managers report of vehicle accident · managers report of vehicle accident instructions: managers...
TRANSCRIPT
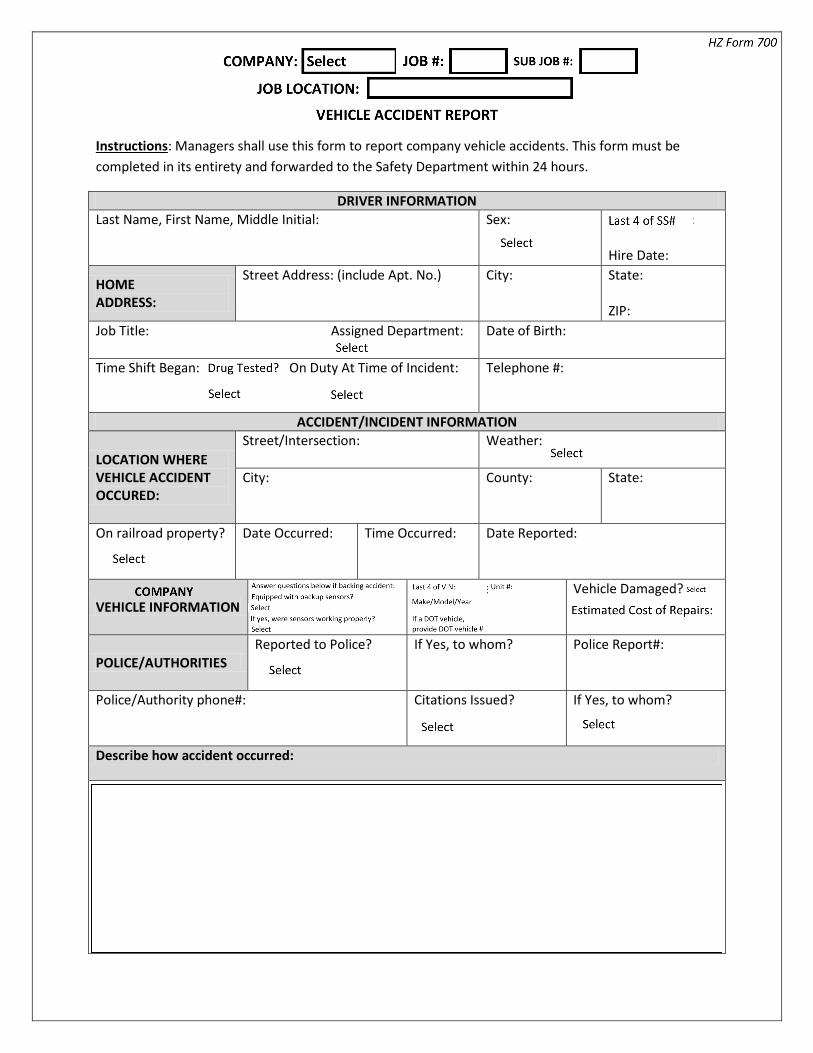
MANAGERS REPORT OF VEHICLE ACCIDENT
Instructions: Managers shall use this form to report company vehicle accidents. This form must be completed in its entirety and forwarded to the Safety Department within 24 hours.
DRIVER INFORMATION Last Name, First Name, Middle Initial: Sex: Employee ID#:
Hire Date:
HOME ADDRESS:
Street Address: (include Apt. No.) City: State: ZIP:
Job Title: Assigned Department: Date of Birth:
Time Shift Began: On Duty At Time of Incident:
Telephone #:
ACCIDENT/INCIDENT INFORMATION
LOCATION WHERE VEHICLE ACCIDENT OCCURED:
Street/Intersection: Weather:
City:
County: State:
On railroad property?
Date Occurred: Time Occurred:
Date Reported:
VEHICLE INFORMATION Vehicle ID #: Vehicle Plate #: Vehicle Damaged?
POLICE/AUTHORITIES Reported to Police?
If Yes, to whom? Police Report#:
Police/Authority phone#:
Citations Issued?
If Yes, to whom?
Describe how accident occurred:

MANAGERS REPORT OF VEHICLE ACCIDENT
Instructions: Managers shall use this form to report company vehicle accidents. This form must be completed in its entirety and forwarded to the Safety Department within 24 hours.
Describe how accident occurred continued:
OTHER DRIVER INFORMATION
VEHICLE OWNER
Name of Owner: Address:
City:
State: Zip:
Phone #:
VEHICLE DRIVER
Name of Driver: Address:
City:
State: Zip:
Phone #:
Driver’s License #: State: Insurance Company: Insurance Policy #:
Was Driver Injured? Was Vehicle Damaged? If Yes, describe damage on lines below:
MANAGERS VEHICLE ACCIDENT REPORT
Instructions: Managers shall use this form to report company vehicle accidents. This form must be completed in its entirety and forwarded to the Safety Department within 24 hours.
List any/all witnesses. Include name, address and phone numbers.
DOCUMENT PREPARERS INFORMATION Name: Signature:
Date: Time:
If employee was injured you must complete the applicable injury forms as well