matthew schumaecker, md, facc ash designated specialist in clinical hypertension carilion clinic...
TRANSCRIPT
Hypertension:Pathophysiology, Epidemiology, and
Treatment
Matthew Schumaecker, MD, FACCASH Designated Specialist in Clinical HypertensionCarilion ClinicAssistant Professor of MedicineVTC School of Medicine

http://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm

NHANES Hypertension Prevalence US Adults; 2003-2010
Hypertension30.4%
Controlled46.5%
Uncontrolled53.5%
Aware and treated44.8%
Aware and untreated
15.8%
Unaware39.4%
CDC MMWR 2012; 61(35);703-709

Hypertension Causes CHF
Circulation 2002;106:3068-3072
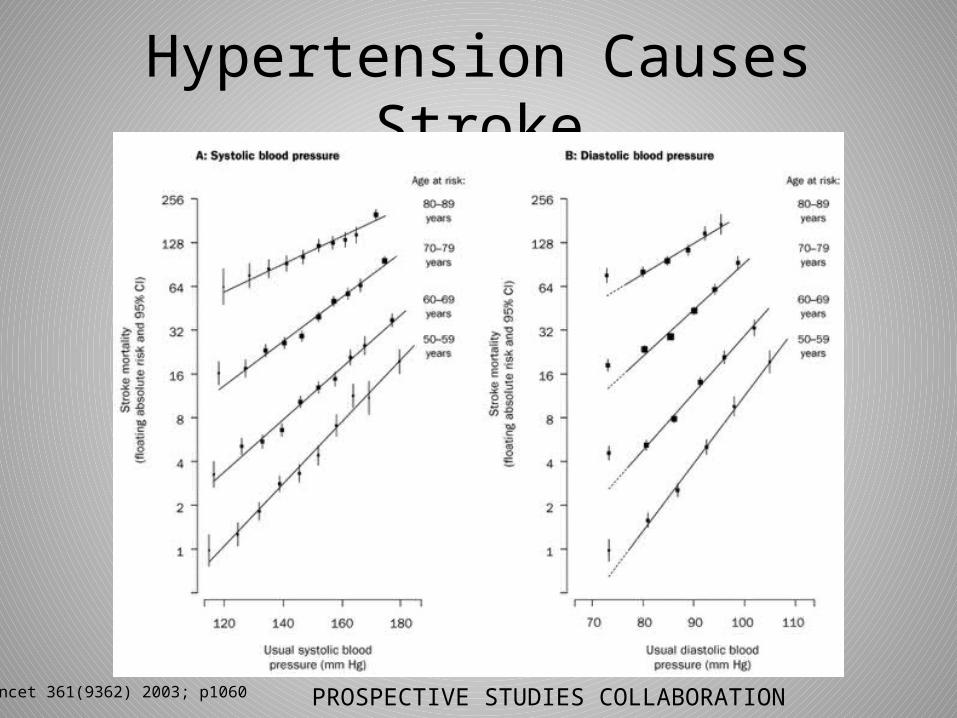
Hypertension Causes Stroke
Lancet 361(9362) 2003; p1060 PROSPECTIVE STUDIES COLLABORATION

Hypertension Causes CAD
Lancet 361(9362) 2003; p1060 PROSPECTIVE STUDIES COLLABORATION

Hypertension Causes CAD
MRFIT Arch Intern Med 1993;153:186-208 via KCH

Hypertension Causes Kidney DiseaseIncidence of ESRD by SBP in x/100,000 person-years
Klag MJ et al JAMA 1997;277:1293

Defining Hypertension
“There is no dividing line. The relationship between arterial pressure and mortality is quantitative – the higher the pressure, the worse the prognosis”
Sir George Pickering
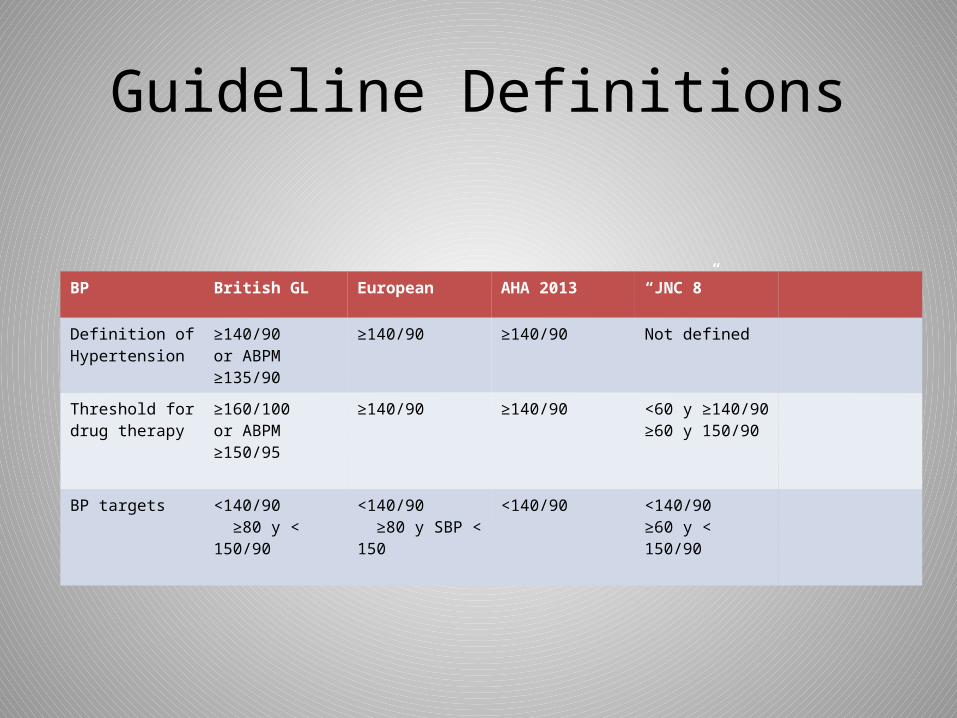
Guideline Definitions
BP British GL European AHA 2013 “JNC 8”
Definition of Hypertension
≥140/90or ABPM ≥135/90
≥140/90 ≥140/90 Not defined
Threshold for drug therapy
≥160/100or ABPM ≥150/95
≥140/90 ≥140/90 <60 y ≥140/90≥60 y 150/90
BP targets <140/90 ≥80 y < 150/90
<140/90 ≥80 y SBP < 150
<140/90
<140/90≥60 y < 150/90

Pathophysiology of Hypertension
• Four major systems– Renal– Vascular– Autonomic Nervous– Endocrine
(heart plays very little role in etiology of HTN)

Problems in Understanding Pathogenesis
• Much of our data is from rodent models• Hypertension is not considered to be one
disease entity– Systolic hypertension in young adults– Diastolic hypertension in middle age– Isolated systolic hypertension in advanced age
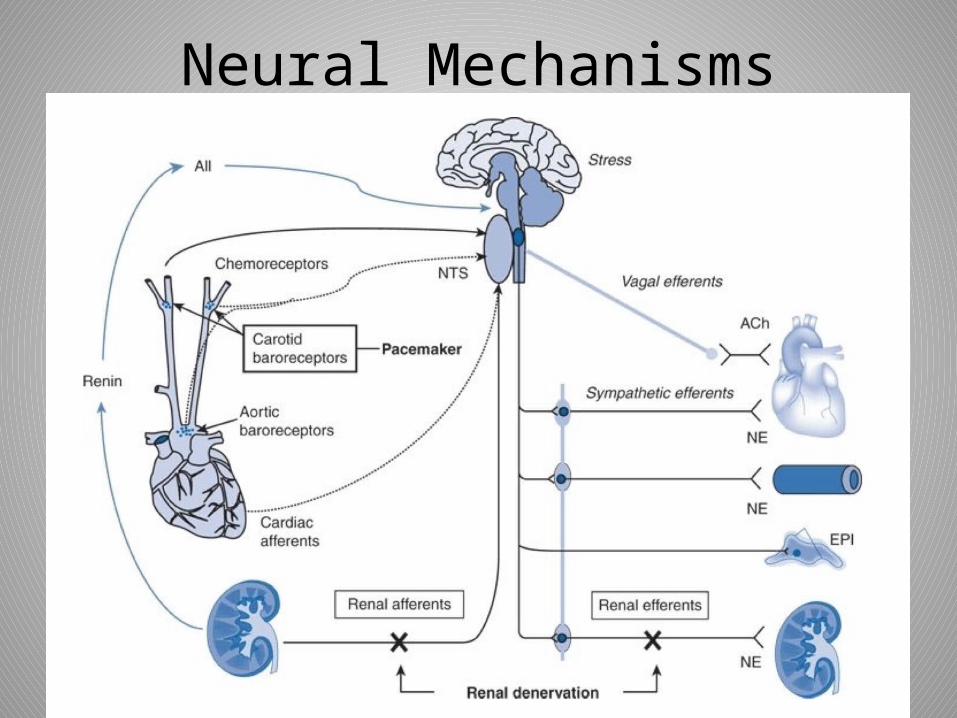
Neural Mechanisms

Baroreceptors
• Receptors that mediate increase in CO and SVR in response to a fall in BP via the NTS
• Play a role in carotid hypersensitivity• Pacing the carotid baroreceptors has been
shown to reduce BP

Neuro-Renal Mechanisms
• Renal sympathetic nerve activity – Causes renin release – Causes renal vasoconstriction– Enhances renal sodium and water reaborption

Peripheral Sympathetic Overactivity• Usually the culprit in young
patients with systolic hypertension
• Thought to be behind the white coat hypertension phenomenon
• Should (but frequently doesn’t) respond to beta blockers

Renal Mechanisms
• Salt Hypothesis• Intra-renal RAAS• Renal medullary endothelin

Pressure-Diuresis Relationship

Resetting of Pressure-Diuresis

Vascular Mechanisms
• Endothelial dysfunction • Chronic vascular inflammation• Large vessel stiffness

Hormonal Mechanisms
• Renin-Angiotensin-Aldosterone• Inherited and acquired endocrinopathies– Cushing’s Disease– Hyperaldosteronism– 11βHSD deficiency – AME
– Many others

We All Measure BP Wrong
Kaplan’s Clinical Hypertension 14th Ed

Home BP Monitoring is (Usually) Better
– Multiple studies show that HBPM is a better prognostic indicator than OBPM
– Should minimize the “white-coat” and “masked” BP effect– Best device is upper arm oscillometric device– Patients have to be instructed:
• No caffeine < 30 min• No smoking < 30 min• Rest 5 min first• No talking• Relax• Use same arm rest on firm surface
Source: escardio.org

Essential Hypertension
• Elevated BP in which secondary causes are not present.
• 95% of all cases of HTN are essential• Etiologic causes include:
1. Obesity2. Insulin resistance3. Aging4. Stress5. High sodium intake6. Low potassium and calcium intakeCarretero and Oparil Circulation. 2000; 101: 329-335
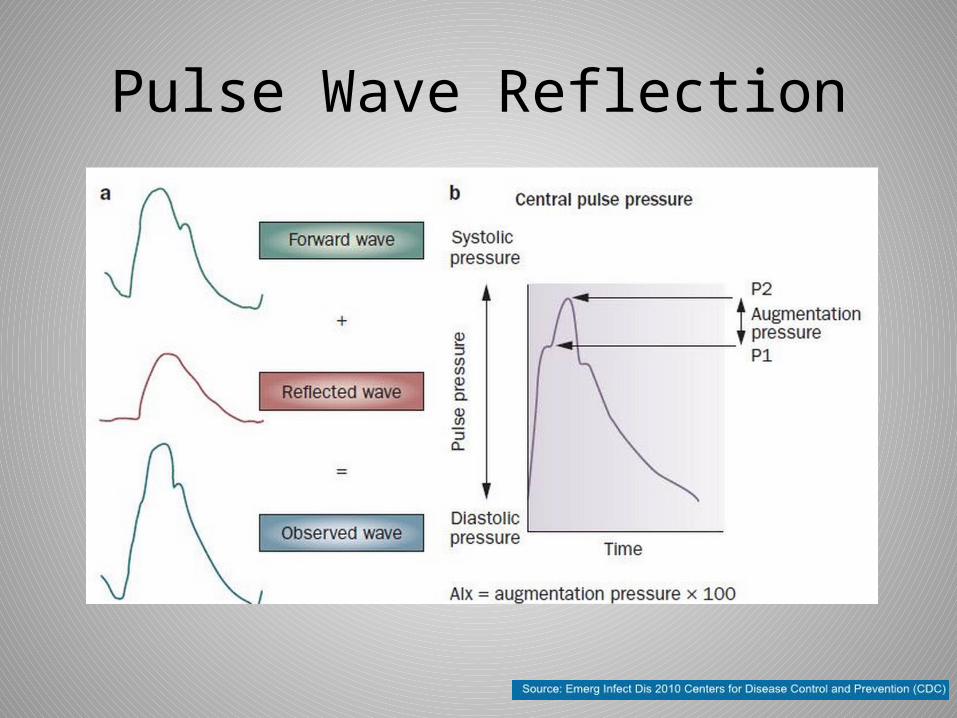
Pulse Wave Reflection

Effect of Age on Reflected Pulse Wave

Pulse Pressure Increases > 55 years
Hypertension 1995;25:305 -> Kaplan Clinical HTN

Common Causes of Secondary Hypertension
Endogenous (common)
• OSA• Primary aldosteronism• Renovascular hypertension• Pre-eclampsia• Hyperparathyroidism• Vitamin D deficiency
Exogenous• Obesity • NSAIDS• SSRI/SNRI• Heavy EtOH use• Epo use in ESRD• Caffeine(???)• Nicotine(???)

Less Common Causes of Secondary Hypertension
• Pheochromocytoma• Acromegaly• Cushing’s Disease• 11β-hydroxysteroid2 inhibition• Calcineurin inhibitors• Intracranial pressure• Thyrotoxicosis• Liddle’s Syndrome• Gordon’s Syndrome• Acute porphyria• Familial dysautonomia• Beriberi• Paget’s disease of bone• Burns• Polycystic kidney disease
• Congenital adrenal hyperplasia• Sickle cell crisis• Perioperative• Nicotine(?)• AV fistula• Patent ductus arteriosus• Carcinoid syndrome• Spinal cord injury• Lead poisoning• Guillian-Barré

Preliminary Secondary HTN workup
• Aldo/Renin Ratio (> 30 abnormal)• Plasma renin activity• Calcium levels -> PTH if elevated• Renal duplex• Sleep study• Metanephrines (commonly ordered, rarely
positive)• Echo in patients with unequal UE/LE BP

Unlike Lipids, There is Abundant Primary CV Prevention Data
• VA Cooperative Study 1&2• ALLHAT• NHANES III• SHEP• HYVET• HOT

VA Cooperative Trial
• Began in 1964• Reserpine/chlorthalidone/hydralazine• Mean age 49 years• 523 men• Stopped after 18 months because of ~ 50% CV
death reduction in treatment arm

SHEP
• 4736 patents > 60 years of age with isolated systolic hypertension
• (Stepped therapy with chlorthalidone +/- atenolol ) vs. (placebo)
• CVA reduction in treatment arm 36%
Syst-Eur
• European version of SHEP done with staged therapy
• Placebo -> nitrendipine +/ lisinopril +/- HCTZ vs placebo
• Treatement of 1000 patients for 5 years will prevent 29 strokes and 53 CV endpoints


• 33,357 patients > 55 years• Sponsored by NHLBI • Randomly assigned to – Chlorthalidone– Amlodipine– Lisinopril– Doxazosin

Doxazosin arm was discontinued because of doubling of CHF incidence

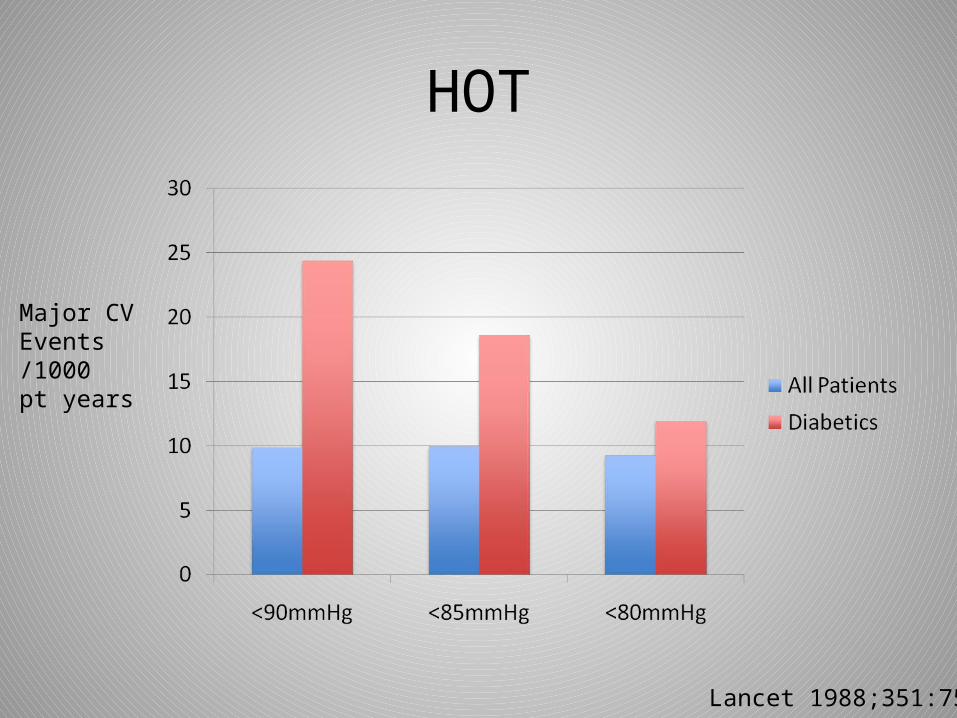
HOT
Major CVEvents/1000 pt years
Lancet 1988;351:755

Renal Denervation
http://www.terumo.com/
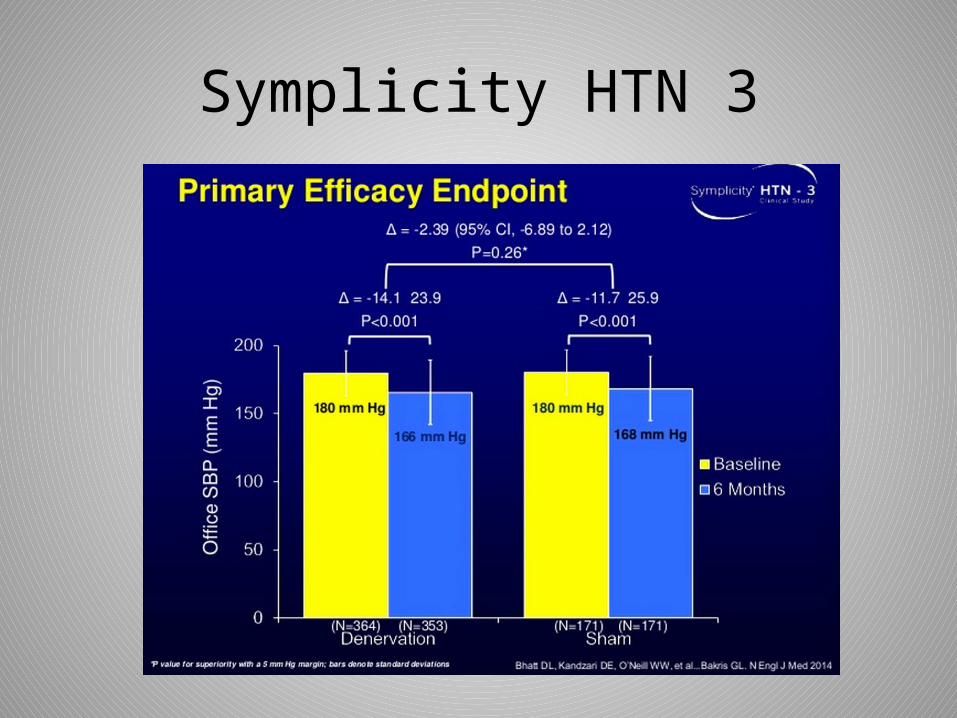
Symplicity HTN 3
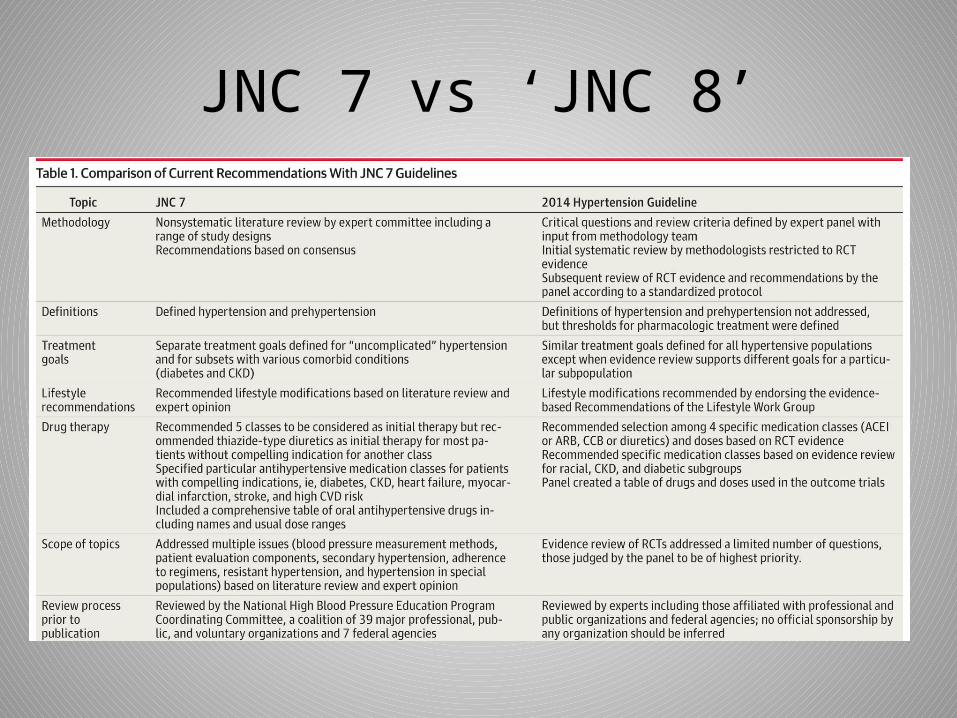
JNC 7 vs ‘JNC 8’

CLONIDINEHYDRALAZINE
Medical Treatment of HTN


NICE Guidelines
• Similar to JNC Guidelines• Recommends ACE-ARB for whites
and CCB for blacks prior to diuretic• Specifically recommends
chlorthalidone or indapamide over HCTZ

CONCLUSIONS
• We can save more lives by treating hypertension before it causes target organ damage
• Lowering BP is proven to be good but in the elderly there may be too much of a ‘good’ thing
• Use diuretics, ACE/ARB and CCB at reasonable doses before trying anything else
• Spironolactone should likely be fourth line• Most people do not have secondary
hypertension
