the plane. The pelvis and legs are inferior to the plane.
● A transverse plane made at the level of the knees divides the body into superior and inferior sections, too. The thighs, abdomen, chest, arms and head are superior to the plane. The calves and toes are inferior to the plane.
Transverse sections

0201604LB02A-08-14
Introduction to Anatomy
8-9
Sagittal Planes and SectionsA sagittal or longitudinal plane divides the body into right and left sections. A midsagittal or median plane divides the body into equal right and left sections. A midsagittal plane is the midline of the body. A parasagittal plane divides the body into unequal right and left sections. A sagittal plane can be made at any point of the body from the right side to left side.
Sagittal sections
Coronal Planes and SectionsA coronal or frontal plane divides the body into anterior (front) and posterior (back) sections. A coronal plane can be made at any point from the front of the body to the back of the body.
● A coronal plane at the level of the ears divides the body into anterior and posterior sections. The face, abdomen and knees are anterior to the plane. The back, buttocks and ankles are posterior to the plane.
● A coronal plane at the level of the nose divides the body into anterior and posterior sections. The nose is anterior to the plane. Almost everything else is posterior to the plane.

0201604LB02A-08-14
Medical Coding Specialist
8-10
Coronal sections
Planes and SectionsYou can divide the body and each organ using planes. For example, a parasagittal plane of the liver divides the liver into unequal left and right sections.
A parasagittal plane of the liver
Study the definitions of these planes until you can form a mental image of them. You’ll remember these concepts more easily if you picture the planes using your own body.

0201604LB02A-08-14
Introduction to Anatomy
8-11
Step 8: Practice Exercise 8-2Determine the term(s) that fit the context of each sentence, and write your answers on scratch paper.
1. When the arms are at the side, the palms of the hands face forward and the thumbs point outward, the body is in the _____.
2. A(n) _____ plane also is called a horizontal plane.
3. A(n) _____ plane divides the body into unequal left and right sections.
4. A frontal plane also is called a _____ plane.
5. A(n) _____ or horizontal plane divides the body into superior and inferior sections.
6. A longitudinal plane also is called a(n) _____ plane.
7. A(n) _____ or frontal plane divides the body into anterior and posterior sections.
8. A(n) _____ or median plane divides the body into equal left and right sections.
9. A midsagittal plane also is called a(n) _____ plane.
10. A plane divides the body or organ into _____.
Step 9: Review Practice Exercise 8-2Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 10: Location TermsThe location terms you learn in this lesson are important to you because doctors use them to describe what they see when they examine a patient. You will learn how to pronounce the terms later in this lesson.
When doctors describe the location of anatomic parts, they use terms that compare the location of one part to another part. A number of terms describe the relative location of body parts and organs. These terms rely on the anatomical position and the anatomic sections you just learned.
Facts About Location TermsThese terms usually come in antonym pairs. Each word of an antonym pair means the opposite of the other word, such as the antonym pairs above and below or left and right.

0201604LB02A-08-14
Medical Coding Specialist
8-12
Transverse plane
If you draw a transverse plane through the body or an organ, these words describe anything above or below that plane.
● Superior means above.
● Inferior means below.
● Cephalad means toward the top of the head.
● Caudad means toward the soles of the feet.
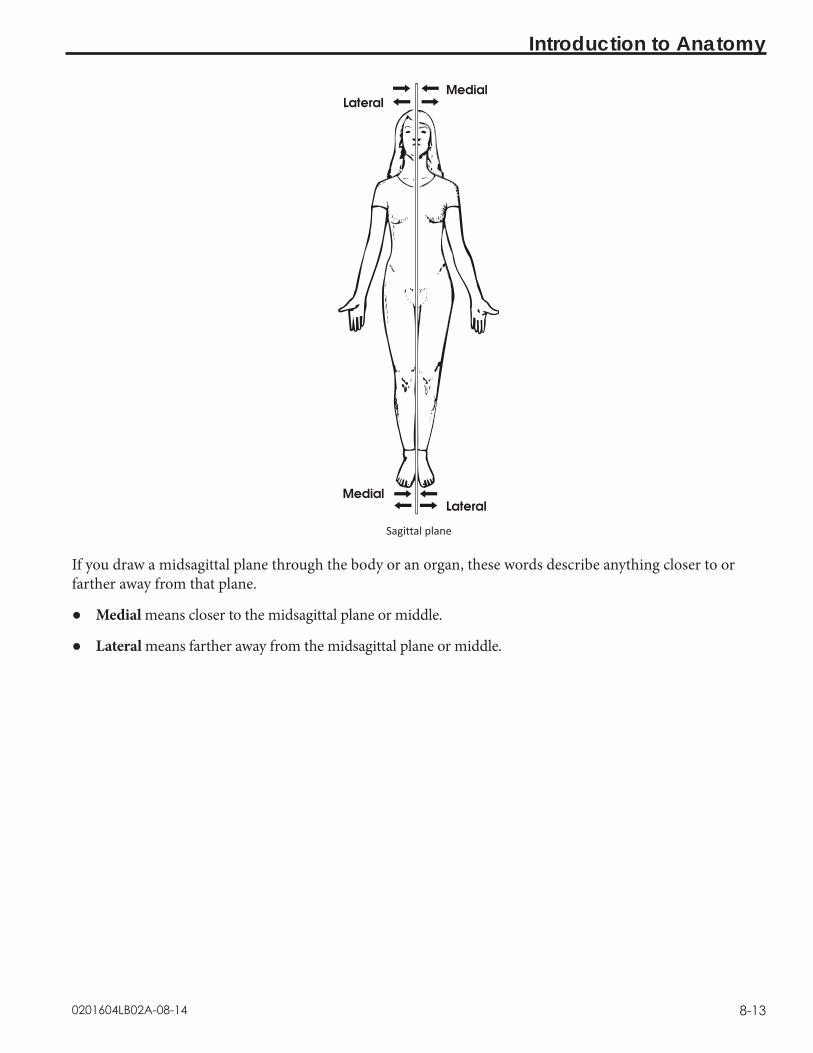
0201604LB02A-08-14
Introduction to Anatomy
8-13
Sagittal plane
If you draw a midsagittal plane through the body or an organ, these words describe anything closer to or farther away from that plane.
● Medial means closer to the midsagittal plane or middle.
● Lateral means farther away from the midsagittal plane or middle.

0201604LB02A-08-14
Medical Coding Specialist
8-14
Coronal plane
If you draw a coronal plane through the body or an organ, these words describe anything in front of or behind that plane.
● Anterior means in front of.
● Posterior means in back of.
● Ventral means on the belly side.
● Dorsal means on the back side.

0201604LB02A-08-14
Introduction to Anatomy
8-15
The following chart summarizes these location terms and how they are used.

0201604LB02A-08-14
Medical Coding Specialist
8-16
Look at some sentences showing how these words are used. Compare these statements to your own body. Be sure your body is in the anatomic position when you do so.
The lungs are superior to the liver.
The liver is inferior to the heart.
The incision was made in a cephalad direction.
The arteries for the lower extremities travel in a caudad direction.
The nose is medial to the eye.
The right thumb is lateral to the right index finger.
The sternum is anterior to the heart.
The lungs are posterior to the sternum.
The ventral hernia was repaired.
The spine is dorsal to the stomach.
The following terms are used for the body or an organ as a whole. They describe parts that are nearer the center or parts that are nearer the surface of the body or an organ. Examples of how these words are used follow the terms.
● Proximal means nearer to the center of the body or organ.
The knee is proximal to the foot.
● Distal means farther away from the center of the body or organ.
The foot is distal to the knee.
● Superficial means on or closer to the skin or surface of an organ.
The wound was superficial, not involving the muscles, and did not require sutures.
● Deep means under or farther away from the skin or surface of an organ.
The wound was deep and penetrated the liver.
● Central means within or near the center.
The heart is central within the rib cage.
● Peripheral means at or near the rim or edge.
The peripheral veins of the arms and hands can be seen easily.
● Parietal means the outer wall of a body cavity.
The parietal pleura forms the outer layer that surrounds the lungs.

0201604LB02A-08-14
Introduction to Anatomy
8-17
● Visceral means the covering of an organ.
The visceral pleura covers the lungs.
● External means outside or closer to the skin or surface of an organ.
The pericardium is external to the heart.
● Internal means inside or farther away from the skin or surface of an organ.
The lungs are internal to the ribs.
● Ipsilateral means situated on or affecting the same side of the body.
The left leg and left arm are ipsilateral.
● Contralateral means situated on or affecting the opposite side of the body.
The right leg and left arm are contralateral.
Some things in the body, like blood cells, fluid or nerve messages, can move. The next two terms describe body parts that carry things that move.
● Afferent means carrying toward a body part or the center of an organ.
An afferent neuron is a nerve that carries nerve messages to the brain from a muscle.
● Efferent means carrying away from a body part or the center of an organ.
An efferent neuron is a nerve that carries nerve messages away from the brain to a muscle.
Step 11: Pronounce New TermsFollow these steps:
a. Take your Quick-Learn Tutor and your Set 9 flashcards out of your Quick-Learn Kit. Insert the first flashcard for Set 9 into Side A of the Tutor.
b. Access your pronunciation audio and play the files for Flashcard Set 9.c. Listen to the flashterm. Put the audio on pause. d. Practice pronouncing the term out loud. Take your time. Push the flashcard up and read the
meaning of the word part or term.e. Do this for each term in this set. f. Put the flashcards in order and play the audio again, pronouncing each word part or term
after you hear it on the audio. Don’t forget to listen to your own pronunciation of each term. If you mispronounce one, put a check mark next to that flashterm.
g. Practice the terms you mispronounced by listening again. Be sure you can pronounce the terms clearly and easily.
0201604LB02A-08-14
Medical Coding Specialist
8-18
Step 12: Write New TermsFollow these steps:
a. Insert the first flashcard for this set into Side A of your Quick-Learn Tutor.b. Look at each term as it appears in the window and say it out loud. Write the flashterm on
scratch paper. Remember to include the slash if it is a word part.c. Push the card up until the meaning appears in the right window and read the meaning out
loud. Write the meaning beside the flashterm. d. Do this for each term.
Step 13: Meanings of New Terms Follow these steps:
a. Again insert the first flashcard into Side A of your Quick-Learn Tutor. Pronounce each word part or term and then say the meaning. Check yourself by pushing the flashcard up until you can see the meaning in the right window.
b. Now insert the flashcard into Side B of your Quick-Learn Tutor. Push the card up until you see the meaning of the first flashterm in the right window. Read each meaning out loud, and then say the term. Again, check yourself by pushing the flashcard up until you can see the term in the left window.
c. Practice with the flashcards several times until you are familiar with the flashterms and their meanings. You may use the flashcards for the Practice Exercises and Quizzes.
d. When you feel comfortable with the spelling, pronunciation and meaning of each flashterm, go on to the next step.
Step 14: Organ and Organ SystemsNow that you’ve laid a foundation in basic anatomy concepts, let’s take a look at the body’s major organs and organ systems.
Tissues are grouped together to form an organ. In an organ, all the tissues work as a team. Each type of tissue has its own job to do, but together the tissues have a common purpose: the function of the organ.
Each type of tissue does its own job. For example, the liver contains tissues from each of the basic tissue groups (epithelium, connective, muscle, nervous). The epithelium covers and protects the organ and makes the glands of the organ. Connective tissue holds the organ together and provides support or repair. Muscle tissue provides motion, contraction or pressure in ducts and vessels. Nervous tissue provides connection to the brain and warning of danger. Then, all the groups of tissues in the liver work together to perform the functions of the liver.
In the same way, the heart contains tissues from each of the tissue groups, all acting together to perform the function of the heart. However, from a practical point of view, when a patient has a problem, the problem is not with a tissue type but with a particular organ, such as the liver or the heart.
0201604LB02A-08-14
Introduction to Anatomy
8-19
An organ usually interacts with other organs that help it perform its function. For example, the liver, pancreas, stomach and bowel are organs that all work together to digest food. Thus, organs with similar functions or physiology are grouped together in organ systems. In fact, the different specialties of medicine represent the various organ systems. You can probably recognize some of these systems and areas of specialization already.
Respiratory SystemThe respiratory system is the gas exchange system that provides oxygen to the body while removing the by-product of oxygen metabolism, carbon dioxide. The body as a whole cannot do without oxygen for more than three to five minutes because a lack of oxygen to the most sensitive parts of the body—the brain and the heart—can cause permanent, if not fatal, damage.
Circulatory/Cardiovascular SystemThe cardiovascular system is the supply transportation system for the body. It brings nutrients like oxygen, glucose, amino acids and hormones to all the cells in the body and carries off the waste products of cell metabolism. The cardiovascular system includes the heart, blood vessels, lymph vessels and the blood or lymph they contain.
The heart is like the dispatcher, sending blood out in regular shipments through all the organs and cells of the body. The vascular system includes arteries, veins, capillaries and lymph channels, which are like highways and city streets. They provide a well-planned flow to and from delivery and pick up points. The blood and lymph do the actual transporting of all these materials to and from their destinations. Each type of cell specializes in the supplies and waste materials it transports.
Nervous SystemThe nervous or neurological system includes the central nervous system, which is made up of the brain and spinal cord, and the peripheral nervous system, which includes the nerves that reach each organ in the body. Because this system includes the mind, it can also be called the neuropsychiatric system.
Muscular SystemThe muscular system consists of organs that produce movement as they contract and relax. Muscles are not only in the extremities, such as the biceps muscle that bulges when you flex your elbow, but also in almost every other organ system in the body except the neurological system. The muscular system also includes the tendons and aponeuroses, which is connective tissue that attaches the ends of muscles to bones.
Skeletal SystemThe skeletal system includes bones, joints, cartilage and spine. Since it is so difficult to separate the functions of the voluntary muscles and bones, some people combine the muscular and skeletal organ systems into one system, the musculoskeletal system. Most people think bones aren’t living tissue, but rather something hard, like a rock. But each bone in your body is a living organ, just like your heart.

0201604LB02A-08-14
Medical Coding Specialist
8-20
Integumentary SystemThe integumentary system includes skin, nails, hair, sweat and sebaceous glands. Integument means in the covering or in the skin. The skin and the organs the skin contains are part of this system. The skin is the largest single organ in the body! This fact explains why a large skin injury, such as a burn, can be fatal.
Endocrine SystemThe endocrine system includes the glands that don’t have ducts. These glands secrete within themselves directly into their blood vessels. Endocrine glands are made of epithelium tissue. They secrete hormones. Endocrine glands include the thyroid, parathyroid, pituitary and adrenal glands as well as the hypothalmus, pancreas, testes and ovaries. The testes and ovaries are also part of the reproductive system.
Digestive SystemThe digestive system is concerned with digestion of food. This system begins with the mouth and ends at the anus. The stomach, intestines, liver, pancreas, mouth and esophagus all belong to the digestive system. This system is also called the gastrointestinal system.
Urinary SystemThe urinary system filters the blood and produces urine. It includes the kidneys, ureters, urinary bladder and urethra.
Reproductive SystemThis organ system involves the organs for reproduction. The reproductive system includes such organs as the ovaries, uterus, vagina, breasts, testes and penis.
The Immune SystemOne system you may not have heard about is the immune or immunologic system. That is because this system that defends the body from disease is not clearly understood. The immune system appears to use parts of the cardiovascular system, the nervous system and the endocrine system to provide defense against some kinds of disease. The immune system provides immunity, or resistance, to diseases caused by stress, viruses and degeneration. This system helps fight cancer and tries to kill any foreign substance in the body, even a transplanted organ.

0201604LB02A-08-14
Introduction to Anatomy
8-21
Step 15: Practice Exercise 8-3For each sentence, write the bracketed term on scratch paper that will make the sentence true. You may refer to the drawings in the text. Answer all questions as they pertain to the anatomic position.
1. The hand is [caudad cephalad] to the elbow.
2. Separating the body into right and left halves is called a [sagittal coronal] plane.
3. The knee is [superior inferior] or [caudad cephalad] to the chest.
4. The belly button is [anterior posterior] to the spine.
5. A blood vessel that carries blood away from the heart is called an [efferent afferent] vessel.
6. In the anatomic position, the palms of the hands are [posterior anterior] to the backs of the hands.
7. The nose is [lateral medial] to the eyes.
8. The buttocks are [ventral dorsal] and [cephalad caudad] to the breastbone.
Step 16: Review Practice Exercise 8-3Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 17: Lesson SummaryThis lesson brings you along in your journey to become an effective healthcare professional. Anatomy is an integral part of every aspect of medicine, so the ability to recognize terms and their medical context makes you a valuable member of the healthcare team.
This lesson explained the basics of human biology—the study of how the body is put together and how it works in health and disease. Human biology in the healthy state includes anatomy and physiology. Human biology in disease deals with pathology.
You learned that anatomy is the science of the structure of the body, including the appearance and relationships of body parts. The two kinds of anatomy are macroscopic anatomy and microscopic anatomy. Physiology is the study of how the body works; it describes the function of the body and its organs, tissues and cells. Physiology also can be divided into macroscopic physiology, which usually is called gross physiology, and microscopic physiology, which usually is called cell physiology.
We explained that pathology is the study of human biology when anatomy and/or physiology are abnormal. Abnormal physiology sometimes is called pathophysiology. Abnormal anatomy is called pathology or pathologic anatomy. When doctors describe the location of anatomic parts, they refer to the anatomic position and the anatomic sections with the corresponding anatomic planes. There also are specific location terms that doctors use to describe the relative locations of body parts and organs.
0201604LB02A-08-14
Medical Coding Specialist
8-22
As you continue with the next few lessons, keep in mind that everything you learn about the human body will help you in your new career. You are learning terms you will see in your daily work with physicians and other healthcare professionals.
Step 18: Quiz 8Once you’ve mastered the course content, locate this Quiz in your Online Course or your Assignment Pack. Read and follow the Quiz instructions carefully.

Lesson 9Anatomy: Landmarks and Divisions
Step 1: Learning Objectives for Lesson 9When you have completed the instruction in this lesson, you will be trained to:
● Discuss landmarks and divisions as they apply to anatomy.
● Talk about the basic body cavities.
● Explain how the body is organized.
Step 2: Lesson PreviewIn previous lessons you learned some of the language that goes along with the medical field. In this lesson, we’ll talk about the body—how it works, how it is organized and how its systems are connected.
Don’t worry if you don’t remember everything about this lesson. It is an introduction designed to give you a knowledge base. This base enables you to understand what medical providers face every day. As a medical coding specialist, you need this basic understanding to communicate with doctors and other healthcare professionals in your work just as you need to understand the medical terminology we talked about in previous lessons.
Step 3: Gross AnatomyContrary to what you might think, gross anatomy does not mean disgusting anatomy! Instead, as you learned in the previous lesson, it refers to the study of body parts and systems that can be seen without the aid of a microscope. In this context, the word gross means large.
Landmarks and DivisionsWhen a doctor examines the surface of the body, he uses several gross anatomy terms to describe location. The study of the surface of the body often is called superficial anatomy. These location terms, or landmarks, have been used for hundreds of years, long before providers could see inside the body with x-ray or ultrasound machines. These terms are used every day in physical examinations, medical histories and surgery reports. As a medical coding specialist, you’re likely to encounter these terms often.

0201604LB02A-09-14
Medical Coding Specialist
9-2
Superficial Landmarks, Face UpWhen the body is supine, which means lying flat on the back, the doctor sees the anterior or ventral side of the body. Let’s look at the terms used for superficial landmarks on the anterior surface. The following figure shows the surface landmarks in the supine position. The surface landmarks are labeled. Can you find these parts on your own body? If you are not sure what a new term means, consult the list of meanings that follows the picture.
Surface landmarks, supine

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-3
Surface Landmarks, Supine Meaningfrons foreheadorbit eyebucca cheekcervix neckclavicle collarboneaxilla armpitthorax chestcostochondral margin rib and cartilageabdomen trunkumbilicus navel, bellybuttonpubis front pelvic bonefemur thighpatella kneecaptalus anklebrachium upper armantecubital fossa front of elbowantebrachium forearmcarpus wristdigit finger/toeflank side from ribs to hip boneiliac crest top rim of hip boneinguen grointibia shindigit toe/finger

0201604LB02A-09-14
Medical Coding Specialist
9-4
Superficial Landmarks, Face DownWhen the body is lying prone, or face down, the doctor sees the posterior or dorsal side of the body. The following drawing shows the surface landmarks in the prone position. The surface landmarks are labeled. Can you find these parts on your own body? You may not be able to reach all of them. Check off each landmark after you find it. If you need help, consult the list of meanings that follows the picture.
Surface landmarks, face down
Surface Landmarks, Prone Meaningcubitus elbowocciput back of headcervix neckscapula shoulder bladedorsum upper back lumbus lower backsacrum spinal bones located
between the buttocksgluteus buttockpopliteal fossa back of kneesura calfcalcaneus heelplantar surface sole of foot

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-5
Step 4: Pronounce New TermsFollow these steps:
a. Take your Quick-Learn Tutor and your Set 10 flashcards out of your Quick-Learn Kit. Insert the first flashcard for this set into Side A of the Tutor.
b. Access your pronunciation audio and play the files for Flashcard Set 10.c. Listen to the flashterm. Put the audio on pause. d. Practice pronouncing the term out loud. Take your time. Push the flashcard up and read the
meaning of the word part or term. e. Do this for each term in this set. f. Put the flashcards in order and play the audio again, pronouncing each word part or term
after you hear it on the audio. Don’t forget to listen to your own pronunciation of each term. If you mispronounce one, put a checkmark next to that flashterm.
g. Practice the terms you mispronounced by listening again. Be sure you can pronounce the terms clearly and easily.
Step 5: Write New Terms Follow these steps:
a. Insert the first flashcard into Side A of your Quick-Learn Tutor.b. Look at each term as it appears in the window and say it out loud. Write the flashterm on
blank paper. Remember to include the slash if it is a word part.c. Push the card up until the meaning appears in the right window and read the meaning out
loud. Write the meaning beside the flashterm. d. Do this for each term in this set.
Step 6: Meanings of New TermsFollow these steps:
a. Again insert the first flashcard into Side A of your Quick-Learn Tutor. Pronounce each word part or term and then say the meaning. Check yourself by pushing the flashcard up until you can see the meaning in the right window.
b. Now insert the flashcard into Side B of your Quick-Learn Tutor. Push the card up until you see the meaning of the first flashterm in the right window. Read each meaning out loud and then say the term. Again, check yourself by pushing the flashcard up until you see the term in the left window.
c. Practice with the flashcards several times until you are familiar with the word parts and terms and their meanings. You may use the flashcards for your Practice Exercises and Quizzes.
d. When you feel comfortable with the spelling, pronunciation and meaning of each flashterm, go on to the next step.

0201604LB02A-09-14
Medical Coding Specialist
9-6
Step 7: Adjective Forms for Landmark NamesSome of the landmark names you just learned probably were unfamiliar to you, but you may have heard these terms in their adjective form. Read the following chart:
Landmark Name (Noun Form) Meaning Root Word Adjective Form
frons forehead front/o frontalorbit eye orbit/o orbitalbucca cheek bucc/o buccalcervix neck cervic/o cervicalclavicle collarbone clavicul/o clavicularaxilla armpit axill/o axillarythorax chest thorac/o thoracicbrachium upper arm brachi/o brachialcarpus wrist carp/o carpaldigit finger or toe digit/o digitalabdomen trunk abdomin/o abdominalumbilicus navel, belly button umbilic/o umbilicalinguen groin inguin/o inguinalpubis front pelvic bone pub/o pubicfemur thigh femor/o femoraltibia shin tibi/o tibialpatella kneecap patell/o patellartalus ankle tal/o talarcubitus elbow cubit/o cubitalocciput back of head occipit/o occipitalscapula shoulder blade scapul/o scapulardorsum upper back dors/o dorsallumbus lower back lumb/o lumbarsacrum spine between
buttockssacr/o sacral
gluteus buttock glute/o glutealsura calf sur/o suralcalcaneus back of ankle calcane/o calcaneal

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-7
Step 8: Practice Exercise 9-1 Look at the two drawings that follow and write the correct term for each landmark indicated on scratch paper.
1.
2.
3.
4.
5.
6.
7.
8.
9.10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
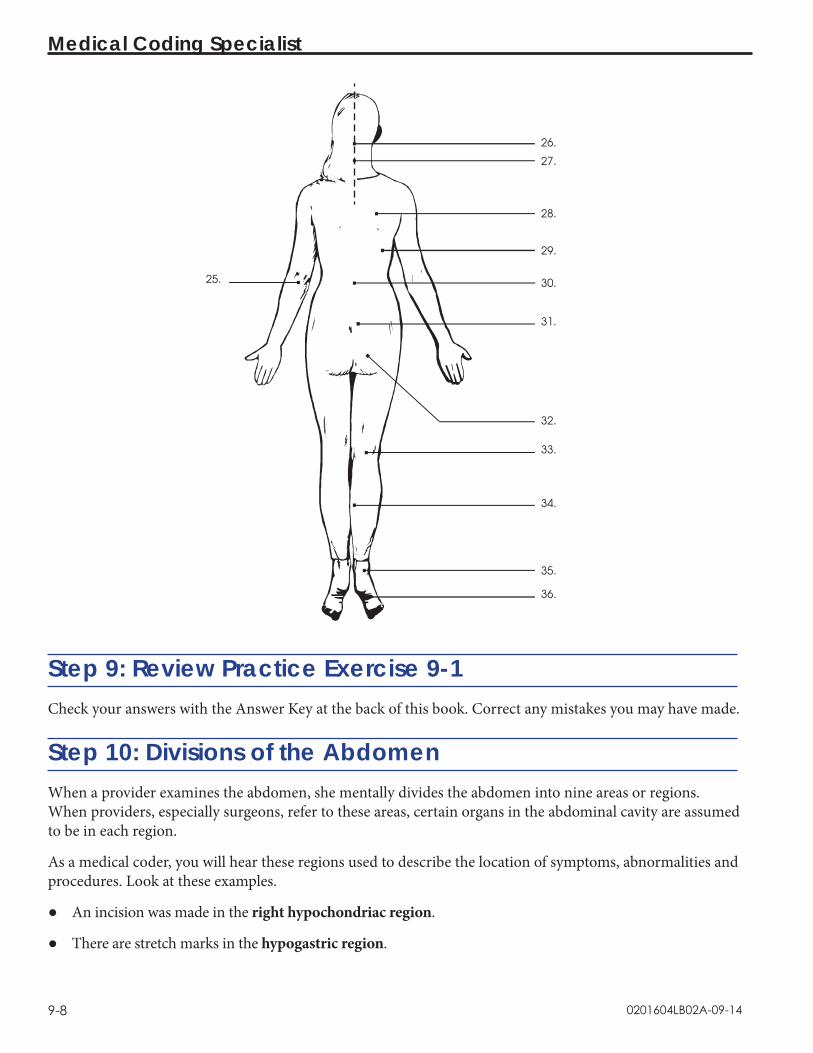
0201604LB02A-09-14
Medical Coding Specialist
9-8
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
Step 9: Review Practice Exercise 9-1Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 10: Divisions of the AbdomenWhen a provider examines the abdomen, she mentally divides the abdomen into nine areas or regions. When providers, especially surgeons, refer to these areas, certain organs in the abdominal cavity are assumed to be in each region.
As a medical coder, you will hear these regions used to describe the location of symptoms, abnormalities and procedures. Look at these examples.
● An incision was made in the right hypochondriac region.
● There are stretch marks in the hypogastric region.

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-9
These divisions are shown in the drawing that follows. Notice how the names of some regions describe the superficial landmarks where they are located. For example, two regions are named for their relationship to the location of the stomach: the epigastric region and the hypogastric region. As you look at the drawing, point out each region on your own abdomen.
Costochondrial margin
Right hypochondriac region
Right lumbar region
Iliac crest
Right iliac region
Epigastric region
Umbilical region
Hypogastric region
Stomach
Left hypochondriac region
Left lumbar region
Left iliac region
Groin
Divisions of the abdomen
An Alternative Division of the AbdomenSome providers use a simpler way to divide the abdomen. The abdomen is divided into fourths. Each of these areas is called a quadrant, which means a one-fourth section.
The divisions are made by drawing a line along the midsagittal plane (dividing left and right) and a line along the transverse plane (dividing top and bottom) at the level of the umbilicus. This is shown in the drawing that follows.
The four abdominal quadrants are named using the following words. The acronym for each quadrant also is listed.
● Right upper quadrant: RUQ ● Left upper quadrant: LUQ ● Right lower quadrant: RLQ ● Left lower quadrant: LLQ

0201604LB02A-09-14
Medical Coding Specialist
9-10
Right upper quadrant
Pelvis
Right lower quadrant
Left upper quadrant
Left lower quadrant
Umbilicus
Ribs
Quadrants of the abdomen
These terms are very important in assigning medical codes. Look at the coding example for abdominal pain in the left upper quadrant:
R10.12 Abdominal pain, left upper quadrant
Now look at the coding example for abdominal pain in the right lower quadrant:
R10.31 Abdominal pain, right lower quadrant
The location of the abdominal pain changes the code number! As you can see, healthcare professionals must be aware of the four abdominal quadrants to understand coding.
Step 11: Practice Exercise 9-2Determine the correct term(s) for each sentence, and write your answers on scratch paper. Use your flashcards or the previous drawings if you need help.
1. The abdomen may be divided into four _____.
2. The carpal bones are in the _____.
3. A finger is also called a(n) _____.

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-11
4. A break in the kneecap is called a(n) _____ fracture.
5. A buccal smear is a tissue sample taken from the inside of the _____.
6. A person who does not have a collarbone does not have a(n) _____.
7. Lymphadenopathy in the armpit is called _____ lymphadenopathy.
8. Lymphadenopathy in the groin is called _____ lymphadenopathy.
9. You can feel a pulse in the fossa anterior to the elbow, called the _____ fossa.
10. The quadrant where the appendix can cause pain is on the right below the umbilicus and is called the _____.
11. Pain in the lower back is called _____ pain.
12. When you put your hands on your hips, the bone you feel is the _____.
Step 12: Review Practice Exercise 9-2Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 13: Internal Landmarks: The Body CavitiesThe spaces within the body that contain the various internal organs are called body cavities.
Facts About Body CavitiesBody cavities have two functions:
♦ Body cavities protect the organs they contain.
♦ Body cavities keep the organs in a fairly constant location.

0201604LB02A-09-14
Medical Coding Specialist
9-12
The two principal body cavities are the dorsal body cavity and the ventral body cavity. The major body cavities are shown in this drawing.
Body cavities
The dorsal body cavity is subdivided into the cranial cavity and the spinal canal. The cranial cavity is the space inside the skull that contains the brain. The spinal canal is the cavity formed by the vertebrae. The spinal canal contains the spinal cord and the beginning of the spinal nerves. There is no real boundary between the cranial cavity and the spinal canal. The foramen magnum is the opening of the occipital bone that interconnects the two cavities.
The ventral body cavity also is subdivided into the thoracic cavity and the abdominopelvic cavity. The thoracic cavity contains smaller cavities and subdivisions. The mediastinum is a mass of tissue between the lungs extending from the sternum to the vertebral column. Included in the mediastinum is the pericardial cavity, which encloses the heart. The two pleural cavities each contain a lung. The boundary between the thoracic cavity and the abdominopelvic cavity is the muscular diaphragm, a dome-shaped muscle.
The abdominopelvic cavity consists of upper and lower portions. The upper portion is called the abdominal cavity. It contains the gallbladder, liver, spleen, stomach, small intestine, most of the large intestine, kidneys, pancreas and the ureters. The lower portion, called the pelvic cavity, contains the bladder, colon, rectum and the internal reproductive organs. There is no physical boundary between the abdominal cavity and the pelvic cavity. The imaginary boundary lies at the level of the rim of the pelvic bone.

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-13
Step 14: Membranes That Line the Body CavitiesMembranes are layers of tissue that cover organ surfaces, line body cavities and form tubes. Body membranes come from two basic tissue groups:
● epithelial tissue
● connective tissue
Epithelial Tissue MembranesEpithelial membranes are classified by where they are located in the body. Epithelial membranes include cutaneous membrane, mucous membrane and serous membrane.
Cutaneous MembraneThe outer layer of the skin is a cutaneous membrane. It is made of stratified squamous epithelium. The surface of the skin, the outer layer of the stratified squamous epithelium, dries to a tough, nonliving, keratinized layer of squamous cells that waterproofs the skin.
Mucous MembraneMucous membranes, or mucosa, line every tube or cavity that connects to the surface of the body. The mucous membranes often secrete mucus, which prevents body cavities from drying out. The digestive, respiratory, reproductive and urinary tracts all are covered with mucous membranes.
Serous MembraneSerous membranes (serosa) line the major body cavities that do not connect to the surface of the body. Serous membranes occur in pairs—the visceral layer lines the organ, and the parietal layer lines the cavity. The serous membranes secrete serous fluid or serum, which lubricates the organs and reduces friction as they glide across each other and the cavity walls.
The Thoracic Cavity MembranesThe thoracic cavity is protected by a serous membrane lining called the pleura. The serous membrane lining the pericardial cavity is the parietal pericardium. The visceral pericardium is the thin, transparent serous membrane covering the heart itself. The lungs are protected by two layers of serous membranes—the parietal pleura lines the pleural cavities, and the visceral pleura covers the lungs themselves.
The Abdominopelvic Cavity MembraneThe abdominopelvic cavity is protected by the largest serous membrane of the body, which is called the peritoneum. Unlike other membranes, the peritoneum contains large folds that bind organs to each other and to the cavity wall. The parietal peritoneum lines the cavity wall. The visceral peritoneum covers some of the organs within the cavity.
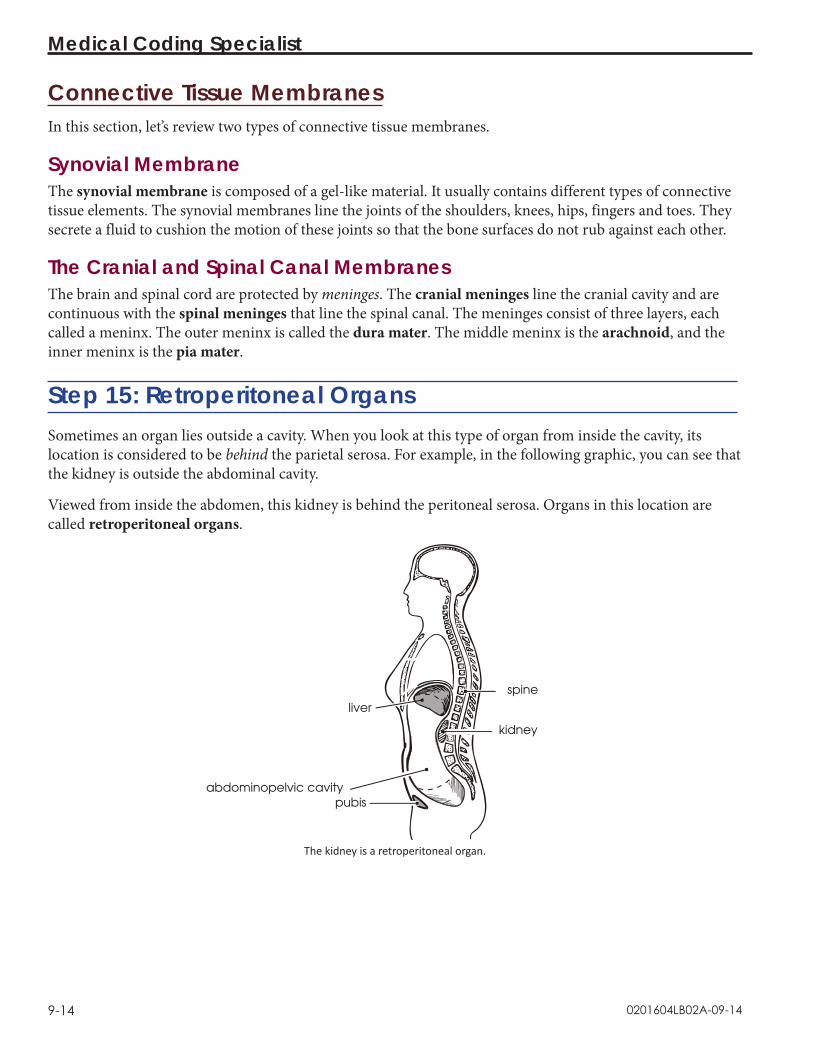
0201604LB02A-09-14
Medical Coding Specialist
9-14
Connective Tissue MembranesIn this section, let’s review two types of connective tissue membranes.
Synovial MembraneThe synovial membrane is composed of a gel-like material. It usually contains different types of connective tissue elements. The synovial membranes line the joints of the shoulders, knees, hips, fingers and toes. They secrete a fluid to cushion the motion of these joints so that the bone surfaces do not rub against each other.
The Cranial and Spinal Canal MembranesThe brain and spinal cord are protected by meninges. The cranial meninges line the cranial cavity and are continuous with the spinal meninges that line the spinal canal. The meninges consist of three layers, each called a meninx. The outer meninx is called the dura mater. The middle meninx is the arachnoid, and the inner meninx is the pia mater.
Step 15: Retroperitoneal OrgansSometimes an organ lies outside a cavity. When you look at this type of organ from inside the cavity, its location is considered to be behind the parietal serosa. For example, in the following graphic, you can see that the kidney is outside the abdominal cavity.
Viewed from inside the abdomen, this kidney is behind the peritoneal serosa. Organs in this location are called retroperitoneal organs.
Sspine
Kkidney
Aabdominopelvic cavityPpubis
Lliver
The kidney is a retroperitoneal organ.

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-15
Step 16: Pronounce New TermsYou will need to be able to understand a healthcare professional’s pronunciation of terms, and you will need to pronounce anatomical terms yourself. This exercise will help you understand and pronounce the terms you just learned.
a. Take your Quick-Learn Tutor and your Set 11 flashcards out of your Quick-Learn Kit. b. Access your pronunciation audio and play the files for Flashcard Set 11.c. Listen to the flashterm as it is pronounced on the audio. After you hear a term, put the audio
on pause.d. Practice pronouncing the term out loud. Take your time. Push the flashcard up and read the
meaning of the word part or term.e. Continue this process for each flashcard in this set.f. Put the flashcards in order and play the audio again, pronouncing each word part or term
after you hear it on the audio. Don’t forget to listen to your own pronunciation of each term. If you mispronounce one, put a check mark next to that flashterm.
g. Practice the terms you mispronounced by listening again. Be sure you can pronounce each term clearly and easily.
Step 17: Write New TermsThe next step in your lesson is to practice writing the terms you learned. Follow the instructions.
a. Insert the first flashcard for this set into Side A of your Quick-Learn Tutor.b. Look at each term as it appears in the window and say it out loud. Write the flashterm on
blank paper. Remember to include the slash if it is a word part.c. Push the card up until the meaning appears in the right window and read the meaning out
loud. Write the meaning beside the flashterm.d. Do this for each flashcard.
Step 18: Meanings of New TermsFollow these steps to learn the meanings of the terms you have pronounced and written.
a. Again insert the first flashcard into Side A of your Quick-Learn Tutor. Pronounce each word part or term out loud and then say the meaning. Check yourself by pushing the flashcard up until you can see the meaning in the right window.
b. Now insert the flashcard into Side B of your Quick-Learn Tutor. Push the card up until you see the meaning of the first flashterm in the right window. Read each meaning out loud. Before you look, see if you can remember the term that goes with that meaning. Check yourself by pushing the flashcard up until you can see the term in the left window.
c. Practice with the flashcards several times until you are familiar with the terms and their meanings. You may use the flashcards for the Practice Exercises and Quizzes.
d. When you feel comfortable with the spelling, pronunciation and meaning of each flashterm, go on to the next step.

0201604LB02A-09-14
Medical Coding Specialist
9-16
Step 19: Organization of the BodySo far, you’ve discovered how the body is organized anatomically. You learned the locations of different body parts and how the internal parts of the body are divided into cavities. Now you will study how the body is organized physiologically, that is, how the body is organized to do its work.
Your body has many tasks to perform to keep you alive. These tasks often must be performed simultaneously, and this requires great organization. Your body has to work efficiently, like an army. In any army, there are many individual soldiers, and these individuals must be organized so that various tasks can be completed. Soldiers are grouped into squads, squads are grouped into platoons, platoons are grouped into regiments, then divisions. The whole unit is called an army. The army then works with other groups, just as the U.S. Army works with the Navy, Marines and Air Force to accomplish tasks.
The smallest unit in your body is the cell. In fact, your body is composed of millions of cells. The work of the body, although it appears to be the work of large parts, is really the combined work of all the different types of cells in the body.
Similar types of cells group together to form tissues. There are four types of tissues:
● Epithelial tissue covers every body surface, including the outer surface, body cavities and organs.
● Connective tissue connects other types of tissues, helps support the body and has its own blood supply.
● Muscle tissue can extend and contract, allowing movement.
● Nervous tissue transmits electrical impulses and makes up the brain, spinal cord and peripheral nerves.
For example, muscle cells group together to form muscle tissue. Liver cells group together to form liver tissue. Nerve cells form nerve tissue.
Different types of tissue group together to form organs. For example, liver tissue, blood vessel tissue, nerve tissue and bile tissue group together to form the liver. Muscle tissue, connective tissue, nerve tissue and blood vessel tissue group together to form a muscle, such as the biceps muscle.
Body organs with similar functions can be grouped into organ systems. For example, the liver, stomach, intestines and pancreas are all organs whose function is digestion. As a group, they form the digestive system.
As you can see, body organization begins with the cell and progresses to tissues, organs and organ systems.

0201604LB02A-09-14
Anatomy: Landmarks and Divisions
9-17
Step 20: Practice Exercise 9-3On scratch paper, match each of the following term(s) with the correct definition.
1. Dorsal body cavity a. The smallest unit in your body2. Cell b. The largest serous membrane of the body3. Abdominal cavity c. Protect the brain and spinal cord 4. Peritoneum d. Layers of tissue that cover organ surfaces, line
body cavities and form tubes 5. Ventral body cavity e. Subdivided into the cranial cavity and the
spinal canal6. Membranes f. The outer layer of the skin7. Cutaneous membrane g. Line the joints of the shoulders, knees, hips,
fingers and toes8. Meninges h. Contains the gallbladder, liver, spleen, stomach,
small intestine, most of the large intestine, kidneys, pancreas and the ureters
9. Synovial membranes i. Subdivided into the thoracic cavity and the abdominopelvic cavity
Step 21: Review Practice Exercise 9-3Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 22: Lesson SummaryThis lesson continued your introduction to anatomy—how the body works, how it is organized and how its systems are connected. Providers use terms, called landmarks, to describe locations on the body. These include superficial, or surface, landmarks for the body in the supine and prone positions. To accurately describe locations on the abdomen, surgeons divide the abdomen into nine areas that refer to certain organs in the abdominal cavity in each region. A simpler way to describe locations on the abdomen is by dividing the abdomen into fourths, or quadrants.
The body is organized into a complex structure that enables it to work effectively. The smallest unit is the cell. Cells group together to form tissues, tissues group together to form organs, and organs form organ systems. These systems function as a whole to operate the amazing mechanism we call the body.
Everything you learned in this lesson is a base to help you understand the context of terminology used in the healthcare profession and to help you communicate effectively with other healthcare professionals. You don’t need to memorize the terms, but being familiar with anatomical terms will help you in your new career. You’re ready for your next Quiz.

0201604LB02A-09-14
Medical Coding Specialist
9-18
Step 23: Quiz 9Once you’ve mastered the course content, locate this Quiz in your Online Course or your Assignment Pack. Read and follow the Quiz instructions carefully.
Just for FunWhew! You need to relax after all this. Relaxation does not come automatically for many of us—often we are terrible at it. We may not realize that we are stressed mentally or physically until a problem develops.
When your body is relaxed, your mind works more efficiently. There are some very simple physical relaxation exercises you can do as you work.
● Give your eyes a rest as you work. Try the 20, 20, 20 method. Every 20 minutes, let your eyes rest on an object at least 20 feet away, and look at that object for 20 seconds.
● Every hour or so, get up out of your chair and walk. Slowly stretch your arms up over your head. Then let your head and hands hang toward the ground. Get that blood circulating!
● Watch your posture. Are you slumped over? It’s harder for your body to breathe when in a poor position. Sit up straight and take a few long, slow breaths.
● Let other areas of your body have a chance to move. Tense and then relax various muscle groups in your body as you sit. For example, tighten your gluteus maximus, hold for a few seconds and then relax. Rotate your shoulders and head. If your work area allows, stretch your legs out. Rotate your feet at the ankles.
There are many paths to relaxation and reduction of stress. Some are quite simple, others very sophisticated. A common element to all is that they be practiced regularly and that work and worries be left behind. Do any of these ideas appeal to you?
● Going for a walk
● Meditation
● Visualization exercises
● Long hot bath
● Physical exercise
● Massage
● Yoga
● Guided relaxation using audiotapes or CDs
Friends also can be great stress relievers. Plan fun times. Laugh. Laughter benefits the heart, lungs, stomach and other organs. Above all, make sure you are kind to yourself. Have some fun every day. Give yourself time off—and don’t feel guilty about it! Work when you work and then leave it. Give your mind some time off, too.

Lesson 10Cell and Tissue Anatomy and Pathology
Step 1: Learning Objectives for Lesson 10When you have completed the instruction in this lesson, you will be trained to:
● Describe the components of a cell.
● Understand the primary functions of each cell component.
● Determine the different categories of etiologies.
● Explain cell damage and how cells respond to injury.
● Determine how the body reacts to injury through inflammation, repair and damage or death.
Step 2: Lesson PreviewFrom a previous lesson you already know that the cell is the smallest unit in the human body; it’s the basic unit of life. Humans all started with one cell. That one cell changed to many different kinds of cells. But what makes up a cell? How does it function? As a healthcare professional it’s important you understand this basic component of the body and that you see how it works to allow the human body to do all of which it is capable.
In this lesson you’ll also learn about what happens when the body isn’t operating at peak efficiency. You will study the concepts of pathology and the disease process. Why is this important? You must understand how the body defends itself from disease and what mechanisms are at work in the body to promote health. Knowing why people seek medical care in the first place also will help you as you assign accurate codes to those medical records you learned about in the first pack of lessons.
Step 3: Cell Components and Their Primary FunctionsAs you know, the human body is composed of an extraordinarily large number of minute elements known as cells. Cells are the building blocks of the body. Every structure in the body is made of cells. There are, of course, different types of cells. But regardless of the type and function, all cells consist of the same basic components.
In your previous anatomy lessons you learned that a large number of combined cells with special properties form tissues. For example, certain cells form muscle tissue, and others with quite different properties form nervous tissue. These and other tissues, called connective tissues, combine to form organs, such as the heart and brain.

0201604LB02A-10-14
Medical Coding Specialist
10-2
Now you’ll learn about the parts of the cell. All cells contain a nucleus, cell membrane, cytoplasm, mitochondria, endoplasmic reticulum, lysosomes and Golgi apparatus. The following illustration shows some of these parts. Each of these structures has unique functions that are critical to the life of the cell.
Basic parts of a cell
Cell MembraneThe cell membrane or plasma membrane forms the outer surface of the cell. This membrane is made up of proteins, lipids and carbohydrates that provide energy to the cell, assist other cellular particles in moving through the cell, and assure balance. The membrane serves as the site of contact between the cell and its environment. The cell membrane’s role in the structure and integrity of the cell is invaluable because this membrane is responsible for the maintenance of all essential cellular functions. If rupture or major damage to the cell membrane occurs and cannot be repaired, the cell will die.
Cell surface

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-3
CiliaCilia are like hairs that wave in the fluid around a cell. They move the fluid and anything it contains past the cell. Cells that have cilia are called ciliated cells. For example, ciliated cells lining the trachea move mucus up and out of the lungs.
FlagellaFlagella are long single projections, like rat tails. They move a cell in the body fluids. Very few cells have flagella. The sperm cell is one that does. It has one flagellum, like a tail, to help it move in body fluids.
VilliVilli are short projections of the cell membrane that look like fingers projecting from the cell membrane. Only some cells have villi. On the other hand most cells form microvilli, which are very small villi or wrinkles in the cell membrane. Because microvilli are only wrinkles in the cell membrane, they are no different than the rest of the cell membrane. Cells form microvilli when they need them. Microvilli act like the webbing of a sponge to absorb materials transported across the cell membrane.
Step 4: More Cell Components and Their FunctionsNow that you know a little about the features on the outside of the cell, let’s talk about what goes on inside these little building blocks.
CytoplasmThe cytoplasm does most of a cell’s everyday work. Cytoplasm surrounds the nucleus, which we’ll discuss in detail in a bit, and contains other cellular structures such as mitochondria and the endoplasmic reticulum. These structures, called organelles, provide energy and nutrients and are imperative to the life of the cell.
In addition to organelles, the cytoplasm contains supplies of food and water, called inclusions or inclusion bodies. Inclusions are like little bubbles floating through the cytoplasm.

0201604LB02A-10-14
Medical Coding Specialist
10-4
The drawing that follows shows the organelles that lie in the cytoplasm. After you read about each organelle, look at the organelle in the drawing. Sometimes organelles are named for how they look.
Organelles in the cytoplasm
RibosomesThe ribosomes are where protein is made. Ribosomes either float freely in the cytoplasm or attach to the membrane called the endoplasmic reticulum.
Endoplasmic ReticulumThe endoplasmic reticulum (ER) is a spider web-type membrane inside the cytoplasm. This structure is a series of little tubes called tubules or canals that work like a subway to move materials around the cell.
There are two types of ER. Differentiated cells have either one or both types of ER. Granular ER, also called rough ER, is covered with ribosomes on its surface. This gives the ER a grainy appearance. The ribosomes use the granular ER to store and transport protein. The more protein a cell makes, the more granular ER it has to store and move the protein. Agranular ER, also called smooth ER, does not have ribosomes on its surface, so it is not grainy. It transports fatty materials called lipids. The more lipids a cell makes or handles, the more agranular ER it has to handle this job.
MitochondriaMitochondria are thread-like bodies within the cytoplasm responsible for the cell’s use of oxygen, a required element for all cells of the body to function normally. Mitochondria use oxygen to digest food in the cell. This process is called oxidation. When food is digested, there are two products: heat and energy. The energy is stored in molecules called adenosine triphosphate, or ATP. ATP provides the fuel, the energy, for all of the activities in the cell.
Mitochondria are regarded as the power plants of the cell because they exist in large numbers in those human cells that require an enormous amount of energy to do their work, such as nerve and liver cells.

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-5
LysosomesLysosomes are membrane-bound bodies, or sacs of enzymes, in the digestive part of the cell. These enzymes digest living material like debris and old organelles and allow them to enter the cytoplasm. If the lysosome sac breaks, the cell itself can be digested.
CentriolesCentrioles only are active during reproduction. They become the mitotic spindles, which pull the nucleus of a dividing cell apart to form two new cells.
Golgi Apparatus The Golgi apparatus is an organelle that packages proteins and other products of a cell for delivery to the rest of the body. Enzymes or other products of a cell are delivered to the Golgi apparatus. A sac is formed around the product and sealed off, like a heat-sealed storage bag. This sac is called a vesicle. The vesicle moves to the surface of the cell membrane, fuses with it, and bursts. The contents of the vesicle are distributed outside the cell. A vesicle acts just like a bubble in a pot of boiling water. The bubble forms, rises to the top and bursts to let the steam out of the water.
VacuoleA vacuole is any small cavity in the cytoplasm of a cell.
Step 5: The NucleusYou’ve already learned about the cell membrane, which forms the outside surface of the cell. Now let’s talk about the nucleus. The nucleus lies inside the cell and is surrounded by a nuclear membrane.
Both the cell and nuclear membranes are separate compartments filled with a gelatin-like material called protoplasm. In the cell compartment, protoplasm is called cytoplasm. Inside the nucleus, protoplasm is called karyoplasm or nucleoplasm. The suffix /plasm means growth.
DNAThe nucleus contains deoxyribonucleic acid, or DNA, which is the material that directs how the cell will run and how it will reproduce. It is made up of genes, the code for making proteins. DNA looks like a spiral staircase. Each gene is a many-stepped segment of the DNA staircase. During reproduction, the DNA coils tightly and is called a chromosome. Human cells have 23 pairs of chromosomes.
When the cell is not reproducing, the DNA is scattered throughout the nucleoplasm like pieces of lint. In this form, the DNA is called chromatin.

0201604LB02A-10-14
Medical Coding Specialist
10-6
DNA looks like a spiral staircase.
RNARibonucleic acid, or RNA, is a messenger and helper for the DNA. It shuttles the instructions for making protein from the nucleus to the cytoplasm, where the proteins actually are made.
NucleoliNucleoli are small, round bodies that make ribosomes. The ribosomes are sent out of the nucleus to the cytoplasm.
You now know about the basic components of the cell; however, before you move on, let’s take a moment to review what you’ve learned so far.
Step 6: Practice Exercise 10-1Select the best answer from the choices provided, and write your answers on scratch paper.
1. Every structure in the body is made of _____. a. ribosomesb. organsc. cellsd. nuclei
2. _____ are like hairs that wave in the fluid around a cell. a. Flagellab. Ciliac. Threadsd. Organelles

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-7
3. _____ act like the webbing of a sponge to absorb materials transported across the cell membrane.a. Villib. Microvillic. Flagellad. Cilia
4. The ribosomes make _____. a. organellesb. other cellsc. carbohydratesd. protein
5. _____ ER, also called smooth ER, does not have ribosomes on its surface.a. Agranularb. Granularc. Softd. Hard
6. Mitochondria are regarded as the _____ of the cell because they exist in large numbers in those human cells that require an enormous amount of energy to do their work.a. power plantsb. nucleusc. braind. heaviest part
7. _____ are only active during reproduction. a. Vacuolesb. Lysosomesc. Centriolesd. Mitochondria
8. A vacuole is any small cavity in the _____ of a cell.a. Golgi apparatusb. nucleusc. membraned. cytoplasm

0201604LB02A-10-14
Medical Coding Specialist
10-8
9. DNA stands for _____.a. denucleus acidb. deoxyribonucleic acidc. deoxyribonucleic action d. deribosome acid
10. RNA is _____ the DNA.a. a messenger forb. an enemy ofc. the same asd. another name for
Step 7: Review Practice Exercise 10-1Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 8: Pronounce New TermsFollow these steps:
a. Take your Quick-Learn Tutor and your Set 12 flashcards out of your Quick-Learn Kit. Insert the first flashcard for this lesson into Side A of the Tutor.
b. Access your pronunciation audio and play the files for Flashcard Set 12.c. Listen to the flashterm. Put the audio on pause. d. Practice pronouncing the term out loud. Take your time. Push the flashcard up and read the
meaning of the word part or term. e. Do this for each term in this set. f. Put the flashcards in order and play the audio again, pronouncing each word part or term
after you hear it on the audio. Don’t forget to listen to your own pronunciation of each term. If you mispronounce one, put a check mark next to that flashterm.
g. Practice the terms you mispronounced by listening again. Be sure you can pronounce the terms clearly and easily.
Step 9: Write New Terms Follow these steps:
a. Insert the first flashcard into Side A of your Quick-Learn Tutor.b. Look at each term as it appears in the window and say it out loud. Write the flashterm on
scratch paper. Remember to include the slash if it is a word part.c. Push the card up until the meaning appears in the right window and read the meaning out
loud. Write the meaning beside the flashterm. d. Do this for each term in this set.

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-9
Step 10: Meanings of New TermsDo the following steps:
a. Again insert the first flashcard into Side A of your Quick-Learn Tutor. Pronounce each word part or term and then say the meaning. Check yourself by pushing the flashcard up until you see the meaning in the right window.
b. Now insert the flashcard into Side B of your Quick-Learn Tutor. Push the card up until you see the meaning of the first flashterm in the right window. Read each meaning out loud and then say the term. Again, check yourself by pushing the flashcard up until you see the term in the left window.
c. Practice with the flashcards several times, until you are familiar with the word parts and terms and their meanings. You may use the flashcards for your Practice Exercises and Quizzes.
d. When you feel comfortable with the spelling, pronunciation and meaning of each term or word part, go on to the next step.
Step 11: Cell PathologyNow that you have read about cell anatomy and know how cells function when they are healthy, let’s talk about pathology. From a previous lesson, you know that pathology is the study of human biology when anatomy and/or physiology are abnormal.
Even though pathology means the process of studying disease, disease does not cause all pathologic processes. Instead, pathology may be a result of an injury. In some cases, pathology may be due to an abnormality of growth.
The type of abnormality seen in tissues and organs is determined by two factors.
● The cause of the abnormalityFor example, diseases injure tissue. Trauma can injure tissue. Growth or development abnormalities don’t injure tissue but can cause a tissue to look or act differently than normal. The cause of an abnormality or injury is called the etiology.
● How a tissue responds to injury Each type of tissue only can respond to injury in a few limited ways. For example, bone can break, but it doesn’t swell. Muscle tissue can’t break, but it can be torn, and it can swell. Both bone and fat can develop pus in an infection.
Step 12: EtiologiesEtiologies, the causes of pathology, can be put into categories. Doctors use these categories to help themselves remember the kinds of etiologies there are for each abnormality they find. When doctors don’t know the exact cause of an abnormality, they may use the name of the category.
The basic categories follow.

0201604LB02A-10-14
Medical Coding Specialist
10-10
Developmental AbnormalityThis category includes abnormalities in the growth or development of a particular tissue or organ. Developmental abnormalities have etiologies that are either hereditary, congenital or acquired.
Hereditary etiologies are genetic. They exist because there is an abnormality in one of the genes that was passed down from a parent. The abnormality is inherited. For example, some dwarves have abnormal bone development caused by an abnormal gene.
Congenital etiologies exist from birth. They are not inherited but exist because of an abnormality that occurred while the fetus was developing. An example is hydrocephalus, which means “water on the brain.”
An acquired etiology is an abnormality that the person “got” after birth and did not inherit from a parent. An example of an acquired developmental abnormality is childhood rickets, which is caused by a diet that does not have enough vitamin D.
Inflammatory DiseaseInflammation is a common tissue response to any kind of tissue injury: infection, trauma or disease. However, if the cause or etiology of a widespread inflammation is not known, the condition is classified as an inflammatory disease. Rheumatoid arthritis would fall into this category because it is not caused by infection, trauma or another disease.
Infection is caused by the action of bacteria, viruses and parasites. These living organisms and viruses invade the body and cause disease as long as they are alive and reproducing in the human body. Antibiotics only work on infectious diseases caused by bacteria. They do not work for viral infections or parasitic infestations.
Trauma is injury caused by the inappropriate application of force or toxic agents. An automobile accident can cause traumatic injuries. A chemical burn is trauma. For example, swallowing lye causes traumatic injury. The word trauma is used to mean that the tissue or organ injury was not due to infection or disease.
Hyperplasia and NeoplasiaThis category includes conditions that have an abnormal increase in the number of cells in a tissue or an organ. Hyperplasia means an increase in the number of normal cells, usually due to a reaction from an outside irritation. The anatomy and physiology of hyperplastic cells is normal.
Neoplasia is a new growth of cells whose anatomy is very abnormal. These cells are bizarre versions of normal cells. Neoplastic cell physiology is abnormal, especially the rate of reproduction. If a neoplasm grows slowly and does not spread or destroy normal organ function, it is called a benign neoplasm. If neoplasms grow rapidly, spread quickly, and destroy normal organ function, they are called malignant neoplasms or cancers.
As a medical coding specialist you must know if a neoplasm is benign or malignant to arrive at the correct code. This information will be documented in the patient’s medical record.

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-11
Look at these coding examples of a benign and malignant breast neoplasm for a woman:
D24.1 Benign neoplasm of right breast
C50.911 Malignant neoplasm of unspecified site of right female breast
Do you see the importance in knowing the difference between a benign and malignant neoplasm? Good! You are developing the skills needed to become a successful healthcare professional.
Metabolic DiseaseAbnormalities in the function, or physiology, of cells and tissues cause these diseases or conditions. They are due to abnormal metabolism of cells or tissues. Unlike neoplasia, the rate of cell reproduction is normal. Sometimes metabolic diseases are genetic or congenital. Sometimes they occur later in life and are called acquired, meaning the body was normal at birth and up to the time the patient developed the abnormality. Diabetes mellitus is a disease caused by abnormal sugar metabolism.
Vascular DiseaseConditions that cause bleeding, blood vessel blockage or abnormal blood flow fall in the category of vascular disease. Atherosclerosis, or hardening of the arteries, is a good example. Diabetes mellitus, even though it has a metabolic etiology, causes abnormalities of the blood vessels. It can be categorized as a vascular disease for this reason.
Immunologic DiseaseImmunologic diseases include abnormalities of the immune system. An allergy is a good example. Allergies like hayfever and drug reactions are included in this category. Some patients are allergic to their own tissues, which causes tissue injury. This condition is called an autoimmune disease.
Idiopathic AbnormalityIdiopathic is a term used for any diseases or conditions where the etiology is unknown. For example, the causes of many cancers or diabetes are unknown. The idiopathic category is for a pathology that doesn’t have a known etiology or won’t fit into any other category.
Iatrogenic AbnormalityIatrogenic pathology is caused by the actions of a doctor, treatment, procedure or medication. Have you ever had an allergic reaction to medication prescribed by a doctor? This is an example of iatrogenic pathology. Every side effect listed for a drug is an iatrogenic abnormality. In other words, if the patient had not seen a doctor or taken a medication, he wouldn’t have the iatrogenic abnormality. Iatrogenic diseases and conditions can be the same conditions found in other categories. The difference here is that the patient acquired them as a result of a medical treatment.

0201604LB02A-10-14
Medical Coding Specialist
10-12
Nosocomial DiseaseNosocomial diseases are diseases acquired in a hospital environment. A number of factors account for this. You can catch a disease from someone who already has it. Some hospital patients have lowered resistance to disease and catch things a healthy person wouldn’t normally catch. Bacteria that grow on the metal instruments in a hospital but rarely grow outside a hospital can cause unusual infections.
Step 13: Cell DamageYou’ve read about the categories of etiologies or the causes of pathology. Now, let’s look more closely at five specific ways in which cells can be damaged.
Hypoxia and Anoxia Hypoxia is the decreased availability of oxygen to the cells. Anoxia is the complete lack of oxygen. These two conditions are the most common causes of cell injury.
All humans breathe, and while breathing, oxygen is brought into the body. Other body functions serve to distribute this vital gas throughout the body, feeding the cells. When this process is interrupted, either because breathing has stopped or the body’s oxygen distribution process malfunctions, the cells immediately suffer.
Hypoxia or anoxia occurs in many circumstances, including obstruction of the respiratory tubes, such as in suffocation or drowning; reduced intake of oxygen across the respiratory surfaces of the lung, such as when one has pneumonia; inadequate transport of oxygen in the blood, such as when one has anemia; or the inability of the cell to use oxygen for respiration, such as in cyanide poisoning.
Of course, not all cells respond the same way to injury, and the final outcome of anoxia will depend on many factors. Brain cells, for example, cannot survive without oxygen for more than a few minutes, heart cells can survive one to two hours and kidney cells can survive for several hours.
Toxic Agents Toxic agents can damage cells. Poisons are toxic agents. Poisons are substances that adversely affect the body and its functions. Some poisons act by directly destroying cells. Others coat the outside of cells and keep them from interacting in their required manner. If enough poison is ingested, the cells suffer permanent injury. If enough cells are killed, then the person dies.
Poisons are often compounds and chemicals. Toxic injury is caused by substances known for their direct toxic effects on cells and by substances that are not directly toxic but that destroy cells after the body metabolizes the substances.
For example, a heavy metal, such as mercury, is directly toxic because it immediately destroys the cytoplasm of the cell. Carbon tetrachloride, a component of metal cleaning solutions (metal polish), is an indirect toxin because when digested, this poison changes characteristics and eventually affects the cell membranes.
0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-13
Drugs prescribed for medical conditions are not usually considered poisons; however, it is important to note that drugs can be toxic and can cause cell injury, especially if they are given in large amounts. Most drugs taken in large amounts are toxic, and many are even lethal. Suicide by drug overdose is probably the best example of drug-induced toxicity. However, while medical treatments for cancer, such as chemotherapy, kill the cancerous cells, they also might kill healthy cells, and they often cause toxic effects on the body. Certain drugs have side effects that might cause organ shutdown or other medical problems.
Microbial Infection Microbial pathogens or bacteria cause cell injury in several ways. Bacteria often produce toxins, which interfere with various cell functions such as respiration or protein synthesis.
Have you ever been instructed not to consume food contained in dented cans? The reason is that when a can is dented, microscopic breaks in the seal can occur, allowing bacteria to grow. This bacteria, known as a microbial pathogen, is harmful to humans.
Food poisoning is one example of how the microbes can infect human cells and damage them. A familiar scare that has occurred throughout the country in recent years is the result of E coli bacteria, a form of which can be found in meat that is not thoroughly cooked.
Another type of microbial pathogen is the virus. Certain viruses invade cells and destroy them either by disturbing various cellular processes or by changing the cell’s makeup in the nucleus or plasma membrane.
Allergic/Immune ReactionsWhen the body produces antibodies to fight infections or other invasions, the body’s own immune system can damage cells. This process often is harmless because the body regenerates new cells to replace the damaged and dead cells. However, in some rare disorders, the body’s defense mechanisms try to kill off its own cells. In such instances, these people become allergic to themselves, which is called immunopathy.
Metabolic and Genetic Disturbances Some metabolic disorders damage cells. Metabolic disturbances such as diabetes mellitus, a disease caused by insulin deficiency, produce changes in the small blood vessels of the body that cause vessel wall injury. Such injury often leads to tissue death or pathologic changes in many, if not all, body organs.
In addition to metabolic problems, genetic problems exist, whereby parents pass along defective genes to children. Some genetic problems can be dramatic and devastating. For example, Tay-Sachs disease, a genetic deficiency of a certain hormone, causes destruction of the lysosomes of nerve and eye cells. Severe mental deficiency and blindness develop, and death usually occurs in early childhood.

0201604LB02A-10-14
Medical Coding Specialist
10-14
Step 14: Practice Exercise 10-2Select the best answer from the choices provided, and write your answers on scratch paper.
1. The type of abnormality seen in tissues and organs is determined by _____ factors.a. manyb. twoc. threed. four
2. _____ are the causes of pathology.a. Geneticsb. Etiologiesc. Cellsd. Abnormalities
3. _____ is caused by the action of bacteria, viruses and parasites.a. Anoxiab. Hypoxiac. Infectiond. Inflammation
4. Hyperplasia means _____ in the number of normal cells, usually due to a reaction from an outside irritation.a. an increaseb. there is no changec. constant fluctuationd. a decrease
5. Atherosclerosis, or hardening of the arteries, is a good example of _____.a. vascular diseaseb. immunologic diseasec. metabolic diseased. a genetic disorder
6. _____ diseases are diseases acquired in a hospital environment. a. Microbialb. Iatrogenicc. Idiopathicd. Nosocomial

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-15
7. Anoxia is the complete lack of _____.a. hydrogenb. carbon dioxidec. oxygend. nitrogen
8. _____ are examples of toxic agents.a. Allergiesb. Spoiled foodsc. Abnormal genesd. Poisons
9. People who become allergic to themselves have a condition called _____. a. a genetic disturbanceb. hypoxiac. immunopathyd. ammunopathy
10. _____, a genetic deficiency of a certain hormone, causes destruction of the lysosomes of nerve and eye cells.a. Tay-Sachs diseaseb. Down syndromec. Diabetesd. Arthritis
Step 15: Review Practice Exercise 10-2Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 16: Cell Response In this step, you’ll look at how cells adapt to injury and how the cell structure might change in this healing process. You’ll also learn the natural aging process of cells that ultimately leads to cell death.
The term for when the body is not injured and cells are balanced with their environment is homeostasis. However, prolonged exposure of cells to adverse stimuli causes the cells to change. When the cause of the injury is removed, the cells often are able to heal and revert to their normal state. These minor injuries are reversible. On the other hand, some forms of adaptation, especially those associated with cell loss due to aging, such as bone loss in osteoporosis, are irreversible. Other forms of adaptation cause permanent changes in the cell size—changes that affect organ function after the cell has regenerated. Cell adaptation, a necessary process the cell undergoes to survive injury, also often causes secondary medical problems.
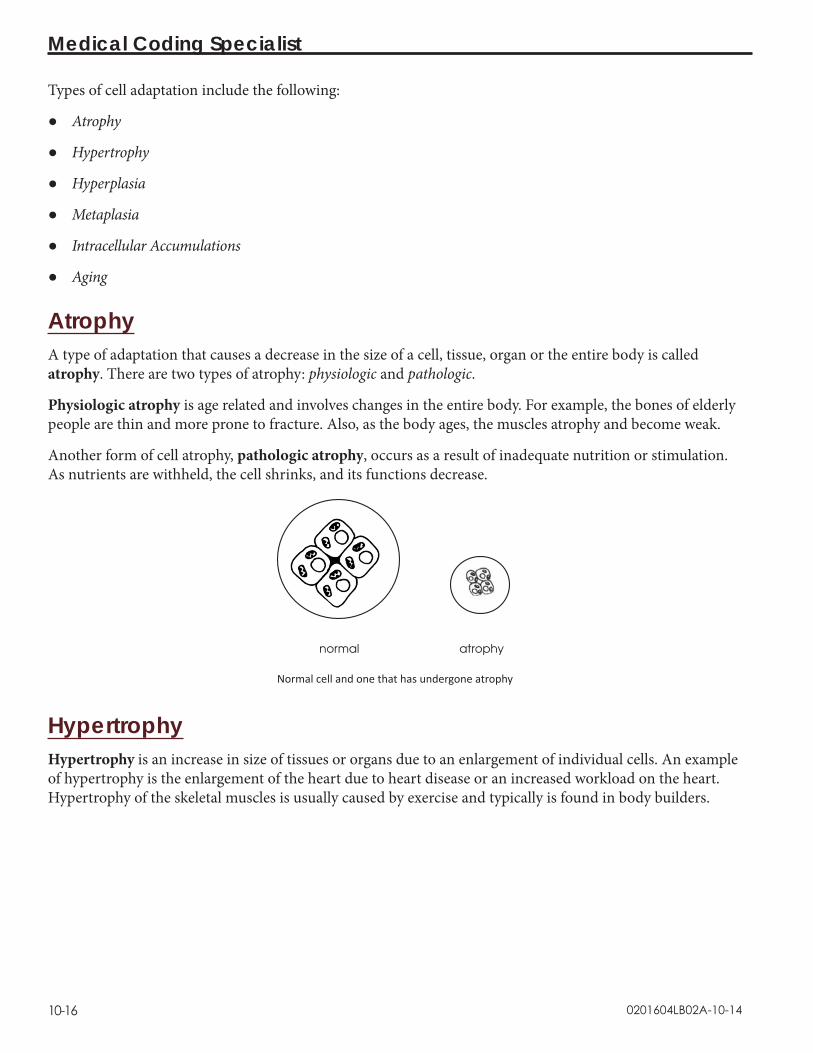
0201604LB02A-10-14
Medical Coding Specialist
10-16
Types of cell adaptation include the following:
● Atrophy
● Hypertrophy
● Hyperplasia
● Metaplasia
● Intracellular Accumulations
● Aging
Atrophy A type of adaptation that causes a decrease in the size of a cell, tissue, organ or the entire body is called atrophy. There are two types of atrophy: physiologic and pathologic.
Physiologic atrophy is age related and involves changes in the entire body. For example, the bones of elderly people are thin and more prone to fracture. Also, as the body ages, the muscles atrophy and become weak.
Another form of cell atrophy, pathologic atrophy, occurs as a result of inadequate nutrition or stimulation. As nutrients are withheld, the cell shrinks, and its functions decrease.
normal atrophy
Normal cell and one that has undergone atrophy
Hypertrophy Hypertrophy is an increase in size of tissues or organs due to an enlargement of individual cells. An example of hypertrophy is the enlargement of the heart due to heart disease or an increased workload on the heart. Hypertrophy of the skeletal muscles is usually caused by exercise and typically is found in body builders.

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-17
normal hypertrophy
Normal cell and one that has undergone hypertrophy
Would you like to see a coding example for cardiac hypertrophy?
I51.7 Cardiomegaly
If you think back to your lessons on word parts, you probably can figure out that cardiomegaly means enlargement of the heart. You know that hypertrophy increases the size of tissues or organs, so this is an accurate code.
Hyperplasia In contrast to hypertrophy, hyperplasia is an increase in the size of the tissues and organs caused by an increased number of cells, usually brought about by hormonal stimulation. Examples of hyperplasia are the thickening of the lining of a woman’s uterus due to an increase in cells (endometrial hyperplasia) and the enlargement of the prostate in elderly men.
Hyperplasia also can occur in cases of chronic injury. Sometimes the cause of hyperplasia is obvious: Chronic irritation of the foot from tight shoes causes the cells to undergo hyperplasia and form a callous or corn. Other hyperplasic lesions have no obvious cause, such as polyps or benign growths in the large intestine.
normal hyperplasia
Normal cell and one that has undergone hyperplasia
Now that you understand hyperplasia, let’s look at the diagnosis code for endometrial hyperplasia.
N85.00 Endometrial hyperplasia, unspecified
As a healthcare professional, your knowledge of cell anatomy and responses will help you succeed!

0201604LB02A-10-14
Medical Coding Specialist
10-18
MetaplasiaAnother example of cellular adaptation is metaplasia. Metaplasia occurs when cells change from one type to another. For example cigarette smoke causes the bronchial tissues to change. Metaplasia often is reversible. For example, if a person who smokes cigarettes stops smoking, their damaged lung cells can revert to their original, normal structure.
Intracellular Accumulations Intracellular accumulations might be the result of an overload of various metabolites or external materials such as a disease-producing agent, or they might be the result of metabolic disturbances. Intracellular accumulations are materials that lie immediately near the cell. These cells are attached to one another by junctions, and they communicate across these junctions. The main products of intracellular accumulations are collagen and complex sugars, which are extremely important in repairing damage to tissue and maintaining the balance of the inner cell complex.
Aging The last cell adaptation process we will talk about is the natural process of aging and death of cells. Cell aging includes many forms of adaptation and, unfortunately, many cell changes that are irreversible. Aging cannot be avoided or prevented, and the best you can do is try to lessen aging’s adverse effects on the body.
Because cells represent the basic living units of all tissues and organs, scientists know that age-related illness and eventual death are the result of cells being unable to regenerate and provide the specialized body functions necessary to sustain life.
Pathologic changes associated with aging vary from person to person. Most organs undergo atrophy and have a reduced functional reserve—that is, they cannot reproduce new cells as needed. Resistance to infection declines with advancing age, and the incidence of cancer and heart disease increases.
Before you move on, take a few minutes to complete the following Practice Exercise to review what you’ve learned so far.
Step 17: Practice Exercise 10-3Select the best answer from the choices provided, and write your answers on scratch paper.
1. The term for when the body is not injured and cells are balanced with their environment is _____.a. hypoxiab. homeostasisc. necrosisd. aging

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-19
2. Minor injuries from which the cell recovers and returns to its original state are referred to as _____.a. hyperplasiab. atrophyc. reversibled. anoxia
3. Cell atrophy that is directly related to age and involves change in the entire body is called _____.a. physiologic atrophyb. pathologic atrophyc. hyperplasic atrophyd. hypertrophy
4. Cellular adaptation that occurs when a cell changes from one type of cell to another is called _____.a. hypertrophyb. hypoxiac. metaplasiad. microbial infection
5. An increase in the size of tissues or organs caused by an increased number of cells is called _____.a. hyperplasiab. hypertrophyc. metaplasia d. metabolic disturbance
6. An increase in the size of tissues or organs due to an enlargement of individual cells is called _____.a. metaplasiab. hypoxiac. hyperplasiad. hypertrophy
7. The main products of intracellular accumulations are collagen and complex _____.a. vitaminsb. proteinsc. carbohydratesd. sugars

0201604LB02A-10-14
Medical Coding Specialist
10-20
8. _____ cannot be avoided or prevented, and the best one can do is try to lessen its adverse effects on the body.a. Inflammationb. Agingc. Diseased. Bacteria
Step 18: Review Practice Exercise 10-3Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 19: Tissue ResponseYou know how cells adapt to injury and how the cell structure might change in this healing process. But how can you tell when cellular damage has occurred? Well, let’s get started by discussing the body’s reaction to injury.
Injury to cells, tissues, or organs means that their physiology is interrupted or they are anatomically changed. When the body is injured, there are three ways tissues can respond.
● Inflammation
● Repair
● Damage or death
Tissue response

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-21
InflammationInflammation is the response of the body to injury in cells, tissues or organs. The function of the inflamed area decreases while it is inflamed. Inflammation has four symptoms or signs, rubor, calor, tumor and dolor. A symptom is what a patient feels; a sign is what a doctor observes.
RuborRubor means redness. Increased blood flow in the area causes this redness. The medical term for this is hyperemia. The blood flow increases to bring leukocytes to fight infection. Neutrophils and monocytes are two leukocytes that eat foreign materials and bacteria. Neutrophils also are called polymorphonuclear leukocytes. The slang term for neutrophils is polys; the slang term for monocytes is monos.
CalorCalor means heat. Hyperemia creates heat. Sometimes heat can kill bacteria or viruses.
Tumor Tumor means swelling. Increased fluid in the area causes swelling. The medical term for this swelling is edema, and this can occur when cells are damaged and lose water abnormally into the space surrounding the tissues. A swollen area is edematous. Tumor also means a lump. Because cancers feel like lumps, they are called tumors. But tumor only means a lump. Just because something feels tumorous, it is not necessarily a cancer.
DolorDolor means pain. Pain is caused when swelling of the tissues pinches nerve cells. There is no pain if the nerve cells have died from the injury.
Which of the four symptoms of inflammation are present or which are most noticeable depends on the severity of the injury and when it occurred.
The terms you have learned for injury also apply to the types of inflammatory response.
Acute Inflammation Acute inflammation is what most people think of as inflammation. The changes usually are very dramatic. It is a response to acute injury, pyogenic infection or severe allergy. The distinguishing feature of acute inflammation is the fluid that is produced, which is what causes swelling. Acute inflammation also may have redness, heat and pain.
The fluid of inflammation is called an exudate. An exudate is cloudy and contains protein, which leaked from damaged cells and bacteria. By comparison, a transudate is clear fluid that doesn’t contain protein. It is related to vascular disease, not inflammation.
There are several types of exudate. Serous exudate is the clear yellow fluid that oozes from burns. It has more fluid than protein.
Fibrinous exudate has a blood clotting material called fibrin, which traps bacteria in its net. Fibrinous exudate forms scabs.

0201604LB02A-10-14
Medical Coding Specialist
10-22
Purulent exudate is commonly referred to as pus. It gets its appearance from dead bacteria and neutrophils. Pyogenic means forming pus. A pyogenic infection is one that forms a purulent exudate in the acute inflammatory response. When an inflammatory response has a large amount of pus, it is called a suppurative infection. When a collection of pus is closed off in a sac by fibrous connective tissue, it is called an abscess. A small abscess is called a carbuncle.
Ulcerative and pseudomembranous inflammation are two types of acute inflammation.
Ulcerative inflammation is inflammation of the body surfaces or the mucosa of hollow organs, such as the stomach or intestines, that results in ulceration.
Pseudomembranous inflammation is a form of ulcerative inflammation combined with fibrinopurulent drainage. That is, the fluid contains fibrin, pus, cellular debris and mucus. This fluid forms a type of membrane on the surface of the ulcers.
Chronic InflammationInfections that don’t completely heal, slow injury and slow allergic irritation cause chronic inflammation. The symptoms of chronic inflammation are not as dramatic as the symptoms of acute inflammation. In chronic inflammation, there is less exudate or fluid and more fibrous tissue repair. Pain is more prominent than redness or heat. Arthritis is a good example of a disease with chronic inflammation as the body’s response to disease.
Subacute InflammationSubacute inflammation is a “flare-up” of a chronic inflammation. The pain, redness, heat and/or edema are suddenly more noticeable than in the chronic state.
Granulomatous InflammationGranulomatous inflammation forms tumors rather than heat, redness or pain. The tumor that is formed is more like a lump than swelling. The tumor is called a granuloma. In this type of inflammation, the cells that come to clear out the infection are called macrophages.
Granulomatous inflammation has special causes. It is seen with fungus infections, tuberculosis and foreign bodies, like popcorn in the trachea. Any disease that causes a granulomatous inflammatory response is called a granulomatous disease.
RepairThere are two ways tissues can repair damage: regeneration and repair.
RegenerationNormally, tissue replaces itself as old cells degenerate and die. For example, the lining of the stomach replaces itself every three days or so. Red blood cells are replaced every 120 days. When your skin flakes, you can see the dead cells that are removed. They are replaced by new young cells.
Regeneration is a normal process. However, in disease, this process is sped up to replace damaged cells. Your skin flakes much more after the trauma of sunburn, for example.

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-23
RepairRepair is the response to injury when regeneration won’t repair the damage that disease caused. Here the damaged tissues cannot regenerate, so they are replaced by fibrous connective tissue. This is called fibrous connective tissue repair. This also is called scarring or fibrosis.
Fibrous tissue doesn’t have the function of the tissue it replaced and usually is firmer. A wound will heal with fibrous tissue repair whether it is secondary to trauma or to surgery. The body doesn’t know the difference.
A wound that is sewn shut by surgery will heal with a smaller scar than one that is not sewn shut. When the wound is sewn shut, there is less damaged tissue to replace with fibrous tissue. That is why large cuts are closed with “stitches.” This is called healing by primary intention or primary union.
When a wound heals with the borders separated, there is more inflammatory response, and the tissue that forms during healing is called granulation tissue. The tissue is friable, meaning it breaks easily. It takes longer for the fibrous tissue to repair the wound. The scar is larger. This is called healing by secondary intention or secondary union.
Damage or DeathWhen cells, tissues or organs are injured, there is damage. When cells are damaged, there is degeneration, and the function decreases. The body can do one of the following: repair the damage, not repair the damage or allow the tissue to die. If there is no repair, the following things can happen.
MorbidityMorbidity means damage to a whole organism, like the human body. This damage usually is not a desired outcome of treatment. For example, after a stroke the human body doesn’t die, but it may not return to normal function. This loss of function is a morbid change.
Atrophy and HypertrophyRemember these terms from earlier in the lesson? You know that atrophy means cells slowly have decreased in size and/or number over a long time. Atrophic changes are caused by chronic injury.
Hypertrophy means that cells enlarge or swell but don’t increase in number. Chronic injury can do this. In hypertrophic change, the swelling is in the cells. In inflammation, the swelling is in the fluid surrounding the cells. Hypertrophy is one of two ways that tissues or organs become bigger. The other way tissues enlarge is hyperplasia, an increase in the number of cells, although the cells are not larger in size.
Accumulated CompoundsChronic injury usually leads to increased collections of abnormal, unwanted or waste materials in cells. This will increase the size of cells and organs and change their color and texture as well.
For example, when the liver is damaged, it can accumulate fat. This is called fatty metamorphosis. The liver is becoming larger and more yellow in color because it contains more fat than normal; it is changing from a morphologically normal liver to a morphologically abnormal liver.

0201604LB02A-10-14
Medical Coding Specialist
10-24
DeathNecrosis is death of cells, tissues or organs in a living body. The change is not reversible. That is, death cannot be reversed to life. Death occurs when cells are so damaged that they cannot repair or regenerate; the tissues are necrotic. Necrosis often results from an acute injury.
Mortality means death of an organism, like the human body. Anything that kills is called lethal. For example, if a gene causes a genetic or congenital abnormality that kills the body, the gene is called a lethal gene.
Different types of necrosis are seen microscopically. They include coagulation necrosis, liquefaction necrosis and caseous necrosis. The type of necrosis tells you its cause. Interruption of the blood supply causes coagulation necrosis. Liquefaction necrosis is the result of infection. The liquid pus you see is the debris left by the inflammatory response, including dead tissue cells and white blood cells. Caseous necrosis, which is seen in granulomatous inflammation, looks like cheese and contains dead tissue with tuberculosis bacteria in it.
Step 20: Pronounce New TermsFollow these steps:
a. Take your Quick-Learn Tutor and the flashcards labeled Set 13 out of your Quick-Learn Kit. Insert the first flashcard into Side A of the Tutor.
b. Access your pronunciation audio and play the files for Set 13.c. Listen to the term. Put the audio on pause.d. Practice pronouncing each term out loud. Take your time. Push the flashcard up and read
the meaning of the term. e. Do this for each term in this set. f. Put the flashcards in order and play the audio again, pronouncing each word part or term
after you hear it on the audio.g. Don’t forget to listen to your own pronunciation of each term. If you mispronounce one, put
a check mark next to that flashterm.h. Practice the terms you mispronounced by listening again. Be sure you can pronounce the
terms clearly and easily.
Step 21: Write New TermsFollow these steps:
a. Insert the first flashcard into Side A of your Quick-Learn Tutor.b. Look at each term as it appears in the window and say it out loud. Write the term on blank paper.c. Push the card up until the meaning appears in the right window and read the meaning out
loud. Write the meaning beside the term.d. Do this for each flashcard.

0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-25
Step 22: Meanings of New TermsFollow these steps:
a. Again insert the first flashcard into Side A of your Quick-Learn Tutor. Pronounce each term out loud and then say the meaning. Check yourself by pushing the flashcard up until you can see the meaning in the right window.
b. Now insert the flashcard into Side B of your Quick-Learn Tutor. Push the card up until you see the meaning of the first flashterm in the right window. Read each meaning out loud. Before you look, see if you can remember the term that goes with that meaning. Check yourself by pushing the flashcard up until you can see the term in the left window.
c. Practice with the flashcards several times until you are familiar with the terms and their meanings. You may use the flashcards for the Progress Checks and the Quizzes.
Step 23: Practice Exercise 10-4Select the best answer from the choices provided, and write your answers on scratch paper.
1. There are three ways tissues can respond to injury: damage or death, inflammation and _____.a. agingb. metaplasiac. rebelliond. repair
2. Rubor is a symptom of _____.a. inflammationb. repairc. regenerationd. death
3. ______ means heat.a. Ruborb. Tumorc. Dolord. Calor
4. The fluid of inflammation is called _____. a. an exudateb. acutec. a tumord. chronic

0201604LB02A-10-14
Medical Coding Specialist
10-26
5. _____ inflammation has special causes such as fungus infections and tuberculosis.a. Chronicb. Subacutec. Granulomatousd. Acute
6. Regeneration is how _____ replaces itself as old cells degenerate and die.a. an organb. tissuec. a celld. an body part
7. _____ is the response to injury when regeneration won’t repair the damage that disease caused.a. Deathb. Inflammationc. Repaird. Swelling
8. _____ is an example of morbidity.a. Diabetesb. A coldc. A stroked. Tay-Sachs disease
9. _____ is death of cells, tissues or organs in a living body.a. Morbidityb. Necrosisc. Atrophyd. Hypertrophy
10. Mortality means the _____.a. organism will survive the damageb. inflammation contains fluidc. regeneration of cellsd. death of an organism
Step 24: Review Practice Exercise 10-4Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
0201604LB02A-10-14
Cell and Tissue Anatomy and Pathology
10-27
Step 25: Lesson SummaryWow! We’ve covered a lot of information here! If you’re feeling a little overwhelmed, just relax. It’s not necessary that you memorize all the new terms you’ve just learned. In general, you won’t be asked to describe ribosomes or give an example of chronic inflammation. However, it’s important that you have an understanding of cells, how they work properly and what happens when they aren’t operating at their peak.
Let’s do a quick review before you move on to your Quiz. This lesson taught you the basic components of a cell and each component’s function. You learned about everything from cytoplasm to the nucleus. You studied etiologies, or the cause of abnormalities and injuries. You also looked at how cells adapt to injury and how the cell structure might change in the healing process. Lastly, you learned the body reacts to injury through inflammation, repair and damage or death.
Hopefully, you found parts of this lesson fascinating. Learning about how the human body responds to damage can be an interesting read. Perhaps you’ve experienced your own body healing in a way we’ve discussed here. If there were parts of this lesson that you found particularly confusing, go back and reread those sections before taking your Quiz. A little extra studying will pay off!
Step 26: Quiz 10Once you’ve mastered the course content, locate this Quiz in your Online Course or your Assignment Pack. Read and follow the Quiz instructions carefully.

0201604LB02A-10-14
Medical Coding Specialist
10-28

Lesson 11Diagnostic Coding 101
Step 1: Learning Objectives for Lesson 11When you complete the instruction in this lesson, you will be trained to:
● Describe the history and development of the diagnostic coding system.
● Explain the organization of the ICD-10-CM manual.
Step 2: Lesson PreviewBy now, you have a good understanding of anatomy, medical terminology and ethics. This lesson will provide you the background you need to understand the history and use of the ICD-10-CM coding manual. You will not need the manual to complete this lesson, as you’re just learning the basics of the book, including how the codes are using in the reimbursement process.
Whenever a patient sees a provider for a health-related problem, the patient is asking for a diagnosis. When a provider makes a diagnosis, the medical coding specialist codes it. The diagnosis codes assigned are then used to determine medical necessity. This helps payers, such as insurance companies, to determine reimbursement for the provider’s services.
Let’s begin by exploring the history of diagnostic coding.
Step 3: History of the International Classification of DiseasesThe history of the ICD system dates back to the 1600s in England! The ICD system came to the United States in the mid-1700s. This classification of diseases was originally used to track mortality statistics to determine how many people died of different diseases.
In the 17th century, the statistical study of diseases began with the work of John Graunt on the London Bills of Mortality. This study was initially a list of the number of burials. Graunt added to the Bills to include the cause of those deaths. He tabulated and studied data from the annual bills from 1629 through 1660, and published Natural and Political Observations Made upon the Bills of Mortality in 1662. This publication is considered one of the forerunners of today’s international mortality classifications.
0201604LB02A-11-14
Medical Coding Specialist
11-2
In 1837, the General Register Office of England and Wales found its first medical statistician, William Farr. Farr labored to secure an improved classification, as well as international uniformity. In 1853, the first International Statistical Congress (ISC) asked Farr to prepare an internationally applicable, uniform classification of causes of death.1 Although this classification was never universally accepted, the general arrangement survived as the basis for the International List of Causes of Death.
Later, the International Statistical Institute created a committee, chaired by Dr. Jacques Bertillon, to prepare a classification of causes of death. The report was presented in 1893, and the Bertillon Classification of Causes of Death, as it was first called, received general approval. Several countries adopted it at that point. Jesus E. Monjaras first used the classification in the Americas for the statistics of San Luis de Potosi, Mexico.2
In 1900, the first international conference for the revision of the Bertillon or International List of Causes of Death convened. Representatives from 26 countries attended, and adopted the first of the ICDs, or International Classification of Diseases. It was determined that the classifications should be revised every 10 years. Therefore, the succeeding conferences were held in 1909, 1920, 1929 and 1938, and a new version of the ICD was adopted at each.3
The WHOThe World Health Organization (WHO) is the directing and coordinating authority for health within the United Nations system. It is responsible for providing leadership on global health matters, shaping the health research agenda, setting norms and standards, articulating evidence-based policy options, providing technical support to countries and monitoring and assessing health trends.4 In 1946, the United Nations gave the responsibility of the ICD to the WHO, which issued the sixth and subsequent revisions in 1948, 1958 and 1967.
The ICD is the international standard diagnostic classification. It classifies diseases and other health problems recorded in many types of vital records, including death certificates and health records.5
The World Health Organization published the 9th Revision, International Classification of Diseases (ICD-9) in 1977. In 1979, the United States adopted the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) based on the ICD-9. The clinical modification expanded the number of diagnosis codes, and developed a procedural coding system, making the ICD-9-CM specific to the United States.
ICD-10After 30 years, the ICD-9 needed to be replaced. The terminology and classification of some conditions were outdated and/or obsolete. The outdated codes produced inaccurate and limited data. And, limits of the categories resulted in an increasing lack of specificity. Finally, the ICD-9-CM hindered comparisons with international data. It was clear that the next version needed to be flexible enough to adjust for emerging diagnoses and procedures, and exact enough to identify precise diagnoses and procedures.

0201604LB02A-11-14
Diagnostic Coding 101
11-3
In 1989, the WHO prepared the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), which was released in 1994. The United Kingdom adopted it in 1995, followed by the Nordic countries of Denmark, Finland, Iceland, Norway and Sweden from 1994 through 1997. Each year, another country adopted the ICD-10: France (1997), Australia (1998), Belgium (1999), Germany (2000) and Canada (2001). On January 15, 2009, the U.S. Department of Health and Human Services (HHS) released the final rule for implementation of the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) and the International Classification of Diseases, 10th Revision, Procedural Classification System (ICD-10-PCS). The final rule established the upcoming ICD-10 (both CM and PCS) transition.
To read about the ICD-10 Final Rule, visit: http:edocket.access.gpo.gov/2009/pdf/E9-743.pdf.
Step 4: Practice Exercise 11-1Determine the term(s) to complete each sentence, and write your answers on scratch paper.
1. The ICD was originally used to track _____.
2. The Bertillon Classification of Causes of Death was first used in _____.
3. In 1946, the United Nations gave the responsibility for the ICD to the _____.
4. The United States adopted the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), based on the ICD-9, in _____.
Step 5: Review Practice Exercise 11-1Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.
Step 6: Contents of the ICD-10-CMThe ICD-10-CM is a wealth of information. You know that diagnostic codes are alphanumeric characters that identify the physician’s opinion about what is wrong with the patient. These codes are not random alphanumeric characters, but are based on a system from the International Classification of Diseases 10th Edition Clinical Modification, or ICD-10-CM manual.
While this lesson will not provide in-depth knowledge of the ICD-10-CM, you will have a better understanding of the manual and how it’s used in the healthcare profession. Let’s look at each part of the manual now.

0201604LB02A-11-14
Medical Coding Specialist
11-4
Conventions for the ICD-10-CM According to the ICD-10-CM, “The ICD-10-CM conventions are general rules for use of the classification, independent of the guidelines. These conventions are incorporated within the Index or Tabular List as instructional notes.”6 The Conventions for the ICD-10-CM are at the front of the manual. The Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) provide these guidelines to accompany and complement the conventions and instructions you’ll find within the ICD-10-CM. Keep in mind that the Cooperating Parties for the ICD-10-CM—the American Hospital Association (AHA), the American Health Information Management Association (AHIMA), CMS and NCHS—have approved these guidelines. And, Health Insurance Portability and Accountability Act (HIPAA) adopted these diagnosis codes for all healthcare settings and require you to adhere to the guidelines.
These general rules define the format and structure of codes; provide definitions of acceptable abbreviations and punctuations; and explains notes and terms used throughout the manual.
General Coding Guidelines The General Coding Guidelines are used when selecting the correct ICD-10-CM code. Here, you will find some of the key guidelines, such as the steps to ICD-10-CM codes and coding rules. The coding rules include when to code a sign and symptom and how to code acute and chronic conditions. These rules will be referenced when determining the accurate diagnostic code to assign to the medical record.
Chapter-Specific GuidelinesThe ICD-10-CM provides guidelines for specific diagnoses and/or conditions. These chapter-specific guidelines are used in conjunction with the general coding guidelines when selecting a diagnostic code. The key to accurate coding is to be familiar with these guidelines.
Alphabetic Index to Diseases The Alphabetic Index to Diseases is divided into four parts: the Index to Diseases and Injuries, the Neoplasm Table, the Table of Drugs and Chemicals and the Index to External Causes. Now, let’s briefly look at the content of each so that you’ll understand how to use it correctly.
Index to Diseases and Injuries The first section of the Alphabetic Index to Diseases is the Index to Diseases and Injuries, also called simply the Index. This is an alphabetical list of terms and their corresponding codes. The terms are arranged by specific illness, injury, eponym, abbreviation or other descriptive diagnostic terms. Using the Index is a straightforward process when you have a good base knowledge of medical terminology and anatomy.

0201604LB02A-11-14
Diagnostic Coding 101
11-5
Here is an example of what you’d see in the Index, if you were looking up abdominal pain:Pain(s) (see also Painful) R52
abdominal R10.9 colic R10.83 generalized R10.84 with acute abdomen R10.0 lower R10.30 left quadrant R10.32 pelvic or perineal R10.2 periumbilical R10.33 right quadrant R10.31
Neoplasm TableThe ICD-10-CM manual places the Neoplasm Table in the Alphabetical Index at the end of the Index to Diseases and Injuries. The term neoplasm refers to any new and abnormal growth. You locate codes based on the type and location of the neoplasm. Let’s briefly look at the types of neoplasms:
Malignant Primary refers to the site at which a neoplasm originated.
Malignant Secondary refers to the site or sites to which the neoplasm has spread from the primary site.
Ca in situ, which is short for Carcinoma in situ, describes the situation in which tumor cells are undergoing malignant changes but are still confined to the point of origin without invasion of the surrounding normal tissue.
Benign refers to noncancerous growth that does not invade adjacent structures or spread to distant sites, but might displace or exert pressure on adjacent structures.
Uncertain refers to tumors that the pathologist cannot classify as benign or malignant because some features of each type are present.
Unspecified Behavior refers to tumors in which neither the behavior nor the histological type is specified in the diagnosis.
To locate the code for a neoplasm of the middle lob of the bronchus, the table looks like this:
Mal
igna
nt
Prim
ary
Mal
igna
ntSe
cond
ary
Ca
in s
itu
Beni
gn
Unce
rtain
Be
havi
or
Unsp
ecifi
ed
Beha
vior
Neoplasm, neoplastic—bronchus
middle lobe of lungC34.2 C78.0- D02.21 D14.31 D38.1 D49.1
Starting at the Neoplasm Table, you locate the location of the neoplasm. Then you move across the columns until you found the specific behavior. The code listed in the column is the tentative ICD-10-CM code.

0201604LB02A-11-14
Medical Coding Specialist
11-6
Table of Drugs and Chemicals The ICD-10-CM Table of Drugs and Chemicals appears just after the Neoplasm Table. You’ll see reference to this as Table of Drugs for short. This table is used to code a poisoning by adverse effect of or underdosing. Here is an example for Ibuprofen in the Table of Drugs:
Poiso
ning
, A
ccid
enta
l (u
nint
entio
nal)
Poiso
ning
, In
tent
iona
l Se
lf-ha
rm
Poiso
ning
, A
ssau
lt
Poiso
ning
, Un
det
erm
ined
Ad
vers
e Ef
fect
Und
erd
osin
g
T39.311 T39.312 T39.313 T39.314 T39.315 T39.316
The first column contains the substance; then, there are several columns to identify the intent. Poisoning is classified as accidental or unintentional; intentional with self-harm in mind; an assault; or undetermined. After the poisoning columns, there are columns for adverse effect and underdosing. So, after locating the drug, move to the accurate intent column and note the tentative code
Index to External CausesExternal causes of morbidity, often known just as external causes, is used to completely describe the cause, the intent, the place of occurrence and, if applicable, the activity of the patient at the time of the event, and the patient’s status for all injuries and other health conditions due to an external cause. These codes are supplemental to the diagnostic code. The external cause codes are intended to provide data for research and analysis for injury prevention.
The Index of External Causes appears right after the Table of Drugs and Chemicals and before the Tabular List.
Tabular List of Diseases and InjuriesThis section of the ICD-10-CM is arranged numerically within 21 separate chapters according to body system or nature of injury and disease. The ICD-10-CM is an alphanumeric classification system divided into “blocks.” A valid code may have from three to seven characters, with a decimal between the third and fourth character. If there is not a fourth character, you will not apply the decimal.
X X X
Subcategory
X
Extension
X X X
Category
CategoryThe first three characters of the ICD-10-CM code are considered the category. The first character of the three-digit category is a letter. The second and third character of the three-digit category may be numbers or alphabetic characters. The three-digit category is considered the “block” of the code. According to the ICD-10-CM Conventions, a three-digit category without further subclassification is equivalent to a valid three-digit code.

0201604LB02A-11-14
Diagnostic Coding 101
11-7
SubcategoryThe subcategories are characters four, five and/or six, all of which may be either letters or numbers. The fourth, fifth and sixth characters of the ICD-10-CM code represent the etiology, anatomical site or severity of the condition.
Extension Certain categories of the ICD-10-CM manual have a seventh-character extension, which is required as an addition to codes from these categories. The extension is the 7th character in the code. According to the ICD-10-CM, the seventh-character extension must always be the last character in the data field.
Step 7: Practice Exercise 11-2Select the best answer from the choices provided, and write your answers on scratch paper.
1. The first _____ characters of the ICD-10-CM code are considered the category.a. twob. threec. fourd. five
2. The _____ is not found within the Alphabetic Index.a. Neoplasm Tableb. Table of Drugs and Chemicalsc. Index to External Causesd. Tabular List
3. The _____ is found within the Alphabetic Index at the end of the Index to Diseases and Injuries.a. Neoplasm Tableb. Table of Drugs and Chemicalsc. Index to External Causesd. Tabular List
Answer the following as directed and write your answers on scratch paper.
4. List the Cooperating Parties for the ICD-10-CM that have approved the Conventions for the ICD-10-CM.
Step 8: Review Practice Exercise 11-2Check your answers with the Answer Key at the back of this book. Correct any mistakes you may have made.

0201604LB02A-11-14
Medical Coding Specialist
11-8
Step 9: Lesson SummaryA basic knowledge of the manual used for diagnostic coding is essential to the healthcare professional. You understand the history and use of the ICD-10-CM coding manual, as well as the organization of the manual.
Now, complete the Quiz to reinforce what you’ve learned about the ICD-10-CM.
Step 10: Quiz 11Once you’ve mastered the course content, locate this Quiz in your Online Course or your Assignment Pack. Read and follow the Quiz instructions carefully.
Endnotes1 The WHO Family of International Classifications. World Health Organization, 2010. Web. 4 October 2013. 2 Bertillon J. Classification of the causes of death (abstract). In: Transactions of the 15th International Congress on Hygiene Demography. Washington, 1912. Print.3 The WHO Family of International Classifications. World Health Organization, 2010. Web. 4 October 2013. 4 About WHO. World Health Organization, 2010. Web. 4 October 2013. 5 International Classification of Diseases. World Health Organization, 2010. Web. 4 October 2013. 6 ICD-10-CM The Complete Official Draft Code Set. Salt Lake City, Ingenix: 2013. Print.
Answer KeyMedical Coding Specialist
Lesson 7
Practice Exercise 7-11. Th e two main objectives of HIPAA are portability and accountability.
2. Covered entities are healthcare professionals who transmit any health information in electronic form.
3. Th e Privacy Rule addresses the use and disclosure of patients’ health information.
4. TPO stands for treatment, payment and healthcare operations.
5. Th e Security Rule does not apply to PHI transmitted orally or in writing.
6. Employer Identifi cation Number (EIN), is issued by the Internal Revenue Service (IRS) to identify employers on standard transactions.
7. Th e NPI is a 10-position, numeric identifi er that does not carry other information about healthcare providers.
8. Th e term breached refers to a violation or infraction of a standard.
9. When protected health information is unsecured it means the information hasn’t been encrypted.
10. A conscious, intentional failure or reckless indiff erence to the obligation to comply with the administrative simplifi cation provision is willful neglect.

0201604LB02A-AK-14
Medical Coding Specialist
AK-2
Practice Exercise 7-21. As a healthcare professional, you cannot release any medical information unless it is to an
authorized person because the information is confi dential.
2. Ethical guidelines are oft en spelled out in a document called a code of ethics.
3. You should never fax sensitive test information.
4. Damages directly related to fraud are termed compensatory damages.
5. Th e Federal False Claims Act or FCA prohibits anyone from presenting a false or fraudulent claim to be paid by the government.
6. Fraud includes inaccurate information that is used to wrongfully gain compensation.
7. Fraud and abuse can be reported to the Offi ce of Inspector General.
8. A(n) insurance audit is a thorough review by the insurance company of a claim and all related documentation.
9. RACs are paid on a contingency fee basis, receiving a percentage of the improper payments they collect from providers.
10. A(n) subpoena can authorize the legal release of confi dential medical records.
11. A(n) arbitrator is a person chosen to decide a dispute or settle diff erences.
12. When a person lies during testimony, he can be charged with perjury.

0201604LB02A-AK-14
Answer Key
AK-3
Lesson 8
Practice Exercise 8-11. Anatomy, physiology and pathology are included in the study of life called human biology.
2. Th e study of the form of an organ, such as size, shape or color, is called morphology.
3. Th e science of the appearance and relationships of body parts is called anatomy.
4. Th e study of the function of body parts is called physiology.
5. Th e study of disease is called pathology.
6. Th e study of tissues is called histology.
7. Th e science of the appearance of cells and tissues is called microscopic anatomy.
8. To see a cell, you would use an instrument called a(n) microscope.
9. Changes in the function of an organ are called physiologic changes.
10. Th e disease changes you see in an organ are called pathologic changes.

0201604LB02A-AK-14
Medical Coding Specialist
AK-4
Practice Exercise 8-21. When the arms are at the side, the palms of the hands face forward and the thumbs point
outward, the body is in the anatomic position.
2. A(n) transverse plane also is called a horizontal plane.
3. A(n) parasagittal plane divides the body into unequal left and right sections.
4. A frontal plane also is called a(n) coronal plane.
5. A(n) transverse or horizontal plane divides the body into superior and inferior sections.
6. A longitudinal plane also is called a(n) sagittal plane.
7. A(n) coronal or frontal plane divides the body into anterior and posterior sections.
8. A(n) midsagittal or median plane divides the body into equal left and right sections.
9. A midsagittal plane also is called a(n) median plane.
10. A plane divides the body or organ into sections.
Practice Exercise 8-31. Th e hand is caudad to the elbow.
2. Separating the body into right and left halves is called a sagittal plane.
3. Th e knee is inferior or caudad to the chest.
4. Th e belly button is anterior to the spine.
5. A blood vessel that carries blood away from the heart is called an eff erent vessel.
6. In the anatomic position, the palms of the hands are anterior to the backs of the hands.
7. Th e nose is medial to the eyes.
8. Th e buttocks are dorsal and caudad to the breastbone.

0201604LB02A-AK-14
Answer Key
AK-5
Lesson 9
Practice Exercise 9-1
1.
2.
3.
4.
5.
6.
7.
8.
9.10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.

0201604LB02A-AK-14
Medical Coding Specialist
AK-6
25. cubitus
26. occiput
27. cervix
28. scapula
29. dorsum
30. lumbus
31. sacrum
32. gluteus
33. popliteal fossa
34. sura
35. calcaneus
36. plantar surface
Practice Exercise 9-21. Th e abdomen may be divided more simply into four quadrants.
2. Th e carpal bones are in the wrist.
3. A fi nger is also called a(n) digit.
4. A break in the kneecap is called a(n) patellar fracture.
5. A buccal smear is a tissue sample taken from the inside of the cheek.

0201604LB02A-AK-14
Answer Key
AK-7
6. A person who does not have a collarbone does not have a(n) clavicle.
7. Lymphadenopathy in the armpit is called axillary lymphadenopathy.
8 Lymphadenopathy in the groin is called inguinal lymphadenopathy.
9. You can feel a pulse in the fossa anterior to the elbow, called the antecubital fossa.
10. Th e quadrant where the appendix can cause pain is on the right below the umbilicus and is called the right lower quadrant.
11. Pain in the lower back is called lumbar pain.
12. When you put your hands on your hips, the bone you feel is the iliac crest.
Practice Exercise 9-31. e. Subdivided into the cranial cavity and the spinal canal Dorsal body cavity
2. a. Th e smallest unit in your body Cell
3. h. Contains the gallbladder, liver, spleen, stomach, small intestine, most of the large intestine, kidneys, pancreas and the ureters Abdominal cavity
4. b. Th e largest serous membrane of the body Peritoneum
5. i. Subdivided into the thoracic cavity and the abdominopelvic cavity Ventral body cavity
6. d. Layers of tissue that cover organ surfaces, line body cavities and form tubes Membranes
7. f. Th e outer layer of the skin Cutaneous membrane
8. c. Protect the brain and spinal cord Meninges
9. g. Line the joints of the shoulders, knees, hips, fi ngers and toes Synovial membranes
0201604LB02A-AK-14
Medical Coding Specialist
AK-8
Lesson 10
Practice Exercise 10-11. Every structure in the body is made of c. cells.
2. b. Cilia are like hairs that wave in the fl uid around a cell.
3. b. Microvilli act like the webbing of a sponge to absorb materials transported across the cell membrane.
4. Th e ribosomes make d. protein.
5. a. Agranular ER, also called smooth ER, does not have ribosomes on its surface.
6. Mitochondria are regarded as the a. power plants of the cell because they exist in large numbers in those human cells that require an enormous amount of energy to do their work.
7. c. Centrioles are only active during reproduction.
8. A vacuole is any small cavity in the d. cytoplasm of a cell.
9. DNA stands for b. deoxyribonucleic acid.
10. RNA is a. a messenger for the DNA.
Practice Exercise 10-21. Th e type of abnormality seen in tissues and organs is determined by b. two factors.
2. b. Etiologies are the causes of pathology.
3. c. Infection is caused by the action of bacteria, viruses and parasites.
4. Hyperplasia means a. an increase in the number of normal cells, usually due to a reaction from an outside irritation.
5. Atherosclerosis, or hardening of the arteries, is a good example of a. vascular disease.

0201604LB02A-AK-14
Answer Key
AK-9
6. d. Nosocomial diseases are diseases acquired in a hospital environment.
7. Anoxia is the complete lack of c. oxygen.
8. d. Poisons are examples of toxic agents.
9. People who become allergic to themselves have a condition called c. immunopathy.
10. a. Tay-Sachs disease, a genetic defi ciency of a certain hormone, causes destruction of the lysosomes of nerve and eye cells.
Practice Exercise 10-31. Th e term for when the body is not injured and cells are balanced with their environment
is b. homeostasis.
2. Minor injuries from which the cell recovers and returns to its original state are referred to as c. reversible.
3. Cell atrophy that is directly related to age and involves change in the entire body is called a. physiologic atrophy.
4. Cellular adaptation that occurs when a cell changes from one type of cell to another is called c. metaplasia.
5. An increase in the size of tissues or organs caused by an increased number of cells is called a. hyperplasia.
6. An increase in the size of tissues or organs due to an enlargement of individual cells is called d. hypertrophy.
7. Th e main products of intracellular accumulations are collagen and complex d. sugars.
8. b. Aging cannot be avoided or prevented, and the best one can do is try to lessen its adverse eff ects on the body.

0201604LB02A-AK-14
Medical Coding Specialist
AK-10
Practice Exercise 10-41. Th ere are three ways tissues can respond to injury: damage or death, infl ammation and
d. repair.
2. Rubor is a symptom of a. infl ammation.
3. d. Calor means heat.
4. Th e fl uid of infl ammation is called a. an exudate.
5. c. Granulomatous infl ammation has special causes such as fungus infections and tuberculosis.
6. Regeneration is how b. tissue replaces itself as old cells degenerate and die.
7. c. Repair is the response to injury when regeneration won’t repair the damage that disease caused.
8. c. A stroke is an example of morbidity.
9. b. Necrosis is death of cells, tissues or organs in a living body.
10. Mortality means the d. death of an organism.

0201604LB02A-AK-14
Answer Key
AK-11
Lesson 11
Practice Exercise 11-11. Th e ICD was originally used to track mortality statistics.
2. Th e Bertillon Classifi cation of Causes of Death was fi rst used in Mexico.
3. In 1946, the United Nations gave the responsibility for the ICD to the World Health Organization (WHO).
4. Th e United States adopted the International Classifi cation of Diseases, 9th Revision, Clinical Modifi cation (ICD-9-CM), based on the ICD-9, in 1979.
Practice Exercise 11-21. Th e fi rst b. three characters of the ICD-10-CM code are considered the category.
2. Th e d. Tabular List is not found within the Alphabetic Index.
3. Th e a. Neoplasm Table is found within the Alphabetic Index at the end of the Index to Diseases and Injuries.
4. List the Cooperating Parties for the ICD-10-CM that have approved the Conventions for the ICD-10-CM. Th e American Hospital Association (AHA), the American Health Information Management Association (AHIMA), Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS)

0201604LB02A-AK-14
Medical Coding Specialist
AK-12