king saud university college of nursing
DESCRIPTION
BurnHatem AlsrourKing Saud UniversityCollege of NursingTRANSCRIPT
BurnHatem Alsrour
King Saud UniversityCollege of Nursing
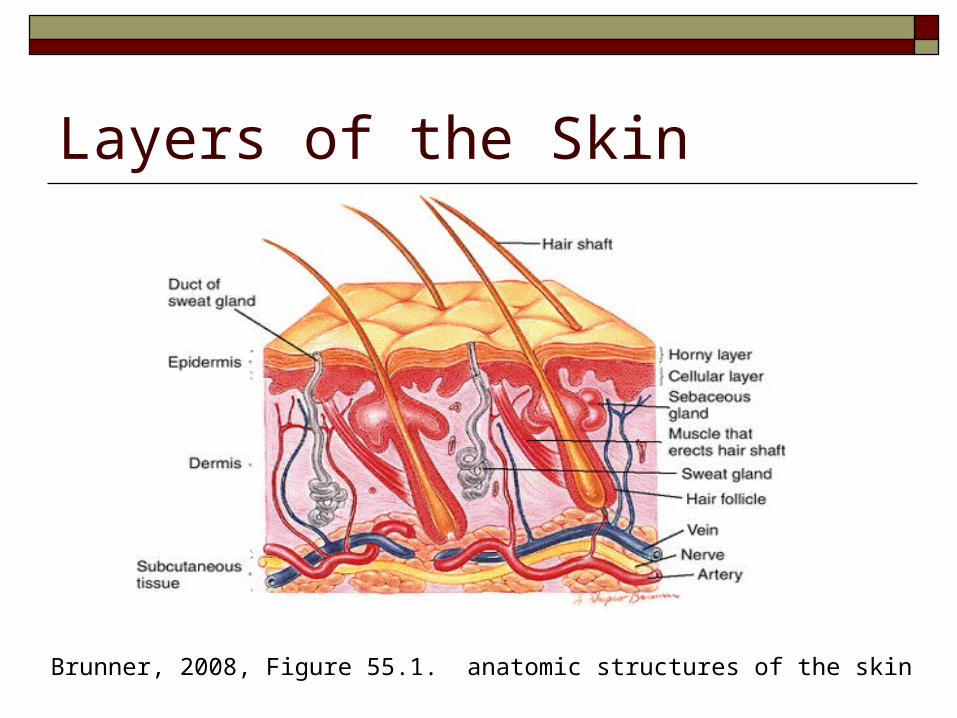
Layers of the Skin
Brunner, 2008, Figure 55.1. anatomic structures of the skin
EpidermisOutermost layer, composed of cornified epithelial cells.
Outer surface cells are dead and sloughed off.
DermisMiddle layer, composed primarily of connective
tissue .
Contains capillaries that nourish the skin, nerve endings and hair follices
HypodermisLayer of adipose and connective tissue
between the skin and underlying tissues.
Function of SkinFunction of Skin
Protection from infection & injury Prevention of loss of body fluid Regulation of body temperature Sensory contact with environment
What is a BurnWhat is a Burn?? An injury to tissue from:
–Exposure to flames or hot liquids–Contact with hot objects–Exposure to caustic chemicals or radiation–Contact with an electrical current
Types (Causes) of Burn InjuryThermalOpen flame, steam, hot liquids
ChemicalAcids, strong alkalis, organic compounds
ElectricalDirect or alternating current, lightning
RadiationRadioactive agents
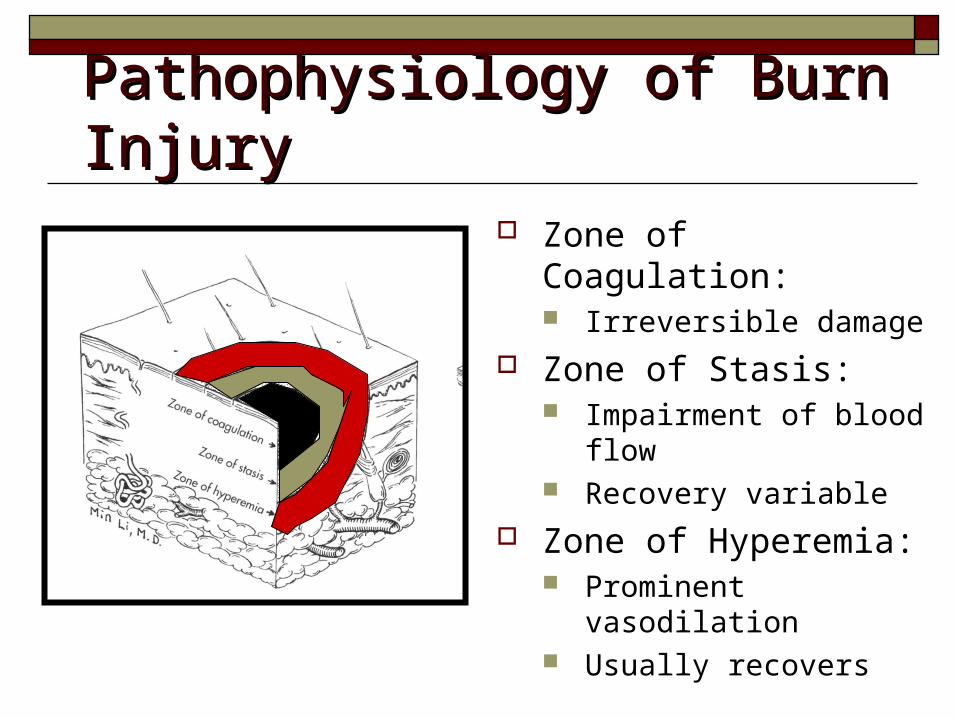
Pathophysiology of Burn InjuryPathophysiology of Burn Injury Zone of Coagulation:
Irreversible damage Zone of Stasis:
Impairment of blood flow Recovery variable
Zone of Hyperemia: Prominent vasodilation Usually recovers
Severity of a BurnSeverity of a Burn
Depends on: Depth of burn Extent of burn Location of injury Patient’s age
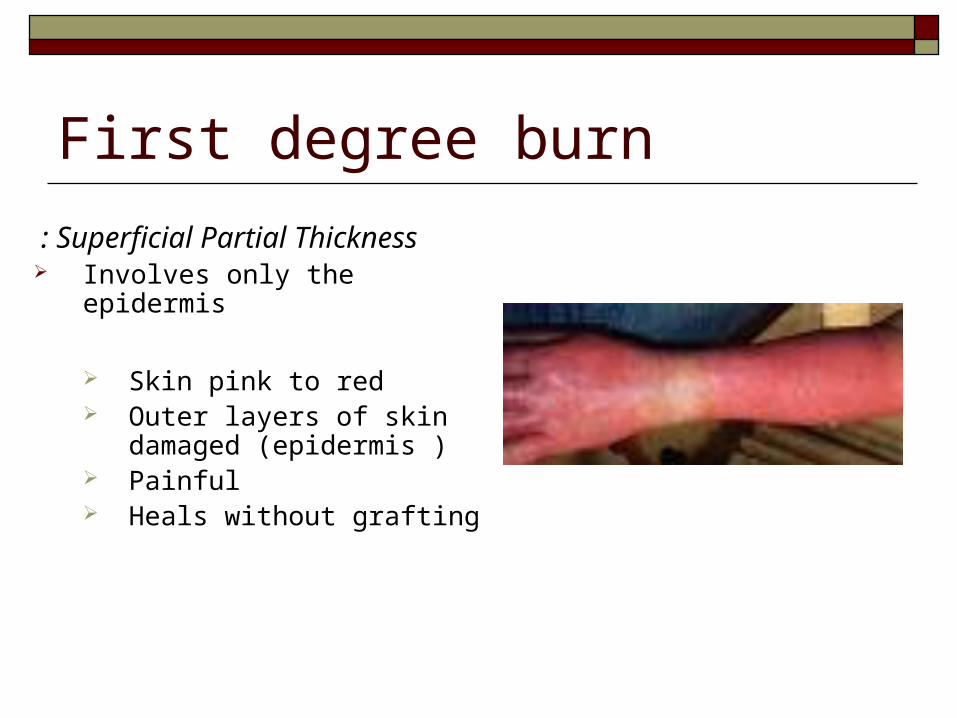
First degree burn
Superficial Partial Thickness : Involves only the epidermis
Skin pink to red Outer layers of skin
damaged (epidermis ) Painful Heals without grafting
Second degree burn
Deep partial thickness Involve the epidermis and
portions of the dermis Skin red to white Blisters Weeping surface Edema All epidermis and much of
dermis damaged Painful Heals without grafting

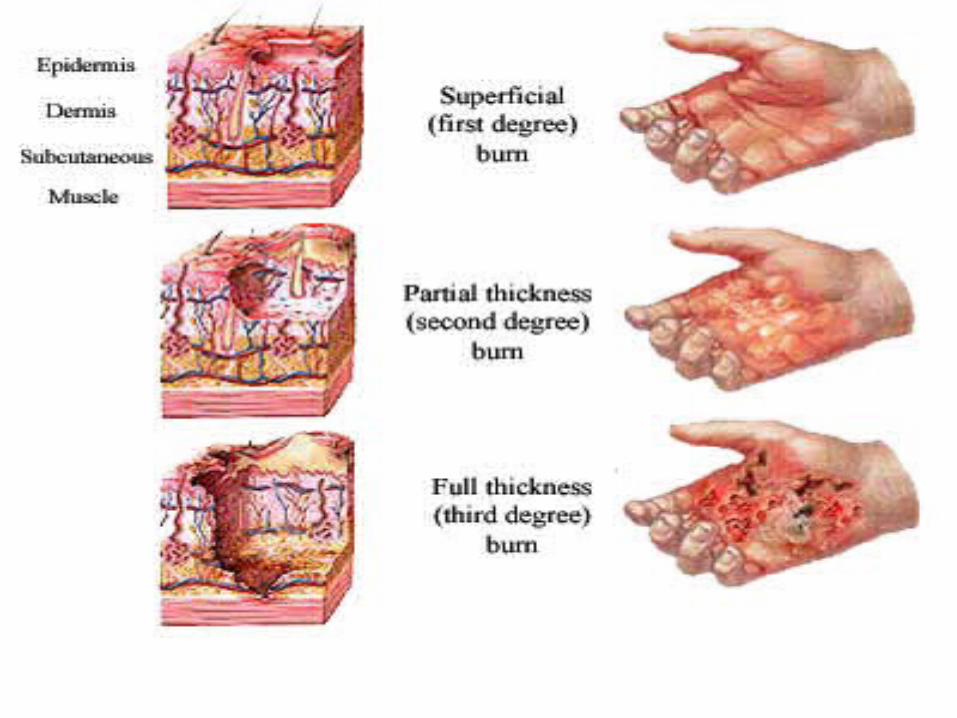
Partial thickness Partial thickness (second-degree) (second-degree)
burnsburns
Superficial (first-Superficial (first-degree) burnsdegree) burns
Third degree burn
Referred to as full-thickness burns Charred appearance(black, brown, leathery) Waxy, white Edema All layers of skin destroyed Nerves, muscle tissue, and bone may be
destroyed Grafting preferred

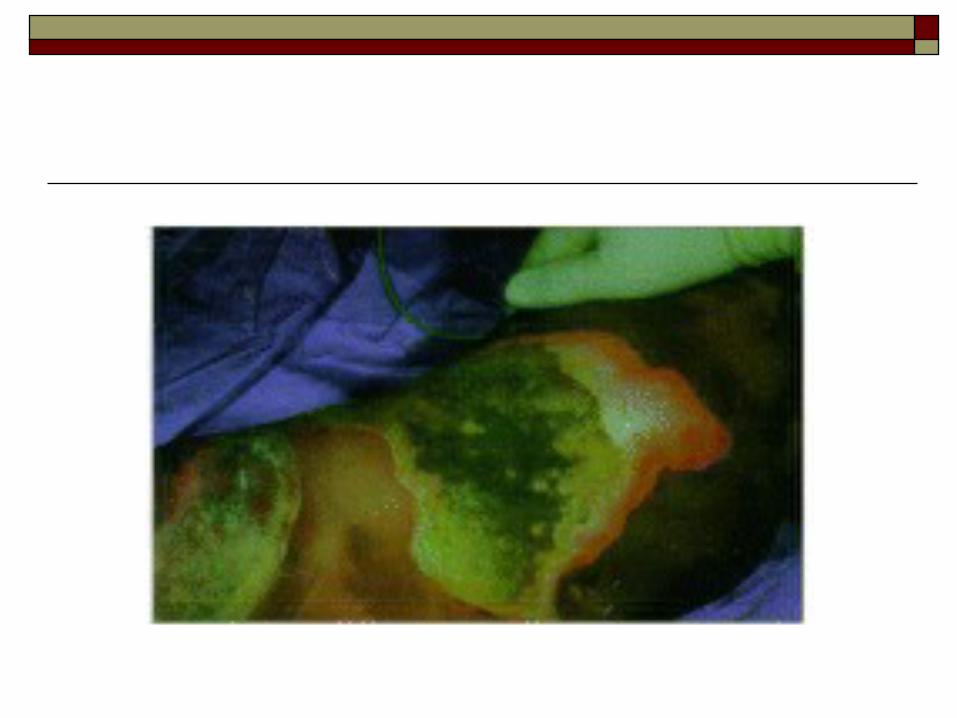

Full thickness (third-degree) burnsFull thickness (third-degree) burns
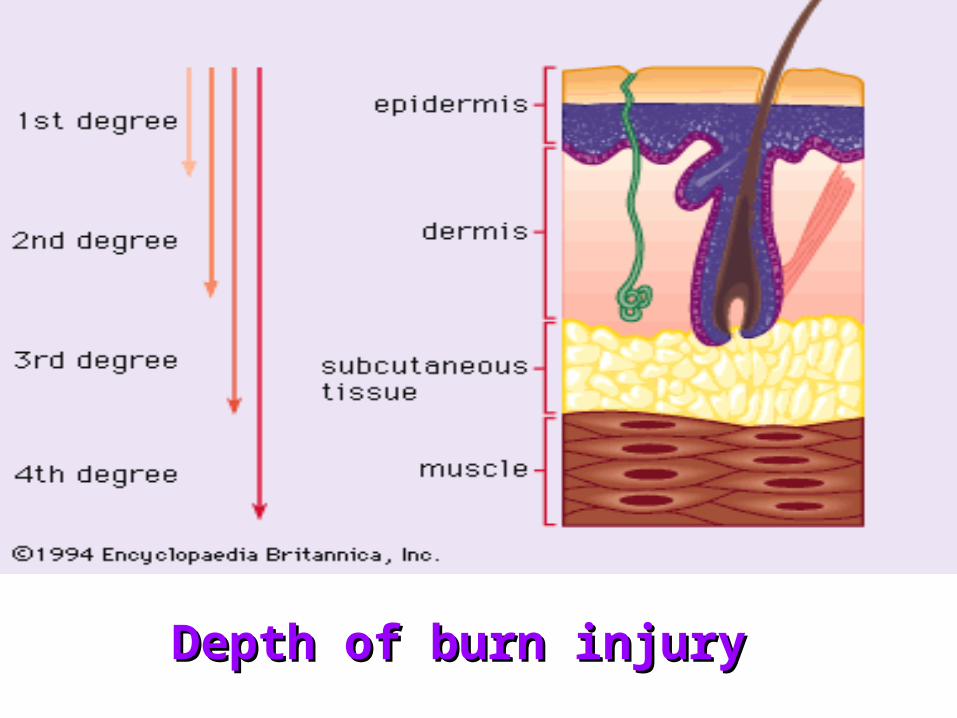
Depth of burn injuryDepth of burn injury
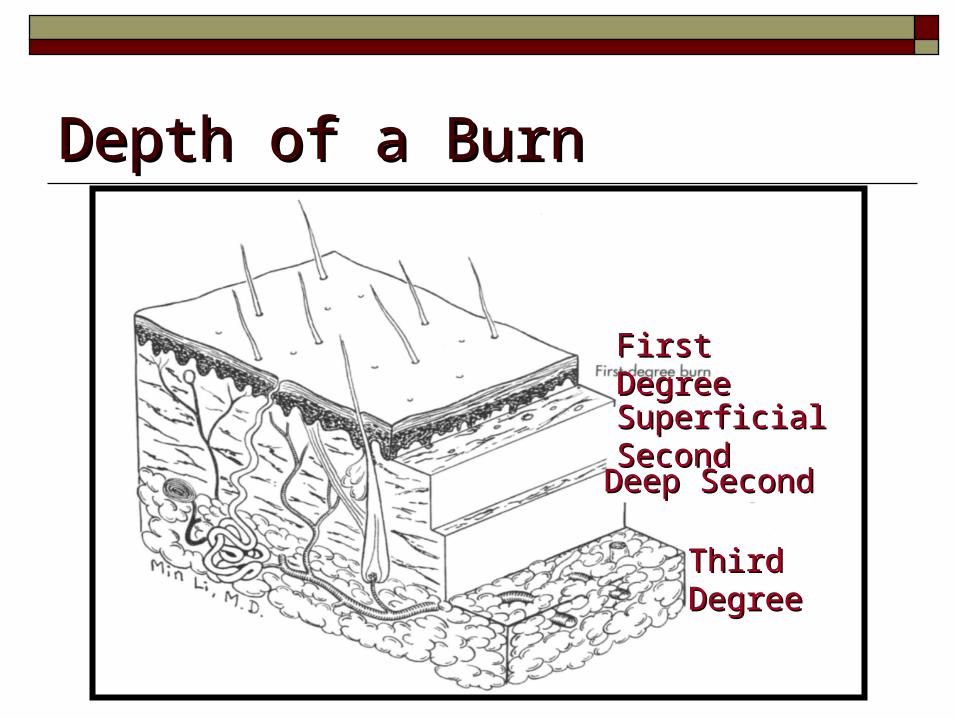
Depth of a BurnDepth of a Burn
First DegreeFirst Degree
SuperficialSuperficial SecondSecond
Deep SecondDeep Second
Third DegreeThird Degree
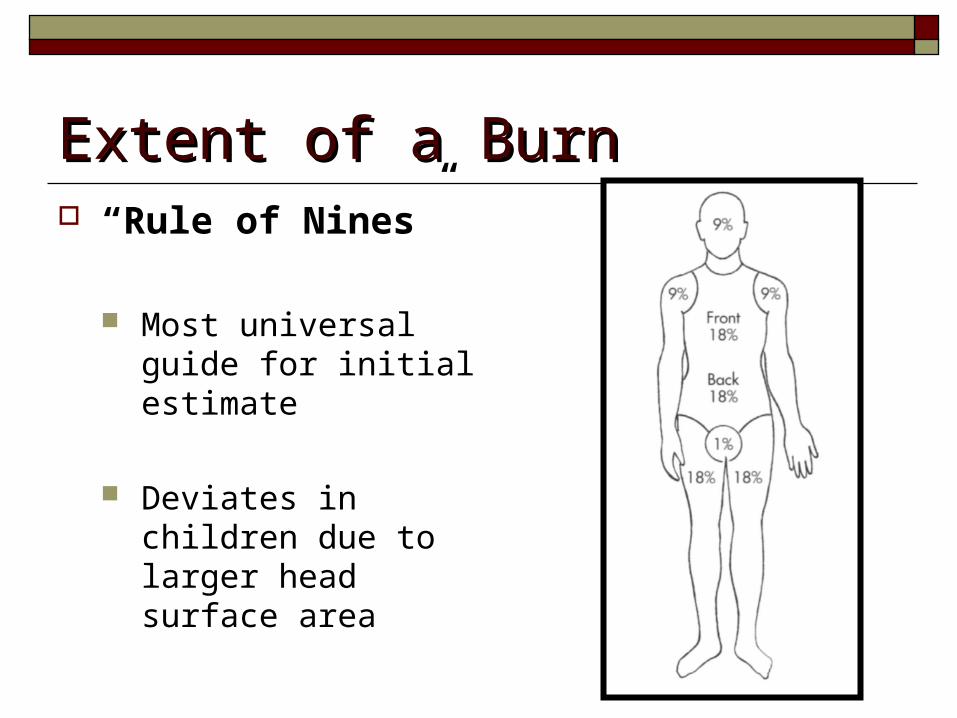
Extent of a BurnExtent of a Burn “Rule of Nines”
Most universal guide for initial estimate
Deviates in children due to larger head surface area
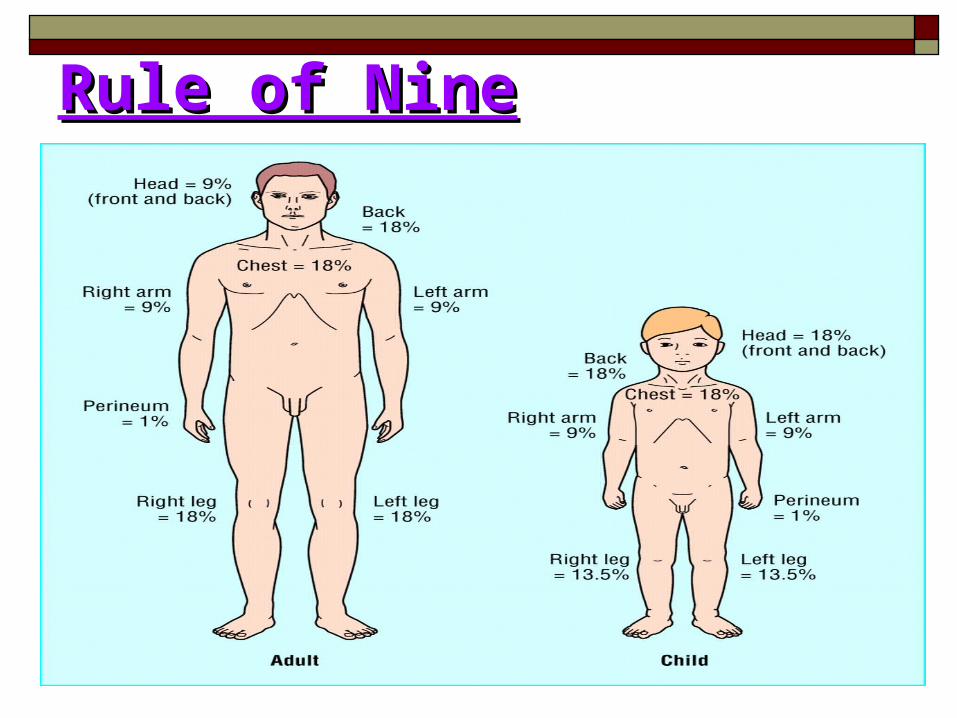
Rule of NineRule of Nine
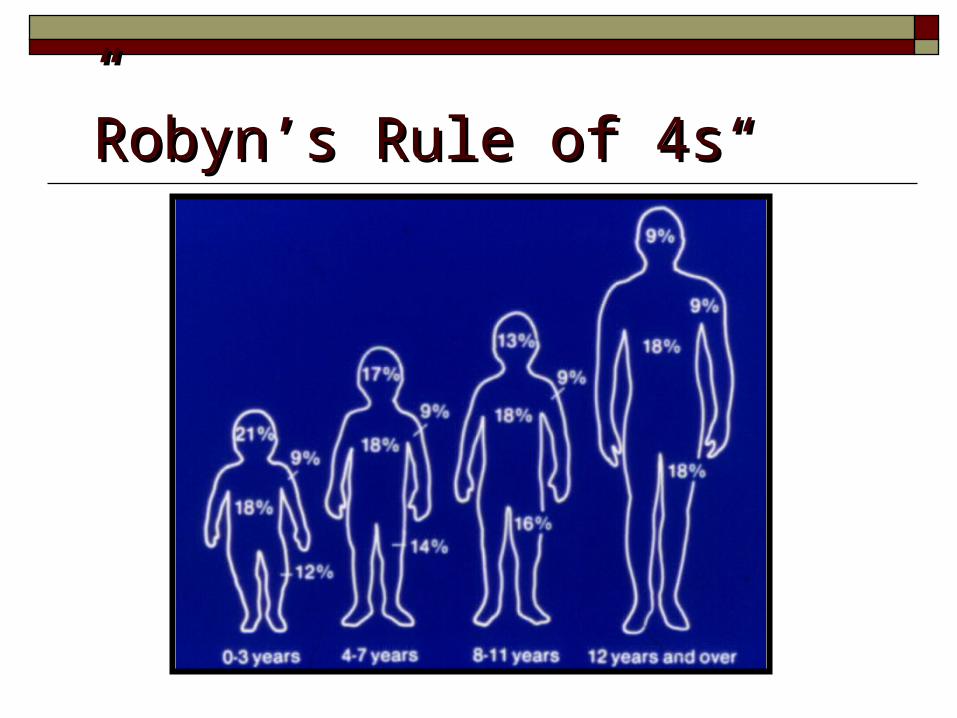
““RobynRobyn’’s Rule of 4ss Rule of 4s””
Carbon Monoxide PoisoningCarbon Monoxide Poisoning
Colorless, odorless gas Binds to hemoglobin 200 times more than oxygen Most immediate threat to life in survivors with
severe inhalation injury Toxicity related directly to percentage of
hemoglobin it saturates
Carbon Monoxide PoisoningCarbon Monoxide PoisoningSigns & Symptoms of Carbon Monoxide ToxicitySigns & Symptoms of Carbon Monoxide Toxicity
Carboxyhemoglobin (%)Carboxyhemoglobin (%) Signs/SymptomsSigns/Symptoms
0-100-10 NoneNone
10-3010-30 HeadacheHeadache
30-5030-50 Headache, nausea, Headache, nausea, dizziness, tachycardiadizziness, tachycardia
50-6050-60 CNS dysfunction, CNS dysfunction, comacoma
60+60+ DeathDeath
CO Poisoning: TreatmentCO Poisoning: Treatment 100% oxygen until carboxyhemoglobin levels
less than 15
Shock & Fluid ResuscitationShock & Fluid ResuscitationGoal:
To maintain vital organ function while avoiding the complications of inadequate or excessive therapy
Resuscitation Fluid NeedsResuscitation Fluid Needs Related to:
extent of burn (rule of nines) body size (pre-injury weight estimate)
Delivered through large bore peripheral IV Attempt to avoid overlying burned skin Can use venous cut down or central line
Parkland Formula: Adults : 2-4 ml RL x Kg body weight x % burn Children: 3-4 ml RL x Kg body weight x %
burn
Monitoring of ResuscitationMonitoring of Resuscitation
Urinary output is a reliable guide to end organ perfusion Adults: 30-50 ml per hour Children (less than 30 Kg): 1 ml/Kg per hour
Chemical Burns Occur whenever a toxic substance contacts
the body Eyes are particularly vulnerable. Fumes can cause burns. To prevent exposure, wear appropriate gloves
and eye protection.
Care for Chemical Burns Remove the chemical from the patient. If it is a powder chemical, brush off first. Remove all contaminated clothing. Flush burned area with large amounts of
water for about 15 to 20 minutes.
Electrical Burns Make sure the power is off before touching
the patient. There will be two wounds (an entrance and an
exit wound) to bandage. Arrange for prompt transport and be prepared
to administer CPR.
Pre-hospital CareStop the burning processThermal – smother; stop, drop, and rollChemical – remove clothing and flush / irrigate skin / eyesElectrical – shut off electrical current or separate person from source with a nonconducting implement (such as wooden broomstick)Radiation – limit exposure
1-Stop the burning process, if still active
2 -Remove all clothing and jewelry, rings, in anticipation of edema formation.
3 -Ensure patent airway. Prepare for early intubation
4 -Administer oxygen via a mask at flow rate sufficient enough to keep reservoir bag inflated;
usually requires 12 to 15L\minute
5-Assist Ventilation, if needed
Emerncy impelementation : Emerncy impelementation :
6 -Cannulate two veins with large-bore, 14- or 16-gauge catheters, and initiate infusion of an IV solution
7 -Infuse a crystalloid solution such as lactated Ringer's solution according to a pre established fluid protocol.
8 -Fluid resuscitation is based on the individual patient's response to the injury. Patients who may require more fluid than predicted are those patients who have:
An inhalation injury A high voltage electrical injury
Delayed fluid resuscitation since the time of injury
9 -Administer analgesic medications, e.g., morphine, IV
10 -Insert a gastric tube. If patient has TBSA more than 25%, nausea & vomiting are present
11 -Apply cool, saline-moistened, sterile dressings to TBSA burns less than 10% .
* Do not use ice * Keep the area cool will help to relieve pain
* Apply cool dressings within 10 minutes of the burn to reduce the heat content of the tissues and the depth of the burn injury
ABCs of Emergency Burn Care (Advanced Burn Life Support)
A = Airway (with cervical spine assessment) B = Breathing C = Circulation D = Disability E = Exposure and Environmental Control F = Fluid Resuscitation based on Burn Size and
Weight Measurement Secondary Survey
A: Airway Assess the patient’s airway Upper airway edema due to inhalation injury
Rapid or delayed progression Decision to intubate: individualized
B: Breathing Look, listen, feel for breath sounds and chest
movement Give 100% oxygen to all victims of major
burn beginning in the field Pulse oximetry Arterial blood gases
Required for definitive diagnosis of CO Baseline chest x-ray
C: Circulation Who needs fluid resuscitation?
All >20% total body surface area burned (TBSA) Young and old with >10% TBSA
2 large bore peripheral IVs
D: Disability Assess level of consciousness: AVPU
Alert Responds to verbal stimuli Responds to painful stimuli Unresponsive
Alteration in mental status is not normal Moves extremities
E: Exposure and Environment Remove clothing, jewelry Keep warm
blankets warm I.V. fluids heating lamps heat the room
Keep Patient Dry
F: Fluid Resuscitation(based on burn size and weight)
Determine fluid needs based on burn size and weight
Burn size: include second and third degree only Rule of Nines
Nursing ConsiderationsGoals:Correct fluid and electrolyte imbalancePromote wound healingSupport nutritionControl painPrevent complications of immobilitySupport patient
QuestionsWhich nursing intervention holds the highest priority of a patient with burns to her face and upper respiratory tract?
A – Elevate the head of the bed to at least 30ºB – Administer six liters of oxygen via nasal
cannulaC – Medicate the patient prior to repositioning
the patient in bedD – Prevent moving the skin around the burn
site
Answer: Which nursing intervention holds the highest priority of a patient with burns to her face and upper respiratory tract?
A – Elevate the head of the bed to at least 30º
B – Administer six liters of oxygen via nasal
cannulaC – Medicate the patient prior to repositioning
the patient in bedD – Prevent moving the skin around the burn
site
QuestionsWhat is the highest priority for the nurse when caring for a patient who has just received an electrical burn?Disconnect the patient from the electrical
sourceB. Ensure the patients have a cervical collar
and be placed on a back board prior to care.C. Monitor for cardiac dysrhythmia.D. Patients may require changes in fluid
resuscitation as compared to patients with other types of burns.
Answer : What is the highest priority for the nurse when caring for a patient who has just received an electrical burn?A. Disconnect the patient from the electrical
sourceB. Ensure the patients have a cervical collar
and be placed on a back board prior to care.C. Monitor for cardiac dysrhythmia.D. Patients may require changes in fluid
resuscitation as compared to patients with other types of burns.