inibitori neprilisina - aristea - performance beyond your ... canepa heartline... · cardiologia,...
TRANSCRIPT

Marco Canepa, MD, PhD
Università degli Studi di Genova
Cardiologia, Ospedale Policlinico San Martino IRCCS
INIBITORI
NEPRILISINA


ARNI: ANGIOTENSIN RECEPTOR
NEPRILYSIN INHIBITORS
ARNI
VALSARTAN
SACUBITRIL
SACUBITRILAT
Sing JSS et al. HEART 2017


PARADIGM-HF. NEJM 2014
PARADIGM-HF Primary endpoint
Ka
pla
n-M
eie
r E
sti
ma
tes
of
Cu
mu
lati
ve R
ate
s (
%)
Days After Randomization
Cardiovascular Death or HF hospitalization

PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III
INCREASED
BNP or
NT-proBNP
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

PARADIGM-HF Characteristics at baseline
PARADIGM-HF. NEJM 2014

PARADIGM-HF LVEF
Solomon S et al. PARADIGM-HF. CIRC HF 2016

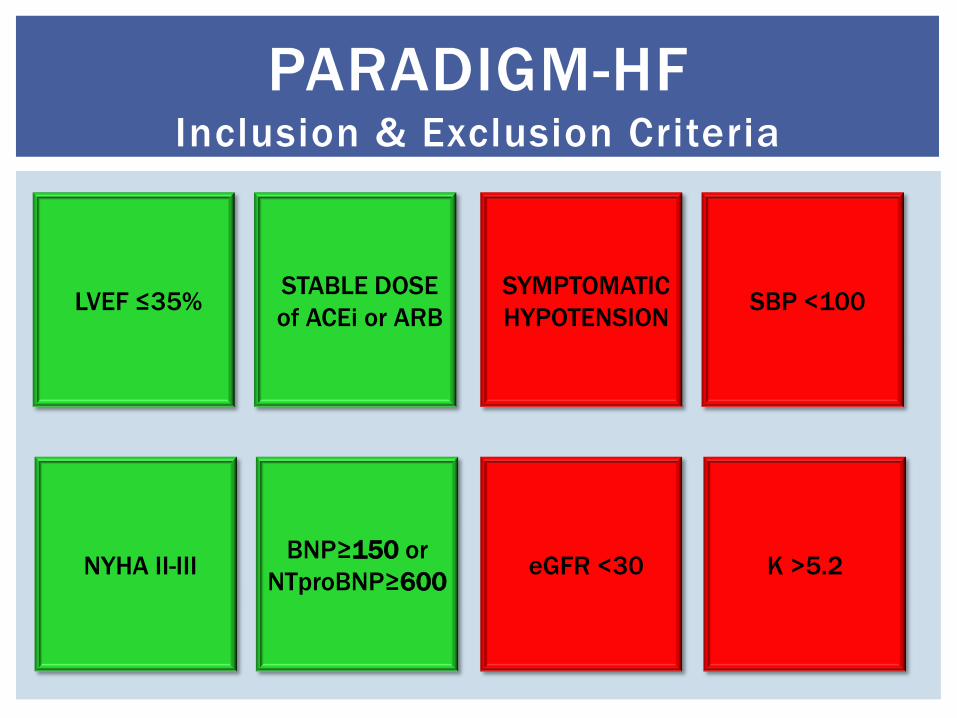
PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

PARADIGM-HF SBP trends
PARADIGM-HF. NEJM 2014

PARADIGM-HF Run-In Period & Study Period
PARADIGM-HF. NEJM 2014
N=10521 N=9419
RUN-IN PERIOD STUDY PERIOD
Desai et al. PARADIGM-HF. CIRC HEART FAIL 2016
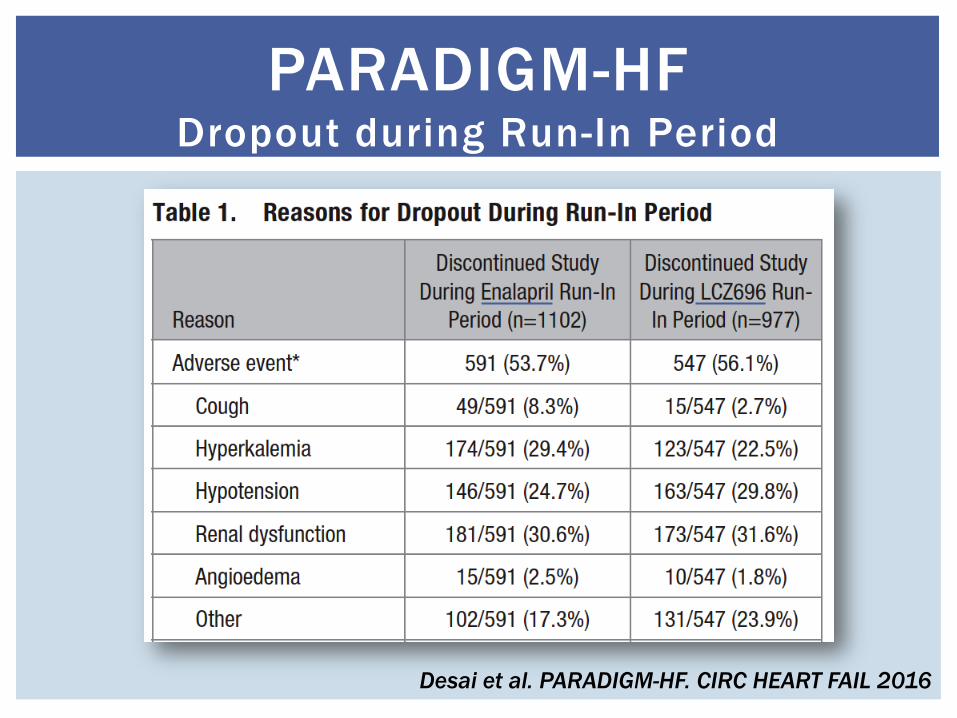
PARADIGM-HF Dropout during Run-In Period
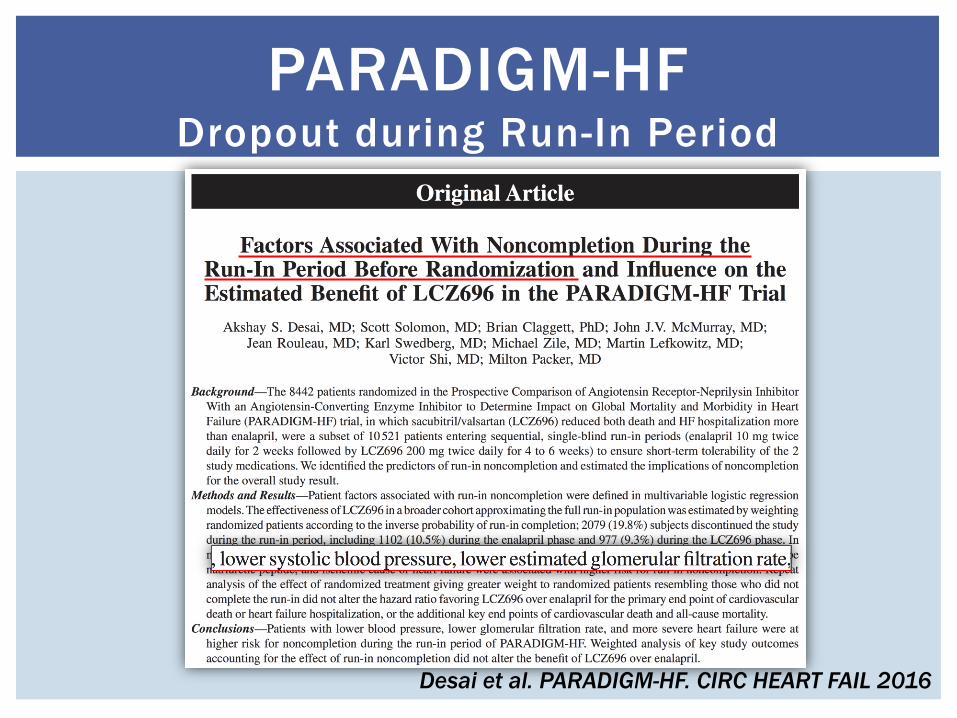
Desai et al. PARADIGM-HF. CIRC HEART FAIL 2016
PARADIGM-HF Dropout during Run-In Period

PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

PARADIGM-HF SBP trends
PARADIGM-HF. NEJM 2014

McMurray JJ et al. PARADIGM-HF. NEJM 2014
PARADIGM-HF AEs and Discontinuation during Study
Vardeny et al. PARADIGM-HF. EUR J HEART FAILURE 2016
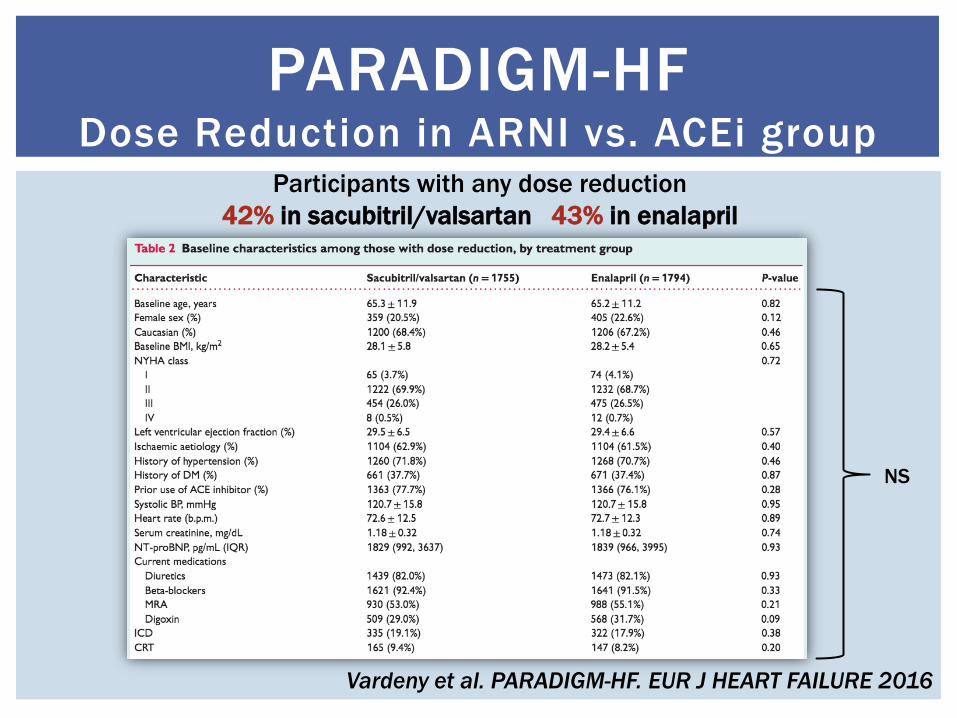
PARADIGM-HF Dose Reduction in ARNI vs. ACEi group
Participants with any dose reduction
42% in sacubitril/valsartan 43% in enalapril
NS

Vardeny et al. PARADIGM-HF. EUR J HEART FAILURE 2016
PARADIGM-HF Dose Reduction Predictors

Vardeny et al. PARADIGM-HF. EUR J HEART FAILURE 2016
PARADIGM-HF Dose Reduction & Prognosis
Cardiovascular Death or HF hospitalization

Vardeny et al. PARADIGM-HF. EUR J HEART FAILURE 2016
PARADIGM-HF Dose Reduction & Prognosis ARNI vs. ACEi
Cardiovascular Death or HF hospitalization
PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

PARADIGM-HF Minimum required pre-study daily doses
McMurray et al. PARADIGM-HF. EJHF 2013

PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35%
TARGET
STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

Pellicori P, Clark AL et al. EJHF 2017

1396 ambulatory CHF patients in UK
Pellicori P, Clark AL et al. EJHF 2017
1. LVEF≤40% at baseline
2. LVEF≤40% at fup
3. Alive at fup
4. Available at fup
5. On target dose ACEi/ARB
6. No controindications
7. Symptoms
8. NTproBNP>400
9. NTproBNP>600
Proportion of patients
eligible for ARNI

Only 28% of the 5000 HFrEF patients
in the ESC HF Long-Term Registry are
at ACEi/ARB target dose
- still up-titration
- side effects (symptomatic hypotension
and/or worsening renal function)
- no obvious reason (>30%!)
No loss of the advantage of
sacubitril–valsartan over enalapril for
morbidity and mortality in >40% of
patients in PARADIGM-HF who had
doses reduction of trial medication
during follow-up.
Rather than going to the trouble of
titrating patients to full dose
ACEi/ARB and then switching to an
ARNI, it may be appropriate to
initiate patients on the latter from
the outset.
Pellicori P, Clark AL et al. EJHF 2017

AHA/ACC HF Guidelines. Focused Update 2017

1396 ambulatory CHF patients in UK
Pellicori P, Clark AL et al. EJHF 2017
1. LVEF≤40% at baseline
2. LVEF≤40% at fup
3. Alive at fup
4. Available at fup
On target dose ACEi/ARB
5. No controindications
6. Symptoms
7. NTproBNP>400
8. NTproBNP>600
Proportion of patients
eligible for ARNI
COSTS
BENEFITS
HIGH
LOW
LOW HIGH

56 cp (bid) = 200 €
28 cp (od) = 5 € 28 cp (od) = 10 €
Cost of one-month therapy
with ARNI vs. ACEi/ARB

COSTS
BENEFITS
HIGH
LOW
LOW HIGH
King et al. JACC HF 2014


PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

“Three major regulatory authorities [the Food and Drug
Administration (FDA), the European Medicines Agency (EMA),
and the National Institute for Health and Care Excellence
(NICE)] have not suggested that initiation of sacubitril–
valsartan should be restricted to patients with an elevated NT-
proBNP. We believe this is a mistake” .
Natriuretic peptides are powerful prognostic markers . Low
values will identify patients at low risk in whom sacubitril–
valsartan is unlikely to be cost -effective. Even if the relative
reduction in risk is similar, patients at low risk of events will
have a small absolute benefit.
Natriuretic peptides
in the prescription of ARNI
Pellicori P, Clark AL et al. EJHF 2017; Van Veldhuisen et al. JACC 2013

De
ath
an
d H
F h
osp
ita
liza
tio
n
Van Veldhuisen et al. JACC 2013; AHA/ACC 2017 HF Guidelines update

“In our opinion, measuring plasma natriuretic peptides would
be a simple, effective and probably cost -effective strategy
that would reduce prescriptions of sacubitril–valsartan for
patients who had little to gain and greatly increase them in
those most l ikely to benefit . We predict that this would lead to
an overall increase in sacubitril–valsartan use but,
importantly, a greater increase in what we consider
appropriate use”.
Pellicori P, Clark AL et al. EJHF 2017; Van Veldhuisen et al. JACC 2013
Natriuretic peptides
in the prescription of ARNI

PARADIGM-HF Inclusion & Exclusion Criteria
LVEF ≤35% STABLE DOSE
of ACEi or ARB
NYHA II-III BNP≥150 or
NTproBNP≥600
SYMPTOMATIC
HYPOTENSION SBP <100
eGFR <30 K >5.2

SELECTING THE RIGHT PATIENTS
FOR ARNI YES
• HFrEF patients with LVEF≤35%
• NYHA II-III & increased BNP/NT-proBNP
• SBP>100 mmHg
• Tolerating target ACEi/ARB
MAYBE • On low-dose ACEi/ARB
• ACEi/ARB naïve
NO DATA • NYHA IV/stage D HF
• Hospitalized HF
• HFpEF
• NYHA I/asymptomatic LVH

ARNI
UPCOMING CLINICAL STUDIES
Prospective ARNI vs ACE Inhibitor Trial to
DetermIne Superiority in Reducing Heart
Failure Events After MI (PARADISE-MI)
ARNI in Asymptomatic Patients With
Elevated Natriuretic Peptide and Elevated
Left Atrial Volume Index eLEvation
(PARABLE)
Efficacy and Safety of LCZ696 Compared to
Valsartan, on Morbidity and Mortality in
Heart Failure Patients With Preserved
Ejection Fraction (PARAGON-HF)
comParIson Of Sacubitril/valsartaN Versus
Enalapril on Effect on ntpRo-bnp in Patients
Stabilized From an Acute Heart Failure
Episode (PIONEER-HF)
A Randomized, Double-blind Controlled
Study Comparing LCZ696 to Medical
Therapy for Comorbidities in HFpEF Patients
(PARALLAX)
Comparison of Pre- and Post-discharge
Initiation of LCZ696 Therapy in HFrEF
Patients After an Acute Decompensation
Event (TRANSITION)
www.clinicaltrials.gov


TITRATION CONSERVATIVE vs. CONDENSED initiation
Senni et al. TITRATION. EUR J HEART FAILURE 2016
CONDENSED
CONSERVATIVE

Jhund PS et al. PARADIGM-HF. EUR HEART J 2015
ARNI Efficacy According to Age

Shen et al. NEJM 2017

THE BUILDING BLOCKS
OF HFrEF THERAPY

TODAY PROGNOSIS
OF CHRONIC HFrEF
1990 1995 2000 2005 2010 2015 TODAY
TOTAL MORTALITY
SUDDEN DEATH
COMORBIDITIES
MO
RTA
LIT
Y/Y
EA
R
5%
10%