level 3 investment proposal template revenue funding … · 2017-05-17 · approval of investment...
TRANSCRIPT
1 | P a g e
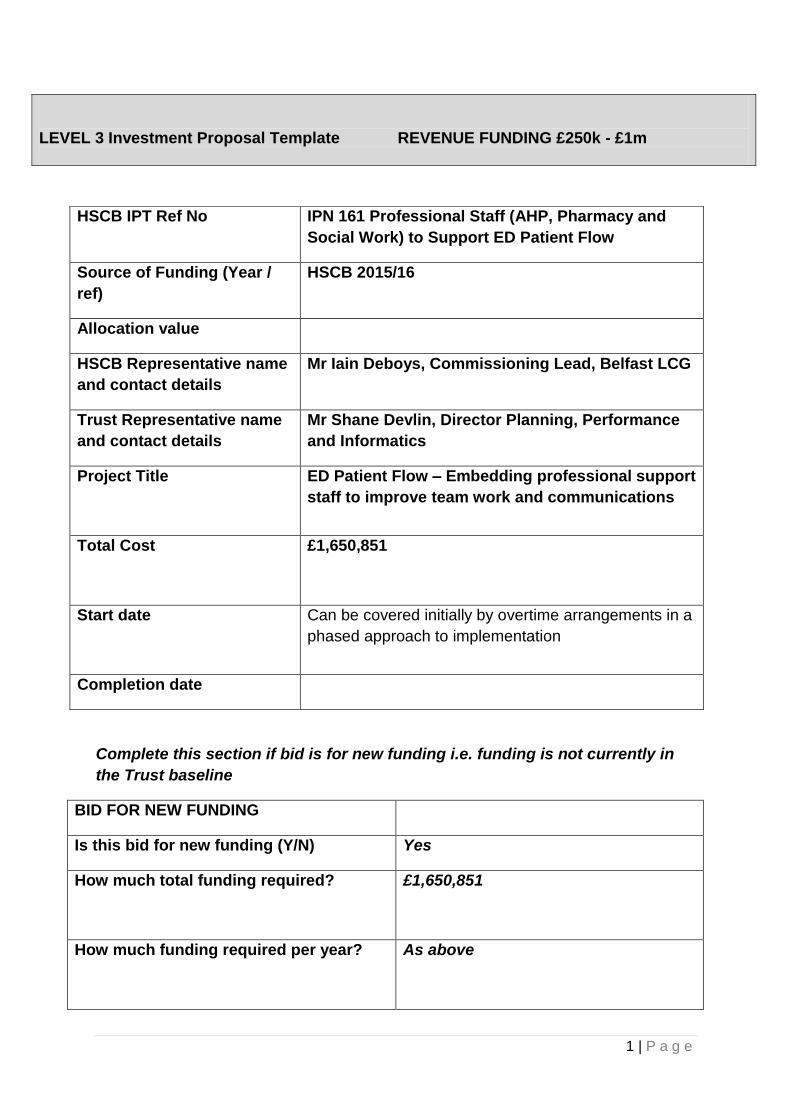
LEVEL 3 Investment Proposal Template REVENUE FUNDING £250k - £1m
Complete this section if bid is for new funding i.e. funding is not currently in
the Trust baseline
BID FOR NEW FUNDING
Is this bid for new funding (Y/N) Yes
How much total funding required?
£1,650,851
How much funding required per year?
As above
HSCB IPT Ref No IPN 161 Professional Staff (AHP, Pharmacy and
Social Work) to Support ED Patient Flow
Source of Funding (Year /
ref)
HSCB 2015/16
Allocation value
HSCB Representative name
and contact details
Mr Iain Deboys, Commissioning Lead, Belfast LCG
Trust Representative name
and contact details
Mr Shane Devlin, Director Planning, Performance
and Informatics
Project Title
ED Patient Flow – Embedding professional support
staff to improve team work and communications
Total Cost
£1,650,851
Start date
Can be covered initially by overtime arrangements in a
phased approach to implementation
Completion date
2 | P a g e
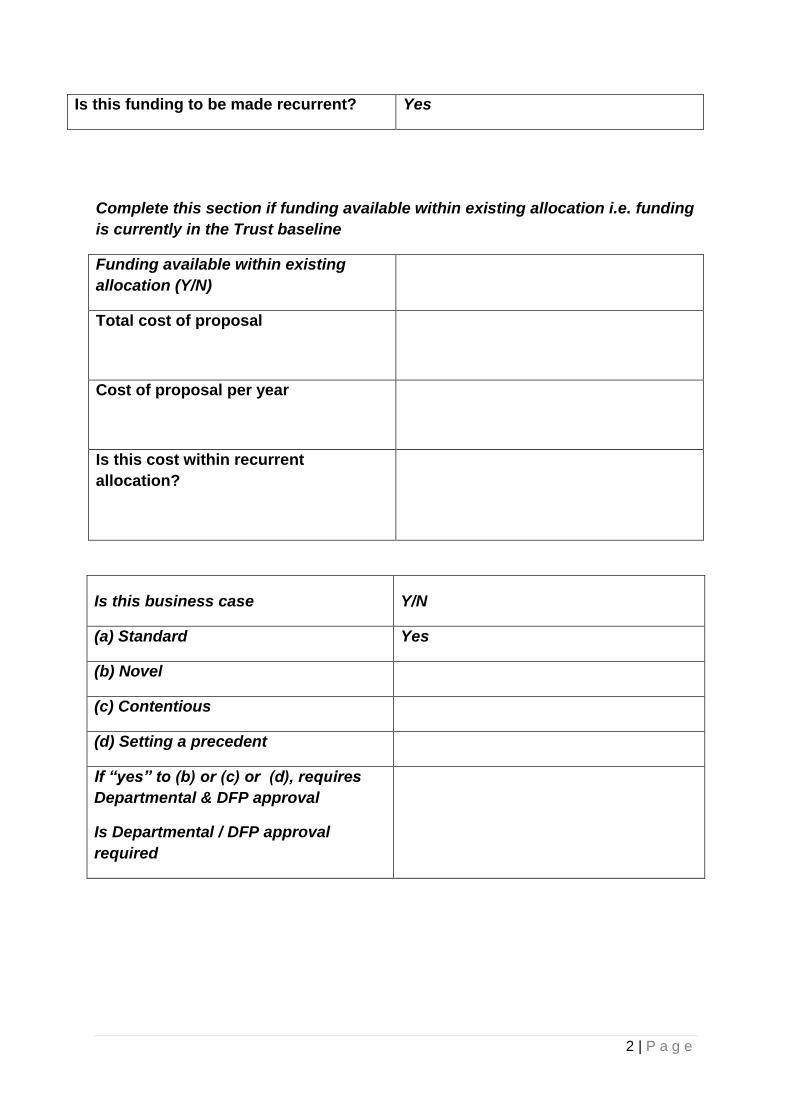
Is this funding to be made recurrent? Yes
Complete this section if funding available within existing allocation i.e. funding
is currently in the Trust baseline
Funding available within existing
allocation (Y/N)
Total cost of proposal
Cost of proposal per year
Is this cost within recurrent
allocation?
Is this business case Y/N
(a) Standard Yes
(b) Novel
(c) Contentious
(d) Setting a precedent
If “yes” to (b) or (c) or (d), requires
Departmental & DFP approval
Is Departmental / DFP approval
required
3 | P a g e
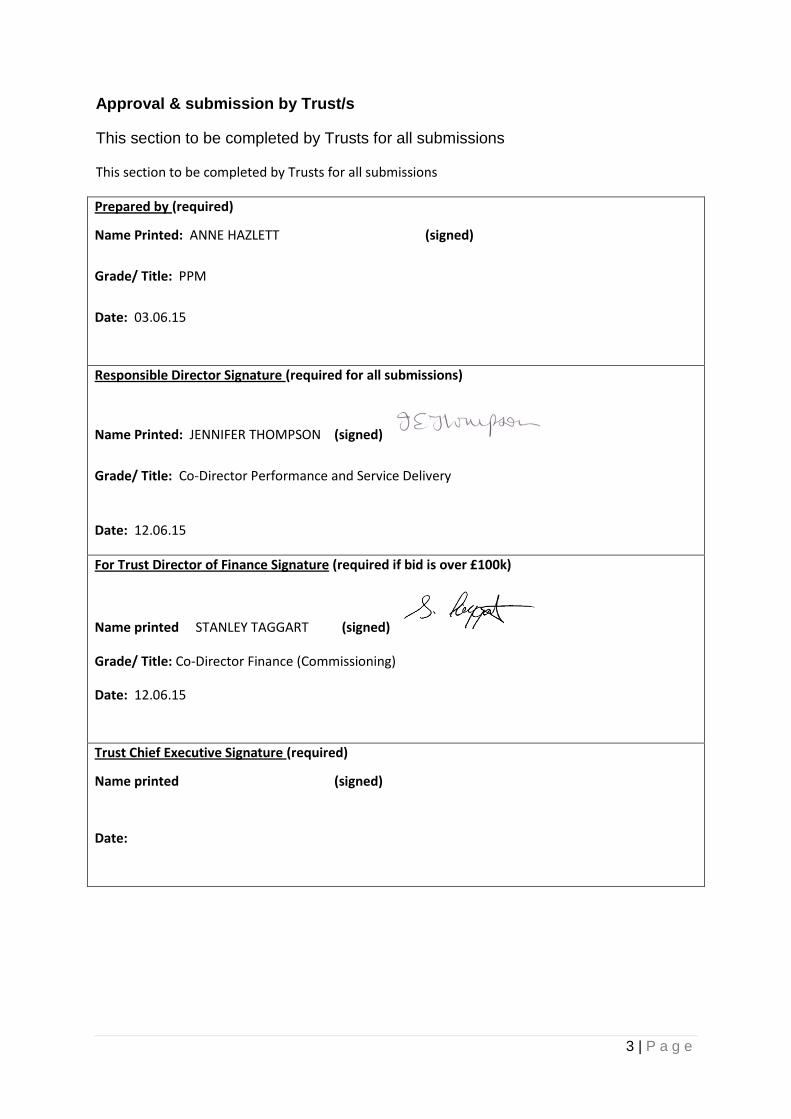
Approval & submission by Trust/s
This section to be completed by Trusts for all submissions
This section to be completed by Trusts for all submissions
Prepared by (required)
Name Printed: ANNE HAZLETT (signed)
Grade/ Title: PPM
Date: 03.06.15
Responsible Director Signature (required for all submissions)
Name Printed: JENNIFER THOMPSON (signed)
Grade/ Title: Co-Director Performance and Service Delivery
Date: 12.06.15
For Trust Director of Finance Signature (required if bid is over £100k)
Name printed STANLEY TAGGART (signed)
Grade/ Title: Co-Director Finance (Commissioning)
Date: 12.06.15
Trust Chief Executive Signature (required)
Name printed (signed)
Date:
4 | P a g e
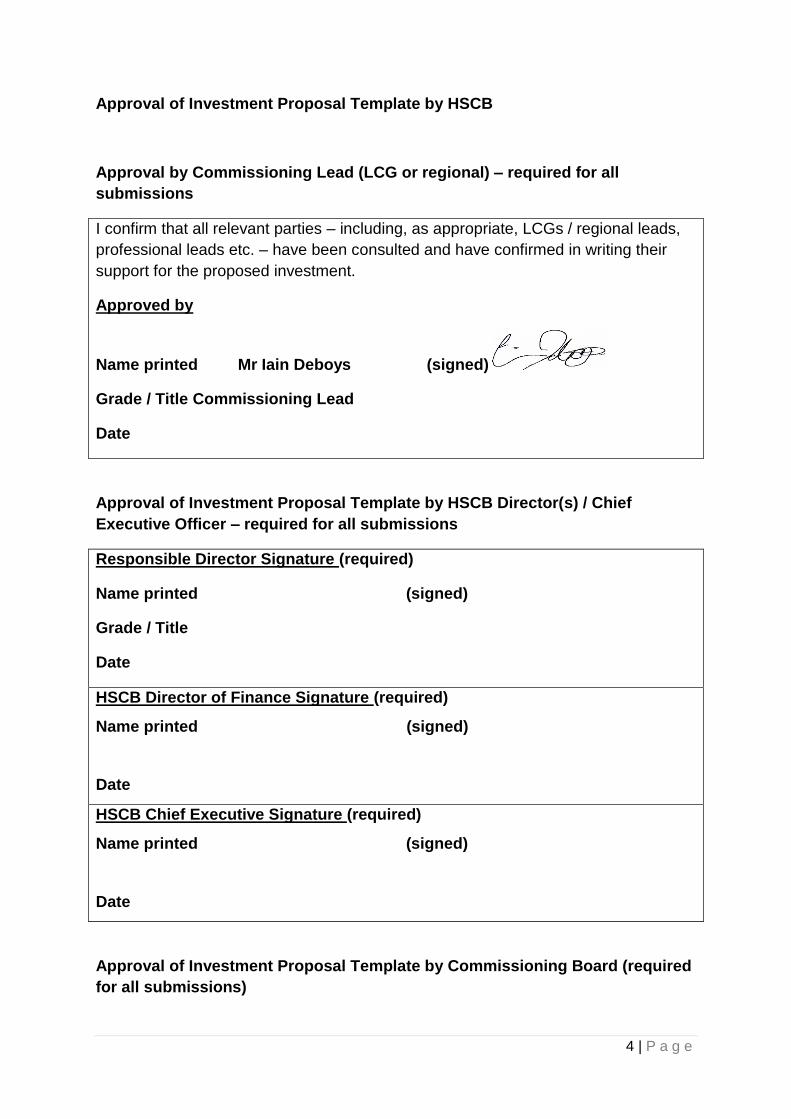
Approval of Investment Proposal Template by HSCB
Approval by Commissioning Lead (LCG or regional) – required for all
submissions
I confirm that all relevant parties – including, as appropriate, LCGs / regional leads,
professional leads etc. – have been consulted and have confirmed in writing their
support for the proposed investment.
Approved by
Name printed Mr Iain Deboys (signed)
Grade / Title Commissioning Lead
Date
Approval of Investment Proposal Template by HSCB Director(s) / Chief
Executive Officer – required for all submissions
Responsible Director Signature (required)
Name printed (signed)
Grade / Title
Date
HSCB Director of Finance Signature (required)
Name printed (signed)
Date
HSCB Chief Executive Signature (required)
Name printed (signed)
Date
Approval of Investment Proposal Template by Commissioning Board (required
for all submissions)
5 | P a g e
Date approved by Commissioning Board
Date
Complete this section if Department / DFP approval required
Date submitted to Department
Department/ DFP approval (y/n)
Date approved

6 | P a g e
SECTION 1(a): Commissioner Specification to include strategic context and need (to be
completed by the Commissioner).
In July 2014 the Health Minister announced to the Assembly his intention to establish a Regional Task Group to take forward the RQIA’s recommendations in relation to Unscheduled Care. The Task Group was placed under the leadership of the Chief Medical Officer, Dr Michael McBride, and the Chief Nursing Officer, Charlotte McArdle. The Task Group established 7 work streams to mirror the principal thematic findings of the RQIA. One of the work stream groups was tasked with Improving Patient Flow. Through this IPT Belfast Trust is asked to bring forward proposals to improve patient flow and thereby reduce the length of time patients wait in the RVH Emergency Department following a decision to admit, including the number that wait for more than 12 hours. The Task Group’s recommendations are wide ranging therefore to initiate implementation from this work the HSCB SMT agreed five key priority tasks to be progressed in the immediate term. These priorities are: 1) To ensure radiology services are available 7 days a week that enable same day/next morning
investigation and reporting (to include CT, MRI & Non Obstetric Ultrasound Scans). This applies to all radiological work including GP, ED and inpatient referrals.
2) To ensure there is twice daily senior decision making for inpatients 3) To establish a dedicated minor injury stream in main Emergency Departments (9am-9pm, 7/7)
4) To embed Physiotherapy, Occupational Therapy, Pharmacy and Social Work support within
main ED’s and Short Stay Wards (9-5, 7/7)
5) To organise ward rounds to ensure clinical priority patients are seen first followed by potential discharges to facilitate early discharge.
SECTION 1(b): DEMONSTRATE THE NEED FOR THE PROJECT
Part of the approach to embedding multidisciplinary staff in the main ED, including the Short Stay Observation Unit, is to ensure Social Work, Pharmacy, Physiotherapy and Occupational Therapy work as part of the ED team i.e. are embedded and dedicated to ED to enable good team relationships, communication and working. These professions are recommended to be available in the main ED 9am-5pm 7-days a week. The Commissioner invites proposals from Belfast Trust to secure the presence of these professions in such a way that maximise their potential.

7 | P a g e
Deployment should also maximise opportunities for good team relationships, communication and working. It is not expected that the proposals would meet the full potential demand for each profession but that the beginning of 7 day consistency is achieved. WTE requirements should be based on the agreed assumption that 430 sessions equates to 1 WTE Mon to Friday, 520 sessions are required for a full year and that annualised weekends require a further 208 sessions of cover. Social Work There are currently 19 WTE across the RVH acute, USC and ED service. These are mainly Band 6 posts. There are 3 teams each led by one Band 7( 2.5 WTE), reporting to Assistant Service Manager/Professional Lead, through to Service Manager Integrated Care Teams . The present service relies on a pool of experienced staff being willing to work additional hours at weekends. The Commissioner invites proposals that build a sustainable rota, relying less on bank staff. The preference is for additional 3 WTE Band 7 positions. This will support senior practitioner decision making and autonomous working. Some bank input will continue to be required but at a reduced level. Proposals should ensure that 2 staff are on duty at weekends and more hours provided (via a third session) on Thursdays, Fridays and Mondays. This will ensure a more consistent level of input to the service with full day cover at weekends instead of mornings only. The improved cover should provide rapid access social care discharge planning for older people in unscheduled care admissions and presentations to ED. Pharmacy Current baseline week day cover is provided to Short Stay by 0.5 WTE Band 8a. There is also an element of non-recurrent ATO support to undertake daily top-up service to ED writing orders and stock control. The NI clinical pharmacy standards indicate a ratio of one pharmacist and one technician post per 100,000 attendances. RVH attendances are in the region of 84000. On this basis it is recommended to plan for one post of each type. This translates into the following WTE when taking 7 day working into account:
1.1 WTE Pharmacist to add to the existing 0.5 WTE
Band 5 Technical 1.6 WTE
Band 2 – make current 0.5 WTE recurrent Allied Health Professions
8 | P a g e
The current baseline line equates to 1.0 WTE OT embedded in ED / 5 days a week / 43 weeks per year. A second Band 6 OT is in service but unfunded (similar schedule to above). No Physiotherapy staff are in place. The Commissioner will consider a range of options from one member of each profession 7 days a week / 52 weeks per year to 2.0 WTE from each profession for the same duration. Other options based on this theme can be included. Proposals should also incorporate a mix of Band 6 and 7 positions to provide for autonomous working and a flexible skill-mix across the service.

9 | P a g e
SECTION 2(a): OBJECTIVES
Project Objectives Measurable Targets
1. To provide rapid access to social care discharge
planning, pharmacy and allied health professional
assessment, 8 hours per day, 7 days per week, 52
weeks per annum to the RVH Emergency
Department
1.1 No of referrals made per day and
turnaround times to aid flow
2. To ensure that the investment in social work,
pharmacy and allied health professionals leads to
an improvement in the flow of patients
2.1 No of referrals made per day and
turnaround times,
2.2 Measurement of patients referred to social
work and AHP services where the patients
were not admitted
3. To provide rapid access to social care discharge
planning, pharmacy and allied health professional
assessment, 8 hours per day, 7 days per week, 52
weeks per annum to the RVH Emergency
Department and AMU
3.1 No of referrals made per day and
turnaround times to aid flow
SECTION 2(b): CONSTRAINTS
Constraints Measures to address constraints
Recruitment of staff to populate permanent
weekend rotas in all three professional areas
This will have to be addressed in the
recruitment process
SECTION 3: IDENTIFY AND SHORTLIST OPTIONS
Option Number/ Description
1.0 Option one
Status Quo - continue with a 5 day service
The service would continue to be delivered as per recurrent funding arrangements. This option
would have no impact on improving patient flow or developing a 7 day service.
10 | P a g e
2.0 Option two – Provide Professional Staff support to the RVH Emergency Department 8
hours per day, 7 days per week, 52 weeks per annum
This option proposes that there should be Social work, Pharmacy and Allied Health Professional
presence (Physiotherapy and Occupational Therapy) in the RVH Emergency department 8 hours per
day, 7 days per week, 52 weeks per annum. This would assist in the flow of patients through the
Department and prevent admission of patients who would have been previously admitted for social
work and AHP assessment. Each of the proposals within these 3 areas are detailed below:
2.1 Social work
In AMU and ED there is a need for a mainstream constant, consistent and coordinated Social work
service across all seven days. The Emergency department and the short stay unit are the areas of
highest demand Monday to Friday and at weekends this shifts to AMU. This is in relation especially
for Older people admitted from ED for short medical admissions and is vital to ensure the timely flow
of discharges to support the capacity of AMU to admit patients. Staff should be embedded in AMU
and attached as ED liaison as a whole system to managing demand.
It is proposed that the service recruits an additional 3 wte social workers would be rostered across
seven day cover inclusive of the Emergency department, short stay and AMU to provide rapid
access social care discharge planning. These posts would be Band 7 as this is in line with the level
of autonomous experienced decision making required to undertake safe and effective weekend
discharges.
The 3 WTE would provide a total of 27 sessions per week to AMU and ED across seven days (8 to
12 sessions every weekend)
2.2 Pharmacy
The RVH ED pharmacy service currently has 0.5 Band 8a who provides support to the short stay
ward in the Emergency Department. There is also an element of non recurrent ATO support at the
moment who undertakes daily top up service, writing orders and stock control. The table below
identifies and highlights the role of staff required to carry out a 7 day dedicated service to the RVH
ED. This resource would provide 2 pharmacists and 1 technician in ED each day with one
pharmacist based in ED and the other in short stay.
Roles which pharmacy staff identified in the bid for RVH ED will carry out
Band 8a Pharmacist – Required 0.5, This post would provide a full time 1.0WTE strategic and
operational pharmacy lead and undertake the clinical duties below.
Band 7 Pharmacist – Required 2.36. These posts would provide medicines reconciliation on
attendance, prescribing advice to medical staff, support nursing staff treating patients using patient
group directions and act as non-medical prescribers for specific patient groups
Band 5 Technician – Required 1.68. These posts would provide a dispensing service in ED, supply

11 | P a g e
urgently required medicines, assess patients own medicines for on-going use supporting admission
and ensure medicines move with the patient
Band 2 Pharmacy support – Required 0.5. This post would maintain the stock of medicines on a
daily basis in ED ordering, collecting and putting away.
Table one
The table below summarises the resource required for pharmacy to support 7 day working,
52 weeks per annum, 8 hours per day.
RVH Emergency
Department
Pharmacist 8a 0.5 wte
Pharmacist band 7 2.36 wte
Technician band 5 1.68 wte
Pharmacy support band 2 0.5 wte
2.3 Allied Health Professionals
There is currently one full time Occupational Therapist dedicated to the RVH Emergency Department
with all other staff providing service on a non recurrent/overtime basis. At the moment a 2 day
session Monday to Friday is provided (43 weeks per annum) by 2 WTE physios and 2 WTE OTs.
Referral levels are approximately 120 new patients per month to each of the 2 Professions. The
range of new patients per day is 7 to 8 on average with a maximum capacity of 9 new patients per
day seen per profession.
The patient categories presenting include:
Occupational Therapy – patients requiring mobility/functional assessments (generally undertaken in
conjunction with Physio) and Upper limb soft tissue injuries
Physiotherapy – patients requiring mobility assessments (as above) and MSK/Minor injuries (soft
tissue and factures)
The minor injuries work encompasses some fracture work which allows patients to be treated and
discharged rather than be sent for medical management via the facture clinic services. For this
group of patients the professions also offer a limited review service where clinically appropriate (150
slots per annum).
Treatment time ranges from one to two hours across the spectrum of patients presenting. The
higher end of the treatment pathway relates to complex functional/mobility/social assessments as
these are undertaken by the 2 AHP professions alongside Social work staff. Response time for the
service is typically 0 to 2 hours. An analysis of the previous years activity would demonstrate that
12 | P a g e
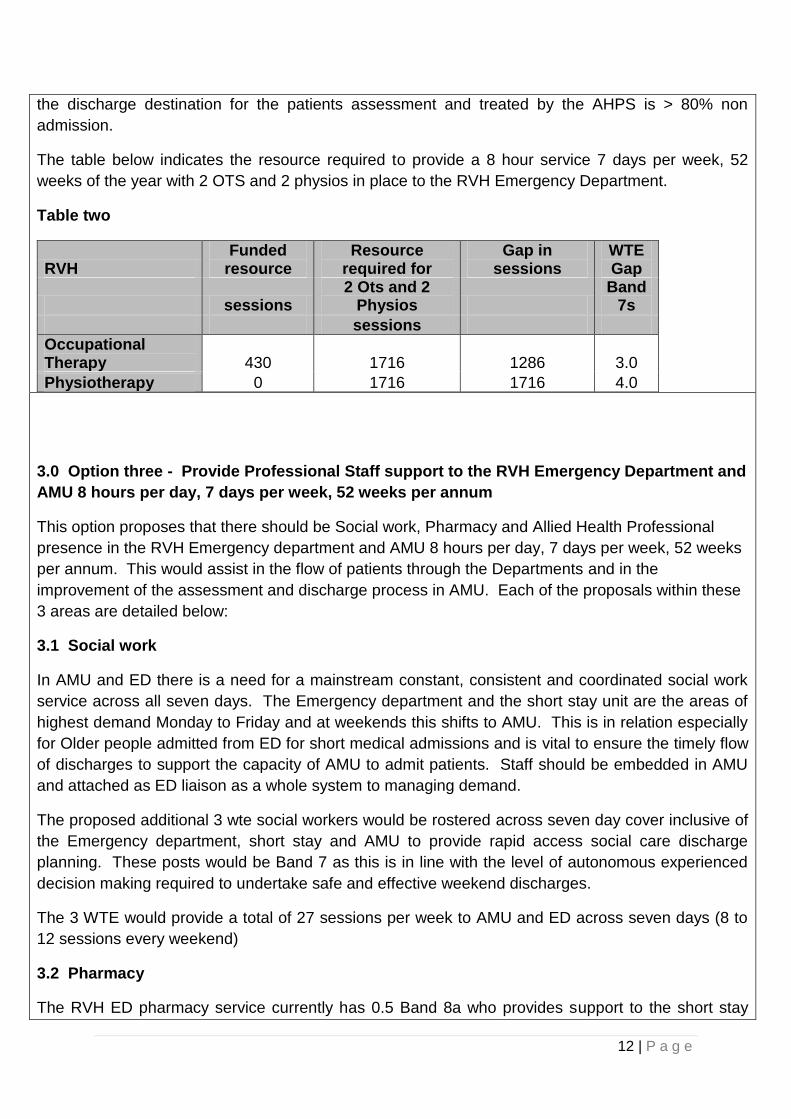
the discharge destination for the patients assessment and treated by the AHPS is > 80% non
admission.
The table below indicates the resource required to provide a 8 hour service 7 days per week, 52
weeks of the year with 2 OTS and 2 physios in place to the RVH Emergency Department.
Table two
RVH Funded
resource Resource
required for Gap in
sessions WTE Gap
sessions 2 Ots and 2
Physios Band
7s
sessions
Occupational Therapy 430 1716 1286 3.0
Physiotherapy 0 1716 1716 4.0
3.0 Option three - Provide Professional Staff support to the RVH Emergency Department and
AMU 8 hours per day, 7 days per week, 52 weeks per annum
This option proposes that there should be Social work, Pharmacy and Allied Health Professional
presence in the RVH Emergency department and AMU 8 hours per day, 7 days per week, 52 weeks
per annum. This would assist in the flow of patients through the Departments and in the
improvement of the assessment and discharge process in AMU. Each of the proposals within these
3 areas are detailed below:
3.1 Social work
In AMU and ED there is a need for a mainstream constant, consistent and coordinated social work
service across all seven days. The Emergency department and the short stay unit are the areas of
highest demand Monday to Friday and at weekends this shifts to AMU. This is in relation especially
for Older people admitted from ED for short medical admissions and is vital to ensure the timely flow
of discharges to support the capacity of AMU to admit patients. Staff should be embedded in AMU
and attached as ED liaison as a whole system to managing demand.
The proposed additional 3 wte social workers would be rostered across seven day cover inclusive of
the Emergency department, short stay and AMU to provide rapid access social care discharge
planning. These posts would be Band 7 as this is in line with the level of autonomous experienced
decision making required to undertake safe and effective weekend discharges.
The 3 WTE would provide a total of 27 sessions per week to AMU and ED across seven days (8 to
12 sessions every weekend)
3.2 Pharmacy
The RVH ED pharmacy service currently has 0.5 Band 8a who provides support to the short stay
13 | P a g e
ward. There is also an element of non recurrent ATO support who undertakes daily top up service,
writing orders and stock control. The table below identifies the staff required to carry out a 7 day
dedicated service to the RVH ED. This resource would provide 2 pharmacists and 1 technician in ED
each day with one pharmacist based in ED and the other in short stay
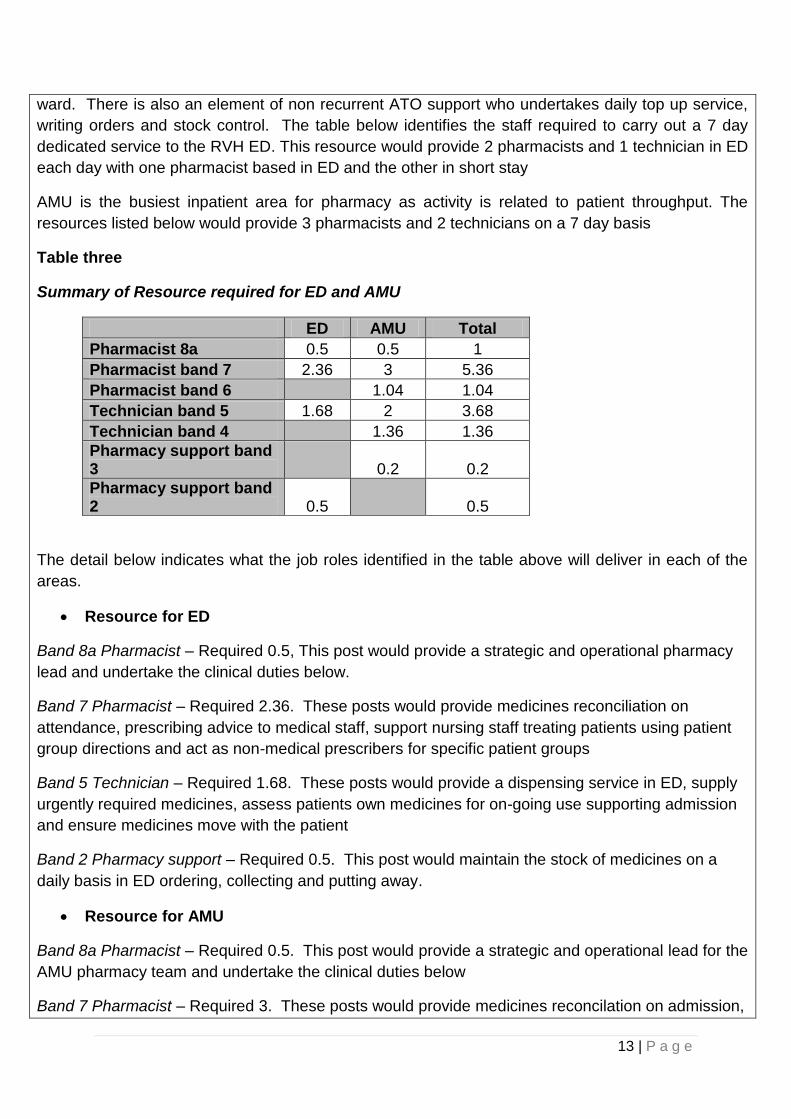
AMU is the busiest inpatient area for pharmacy as activity is related to patient throughput. The
resources listed below would provide 3 pharmacists and 2 technicians on a 7 day basis
Table three
Summary of Resource required for ED and AMU
ED AMU Total
Pharmacist 8a 0.5 0.5 1
Pharmacist band 7 2.36 3 5.36
Pharmacist band 6
1.04 1.04
Technician band 5 1.68 2 3.68
Technician band 4
1.36 1.36
Pharmacy support band 3
0.2 0.2
Pharmacy support band 2 0.5
0.5
The detail below indicates what the job roles identified in the table above will deliver in each of the
areas.
Resource for ED
Band 8a Pharmacist – Required 0.5, This post would provide a strategic and operational pharmacy
lead and undertake the clinical duties below.
Band 7 Pharmacist – Required 2.36. These posts would provide medicines reconciliation on
attendance, prescribing advice to medical staff, support nursing staff treating patients using patient
group directions and act as non-medical prescribers for specific patient groups
Band 5 Technician – Required 1.68. These posts would provide a dispensing service in ED, supply
urgently required medicines, assess patients own medicines for on-going use supporting admission
and ensure medicines move with the patient
Band 2 Pharmacy support – Required 0.5. This post would maintain the stock of medicines on a
daily basis in ED ordering, collecting and putting away.
Resource for AMU
Band 8a Pharmacist – Required 0.5. This post would provide a strategic and operational lead for the
AMU pharmacy team and undertake the clinical duties below
Band 7 Pharmacist – Required 3. These posts would provide medicines reconcilation on admission,
14 | P a g e
daily review to optimise treatment, prepare the prescription aspect of discharge letter, medicines
reconciliation on discharge, pre-empt issues regarding compliance aids, work with patient to reduce
risk of reattendance/admission, counsel patients on changes to medicines, support patients
transferring to other facilities
Band 6 Pharmacist – Required 1.04. These posts would undertake the above duties under the
direction of a senior pharmacist
Band 5 Technician – Required 2 – These posts would provide one-stop dispensing including the use
of patients own drugs, minimising waste. They would order newly prescribed medicines supporting
timely treatment. They will ensure medicines move with the patient reducing duplication and waste
Band 4 Technician – Required 1.36 – These posts would undertake the above duties under the
direction of a senior technician
Band 3 Pharmacy support – Required 0.2. This post would maintain the stock of medicines on a
weekly basis ordering, collecting and putting away.
3.3 Allied Health Professionals
RVH Emergency Department
There is currently one full time Occupational Therapist dedicated to the RVH Emergency Department
with all other staff providing service on a non recurrent/overtime basis. At the moment a 2 day
session Monday to Friday is provided (43 weeks per annum) by 2 WTE physios and 2 WTE OTs.
Referral levels are approximately 120 new patients per month to each of the 2 Professions. The
range of new patients per day is 7 to 8 on average with a maximum capacity of 9 new patients per
day seen per profession.
The patient categories presenting include:
Occupational Therapy – patients requiring mobility/functional assessments (generally undertaken in
conjunction with Physio) and Upper limb soft tissue injuries
Physiotherapy – patients requiring mobility assessments (as above) and MSK/Minor injuries (soft
tissue and factures)
The minor injuries work encompasses some fracture work which allows patients to be treated and
discharged rather than be sent for medical management via the facture clinic services. For this
group of patients the professions also offer a limited review service where clinically appropriate (150
slots per annum).
Treatment time ranges from one to two hours across the spectrum of patients presenting. The
higher end of the treatment pathway relates to complex functional/mobility/social assessments as
these are undertaken by the 2 AHP professions alongside Social work staff. Response time for the
service is typically 0 to 2 hours. An analysis of the previous years activity would demonstrate that

15 | P a g e
the discharge destination for the patients assessment and treated by the AHPS is > 80% non
admission.
The table below indicates the resource required to provide a 8 hour service 7 days per week, 52
weeks of the year with 2 OTS and 2 physios in place to the RVH Emergency Department.
AMU – RVH
There are currently 2 OTs and 3.8 Physios working within the AMU in RVH and all other staff
providing service on a non recurrent/overtime basis. At the moment a 2 day session Monday to
Friday is provided (43 weeks per annum).
The role of Occupational Therapy in AMU is to provide an on the day response to referrals with
Expected date of discharge so that an individual patient’s optimal functional and cognitive abilities
are assessed, appropriate interventions are completed to ensure patients gain maximum benefit
from their hospital stay and to ensure safe and timely discharge. This is delivered by assisting in the
discharge planning through participation at the “white board” meetings, by prioritising assessments
to ensure greatest benefits to patients identified as fit for discharge, and provide focussed acute
rehabilitation to enable patients (< 2 midnights) to regain their optimum level of independence so that
the most appropriate care arrangements are put in place on discharge.
Treatment time ranges from 2 ½ hours to 4 ½ hours across the spectrum of patients presenting. The
higher end of the treatment pathway relates to complex functional and cognitive assessments.
The role of the physiotherapy service in AMU will provide a rapid assessment, treatment, discharge and/ or transfer for acute medically patients admitted to the medical assessment unit within the RVH. The physiotherapy service will work as part of the multidisciplinary team to assist in early identification of appropriate patients engaging in ward white board meetings/patient flow meetings and contribute to the discharge or transfer planning for patients referred. Currently the weekend service is supported by staff working additional hours for Sat /Sun and will depend on availability of staff if there is one or two physiotherapy staff available on any given day. Current clinical prioritisation criteria for Physiotherapy weekend is as follows:
Respiratory condition requiring input to prevent deterioration outside of emergency protocol
Mobilisers to include falls, general debility, fractures
Reviews where input maintains progress towards discharge
Outside of these hours, emergency respiratory input will be provided through the out of hours
Physiotherapy service.
The table below shows the resource required to provide 8 hours per day, 7 days per week, 52 weeks
cover to the Royal Emergency department as in Option 2 and provide this cover to the Acute Medical
Unit for the same period.
16 | P a g e
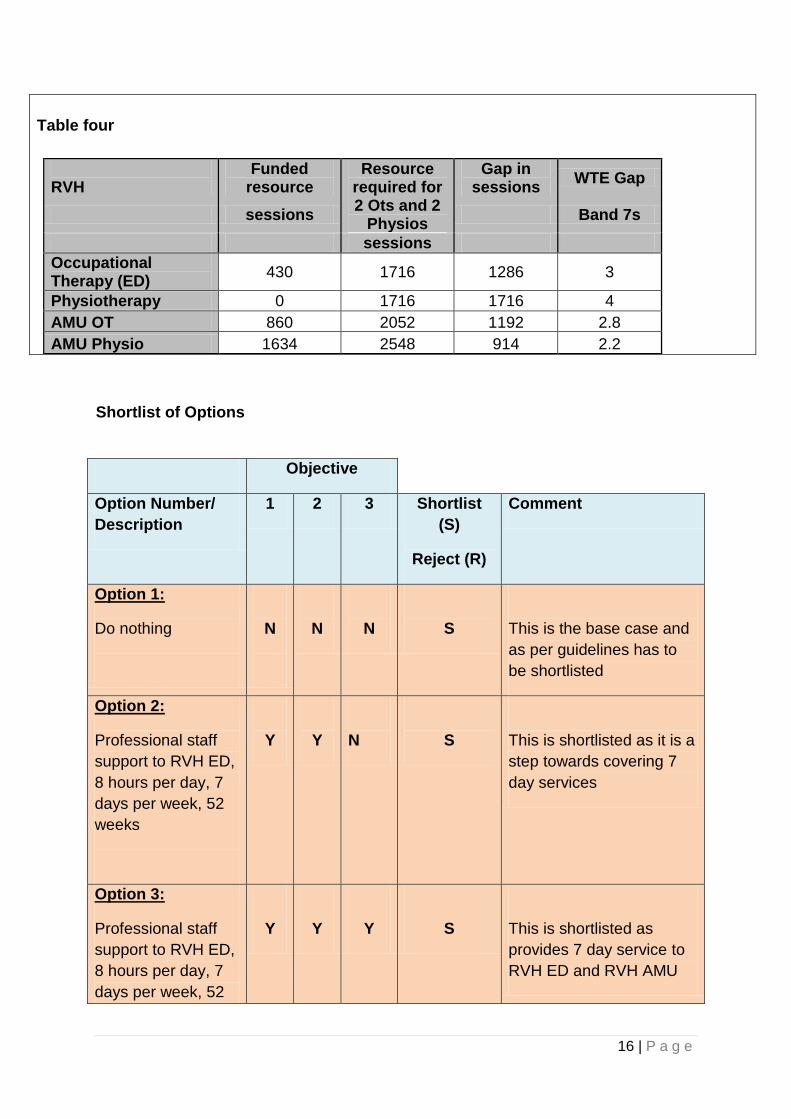
Table four
RVH
Funded resource
Resource required for
Gap in sessions
WTE Gap
sessions 2 Ots and 2
Physios Band 7s
sessions
Occupational Therapy (ED)
430 1716 1286 3
Physiotherapy 0 1716 1716 4
AMU OT 860 2052 1192 2.8
AMU Physio 1634 2548 914 2.2
Shortlist of Options
Objective
Option Number/
Description
1 2 3 Shortlist
(S)
Reject (R)
Comment
Option 1:
Do nothing
N
N
N
S
This is the base case and
as per guidelines has to
be shortlisted
Option 2:
Professional staff
support to RVH ED,
8 hours per day, 7
days per week, 52
weeks
Y
Y
N
S
This is shortlisted as it is a
step towards covering 7
day services
Option 3:
Professional staff
support to RVH ED,
8 hours per day, 7
days per week, 52
Y
Y
Y
S
This is shortlisted as
provides 7 day service to
RVH ED and RVH AMU
17 | P a g e
weeks
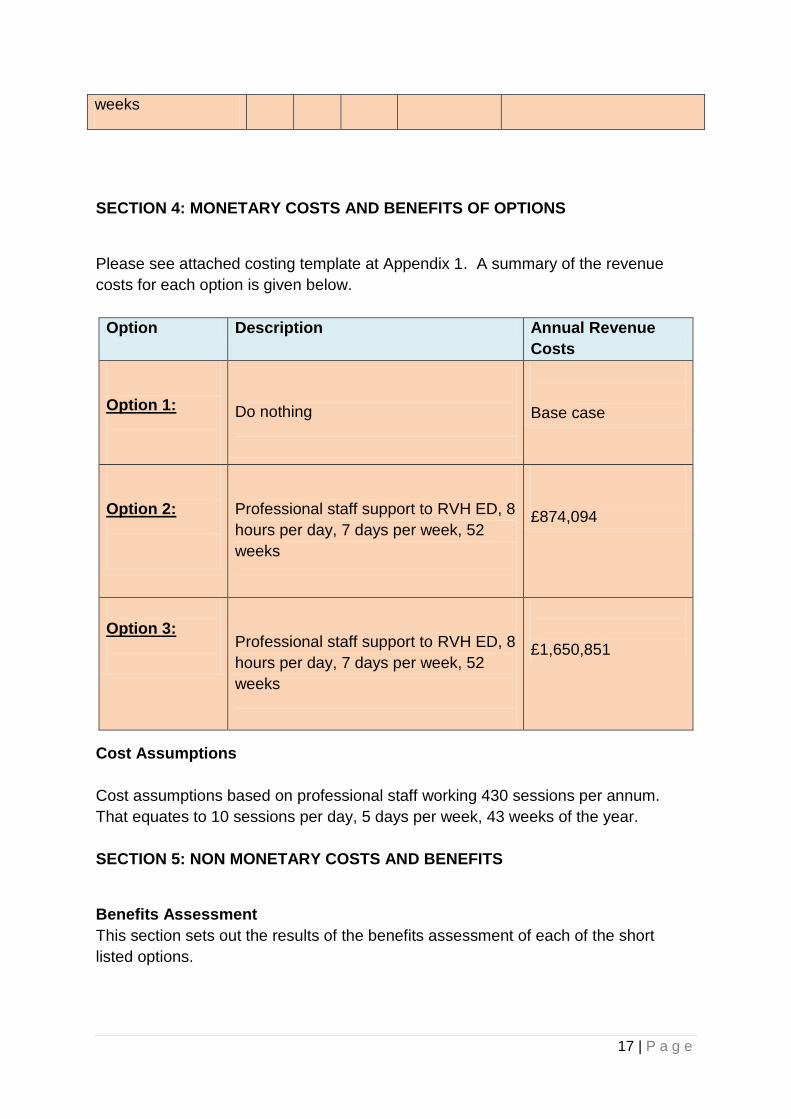
SECTION 4: MONETARY COSTS AND BENEFITS OF OPTIONS
Please see attached costing template at Appendix 1. A summary of the revenue
costs for each option is given below.
Option Description Annual Revenue
Costs
Option 1:
Do nothing
Base case
Option 2:
Professional staff support to RVH ED, 8
hours per day, 7 days per week, 52
weeks
£874,094
Option 3:
Professional staff support to RVH ED, 8
hours per day, 7 days per week, 52
weeks
£1,650,851
Cost Assumptions
Cost assumptions based on professional staff working 430 sessions per annum.
That equates to 10 sessions per day, 5 days per week, 43 weeks of the year.
SECTION 5: NON MONETARY COSTS AND BENEFITS
Benefits Assessment
This section sets out the results of the benefits assessment of each of the short
listed options.

18 | P a g e
In order to do this the Project Team has applied a weighting and scoring system (the
approved methodology for option appraisal in the Health Service) based on the
following approach:
(a) Identification and description of the major benefits to be achieved (the relevant
qualitative performance indicators (“QPI’s”));
(b) Allocation of weighting factors to each QPI resulting in a total score of 100;
(c) Scoring each option against the selected QPI’s;
(d) Calculation of a weighted score (score x weighting factor) for each option;
(e) Ranking and evaluation of results.
Benefit Criteria
Based on the objectives identified the following benefits have been identified and will
be used to evaluate the options.
Safety & Quality
Deliverability
Access
Sustainability
A description of the rationale behind each criteria and the relevant weighting is
outlined in the table below.
Weighting of Benefit Criteria
The weighting of the individual benefits determines their relative importance. The
more significant benefits will achieve higher weighting while those of lower impact
will achieve lower weighting.
Weighting was apportioned to the benefit criteria as follows:
Criterion Description Weighting
Safety &
Quality
Ensure compliance with clinical
guidance and standards. Ensure
staff have required experience to
undertake the patient decisions
and treatments required
40
Sustainability Ensure that services are
supported by sufficient staffing
and remain resilient in future.
20
Deliverability This considers readiness for
implementation and delivery of
30

19 | P a g e
additional proposed activity and
impact on patient flow
Access
This considers the ability to
improve timely access senior
decision making thereby
improving the patient journey
and flow.
10
Total 100
Explanation of the Weighting Scores
Safety and Quality
This criterion is weighted at 40/100 and reflects the need to assess the options in
respect of the ability to deliver quality outcome measures and comply with guidance
to meet the required professional standards.
Sustainability
This criterion is weighted at 20/100 and will reflect the need for adequate number of
staff with the appropriate skill mix to ensure a resilient service within the respective
areas
Deliverability
This criterion is weighted 30/100 and reflects the requirement for the service to
deliver additional activity within expected timeframe and impact on existing services.
Access
Weighted at 10/100 this criterion reflects the ability of the service to provide timely
access to the service to meet clinical access standards and reduction in hospital
length of stay.
Scoring of Options
The short-listed options were scored on each of the benefit criteria on a scale of 0 to
10. The short-listed options were considered in relation to how well they fulfilled the
non-monetary criteria. A score out of 10 was allocated to each of the options. This
demonstrated the ability of an option to achieve the full quality of a criterion. A higher
score indicated that an option met the criterion to a higher degree. The following
guide reflects the basis for each score. Total points available = 10.
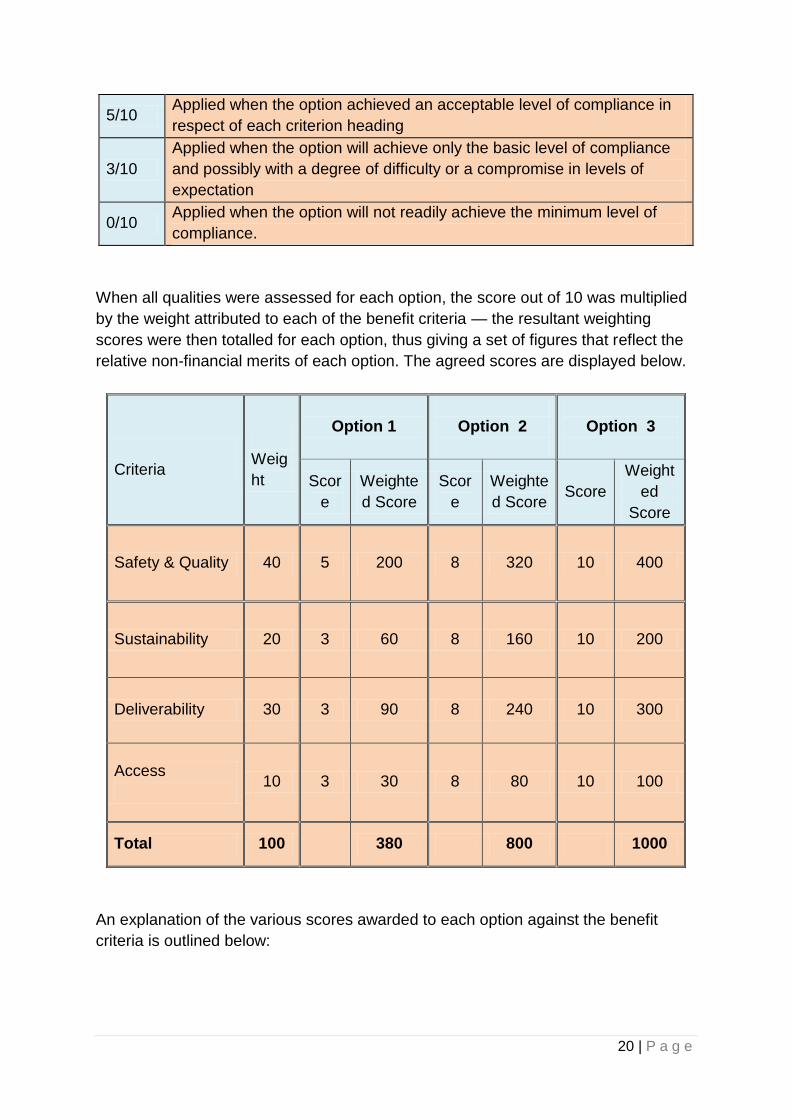
10/10 Applied where the option provides the ideal solution in respect of each
criterion heading
8/10 Applied when the option significantly achieved compliance in respect of
each criterion heading
20 | P a g e
5/10 Applied when the option achieved an acceptable level of compliance in
respect of each criterion heading
3/10
Applied when the option will achieve only the basic level of compliance
and possibly with a degree of difficulty or a compromise in levels of
expectation
0/10 Applied when the option will not readily achieve the minimum level of
compliance.
When all qualities were assessed for each option, the score out of 10 was multiplied
by the weight attributed to each of the benefit criteria — the resultant weighting
scores were then totalled for each option, thus giving a set of figures that reflect the
relative non-financial merits of each option. The agreed scores are displayed below.
Criteria
Weig
ht
Option 1
Option 2
Option 3
Scor
e
Weighte
d Score
Scor
e
Weighte
d Score Score
Weight
ed
Score
Safety & Quality 40 5 200 8 320 10 400
Sustainability 20 3 60 8 160 10 200
Deliverability 30 3 90 8 240 10 300
Access
10 3 30 8 80 10 100
Total 100
380 800 1000
An explanation of the various scores awarded to each option against the benefit
criteria is outlined below:

21 | P a g e
Criterion 1 - Quality and safety
Option 1 scored 5 out of 10 against this benefit, as the “do nothing” option
suggests continuing with the 5 day service that is currently in place. This service
does offer quality and safety but does not contribute to this 7 days per week. 52
weeks of the year. Therefore delays in decision making take place.
Options 2, scored 8 out of 10 against this benefit as this offers more resource over
the 7 days for the RVH Emergency department but does not provide the extended
resource for AMU
Option 3 offers the extended Professional staff service to both RVH ED and AMU
thereby ensuring that staff are there to carry out the duties and treatments in both
these areas over the required hours seven days per week.
Criterion 2 – Sustainability
Option 1 scored 3 out of 10 against this benefit. This option would only have a
small pool of staff available covering the service 5 days per week and would not
be adequately able to extend the service to meet the demands of 7 day working.
Option 2 scored 8 out of 10 against this benefit as this offers more resource over
the 7 days for the RVH Emergency department but does not provide the extended
resource for AMU
Option 3 scored 10 out of 10 against this benefit as it offers the extended
Professional staff service to both RVH ED and AMU thereby ensuring that staff
are there to carry out the duties and treatments in both these areas over the
required red hours seven days per week
Criterion 3 - Deliverability
Option 1 scored 3 out of 10 against this benefit. This option would only have a
small pool of staff available covering the service 5 days per week and would not
be adequately able to extend the service to meet the demands of 7 day working.
Option 2 scored 8 out of 10 against this benefit as this offers more resource over
the 7 days for the RVH Emergency department but does not provide the extended
resource for AMU
22 | P a g e
Option 3 scored 10 out of 10 against this benefit as it offers the extended
Professional staff service to both RVH ED and AMU thereby ensuring that staff
are there to carry out the duties and treatments in both these areas over the
required hours seven days per week.
Criterion 4 – Access
Option 1 scored 3 out of 10 against this benefit as “do nothing” does not facilitate
additional capacity and therefore does not improve service.
Option 2 scored 8 out of 10 against the benefit criteria. This option would improve
access to Professional staff for patients within the RVH ED but not to AMU.
Option 3 scored 10 out of 10 against the benefit criteria. This option would
improve access to Professional staff for patients within the RVH ED and RVH
AMU.
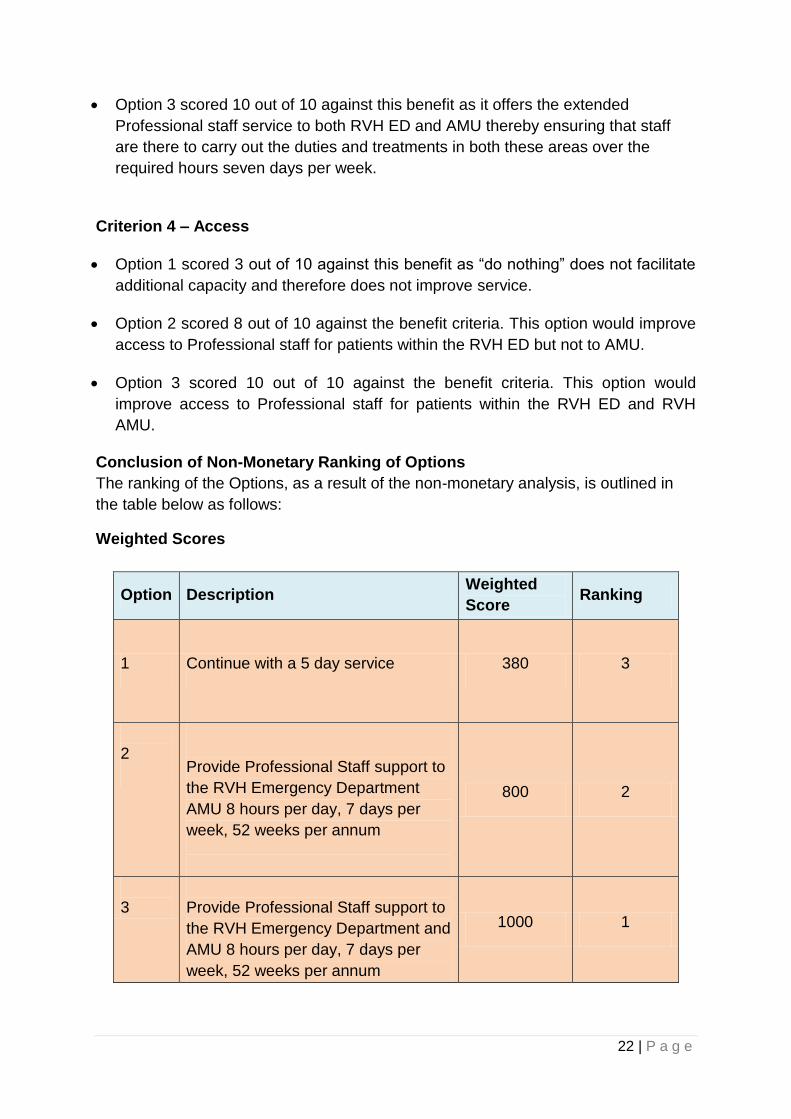
Conclusion of Non-Monetary Ranking of Options
The ranking of the Options, as a result of the non-monetary analysis, is outlined in
the table below as follows:
Weighted Scores
Option Description Weighted
Score Ranking
1 Continue with a 5 day service 380 3
2
Provide Professional Staff support to
the RVH Emergency Department
AMU 8 hours per day, 7 days per
week, 52 weeks per annum
800 2
3
Provide Professional Staff support to
the RVH Emergency Department and
AMU 8 hours per day, 7 days per
week, 52 weeks per annum
1000 1
23 | P a g e
The preferred option from the non-financial analysis is:
Option 3:
Provide Professional Staff support to the RVH Emergency Department and AMU 8
hours per day, 7 days per week, 52 weeks per annum
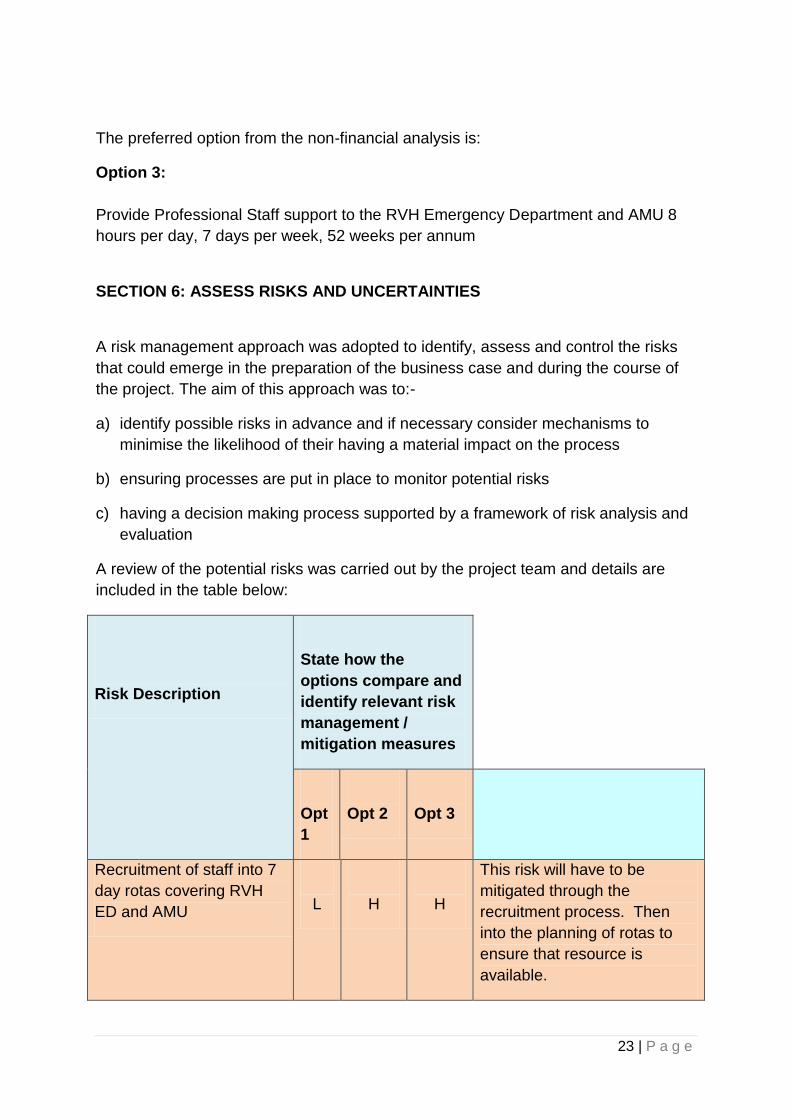
SECTION 6: ASSESS RISKS AND UNCERTAINTIES
A risk management approach was adopted to identify, assess and control the risks
that could emerge in the preparation of the business case and during the course of
the project. The aim of this approach was to:-
a) identify possible risks in advance and if necessary consider mechanisms to
minimise the likelihood of their having a material impact on the process
b) ensuring processes are put in place to monitor potential risks
c) having a decision making process supported by a framework of risk analysis and
evaluation
A review of the potential risks was carried out by the project team and details are
included in the table below:
Risk Description
State how the
options compare and
identify relevant risk
management /
mitigation measures
Opt
1
Opt 2
Opt 3
Recruitment of staff into 7
day rotas covering RVH
ED and AMU
L
H
H
This risk will have to be
mitigated through the
recruitment process. Then
into the planning of rotas to
ensure that resource is
available.

24 | P a g e
Overall Risk (H/M/L):
L
H
H
SECTION 7: PREFERRED OPTION AND EXPLANATION FOR SELECTION
Non-Financial Analysis
The summary of scores and ranking of the non-financial analysis is detailed below.
Option Description Weighted
Score
Ranking
1 Continue with 5 day service 380 3
2
Provide Professional Staff support to
the RVH Emergency Department 8
hours per day, 7 days per week, 52
weeks per annum
800 2
3 Provide Professional Staff support to
the RVH Emergency Department and
AMU 8 hours per day, 7 days per
week, 52 weeks per annum
1000 1
Financial Analysis
The summary of costs from the financial analysis is detailed below.
Option Description Annual
Revenue Costs
Ranking
1 Continue with 5 day service Base case 3
2 Provide Professional Staff support
to the RVH Emergency
Department 8 hours per day, 7
days per week, 52 weeks per
annum
£874,094 2
3 Provide Professional Staff support £1,650,851 1

25 | P a g e
to the RVH Emergency
Department and AMU 8 hours per
day, 7 days per week, 52 weeks
per annum
The preferred option from the financial analysis is:
Option 3: Provide Professional Staff support to the RVH Emergency Department
and AMU, 8 hours per day, 7 days per week, 52 weeks per annum
Preferred Option and Reason for selection
The Preferred option for the purposes of meeting the objectives is Option number 3.
This would provide a social work, pharmacy service, Occupational Therapy and
Physiotherapy service to the RVH Emergency Unit and the Acute Medical Unit 8
hours per day, 7 days per week and 52 weeks of the year. Therefore assessments,
treatment and discharge could take place more effectively and delays in these
patient pathways would be minimised. The cost of this option is £1,650,851. Option
number two is a first step towards this option in delivering the extended service for
the RVH Emergency Department and would provide the above benefits to that area
only. The cost of this option is £874,094.
SECTION 8: ASSESS AFFORDABILITY AND FUNDING ARRANGEMENTS
This section of the business case considers the potential impact on the recurring
revenue position for the Trust and the initial capital investment required to deliver the
preferred option.
To proceed with the preferred option requires the below investment:
Additional Capital Investment Nil
Additional Revenue Costs £1,650,851
Full costings are available in Appendix 1.
SECTION 9: PROJECT MANAGEMENT
The delivery of this business case will be managed through the respective service
areas. The Post Project evaluation will be carried out 6 months after the services
have been put in place but outcomes will be monitored monthly.
26 | P a g e
SECTION 10: MONITORING AND EVALUATION
(To include post project evaluation)
The implementation of a recurrently funded service will be led from within the
BHSCT Unscheduled and Acute Care Service Group. It will be managed by the
Service Manager.
The following table demonstrates how the monitoring and evaluation will be
undertaken.
SECTION 11: ADDITIONAL ACTIVITY
Activity levels expected for each of the 3 Professional areas will need to be set
dependent on the investment made.
27 | P a g e
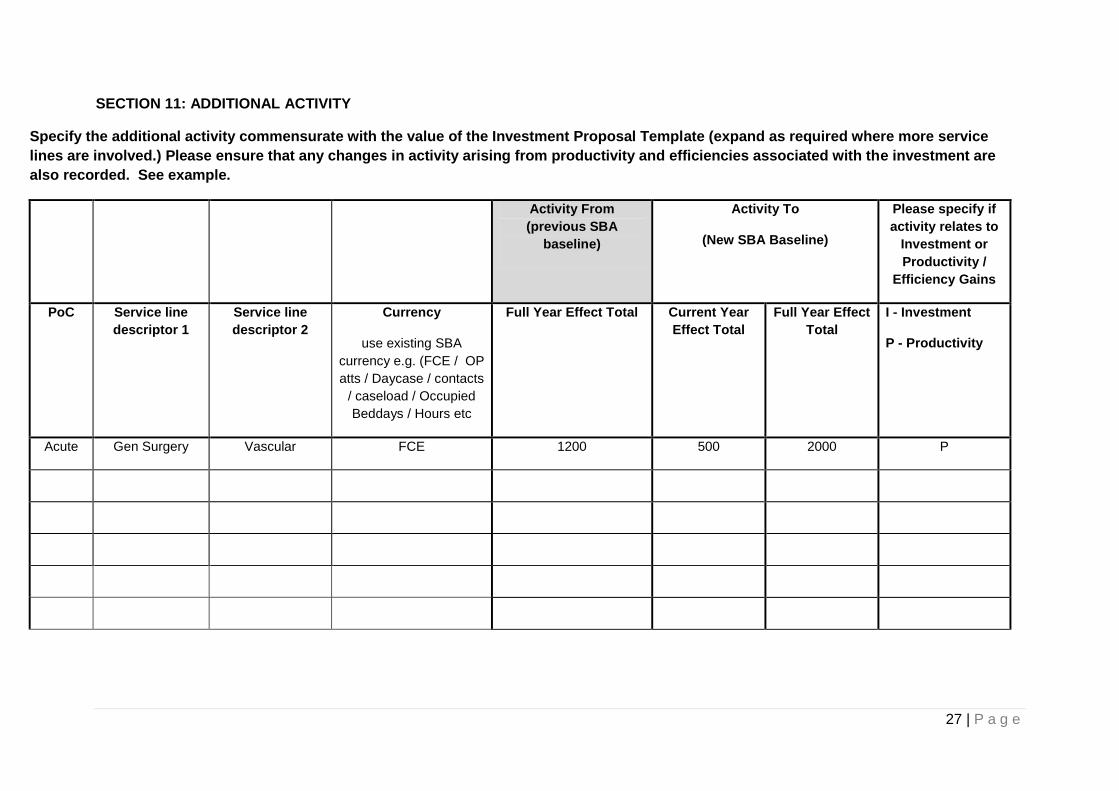
SECTION 11: ADDITIONAL ACTIVITY
Specify the additional activity commensurate with the value of the Investment Proposal Template (expand as required where more service
lines are involved.) Please ensure that any changes in activity arising from productivity and efficiencies associated with the investment are
also recorded. See example.
Activity From
(previous SBA
baseline)
Activity To
(New SBA Baseline)
Please specify if
activity relates to
Investment or
Productivity /
Efficiency Gains
PoC Service line
descriptor 1
Service line
descriptor 2
Currency
use existing SBA
currency e.g. (FCE / OP
atts / Daycase / contacts
/ caseload / Occupied
Beddays / Hours etc
Full Year Effect Total Current Year
Effect Total
Full Year Effect
Total
I - Investment
P - Productivity
Acute Gen Surgery Vascular FCE 1200 500 2000 P

28 | P a g e