venography - karary.edu.sd
TRANSCRIPT

Venography
Dr. Ahmed Alsharef FarahDr. Ahmed Alsharef Farah 1

• Injection into a central venous structure maynot opacify the peripheral veins that anastomoseto it.
• Place the patient in the supine position for eithera single-plane AP or PA projection or biplaneprojections.
Central Venography
Dr. Ahmed Alsharef Farah 2

• Move the patient‘s arms out of the field of view.• Collimation to the long axis of the vena cava
improves image quality but may preventvisualization of peripheral or collateral veins.
Dr. Ahmed Alsharef Farah 3

• Venography of the superior vena cava isperformed primarily to rule out the existence ofthrombus or the occlusion of the superior venacava.
Superior Venacavogram:
Dr. Ahmed Alsharef Farah 4

• The contrast medium may be injected througha needle or an angiographic catheterintroduced into a vein in an antecubital fossa.
• Radiographs should include the opacifiedsubclavian vein, brachiocephalic vein, thesuperior vena cava, and the right atrium.
Dr. Ahmed Alsharef Farah 5

• A representative program for a catheter injectionis 10 to 15 ml/sec for a 30 to 50 ml total volumeof contrast medium.
• Images are produced in both planes, if desired,at a rate of one or two images per second for 5to 10 seconds and are made at the end ofsuspended inspiration.
Dr. Ahmed Alsharef Farah 6

• Venography of the inferior vena cava isperformed primarily to rule out the existence ofthrombus or the occlusion of the inferior venacava.
Inferior Venacavogram:
Dr. Ahmed Alsharef Farah 7

• The contrast medium is injected through amultiple side hole catheter inserted through thefemoral vein and positioned in the commoniliac vein or the inferior aspect of the inferiorvena cava.
• Radiographs may need to include the opacifiedvasculature from the catheter tip to the rightatrium.
Dr. Ahmed Alsharef Farah 8

• Representative injection and imaging programsare 20 ml/sec for a 40 ml total volume ofcontrast medium and two images per second for4 to 8 seconds in both planes.
• Imaging begins at the end of suspendedexpiration.
Dr. Ahmed Alsharef Farah 9

Dr. Ahmed Alsharef Farah 10

Dr. Ahmed Alsharef Farah 11

• The visceral veins are often visualized byextending the imaging program of thecorresponding visceral artery injection.
Selective Visceral Venography
Dr. Ahmed Alsharef Farah 12

• Portal Venography, can be performed byinjecting the portal vein directly from aPercutaneous approach, but it is usuallyaccomplished by late-phase imaging of asplenic artery injection or an SMA injection.
Dr. Ahmed Alsharef Farah 13
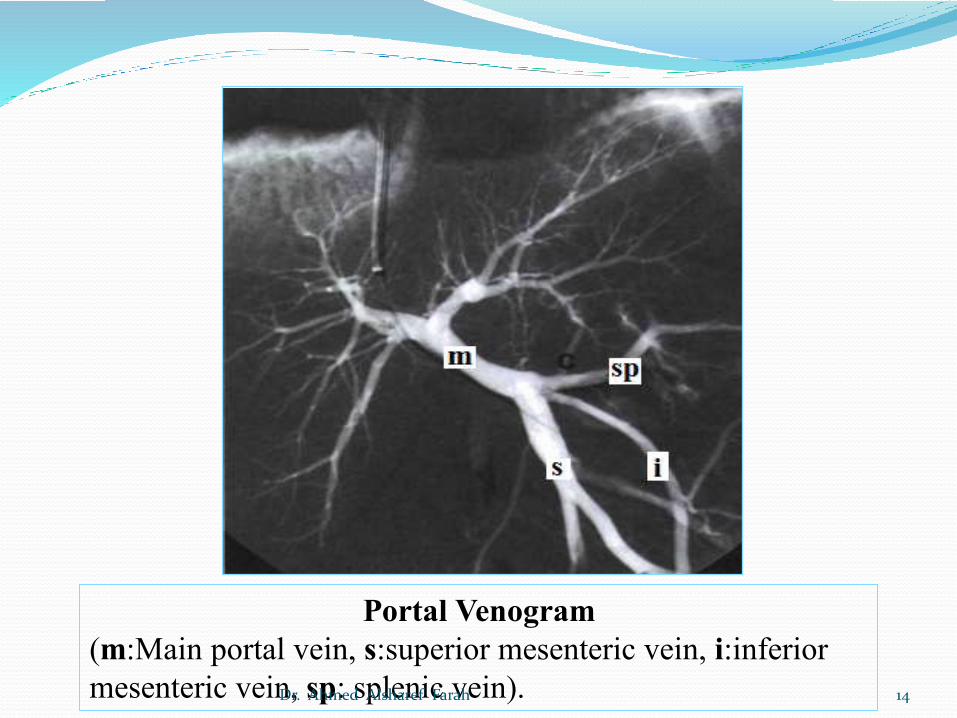
Portal Venogram(m:Main portal vein, s:superior mesenteric vein, i:inferior mesenteric vein, sp: splenic vein).Dr. Ahmed Alsharef Farah 14

• Hepatic Venography is usually performed torule out stenosis or thrombosis of the hepaticveins.
• The hepatic veins are most easily catheterizedfrom a jugular vein or an upper limb veinapproach, but a femoral vein approach mayalso be used.
Hepatic Venogram:
Dr. Ahmed Alsharef Farah 15

• Place the patient in the supine position for APor PA projections that include the liver tissueand the extreme upper inferior vena cava.
• Make the exposures.Representative injection and imaging programsare 10 ml/sec for a 30 ml total volume ofcontrast medium and one image per second for8 seconds.Make exposures at the end of suspendedexpiration.
Dr. Ahmed Alsharef Farah 16

• Renal Venography is usually performed to ruleout thrombosis of the renal vein.
• The renal vein is most easily catheterized froma femoral vein approach.
Renal Venogram:
Dr. Ahmed Alsharef Farah 17

• Place the patient in the supine position for asingle-plane AP or PA projection.
• Center the selected kidney to the imagereceptor, and collimate the field to include thekidney and area of the inferior vena cava.
Dr. Ahmed Alsharef Farah 18

• Make the exposures.Representative injection and imaging programsare 8 ml/sec for a 16 ml total volume of contrastmedium and two images per second for 4seconds.Make exposures at the end of suspendedexpiration.
Dr. Ahmed Alsharef Farah 19

A. Hepatic vein visualization from reflux from an inferiorvena cava injection.
B. Selective left renal venogram. AP projection.Dr. Ahmed Alsharef Farah 20

Peripheral Angiography
Dr. Ahmed Alsharef Farah 21
• Upper limb Arteriography is most oftenperformed to evaluate traumatic injury,atherosclerotic disease or other vascularlesions.
Upper Limb Arteriograms:
Dr. Ahmed Alsharef Farah 22

• The arteriograms are usually obtained by usingthe Seldinger technique to introduce a catheterusually at a femoral artery site for selectiveinjection into the subclavian or axillary artery.
• The area to be radiographed may therefore bejust a hand or other selected part of the arm, orit may include the entire upper limb and thorax.
Dr. Ahmed Alsharef Farah 23
• The recommended projection is a true APprojection with the arm extended and the handsupinated.
• The injection varies from 3 or 4 ml/sec througha catheter positioned distally to 10 ml/secthrough a proximally positioned catheter.
• A representative program for a rapid imagingsystem may be two films per second for 5seconds followed by one per second for 5seconds.
Dr. Ahmed Alsharef Farah 24

Right hand arteriogram (2:1 magnification)showing severe arterio-occlusive disease (arrows).Dr. Ahmed Alsharef Farah 25

• Upper limb Venography is most oftenperformed to look for thrombosis.
• The contrast medium is injected through aneedle or catheter into a superficial vein at theelbow or wrist.
Upper Limb Venograms:
Dr. Ahmed Alsharef Farah 26

• The radiographs should cover the vasculaturefrom the wrist or elbow to the superior venacava.
• Injections may be made by hand, or anautomatic injector may be set to deliver a totalof 40 to 80 ml at a rate of 1 to 4 ml/sec,depending on whether a needle or catheter isused.
Dr. Ahmed Alsharef Farah 27

Normal right upper limb Venogram.
Dr. Ahmed Alsharef Farah 28

• Aortofemoral Arteriography is usuallyperformed to determine if atheroscleroticdisease is the cause of claudication.
Aortofemoral arteriograms:
Dr. Ahmed Alsharef Farah 29

• A catheter is usually introduced into a femoralartery using the Seldinger technique.
• The catheter tip is positioned superior to theaortic bifurcation so that bilateralarteriograms are obtained simultaneously.
Dr. Ahmed Alsharef Farah 30

• When only one leg is to be examined, thecatheter tip is placed below the bifurcation, orthe contrast medium is injected through a needleplaced in the femoral artery.
• A representative injection program designed tocreate a long bolus of contrast medium is 10ml/sec for an 100 ml total volume.
Dr. Ahmed Alsharef Farah 31

• Lower limb Venography is common and isusually performed to rule out thrombosis of thedeep veins of the leg.
Lower Limb Venograms:
Dr. Ahmed Alsharef Farah 32

• Venograms are usually obtained with contrastmedium injected through a needle placeddirectly into a superficial vein in the foot.
• Begin imaging at the patient's ankle, andproceed superiorly to include the inferior venacava as the injection continues.
Dr. Ahmed Alsharef Farah 33

• Without fluoroscopy, usually obtain APprojections with the leg internally rotated 30degrees to include the entire area of interest.
• Perform lateral projections if needed.• Injections may be made by hand, or an
automatic injector may be set to deliver 1 or 2ml/sec for a total of 50 to 100 ml.
Dr. Ahmed Alsharef Farah 34

Dr. Ahmed Alsharef Farah 35

The END
Dr. Ahmed Alsharef Farah 36