introduction to parkinson’s disease & cognition rob white, md, phd may 9, 2013 pd forum...
TRANSCRIPT

Introduction to Parkinson’s Disease & Cognition
Rob White, MD, PhD
May 9, 2013
PD Forum Presentation

2
A Little About Your Presenter…
Affiliations
– Clinical Instructor, Movement Disorders Group, Department of Neurology, UCSF
– Staff Neurologist, Center for Parkinson's Disease and Movement Disorders, San Francisco VA Medical Center
– Visiting Researcher, Helen Wills Neuroscience Institute, UC Berkeley
Training
– MD (Medicine) & PhD (Neuroscience), Washington University, St. Louis, MO 1999-2007
– Adult Neurology Residency, UCSF, 2007-2011
– Fellowship in Behavioral Neurology & Movement Disorders, UCSF, 2011-2012
PD & Cognition

3
Outline
• Illustrative Cases
– Idiopathic Parkinson’s Disease
– Parkinson’s Disease Dementia
– Dementia with Lewy Bodies
• Opportunities To Participate In Research
• Questions
PD & Cognition
4
Some Goals
• Understand the importance of dopamine in certain aspects of cognition and the complexity of the underlying neuro-anatomy
• Learn how we test cognitive function
• Understand the distinction between “cognitive impairment” and “dementia”
PD & Cognition
5
Cognition in Parkinson’s Disease
Ms. Keen
• A 71-year-old woman with motor symptoms for 2 years was recently diagnosis of idiopathic PD.
• She is easily distracted, and often loses her train of thought.
• It takes her more time to read a map or use a computer than in the past.
• Sometimes, she has difficulty with calculations, but keeps up with her bills and finances.
PD & Cognition

6
Cognition in Parkinson’s Disease
• Over 50% of people with PD experience some form of cognitive impairment
• Difficulties are typically in the following areas:
– attention
– short-term memory
– executive (problem-solving, multi-tasking)
– visuo-spatial (perception, navigation, calculation)
PD & Cognition

7
Cognition in Parkinson’s Disease
• Dopamine-producing neurons in the substantial nigra send signals to the striatum, a part of the basal ganglia
• Dopamine-producing neurons in the ventral tegmental area send signals to the frontal lobes
• The striatum and cerebral cortex communicate information back and forth
• Different parts of the striatum are connected to different parts of the cortex with specialized functions (visual, motor, executive, motivation)
PD & Cognition

8
Dopamine and Cognition
• ”Inverted U” relationship between cognitive function and brain dopamine
• Too little dopamine poor cognitive performance (“depletion”)
• Too much dopamine poor cognitive performance (“over-dosing”)
• Optimal dopamine level may change depending on the nature of the task
PD & Cognition

9
Cognitive Screening Tests
abnormal screening test results should usually prompt more detailed cognitive testing, usually performed by a neuropsychologist
PD & Cognition
Mini-Mental Status Examination (MMSE)
– orientation
– word recall
– attention
– language
– visuo-spatial
normal = ≥ 25 of 30 points
Montreal Cognitive Assessment (MoCA)
– orientation
– word recall
– attention
– language
– visuo-spatial
– abstraction
– executive function
normal = ≥26 of 30 points

10
Cognitive Screening Tests
PD & Cognition
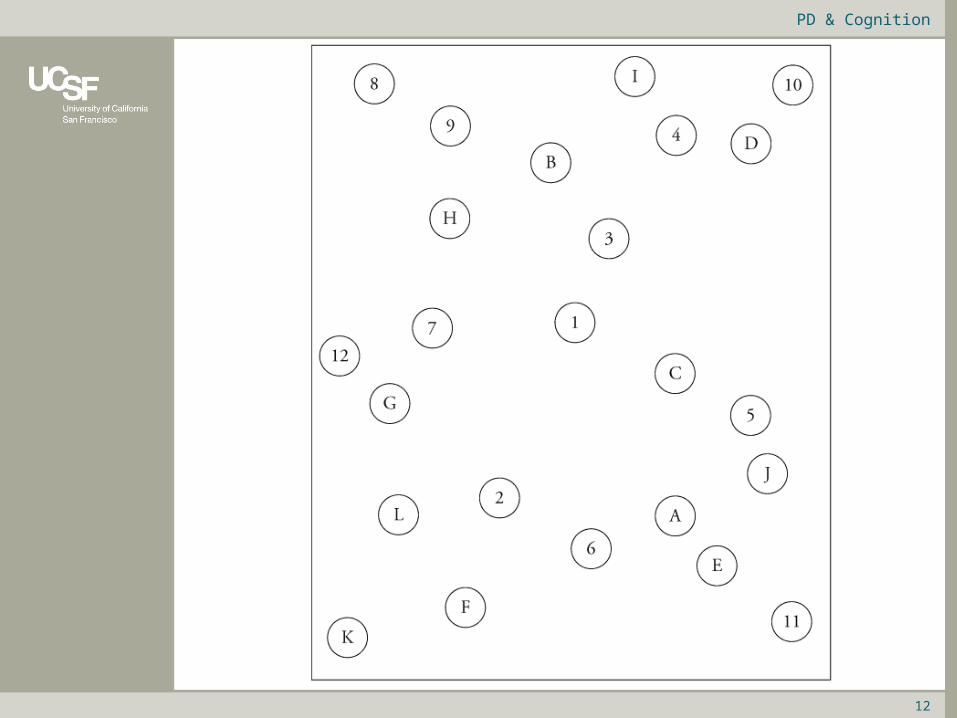
Word Recall

11
Cognitive Screening Tests
PD & Cognition
Word Recall
TRAIN EGG HAT CHAIR BLUE
12
PD & Cognition

13
PD & Cognition

14
PD & Cognition

15
Cognitive Screening Tests
PD & Cognition
Word Recall
? ? ? ? ?

16
Cognitive Screening Tests
PD & Cognition
Word Recall
TRAIN EGG HAT CHAIR BLUE

17
Parkinson’s Disease Dementia
Mr. Dee
• A 79 year old man was diagnosed with idiopathic PD in 2002.
• He began having some forgetfulness and difficulty with bookkeeping in 2008.
• Neuropsychological testing showed mild deficits in processing speed, executive function, and memory.
• There was gradual progression of memory problems. He stopped participating in activities he enjoyed.
• MMSE gradually declined from 29 to 25.
• In 2011, more rapid decline in memory over 6 months (MoCA = 11) and having trouble with driving, needed help from friends/family to to dress, cook.
PD & Cognition

18
Parkinson’s Disease Dementia
• Cognitive Impairment: abnormal cognitive function that does not significantly affect daily activities
– Can be irritating or concerning to an individual
– Can be measured by objective tests and compared to age-appropriate norms
– May involve one or more cognitive domains
• Dementia: problems with cognition that interfere with daily activities and quality of life
– More advanced problems in cognition
– Typically, memory + another domain (problem-solving, attention)
PD & Cognition

19
Parkinson’s Disease Dementia
• Features:
– More difficulty with memory and slowness of thinking.
– Language is relatively unaffected (unlike in Alzheimer’s disease).
• Risk factors for dementia:
– longer duration of illness
• 10-30% of patients develop dementia over 10-12 years
• up to 80% by 20 years in some studies
– older age
– family history of dementia
PD & Cognition

20
Parkinson’s Disease Dementia
• Other causes of impaired cognition/dementia:
– People with Parkinson’s disease can get Alzheimer’s disease (up to 33% of advanced PD, increased risk with older age).
– Vascular disease (small, unnoticed strokes) can contribute to dementia, so monitoring and controlling stroke risk factors, like blood pressure, is important.
– Certain anti-Parkinson’s medications can cause cognitive side effects (e.g. slow thinking, hallucinations).
– Depression and anxiety can interfere with thinking and memory.
– Poor sleep can interfere with attention and judgment.
PD & Cognition

21
Do You Remember?
PD & Cognition
Word Recall
? ? ? ? ?

22
Do You Remember?
PD & Cognition
Word Recall
TRAIN EGG HAT CHAIR BLUE

23
Dementia with Lewy Bodies
Mr. Lobe
• A 68-year-old man had a same-day urologic procedure performed.
• When he awoke from anesthesia, he was agitated, disoriented, and hallucinating. He received haloperidol (a sedating drug) and developed significant sleepiness and rigidity that lasted 24 hours, requiring hospitalization.
• Afterwards, he gradually improved to close to his baseline functioning. He continued to have some visual misperceptions (for example, looking out the window and stating that it was raining when it was not).
PD & Cognition
24
Dementia with Lewy Bodies
• He had been more forgetful in the past year.
• He had developed trouble parallel-parking his car.
• On a recent family trip, he did not walk as fast as the others in the group, which was atypical for him.
• On examination, MMSE was 26 out of 30 (difficulties with attention and ability to draw intersecting pentagons and a clock face. He had intact delayed recall.
• There were signs of Parkinson’s (decreased facial expression, low volume of voice, slight tremor, rigidity in both arms, stooped posture, slow walking, and decreased arm swing when walking).
• Re-evaluation 6 months later showed continuing evidence of Parkinson’s and increasing cognitive impairment (MMSE = 24). He still had intermittent visual hallucinations, especially in the evening hours.
PD & Cognition

25
Dementia with Lewy Bodies
• Features:
– Cognitive impairment and Parkinson’s motor symptoms began approximately at the same time.
– Fluctuations in attention and alertness, especially with surgeries, medications.
– Frequent visual hallucinations.
PD & Cognition

26
Dementia Treatment
• Medications:
– Cholinesterase inhibitors
• rivastigmine (Exelon)
• galantamine (Razadyne)
• donepezil (Aricept)
– NMDA receptor antagonist
• memantine (Namenda)
• Cardiovascular Exercise!
PD & Cognition

27
Research in our Laboratory
• Principal Investigators:
– Mark D’Esposito, M.D.
– Rich Ivry, Ph.D.
• We study the neurologic basis of various cognitive processes:
– Short-term memory
– Multi-tasking
– Problem-solving
• We use a variety of methods:
– Behavioral testing
– Functional MRI
– Electroencephalography (EEG)
– Transient Magnetic Stimulation (TMS)
• We are actively recruiting paid volunteers
– Healthy young adults
– Healthy older adults
– Adults with brain injury/stroke
– Adults with mild/moderate Parkinson’s Disease
PD & Cognition
28
Research at UC Berkeley
• Design: The study involves 2 sessions (ON and OFF medications), scheduled at least a week apart.
– Each session takes about 4 hours.
– There is about 1 hour of testing in the MRI scanner.
– The remainder of the time is for clinical/neuropsychological testing, breaks, and paperwork/consents.
• Reimbursement: $20/hr, as well as any travel expenses.
• Transportation: we provide parking permits or transportation with a driver to and from our lab at UC Berkeley.
• Inclusion criteria:
– Mild/moderate Idiopathic Parkinson's disease (walking/balance)
– Taking medication for PD and willing to hold meds for one session
– Right-handed, non-smokers, normal color vision
• Exclusion criteria:
– Cognitive impairment or dementia
– A history of major neurologic or psychiatric disorder, major systemic disease
– Any MRI-incompatible implants (e.g. DBS, pacemaker) or other medical contraindication to MRI scanning
• We are also recruiting healthy adults ages 55-75 as a control group
PD & Cognition

29
Research at UCSF/SFVA
• Principal Investigator:
– Maya Katz, M.D.
• Preliminary study of N-acetyl-cysteine (NAC) as a medication that could potentially delay the progression of Parkinson's disease.
– NAC is an FDA approved, well tolerated medication that has been available for decades. Before we can do a larger study, we need to understand what dose adequately enters the brain, and that is why we are recruiting patients for this preliminary study.
• Design: participants will take NAC for 2 days, and will have a lumbar puncture (spinal tap) before and after they take this
• Inclusion criteria:
– Parkinson’s Disease
– Stable PD medications for 2 weeks
– No allergies to N-acetyl-cysteine
– No antiplatelet or anticoagulation (no Plavix, Coumadin, but aspirin is okay)
– DBS is okay
• Participants will receive $100.
PD & Cognition

30
Do You Still Remember?
PD & Cognition
Word Recall
? ? ? ? ?

31
Do You Still Remember?
PD & Cognition
Word Recall
TRAIN EGG HAT CHAIR BLUE

32
• Web Resources
– National Parkinson Foundation• www.parkinson.org
– Parkinson’s Disease Foundation
• www.pdf.org
– NINDS Parkinson’s Disease Research Web• www.ninds.nih.gov/research/parkinsonsweb/patients/
patients.htm
– Worldwide Education and Awareness of Movement Disorders
• www.wemove.org
PD & Cognition
• Contact Information