management of apical lesions
TRANSCRIPT
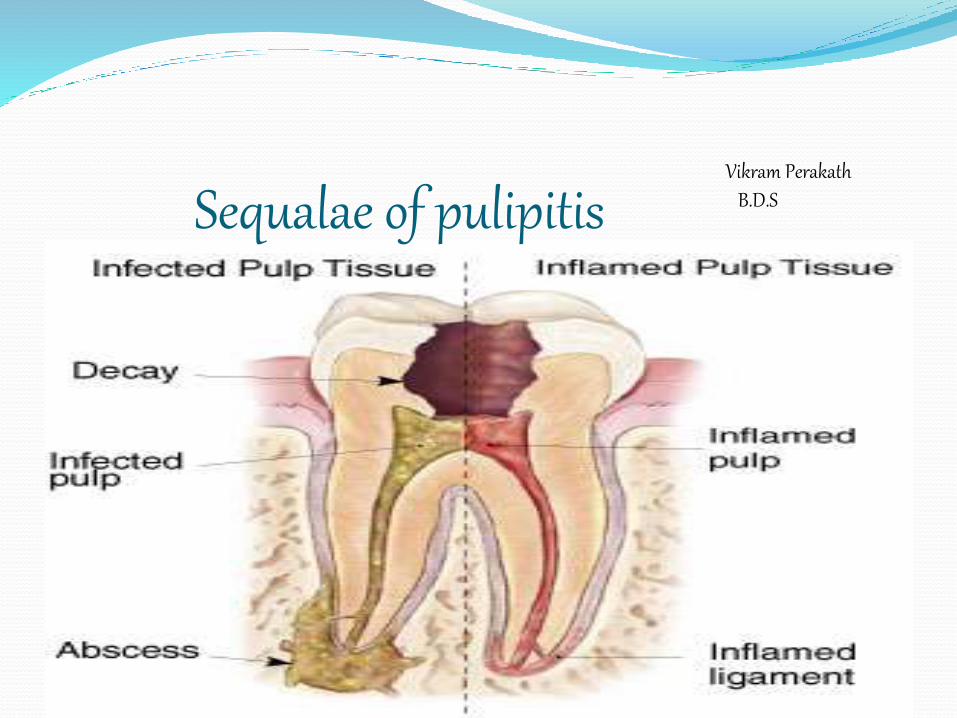
Sequalae of pulipitisVikram Perakath
B.D.S
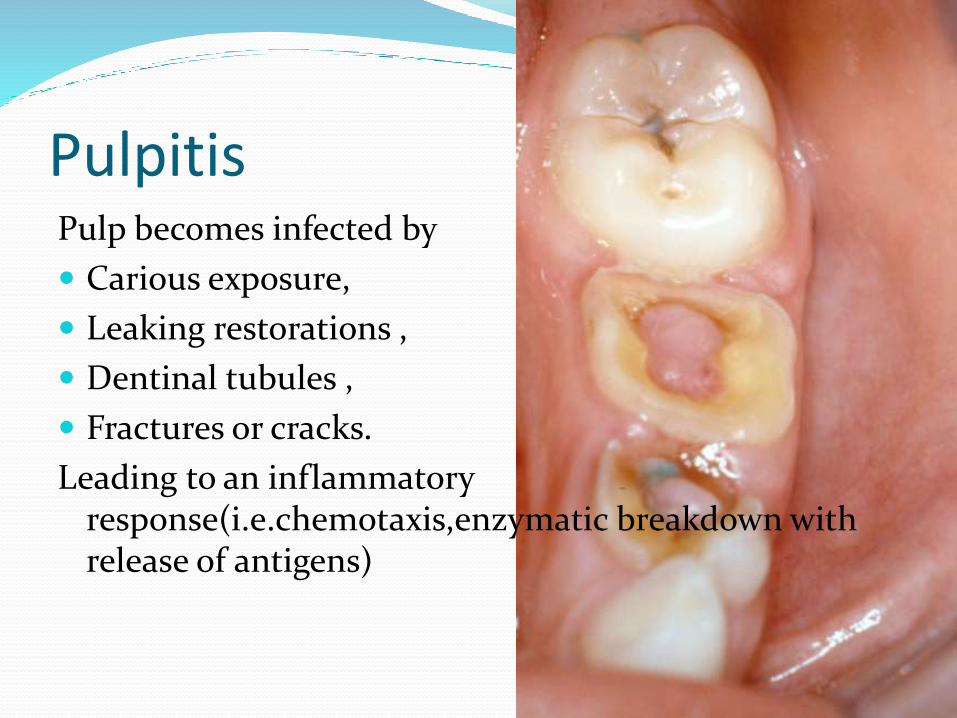
PulpitisPulp becomes infected by
Carious exposure,
Leaking restorations ,
Dentinal tubules ,
Fractures or cracks.
Leading to an inflammatory response(i.e.chemotaxis,enzymatic breakdown with release of antigens)
Antigens in the surrounding tissue.
Leads to an immune response from the tissue-antibodies.
The response destroys much of the peripicaltissue leading to the formation of various types of apical periodontal lesions.
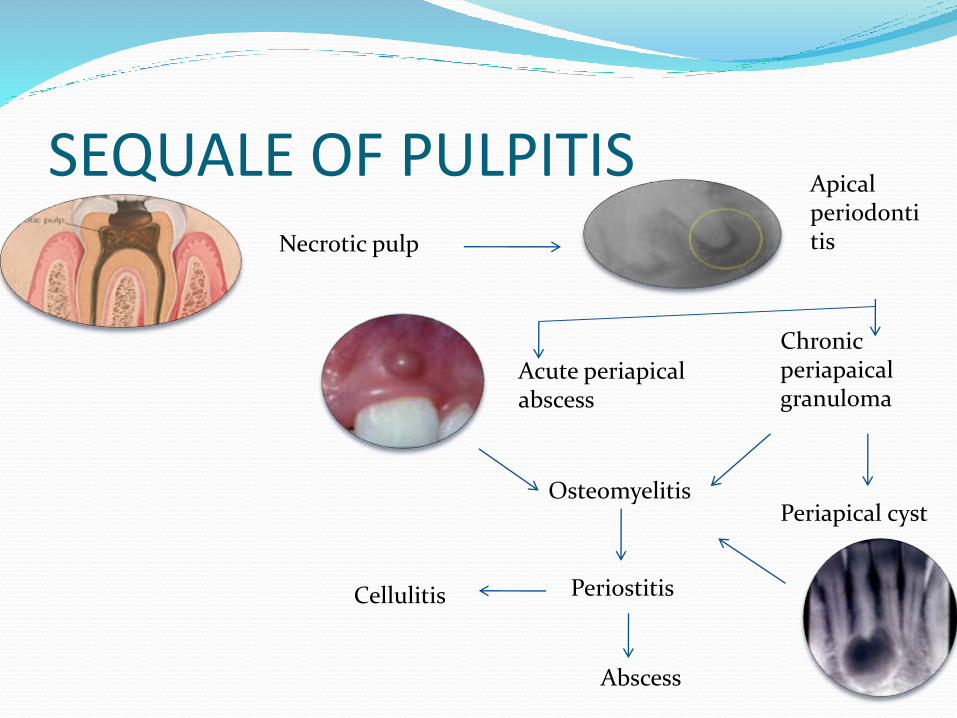
SEQUALE OF PULPITISNecrotic pulp
Apical periodontitis
Acute periapicalabscess
Chronic periapaicalgranuloma
Periapical cystOsteomyelitis
PeriostitisCellulitis
Abscess
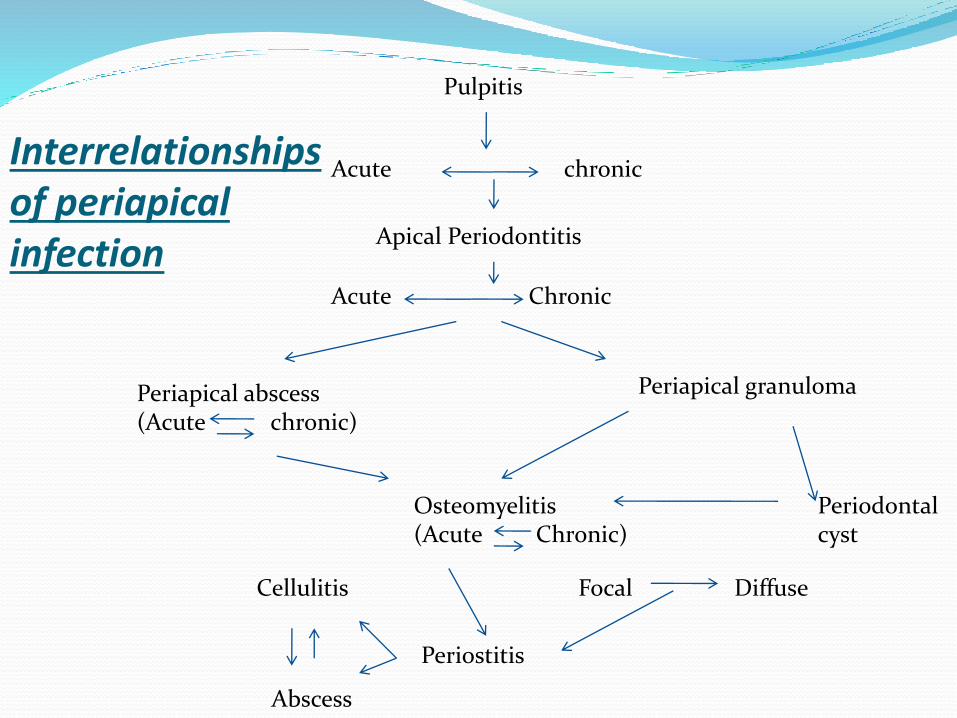
Apical Periodontitis
Periapical abscess(Acute chronic)
Periapical granuloma
Osteomyelitis(Acute Chronic)
Periodontal cyst
Periostitis
Cellulitis
Abscess
Acute chronic
Pulpitis
Acute Chronic
Focal Diffuse
Interrelationships of periapicalinfection
Apical periodontitis It is the inflammation of the periodontal ligament around the root apex.
The common causes are
Spread of Infection following pulp necrosis
Occlusal Trauma,
Chemical irritation(Overextended R.C.T medicaments)
There are two types-Acute Apical Periodontitis(AAP)
Chronic Apical Periodontitis(CAP)
Acute periodontitis
Previous h/o pulpitis
Thermal changes do not induce pain
Tooth is elevated from the socket with tenderness
•AKA periapical granuloma
•Sequale of pulpitis or acute periapical periodontitis.
•Tooth involved is usually non-vital & maybe tender
Chronic periodontitis
Treatment Acute periodontitis-
If there is occlusal trauma-selective grinding
If pulpally involved-R.C.T/Extraction
Chronic periodontitis(Periapical granuloma)-
Extraction of involved teeth
R.C.T/R.C.T with apisectomy
If left untreated it will transform intoApical periodontal cyst
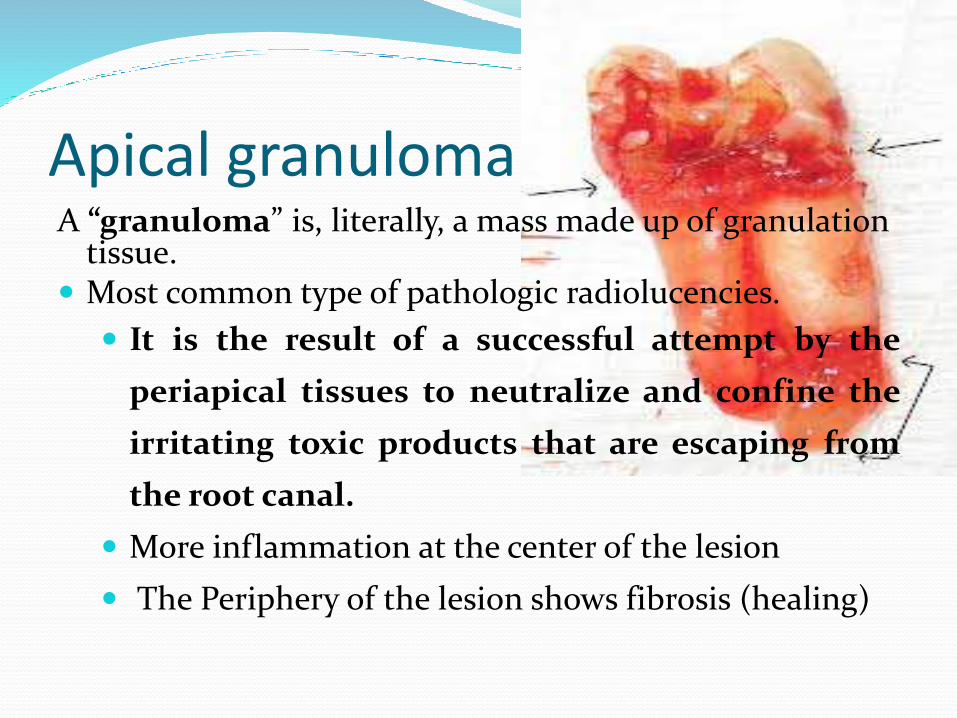
Apical granulomaA “granuloma” is, literally, a mass made up of granulation
tissue. Most common type of pathologic radiolucencies.
It is the result of a successful attempt by the
periapical tissues to neutralize and confine the
irritating toxic products that are escaping from
the root canal.
More inflammation at the center of the lesion
The Periphery of the lesion shows fibrosis (healing)
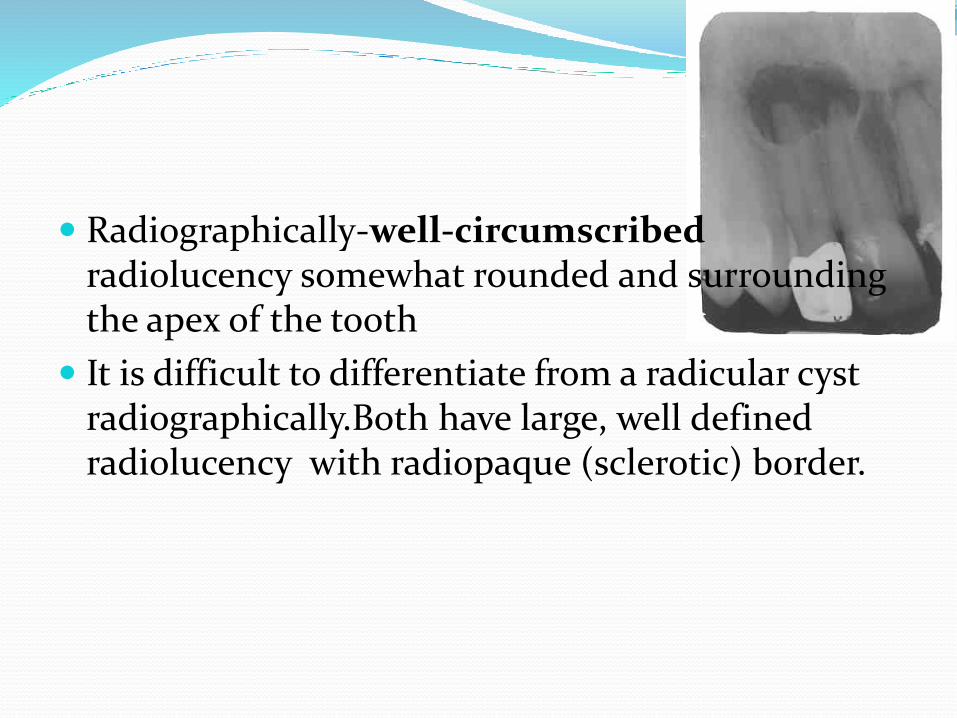
Radiographically-well-circumscribed radiolucency somewhat rounded and surrounding the apex of the tooth
It is difficult to differentiate from a radicular cyst radiographically.Both have large, well defined radiolucency with radiopaque (sclerotic) border.

Apical periodontal cyst(AKA Radicular cyst,Periapicalcyst,Dental cyst,Root end cyst) It is usually a sequale of Periapical Granuloma
It is a true cyst,since the lesion consists of a pathological cavity lined by epithelium and is often fluid filled.
The epithelium is from cell rests of Malassez.
Clinical features:
Usually asymptomatic
Most common in maxillary anteriors.
May undergo acute exacerbation of the inflammatory process and develop rapidly into an abscess,then cellulitis.
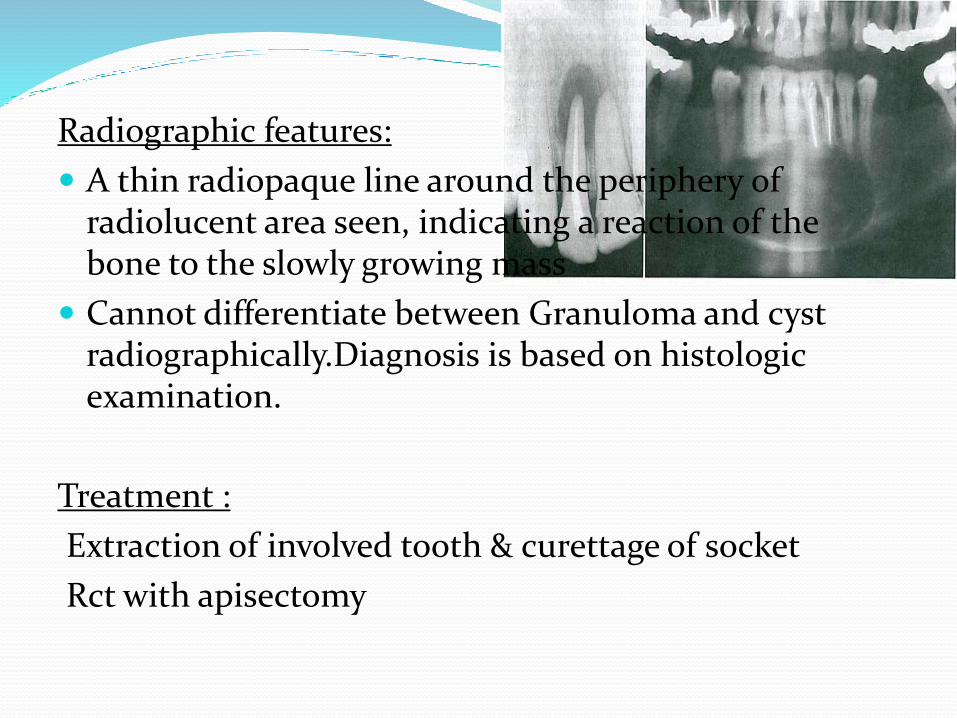
Radiographic features:
A thin radiopaque line around the periphery of radiolucent area seen, indicating a reaction of the bone to the slowly growing mass
Cannot differentiate between Granuloma and cyst radiographically.Diagnosis is based on histologicexamination.
Treatment :
Extraction of involved tooth & curettage of socket
Rct with apisectomy
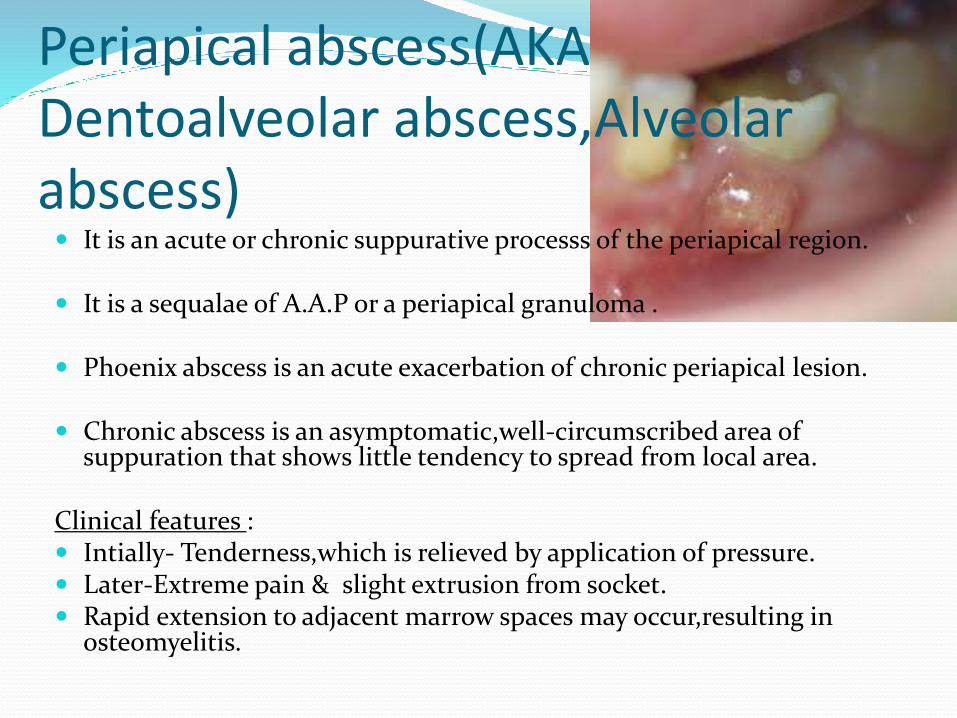
Periapical abscess(AKA Dentoalveolar abscess,Alveolarabscess) It is an acute or chronic suppurative processs of the periapical region.
It is a sequalae of A.A.P or a periapical granuloma .
Phoenix abscess is an acute exacerbation of chronic periapical lesion.
Chronic abscess is an asymptomatic,well-circumscribed area of suppuration that shows little tendency to spread from local area.
Clinical features : Intially- Tenderness,which is relieved by application of pressure. Later-Extreme pain & slight extrusion from socket. Rapid extension to adjacent marrow spaces may occur,resulting in
osteomyelitis.
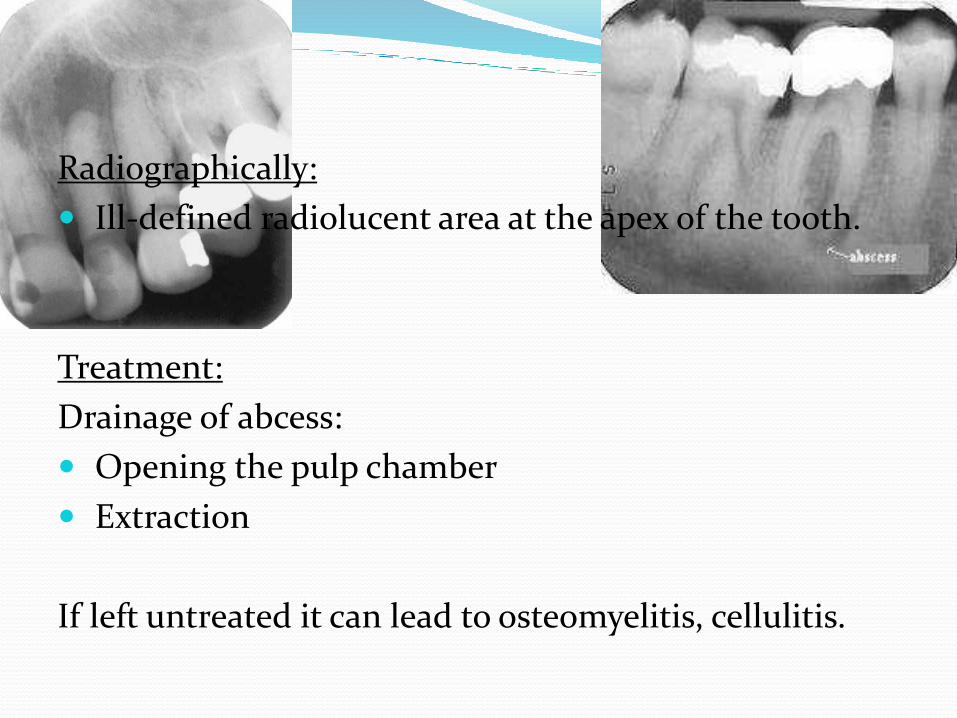
Radiographically:
Ill-defined radiolucent area at the apex of the tooth.
Treatment:
Drainage of abcess:
Opening the pulp chamber
Extraction
If left untreated it can lead to osteomyelitis, cellulitis.
Osteomyelitis Inflammation of bone & its marrow contents.
Though the dividing line between osteomyelitis and an abscess is unclear,osteomyelitis is usually reserved for infections that spread through the bone to a larger extent.
Predisposing factors :
Fracture due to trauma,RTA, radiation damage, ostopetrosis,gun-shot wounds,Paget’s disease.
Systemic conditions: DM, sickle cell anemia, chronic alcoholism,malnutrition,acute leukemia.
Acute suppurative osteomyelitis It is a serious sequale of periapical infection resulting in the diffuse spread of infection
throughout the medullary spaces with subsequent necrosis of varible amount of bone.
Common causes: Dental infection Abscess(if virulent and not walled off) Acute exacerbation of a granuloma or cyst
Clinical features:
In the maxilla,tends to be localised to involved tooth but in the mandible it is more diffuse & widespread.
Pain, trismus, paresthesia of lip, elevation of temp,regional lymphadenopathy,loose and tender involved teeth
Wbc is elevated, pus from gingival margin.
Radiographically:
Changes can be seen after 1-2 weeks.Ill-defined margins & moth eaten appearance.
Treatment :
Debridement , Drainage & Drugs(antibiotic therapy)
Surgical removal for lesions with large sequestrum.
If left untreated,may proceed to Periostitis,soft-tissue abscess or cellulitis.
Chronic suppuartive osteomyelitis
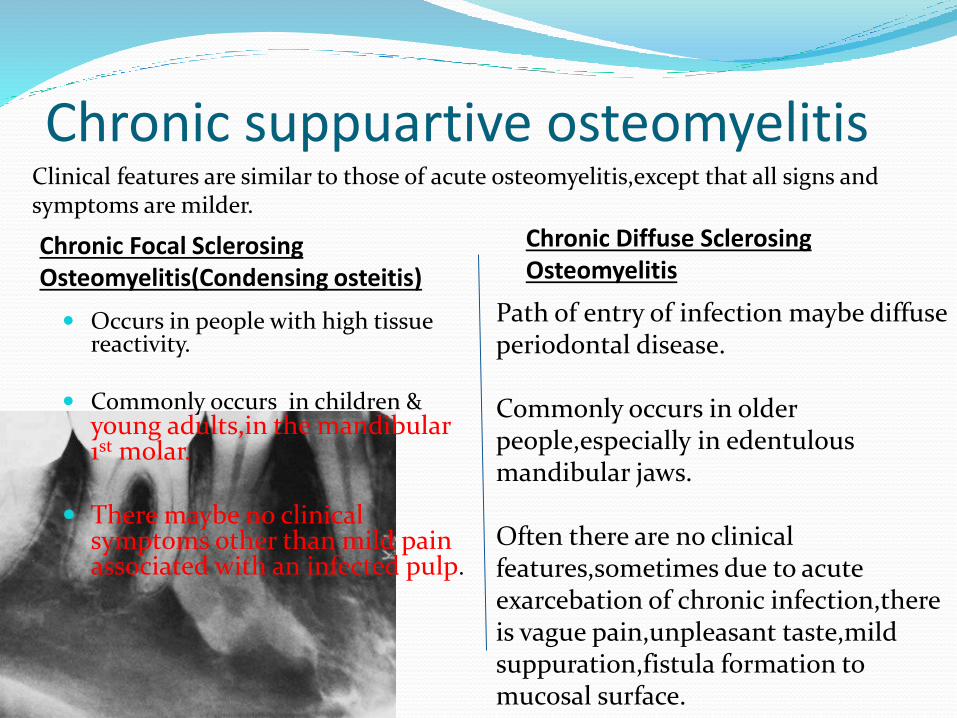
Occurs in people with high tissue reactivity.
Commonly occurs in children & young adults,in the mandibular1st molar.
There maybe no clinical symptoms other than mild pain associated with an infected pulp.
Clinical features are similar to those of acute osteomyelitis,except that all signs and symptoms are milder.
Path of entry of infection maybe diffuse periodontal disease.
Commonly occurs in older people,especially in edentulous mandibular jaws.
Often there are no clinical features,sometimes due to acute exarcebation of chronic infection,thereis vague pain,unpleasant taste,mildsuppuration,fistula formation to mucosal surface.
Chronic Focal SclerosingOsteomyelitis(Condensing osteitis)
Chronic Diffuse SclerosingOsteomyelitis
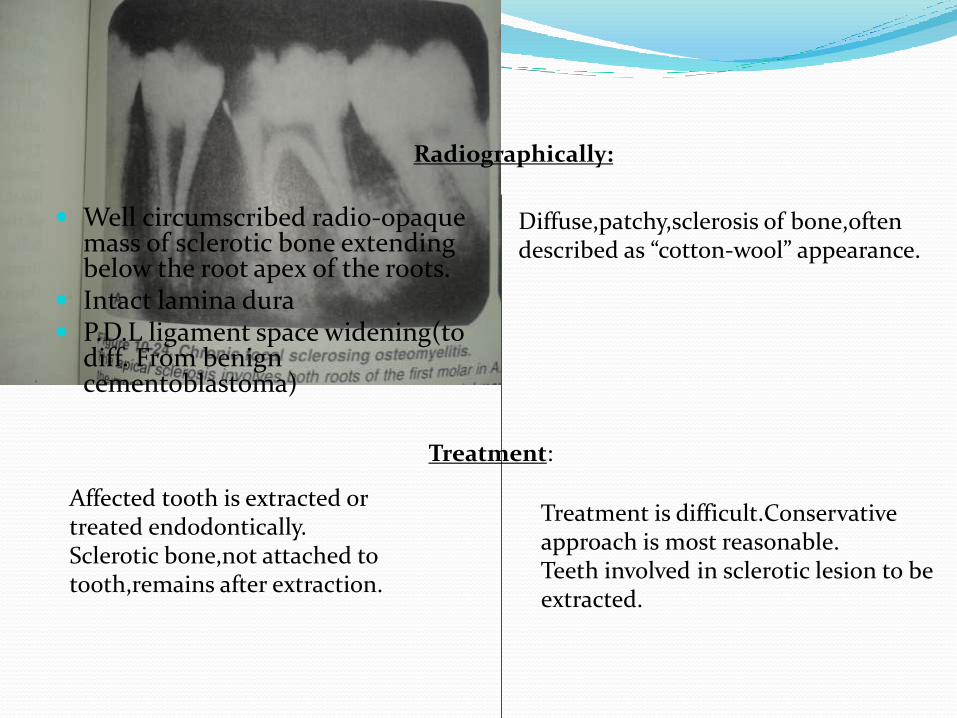
Well circumscribed radio-opaque mass of sclerotic bone extending below the root apex of the roots.
Intact lamina dura P.D.L ligament space widening(to
diff. From benign cementoblastoma)
Diffuse,patchy,sclerosis of bone,oftendescribed as “cotton-wool” appearance.
Radiographically:
Treatment:
Affected tooth is extracted or treated endodontically.Sclerotic bone,not attached to tooth,remains after extraction.
Treatment is difficult.Conservativeapproach is most reasonable.Teeth involved in sclerotic lesion to be extracted.
Chronic Osteomyelitis with Proliferative Periostitis(Garre’s chronic non-suppurative sclerosingosteitis,periostitis ossificans)
Shows focal gross thickening of the periosteum,withperipheral reactive bone formation due to infection or irritation.
Clinical features:
Almost exclusive to mandible,in premolar and molar region,of children and young adults.
Presents as pain in the jaw with a bony hard swelling on the outer surface of the jaw.
Radiographically:
Occlusal radiograph shows focal overgrowth of bone on the outer surface of the cortex,which maybe described as duplication of the cortical layer of bone.
Intraoral radiograph will reveal a carious tooth opposite the hard bony mass.
Treatment:
Extraction or R.C.T of infected tooth.
Biopsy to confirm diagnosis.
References Shafer’s Textbook of Oral Pathology(7th edition)
Dr.Vikram Perakath
B.D.S
Non Surgical management of apical lesions The aim of non-surgical root canal therapy is
the elimination of infection from the root canal and the prevention of re-infection by root filling
Periapical lesions develop as sequelae to pulp disease. They often occur without any episode of acute pain and are discovered on routine radiographic examination.
All inflammatory periapical lesions should be initially treated with conservative nonsurgical procedures.
The ultimate goal of endodontic therapy should be to return the involved teeth to a state of health and function without surgical intervention.
METHODS FOR NONSURGICALMANAGMENT OF PERIAPICALLESIONS1. Conservative root canal treatment without
adjunctive therapy
2. Decompression technique
3. Active nonsurgical decompression technique
4. Aspiration and irrigation technique
5. Method using calcium hydroxide
6. Lesion sterilization and repair therapy
7. Apexum procedure
Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen.
Establishes drainage and relieves pressure. Once the drainage stops,fibroblasts begin to proliferate and deposit collagen; this compresses the capillary network, and the epithelial cells are thus starved, undergo degeneration, and are engulfed by the macrophages.
Causes transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst.
Weekly debridement and drying of the canals over a period of two to three weeks, followed by obturationhas led to a complete resolution of lesions by 12 to 15 months.
Decompression technique
The placement of a drain into the lesion, daily irrigation using 0.12% chlorhexidine, periodic length adjustment, and maintenance of the drain, for various periods of time
Advantages: Simple procedure,minimal damage,easilytolerated.
Contraindicated: Large dental granulomas or any solid cellular lesion.
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system (Ultradent,Salt Lake, Utah) to create a negative pressure, which results in the decompression of large periapical lesions.
The high-volume suction aspirator is connected to a micro 22-gauge needle, which is inserted in the root canal and activated for 20 minutes, creating a negative pressure, which results in aspiration of the exudate.
When the drainage partially stops, the access cavity is closed with temporary cement,which helps in maintaining bacterial control.
Advantage: Minimally invasive, as the entire procedure is done through the root canal and causes less discomfort for the patient
Aspiration and irrigation techniqueAspiration of the cystic fluid from the periapcial lesion
using a bucco-palatal approach. An 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid.
A second syringe filled with saline is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant.
Disadvantage: Buccal and palatal wounds that may cause discomfort to the patient.
Method using calcium hydroxideCalcium hydroxide has bactericidal effects. It creates
favourable conditions for periapical repair and stimulates hard tissue formation.
The four- fold effect of Ca(OH)2:
(a) anti-inflammatory activity,
(b) neutralization of acid products,
(c) activation of the alkaline phosphatase, and
(d) antibacterial action
Calcium hydroxide is used as an antibacterial agent for only 15 days, following which it is irrigated out of the canal using sodium hypochlorite.
Lesion sterilization and repair therapy The Cariology Research Unit of the Niigata UniversitySchool of Dentistry has developed the concept of ‘LesionSterilization and Tissue Repair (LSTR)’ therapy that usesa triple antibiotic paste of ciprofloxacin, metronidazole,and
minocycline, for disinfection of oral infectious lesions. Repair of damaged tissues can be expected if lesions are
disinfected. The combination of drugs has been shown to penetrate
efficiently through dentine from the prepared root canals. The commercially available drugs are powdered and mixed in a
ratio of 1:3:3 (3 Mix) and mixed either with macrogol-propylene glycol (3 Mix-MP) or a canal sealer(3 Mix-sealer)
Disadvantage is tooth discoloration induced by minocycline.
Apexum procedure The Apexum procedure uses two sequential rotary
devices, the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd, Or Yehuda, Israel), designed to extend beyond the apex and mince the periapicaltissues on rotation in a lowspeed handpiece, followed by washing out the minced tissue.
Significantly faster periapical healing is noted with this technique.

Surgical management of apical lesions
In the following slides I will talk about the principles of management of apical lesions or odontogenic deep fascial space infections,as laid down by The late Dr. Larry Peterson.
There are eight sequential steps that are to be followed with thoroughness andgood judgment to ensure a high level ofcare for these occasionally life-threatening infections.
The eight steps in the management of odontogenicinfections are as follows:
1. Determine the severity of infection.
2. Evaluate host defenses.
3. Decide on the setting of care.
4. Treat surgically.
5. Support medically.
6. Choose and prescribe antibiotic therapy.
7. Administer the antibiotic properly.
8. Evaluate the patient frequently.
OR
1.Severity of infection
2.Host defenses
3.Care setting
4.Surgical treatment
5. Medical support
6. Prescribe antibiotics
7.Administer antibiotics properly
8.Evaluate Frequently
Step 1:
Determine the Severity of Infection
Three major factors must be considered
in determining the severity of an infection of the head and neck:
1.Anatomic location
2.Rate of progression
3.Airway compromise.
Anatomic LocationThe anatomic spaces of the head and neck can be graded in severity by the level to which they threaten the airway or vital structures, such as the heart and mediastinum or the cranial contents.
Buccal
Infraorbital
low severity
Vestibular
Subperiosteal
Masticatory space:
Submasseteric
Pterygomandibular,
Superficial and
Deep temporal spaces
Perimandibular spaces:
Submandibular
Submental
Sublingual
Moderate severity
Lateral pharyngeal
Retropharyngeal
The danger space highseverity
Mediastinum
Cavernous sinus thrombosis
The Danger space
It is found between the buccopharnygeal fascia and alarfascia,posterior to retropharygeal space,it gets its common name from the risk that an infection in this space can spread directly to the thorax, it is sometimes also referred to as the Alar space.)
A severity score (SS) was devised that assigned a numerical value of 1 to 4 for involvement
of each of the anatomic spaces involved,be it low(1), moderate(2), severe(3) or extreme severity(4), respectively.
Severity score = 1 (low risk to airway or vital structures)
Vestibular
Subperiosteal
Space of the body of the mandible
Infraorbital
Buccal
Severity score = 2 (moderate risk to airway or vital structures )
Submandibular
Submental
Sublingual
Pterygomandibular
Submasseteric
Superficial temporal
Deep temporal (or infratemporal)
Severity score = 3 (high risk to airway or vital structures)
Lateral pharyngeal
Retropharyngeal
Pretracheal
Severity score = 4 (extreme risk to airway or vital structures)
Danger space
Mediastinum
Intracranial infection
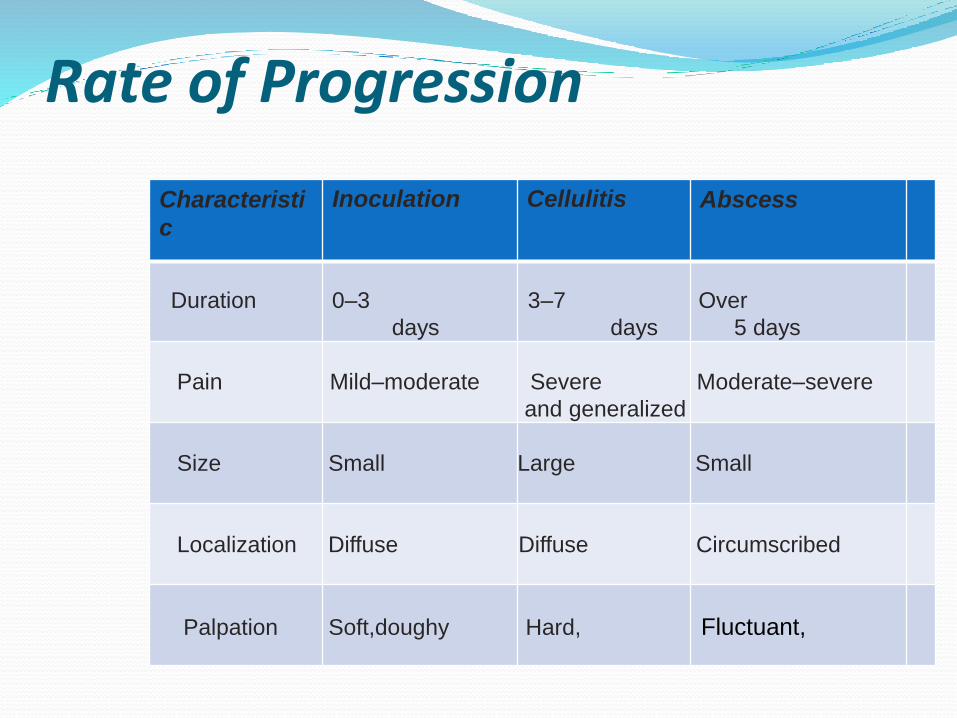
Characteristi
c
Inoculation Cellulitis Abscess
Rate of Progression
Duration 0–3 3–7 Over
days days 5 days
Pain Mild–moderate Severe Moderate–severe
and generalized
Size Small Large Small
Localization Diffuse Diffuse Circumscribed
Palpation Soft,doughy Hard, Fluctuant,
Necrotising fasciitisA special note should be made of an especially rapidly
progressive infection called necrotizing fasciitis.
It is a rapidly spreading infection that follows the platysma muscle down the neck and onto the anterior chest wall.
Airway CompromiseThe most frequent cause of death in odontogenic infections
is airway obstruction.
Complete airway obstruction is a surgical emergency. Insufficient or absent air movement inspite of inspiratoryefforts will be apparent.Check O2 saturaltion levels.
One brief attempt at endotracheal intubation maybe made,but a direct surgical approach to the airway by cricothyroidotomy or tracheotomy is more predictably successful.
Infection in the region of surgical airway access is not a contraindication to an emergency cricothyroidotomy or tracheotomy.
Step 2: Evaluate Host DefensesImmune System Compromise:The medical conditions that can interfere with proper
function of the immune system Diabetes Steroid therapy Organ transplants Malignancy Chemotherapy Chronic renal disease Malnutrition Alcoholism End-stage AIDS

Other conditions that impair immune function:
Malnutrition,
Alcoholism,
Chronic renal disease.
Systemic Reserve The host response to severe infection can place a
severe physiologic load on the body.
An elevated temperature at an advanced age is not only a sign of a particularly severe infection, but also of decreased cardiovascular and metabolic reserve, due to the demands placed on the elderly patient’s physiology by the high grade long standing fever associated with the infection.
Evaluation of W.B.C count is important in determining the severity of infection as well as in estimating the length of hospital stay.
The physiologic stress of a serious infection can disrupt previously well established control of systemic diseases such as diabetes, hypertension, and renal disease.
An otherwise mild or moderate infection may be a significant threat to the patient with systemic disease, and the surgeon should be careful to evaluate and manage concurrent systemic diseases in conjunction with direct management of the infection
Step 3: Decide on theSetting of CareAdmission of a patient to hospital is indicated when: Temperature > 101°F (38.3°C) Dehydration -This can be assessed by elevated urine
specific gravity (over 1.030) or an elevated blood urea nitrogen (BUN).
Infections in deep spaces that have a severity score of 2 or greater, can hinder access to the airway for intubation by causing trismus, directly compress the airway by swelling, or threaten vital structures directly and indicates hospital admission.
Need for general anesthesia Need for inpatient control of systemic disease
Step 4: Treat Surgically Secure the airway
Incision and drainage
Straight forward treatments, such as removal of the involved teeth, intraoral incision and drainage, and empiric antibiotic therapy, are almost always successful.
Culture and Sensitivity Testing if economically viable.

Step 5: Support Medically Hydration -Reestablishment of electrolyte balance. A
70 kg patient with a fever of 102.2°F would have a daily fluid requirement of about 3,100 mL.
Nutrition,
Control of fever-
Initial temperature- Above 39.4’C or 103’F fever,it can become destructive by increasing metabolic and cardiovascular demands, beyond physiologic reserve capacity of the patient.
Administration of acetaminophen or aspirin
Step 6: Choose and PrescribeAntibiotic Therapy
Severity of Infection Antibiotic of Choice
Outpatient Penicillin
Clindamycin
Cephalexin
In case of penicillin allergy:
Clindamycin
Moxifloxacin
Metronidazole alone
Inpatient Clindamycin
Ampicillin + metronidazole
Ampicillin + sulbactam
In case of Penicillin allergy:
Clindamycin
MoxifloxacinMetronidazole alone
Step 7: Administer theAntibiotic Properly The tissue-serum level of antibiotics determines their
effectiveness.
Orally administered antibiotics achieve much lower serum levels at a slower rate than when they are injected directly into the vascular system intravenously.
Step 8: Evaluate the PatientFrequentlyIn outpatient infections that have been treated by tooth
extraction and intraoral incision and drainage, The most appropriate initial follow-up appointment is usually at 2 days postoperatively for the following reasons:
1. Usually the drainage has ceased and the drain can be discontinued at this time.
2. There is usually a discernible improvement or deterioration in signs and symptoms.
For odontogenic deep fascial space infections that are serious enough for hospitalization, daily clinical evaluation and wound care are required for at least two to three days.
If there are no signs of clinical improvement in these 2-3 days, then it may be necessary to begin an investigation for possible treatment failure.
One of the best methods of re-evaluation is the postoperative C.T scan.
Severe odontogenic infections can be the most challenging cases that an oral and maxillofacial surgeon will be called on to treat.
Often the patient with a severe odontogenic infection has significant systemic or immune compromise, and the constant threat of airway obstruction due to infections in the maxillofacial region raises the risk of such cases severely
The eight steps in the treatment of severe odontogenicinfections, first outlined by Dr. Larry Peterson, remain the fundamental guiding principles that oral and maxillofacial surgeons must use in successful management of these cases.
The surgeon’s mind must always remain open to the possibility of treatment failure, an error in initial diagnosis, antibiotic resistance, and previously undiagnosed medically compromising conditions.
References Nonsurgical management of periapical lesions-
Marina Fernandes, Ida de Ataide,Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Bambolim, Goa - 403 601, IndiaJournal of Conservative Dentistry | Oct-Dec 2010 | Vol 13 | Issue 4
Peterson's Principles of Oral and Maxillofacial Surgery 2nd Ed 2004.

Thank you