inhibition of pai-1 via pai-039 improves dermal wound...
TRANSCRIPT

Irena A. Rebalka, Matthew J. Raleigh, Donna M. D’Souza, Samantha K. Coleman,Alexandra N. Rebalka, and Thomas J. Hawke
Inhibition of PAI-1 Via PAI-039Improves Dermal Wound Closurein DiabetesDiabetes 2015;64:2593–2602 | DOI: 10.2337/db14-1174
Diabetes impairs the ability to heal cutaneous wounds,leading to hospitalization, amputations, and death.Patients with diabetes experience elevated levels ofplasminogen activator inhibitor 1 (PAI-1), regardless oftheir glycemic control. It has been demonstrated thatPAI-1–deficient mice exhibit improved cutaneous woundhealing, and that PAI-1 inhibition improves skeletal mus-cle repair in mice with type 1 diabetes mellitus, leading usto hypothesize that pharmacologically mediated reduc-tions in PAI-1 using PAI-039 would normalize cutaneouswound healing in streptozotocin (STZ)-induced diabetic(STZ-diabetic) mice. To simulate the human condition ofvariations in wound care, wounds were aggravated orminimally handled postinjury. Following cutaneous injury,PAI-039 was orally administered twice daily for 10 days.Compared with nondiabetic mice, wounds in STZ-diabetic mice healed more slowly. Wound site aggra-vation exacerbated this deficit. PAI-1 inhibition had noeffect on dermal collagen levels or wound bed size. PAI-039 treatment failed to improve angiogenesis in thewounds of STZ-diabetic mice and blunted angiogenesisin the wounds of nondiabetic mice. Importantly, PAI-039treatment significantly improved epidermal cellular mi-gration and wound re-epithelialization compared withvehicle-treated STZ-diabetic mice. These findings sup-port the use of PAI-039 as a novel therapeutic agent toimprove diabetic wound closure and demonstrate theprimary mechanism of its action to be related toepidermal closure.
Diabetes is a family of metabolic disorders characterizedby elevated blood glucose levels and impaired insulinsignaling. Currently, it is estimated that .29 million
individuals in the U.S. and .347 million individualsworldwide have diabetes (1,2). By 2030, the worldwideprevalence of diabetes will approach 8% of the world’spopulation (3). Individuals with diabetes are at a signifi-cantly elevated risk for a number of comorbidities, includ-ing nephropathy, neuropathy, peripheral artery disease,stroke, and retinopathy. Another major complication asso-ciated with diabetes is nonhealing dermal wounds. Thesewounds are especially common in the lower distal extrem-ities, namely, diabetic foot ulcerations. Foot ulcers are theleading cause of hospital admissions for persons with di-abetes, are estimated to occur in 15% of all patients withdiabetes, and precede 85% of all diabetic lower leg ampu-tations (4,5). In the U.S., the average cost of treating onesingle infected diabetic foot ulcer is $17,000, and amputa-tion costs approach $45,000 per amputation (5,6). Ap-proximately 72,000 nontraumatic diabetic lower-limbamputations are performed in North America each year(5). Despite significant medical advancements in the treat-ment of diabetic wounds, these statistics have not falteredsignificantly in the past 30 years, highlighting the neces-sity to develop effective strategies to expedite diabeticwound healing in order to avoid amputation (6).
Wound healing in individuals without diabetes isa multifactorial process that follows a basic series ofoverlapping processes: 1) hemostasis (clotting); 2) inflam-mation (clean out debris and bacteria); 3) proliferation (re-build wound site); and 4) maturation (regeneration ofdamaged tissue and vessels). In patients with diabetes, itis reported (4) that there are .100 known physiologicalfactors that contribute to the deficits in wound healing. Ingeneral, the impairments in diabetic wound healing appearto be concentrated in the inflammatory and proliferative
Department of Pathology and Molecular Medicine, McMaster University, Hamilton,Ontario, Canada
Corresponding author: Thomas J. Hawke, [email protected].
Received 30 July 2014 and accepted 2 March 2015.
This article contains Supplementary Data online at http://diabetes.diabetesjournals.org/lookup/suppl/doi:10.2337/db14-1174/-/DC1.
© 2015 by the American Diabetes Association. Readers may use this article aslong as the work is properly cited, the use is educational and not for profit, andthe work is not altered.
Diabetes Volume 64, July 2015 2593
COMPLIC
ATIO
NS

phases, and include the prolonged presence of neutrophilsand macrophages, an impaired angiogenic response, de-creased migration and proliferation of fibroblasts and ker-atinocytes, decreased quantity/quality of granulation tissue,and altered growth factor/cytokine expression (4).
Though diabetes is characterized by altered bloodglucose regulation and dysregulation of insulin (and/orinsulin signaling), numerous other endocrine factors arealso known to be differentially regulated. One hormone ofparticular interest is plasminogen activator inhibitor 1(PAI-1), a member of the serine protease inhibitor family.PAI-1 has actions that are largely determined through twodistinct, yet interrelated, cascades. First, PAI-1 is involvedin fibrinolysis via the inhibition of plasminogen activators;and second, in cell migration, survival, and proliferation,through binding to urokinase plasminogen activator, theurokinase plasminogen activator receptor vitronectin, andlow-density lipoprotein-related protein. Plasma PAI-1 levelsare significantly elevated in individuals with diabetes, obe-sity, and insulin resistance, and have been implicated inthe development of vulnerable atherosclerotic plaquesand nephropathy (7–9).
Based on the work of Chan et al. (10), who demonstratedthat PAI-1–deficient mice display accelerated wound heal-ing, we hypothesized that elevations in PAI-1 levels werecontributing to the impairments in dermal wound healingin diabetes mellitus. Furthermore, we hypothesized thatpharmacologically decreasing PAI-1 levels may serve asa useful therapeutic strategy to improve wound healing indiabetes mellitus. The results of the present investigationdemonstrate that PAI-1 inhibition significantly improvesepidermal closure in diabetic wounds, a process that is crit-ical for the formation of a protective barrier atop the woundsite, preventing bacterial entry and infection, and allowingthe expedition of the healing process. These findings sup-port the use of PAI-1 inhibitors as a novel therapeutic agentto improve diabetic cutaneous wound repair.
RESEARCH DESIGN AND METHODS
Animal HandlingMale C57BL/6J mice (The Jackson Laboratory, BarHarbor, ME) were provided enrichment material, chow(OpenSource Diets D12450K; Research Diets, NewBrunswick, NJ), and water ad libitum. Animal housingconditions were maintained at 21°C, 50% humidity, anda 12-h/12-h light-dark cycle. Experimentation wasapproved by the McMaster University Animal ResearchEthics Board, in accordance with the guidelines of theCanadian Council for Animal Care.
At 10–12 weeks of age, animals were randomlyassigned to streptozotocin (STZ)-induced diabetic (STZ-diabetic) or control (wild-type [WT]) groups. Cohortswere then subdivided into groups with aggravatedwounds and minimally handled wounds.
Aggravated wounds: STZ-diabetic animals received threedaily injections of STZ anomer (Streptozocin; Sigma-
Aldrich, Oakville, ON, Canada) dissolved in sterile salineat 50 mg/kg, and one final injection at 200 mg/kg.
Minimally handled wounds: STZ (Calbiochem, Gibbstown,NJ) was dissolved in sodium citrate buffer, pH 4.5, andone injection at 150 mg/kg was administered. Nosignificant differences were observed between groups inbody mass (P = 0.49) or blood glucose values as a result ofthe two distinct STZ protocols (Supplementary Fig. 1).
Six weeks after diabetic onset (blood glucose .14mmol/L), punch biopsies were conducted. Hair removaltook place 2 days prior to punch biopsy. On the day ofthe biopsy, all mice were anesthetized via isoflurane.After surgical preparation (a sequential application of0.5% proviodine scrub, 70% ethanol, and 1% proviodinesolution), each animal received two 6-mm-diameter full-thickness wounds via punch biopsy (Miltex, York, PA) intheir dorsal scapular region. Oral analgesic (Tempra;Bristol-Myers Squibb Canada, Montreal, QC, Canada)was administered 2 h prior to biopsy, and topical anal-gesic (Emla Cream; AstraZeneca, Mississauga, ON, Can-ada) was applied prior to surgical preparation. Oralanalgesic was also provided to all animals every 4–6 hfor the first 48 h postbiopsy.
PAI-1, PAI-039 Treatment, and Wound Care. Changes inPAI-1 levels were confirmed using the mRNA expressionlevels observed in cardiac tissue (11). Briefly, cDNA wasprepared from cardiac tissue of WT and STZ-diabeticmice. Semiquantitative PCR was performed usingsequence-specific primers for PAI-1 (ACGTTGTGGAACTGCCCTAC and GCCAGGGTTGCACTAAACAT) and b-2 mi-croglobulin (ATCCAAATGCTGAAGAACGGG and CATGCTTAACTCTGCAGGCG), and the findings were quantifiedusing CareStream Imager software. Consistent with thefindings of others (11), PAI-1 levels were significantly ele-vated in STZ-diabetic mice (0.55 6 0.03 WT vs. 0.76 60.03 STZ, P , 0.01).
To determine whether elevations in PAI-1 levels werecontributing to impaired cutaneous wound repair, PAI-039 (Axon Medchem, Groningen, the Netherlands), anorally effective PAI-1 inhibitor, was administered. STZ-diabetic and WT mice were randomly assigned to receivetreatment with vehicle (V) (0.5% methylcellulose and 2%Tween-80 in sterile H2O) or PAI-039 (2 mg/kg PAI-039in V) at both 11:00 A.M. and 3:00 P.M. daily, beginning onthe day of wounding and terminating on the day of har-vest, 10 days postbiopsy. This PAI-039 administrationprotocol has previously been demonstrated to reducePAI-1 levels to those of nondiabetic mice (12).
Animals received one of the following two variations ofwound care: aggravation or minimal handling. In order tomodel improper wound care, wounds were manuallygrasped and held during treatment administration viaoral gavage, twice daily. In order to model the proper careof diabetic wounds and remove wound site aggravation(13), treatment was combined with sugar-free cherry-
2594 PAI-1 Inhibition and Dermal Wound Closure Diabetes Volume 64, July 2015

flavored Tempra (Bristol-Myers Squibb Canada), a solutionthat allowed simple oral administration via dropper with-out handling of the dorsal scapular wounds.
Tissue Collection. Ten days postbiopsy, animals wereeuthanized via cervical dislocation; and wounds wereisolated, bisected, fixed in 4% paraformaldehyde, pro-cessed (TP 1020 Tissue Processor; Leica Biosystems,Wetzlar, Germany), and paraffin embedded. All macro-scopic images were taken with a Powershot SX 200 IXCamera (Canon, Tokyo, Japan) at a standardized heightand magnification. All microscopic images were obtainedwith a 90i Eclipse Microscope (Nikon, Inc., Melville, NY).All analysis was completed using NIS Elements AnalysisSoftware (Nikon, Inc.).
Macroscopic, Histochemical, and ImmunofluorescentAnalysis
Macroscopic Analysis. Healing was assessed by imagingand quantifying eschar size throughout the 10-day healingperiod. Animals were briefly anesthetized via isoflurane,and images were taken at a standardized height at 0, 2, 4,6, 8, and 10 days postwounding. To obtain the percentdecrease in eschar size at each time point, the eschar areawas measured and transformed via Formula A (the highestand lowest values were removed).
�AxA0
31001
�¼ % original eschar size ðAÞ
where Ax represents the eschar area measurement takenat day 2, 4, 6, 8, or 10, and A0 represents the wound areameasurement at day 0.Histology. The 6-mm paraffin sections were air driedovernight, deparaffinized, and rehydrated. Hematoxylin-eosin (H-E) and Masson trichrome staining was per-formed using standard protocols. H-E–stained sectionstaken from the center of the excised wounds were ana-lyzed. If the leading epidermal edges were fully fused,wounds were considered to be fully closed. The numberof fully closed wounds per group was tallied and graphedaccordingly. Masson trichrome–stained sections takenfrom the center of the excised wounds were used to de-termine epidermal thickness differences between woundedges and unwounded tissue (Formula B, below), thetotal presence of collagen in the wound bed dermis (sig-nal threshold settings were used as the detectionmethod), and the dermal depth of the wound bed (sixevenly spaced depth measurements provided an averagewound depth):
E8 2U4 ¼ Difference in epidermal thickness ðBÞ
Formula B represents the difference in thickness betweenthe wound edges and the unwounded epidermis. Theaverage of four cross-sectional measurements of un-wounded epidermis (U4) was subtracted from the average
of eight epidermal cross-sectional measurements from thewound edges (E8; four measurements were made on eachside of the wound).Immunofluorescent Staining. The 6-mm sections were airdried overnight, deparaffinized, and rehydrated. Heat-mediated antigen retrieval of sections took place in citratebuffer (pH 6) at 65°C for 30 min.CD206 and NOS2/CD86 Staining. Sections were incu-bated in 0.2% Triton X-100 for 30 min, 5% normal goatserum for 40 min, and CD206 antibody (1:2,500)(Abcam, Cambridge, MA), or CD86 and NOS2 antibody(1:50 each) (Santa Cruz Biotechnology, Dallas, TX) for2 h at room temperature. To visualize CD206, sectionswere incubated in goat-anti-rabbit Alexa Fluor 488(1:250) (Abcam) for 60 min. To visualize NOS2 andCD86, sections were incubated in goat-anti-rabbit AlexaFluor 594 or goat-anti-mouse Alexa Fluor 488, respec-tively (1:250) (Abcam) for 60 min. DAPI (1:10,000) wasused to stain and identify nuclei. Analysis included thedetermination of CD206-, NOS2-, and CD86-positiveareas via manual quantification. If a macrophagestained via the CD86/NOS2 costain produced a posi-tive signal for both antibodies, it was classified as anM1 macrophage; however, if a macrophage stainedpositive only for CD86, it was classified as an M2bmacrophage.CD31, Collagen I, and Collagen III Staining. Sectionswere incubated with CD31 antibody (1:50), anti-collagen Iantibody (1:200), or anti-collagen III antibody (1:500)(Abcam) for 1 h at 37°C, and biotinylated anti-rabbit IgG(1:1,000) (Vector Laboratories, Burlingame, CA) for 40min; and were counterstained with H-E. Analysis includedthe determination of CD31-, collagen I-, or collagen III-positive areas using signal threshold settings as the de-tection method.
StatisticsAll statistical analyses were performed using Prism 6(GraphPad Software, La Jolla, CA). For all analyses, apartfrom the analysis of epidermal closure, statistical signif-icance was determined using a two-way ANOVA followedby Tukey multiple-comparison post hoc test. Statisticalsignificance for the analysis of epidermal closure wasdetermined using a Pearson x2 test. Statistical significancewas defined as P # 0.05.
RESULTS
Eschar SizeFigure 1 highlights improvements in eschar size from theday of wounding (day 0) to the day of harvest (day 10).Significant differences in the eschar size of aggravatedwounds (Fig. 1A and C) between groups at 10 days post-wounding was noted. Significant differences in the per-cent eschar area between groups at days 2, 4, 6, and 8were revealed in minimally handled wounds (Fig. 1B andD). Wound aggravation delayed reductions in eschar sizeregardless of treatment (Fig. 1A and C). The coupling of
diabetes.diabetesjournals.org Rebalka and Associates 2595
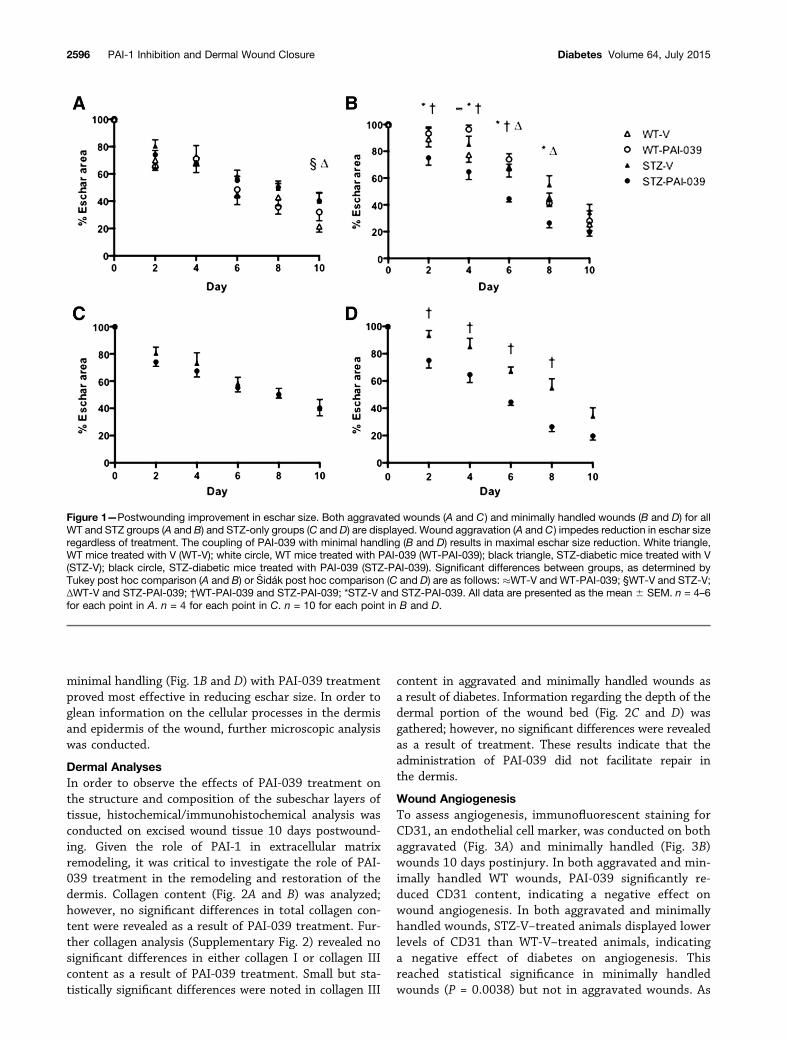
minimal handling (Fig. 1B and D) with PAI-039 treatmentproved most effective in reducing eschar size. In order toglean information on the cellular processes in the dermisand epidermis of the wound, further microscopic analysiswas conducted.
Dermal AnalysesIn order to observe the effects of PAI-039 treatment onthe structure and composition of the subeschar layers oftissue, histochemical/immunohistochemical analysis wasconducted on excised wound tissue 10 days postwound-ing. Given the role of PAI-1 in extracellular matrixremodeling, it was critical to investigate the role of PAI-039 treatment in the remodeling and restoration of thedermis. Collagen content (Fig. 2A and B) was analyzed;however, no significant differences in total collagen con-tent were revealed as a result of PAI-039 treatment. Fur-ther collagen analysis (Supplementary Fig. 2) revealed nosignificant differences in either collagen I or collagen IIIcontent as a result of PAI-039 treatment. Small but sta-tistically significant differences were noted in collagen III
content in aggravated and minimally handled wounds asa result of diabetes. Information regarding the depth of thedermal portion of the wound bed (Fig. 2C and D) wasgathered; however, no significant differences were revealedas a result of treatment. These results indicate that theadministration of PAI-039 did not facilitate repair inthe dermis.
Wound AngiogenesisTo assess angiogenesis, immunofluorescent staining forCD31, an endothelial cell marker, was conducted on bothaggravated (Fig. 3A) and minimally handled (Fig. 3B)wounds 10 days postinjury. In both aggravated and min-imally handled WT wounds, PAI-039 significantly re-duced CD31 content, indicating a negative effect onwound angiogenesis. In both aggravated and minimallyhandled wounds, STZ-V–treated animals displayed lowerlevels of CD31 than WT-V–treated animals, indicatinga negative effect of diabetes on angiogenesis. Thisreached statistical significance in minimally handledwounds (P = 0.0038) but not in aggravated wounds. As
Figure 1—Postwounding improvement in eschar size. Both aggravated wounds (A and C) and minimally handled wounds (B and D) for allWT and STZ groups (A and B) and STZ-only groups (C and D) are displayed. Wound aggravation (A and C ) impedes reduction in eschar sizeregardless of treatment. The coupling of PAI-039 with minimal handling (B and D) results in maximal eschar size reduction. White triangle,WT mice treated with V (WT-V); white circle, WT mice treated with PAI-039 (WT-PAI-039); black triangle, STZ-diabetic mice treated with V(STZ-V); black circle, STZ-diabetic mice treated with PAI-039 (STZ-PAI-039). Significant differences between groups, as determined byTukey post hoc comparison (A and B) or �Sidák post hoc comparison (C and D) are as follows: �WT-V and WT-PAI-039; §WT-V and STZ-V;ΔWT-V and STZ-PAI-039; †WT-PAI-039 and STZ-PAI-039; *STZ-V and STZ-PAI-039. All data are presented as the mean 6 SEM. n = 4–6for each point in A. n = 4 for each point in C. n = 10 for each point in B and D.
2596 PAI-1 Inhibition and Dermal Wound Closure Diabetes Volume 64, July 2015
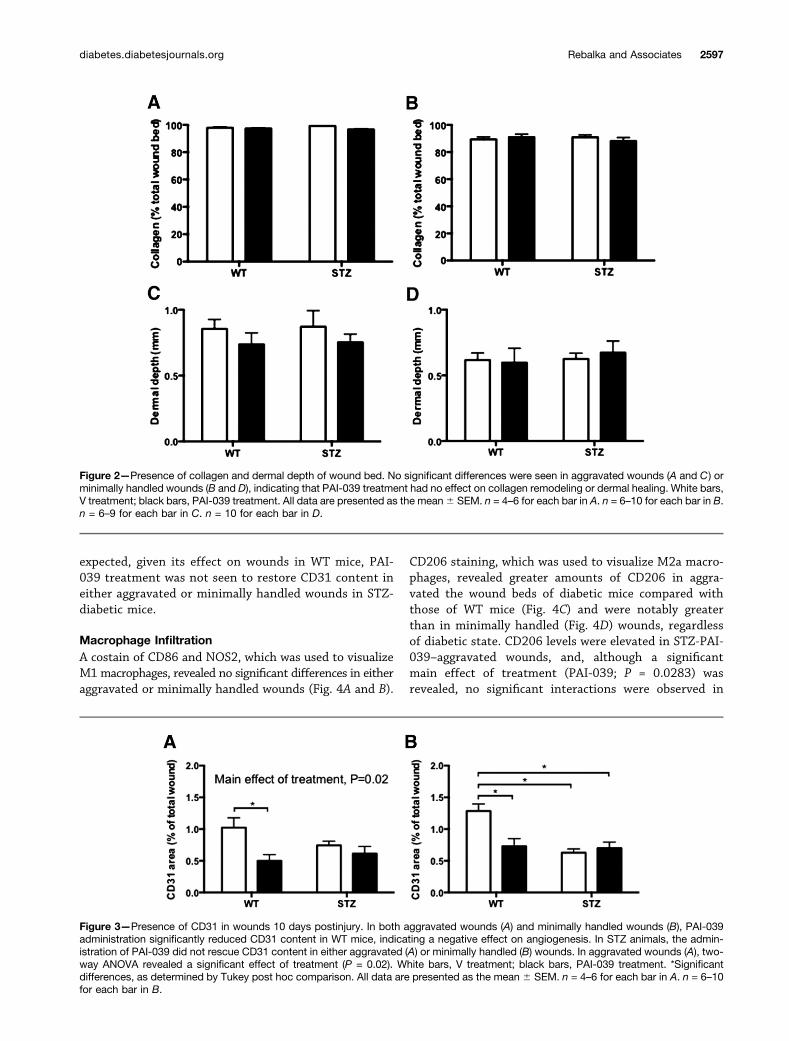
expected, given its effect on wounds in WT mice, PAI-039 treatment was not seen to restore CD31 content ineither aggravated or minimally handled wounds in STZ-diabetic mice.
Macrophage InfiltrationA costain of CD86 and NOS2, which was used to visualizeM1 macrophages, revealed no significant differences in eitheraggravated or minimally handled wounds (Fig. 4A and B).
CD206 staining, which was used to visualize M2a macro-phages, revealed greater amounts of CD206 in aggra-vated the wound beds of diabetic mice compared withthose of WT mice (Fig. 4C) and were notably greaterthan in minimally handled (Fig. 4D) wounds, regardlessof diabetic state. CD206 levels were elevated in STZ-PAI-039–aggravated wounds, and, although a significantmain effect of treatment (PAI-039; P = 0.0283) wasrevealed, no significant interactions were observed in
Figure 2—Presence of collagen and dermal depth of wound bed. No significant differences were seen in aggravated wounds (A and C) orminimally handled wounds (B and D), indicating that PAI-039 treatment had no effect on collagen remodeling or dermal healing. White bars,V treatment; black bars, PAI-039 treatment. All data are presented as the mean6 SEM. n = 4–6 for each bar in A. n = 6–10 for each bar in B.n = 6–9 for each bar in C. n = 10 for each bar in D.
Figure 3—Presence of CD31 in wounds 10 days postinjury. In both aggravated wounds (A) and minimally handled wounds (B), PAI-039administration significantly reduced CD31 content in WT mice, indicating a negative effect on angiogenesis. In STZ animals, the admin-istration of PAI-039 did not rescue CD31 content in either aggravated (A) or minimally handled (B) wounds. In aggravated wounds (A), two-way ANOVA revealed a significant effect of treatment (P = 0.02). White bars, V treatment; black bars, PAI-039 treatment. *Significantdifferences, as determined by Tukey post hoc comparison. All data are presented as the mean 6 SEM. n = 4–6 for each bar in A. n = 6–10for each bar in B.
diabetes.diabetesjournals.org Rebalka and Associates 2597
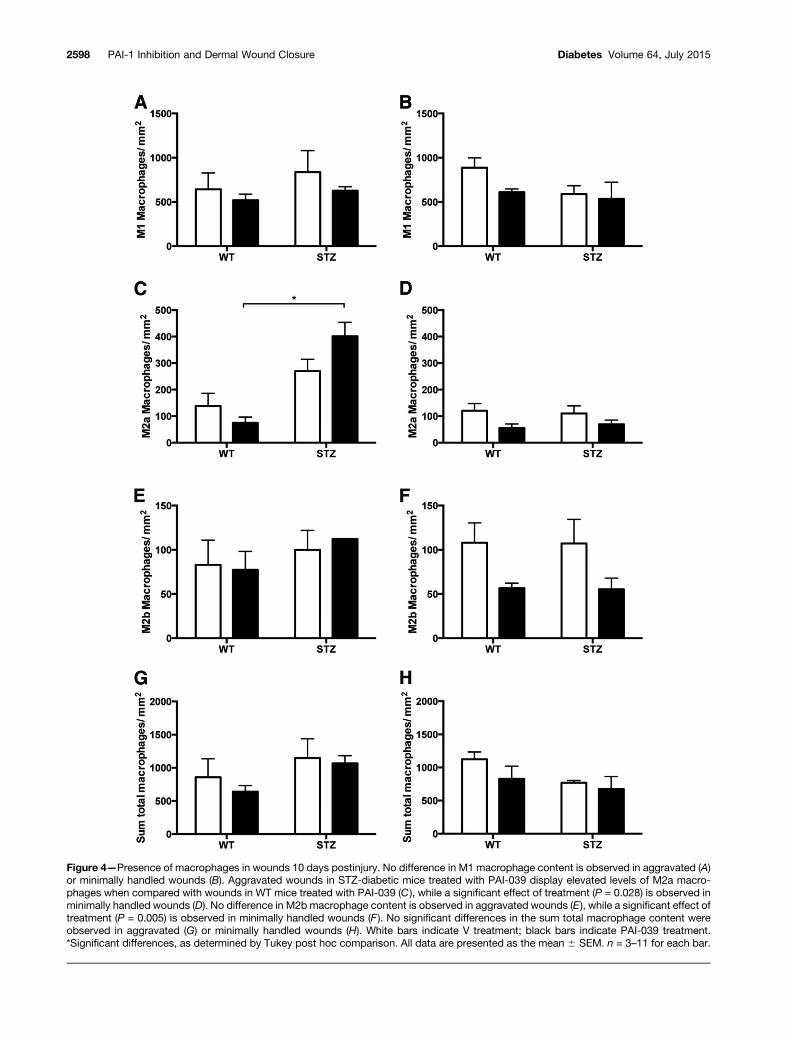
Figure 4—Presence of macrophages in wounds 10 days postinjury. No difference in M1 macrophage content is observed in aggravated (A)or minimally handled wounds (B). Aggravated wounds in STZ-diabetic mice treated with PAI-039 display elevated levels of M2a macro-phages when compared with wounds in WT mice treated with PAI-039 (C ), while a significant effect of treatment (P = 0.028) is observed inminimally handled wounds (D). No difference in M2b macrophage content is observed in aggravated wounds (E), while a significant effect oftreatment (P = 0.005) is observed in minimally handled wounds (F ). No significant differences in the sum total macrophage content wereobserved in aggravated (G) or minimally handled wounds (H). White bars indicate V treatment; black bars indicate PAI-039 treatment.*Significant differences, as determined by Tukey post hoc comparison. All data are presented as the mean 6 SEM. n = 3–11 for each bar.
2598 PAI-1 Inhibition and Dermal Wound Closure Diabetes Volume 64, July 2015
minimally handled wounds (Fig. 4D). CD86, which wasused to visualize M2b macrophages, revealed no significantdifferences in aggravated wounds (Fig. 4E), and, althougha significant main effect of PAI-039 (P = 0.0049) wasrevealed, no significant interactions were observed in min-imally handled wounds (Fig. 4F). A sum total of all afore-mentioned macrophage quantification was calculated(M1 + M2a + M2b), and no significant differences betweengroups were found (Fig. 4G and H). In an effort to identifydifferences between groups with aggravated and minimallyhandled wounds in terms of the total number of macro-phages, we undertook a series of unpaired t tests. While nodifferences between WT groups were noted, this analysisrevealed wound aggravation to exacerbate the presence ofmacrophages, namely, as a significant increase in the sumtotal macrophage content in aggravated wounds in bothSTZ-diabetic mice and STZ-diabetic mice treated with PAI-039 (P = 0.01 and P = 0.05, respectively) compared withminimally handled wounds.
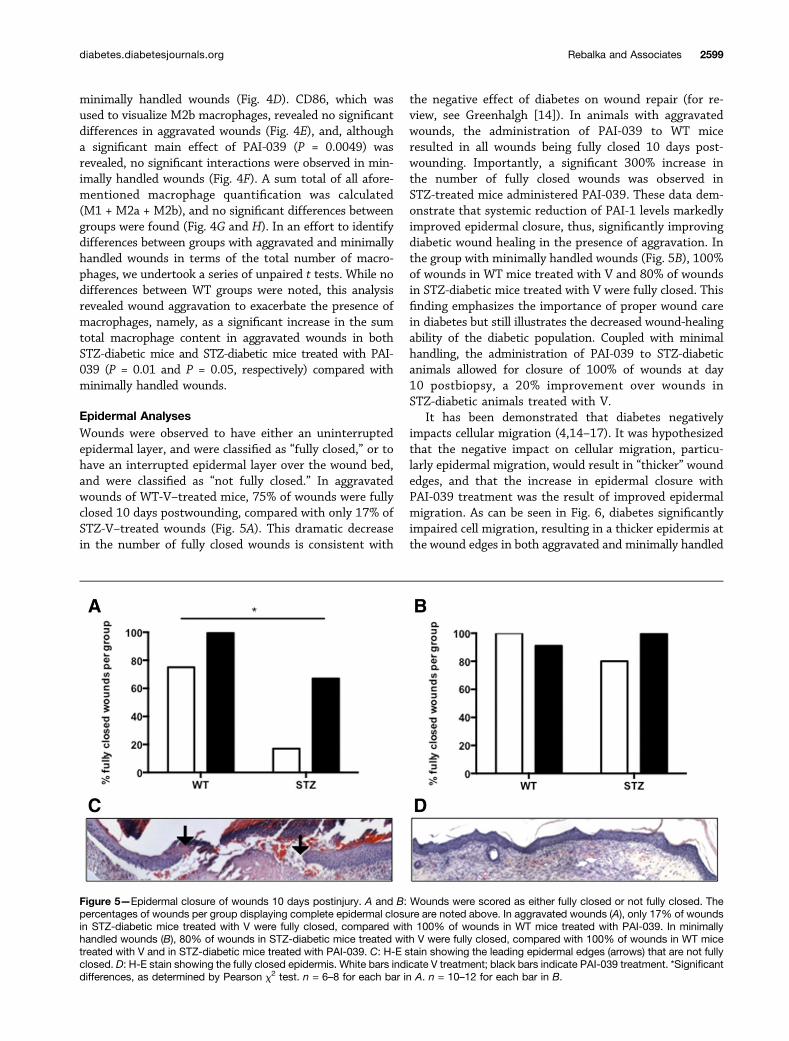
Epidermal AnalysesWounds were observed to have either an uninterruptedepidermal layer, and were classified as “fully closed,” or tohave an interrupted epidermal layer over the wound bed,and were classified as “not fully closed.” In aggravatedwounds of WT-V–treated mice, 75% of wounds were fullyclosed 10 days postwounding, compared with only 17% ofSTZ-V–treated wounds (Fig. 5A). This dramatic decreasein the number of fully closed wounds is consistent with
the negative effect of diabetes on wound repair (for re-view, see Greenhalgh [14]). In animals with aggravatedwounds, the administration of PAI-039 to WT miceresulted in all wounds being fully closed 10 days post-wounding. Importantly, a significant 300% increase inthe number of fully closed wounds was observed inSTZ-treated mice administered PAI-039. These data dem-onstrate that systemic reduction of PAI-1 levels markedlyimproved epidermal closure, thus, significantly improvingdiabetic wound healing in the presence of aggravation. Inthe group with minimally handled wounds (Fig. 5B), 100%of wounds in WT mice treated with V and 80% of woundsin STZ-diabetic mice treated with V were fully closed. Thisfinding emphasizes the importance of proper wound carein diabetes but still illustrates the decreased wound-healingability of the diabetic population. Coupled with minimalhandling, the administration of PAI-039 to STZ-diabeticanimals allowed for closure of 100% of wounds at day10 postbiopsy, a 20% improvement over wounds inSTZ-diabetic animals treated with V.
It has been demonstrated that diabetes negativelyimpacts cellular migration (4,14–17). It was hypothesizedthat the negative impact on cellular migration, particu-larly epidermal migration, would result in “thicker” woundedges, and that the increase in epidermal closure withPAI-039 treatment was the result of improved epidermalmigration. As can be seen in Fig. 6, diabetes significantlyimpaired cell migration, resulting in a thicker epidermis atthe wound edges in both aggravated and minimally handled
Figure 5—Epidermal closure of wounds 10 days postinjury. A and B: Wounds were scored as either fully closed or not fully closed. Thepercentages of wounds per group displaying complete epidermal closure are noted above. In aggravated wounds (A), only 17% of woundsin STZ-diabetic mice treated with V were fully closed, compared with 100% of wounds in WT mice treated with PAI-039. In minimallyhandled wounds (B), 80% of wounds in STZ-diabetic mice treated with V were fully closed, compared with 100% of wounds in WT micetreated with V and in STZ-diabetic mice treated with PAI-039. C: H-E stain showing the leading epidermal edges (arrows) that are not fullyclosed. D: H-E stain showing the fully closed epidermis. White bars indicate V treatment; black bars indicate PAI-039 treatment. *Significantdifferences, as determined by Pearson x2 test. n = 6–8 for each bar in A. n = 10–12 for each bar in B.
diabetes.diabetesjournals.org Rebalka and Associates 2599

wounds. PAI-039 treatment reversed this defect, resultingin wound edge thicknesses comparable to those of the WTcohort, regardless of the level of handling.
DISCUSSION
One of the most prominent diabetic complications is theimpaired ability to heal wounds (14,18–21). In the cur-rent investigation, decreases in epidermal closure andCD31 content, as well as an increase in epidermal edgethickness exemplify the impairments in healing associatedwith diabetes. In 2001, Chan et al. (10) reported an ac-celerated rate of cutaneous wound healing in nondiabeticPAI-1–deficient mice. As previously mentioned, diabeticpatients experience elevated levels of PAI-1 regardless oftheir level of glycemic control (10,22). Due to the increasedexpression of PAI-1 in the diabetic population, as well asthe aforementioned improvements in WT dermal woundrepair observed as a result of genetically mediated knock-out of PAI-1 (10,22), investigations into the pharmacolog-ical reduction of PAI-1 levels for the restoration of diabeticwound healing were executed. To the best of our knowl-edge, this is the first study to analyze the effects of PAI-1inhibition on wound repair in the diabetic state.
Epidermal migration prompts wound re-epithelializationand is consequently responsible for initiating the processof wound repair (23). Therefore, epidermal closure is themost important step in wound healing, as all other cellu-lar proliferative and migratory events in the healing cas-cade follow epidermal closure (24). After wound closure,newly formed epidermis around the wound edgesbecomes hyperplastic due to the accumulation of cellsthat will migrate inward to close the wound gap (23).The thickness of this hyperplastic epidermal edge isexpected to return to “nearly normal” by 5 to 7 days post-injury in a nondiabetic environment (25). Consistent withthe literature (14–17), impairments in cellular prolifera-tion and migration associated with diabetic wound heal-ing, namely, attenuation of epidermal closure andincreased epidermal thickness, have been shown in thecurrent study. Importantly, the administration of PAI-039
to diabetic mice accelerated epidermal cellular migration,facilitating the restoration of epidermal thickness and totalwound closure to a level consistent with that in wounds ofWT mice.
Given the prominent role of PAI-1 in regulating thefibrinolytic pathway and in the remodeling of theextracellular matrix, a significant impact of PAI-1 in-hibition on fibrosis in the regenerating wounds wasexpected. This expectation was consistent with the pre-viously reported attenuation of skeletal muscle collagenaccumulation in diabetic mice postinjury after PAI-039treatment (12). What we found, however, was that PAI-039 treatment had no effect on dermal collagen contentpostwounding, suggesting that the mechanism of PAI-039action does not include mediating changes in the wounddermis.
Increases in PAI-1 expression, as well as alterationsin the inflammatory response (including prolongedinflammation and defective macrophage function) areassociated with impaired wound healing in diabetes(10,17,19,22,24,26–28). In a genetically induced diabeticmouse model (Akita), elevated PAI-1 levels attenuatedcollagen turnover and, ultimately, impaired macrophageinfiltration into damaged skeletal muscle. This impair-ment in infiltration was restored with the systemic ad-ministration of PAI-039 (29). Similarly, previous findingsindicate an increase in the number of lung exudate macro-phages in the presence of PAI-1, while, contrarily, theadministration of a small-molecule PAI-1 inhibitor atten-uated renal macrophage migration in nondiabetic animals(30,31). In the current investigation, PAI-039 treatmentconsistently decreased macrophage content (M2a andM2b) in minimally handled wounds. This effect was notconsistently observed in aggravated wounds; however,differences between aggravated and minimally handledwounds were also observed in other ways. A lesser overallamount of CD206, a marker of M2a macrophages witha wound-healing phenotype, was observed in minimallyhandled wounds. As CD206 is indicative of repair andregeneration, these data, most notably in diabetic wounds,
Figure 6—Difference in epidermal thickness between wound edges and unwounded epidermis. Both aggravated wounds (A) and minimallyhandled wounds (B) display a significant thickening of wound edge epidermis as a result of diabetes and a significant restoration ofepidermal thickness as a result of PAI-039 treatment in STZ animals. White bars, V treatment; black bars, PAI-039 treatment. *Significantdifferences, as determined by Tukey post hoc comparison. All data are presented as the mean 6 SEM. n = 6–7 for each bar in A. n = 10 foreach bar in B.
2600 PAI-1 Inhibition and Dermal Wound Closure Diabetes Volume 64, July 2015

suggests that minimally handled wounds may have pro-gressed further in the wound-healing process, and thushave fewer CD206 macrophages. Furthermore, when thesum total of all macrophages was compared between di-abetic groups, aggravated wounds displayed significantlymore macrophages, regardless of treatment, than theirminimally handled counterparts. Taken together, how-ever, as both aggravated and minimally handled woundsstill displayed great improvements in epidermal closure inthe presence of these macrophages, it is likely that thechanges in dermal macrophage content did not hinder theability of PAI-039 to facilitate wound closure.
Peripheral vasculature complications are prevalent inpatients with diabetes and pose as a significant hurdle towound healing, as the formation of vasculature in thewound bed is critical for sustaining migrating cells andnewly formed granulation tissue (32,33). Elevations inPAI-1 are seen to increase angiogenesis in cancerous tissue(34,35). In noncancerous tissue, however, thickening ofthe basement membrane due to matrix metalloproteinaseinhibition and a subsequent decrease in extracellular ma-trix turnover would be expected to impair the ability ofendothelial cells to infiltrate the wound site. Mice over-expressing PAI-1 display significantly increased numbersof venous occlusions, resulting in necrotic tails and swol-len limbs (36), and it has been known for some time thatthere is a connection between depressed fibrinolysis(through elevated PAI-1) and venous thrombosis (37). Col-lectively, it is evident that PAI-1 is involved in the regula-tion and dysregulation of angiogenesis. In the currentstudy, PAI-039 treatment failed to restore CD31 contentand improve angiogenesis; however, epidermal wound clo-sure was not hindered as a result.
Although there is no animal model that fully reflects allaspects of diabetes and its complications in humans, STZis the most widely used rodent diabetogenic chemicalagent, and has been so since it was first described in 1963(38). It is for this reason that we chose the STZ-diabeticmodel, as it is the most widely studied and would allowour results to be compared with the hundreds of pub-lished research studies investigating wound healing inSTZ-diabetic animals. Clearly, future studies investigatingother animal models of diabetes (such as the db/db orNONcNZO10 polygenic mice [39]) with and withoutPAI-039 would prove to be fruitful in further validatingthe efficacy of this inhibitor. Given the lack of concomi-tant vascular disease in STZ-diabetic mice, further exper-imentation using other models of diabetes that moreclosely mimic the vascular aspects of diabetes may providefurther insight into the impact of PAI-039 administrationon angiogenesis.
An important consideration of the current study is thefact that two models of wound care were undertaken. Thecontinuous disruption of the wounds with routine han-dling would be reflective of the repeated aggravation offoot ulcers in diabetic humans who continue to ambulateand wear improper footwear after experiencing a dermal
wound. In contrast, the minimal handling model exemplifiesoffloading, a critical component of diabetic wound care.Resting the wound site and minimizing pressure on thelesion or ulcer is, to date, the most effective intervention topromote diabetic wound healing, and is the first step in thetreatment of a neuropathic diabetic injury (13,40). To avoidwound chronicity, activities that may lead to wound siteaggravation should be avoided until proper healing has oc-curred (13). Consistent with these recommendations, thewound site aggravation used in this study exacerbated thewound-healing deficit observed in STZ-diabetic mice. This is,to our knowledge, the first histological investigation thatcombines pharmacological treatment with variations inwound care, highlighting the benefit to wound closure asa result of a reduction in wound site aggravation. This studyalso identifies the effectiveness of PAI-039 treatment in pro-moting wound closure to nondiabetic levels even in the pres-ence of wound aggravation. In fact, the greatest impact ofPAI-1 inhibition on epidermal wound closure was observed inaggravated wounds. These findings are of particular clinicalimportance, as it is estimated that more than half of diabeticindividuals with foot ulcers do not follow the recommendedguidelines for wound monitoring and maintenance (41).
Coupled with the absence of apparent changes in thewound dermis, the restoration of epidermal closure andepidermal edge thickness in STZ-diabetic mice as a resultof PAI-039 treatment reveals the mechanism of PAI-039action to be primarily epidermal in origin. PAI-039treatment facilitates the migration of epidermal cells, accel-erating the initiation of epidermal migratory edges andfacilitating wound closure, allowing the proceeding steps inthe healing cascade to commence in the presence of diabetes.
Funding. This work was supported by a Canadian Institutes of Health ResearchDoctoral Fellowship (D.M.D.), the Natural Sciences and Engineering ResearchCouncil of Canada (T.J.H.), and the Canadian Foundation for Innovation (T.J.H.).Duality of Interest. No potential conflicts of interest relevant to this articlewere reported.Author Contributions. I.A.R. designed the study; interpreted the results;performed animal care, sample collection, and data analysis; and wrote the initialdraft of the manuscript. M.J.R. performed sample collection and data analysis,interpreted the results, and edited the manuscript. D.M.D., S.K.C., and A.N.R.performed sample collection and data analysis and edited the manuscript. T.J.H.designed the study, interpreted the results, performed animal care, and editedthe manuscript. All authors contributed to the final version of the manuscript.T.J.H. is the guarantor of this work and, as such, had full access to all the data inthe study and takes responsibility for the integrity of the data and the accuracy ofthe data analysis.Prior Presentation. Parts of this study were presented in abstract form atthe Keystone Symposia on Complications of Diabetes, Whistler, BC, Canada,23–28 March 2014.
References1. Centers for Disease Control and Prevention (CDC). National Diabetes Sta-tistics Report: Estimates of Diabetes and Its Burden in the United States. Atlanta,GA, U.S. Department of Health and Human Services, 20142. Danaei G, Finucane MM, Lu Y, et al.; Global Burden of Metabolic Risk Factorsof Chronic Diseases Collaborating Group (Blood Glucose). National, regional, and
diabetes.diabetesjournals.org Rebalka and Associates 2601

global trends in fasting plasma glucose and diabetes prevalence since 1980:systematic analysis of health examination surveys and epidemiological studieswith 370 country-years and 2.7 million participants. Lancet 2011;378:31–403. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence ofdiabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87:4–144. Brem H, Stojadinovic O, Diegelmann RF, et al. Molecular markers in patientswith chronic wounds to guide surgical debridement. Mol Med 2007;13:30–395. Public Health Agency of Canada (PHAC). Diabetes in Canada: Facts andFigures from a Public Health Perspective. Ottawa, ON, Canada, Public HealthAgency of Canada, 2011, p. 43–516. Kruse I, Edelman S. Evaluation and treatment of diabetic foot ulcers. ClinDiabetes 2006;24:91–937. Goldberg RB. Cytokine and cytokine-like inflammation markers, endothelialdysfunction, and imbalanced coagulation in development of diabetes and itscomplications. J Clin Endocrinol Metab 2009;94:3171–31828. Lyon CJ, Hsueh WA. Effect of plasminogen activator inhibitor-1 in diabetesmellitus and cardiovascular disease. Am J Med 2003;115(Suppl. 8A):62S–68S9. Nicholas SB, Aguiniga E, Ren Y, et al. Plasminogen activator inhibitor-1deficiency retards diabetic nephropathy. Kidney Int 2005;67:1297–130710. Chan JC, Duszczyszyn DA, Castellino FJ, Ploplis VA. Accelerated skin woundhealing in plasminogen activator inhibitor-1-deficient mice. Am J Pathol 2001;159:1681–168811. Oishi K, Ohkura N, Kasamatsu M, et al. Tissue-specific augmentation ofcircadian PAI-1 expression in mice with streptozotocin-induced diabetes. ThrombRes 2004;114:129–13512. Krause MP, Moradi J, Nissar AA, Riddell MC, Hawke TJ. Inhibition ofplasminogen activator inhibitor-1 restores skeletal muscle regeneration in un-treated type 1 diabetic mice. Diabetes 2011;60:1964–197213. Kalish J, Hamdan A. Management of diabetic foot problems. J Vasc Surg2010;51:476–48614. Greenhalgh DG. Wound healing and diabetes mellitus. Clin Plast Surg 2003;30:37–4515. Brem H, Tomic-Canic M. Cellular and molecular basis of wound healing indiabetes. J Clin Invest 2007;117:1219–122216. Izuhara Y, Takahashi S, Nangaku M, et al. Inhibition of plasminogen acti-vator inhibitor-1: its mechanism and effectiveness on coagulation and fibrosis.Arterioscler Thromb Vasc Biol 2008;28:672–67717. Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med 1999;341:738–74618. Darby IA, Bisucci T, Hewitson TD, MacLellan DG. Apoptosis is increased ina model of diabetes-impaired wound healing in genetically diabetic mice. IntJ Biochem Cell Biol 1997;29:191–20019. Fahey TJ 3rd, Sadaty A, Jones WG 2nd, Barber A, Smoller B, Shires GT.Diabetes impairs the late inflammatory response to wound healing. J Surg Res1991;50:308–31320. Nguyen PD, Tutela JP, Thanik VD, et al. Improved diabetic wound healingthrough topical silencing of p53 is associated with augmented vasculogenicmediators. Wound Repair Regen 2010;18:553–55921. Wall SJ, Bevan D, Thomas DW, Harding KG, Edwards DR, Murphy G.Differential expression of matrix metalloproteinases during impaired woundhealing of the diabetes mouse. J Invest Dermatol 2002;119:91–98
22. Oishi K. Plasminogen activator inhibitor-1 and the circadian clock in met-abolic disorders. Clin Exp Hypertens 2009;31:208–21923. Braiman-Wiksman L, Solomonik I, Spira R, Tennenbaum T. Novel insightsinto wound healing sequence of events. Toxicol Pathol 2007;35:767–77924. Falanga V. Wound healing and its impairment in the diabetic foot. Lancet2005;366:1736–174325. Odland G, Ross R. Human wound repair. I. Epidermal regeneration. J CellBiol 1968;39:135–15126. Mirza R, Koh TJ. Dysregulation of monocyte/macrophage phenotype inwounds of diabetic mice. Cytokine 2011;56:256–26427. Ochoa O, Torres FM, Shireman PK. Chemokines and diabetic woundhealing. Vascular 2007;15:350–35528. Wetzler C, Kämpfer H, Stallmeyer B, Pfeilschifter J, Frank S. Large and sus-tained induction of chemokines during impaired wound healing in the geneticallydiabetic mouse: prolonged persistence of neutrophils and macrophages during thelate phase of repair. J Invest Dermatol 2000;115:245–25329. Krause MP, Al-Sajee D, D’Souza DM, et al. Impaired macrophage andsatellite cell infiltration occurs in a muscle-specific fashion following injury indiabetic skeletal muscle. PLoS One 2013;8:e7097130. Ichimura A, Matsumoto S, Suzuki S, et al. A small molecule inhibitor toplasminogen activator inhibitor 1 inhibits macrophage migration. ArteriosclerThromb Vasc Biol 2013;33:935–94231. Osterholzer JJ, Christensen PJ, Lama V, et al. PAI-1 promotes the accu-mulation of exudate macrophages and worsens pulmonary fibrosis following typeII alveolar epithelial cell injury. J Pathol 2012;228:170–18032. Clark R. The Molecular and Cellular Biology of Wound Repair. 2nd ed. ClarkR, Ed. New York, NY, Springer, 199633. Cooper ME, Gilbert RE, Jerums G. Diabetic vascular complications. Clin ExpPharmacol Physiol 1997;24:770–77534. Bajou K, Masson V, Gerard RD, et al. The plasminogen activator inhibitorPAI-1 controls in vivo tumor vascularization by interaction with proteases, notvitronectin. Implications for antiangiogenic strategies. J Cell Biol 2001;152:777–78435. Isogai C, Laug WE, Shimada H, et al. Plasminogen activator inhibitor-1promotes angiogenesis by stimulating endothelial cell migration toward fibro-nectin. Cancer Res 2001;61:5587–559436. Erickson LA, Fici GJ, Lund JE, Boyle TP, Polites HG, Marotti KR. De-velopment of venous occlusions in mice transgenic for the plasminogen activatorinhibitor-1 gene. Nature 1990;346:74–7637. Pandolfi M, al-Rushood A. The role of fibrinolytic factors in ischaemia. Eye(Lond) 1991;5:159–16938. Rakieten N, Rakieten ML, Nadkarni MV. Studies on the diabetogenic actionof streptozotocin. Cancer Chemother Rep 1963;29:91–9839. Fang RC, Kryger ZB, Buck DW 2nd, De la Garza M, Galiano RD, Mustoe TA.Limitations of the db/db mouse in translational wound healing research: is theNONcNZO10 polygenic mouse model superior? Wound Repair Regen 2010;18:605–61340. Boada A. Skin lesions in the diabetic foot. Actas Dermosifiliogr 2012;103:348–356 [in Spanish]41. Sanmartin C, Gilmore J. Diabetes-prevalence and care practices. Health Rep2008;19:59–63
2602 PAI-1 Inhibition and Dermal Wound Closure Diabetes Volume 64, July 2015