management of ibs in primary care – haringey guidelines clive onnie bsc(hons) msc phd mrcp...
TRANSCRIPT

Management of IBS in Primary Care – Haringey
GuidelinesClive Onnie
BSc(Hons) MSc PhD MRCP
Consultant Physician and Gastroenterologist
Whittington Hospital


Osler, 1901
Mucous colitis
‘ This Disease is a secretion neurosis of the colon…. Marked nervous symptoms, hysterical outbreaks, hypochondriasis and melancholia. Cases are invariably seen in nervous or hysterical women or in men with neurasthenia….. The diagnosis is rarely doubtful but important not to mistake membranes of other substances thus; the external cuticle of the asparagus and undigested portions of meat or sausage skins not unlike mucus casts….. Treatment is very unsatisfactory. Drugs are of doubtful benefit…. Measures directed to nervous condition are perhaps most important. Sometimes local treatment with Kelly’s long rectal tubes is beneficial. Systematic irrigation of colon should be practiced. Right inguinal colotomy has been performed for intractable cases.….

Aetiology
• Visceral hypersensitivity
• Altered gut flora (SIBO)
• Post infective IBS
• Brain-gut axis

Brain-gut axis

Diagnosis
• Wide array of symptoms, making diagnosis frustrating
• Chronic abdominal pain and altered bowel habits remain the central characteristic of IBS.
• There are no biochemical markers
• Based on symptom based criteria
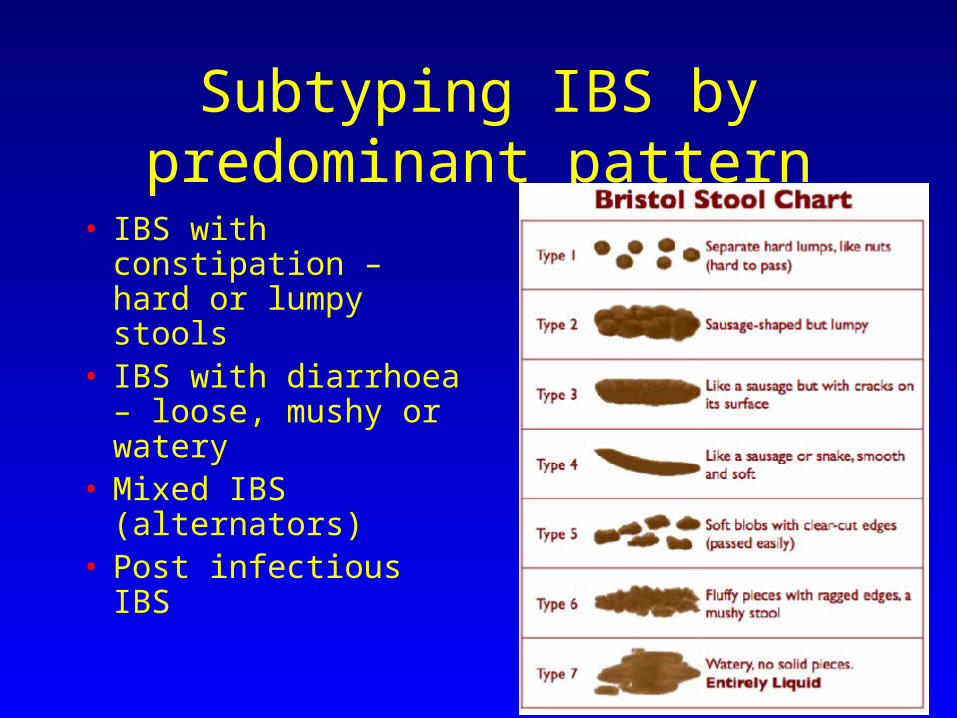
Subtyping IBS by predominant pattern
• IBS with constipation – hard or lumpy stools
• IBS with diarrhoea – loose, mushy or watery
• Mixed IBS (alternators)
• Post infectious IBS
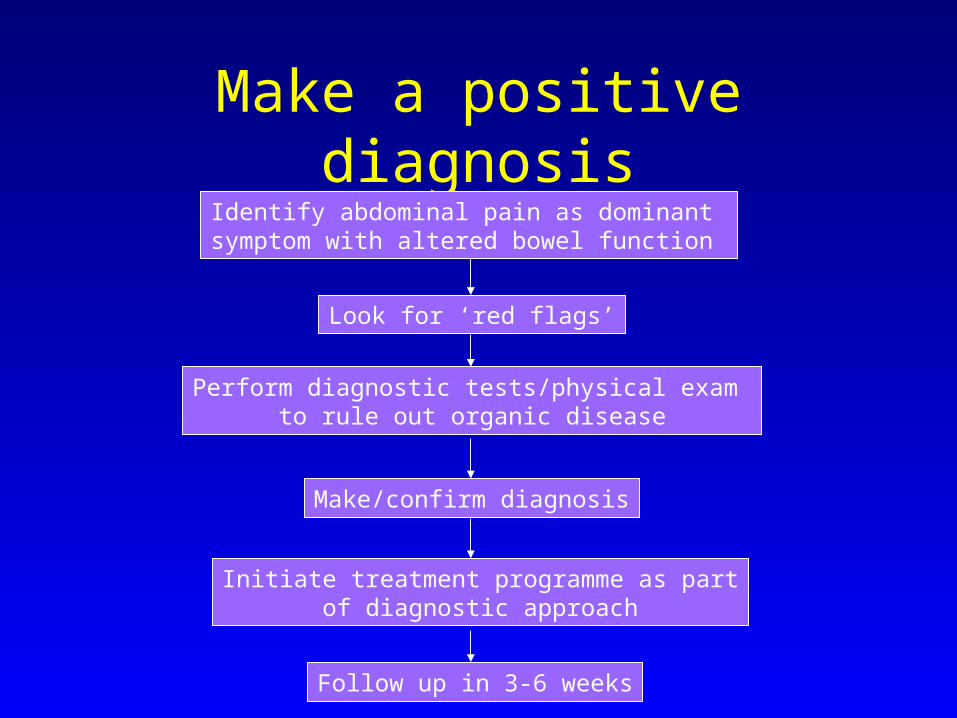
Make a positive diagnosisIdentify abdominal pain as dominant symptom with altered bowel function
Look for ‘red flags’
Perform diagnostic tests/physical exam to rule out organic disease
Make/confirm diagnosis
Initiate treatment programme as partof diagnostic approach
Follow up in 3-6 weeks

Red flag symptoms
• Iron deficiency anaemia
• Fever• Persistent diarrhoea• Rectal bleeding• Weight loss• Palpable mass
• Nocturnal symptoms• Fhx of IBD, CRC,
ovarian cancer, Coeliac
• New onset in patients > 50yrs

Diagnostic tests
• FBC,electrolytes, inflammatory markers, TFT, Coeliac serology + IgA
• ? Faecal calprotectin
Diagnostic tests – faecal calprotectin
• Found in cytoplasm of neutrophils
• Influx of neutrophils into bowel lumen at site of inflammation
• Dead neutrophils release calprotectin, detected in stool
• Cost: £35 ( vs colonoscopy £700)
• Validated + NICE approved

Diagnostic tests:What? When? Who?
• FBC,electrolytes, inflammatory markers, TFT, Coeliac serology + IgA, stool
• Faecal calprotectin
• ?sigmoidoscopy/colonoscopy

Therapeutic Approach• Establish an
empathetic physician-patient relationship
• Education• Reassurance• Chronic benign
nature

Treatment strategy for IBS• End-organ and dietary treatment
– Exploration of dietary triggers– Low FODMAP diet– Anti-diarrhoeals and low dose TCA– Smooth-muscle relaxants for pain
• Centrally targeted treatment– Physiological explanation of symptoms / education + reassurance– Hypnotherapy / pyschotherapy / CBT / biofeedback– antidepressants
• Receptor-active agents– 5HT4 receptor agonists, linaclotide, lubiprostone
• Probiotics / Antibiotics – metronidazole / rifaximin• Herbal / aloe vera

End organ treatment - diet
• Many patients benefit from caffeine and alcohol exclusion
• Lactose intolerance: ‘milk challenge’
• Wheat exclusion
• 20-70% response from exclusion diets – usefulness of dietician

Diet

What are FODMAPs?
Fermentable
Oligosaccharides – fructans, galactans
D
M
A
P

What are FODMAPs?
Fermentable
O
Disaccharides - lactose
M
A
P

What are FODMAPs?
Fermentable
O
D
Monosaccharides
A
P

What are FODMAPs?
Fermentable
O
D
M
And
Polyols
FODMAPs – mechanisms of action
Fructose Fructans Lactose Galactans Polyols

FODMAPs – mechanisms of action
Osmotic load Rapidly fermented
CH4 H2
Fructose Fructans Lactose Galactans Polyols
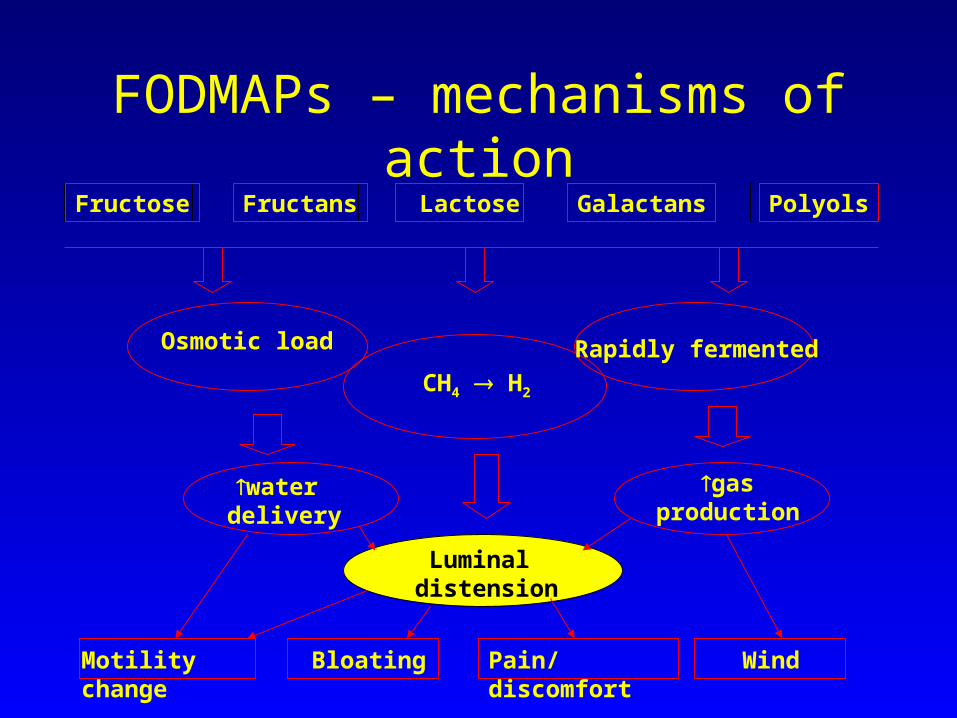
FODMAPs – mechanisms of action
Osmotic load Rapidly fermented
CH4 H2
water delivery
gasproduction
Luminal distension
Motility change Bloating Pain/discomfort Wind
Fructose Fructans Lactose Galactans Polyols
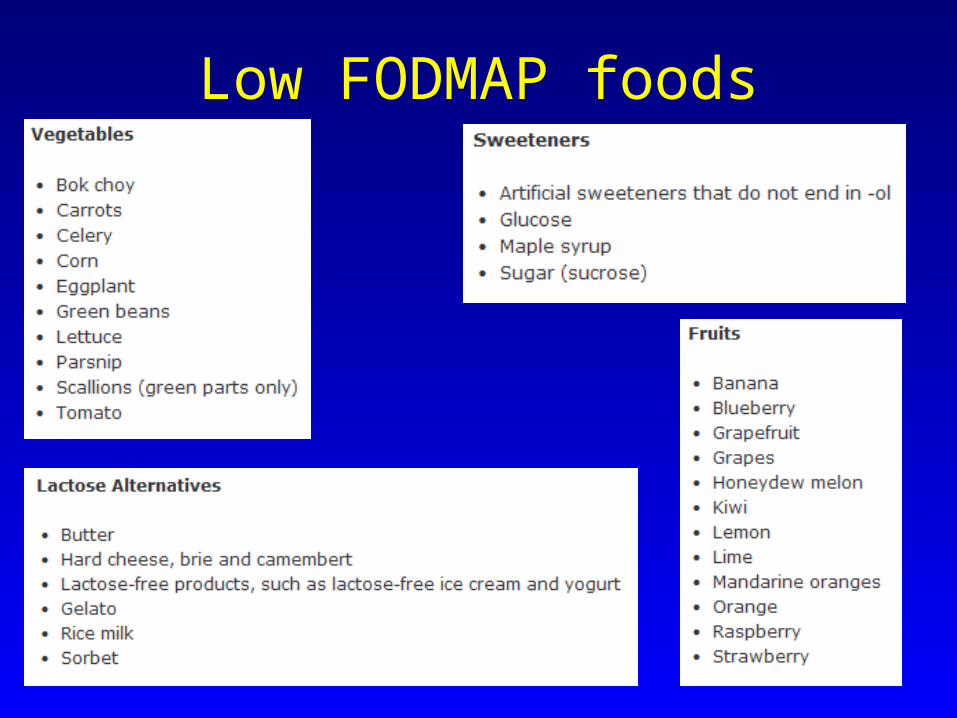
Low FODMAP foods

Low FODMAP diet
• Validated
• Rationale is attractive and easily understood
• Advice given in the context of usual diet
• Messages delivered positively
• High adherence (> 70%)

End organ: Anti-diarrhoeals and TCA
• Loperamide – single or divided doses on regular basis
• Tricyclic antidepressants: exert an end-organ effect on small-intestinal motility and to prolong orocaecal and whole-gut transit time
• SSRI – less evidence. Shortens transit time.• Cholestyramine 4g 1-6x/day

End organ: Laxatives and IBS
• Osmotic preferably• Lactulose is avidly metabolised gas and
bloating• Polyethylene glycol preparations (movicol /
laxido)• Stimulants – bisacodyl/senna• Alternatives:
– Prucalopride– Linaclotide– Lubiprostone

End organ: Smooth muscle relaxants
• Direct smooth muscle relaxants or antimuscarinic drugs
• eta-analysis does suggest usefulness in treatment of abdominal pain
• Peppermint oil – RCT suggests benefit• Patients often benefit from combination
treatment e.g laxative + antispasmodic

Centrally targeted treatment
• Most results of centrally targeted therapies show a beneficial effect on IBS
• Emphasizes multi-disciplinary approach
• Relaxation therapy – reduces symptoms and number of medical consultations

Hypnotherapy

Haringey IBS care pathway


Graduated Treatment Approach
Severe
Moderate
Mild
•Multidisciplinary approach•Referral to pain management
+
•Pharmacotherapy•Pyschological treatments
+•Education•Reassurance•Dietary modification

Summary
• Important to establish a positive diagnosis of IBS
• Most patients will respond to therapy
• Optimum medical management will involve a multi-modality approach
• NICE and GUT guidelines

Case scenario 1
• 36 yr old male• 2yr history significant bloating, cramp
relative constipation then explosive diarrhoea
• Dietary changes no help following dietetic review
• Otherwise well

Case scenario 1
• Blood tests, Coeliac serology normal
• OGD/colon normal
• Previous review by dietician
Case scenario 1
• Blood tests, Coeliac serology normal
• OGD/colon normal
• Previous review by dietician
• Low FODMAP diet
• PRN mebeverine
• Education

Case scenario 1
Low FODMAP diet:
• Much better
• Able to identify precipitants
• More in control
• Uses mebeverine PRN basis

Case scenario 2
• 30yr old female• Longstanding abdominal pain• Endometriosis – most recent
laparoscopy NAD• Weight loss• Previous CBT for depression/anxiety• Chronic constipation – BO every 2/52,
nausea
Case scenario 2
• Multiple previous investigations – bloods/OGD/colon/CT/laparoscopy
• Transit study – slow transit
• Multiple laxatives – senna,movicol, dulcolax

Case scenario 2
• Prescribed prucalopride 2mg od
• 2/12 f/u: bowels open most days
• Weight increased
• Eating more