insights from carilion clinic: transformation and the accountable physician group mark werner, md...
Post on 22-Dec-2015
219 views
TRANSCRIPT

Insights from Carilion Clinic: Transformation and the
Accountable Physician Group
Mark Werner, MDPresident, Carilion Clinic Physicians


Carilion• Headquarters: Roanoke, VA
• 8 Hospitals
• Significant teaching programs- 170 residents, 60 medical students
• Large multi-specialty physician group
• $ 1.3 B net revenue
• Historic 4% operating margin; 12% EBIDA
• AA(-) credit rating
• Strong balance sheet

Key FY ‘09 Carilion Clinic Stats
• Employees 12,305
• Licensed beds 1,215
• Admissions 49,642
• Avg. daily census 624
• Avg. daily ED visits 508.4
• Total ED visits 185,595

Costs vs. Revenue
CostRevenue
Payment/Cost
Time

Prior Cost Containments • Large One Time Cost Reductions
− Staffing
− Revenue cycle
− Eliminate financially non-performing, non-mission critical services
− Consolidate services

• Access & market share– Aging medical staff– Inability of private groups to recruit and
regenerate– Reluctance of private groups to accept
referrals from outside the immediate area– Issues with call coverage– Service offerings exceeding needs of
population base
ISSUES

ISSUES• Financial
– Very slow market growth, little potential to take share from others with current operations
– Harder to find new cost & revenue opportunities• Exited non-core businesses (DME, Health Plan, LTC)• Sought cost savings & revenue cycle opportunities –
E&Y, Hunter Group• Aggressive payer contracting
– Private physicians attempting to capture profitable outpatient services

Past Success Not Sustainable
• Two Converging Factors
1. Physician Issues Supply
Alignment
Fragmentation and variation in care
2.2. Inflation vs. Payment Rate Inflation vs. Payment Rate IncreasesIncreases

Options for Change
• Acquire smaller hospitals– Contiguous– Non-contiguous
• Merge in smaller/weaker system• Merge with larger/better positioned
system• Sell• None acceptable to Board
Healthcare Spending Problematic Dollars are skewed toward separate payments to separate providers for discrete services, particularly specialty and technology intensive services
Volume is rewarded
No incentives for coordination, efficiency
Disincentive for improving quality (in the hospital)
Contributors to Cost Growth• Aging population- 2%
• Price growth- 22%
• New technologies- over 50%
• Defensive medicine- real, complex, lessor contributor
• Overuse and inappropriate care– 1/3 of surgeries of limited value– Up to 2/3 of carotid endarterectomies

Our Responsibility Reclaim 30%,
if not,
- Deterioration
- Continued rationing Produce consistently good, transparent results

Only Physician-Led Health Care Systems Can Do This
Physician orders spend the money and drive care
Clinical teams have the knowledge/experience to ferret out value

Our View of a Clinic
• Large interdisciplinary group practice dedicated to integrated and coordinated care producing excellent efficient patient care supported by education and informed by research
• Physicians are key leaders
• Organized around the physician group
• Hospitals work together with physicians in support of patients’ needs

Key Aspects of Our Culture
• Honest, Forthright, Transparent• Teamwork – about group not individuals• Shared Success – accountable to each other• Through focus on patients we meet the needs
of physicians• Physician Leadership – Must be real and
committed • Change, uncertainty, vagueness, learning

“Hospitals Are Ancillary”
• Humbling
• Loss of Control
• Paired leadership
• Ambiguous
• High degree of trust
• Outcomes superior
• Hard to convey to community and stakeholders

Investments
• Recruit additional physicians
• Build consolidated practice site
• Implement longitudinal electronic medical record
• Bolster nursing staff size & skills
• Cost of medical staff disruption
• VTC Medical School and Research Institute
Investment/Finances
FY06 FY09 VarianceOperating Income 34,414 (56,840) (91,254)
Related to Clinic (29,778)Not Related to Clinic (60,255)

Investments Related to Clinic Decision
Clinical Programs/Recruitment (24,939)
EPIC ENR – Additional (5,114)
New Clinic MOB (3,095)
Medicare Advantage Plan (4,458)
New Nursing Ratios (50%) (3,786)
Bad Debt, Charity (50%) (8,037)
Commercial Payor Contracts 15,000
Increased Hospital Admissions 4,65229,778

Decision Criteria with Private Groups
• Focused on the right thing- not everything is financial, it had to be the right cultural fit, consistent mission, values
• Group agrees on an integrated vision that emphasizes quality and service
• Good strategic long term plan• Sustainable growth potential

Compensation Plan
• Lots of early focus!• Use to promote alignment and accountability• Working toward consistency in
goals/objectives• Is adaptable to a range of needs and
circumstances• Constant pressures on productivity – but
needs to be broadly focused
Evidence it is Working• Reduced costs/in-patient over $200• Reductions in mortality rate• Reductions in hospital-acquired infections• Access and service standards• Navigated or Coordinated scheduling• Team focused care• New programs- neurointerventional,
electrophysiology, interventional pulmonary, adolescent gynecology
• A 26 year old wife and mother
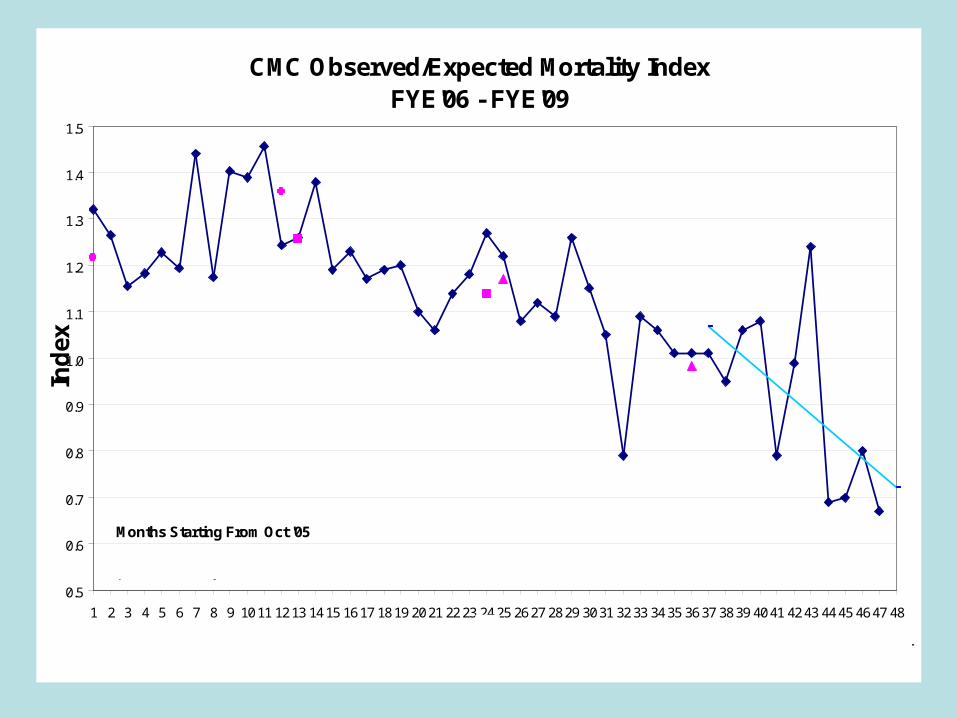
CMC Observed/Expected Mortality IndexFYE'06 - FYE'09
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
1.3
1.4
1.5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 2021 2223 2425 2627 2829 3031 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48
Months Starting From Oct '05
Ind
ex
Oct
'05
Sep
'09
Oct
'06
Oct
'08
Oct
'07
Expected Rates all years based on 2007 Premier benchmarks

$8,000.00
$9,000.00
$10,000.00
$11,000.00
$12,000.00
$13,000.00
$14,000.00
$15,000.00
$16,000.00
$17,000.00
Q1-FY06
Q2 Q3 Q4 Q1-FY07
Q2 Q3 Q4 Q1-FY08
Q2 Q3 Q4 Q1-FY09
Q2 Q3 Q4
Quarter-Fiscal Year
Do
llar
s
400.00
500.00
600.00
700.00
800.00
900.00
1,000.00
1,100.00
Def
ined
Dai
ly D
ose
s
Cost/1000 pt days Defined Daily Doses/1000 pt days
Antimicrobial Use and Cost per 1000 patient-days

Take Home Messages• Must be fully committed to physician
leadership– They see themselves as in charge
• Its about being an accountable physician group– Common bottom line
• Create alignment through shared objectives linked to compensation
• Build your culture purposefully

Take Home Messages
• Integrated care- tactic, planned, many objectives some of which are not about better care at lower cost
• Accountable care- vision, passion, culture focused on better care, lower cost

Forecast• Flawed- health is produced only by
individual actions of “good” clinicians working hard
• New model- Establish teams and organizations accountable for aims and capable of redesigning practice
• Two big questions:– How to change physician behaviors– How to change business model for
providers and payors