lung scan & radionuclide venography for md4-ns students_2017
TRANSCRIPT
Nuclear Medicine Studies for MD4_NS
Jiraporn Sriprapaporn, M.D.
Division of Nuclear Medicine
Department of Radiology
Siriraj Hospital 16 February 2017
Nuclear Oncology
Lung Scan & RNV
Lung Scan: - Ventilation (V) & Perfusion (Q)
Indications : Diagnosis of pulmonary embolism
Radiotracers :
Ventilation (V) lung scan : Xe-133, Tc-99m DTPA aerosol, Technegas
Perfusion (Q) scan :Tc-99m MAA
Patient preparation : None
Lung scan
By Jiraporn Sriprapaporn

Mechanism
Ventilation lung scan: Compartmental localization
Perfusion lung scan: capillary blockage 1/1000
The biologic half-life of the MAA in the lungs is about 1.5–3 hrs.
Principles of V/Q Lung Scan
By Jiraporn Sriprapaporn

Injection of Tc-99m MAA in supine position
Static imaging 6-8 views +/- SPECT/CT
Perfusion Lung Scan
By Jiraporn Sriprapaporn

PE Segmental perfusion defects
Defect size // size of clot, location of occlusion
PE: Pathophysiology
By Jiraporn Sriprapaporn

Bronchopulmonary Segments
By Jiraporn Sriprapaporn

O2
Radioaerosol Ventilation Scan
By Jiraporn Sriprapaporn

Tc-99m DTPA Radioaerosol Ventilation Scan
By Jiraporn Sriprapaporn

Technegas
By Jiraporn Sriprapaporn

Technegas Ventilation Scan
By Jiraporn Sriprapaporn

NORMAL:
Uniform distribution of the radioactivity
ABNORMAL”
Non-uniform distribution
Defects
Size: small (< 25%), medium (25-75%), large (>75%)
Number
Pattern: Segmental (// bronchopulmonary segments) or non-segmental defects.
Interpretation of V/Q Lung Scan
V+ Q + CXR within 24 hrs.
By Jiraporn Sriprapaporn

A: Ventilation
B: Perfusion
Normal V/Q Lung Scan
By Jiraporn Sriprapaporn

V/Q match: parenchymal or airway diseases
V/Q mismatch: vascular occlusion (pulmonary embolism)
Findings
By Jiraporn Sriprapaporn

Comparison of V/Q Scan and Pulmonary CTA
V/Q Lung Scan
• Advantages
• High NPV in patient with low pretest prob.
• High PPV in patient with high pretest prob.
• Safe, no contrast reaction
• Lower radiation- good for F/U
• Disadvantages
• Limited available
• Longer exam time
• Needs Pt. cooperation (V)
• Cannot provide alternative diagnosis
Pulmonary CTA
Advantages
More available, 24 hrs
Short exam time – better for unstable patient
Clearly identify clots
Can provide alternative diagnosis
Disadvantages
Higher radiation*
Possible contrast allergy
Possible nephrotoxic
CTPA: Males = 9.7 mSv, Females = 8.4 mSv [Woo Jk 2012] Q scan (4 mCi) = 1.5 mSv [SNM]
By Jiraporn Sriprapaporn

Can evaluate perfusion defects from PE and
Can diagnose DVT (source of emboli) in the same
setting - by radionuclide venography (RNV) (RNV must be initially requested)
Unique advantage of Q lung scan
By Jiraporn Sriprapaporn

Ventilation, Perfusion, and Radiographic Interpretive Criteria for PE
(SNM guideline v4, 2012)
PIOPED Modified PIOPED II
High LR [> 80% risk]
- >2 large mismatched (V:Q)
segmental defects*
High LR [85-90% risk]
- > 2 large mismatched (V:Q) segmental defects*
Borderline high LR
- 2 large mismatched (V:Q)
segmental defects*
Intermediate LR [20-80% risk]
- 2 moderate or 1 large mismatched
(V:Q) defect*
- Difficult to categorize as high or low
Nondiagnostic [20-80% risk]
- All other findings
Borderline low LR
- 1 matched (V:Q) defect, CXR-negative
Low LR [< 20% risk]
- Nonsegmental perfusion defects†
- Q defect substantially < CXR defect
- Matched (V:Q) defects, CXR-negative
- Any number of small Q defects*
Very low LR [< 10 % risk]
- Nonsegmental†
- Q defect < CXR lesion
- 1–3 small segmental*defects
- Solitary matched (V:Q:CXR) defect (#1 segment) in mid
or upper lung
- Stripe sign‡
- Solitary large pleural effusion§
- > 2 matched (V:Q) defects, regionally normal CXR
Normal
- No Q defects
Normal
- No Q defects
*Or equivalent where large segmental defect, >75% of segment, equals 1 segmental equivalent; moderate defect, 25%–75% of segment, equals 0.5 segmental equivalent; small defect, < 25%, is not counted.
By Jiraporn Sriprapaporn

Modified PIOPED II criteria reported as probability
or likelihood ratio for presence of PE
High prob. : PPV > 85%, ≥ 2 large V/Q mismatched segmental perfusion defects
Non-diagnostic
Very low prob. : PPV < 10%
Normal : Significant PE is excluded.
Interpretation of V/Q Lung Scan: Modified PIOPED II criteria
By Jiraporn Sriprapaporn

V/Q Lung Scan Classification
High Prob
Nondiagnostic
Very low prob
Normal
By Jiraporn Sriprapaporn

Pulmonary Embolism: Before & After Anticoagulant Rx
By Jiraporn Sriprapaporn

Ascending Radionuclide Venography (RNV): Techniques
Radiopharm: Tc-99m phytate/ sulfur colloid, Tc-99m MAA* (+ Q lung scan)
Inject a tracer via (bilateral) foot veins
On tourniquets above ankles to visualize deep veins and off tourniquets for superficial veins
By Jiraporn Sriprapaporn
Ascending RNV: Interpretation
Bilateral comparison, on & off TQ
Normal: Good flow without signs of venous occlusion
Abnormal: Obliteration of flow, filling defect, asymmetric flow +/-collaterals
By Jiraporn Sriprapaporn

Normal Asc RNV
Whole-body Images
phytate
Multiple Static Images
By Jiraporn Sriprapaporn

Normal vs Abnormal RNV
By Jiraporn Sriprapaporn
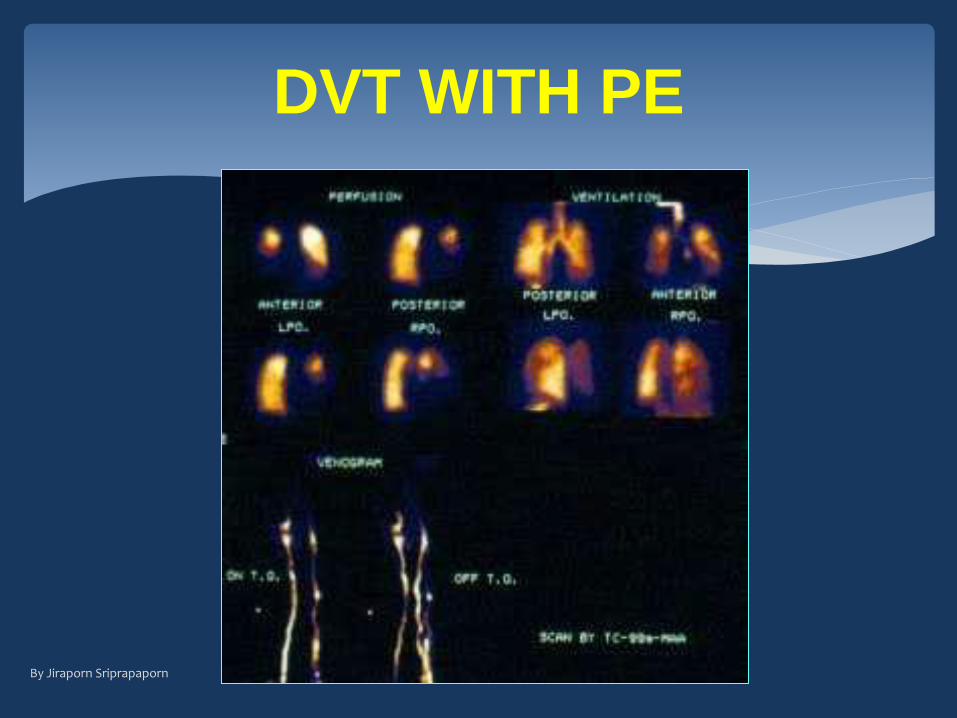
DVT WITH PE
By Jiraporn Sriprapaporn

Accuracy of Asc RNV
Authors Year No. (studies)
Sen (%)
Spec (%)
Corr (%)
Site of DVT
Webber (12) 1974 30 65 92 77 Overall Henkin (13) 1974 25 100 86 96 Proximal Van Kirk (14) 1976 19 100 95 95 Overall Vlahos (15) 1976 52 100 100 100 Pelvis 98 89 100 97 Thigh 98 92 97 95 Calf Ennis (16) 1977 154 90 89 95 Overall
Cordoba (17) 1977 44 100 80 94 Overall Ryo (18) 1977 47 89 66 89 Overall Gomes (19) 1982 51 88 65 67 Overall Mohamadiyeh(20) 1993 32 90 73 89 Proximal
Mangkharak 1998 72 88 96 90 Overall 55 95 97 96 Pelvic 72 95 100 90 Thigh 72 77 96 83 Calf
Mangkharak J, et al. J Med Assoc Thai 1998;81:432-441

Acute Pulmonary Embolism
Perfusion-Ventilation lung scan ***
Multiple segmental V/Q mismatched defects , no
radiographic abnormality
Increasing no. of defects increasing specificity
Pulmonary angiography is the original gold
standard, now usually being replaced with CTPA.
V/Q scan cannot DDx acute from chronic PE, so
F/U scan to evaluate the lung status post Rx *** (Baseline for the new episode, if any)
By Jiraporn Sriprapaporn

V/Q Lung Scan for Dx PE
Advantages
• Simple, noninvasive, safe, and economical
• High specificity (98%) esp. increasing no. of defects
• The usefulness is well documented.
• Can evaluate the cause -DVT in the same setting.
Disadvantages
Not widely available
Minimal radiation
Low sensitivity (41%)
Limitation in abn CXR
V/Q scan cannot DDx acute from chronic PE need F/U
scan
By Jiraporn Sriprapaporn
Management Guideline
Normal Rule out clinically significant PE
Very-low probability Find out other causes of symptoms.
Nondiagnostic Cannot rule out PE and needs further investigations such as ultrasound for DVT.
High prob The patient can be treated for PE.
By Jiraporn Sriprapaporn

High clinical probability Pulmonary CTA followed by
V/Q scan for baseline & F/U
Low clinical probability (normal CXR) V/Q lung scan
Presence of underlying lung disease CTA
Suggestion
Assessment of clinical probability of Pulmonary Embolism (Wells Score) • Symptoms of DVT (3 points) • No alternative diagnosis better explains the illness (3 points) • Tachycardia with pulse > 100 (1.5 points) • Immobilization (>= 3 days) or surgery in the previous 4 wks (1.5
points) • Prior history of DVT or pulmonary embolism (1.5 points) • Presence of hemoptysis (1 point) • Presence of malignancy (1 point)
Score < 2 = Low prob Score 2-6 = Mod. prob Score > 6 = High prob
By Jiraporn Sriprapaporn