intro to health policy basics jamie dhaliwal, md mph emra legislative advisor @denverdhali
TRANSCRIPT
INTRO TO HEALTH POLICY BASICS Jamie Dhaliwal, MD MPH
EMRA Legislative Advisor
@DenverDhali

Goals
• Define legislative and regulatory advocacy
• Understand the components of the SGR fix
• Understand the basics of King vs Burwell
What is advocacy?
The act or process of supporting a cause or proposal
How do we advocate? • Legislative Advocacy
• Convince elected legislators to write, support and vote• Target efforts in context of committee system and rules
• Regulatory Advocacy• Regulations = How a bill gets put into practice• Same opportunities for influence exist
SGR REPEALMedicare and CHIP Reauthorization Act (MACRA)
SGR Basics• Sustainable Growth Rate
• Balanced Budget Act of 1997
• Tied aggregate Medicare spending to GDP growth
• 2002 – Physician reimbursement was threatened with large cuts
• Cost of permanent fix led to 17 short-term fixes
Onward into the Weeds of Billing!• Resource-based Relative Value Scale (RBRVS)
• Current Procedural Terminology (CPT)
• Relative Value Units (RVU)
• Geographic Pricing Cost Index (GPCI or “gypsy”)
• Medicare Correction Factor (CF)
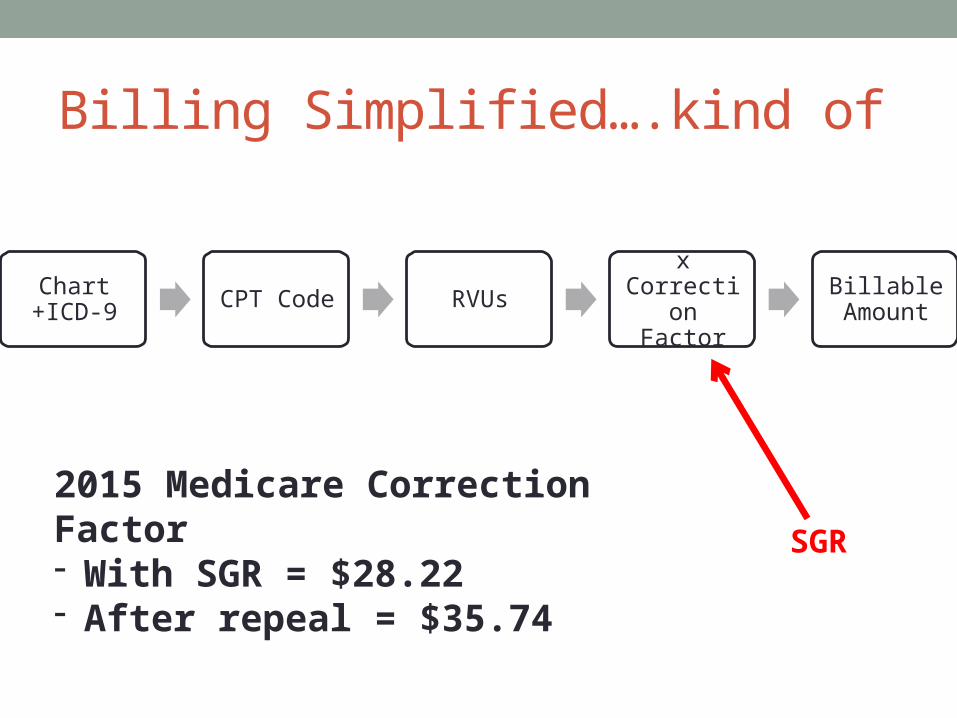
Billing Simplified….kind of
Chart +ICD-9 CPT Code RVUs
x Correction
Factor
Billable Amount
SGR
2015 Medicare Correction Factor- With SGR = $28.22- After repeal = $35.74

Where did MACRA take us?• SGR replaced with +0.5% 2015-2019, 0.0% for 2020-2025
• Replaces PQRS, VBM and EHR MU with MIPS
• CHIP funding extended 2 years (9/30/17)
• Delayed phase-out of DSH payments by 1 year (20172018)
• Premium increase for wealthier Medicare beneficiaries
• Incentive for APMs - 5% increase if 25% of patients by 2019
Merit-based Incentive Payment System (MIPS)
• Replaces:• Physician Quality Reporting System (PQRS)• Value Based Modifier (VBM)• Electronic Health Record Meaningful Use (EHR MU)
• Goal is to reward value instead of volume• Shift from Medicare fee-for-service to value-based and APMs
• Performance in 4 Categories• (1) Quality, (2) Resource Use, (3) Meaningful Use, (4) Clinical
Practice Improvement Activities• Composite score determines incentive/adjustment
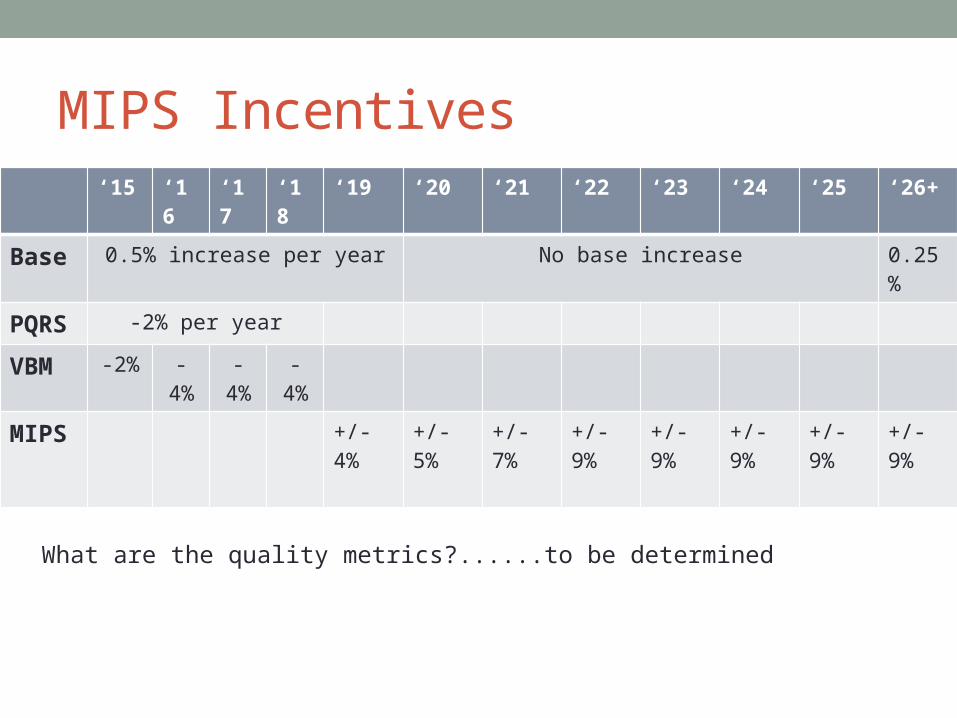
MIPS Incentives‘15 ‘16 ‘17 ‘18 ‘19 ‘20 ‘21 ‘22 ‘23 ‘24 ‘25 ‘26+
Base 0.5% increase per year No base increase 0.25%
PQRS -2% per year
VBM -2% -4% -4% -4%
MIPS +/- 4%
+/- 5%
+/- 7%
+/- 9%
+/- 9%
+/- 9%
+/- 9%
+/- 9%
What are the quality metrics?......to be determined

Opportunities for Advocacy• Legislative
• CHIP Reauthorization in 2017• DSH phase-out (particularly in states without Medicaid expansion)
• Regulatory • MIPS metrics• Role of EM in Alternative Payment Models (eg ACOs, PCMH, etc)• CPT codes, RVU assignment
KING V BURWELL

King v Burwell• Tax benefits (e.g. subsidies) should be granted for such
individuals who purchase their insurance in exchanges “established by the State.”

King v Burwell• Not a constitutional question. Question of statutory
interpretation.
• Does the language in the bill limit subsidies to states with state-run exchanges?
• SCOTUS must determine intent of writers
• Will not change Medicaid expansion.
Review the ACA and “the sit(uation)” • Individual mandate
• Expanded Medicaid to adults <65 and <133% of FPL ($15,521 in 2015)• 2012: Nat’l Fed Independent Businesses v Sebelius
• Establish insurance exchanges to serve as insurance marketplace to individuals and families• State-based, Federally-supported State-based, State partnership,
Federally-facilitated
• Create premium and cost-sharing subsidies for people at 100%-400% of FPL ($11,343 - $45,372)
Subsidies for Exchange Plans • Premium Tax Credit
• Cost-sharing Tax Credit
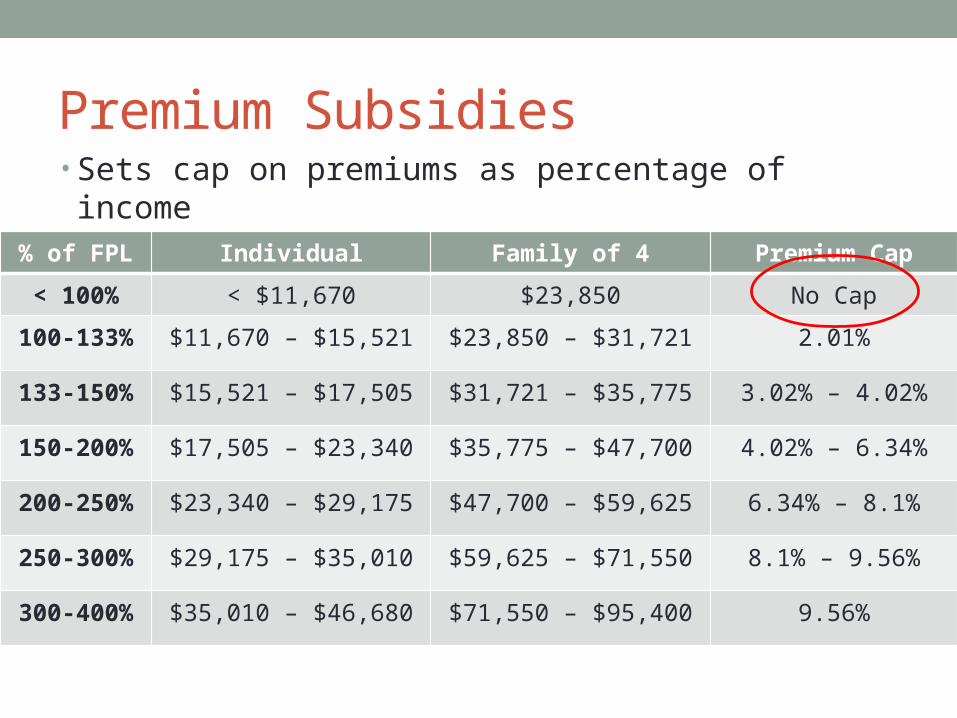
Premium Subsidies• Sets cap on premiums as percentage of income• Eligible if 100%-400% of FPL
% of FPL Individual Family of 4 Premium Cap
< 100% < $11,670 $23,850 No Cap
100-133% $11,670 – $15,521 $23,850 – $31,721 2.01%
133-150% $15,521 – $17,505 $31,721 – $35,775 3.02% – 4.02%
150-200% $17,505 – $23,340 $35,775 – $47,700 4.02% – 6.34%
200-250% $23,340 – $29,175 $47,700 – $59,625 6.34% – 8.1%
250-300% $29,175 – $35,010 $59,625 – $71,550 8.1% – 9.56%
300-400% $35,010 – $46,680 $71,550 – $95,400 9.56%
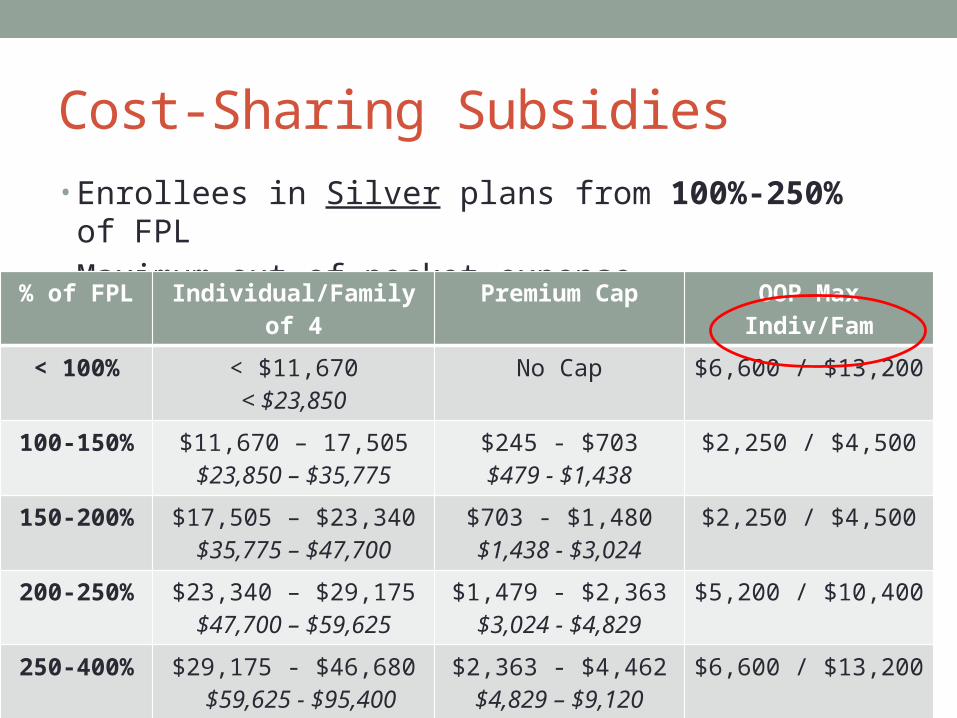
Cost-Sharing Subsidies• Enrollees in Silver plans from 100%-250% of FPL• Maximum out-of-pocket expense $6,600/$13,200
% of FPL Individual/Family of 4 Premium Cap OOP Max Indiv/Fam
< 100% < $11,670< $23,850
No Cap $6,600 / $13,200
100-150% $11,670 – 17,505$23,850 – $35,775
$245 - $703$479 - $1,438
$2,250 / $4,500
150-200% $17,505 – $23,340$35,775 – $47,700
$703 - $1,480$1,438 - $3,024
$2,250 / $4,500
200-250% $23,340 – $29,175$47,700 – $59,625
$1,479 - $2,363$3,024 - $4,829
$5,200 / $10,400
250-400% $29,175 - $46,680 $59,625 - $95,400
$2,363 - $4,462$4,829 – $9,120
$6,600 / $13,200
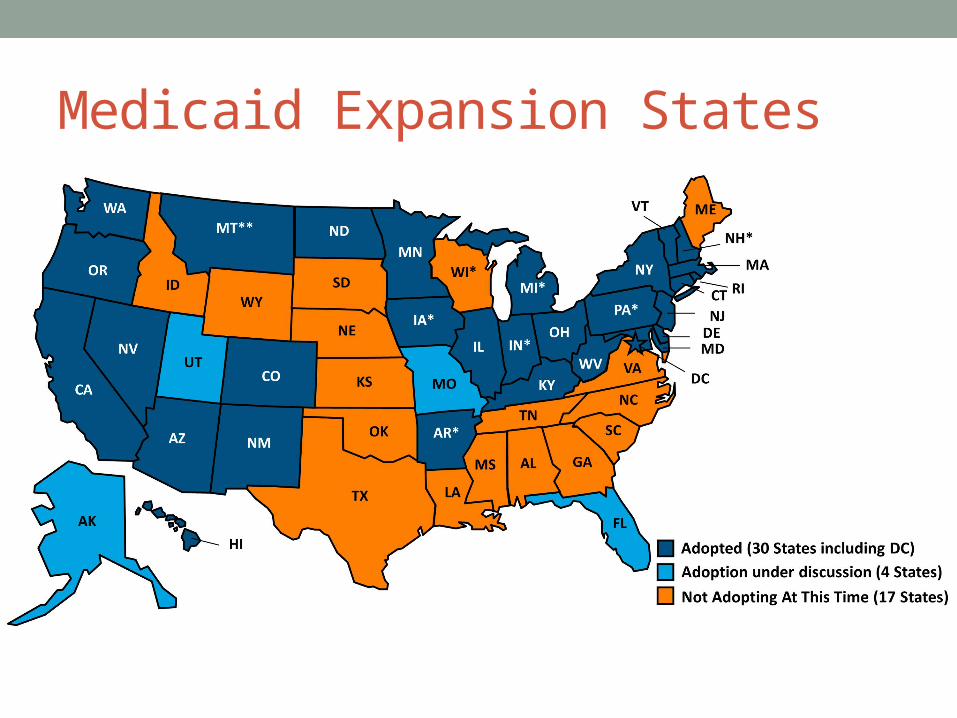
Medicaid Expansion States
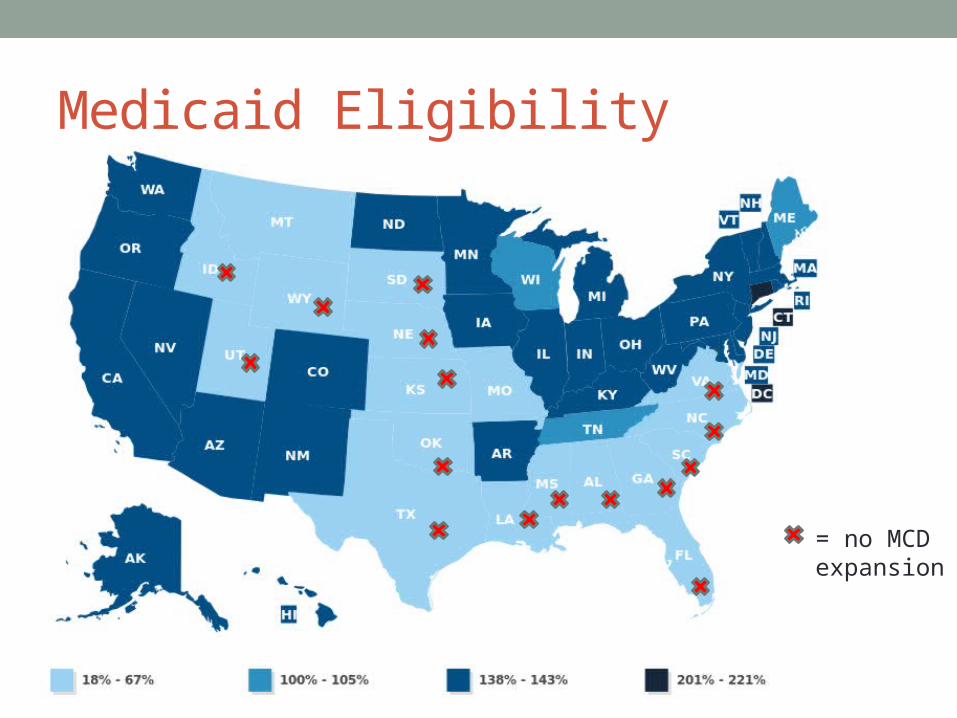
Medicaid Eligibility
= no MCD expansion
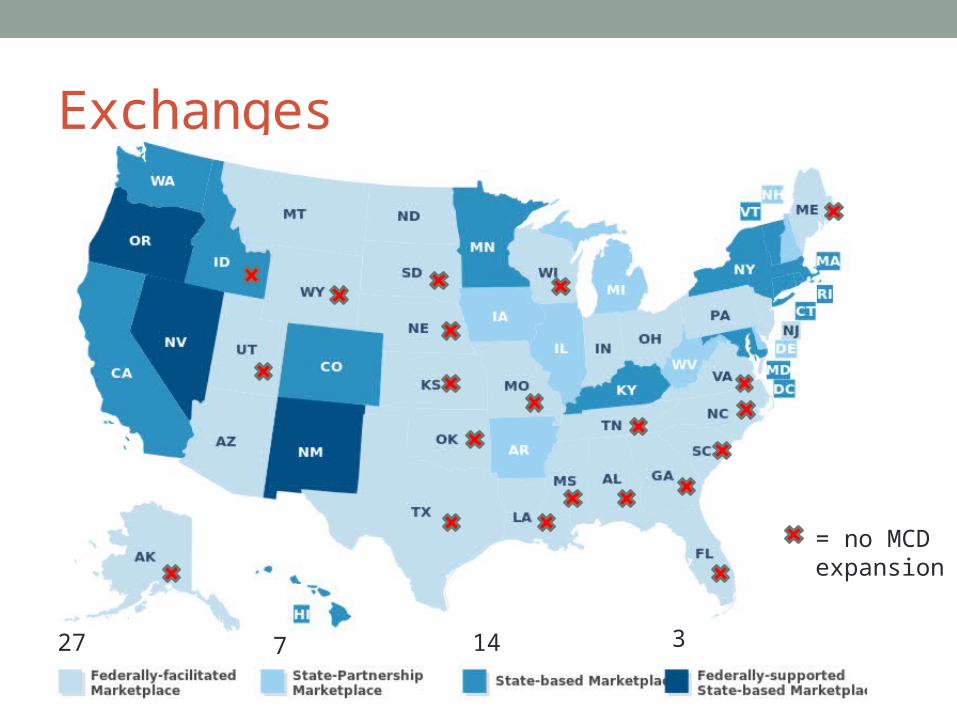
Exchanges
14 327 7
= no MCD expansion
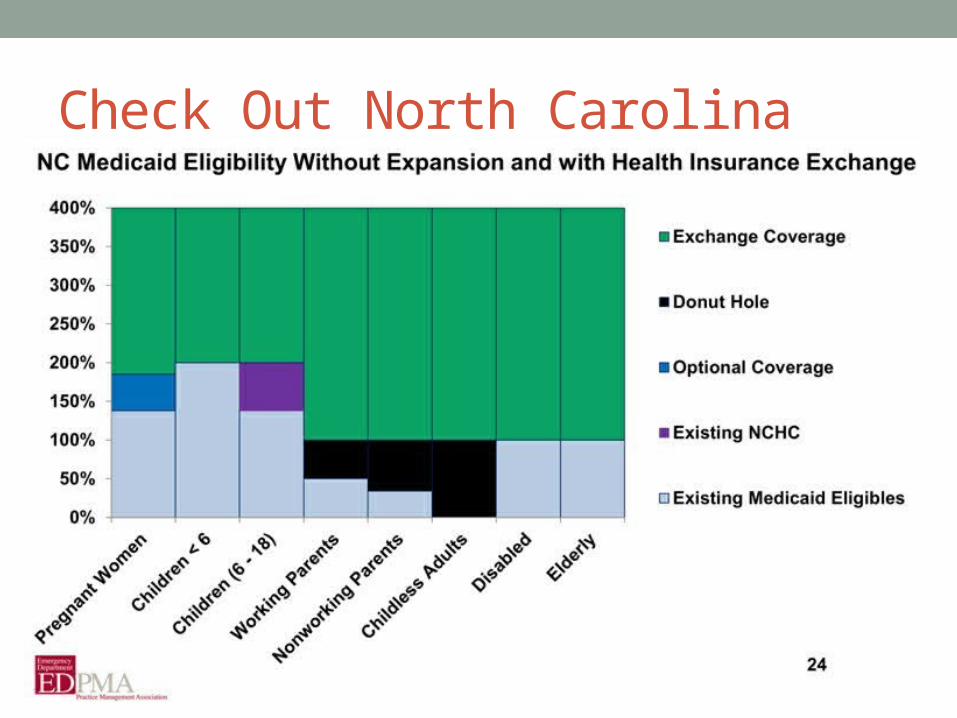
Check Out North Carolina

If King is Victorious…
14 327 7
= no MCD expansion
- Loss of affordability - Loss of individual mandate- Insurance death spiral- Two-tiered system

Opportunities for Advocacy• Legislative
• Lobby governors/legislators to establish state-run exchange• Expand Medicaid to 138% of FPL (federal funding)• Alternative short-term fix for EMTALA-related care?
Summary (in word salad format)• SGR is gone• MACRA is here• MIPS is replacing PQRS, VBM and EHR MU
• King v Burwell is important for exchange subsidies• If King wins:

What can you do? • Learn at LAC
• Join the ACEP 911 Network at www.acepadvocacy.org
• Get involved with your state ACEP chapter
• Donate to NEMPAC• Give-a-shift $120 for residents
• Join EMRA Health Policy Committee
• Follow the HPC on twitter at @EMadvocacy #EMRAadvocacy