influence of a dental ceramic and a calcium aluminate...
TRANSCRIPT

UMEÅ UNIVERSITY ODONTOLOGICAL DISSERTATIONS
New Series No. 98, ISSN 0345-7532, ISBN 91-7264-284-3
Influence of a Dental Ceramic and a Calcium Aluminate Cement on Dental Biofilm
Formation and Gingival Inflammatory Response
Department of Odontology, Dental Hygienist Education,
Faculty of Medicine, Umeå University, Sweden
2007
Katarina Konradsson

2
Copyright © Katarina Konradsson
ISBN 91-7264-284-3
Printed in Sweden by Solfjädern Offset AB
Umeå 2007

Till Lars, Richard och Sofie
Ut audiat sapientiam auris tua, inclina cor tuum ad cognoscendam prudentiam. Liber proverbiorum 2:2
turning your ear to wisdom
and applying your heart to understanding
Proverbs 2:2

4

Abstract
Dental restorative materials interact with their surrounding oral environment.
Interaction factors can be release of toxic components and/or effects on biofilm
formation and gingiva. In the end of the nineties, a calcium aluminate cement (CAC) was
manufactured as a “bioceramic” alternative to resin composite. Dental ceramics are
considered to be chemically stable and not to favour dental biofilm formation. Since the
influence of aged, resin-bonded ceramic coverages is not fully investigated and the
effect of CAC restorations on the dental biofilm formation and gingival response is
unknown, those issues were evaluated in this thesis.
With or without oral hygiene, in clinical trials including cervical surfaces of CAC, and
approximal surfaces of a leucite-reinforced bonded ceramic; biofilm growth, presence of
caries-associated bacteria, clinical expressions of gingivitis, the amounts of gingival
crevicular fluid (GCF) and its levels of IL-1α, IL-1β and IL-1 ra were investigated in
comparison with resin composite and enamel. In addition, the unknown cytotoxic effect
of specimens of CAC on fibroblasts was assessed in vitro.
With current oral hygiene a similar biofilm formation and gingival response, as
evaluated, were observed at sites of CAC, resin composite and enamel. After ceased
oral hygiene, more biofilm was assembled on CAC and on resin composite than on
enamel. Neither with, nor without oral hygiene, biofilm formation, presence of caries-
associated bacteria, clinical gingivitis and the levels of IL-1α, IL-1β and IL-1 ra differed
between sites of ceramic, resin composite and enamel. Higher volumes of GCF were
collected at ceramic sites compared to enamel. Fresh specimens of CAC showed the
lowest cytotoxic effects on fibroblasts compared with three resin composites, zinc
phosphate and glass ionomer cements.
In conclusion, the low cytotoxic effect of CAC and the limited increase in dental biofilm
formation on that material compared with enamel suggest CAC to be a biocompatible
dental material with respect to dental biofilm formation, presence of caries-associated
microflora and gingival response. This finding, together with the observation that the
influence of bonded ceramic on dental biofilm formation, caries-associated microflora
and clinical gingivitis was not different from that of enamel, implicates for both CAC
restorations and bonded ceramic that the need of oral hygiene and professional oral
health care is not reduced.
Key words: cements, ceramics, cytotoxicity, dental biofilm, gingivitis, interleukin-1, oral
hygiene, resin composite

6
Table of Contents
Page
Abbreviations ............................................................................... 7
Preface ......................................................................................... 8
Introduction ................................................................................. 9
Dental biofilm ............................................................................... 9
Gingival inflammation ................................................................... 10
Dental caries ................................................................................. 14
Dental materials ........................................................................... 15
Aims ............................................................................................ 19
Material and Methods ................................................................. 20
Subjects and surfaces of the in vivo evaluations ........................... 20
Study designs ................................................................................ 21
Statistics ....................................................................................... 25
Results .......................................................................................... 26
Discussion .................................................................................... 34
Conclusions .................................................................................. 46
Acknowledgements...................................................................... 47
References ................................................................................... 49
Papers I-V ........................................................................ Appendix I-V

7
Abbreviations
CAC calcium aluminate cement
CFU colony forming units
CSS cross sectional study
DMEM Dulbecco's Modified Eagle Medium
DMFS decayed, missed and filled surfaces
ELISA enzyme-linked immunosorbent assay
GBI gingival bleeding index
GCF gingival crevicular fluid
GI Gingival Index
IL interleukin
PI plaque index
PPD probing pocket depth
PVC polyvinyl chloride
QHI Quigley Hein plaque index
ra receptor antagonist
SBI sulcus bleeding index
TNF tumor necrosis factor

8
Preface
This thesis is based on the following papers, which are referred to in the text by their Roman numerals I-V: I. Konradsson K, van Dijken JWV. Effect of a novel ceramic filling
material on plaque formation and marginal gingiva. Acta Odontol Scand 2002, 60: 370-4
II. Konradsson K, van Dijken JWV. Interleukin-1 levels in gingival
crevicular fluid adjacent to restorations of CAC and resin composite. J Clin Periodontol 2005, 32: 462-6
III. Franz A, Konradsson K, Koenig F, van Dijken JWV, Schedle A.
Cytotoxicity of a calcium aluminate cement with comparison to other dental cements and resin based materials.
Acta Odontol Scand 2006, 64: 1-8 IV. Konradsson K, Claesson R, van Dijken JWV. Mutans streptococci
and lactobacilli in plaque on a leucite-reinforced dental ceramic, and a calcium aluminate cement. Clin Oral Invest 2006, 10: 175-80
V. Konradsson K, Claesson R, van Dijken JWV. Dental biofilm,
gingivitis and interleukin-1 adjacent to approximal sites of a bonded ceramic. Submitted
Reprints were made with permission from the publishers.

9
Introduction
Dental biofilm
Microbial biofilms develop on solid surfaces in a non-sterile aqueous solution (ten Cate 2006). The biofilm which covers the surfaces of the oral cavity, is protective by preventing colonization of exogenous micro-organisms (Marsh and Bradshaw 1997, Socransky and Haffajee 2002), but it is also a basic prerequisite for developing caries (Fehr von der, and Theilade 1970) and plaque-induced gingivitis (Löe et al. 1965). The complex oral biofilm consists of bacteria, embedded in a matrix of their metabolic products and host-derived components (Marsh 2004, Marsh 2006, Socransky and Haffajee 2002). About 1000 different oral bacterial species are identified, half of which is cultivable (ten Cate 2006). The dental plaque on the non-shedding tooth surfaces is redefined as the dental biofilm (Rudney et al. 2000, Socransky and Haffajee 2002).
The formation of the dental biofilm, involves overlapping phases. Initially, the acquired pellicle, a conditioning film of glycoproteins and proteins, originated from host and bacterial molecules in the saliva and GCF adsorbs to the tooth surfaces (Lendenmann et al. 2000, Rüdiger et al. 2002, Rudney et al. 2000). Colonization of bacteria occurs by adhesion, interaction/communication and growth/metabolism. In the passive transport of oral bacteria to the tooth surface, early bacterial colonizers adhere to the pellicle by non-specific, weak, long-range interactions and specific adhesin-receptor mediated attachments. Other bacteria (co)adhere to already attached cells and multiply (Marsh 2004, Marsh 2006, Teughels et al. 2006). The various exopolysaccharides, which are synthesized by bacteria, confer to the physical and environmental characteristics of the biofilm (Sutherland 2001).
Healthy gingiva is associated with a few layers of the gram positive cocci and rods. Early colonizers are able to withstand the high oxygen concentrations and to resist natural removal mechanisms into the oral cavity (Sbordone and Bortolaia 2003). Species involved are streptococci, such as S. mitis, and S. oralis, and actinomyces, such as A. naeslundii (Li et al. 2004, ten Cate 2006). A pivotal role of actinomyces is to form a mixed biofilm with lactobacilli, which do not form biofilms on their own (Filoche et al. 2004). During biofilm formation, the local microenvironment shifts due to pH changes, the supply of nutrients and decreased oxygen levels

10
(Marsh 1997, Marsh 2003) which enable microbial succession (Socransky and Haffajee 2005). Intermediate, i.e. Fusobacterium, and late colonizers, among them periodontitis-related bacteria, are unable to directly stick to hard tooth surfaces. They will attach when the physiological conditions in the biofilm are more likely to support their growth and survival (Sbordone and Bortolaia 2003, Socransky and Haffajee 2005, ten Cate 2006). After 2-3 weeks of undisturbed growth a mature and relatively stable microflora is established (Marsh and Bradshaw 1995).
The ecological balance of the biofilm is sustained due to bacterial interactions. The microbial homeostasis can, however, be changed by a more substantial alteration of the bacterial and host products. Metabolic waste products affect the underlying teeth or the surrounding periodontal tissues (Marsh 2003). Penetration of those tissues confers to an environmental and microbial shift, and caries and periodontal diseases can be established (ten Cate 2006).
Gingival inflammation
The gingiva is a specialized structure whose structure and function interact with the other periodontal components i. e. periodontal ligament, cementum and alveolar bone (Bartold 2006). Principally, periodontal diseases are infections caused by bacteria in the biofilm that colonize the tooth surface at or below the gingival margin (Socransky and Haffajee, 2002). Nevertheless, oral health or disease depends on the host and the microbial community as a whole (Jenkinson and Lamont 2005). The periodontal diseases are recognized as ‘eco-genetic’ diseases. The role of bacteria, host immune and inflammatory responses, gene polymorphisms, local and systemic environmental factors and various medications are able to impact the structure and function of the connective tissues. In interplay with those factors, the inflammatory process comprises a series of molecular and cellular events that lead to a host response as a defence against trauma and microbial invasion. Eventually, the host response is involved in processes of repair of tissue compartments injured by the direct effect of invaders or trauma or host’s own systems (Bartold 2006).
Broadly, gingival inflammation, i.e. gingivitis, can be described as the complex inflammatory host response on various stimuli to the gingiva. Gingival diseases are either plaque-induced or not primarily associated with dental plaque (Armitage 1999). Most prevalent is plaque-induced gingivitis, which is associated with an organized biofilm of several

11
bacterial cell layers (100-300). The species involved vary. At development of gingivitis the number of gram negative bacteria increases and anaerobic bacteria appear by microbial succession, such as Fusobacterium nucleatum, Campylobacter gracilis, Tannerella forsythia, Capnocytophaga and Prevotella species (Rüdiger et al. 2002, Sbordone 2003, Socransky and Haffajee 2005). Besides, gingivitis favours the rate of dental biofilm formation (Daly and Highfield 1996, Ramberg et al. 1994).
From experimental gingivitis studies of abstained oral hygiene for four weeks, it was concluded that increased quantities (Löe et al. 1965) and an altered quality of the biofilm (Theilade et al. 1966) are followed by clinical signs of gingivitis, manifested by gingival redness, swelling and bleeding. The development of gingivitis is directly associated with the rate of dental biofilm formation which varies to a great extent between different individuals. The plaque-induced gingivitis is reversible. After about one week of oral hygiene the gingivitis fades off (Löe et al. 1965, Theilade et al. 1966).
Oral bacterial infectious diseases can be treated in a physical, antimicrobial and ecological way (Socransky and Haffajee 2002). A good oral hygiene, by removing the dental biofilm, is still the most effective procedure for control of the biofilm-related diseases (Axelsson and Lindhe 1981, Jenkinson and Lamont 2005, Sbordone and Bortolaia 2003).
The histopathology of gingivitis
The development of a gingival inflammatory infiltrate in the marginal connective tissue was studied by Page and Schroeder (1976). Within a few days of dental biofilm accumulation, the acute inflammatory response on bacterial components and products results in an initial gingival lesion. The initial response comprises a release of proinflammatory mediators from stimulated epithelial cells, activation of endothelial cells and dilatation of the vessels. Concomitantly, the flow of the gingival crevicular fluid (GCF) enhances (Zappa 1995). Proteases, originated from epithelial cells, fibroblasts, and leukocytes, degrade the surrounding tissue to an infiltrate which comprises about 10 % of the marginal connective tissue. Neutrophilic or polymorphonuclear leukocytes are responsible for the major tissue degradation. Those have many receptors on their surfaces recognizing and fighting bacteria by antimicrobial substances and phagocytosis. The migration of neutrophiles from the vessels through the connective tissue and epithelium to the sulcus is stimulated by

12
chemotactic signals from bacteria and host cells, and by adhesion molecules on the endothelial cells and neutrophiles (Page 1999). The initial stage of gingivitis is a sub-clinical condition, without obvious clinical expressions. After one week, the vessel permeability increases further, resulting in clinical signs of redness and swelling. The junctional epithelium begins to proliferate. Abundant amounts of T-lymphocytes and macrophages are available in the infiltrate enclosing about 15 % of the connective tissue in which the loss of collagen increases. This early lesion can be changed over to an established lesion by further degradation of the connective tissue, expanded changes of the vessels, increased leukocyte migration, enhanced GCF flow and abundant amounts of leukocytes embedded into the gingival tissue. At this stage, the clinical expressions are apparent in redness, swelling and bleeding. Subject to a persistent biofilm, a chronic gingivitis may be established. In most individuals, the lesion is delimited to the gingiva due to the host response. However, in others, the connective tissue degradation is followed by effects on the periodontal ligament and bone, causing an irreversible lesion due to attachment loss, i.e. periodontitis (Zappa 1995).
Gingival crevicular fluid
The GCF is found in the sulcus or periodontal pocket between the tooth and marginal gingiva. In gingival health, the small amounts of the fluid represent the transudate of gingival tissue interstitial fluid passing through the junctional epithelium, but in course of periodontal disease the fluid is transformed into an inflammatory exsudate (Alfano 1974, Griffiths 2003). GCF is a complex mixture of substances derived from serum, leukocytes, periodontal cells and oral bacteria. The host-derived substances in the GCF include antibodies, cytokines, enzymes and tissue degradation products (Uitto 2003). Prior to the apparent clinical signs of gingivitis, the dental biofilm formation provokes a sub-clinical, gingival inflammatory response, associated with an increase in GCF flow (Löe and Holm-Pedersen 1965). Measurements of the enhancement of the GCF flow are a useful indicator of gingival inflammation (Poulsen et al. 1979). The contents of the GCF reflect bacterial activity in the gingival pocket and inflammatory events taking place in the gingival tissues (Eley and Cox 1998, Embery and Waddington 1994, Giannobile et al. 2003).

13
Cytokines
Cytokines are low-molecular-weight proteins which induce and maintain an inflammatory response. They can be synthesized by most of the host cells in response to bacteria and their products (Dinarello 2000). Bacterial endotoxin i.e. lipopolysaccharides, are capable to stimulate polymorphnuclear leukocytes to release proinflammatory cytokines (Zappa 1995) and also their inhibitors (Yoshimura et al. 1997). Cell stressors of non-microbial origin can also stimulate the synthesis of cytokines. These are divided into different groups due to their biological activities, which can be altered in various biological processes. One group of cytokines is named interleukins (IL). Other cytokines have retained their original description, such as tumor necrosis factor (TNF). Proinflammatory cytokines promote inflammation, whereas the gene expression of those is suppressed by anti-inflammatory cytokines. Inflammation mediated by cytokines is a result of a cascade of gene products usually not produced in healthy individuals. IL-1 and TNF act synergistically to stimulate adhesion molecules on leukocytes and endothelial cells, to initiate other inflammatory mediators, to induce expression of matrix metalloproteinases, to stimulate apoptosis of matrix producing cells and to enhance bone resorption (Graves and Cochran 2003). IL-4, IL-10 and IL-13 are some of the anti-inflammatory cytokines suppressing IL-1, IL-8, TNF and vascular adhesion molecules (Dinarello 2000).
Interleukin-1
IL-1 is one of the major inflammatory mediators and appears early in the inflammatory process. It has different effects on several cell types including stimulation or suppressing of other proteins. IL-1 stimulates small mediator molecules, such as platelet-activating factor and prostaglandins, which are potent vasodilators. Besides, IL-1 increases the synthesis of collagenases and stimulates T and B lymphocytes (Dinarello 2000). Many cell types are producers of IL-1 (Seymour and Gemmell 2001), but primarily producers are mononuclear phagocytes when stimulated by microbial or inflammatory agents. There are two distinct proteins of IL-1, coded by different genes, IL-1α and IL-1β. These are structurally related proteins of different amino acid sequences. Both types of IL-1 can bind to two distinct cell surface receptors, IL-1 R Types I and II, of which IL-1 R type II functions as a decoy molecule (Graves and Cochran 2003). Due to binding to the same receptor, there are no differences between the biological actions of IL-1α and IL-1β. However, IL-1α is a cell-
14
associated cytokine which can also act as a transcription factor, whereas IL-1β is secreted and therefore, more likely to play a role in systemic inflammation (Dinarello 2005). The IL-1 receptor antagonist (IL-1ra) exists as a unitary mechanism within the immune system to control IL-1 activity. This protein acts by binding with high affinity to the same receptors as IL-1α and IL-1β without inducing any of the biological effects (Weber and Iacono 1997, Dinarello and Wolff 1993). Production of IL-1 and IL-1 ra is differently regulated, even in the same cell. Experimental gingivitis models have demonstrated that IL-1 (Kinane et al. 1992) or IL-1β in GCF increases during gingival inflammation prior to the onset of clinical signs of gingivitis (Heasmann et al. 1993, Zhang et al. 2002).
Dental caries
Dental caries is a localized destruction of susceptible dental hard tissues by acidic by-products from bacterial fermentation of dietary carbohydrates. Caries results from the interactions over time between the acid-producing bacteria, a substrate to metabolize and host factors (Selwitz et al. 2007). The multi-factorial caries disease is associated with lifestyle-relating factors, such as the frequency of sugar intake, dietary food, oral hygiene, use of fluoride products, socio-economic factors and related genetic factors (Fejerskov 1997).
Caries develops by microbiological shifts within the dental biofilm and is affected by salivary flow and its composition (Marsh 1994, Selwitz et al. 2007). The microbial shift results in an increase of the proportions of acidogenic and acid-tolerating bacteria, which can rapidly metabolize dietary sugars to weak organic acids, mainly lactic acid, and adapt to low pH with an optimal growth and metabolism. Well-known caries-associated bacteria are mutans streptococci, S. mutans and S. sobrinus, and lactobacilli, although other species may also be involved (Kleinberg 2002, Marsh 1994, Marsh 2006). Mutans streptococci adhere to the oral hard tissues and take a major part of the initiation of caries (Gibbons 1984, Liljemark and Blomquist 1996, Loeshe et al. 1986, Selwitz et al. 2007). They are also able to synthesize extracellular glucans from dietary sucrose specifically (Houte, van 1994, Paes Leme et al. 2006). The concomitant pH-fall in the dental biofilm might enhance the proportions of lactobacilli. They support a caries-inducing environment and attend in the proceeding

15
demineralization of the caries lesion (Crossner et al. 1989, Houte, van 1994, Kleinberg 2002). The acids cause a local pH fall below a critical value in which calcium and phosphate ions dissolve out of the tooth. The balance between this demineralization and the remineralization, through uptake of calcium, phosphate and fluoride, affects the caries development. The saliva acts as a buffer to protect against dissolution of the mineral content at pH-fall (Paes Leme et al. 2006).
Dental materials
Dental materials restore the anatomy and function of the tooth surfaces affected by caries. Aesthetics and concern about the biocompatibility of amalgam have increased the use of tooth-colored restorations. Common direct filling materials are resin composites, glass ionomer cements and intermediary materials between them. The poor mechanical properties of the non-resinous materials limit their use in loaded cavities (Mjör et al 1990).
Secondary caries is the main reason for replacement of those materials (Mjör 2005). Dental caries is even a primary failure of cast restorations. Therefore, an ‘ideal’ luting agent preventing dental biofilm formation and caries is required (Rosenstiel et al. 1998). Filled or unfilled resins and glass ionomer cement function as luting agents with a high adhesive potential, establishing or increasing the retention of the crowns or inlays to the abutments and maintain their integrity. The curing of some resin materials is initiated either chemically, through the application of light, or in both ways (Macorra and Pradies 2002).
Resin Composites
Resin composites are used frequently because of their aesthetics and physiological properties in all cavity classes with a tooth substance saving preparation technique. However, polymerization shrinkage of the resin composites occurs (Friedl et al. 2000, Gladys et al. 2001) which can cause marginal defects (Hansen 1982). Initially, substances can be released from the resin composites because of incomplete monomer-polymer conversion (Ferracane 1994). The substances are potential inducers of cytotoxic and/or contact allergic reactions (Nadarajah et al. 1997, Schedle et al. 1998, Wrangsjö et al. 2001).
16
Ceramics
Ceramics can be defined as inorganic, non-metallic materials, mostly as a result from high-temperature reactions. A wide definition of ceramics comprises also metal oxides and cement. The specific properties of ceramics are hardness, porosity, and brittleness. Early ceramics showed a low fracture resistance, which was improved in leucite crystals reinforced feldspathic porcelain. Ceramic onlays/crowns of the leucite-reinforced glass (Empress I), luted with a dentine bonding adhesive system and a resin composite material, have showed satisfactory clinical performance (Fradeani 1997, Dijken van 2001). Bonding of ceramics has been applied during the last decades for the manufacturing of veneers, inlays/onlays and full crowns. Dental ceramics are suggested to be chemically stable with a high biocompatibility (Schuster et al. 1996) and not to favour plaque accumulation (Chan and Weber 1986, Savitt et al. 1987, Jensen et al. 1990). However, Messer et al. (2003) implicated that “all dental ceramics should be tested for biologic safety because prediction of safety on the basis of composition or class of materials may not be reliable. In particular, newer dental ceramics should be valuated specifically and not be assumed to be equivalent to traditional feldspathic ceramic materials or other contemporary materials of the same type.”
Calcium aluminate cement
In the late nineties, calcium aluminate cement (CAC) was developed as a “bioceramic” alternative to amalgam and resin composite, intending to be directly used in Class I, II and V cavities. The CAC is inorganic and non-metallic. It is based on two essential constituents, alumina and calcium oxides and a small amount of zirconium, ferric and silicone oxides. Fused together at a high temperature, small particles of calcium-aluminates are formed, having a cement-forming potential. To start the hardening reaction the calcium aluminate tablets are brought into contact with the supplied liquid, which contains water and small amounts of lithium as an accelerator. An acid-base reaction is initiated. Water acts as a weak acid and calcium aluminate dissolves to form Ca2+, Al (OH)4
- and OH-. The solutes precipitate to form a gel. Gradually, the amorphous gel changes into a crystalline phase [(CaO)3(Al2O3)(H2O)6] (Sunnegårdh-Grönberg 2004). Poor mechanical properties (Sunnegårdh-Grönberg 2004, Geirsson et al. 2004 a), and low clinical durability have recently been observed (Dijken van and Sunnegårdh-Grönberg, 2004).
17
Dental materials and biofilm formation
All biofilms consist of three ‘components’; the surface for attachment, the microbial community itself, and the “bulk fluid” which passes over the biofilm. Each of the three ‘components’ may be altered to local or subject level factors which may influence the microbial composition of the colonizing biofilm (Socransky and Haffajee 2005). Initially, the adhesion of saliva proteins and the composition of the pellicle can be affected by the adherent surface (Steinberg and Eyal 2002). The biofilm growth on the materials of the restored teeth can vary due to surface characteristics of the materials, i.e. surface-free energy and surface roughness. The surface roughness is likely to have a greater influence on biofilm retention than surface-free energy (Quirynen et al. 1990). Dental biofilm formation starts in cracks and grooves, and in irregularities in which the bacteria are protected. Defects and rough surfaces can promote the dental biofilm accumulation (Quirynen 1995). The surface area increases with the surface roughness and hence, the colonization. Surface roughness provides protection from shear forces and augments the difficulty in cleaning (Socransky and Haffajee 2002). Accumulation of the biofilm on dental cements and resin luting materials is mainly related to achieving and maintaining a highly polished surface which can be influenced by the high porosity of those materials (Macorra and Pradies 2002). The initial antibacterial effect of ion-releasing dental materials is well known (Berg et al. 1990, Dijken van et al. 1997, Foley and Blackwell 2003, Morrier et al. 1998). Still, mutans streptococci tend to colonize restored surfaces to a greater extent than sound tooth surfaces (Lindquist and Emilson 1990), however, not demonstrated by others (Dijken van et al. 1991a). In addition to the properties of the restorative material, overhangs can affect the dental biofilm formation and periodontal health (Lang et al. 1998). Even presence of minute overhangs, difficult to detect clinically, predisposes for development of secondary caries, which indicates that dental biofilm accumulation is a predisposing factor (Mjör 2005).

18
Biocompatibility
A biomaterial is defined as a non-viable material used in a medical device, intended to interact with biological systems. The biocompatibility of a material is its ability to perform with an appropriate host response in a specific situation (Black 1999). Biocompatible materials must be free from any unacceptable risk (Schmalz 1997). The American Dental Association and American National Standard Institute (ADA/ANSI) have recommended biocompatibility testing of dental materials in order to obtain full clinical acceptance. Standards for testing dental materials, which are considered as medical devices, are described in ISO 10993-5 (1997), ISO 7405 (1999) and the ADA guidelines for posterior restorations (1996). Those are used to better compare data. If more appropriate, other tests can be chosen (Schmalz 1997). Restorative materials interact with their surrounding biological environment. Interaction factors can be release of components from dental materials (Ferracane 1994) and the surface characteristics of the material (Quirynen and Bollen 1995). Biofilm formation on tooth restorations may also influence their stability and biocompatibility (Santerre et al. 2001). Adverse biological effects caused by dental restorative materials may be expressed clinically or sub-clinically, toxically and/or allergically (Schmalz and Garhammer 2002, Geurtsen 2000). Consequently, biocompatibility testing can not rely on a single test. A concept of biocompatibility testing is to use initial tests, such as cytotoxicity testing on a cellular level, secondary tests, such as implantation tests, and usage tests, which mirror the patient situation (Schmalz 1997). Studies on the biocompatibility of restorative materials have focused in vitro on inflammatory responses and toxic effects on fibroblasts and epithelial cells (Hanks et al. 1996, Santerre et al. 2001, Schedle et al. 1998, Schmalz et al. 2000, Wataha et al. 1994) as well as in vivo on longitudinal clinical follow-ups of the materials’ efficacy and durability (Mjör et al. 1990, Mjör et al 2000, Dijken van 1999, Dijken van et al. 2001, Dijken van and Sunnegårdh-Grönberg 2004, Sunnegårdh-Grönberg 2004).

19
Aims
The aim of this thesis was to evaluate the influence of a calcium aluminate cement and resin-bonded, leucite-reinforced ceramic on dental biofilm formation and gingival response.
More specifically, the aim was to study dental biofilm growth, clinical signs of gingivitis, the amounts of gingival crevicular fluid, its levels of IL1α, IL-1β and IL-1ra and, the presence of mutans streptococci and lactobacilli on those restoratives in vivo. In addition, the intention was also to study the cytotoxicity of CAC on fibroblasts in vitro.
The purposes of the five studies were as follows:
To evaluate CAC regarding plaque formation and gingival inflammation with or without customary oral hygiene, in comparison with resin composite and enamel (Paper I).
To compare CAC, resin composite and enamel with respect to adjacent levels of IL -1α, IL -1β and IL -1ra in GCF (Paper II).
To compare the cytotoxicity of the CAC with several currently used direct restorative materials (Paper III).
To examine the levels of mutans streptococci and lactobacilli in plaque 1) on approximal surfaces of resin-bonded ceramic restorations, and 2) on Class V restorations of CAC, and compare the levels with those on resin composite and enamel (Paper IV).
To investigate the influence of aged, resin-bonded, leucite-reinforced ceramic restorations on approximal dental biofilm formation and gingival inflammatory response associated with and without customary oral hygiene (Paper V).

20
Material and Methods
The evaluations of the CAC, which was denominated as a ‘novel ceramic filling material’ in Paper I, are described in Paper I-IV. The investigations of the resin-bonded, leucite-reinforced ceramic are reported in Paper IV-V. All papers, except for Paper III, were based on in vivo studies in an intra-individual approach, comparing surfaces/sites of these evaluated materials with resin composite and enamel. Paper I, II, and V are focused on dental biofilm formation and the gingival response. Paper III deals with the cytotoxic effects of the CAC, in vitro, and Paper IV is about the caries-associated microflora.
Subjects and surfaces of the in vivo evaluations
Paper I and II: Intra-individually comparisons were made regarding dental biofilm formation and initiation of gingivitis with and without oral hygiene in 15 subjects (4 females and 11 males, mean age 63 years, range 40-85) within a set of two cervical Class V restorations, one of CAC and one of resin composite, and one control surface of enamel. Twenty sets were included.
Paper IV: The study comprised two study groups. The first one corresponded to the study group described in Paper V. The levels of the mutans streptococci and lactobacilli in ten days old dental biofilm were compared between 11 of the 12 included approximal surfaces of leucite-reinforced bonded ceramic restorations (IPS Empress, Ivoclar, Liechtenstein), Class II restorations of resin composite and enamel. The second study group of subjects was in accordance with those described in Paper I. The levels of the caries-associated bacteria were compared between 18 cervical Class V restorations of CAC and resin composite and smooth non-restored enamel surfaces without detected caries.
Paper V: Intra-individually comparisons were made between one approximal surface of a bonded ceramic coverage (IPS Empress, Ivoclar, Liechtenstein) and one of enamel in 17 subjects (11 females and 6 males, mean age 54 years, range 43-85), regarding dental biofilm formation and initiation of gingivitis with and without oral hygiene. In a subgroup, including 11 of these subjects, an additional approximal surface of a Class II resin composite restoration (>1-year old) was also compared. Two sets

21
of the three surfaces; ceramic, resin composite and enamel, were compared within one subject. In all, 18 sets of ceramic and enamel were compared, 12 of which also included resin composite.
Study Designs
Paper I and V: The evaluations comprised a cross sectional study, investigating the effect of customary oral hygiene on dental biofilm removal and the gingival state adjacent to the included material and the enamel surfaces, and a ten-day experimental study in which the subjects refrained from oral hygiene to allow dental biofilm formation and subsequent initiation of gingivitis. Descriptive data of the subjects were recorded at the start of the study. The clinical parameters measured were intra-individually compared between the surfaces of CAC (Paper I) or leucite-reinforced, resin-bonded ceramic (Paper V), resin composite and enamel in the cross sectional study and on days 0, 3, 7, and 10 of the experimental gingivitis study (Fig. 1)
Cross Sectional Experimental gingivitis
Day 0 Day 3 Day 7 Day 10
1. GCF GCF GCF GCF GCF
2. GI ** GI GI GI GI
3. GBI*
4. QHI QHI QHI QHI QHI
5. PI*
6. SBI SBI
7. PPD PPD
8. DMFS*
Fig 1. Distribution of the clinical parameters included during the study period.
Sampling of gingival crevicular flow (GCF), Gingival Index (GI, Löe 1967),
gingival bleeding index (GBI; Ainamo and Bay 1975), modified Quigley-
Hein’s plaque index (QHI; Turesky 1970), plaque index (PI; Lenox and
Kopzcyk 1973), sulcus bleeding index (SBI; Mühleman 1971), probing pocket
depth (PPD). Descriptive variable of oral characteristics (*). The numbers
indicate the chronological orders of measuring. Healthy gingiva (GI=0),
gingival redness and swelling (GI=1) were estimated as the 2nd
parameter and
gingival bleeding (GI=2) was assessed after the plaque index (**).

22
Collection of GCF
The sites to be collected were isolated with cotton rolls and carefully
sprayed with water to remove saliva. Each site was gently dried using an
air syringe for ten seconds. A paper strip (Periopaper®) was inserted at the
orifice of the gingival crevice and left there for 30 seconds (Paper I) or 10
seconds (Paper V). Fluid volumes were determined from standard curves
using a Periotron 6000® (Paper I) or Periotron 8000® (Paper V) which were
calibrated with certain volumes of human serum.
Paper II and V: The levels of IL-1α, IL-1β and IL-1 ra in the sampled GCF
from each site of CAC, resin composite and enamel in the cross sectional
study and from days 0, 3, 7, (Paper II) and day 10 (Paper V) of the
experimental gingivitis study, as described in Paper I, were analysed,
calculated, and intra-individually compared.
Quigley Hein Plaque Index System
(mod. by Turesky et al. 1971)
Score Criteria
0 No plaque.
1 Separate flecks of plaque at the cervical margin of the
tooth.
2 A thin continuous band of plaque (up to one mm) at the
cervical margin of the tooth.
3 A band of plaque wider than one mm but covering less
than one-third of the crown of the tooth.
4 Plaque covering at least one-third but less than two
thirds of the crown of the tooth.
5 Plaque covering two-thirds or more of the crown.

23
Analysis of Interleukin-1
Immediately after sampling the GCF, the absorbing part of the strip was cut off and transferred to a coded plastic tube. The sample was eluted
twice by adding 50 l 0.9% sodium chloride and centrifuged at 3000 rpm
and 5 ˚C for 20 min. The 100 l supernatant was transferred to a tube
containing 100 l sodium chloride and stored frozen at 80˚ C. The levels of IL-1α, IL-1β and IL-1ra were quantified with Enzyme Linked Immunosorbent Assays (ELISAs) according to the instructions provided by the manufacturer. The supernatants from each individual set of the three sites were similarly diluted and run with the same assay. To calculate the levels of IL-1α, IL-1β and IL-1 ra in the GCF, the dilution factors and the collected volume were taken into account.
Gingival Index System (Löe 1967)
Score Criteria.
0 Normal gingiva.
1 Mild inflammation. Slight change in color, slight
oedema. No bleeding on probing.
2 Moderate inflammation. Gingival redness and
swelling and shiny gingival. Bleeding on probing.
3 Severe inflammation. Marked redness and
oedema. Ulceration. Tendency to spontaneous
bleeding.
24
Paper III: Specimens of three dental composites (QuiXfil, Tetric Ceram, Filtek Supreme), one zinc phosphate cement (Harvard Cement), one glass ionomer cement (Ketac Molar) and one CAC (DoxaDent), were prepared in triplicate, and sterilized with UV-radiation. PVC strips for ISO 10993-5 cytotoxicity test were used as positive and glass specimens as negative control. To be used fresh, half of the specimens was added to the cultures immediately after preparation and sterilization. The other half was preincubated at 37° C, pH 7.2 for seven days in cell culture medium. The culture medium was then removed and the specimens were used for the experiments. The experiments were repeated 6 times, which resulted in 6 observations per material (18 for fresh and 18 for 7 days old specimens).
Cytotoxicity determination
Murine L-929 fibroblasts (5 ml aliquots, containing 3x104 cells/ml), were cultivated in DMEM with 10 % FCS 1% glutamine and 1% penicillin/streptomycin at 37°C/5% CO2 and exposed for the specimens for 72 h in polystyrene 6-well tissue culture plates. The cells were harvested with trypsin, centrifuged and resuspended in 500 µl DMEM. Cells were then counted in a volume of 500 µl DMEM over a fixed time of 30 s with a flow cytometer equipped with an argon laser tuned at 488 nm. Cell numbers after exposure to test specimens were compared to controls (cultures with glass specimens).
Paper IV: Ten days accumulated dental biofilm from the cervical surface of CAC or from the approximal surface of a resin-bonded, leucite-reinforced ceramic, and from the comparable surfaces of resin composite and enamel was collected after preceding water irrigation of the teeth. The plaque was sampled with a tip of a sterile applicator and immersed in 0.5 ml salt buffer (pH 7.2). Each sample was homogenized by pulsed ultrasonic oscillation and then diluted serially in the salt buffer. Aliquots of the samples were cultured on agar plates, which were incubated in 5% CO2 and 95% air at 37º C for two days. Blood agar was used to determine the total counts of bacteria, Mitis salivarius agar supplemented with bacitracin, and Rogosa selective lactobacilli agar were used to estimate mutans streptococci and lactobacilli, respectively. The number of bacteria was counted as colony forming units (CFUs) and the relative number (% of total bacteria) was calculated.

25
Statistics
Paper I: The GCF volumes were analysed by paired t-test, and the
Wilcoxon signed-rank test was used to show differences in plaque and
gingival indices between the materials and enamel. The p-value was set at
0.05 to indicate statistical significance.
Paper II: The concentrations of IL-1α, IL-1β and IL-1 ra were analysed with
Kolmogorov-Smirnov goodness of fit test for normality. Wilcoxon signed
rank test was used for intra-individual comparisons between the materials
and enamels. The p-value was set at 0.05 to indicate statistical
significance.
Paper III: The data were analysed with Analysis of Variance and a post hoc
test, developed by Ryan, Einot and Gabriel, and Welsch. The p-value was
set at 0.05 and at 0.005 regarding multiple testing of the control.
Paper IV: The differences between the materials and enamel regarding
the relative number of mutans streptococci and lactobacilli of the total
bacterial counts were analysed with Wilcoxon signed-rank test and Exact
test (Monte Carlo). The p-value was set at 0.05.
Paper V: The data were analysed with Kolmogorov-Smirnov goodness of
fit test for normality. Wilcoxon signed rank test and Exact test (Monte
Carlo) were used for intra-individual comparisons of plaque index, gingival
index, GCF-volumes, and its concentrations of IL-1α, IL-1β and IL-1 ra. The
p-value was set at 0.05.
In all papers, except for Paper III, the data were processed in SPSS
(Statistical Package for Social Sciences, version 10.0 (Paper I-IV) and
version 13.0 (Paper V). In Paper III, SAS© Release 8.2. was used for the
statistical work.

26
Results
Paper I: In the cross-sectional study, plaque and gingival indices and the
amounts of GCF did not differ between CAC, resin composite and enamel.
An increase (p<0.05) of plaque and gingival indices was found between
day 0 and day 10 of the experimental gingivitis study (Table 1). Neither
the gingival index, nor the amounts of GCF differed between the CAC,
resin composite and enamel on days 0 and 10. In the end of the
experimental gingivitis, dental biofilm was present on all surfaces, but
with a lower plaque index on surfaces of enamel than on surfaces of
calcium aluminate cement (p=0.014) and resin composite (p=0.034).
Table 1. The means of the modified Quigley-Hein’s Plaque Index (QHI), the
Gingival Index (GI), and the gingival crevicular fluid (GCF, μl/30s; standard
deviation), adjacent to calcium aluminate cement (CAC), resin composite and
enamel in the cross-sectional study (CSS) and on days 0, and 10 of the
experimental gingivitis study. * QHI differed significantly between enamel
compared with CAC (p=0.014) and resin composite. (p=0.034).
CAC n Composite n Enamel n
CSS
QHI 0.5 20 0.4 20 0.4 20
GI 0.2 20 0.2 20 0.2 20
GCF 0.31 (0.31) 20 0.36 (0.42) 20 0.21 (0.23) 20
Day 0
QHI 0 18 0 18 0 18
GI 0 18 0 18 0 18
GCF 0.25 (0.30) 18 0.28 (0.33) 18 0.24 (0.26) 18
Day 10
QHI 3.17* 18 3.17* 18 2.83* 18
GI 0.56 18 0.61 18 0.5 18
GCF 0.43 (0.30) 18 0.49 (0.47) 18 0.27 (0.25) 18

27
Paper II: The GCF concentrations of IL-1 α, IL-1 β and IL-1 ra in both the cross-sectional study and the experimental gingivitis study are given in Table. 2. No significant differences were found regarding the IL-1 levels between the materials and enamel. The amount of the supernatants was inadequate to measure IL-1β on day 0. In the experimental gingivitis study, from day 0 to 7, IL-1 α levels increased adjacent to CAC (p=0.011), resin composite (p=0.041) and enamel (p=0.117). The enhanced levels of IL-1 ra were only significant adjacent to resin composite (p=0.002). Table 2. The median concentration (range) of IL-1 α (ng/ml), IL-1 β (ng/ml) and IL-1 ra
(µg/ml) in samples of gingival crevicular fluid adjacent to calcium aluminate cement
(CAC), resin composite and enamel in the cross-sectional study (CSS) and on days 0, 3,
and 7 of the experimental gingivitis study.
CAC n Composite n Enamel n
CSS
IL-1 α 0 (0 – 64.8) 19 0 (0 - 30.2) 19 0 (0 – 201.3) 19
IL-1 β 0 (0 – 17.8) 6 0 (0 – 7.9) 6 0 (0 – 20.5) 5
IL-1 ra 1.6 (0.1 – 8.7) 17 1.3 (0 – 4.8) 17 1.3 (0 – 7.5) 16
Day 0
IL-1 α 0 (0 – 211.1) 16 0 (0 – 134.1) 16 0 (0 – 168.2) 16
IL-1 β - - - - - - - - -
IL-1 ra 0.8 (0 – 24.9) 15 1.0 (0 – 9.4) 15 1.4 (0 – 29.9) 15
Day 3
IL-1 α 9.8 (0 – 287.1) 16 5.8 (0 – 151.9) 16 14.1 (0 – 142.6) 16
IL-1 β 0 (0 – 7.0) 15 0 (0 – 47.0) 15 0 (0 – 8.5) 15
IL-1 ra 2.6 (0.3 – 17.2) 15 1.6 (0.2 – 31.0) 15 2.4 (0.7 – 5.3) 15
Day 7
IL-1 α 28 (0 – 401.0) 16 9.1 (0 – 153.9) 16 12.5 (0 – 147.6) 16
IL-1 β 0 (0 – 12.1) 15 0 (0 – 25.4) 15 0 (0 – 27.6) 15
IL-1 ra 6.0 (1.2 – 22.2) 15 8.6 (2.8 -33.7) 15 5.6 (0 – 70.7) 15

28
Paper III: The six dental direct restorative materials showed different
influences on L-929 fibroblasts cytotoxicity (p<0.0001). The cytotoxicity of
all specimens diminished with increasing preincubation time (p < 0.0001)
but in various degree (p<0.0001). The validity was checked by a positive
control, which reduced cell numbers to 18.7 (±9.8) % of negative control
as expected from previous experiments. All freshly prepared materials
showed reduced cell numbers compared to the negative control. A rank
order of significantly different cytotoxic effects was established for fresh
(Fig. 2a) and 7 days preincubated specimens (Fig. 2b). Fresh specimens of
DoxaDent exhibited the lowest cytotoxicity, followed by QuiXfil and a
group of three materials (Tetric Ceram, Filtek Supreme, Harvard Cement).
Ketac Molar showed the highest cytotoxicity (Fig 2a). As shown in Fig 2b,
after 7 days of preincubation, Harvard Cement and Filtek Supreme
demonstrated more cytotoxicity than the other materials (p < 0.005).
Fig. 2a.
fresh
cell
num
ber
s in
%
0
20
40
60
80
100
120
140
Doxad
ent
***
Quix
Fil
***
Har
var
d *
**
Fil
tek S
upre
me
***
Tet
ric
Cer
am *
**
Ket
ac M
ola
r ***

29
Fig. 2b.
7 days
cell
nu
mb
ers
in %
0
20
40
60
80
100
120
140
Do
xad
ent
Ket
ac M
ola
r *
Qu
ixF
il *
**
Tet
ric
Cer
am *
**
Har
var
d *
**
Fil
tek
Su
pre
me
**
*
Fig. 2a and 2b. Grouping of materials with no different effects: (a) freshly prepared, (b)
7 day preincubated. Specimens were incubated with L-929 fibroblasts for 72 h and cell
numbers determined by flow cytometry. Cell numbers were expressed as a percentage
of controls (cultures with glass specimens). Vertical bars show l second-means ±
standard deviations of 18 observations (= 6 independent experiments with triplicates);
materials covered with the same horizontal bar are not significantly different from each
other. Stars indicate statistical significant difference to control (=100%): *= p<0.05, **
= p<0.01, ***p<0.005 (Because of multiple testing a p-value < 0.005 was considered to
indicate statistical significance for this special question).
30
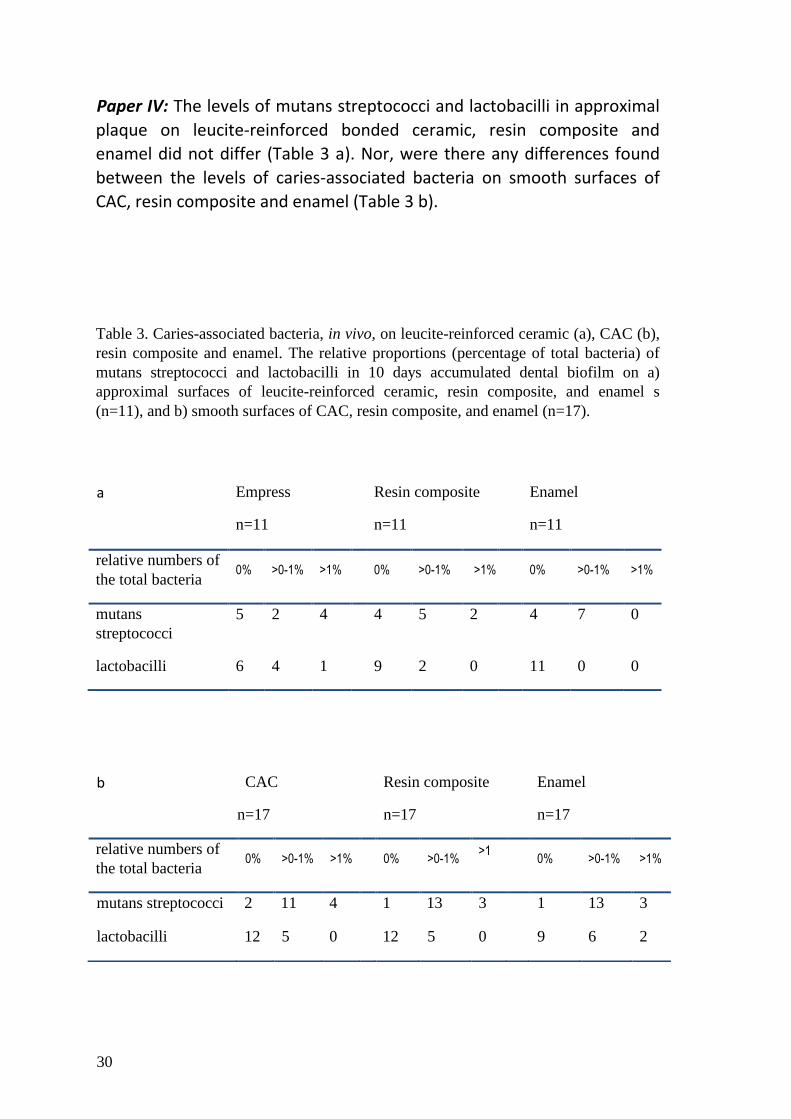
Paper IV: The levels of mutans streptococci and lactobacilli in approximal
plaque on leucite-reinforced bonded ceramic, resin composite and
enamel did not differ (Table 3 a). Nor, were there any differences found
between the levels of caries-associated bacteria on smooth surfaces of
CAC, resin composite and enamel (Table 3 b).
Table 3. Caries-associated bacteria, in vivo, on leucite-reinforced ceramic (a), CAC (b),
resin composite and enamel. The relative proportions (percentage of total bacteria) of
mutans streptococci and lactobacilli in 10 days accumulated dental biofilm on a)
approximal surfaces of leucite-reinforced ceramic, resin composite, and enamel s
(n=11), and b) smooth surfaces of CAC, resin composite, and enamel (n=17).
a
Empress
n=11
Resin composite
n=11
Enamel
n=11
relative numbers of
the total bacteria 0% >0-1% >1% 0% >0-1% >1% 0% >0-1% >1%
mutans
streptococci
5 2 4 4 5 2 4 7 0
lactobacilli 6 4 1 9 2 0 11 0 0
b CAC
n=17
Resin composite
n=17
Enamel
n=17
relative numbers of
the total bacteria 0% >0-1% >1% 0% >0-1%
>1
% 0% >0-1% >1%
mutans streptococci 2 11 4 1 13 3 1 13 3
lactobacilli 12 5 0 12 5 0 9 6 2

31
Paper V: Plaque and gingival indices did not differ between approximal
surfaces of bonded ceramic, resin composite and enamel in the cross-
sectional study and on days 0 and 10 of the experimental gingivitis study.
Sites adjacent to ceramic surfaces showed a significantly higher amount of
GCF compared with enamel in both the cross sectional study (p=0.017),
and day 0 (p=0.019) and day 10 of the experimental gingivitis study
(p=0.016). Each of these parameters increased significantly between day 0
and 10 of the experimental gingivitis study at sites of ceramic restorations
(p<0.001), resin composite restorations (p<0.009) and enamel control
surfaces (p<0.002). Descriptive data are shown in Table 4.
The levels of IL-1 α, IL-1 β and IL-1 ra in the GCF did not differ between the
ceramic, resin composite and enamel surfaces neither in the cross-
sectional study, nor on days 0 and 10 of the experimental gingivitis study.
IL-1 α increased at ceramic sites (p=0.024), resin composite sites (p=0.034)
and enamel sites (p=0.028) from day 0 to day 10 of the experimental
gingivitis. IL-1 ra also increased at the resin composite sites (p=0.027).
Descriptive data are shown in Table 5.

32
Table 4. The means of the modified Quigley-Hein Plaque Index (QHI), Gingival Index
(GI), and gingival crevicular fluid (GCF; μl/10s; standard deviation) adjacent to
approximal surfaces of a leucite-reinforced ceramic, resin composite and enamel in the
cross sectional study (CSS) and on days 0 and 10 of the experimental gingivitis study. n
= number of sets of the intra-individually compared surfaces of ceramic and enamel
(n=18), also including the evaluated composite subgroup (n=12).
* p< 0.05
Ceramic Composite Enamel n
CSS
QHI 0.94
1.1
-
0.83
1.06
1.4
18
12
GI 0.61
0.75
-
0.5
0.28
0.42
18
12
GCF
0.49 (0.10) *
0.49 (0.41)
-
0.32 (0.36)
0.22 (0.23 ) *
0.24 (0.23)
18
12
Day 0
QHI 0. 33
0.1
-
0.1
0.43
0.1
16
12
GI 0
0
-
0
0
0
16
12
GCF 0.30 (0.33) *
0.23 (0.25)
-
0.18 (0.26)
0.13 (0.19) *
0.19 (0.16)
16
12
Day 10
QHI 2.62
2.67
-
3.33
3.06
3.17
16
12
GI 1.00
1.00
-
1.08
0.93
0.83
16
12
GCF 0.82 (0.41) *
0.78 (0.34)
-
0.51 (0.54)
0.49 (0.38) *
0.44 (0.37)
16
12

33
Table 5. The median concentration (range) of interleukin (IL) -1 α (ng/ml), IL -1 β
(ng/ml) and IL-1 receptor antagonist (ra; µg/ml) in samples of GCF adjacent to ceramic,
resin composite and enamel in the cross-sectional study (CSS) and on days 0 and 10 of
the experimental gingivitis study. The digit zero (0) represents all values below the
detection levels (IL-1α, IL-1 β, < 1 pg/ml; IL-1 ra < 14 pg/ml) of the assays. n =
number of sets of the intra-individually compared surfaces of ceramic and enamel, also
including the evaluated composite subgroup.
Ceramic Composite Enamel n
CSS
IL-1 α 15.0
15.6
(0 - 64.6)
(0 - 64.6)
-
2.7
(0 - 273.0)
22.5
57.8
(0 - 98.3)
(0 - 98.3)
18
11
IL-1 β 17.2
9.5
(0 - 117.4)
(0 - 55.4)
-
2.6
(0 - 154.9)
22.6
27.8
(0-1088.7)
(0 - 123.0)
16
9
IL-1 ra 1.3
1.3
(0 - 6.7)
(0 - 6.7)
-
1.4
(0 - 14.3)
2.1
2.4
(0 - 24.3)
(0 - 24.3)
17
11
Day 0
IL-1 α 1.0
2.5
(0 - 49.3)
(0 - 49.3)
-
0
(0 - 131.6)
0
0
(0 - 60.5)
(0 - 60.5)
16
12
IL-1 β 0.7
0
(0 - 33.0)
(0 - 29.5)
-
4.9
(0 - 62.5)
0
0
(0 - 297.5)
(0 - 17.5)
14
9
IL-1 ra 0.8
1.3
(0 - 5.0)
(0 - 5.0)
-
0.7
(0 - 3.1)
1.2
1.0
(0 - 6.3)
(0 - 6.3)
15
10
Day 10
IL-1 α 13.5
19.4
(0 - 113.9)
(1.0 - 113.9)
-
17.3
(0 - 109.0)
10.8
10.8
(0 - 380.6)
(0.9 - 102.0)
16
12
IL-1 β 7.4
8.8
(0 - 63.7)
(0 - 63.7)
-
15.6
(5.4 – 89.6)
6.5
2.5
(0 - 206.7)
(0 - 145.2)
14
9
IL-1 ra 1.4
1.8
(0 - 5.7)
(0.1- 5.7)
-
3.4
(0.5 – 7.1)
2.2
5.4
(0 - 58.0)
(0 - 15.6)
15
10

34
Discussion
The discussion of this thesis focuses on the influence of ceramic
restorative surfaces on dental biofilm formation, subsequent gingival
response and on the caries-associated microflora in vivo. Although
discussed in the same context, leucite-reinforced ceramic and CAC are
totally different types of ceramic materials with regard to their contents,
manufacturing, handling properties and indications for use. The evaluated
ceramic surfaces were compared with resin composite, as a reference
material, and with enamel, as a control, which are both involved in the
discussion. Influence of dental materials on biofilm and gingiva is only a
part of their biocompatibility. At development of a new, alternative
restorative material, its fundamental biocompatibility on a cellular level
should be evaluated. Therefore, even the cytotoxicity of the CAC on
fibroblasts is discussed briefly.
Biofilm formation on CAC (Paper I)
In the in vivo studies described in Paper I and II, an experimental version
of the CAC in the oral environment on smooth, mainly buccal, tooth
surfaces was evaluated. Restorations of both CAC and resin composite
assembled higher amounts of biofilm than enamel after ten days of
neglected oral hygiene (Paper I). In this way the CAC does not seem to be
a superior alternative to resin composite. The clinical relevance of the
differences of the dental biofilm amounts can be considered as small, but
not necessarily scanty in individuals with poor oral hygiene and many
restorations. Still, among individuals with good to moderate oral hygiene,
the buccal/lingual surfaces seem to be possible to clean satisfactorily with
current oral hygiene irrespective of the underlying surface material.
The initial bacterial adhesion is dependent on the physiochemical
properties of the pellicle, which can be influenced by the nature of the
underlying hard surface (Teughels, 2006). Dental biofilm formation in the
first hours can be affected by the surface energy (Quirynen 1995).
However, after six hours of pellicle formation surface, differences
between various dental materials seem to be camouflaged (Hannig 1997)
and a similar biofilm forms within 24 hours (Hannig 1999). After several
days of dental biofilm formation, differences in the amounts of dental

35
biofilm could rather be explained by the roughness of the underlying
surface. Increased surface roughness or porosities and voids of the intra-
oral hard surfaces can facilitate biofilm formation, probably because of a
larger surface area or by affecting the bacterial retention. Dental biofilm
amounts in the defects might function as “plaque reservoirs”, which can
enhance the biofilm formation (Quirynen 1989, 1995). The range in
surface roughness of different hard surfaces is wide (Bollen et al. 1997).
CAC has a heterogenous structure with porosities (Geirsson et al. 2004 b)
which makes it difficult to obtain a surface with low surface roughness,
without chips, pits and grooves, even after finishing (Sunnegård-Grönberg
and van Dijken 2003), which might have contributed to the enhancement
of biofilm formation after ceased oral hygiene.
To summarize, as regards the biofilm formation on Class V restorations of
CAC, this material can be considered as an acceptable one in parity with
resin composite. Without a proper oral hygiene, it could be valuable to
pay attention to possible accumulations of biofilm on available restorative
surfaces of CAC, as well as on surfaces of resin composite.
Biofilm formation on bonded ceramic (Paper V)
With or without oral hygiene, similar amounts of biofilm were present on
the approximal surfaces of the bonded ceramic coverages, as compared to
enamel. That observation is in accordance with clinical follow-ups of
leucite-reinforced ceramic restorations (Sjögren et al. 1999, Stenberg and
Matsson 1993, Tidehag and Gunne 1995). Nevertheless, higher GCF
amounts were found adjacent to the bonded ceramic than adjacent to
enamel (Paper V). As discussed in this paper, there could be a possible
effect of the misallocation of the included restorations. Most ceramic
coverages were placed in molars as compared to resin composite and
enamel surfaces, which were both mainly located in premolars. Molars
have wider approximal contacts, not accessible to ocular surveys.
Therefore, it could be theorized, that the increased amounts of the GCF
were evoked by a response to “hidden” biofilms on the approximal
surfaces. Another reason for this response may be non-detected
overhangs formed by resin composite luting agents (O’Rourke et al. 1995)
and marginal deficits, which can be present irrespectively of the luting
cement used (Krämer and Frankenberger 2005). Overhanging margins can

36
result in enhanced plaque and gingival indices (Lang et al. 1988).
Observations have been made of a slight overextension just above the
cervical margin of 1-2 years old leucite-reinforced ceramic crowns with
subgingival finish lines (Gemalmaz and Ergin 2002) and of approximal
marginal excess of luting cement on radiographs of ceramic inlays
(Pallesen and Dijken, van 2000).
The degradation of dental ceramics generally occurs because of
mechanical forces or chemical attack. Nevertheless, the chemical
durability of dental ceramic is excellent, except for excessive exposure to
acidulated fluoride (Anusavice 1992). To put the light of what is known
about ceramics and dental biofilm formation, even other ceramics than
the evaluated leucite-reinforced ceramic is involved in the discussion. The
dental biofilm formation in vivo on glazed glass ceramics and shaded
sintered ceramics seems to be similar (Castellani et al. 1996, Hahn et al.
1993). In contrast, Hahn et al. (1992) found that biofilm formation differs
between glazed and polished ceramics of various bulk materials.
Over the years, plaque index, bleeding on probing and pocket depth
adjacent to inlays were increasing. Marked wear of ceramic inlays has
been observed at aging. In addition, the surface roughness might increase
because of grinding or finishing at luting (Pallesen and Dijken, van 2000).
With the exception of glazed surfaces, the surface roughness of ceramic
materials can affect the biofilm formation (Kawai et al. 2000). Recently,
preliminary results show a larger tendency to accumulate biofilm on
glazed zirconium ceramics than on the polished ones (Scotti et al. 2006).
Less dental biofilm formation on glazed ceramic surfaces than on non-
glazed ceramic surfaces has been reported (Castellani et al. 1996).
However, marginal defects and wear of the visible part of the approximal
surfaces were only found in a minority of the current restorations in the
clinical follow-up (Dijken van et al. 2001).
Evaluations of biofilm formation on ceramics in comparison with resin
composite are sparsely reported. In vitro, lower amounts of bacteria and
glucans adhere to surfaces of ceramic than to surfaces of resin composite
(Kawai and Urano 2001). It has been observed that the total counts of the
facultative bacteria do not differ between buccal surfaces of ceramic and
restorative composite in situ (Tanner et al. 2005). In Paper V, a similar
37
biofilm formation on approximal surfaces of ceramic and resin composite
restorations was noted.
The dental biofilm formation can be favoured at gingivitis (Quirynen
1991), probably because of an increased supply of the nutrient GCF
(Marsh 2003). Despite the higher amounts of GCF adjacent to the bonded
ceramic surfaces as compared to enamel, the dental biofilm formation on
the visible part of the surface was not enhanced (Paper V). Although the
difference in the supply of GCF can be considered as small, this might
possibly support the observations of a retarded biofilm formation in vivo
on ceramic restorations compared to enamel (Hahn et al. 1993) or
contralateral teeth (Savitt et al. 1987, Jensen et al. 1990). If so, this
advantage of the ceramic material is probably counteracted by side-
effects such as aging/abrasion and luting/bonding, since lower amounts of
dental biofilm on the bonded ceramic coverages than on enamel failed to
be shown.
Thus, resin-bonded ceramic coverages were not shown to disfavour the
biofilm formation, which implicates that the choice of leucite-reinforced
ceramics as a restorative material should rely on other factors. The need
for accurate oral hygiene on this material is not reduced as compared to
that on resin composite and enamel.
The gingival response at sites of CAC and the bonded ceramic
(Paper I, II, V)
The higher biofilm amounts on the surfaces of CAC and of resin composite
than on enamel did not result in corresponding higher amounts of GCF
(Paper I) and its levels of IL-1α, IL-1β and IL-1ra (Paper II). However, in the
end of the biofilm formation period, a non-significant tendency towards
higher crevicular fluid amounts adjacent to the CAC and resin composite
was observed as compared to the remaining low volumes adjacent to the
enamel (Paper I). The higher amounts of GCF at bonded ceramic sites
than at enamel sites were not reflected in higher levels of IL-1α, IL-1β and
IL-1ra (Paper V). There are no available reports in vivo as concerns the
levels of proinflammatory cytokines in GCF adjacent to dental materials.
Lipopolysaccharides, which can initiate a variety of biological responses,
including IL-1, have been shown to have an affinity for resins, alloys, and
even dental ceramics, which could contribute to an inflammatory process

38
(Robinson et al 1996). However, no significant influence of the ceramic
specimens on the response of IL-1 β release from gingival fibroblasts has
been reported in vitro (Ozen et al. 2005).
Restorative surfaces below the gingival margin are associated with
gingivitis (Schätzle et al. 2000), ceramic restorations too (Gemalmaz and
Erging 2002, Reitemeier et al. 2002). The cervical margin of the current
evaluated sub-gingival fillings was not deep extended in an apical
direction. The clinical expressions of gingivitis seem to be mainly low, and
not influenced by the presence of the bonded ceramic and CAC (Paper I
and V). This is also supported by the fact that a low gingival index was
observed both at baseline and after four years for glass ceramic crowns
(Kelsey et al. 1995). That is satisfactory, since gingivitis is a prerequisite of
developing periodontitis (Kinane et al. 2006), and, in elder people
considerably more attachment loss was found at sites with bleeding on
probing (Gingival Index 2) than at sites with a Gingival Index 0 (Schätzle et
al. 2003).
As a whole, the clinical gingival health and the levels of IL-1 do not seem
to be affected by the CAC restorations or the resin-bonded ceramic
coverages, neither at current oral hygiene, nor at initiation of gingivitis.
Secondary findings of dental biofilm formation and gingival response
(Paper I, II, V)
A few issues, not primarily associated with the general aims, will be discussed, that is, the general findings over the experimental gingivitis period, and the discussion as concerns the reference material of resin composite. Dental biofilm formation during experimental gingivitis has shown to be followed by an enhancement of GCF (Zhang et al. 2002) without respect to resin composite and enamel (Dijken van et al. Sjöström 1998). The increase in GCF was also obvious in the study of the approximal surfaces (Paper V), but not significant at the buccal/lingual surfaces evaluated in Paper I. The levels of IL-1α were enhanced during the experimental gingivitis (Paper II and Paper V), which has also been observed previously (Kinane et al 1992). An increase in IL-β during experimental gingivitis has been shown (Deinzer et al. 1999, Gonzales et al. 2001, Zhang et al. 2002).

39
Nevertheless, a significant increase in IL-1 β failed to be demonstrated, to a part, probably because of a low number of sites analyzed (Paper II). Although Wilton et al. (1992) could not correlate IL-1 levels with the plaque and gingival index, Hou et al. (1995) observed a considerable increase in the amount of IL-1β at bleeding sites compared to sites with a Gingival Index < 2. No gingival bleeding could be applied to most of the current evaluated sites (Paper I and V). IL-1α (Rasmussen et al. 2000) and IL-1β (Boström et al. 2000, Gamonal et al. 2000, Hou et al. 1995, Orozco et al. 2006) are associated with inflammation on a periodontitis level but not always detected in the control group of clinically healthy individuals (Gamonal et al. 2000, Wilton et al. 1992). There are contradictory findings regarding the levels of IL-1ra in GCF, at healthy versus inflammatory sites. Higher levels of IL-1 ra have been found at periodontitis sites than at non-inflamed gingival sites (Boström et al. 2000, Ishihara 1997) in divergence to Rawlinson et al. (2000). Experimental gingivitis does not seem to exert effects on the levels of IL-1 ra (Waschul et al. 2003). Among the current findings, increase in IL-ra was only found adjacent to Class V restorations of resin composite (Paper II), but the enhancement was not present at approximal sites (Paper V). The levels of IL-1 ra in GCF were approximately 1000-fold that of IL-1, which is in accordance with Boström et al. (2000). Other cytokines may also contribute to the balance between the production of IL-1 and of IL-1 ra in disease. For example, IL-4 TGF beta and IL-10 increase the production of IL-1 ra but at the same time decrease the production of IL-1 (Dinarello and Wolff 1993).
The higher amounts of dental biofilm, on smooth, cervical surfaces of resin composite as compared to enamel, (Paper I) were not demonstrated on approximal surfaces (Paper V). It is possible, that the approximal surfaces of resin composite compared to the buccal or lingual ones are less exposed for wear and roughening from abrasion via tooth-brushing, which preserves a relatively smooth surface (Folwaczny et al. 2000). When comparing the evaluations in these papers (Paper I and V), one should bear in mind that these studies did not take into consideration the individual variations caused by contributing factors, such as smoking. Aging of resin composite restorations can result in increased dental biofilm retention and degraded surfaces which may favour bacterial recolonization and complicate dental biofilm removal (Dijken van et al. 1985, Dijken van et al. 1987a). On early dental composites, dental biofilm forms more easily than on enamel (Larato 1972). Besides, subgingival resin composite restorations may have some negative effects on the quantity and quality of the plaque, increasing the anaerobic microflora

40
(Paolantonio et al. 2004). Several studies did not reveal any differences in dental biofilm formation (Hahn et al. 1993) or subsequent clinical signs of gingivitis between sites of resin composites and enamel (Dijken van et al. 1987 a, Dijken van et al. 1987 b, Dijken van and Sjöström 1991 b, Dijken van and Sjöström 1998). Nor were there any differences of the gingival response observed between the sites of resin composite and enamel (Paper V). In contrast, less amounts of GCF have been collected at sites of enamel than at sites of resin composite restorations (Dijken van et al. 1987 a, Dijken van et al. 1987 b, Dijken van and Sjöström 1991 b).
Caries-associated bacteria on CAC and bonded ceramic (Paper IV)
Strategies to control caries include the inhibition of biofilm development
such as prevention of attachment of cariogenic bacteria, or enhancement
of the host defences (Marsh 2006). The proportions of mutans
streptococci and lactobacilli in approximal dental biofilm on CAC and on
aged, resin-bonded ceramics resembled those on resin composite and
enamel. These materials did not influence the caries-associated microflora
(Paper IV). The most frequent proportions of mutans streptococci and
lactobacilli observed in this thesis were below 1%, irrespective of the
underlying material. In vivo, the counts of mutans streptococci have not
been showed to be different on buccal surfaces of ceramic and of
restorative composites (Tanner et al. 2005). In vitro, a normal oral flora
has been able to colonize resin materials (Suljak et al. 1995), which in
cultures, however, might have a growth-enhancing effect on mutans
streptococci (Friedl et al. 1992) and on lactobacilli (Hansel et al. 1998).
The lack of influence of the bonded ceramic on the caries-associated flora
is not surprising, since ceramics are considered to be chemically stable. As
discussed in Berglund et al. (2006), a depletion of calcium (Ca) and an
increase in other elements (Al, Si, and Zr) have been found on the surface
of wet specimens of CAC. However, the leakage of components from the
CAC has not been extensively investigated.

41
The cytotoxicity and biocompatibility of the CAC (Paper III)
The CAC was developed in the end of the nineties as a “bioceramic”
restorative material, aimed to be an alternative to the current filling
materials which might have a cytotoxic potential (Ferracane 1994,
Wrangsjö 2001). The cytotoxicity of the CAC on fibroblasts was lower than
that of various resin composites as concerns fresh filling materials (Paper
III). The disparity decreased in time. After one week, only one resin
composite material (Filtek Supreme) and the phosphate cement, which is
used as a temporary material, demonstrated significantly more cytotoxic
effects than the CAC. However, the CAC was the only material which did
not differ from the control. In this way, the CAC seems to be highly
biocompatible.
At present, the use of the CAC as a restorative material is contra-indicated
due to the deficient dimensional stability over time (Berglund et al. 2006),
inferior mechanical properties (Geirsson et al. 2004 a, Sunnegård-
Grönberg 2004) and short clinical durability (Sunnegård- Grönberg 2004).
However, attempts have been made to use CAC, slightly modified, as a
biomaterial in the other parts of the body, such as bone cement (Oh et al.
2002).
Thus, in vitro, fresh CAC exhibited the lowest cytotoxicity compared with
other current dental materials. All materials showed diminished
cytotoxicity over time. Although slightly cytotoxic, CAC can be considered
as a biomaterial, which suggests further development to overcome its low
mechanical properties.
General discussion of the methods
The studies (Paper I, II, IV, and V) were performed in an intra-individual
approach, comparing surfaces within each individual, and ruling out
possible host and life-style factors, which could have an impact on the
results. For example, inter-individual variations are observed as concerns
rate of dental biofilm formation and the development of gingivitis
(Simonsson et al. 1987, Trombelli 2004) and the genotypes of IL-1 (Shapira
2005). Furthermore, GCF flow and IL-1α levels (Kinane and Chestnut
2000), gingival index and bleeding scores (Preber and Bergström, 1986, Lie

42
et al. 1998) are reduced in heavy smokers. The intra-individual study
design decrease the number of participants needed for inclusion.
Efforts were made to compare similar surfaces fulfilling the inclusion
criteria. According to the ecological plaque hypothesis (Marsh 2004), the
local environment is not identical with other sites in the oral cavity. There
are variations in the biofilm composition of smooth surfaces, fissures,
gingival sulcus, in sites close to saliva excretion, and in sites differing in
redox potential or nutrient availability (Arweiler et al. 2004). Besides,
there is an impact of the intra-oral location on the rate of biofilm growth
(Furuichi et al. 1992, Quirynen et al.1991). However, the thickness of the
buccal biofilm does not seem to be related to the location in the oral
cavity (Auschill et al. 2004). With oral hygiene, a relatively good
symmetrical plaque pattern has been observed, however, the plaque per
cent of the tooth area differed between the adjacent first and second
molars (Söder et al. 2003).
Alternative methods to evaluate restorative materials in vivo, are the use
of attached splints, such as in studies of Hahn et al. (1992), or with
temporarily bonded specimens (Tanner et al. 2005), which make it
possible to evaluate different restorative materials at the same site or
location. However, these methods did not, in full, mirror the clinical
situation and the influences of ageing of the restorations. Furthermore,
the local oral environment can be changed in course of time due to
alterations of life-style related factors.
The development of gingivitis is associated with the quantity of the dental
biofilm (Löe et al. 1965, Lie et al. 1998). In both Paper I and V, the plaque
index used measures the extent of the dental biofilm covering the tooth
based on a scale of six steps (Turesky et al. 1970) and quantification
indices are considered to be necessary in clinical trials (Galgut 1999). An
interval-scaled plaque index, developed for approximal surfaces (Matthijs
et al. 2001, Dombret et al. 2003), might have been more appropriate to
utilize in the study of bonded ceramics (Paper V). However, that index
was not well-established at the time for measuring. The thickness and
alterations of the quality of the dental biofilm during experimental
gingivitis were not evaluated in the involved studies (Paper I and V).
Nevertheless, a weak or strong inflammatory response to experimental

43
gingivitis is not caused by major differences in the composition of the oral
microbiota (Lie et al. 1998).
The length of the experimental gingivitis period was based on previous
studies (van Dijken et al. 1987a, 1987 b, Dijken van and Sjöström 1991 b,
Dijken van and Sjöström 1998). If requested, the opposite arch was
polished after measuring to support the compliance. That might have
decreased the rate of dental biofilm formation with a subsequent delay of
the development of gingivitis (Quirynen 1989). Moreover, there are
differences in the gingival response to biofilm between low- and high-
responders (Trombelli 2004). The distribution of low- and high responders
in the study group is not known. However, at the start of the studies, the
full mouth recorded gingival index was mainly low, as compared to the
plaque index. The benefit of a further length of the experimental gingivitis
period can be discussed; however, the primary aim was to compare the
ceramic material under the prevailing conditions at initiation of gingivitis,
not to evaluate the development of gingivitis per se.
The gingival index (Löe and Silness 1965, Löe 1967) is probably the most
widely used index in clinical trials (Ciancio 1996). The determination of the
volumes of GCF with Periotron® is a reliable method (Bickel and Cimasoni
1984), at least at volumes above 0, 2 µl (Chapple et al. 1995) and at
appropriate calibration and handling of the apparatus (Ciantar and
Carauna 1998). Presence of biofilm at collection of GCF can elevate the
measured levels (Stoller et al. 1990), but later it is reported that the
validity of the measurements was not affected by the presence of
supragingival dental biofilm (Deinzer et al. 2000). It is necessary to
distinguish between the initial collected volume of GCF, and its flow rate,
of which the latter could be associated to the Gingival Index and can be a
preferable method (Griffiths et al. 1992). Various tooth types associated
with different sulcus depth or sampling areas might also have an impact
on the sampling of the fluid. However, at collection of the fluid, there was
a great attempt to insert the paper strips until the same depth of the
sulcus. Besides, there is a risk of stimulating the gingival flow at repeated
measures. Not to surpass the potential collection volume of the paper
strip, the time for collection of the GCF was determined in a pilot study,
that is, 30 s for buccal/lingual sites (Paper I) and 10 s for approximal sites
(Paper V). The protein recovery from various paper types used to collect
GCF can vary, and low protein concentrations are less efficiently eluted

44
from the paper strips than high protein concentrations. Although another
type of collecting papers might be more efficient for protein recovery
(Johnson et al. 1999), the used paper strips were adapted to measure the
fluid volume with Periotron® and the papers have been used previously at
sampling of IL-1 (Deinzer et al. 1999, Waschul et al. 2003). It has to be
noted that the measures of the GCF are related to be surrogate measures,
such as the Gingival Index or other measures of gingival inflammation
(Socransky and Haffajee 2005).
Conventional methods of culturing caries-associated bacteria on selective
media and in an aerobic environment supplemented with carbon dioxide
were used (Paper IV). It could be discussed, if culturing the lactobacilli
under anaerobic conditions would be more appropriate for optimal
growth. Though almost all lactobacilli are facultatively anaerobic bacteria
and thus grow both under aerobic and anaerobic conditions, it is known
that the growth is enhanced in an anaerobic or a microaerophilic
environment. However, optimizing growth conditions not necessarily
mean that a higher number of lactobacilli is detected. A pilot study further
supported this assumption. Thus, the outcome of lactobacilli detection
hardly would have been different if an anaerobic incubation had been the
first choice.
More sensitive or sophisticated tests can also be used, such as molecular
biology tests to characterize the quality of the biofilm. In Paper III, the
applied method for cytotoxicity testing of the dental materials was cell
counting by flow cytometry (Schedle et al.1998, Franz et al. 2003)
comprising cells which were not lyzed by apoptosis and/or necrosis. At
flow cytometry, the analysis is performed of a large numbers of cells at a
single-cell level. The measurements are quantitative and, in addition,
many cell parameters can be evaluated simultaneously. Cytotoxicity tests
can also rely on tests of the cell viability measuring cellular metabolic
activity and functional state of the mitochondria such as in Lönnroth et al.
(2001). Nevertheless, to be used as preliminary and as initial tests on the
influence of the restorative materials in comparison to other materials or
controls, the test method used is established and makes the study
comparable to previous studies evaluating restorative materials (Schedle
et al. 1998, Franz et al. 2003).
With the limitations of the methods discussed in mind, the results should
be interpreted carefully.

45
From studies in this thesis, recurrent findings of “no significant differences
between the evaluated materials and enamel” are reported. The bias
against publishing ‘negative’ results has a tremendous impact on the
literature, and recognition of the importance of such results is needed
(Kinane et al. 2005).
By nature, this thesis is focused on a limited part of the influences of
restorative materials on the oral health. One has to bear in mind the
importance of applying any side-effects of the restorative material in a
holistic approach to the oral environment and to the patient, which is
after all necessary to establish and maintain a good oral health.
46
Conclusions
The main conclusions from the findings of this thesis are as follows:
The low cytotoxic effect of CAC and the limited increase in dental biofilm formation on that material compared with enamel suggest CAC to be a biocompatible dental material with respect to dental biofilm formation, presence of caries-associated microflora and gingival response. This finding, together with the observation that the influence of bonded ceramic on dental biofilm formation, caries-associated microflora and clinical gingivitis was not different from that of enamel, implicates for both CAC restorations and bonded ceramic that the need of oral hygiene is not reduced.

47
Acknowledgements
I wish to express my sincere gratitude to my family, all colleagues and friends who have supported me during these years. In particular, I would like to thank:
Professor Jan van Dijken, my supervisor, for introducing me to the world of research, provoking a critical approach, and giving me opportunities to compass this work. Your driving energy to force projects forward is appreciable.
Rolf Claesson, my co-supervisor and co-author, for invaluable help and support. Thanks for providing your place of work at the laboratory, volunteering your professional skill and for worthwhile discussions on research, music and life, and to lengthen my life by humour and laugh.
My co-authors at University Clinic of Dentistry, Medical University, Vienna, Professor Andreas Schedle and Magister Alexander Franz, for giving me insight into a world far from here.
Jörgen Paulander, for teaching and helping with the introductory statistics.
Birgit Andertun and the others at the laboratory of Oral Cell Biology. Thanks for introductions to the ELISA-technique, helpfulness and good advice.
Margaretha Jonsson at the laboratory of Oral Microbiology, for microbiological analysis.
Karin Sunnegårdh-Grönberg for serious discussions on research in the introductory phase of the work.
Staffan Sjöström for advice, support and worthwhile discussions when planning this project. Thanks for arousing my interest in periodontology.
Anitha Persson, my previous teacher and current colleague for mentorship and belief in my ability from the very beginning as a student.
Noomie Hällsten-Nilsson, for your kindness, friendship and encouragement and for good collaboration on dealing with student groups at the clinic.

48
Elisabeth, Margot, Ruth, Tina and Inger, for your indulgence to me when I have been absorbed in my research.
Ulrika Funegårdh, my previous ‘boss’ for a period, for your empathy and insight into my situation as a PhD student and the team leader Ing-Marie Bernhardsson for your wise opinions and all my fellow-workers at 6th and 7th floor. I appreciate you.
My father, Daniel, for introducing me to books and learning and together with my mother Ingegerd support and encourage me.
My sister Anna, for good help concerning proof readings and details of writing, and for your and your family’s generous attitude.
My sister Åsa and her family for encouragement and support.
My parent- in-law, Anna-May, for being there when I need you.
Fadi, for friendship, encouragement and fruitful discussions, for giving me new insights and reminding me to focus on the important values of life.
The Seimel-Schaitberger family, for all wonderful holidays in the summers. Thanks for all pleasure, trekking, vitamins and herbs. You have supplied energy to this project.
The Lindgren- Karlsson family. Thanks for all relaxing periods with you.
Gaudium, the choir of joy, thank you for patience with me during this work. Still, going singing!
My neighbours. That is a privilege to live in Trehörningen and in good fellowship with you.
The participants in the clinical studies, who made this project possible.
The County Council of Västerbotten, Swedish Dental Association and Doxa Certex for financial support.
My family, Lars, Richard and Sofie. Thanks for everything. I love you!
49
References Acceptance Program Guidelines. Restorative materials. American Dental Association.
Council on Scientific Affairs. March 1996.
Ainamo, J. and Bay, I. (1975) Problems and proposals for recording gingivitis and
plaque. Inter Dent J 25, 229-35.
Alfano, M. C. (1974) The origin of gingival fluid. J Theor Biol 47, 127-36.
Anusavice, K. J. (1992) Degradability of dental ceramics. Adv Dent Res 6, 82-9.
Armitage, G. C. (1999) Development of a classification system for periodontal diseases
and conditions. Ann Periodontol 4, 1-6.
Arweiler, N. B., Hellwig, E., Sculean, A., Hein, N. and Auschill, T. M. (2004) Individual
vitality pattern in situ dental biofilms et different locations in the oral cavity.
Caries Res 38, 442-7.
Auschill, T. M., Hellwig, E., Sculean, A., Hein, N. and Arweiler, N. B. (2004) Impact of
the oral intraoral location on the rate of plaque growth. Clin Oral Investig 8, 97-
101.
Axelsson, P. and Lindhe, J. (1981) Effect of controlled oral hygiene procedures on
caries and periodontal disease in adults. Results after 6 years. J Clin Periodontol
8, 239-48.
Barthold, P. M. (2006) Periodontal tissues in health and disease: Introduction.
Periodontol 2000 40, 7-10.
Berg, J. H., Farrell, J. E. and Brown, L. R. (1990) Class II glass ionomer/silver cermet
restorations and their effect on interproximal growth of mutans streptococci.
Pediatr Dent 12, 20-3.
Berglund, A., Hulterström, A:K:, Gruffman, E. and Dijken van, J. (2006) Dimensional
change of a calcium aluminate cement for porsterior restorations in aqueous
and dry media. Dent Mater 22, 470-6.
Bickel, M. and Cimasoni, G. (1984) Reliability of volume measurements with the new
Periotron® 6000. J Periodont Res 19, 313-6.
Black J. Biocompatibility: Definitions and Issues. In: Biological performance of
materials. Fundamentals of biocompatibility. Ed. J Black, Marcel Dekker Inc,
New York 1999; pp 3-12.
50
Bollen, C. M. L., Lambrechts, P. and Quirynen, M. (1997) Comparison of surface
roughness of oral hard materials to the threshold surface roughness for
bacterial plaque retention: A review of the literature. Dent Mater 13, 258-69.
Boström, L., Linder, L. E. and Bergström, J. (2000) Smoking and GCF levels of IL-1β and
IL-1ra in periodontal disease. J Clin Periodontol 27, 250-5.
Castellani, D., Bechelli, C., Tiscione, E., Lo Nostro, A. and Pierloni, M. D. (1996) In vivo
plaque formation on cast ceramic (Dicor) and conventional ceramic. Int J
Prosthodont 9, 459-65.
Chan, C. and Weber, H. (1986) Plaque retention on teeth restored with full-ceramic
crowns. A comparative study. J Prosthet Dent 56, 666-71.
Chapple, I. L. C., Cross, I. A., Glenwright, H. D. and Matthews, J. B. (1995). Calibration
and reliability of the Periotron 6000 for individual gingival crevicular fluid
samples. J Periodont Res 30, 73-9.
Ciancio, S. G. (1986) Current status of indices of gingivitis. J Clin Periodontol 13, 375-8.
Ciantar, M. and Caruana, D, J. (1998) Periotron 8000: calibration characteristics and
reliability. J Periodont Res 33, 259-64.
Crossner, C. G., Claesson, R. and Johansson , T. (1989) Presence of mutans
streptococci and various types of lactobacilli in interdental spaces related to
development of proximal carious lesions. Scand J Dent Res 97, 307-15.
Daly, C. G., Highfield , J. E. (1996) Effect of localized experimental gingivitis on early
supragingival plaque accumulation. J Clin Periodontol 23, 160-64.
Deinzer, R., Förster, P., Fuck, L., Herforth, A., Stiller-Winkler, R. and Idel, H. (1999)
Increase of crevicular interleukin 1β under academic stress at experimental
gingivitis sites and at sites of perfect oral hygiene. J Clin Periodontol 26, 1-8.
Deinzer, R., Mossanen, B. S. and Herforth, A. (2000) Methodological considerations in
the assessment of gingival crevicular fluid volume. J Clin Periodontol 27, 481-8.
Dijken, J. W. V. van. (1999) All-ceramic restorations: classification and clinical
evaluations. Compend Contin Educ Dent 20, 1115-24.
Dijken, J. W. V. van., Hasselrot, L., Örmin, A. and Olofsson, A. L. (2001) Restorations
with extensive dentin/enamel-bonded ceramic coverage. A 5-year follow-up.
Eur J Oral Sci 109, 222-9.
Dijken, J. W. V. van., Hörstedt, P. and Meurman, J. H. (1985) SEM study of surface
characteristics and marginal adaptation of anterior resin restorations after 3-4
years. Scand J Dent Res 93, 453-62.

51
Dijken, J. W. V. van, Kalfas , S., Litra, V. and Oliveby, A. (1997) Fluoride and mutans
streptococci levels in plaque on aged restorations of resin-modified glass
ionomer cement, compomer and resin composite. Caries Res 31, 379-83.
Dijken, J. van, Persson, S. and Sjöström, S. (1991 a) Presence of Streptococcus mutans
and lactobacilli in saliva and on enamel, glass ionomer cement, and composite
resin surfaces. Scand J Dent 99, 13-9.
Dijken, J. W. V. van. and Sjöström, S. (1991 b) The effect of glass ionomer cement and
composite resin fillings on marginal gingiva. J Clin Periodontol 18, 200-3.
Dijken, J. W. V. van. and Sjöström, S. (1998) Development of gingivitis around aged
restorations of resin-modified glass ionomer cement, polyacid-modified resin
composit (compomer) and resin composite. Clin Oral Invest 2, 180-3.
Dijken, J. W. V. van., Sjöström, S., and Wing, K. (1987 a) The effect of different types of
composite resin fillings on marginal gingiva. J Clin Periodontol 14, 185-9.
Dijken, J. W. V. van., Sjöström, S., and Wing, K. (1987 b) Development of gingivitis around different types of composite resin. J Clin Periodontol 14, 257-60.
Dijken, J. W. V. van. and Sunnegårdh-Grönberg, K. (2004) A calcium aluminate cement as restorative material in Class V cavities. Swed Dent J 28, 111-8.
Dinarello, C. A. (2000) Impact of basic research on tomorrow’s medicine.
Proinflammatory cytokines. CHEST 118, 503-8.
Dinarello, C. A. (2005) Interleukin-1β. Crit Care Med 33, S460-2.
Dinarello, C. A. and Wolff, S. H. (1993) The role of interleukin-1 in disease. N Engl J Med 328, 106-13.
Dombret, B., Matthijs, S., Moradi Sabzewar, M. (2003) Interexaminer reproducibility of ordinal and interval-scaled plaque indices. J Clin Periodontol 31, 630-5.
Embery, G. and Waddington, R. (1994) Gingival crevicular fluid: Biomarkers of
periodontal tissue activity. Adv Dent Res 8, 329-336.
Eley, B. M. and Cox, S. W. (1998) Advances in periodontal diagnosis 5. Potential
inflammatory and immune markers. Brit Dent J 184, 220-3.
Fehr, F. R. von der., Löe, H. and Theilade, E. (1970) Experimental caries in man. Caries
Res 4, 131-48.
Fejerskov, O. (1997) Concepts of dental caries and their consequences for
understanding the disease. Community Dent Oral Epidemiol 25, 5-12.
Ferracane, J. L. (1994) Elution of leachable components from composites. J Oral
Rehabil 21, 441-52.

52
Filoche, S. K., Anderson, S. A. and Sissons, C. H. (2004) Biofilm growth of Lactobacillus
species is promoted by Actinomyces species and Streptococcus mutans. Oral
Microbiol Immunol 19, 322-6.
Foley, J. and Blackwell, A. (2003) Ion release from copper phosphate cement and
influence on Streptococcus mutans growth in vitro: a comparative study. Caries
Res 37, 416-24.
Folwaczny, M., Mehl, A., Kunzelmann, K. H. and Hickel, RT. (2000) Determination of
changes on tooth-colored cervical restorations in vivo using a three-
dimensional laser scanning device. Eur J Oral Sci 108, 233-8.
Franz, A., König, F., Anglmayer, M., Rausch-Fan, X., Gille, G., Rausch, W-D., Lucas, T.,
Sperr, W. and Schedle A. (2003) Cytotoxic effects of packable and nonpackable
dental composites. Dent Mater 19, 382-92.
Fradeani, M., Aquilano, A. and Bassein, L. (1997) Longitudinal study of pressed glass-
ceramic inlays for four and a half years. J Prosthet Dent 78, 346-53.
Friedl, K-H., Schmalz, G. and Hiller, K-A. (1992) Flüssigkeitskulturen zur Prüfung der
Wirkung zahnärtzlicher Werkstoffe auf das Bakterienwachstum. Dtsch
Zahnärstl Z 47, 826-31.
Friedl, K-H., Schmalz, G., Hiller, K.A. and Markl, A. (2000) Marginal adaption of Class V
restorations with and without softstart-polymerization. Oper Dent 25, 26-32.
Furuichi, Y., Lindhe, J., Ramberg, P. and Volpe, A. R. (1992) Patterns of de novo plaque
formation. J Clin Periodontol 19, 423-33.
Galgut, P. (1999) A comparison of different indices used in the clinical assessment of
plaque and gingival bleeding. Clin Oral Invest 3, 96-9.
Gamonal J, Acevedo, A, Bascones, A. Jorge, O. and Silva, A. (2000) Levels of interleukin-
1ß, - 8, and 10 and RANTES in gingival crevicular lfuid and cell populations in
adult periodontitis patients and the effect of periodontal treatment. J
Periodontol 71, 1535-45.
Geirsson, J., Bayne, S. C., Swift, E. J. Jr., Thompson, J. Y. (2004 a) Mechanical property
characterization of a novel directly-placed ceramic restorative material. Am J
Dent 17, 417-21.
Geirsson, J., Thompson, J. Y. and Bayne, S. C. (2004 b) Porosity evaluation and pore
size distribution of a novel directly placed ceramic restorative material. Dent
Mater 20, 987-995.
Gemalmaz, D., and Şule, E. (2002) Clinical evaluation of all-ceramic crowns. J Prosthet
Dent 87, 189-96.

53
Geurtsen, W. (2000) Biocompatibility of resin-modified filling materials. Crit Rev Oral
Biol Med 11, 333-55.
Giannobile, W. V., Al-Shammari, K. F and Sarment, D. P. (2003) Matrix molecules and
growth factors as indicators of periodontal disease activity. Periodontol 2000
31, 125-34.
Gibbons RJ (1984) Microbiol ecology. Adherent interactions which may affect
microbial ecology in the mouth. J Dent Res 63, 378-85.
Gladys, S., Meerbeek, Van B., Lambrechts, P. and Vanherle, G. (2001) Microleakage of
adhesive restorative materials. Am J Dent 14, 170-6.
Gonzáles, J. R., Herrmann, J. M., Boedeker, R. H., Francz, P. I., Biesalski, H. and Meyle,
J. (2001) Concentration of interleukin-1β and neutrophil elastase activity in
gingival crevicular fluid during experimental gingivitis. J Clin Periodontol 28,
544-9.
Graves, D.T. and Cochran, D. (2003) The contribution of interleukin-1 and tumor
necrosis factor to periodontal tissue destruction. J Periodontol 74, 391-401.
Griffiths, G. S. (1992) Associations between volume and flow rate of gingival crevicular
fluid and clinical assessments of gingival inflammation in a population of British
male adolescents. J Clin Periodontol 19, 464-70.
Griffiths, G. S. (2003) Formation, collection and significance of gingival crevice fluid.
Periodontol 2000 31, 32-42.
Hahn, R., Netuschil, L. and Löst, C. (1992). Initiale Plaquebesiedelung keramischer
Restaurationsmaterialien. Dtsch Zahnärtzl Z 47, 330-4.
Hahn, R., Weiger, R., Netuschil, L. and Brüch, M. (1993) Microbial accumulation and
vitality on different restorative materials. Dent Mater 9, 312-6.
Hansen, E. K. (1982) Visible light-cured composite resins: polymerisation contraction,
contraction pattern and hygroscopic expansion. Scand J Dent Res 90, 329-35.
Hanks, C. T., Wataha, J.C. and Sun, Z. (1996) In vitro models of biocompatibility: A
review. Dent Mater 12, 186-93.
Hannig, M. (1997) Transmission electron microscopy study of in vivo pellicle formation
on dental restorative materials. Eur J Oral Sci 105, 422-33.
Hannig, M. (1999) Transmission electron microscopy study or early plaque formation
on dental materials in vivo. Eur J Oral Sci 107, 55-64.
Hansel, C., Leyhausen, G., Mai, U. E. H., and Geurtsen, W. (1998) Effects of various
resin composite (co)monomers and extracts on two caries-asociated micro-
organisms in vitro. J Dent Res 77, 60-7.

54
Heasman, P. A., Collins, J.G. and Offenbacher, S. (1993) Changes in crevicular fluid
levels of interleukin-1β, leukotriene B4, prostaglandin E2, thromboxane B2 and
tumor necrosis factor α in experimental gingivitis in humans. J Periodontal Res
28, 241-7.
Hou, L. T., Lir, C. M. and Rossomando, E. F. (1995) Crevicular interleukin-1 beta in
moderate and severe periodontitis patients and the effect of phase I
periodontal treatment. J Clin Periodontol. 22, 162-7.
Houte, J. van. (1994) Role of micro-organisms in caries etiology. J Dent Res 73, 672-81.
International Standard Organization (1999) Biological evaluation of medical devices:
Part 5, Test for cytotoxicity: in vitro methods. 10993-5, Geneva, Switzerland.
International Standard Organization (1997) Dentistry. Preclinical evaluation of
biocompatibility of medical devices used in dentistry. Test methods for dental
materials. 7405, Geneva, Switzerland.
Ishihara, Y., Nishihara, T., Kuroyanagi, T., Shirozu, N., Yamagishi, E., Ohguchi, M.,
Koide, M., Ueda, N., Amano, K. and Noguchi, T. (1997) Gingival crevicular
interleukin-1 and interleukin-1 receptor antagonist levels in periodontally
health and diseased sites. J Periodont Res 32, 524-9.
Jenkinson, H. F. and Lamont, R. J. (2005) Oral microbial communities in sickness and in
health. Trends Microbiol 13, 589-95.
Jensen, ., Schultes, A., Handelman, S. and Proskin, H. M. (1990) Plaque retention on
Dicor crowns and gingival health evaluated over a 4-year period. Int J
Periodontics Restorative Dent 10, 454-63.
Johnson, R. B., Streckfus, C. F., Dai, X. and Tucci, M. A. (1999). Protein recovery from
several paper types used to collect gingival crevicular fluid. J Periodont Res 34,
283-9.
Kawai, K., Urano, M. and Ebisu, S. (2000) Effect of surface roughness of porcelain on
adhesion of bacteria and their synthesizing glucans. J Prosthet Dent 83, 664-7.
Kawai, K. and Urano, M. (2001) Adherence of plaque components to different
restorative materials. Oper Dent 26, 396-400.
Kelsey, W. P., Cavel, T. P., Blankenau, R., J., Barkmeyer, W. W., Wilwerding, T. M. and
Latta, M. A. (1995) 4-year clinical study of castable ceramic crowns. Am J Dent
8, 259-62.
Kinane, D. F., Winstanley, F. P., Adonogianaki, E. and Moughar, N. A. (1992) Bioassay
of interleukin 1 (IL-1) in human GCF during experimental gingivitis. Arch Oral
Biol 37, 153-6.

55
Kinane, D. F., Chestnutt, I.G. (2000) Smoking and periodontal disease. Crit Rev Oral Biol
Med 11, 356-65.
Kinane, D. F., Hideki, S. and Hart, T. C. (2005) The genetic basis of periodontitis.
Periodontol 2000 39, 91-117.
Kinane, D. F., Peterson, M. and Stathopoulou, G. (2006) Environmental and other
modifying factors of the periodontal diseases. Periodontol 2000 40, 107-19.
Kleinberg, I. (2002) A mixed-bacteria ecological approach to understanding the role of
the oral bacteria in dental caries causation: An alternative to Streptococcus
mutans and the specific-plaque hypothesis. Crit Rev Oral Biol and Oppenheim
Med 13, 108-25.
Krämer, N. and Frankenberger, R. (2005) Clinical performance of bonded leucite-
reinforced glass ceramic inlays and onlays after eight years. Dent Mater 21,
262-71.
Lang, N. P., Kaarup-Hansen, D., Joss, A., Siegrist, B., Weber, H-P., Gerber, C., Saxer, U.
P. and Curilovic, Z. (1988) The significance of overhanging filling margins for the
health status of interdental periodontal tissues of young adults. Schweiz
Monatsschr Zahnmed 98, 725-30.
Larato, D. C. (1972) Influence of a composite resin restoration on gingiva. J Prosthet
Dent 28, 402-4.
Lendenmann, K., Grogan, J., F.G. (2000) Saliva and dental pellicle – a review. Adv dent
Res 2000 14, 22-8.
Lenox, J. A. and Kopczyck, R. A. (1973) A clinical system for scoring a patient’s oral
hygiene performance. J Am Dent Assoc 86, 849-52.
Li, J., Helmerhorst, E. J., Leone, C. W., Troxler, R. F., Yaskell, T., Haffajee, A. D.,
Socransky, S. S. and Oppenheim, F. G. (2004) Identification of early microbial
colonizers in human dental biofilm. J Appl Microbiol 97, 1311-8.
Lie, M. A., Weijden van der, G.A:, Timmerman, M. F., Boss, B. G. van Steenbergen, T. J.
and Velden, U. van der. (1998) Oral microbiota in smokers and non-smokers in
natural and experimentally-induced gingivitis. J Clin Periodontol 25, 677-86.
Liljemark, W. F. and Blomquist, C. (1996) Human oral microbial ecology and dental
caries and periodontal diseases. Crit Rev Oral Biol Med 7, 180-98.
Lindquist, B. and Emilson, C. G. (1990) Distribution and prevalence of mutans
streptococci in the human dentition. J Dent Res 69, 1160-6.
Loesche, W. J. (1986) Role of Streptococcus mutans in human dental decay. Microbiol
rev 50, 353-80.

56
Löe, H. (1967) The gingival index, the plaque index and the retention index systems. J
Periodontol 38, 610-6.
Löe, H., Holm-Pedersen, P. (1965) Absence and presence of fluid from normal and
inflamed gingivae. Periodontics 3, 171-7.
Löe, H., Theilade, E. and Jensen, S. B. (1965) Experimental gingivitis in man. J
Periodontol 36, 177-87.
Lönnroth, E-C., Dahl, J. E. (2001) Cytotoxicity of dental glass ionomers evaluated using
dimethylthiazol diphenyltetrazolium and neutral red tests (2001). Acta Odontol
Scand 59, 34-9.
Macorra, de la J. C. and Pradies., G. (2002) Conventional and adhesive luting agents.
Clin Oral Invest 6, 198-204.
Marsh, P. D. (1994) Microbiol ecology of dental plaque and its significance in health
and disease. Adv Dent Res 8, 263-71.
Marsh, P. D. (2003) Are dental diseases examples of ecological catastrophes?
Microbiology 149, 279-94.
Marsh, P. D. (2004) Dental plaque as a microbial biofilm. Caries Res 38, 204-11.
Marsh, P. D. (2006) Dental plaque as a biofilm and microbial community - implications
for health and disease. BMC Oral Health 6, Suppl 1, S14.
Marsh, P. D. and Bradshaw, D. J. (1995) Dental plaque as a biofilm. J Industrial
Microbiol 15, 169-75.
Marsh, P.D. and Bradshaw, D. J. (1997) Physiological approaches to the control of oral
biofilms. Adv Dent Res 11, 176-85.
Matthijs, S., Moradi Sabzewar, M. and Adriaens, P. A. (2001) Intra-examiner
reproducibility of 4 dental plaque indices. J Clin Periodontol 28, 250-4.
Messer, R. L. W., Lockwood, P. E., Wataha, J. C., Lewis, J. B., Norris, S. and Bouillaguet,
S. (2003) In vitro cytotoxicity of traditional versus contemporary dental
ceramics. J Prosthet Dent 90, 452-8.
Morrier, J. J., Suchett-Kaye, G., Nguyen, D., Rocca, J. P., Blanc-Benon, J. and Barsotti, O.
(1998) Antimicrobial activity of amalgams, alloys and their elements and
phases. Dent Mater 14, 150-7.
Mühlemann, H. R. and Son, S. (1971) Gingival sulcus bleeding--a leading symptom in
initial gingivitis. Helv Odontol Acta 15, 107-13. In: Lindhe J. Clinical
Periodontology and Implant Dentistry, 3rd ed, Munksgaard, Copenhagen 1997,
p.70.
Mjör, I. A. (2005) Clinical diagnosis of recurrent caries. JADA 136, 1426-33.
57
Mjör, I. A., Jokstad, A. and Qvist, V. (1990) Longevity of posterior restorations. Int Dent
J 40, 11-7.
Mjör, I. A., Moorhead, J. E. and Dahl, J. E. (2000) Reasons for replacement of
restorations in permanent teeth in general dental practice. Int Dent J 50, 361-6.
Nadarajah, V., Neiders, M. E. and Cohen, R. E. (1997) Local inflammatory effects of
composite resins. Compend Contin Educ Dent 18, 367-8, 370, 372-4.
Oh, S.H., Choi, S. Y., Lee, Y. K., and Kim., K. N. (2002) Preparation of calcium aluminate
cement for hard tissue repair. Effect on lithium fluoride and maleic acid on
setting behaviour, compressive strength, and biocompatibility. J Biomed Mater
Res 15, 593-9.
O’Rourke, B., Wallis A. W. G. and Wassell, R. W. (1995) Radiographic detection of
overhangs formed by resin composite luting agents. J Dent 23, 353-7.
Orozco, A., Gemmel, E., Bickel, M., Seymour, G. J. (2006) Interleukin-1β, interleukin-12
and interleukin-18 levels in gingival crevicular fluid and serum of patienets with
gingivitis and periodontitis. Oral Microbiol Immunol 21, 256-60.
Ozen, J., Atay, A., Beydemir, B., Serdar, M. A., Ural, U. A., Dalkz, M. and Soysal, Y.
(2005) In vitro IL-1beta release from gingival fibroblasts in response to pure
metals, dental alloys and ceramic. J Oral Rebil 32, 511-7.
Paes Leme, A. F., Koo, H., Bellato, C. M., Bedi, G. and Cury, J. A. (2006) The role of
sucrose in cariogenic dental biofilm formation - new insight. J Dent Res 85,
878-87.
Page, R. C. (1999) Milestones in periodontal research and the remaining critical issues.
J Periodont Res 34, 331-9.
Page, R.C. and Schroeder, H. E. (1976) Pathogenesis of inflammatory periodontal
disease. Lab Invest 34, 235-9.
Pallesen, U. and Dijken, J. W. V. van. (2000) An 8-year evaluation of sintered ceramic
and glass ceramic inlays processed by the Cerec CAD/CAM system. Eur J Oral
Sci 108, 239-46.
Paolantonio, M., D’Ercole, S., Pernetti, G., Tripodi, D., Catamo, G., Serral, E., Bruè, C.,
Piccolomini, R. (2004) Clinical and microbiological effects of different
restorative materials on the periodontal tissues adjacent to subgingival class V
restorations. 1-year results. J Clin Periodontol 31, 200-7.
Poulsen, S., Holm-Pedersen, P., Kelstrup, J. (1979) Comparison of different
measurements of development of plaque and gingivitis in man. Scand J Dent
Res 87, 178-83.
58
Preber, H. and Bergström, J. (1986) Cigarette smoking in patients referred for
periodontal treatment. Scand J Dent Res 94, 102-8.
Quirynen, M. and Bollen, C. M. (1995) The influence of surface roughness and surface-
free energy on supra-and subgingival plaque formation in man. A review of the
literature. J Clin Periodontol 22, 1-14.
Quirynen, M., Dekeyser, C. and Steenberghe, D. van. (1991) The influence of gingival
inflammation, tooth type, and timing on the rate of plaque formation. J
Periodontol 62, 219-22.
Quirynen, M., Marechal, M., Busscher, H. J., Weerkamp, A.H., Darius, P. L. and
Steenberghe, D. van. (1990) The influence of surface-free energy and surface
roughness on early plaque formation. An in vivo study in man. J Clin
Periodontol 17, 138-44.
Quirynen, M. and Steenberghe, D. van. (1989) Is early plaque growth rate constant
with time? J Clin Periodontol 16, 278-83.
Ramberg, P., Lindhe, J., Dahlen, G. and Volpe, A. R. (1994) The influence of gingival
inflammation on de novo plaque formation. J Clin Periodontol 21, 51-6.
Rasmussen, L., Hänström, L. and Lerner, U. H. (2000) Characterization of bone
resorbing activity in gingival crevicular fluid from patients with periodontitis. J
Clin Periodontol 27, 41-52.
Rawlinson, A., Dalati, M. H. N., Rahman, S., Walsh, T. F., Fairclough, A.L. (2000)
Interleukin-1 and IL-1 receptor antagonist in gingival crevicular fluid. J Clin
Periodontol 27, 738-43.
Reitemeier, D., Hänsel, K., Walter, M. H., Kastner, C. and Toutenburg, H. (2002) Effect of posterior crown margin placement on gingival health. J Prosthet Dent 87, 167-72.
Robinson, F. G., Knoernschild, K. L., Sterrett, J.D. and Tompkins, G. F. (1996) Porphyromomonas gingivalis endotoxin affinity for dental ceramics. J Prosthet Dent 75, 217-27.
Rosenstiel, S. F., Land, M. F. and Crispin, B. J. (1998) Dental luting agents: A review at the current literature. J Prosthet Dent 80, 280-301.
Rüdiger, S.G., Carlén, A., Meurman, J. H., Kari, K. and Olsson, J. (2002) Dental biofilms at healthy and inflamed gingival margins. J Clin Periodontol 29, 524-30.
Rudney, J. D. (2000) Saliva and dental plaque. Adv Dent Res 14, 29-39.
Santerre, J. P., Shajii, L. and Leung, B. W. (2001) Relation of dental composite formulations to their degradation and the release of hydrolyzed polymeric-resin-derived products. Crit Rev Oral Biol Med 12, 136-51.

59
Savitt, E. D., Malament, K, A., Socransky, S. S., Melcer, A. J. and Backman, K. J. (1987) Effects on colonization of oral microbiota by a cast glass-ceramic restoration. Int J Periodontics Restorative Dent 2, 23-35.
Sbordone, L., Bortolaia, C. (2003) Oral microbial biofilms and plaque-related
diseases:microbial communities and their role in shift from oral health to
disease. Clin Oral Invest 7, 181-8.
Schedle, A., Franz, A., Rausch-Fan, X., Spittler, A., Lucas, T., Samorapoompichit, P. and
Sperr, W. (1998) Cytotoxic effects of dental composites, adhesive substances,
compomers and cements. Dent Mater 14, 429-40.
Schmalz, G. (1997) Concepts of biocompatibility testing of dental restorative materials.
Clin Oral Investig 1, 154-62.
Schmalz, G. and Garhammer, P. (2002) Biological interactions of dental cast alloys with
oral tissues. Dent Mater 18, 396-406.
Schmalz, G., Schweikl, H. and Hiller, K. A. (2000) Release of prostaglandin E2 , IL-6 and
IL-8 from human oral epithelial culture models after exposure to compounds of
dental materials. Eur J Oral Sci 108, 442-8.
Schuster, G. S., Lefebre, C. A., Wataha, J. C. and White, S. N. (1996) Biocompatibility of
posterior restorative materials. J Calif Dent Assoc 24, 17-31.
Schätzle, M., Lang, N. P., Ånerud, Å, Boysen, H., Burgin, W. and Löe, H. (2000) The
influence of margins of restorations on periodontal tissues over 26 years. J Clin
Periodontol 27, 57-64.
Schätzle, M., Loe, H. Burgin, W., Anerud, A., Boysen, H. and Lang, N. P. (2003) Clinical
course of chronic periodontitis I . Role of gingivitis. J Clin Periodontol 30, 887-
901.
Scotti, R., Zanini, K. K. Scotti, N., Monaco, C., Valandro, L. F., Bottino, M. A. (2006) Early
colonization on polished- and glazed zirconium ceramic surface. Minerva
Stomatol 55, 493-502.
Selwitz, R. H., Ismail, A. I. and Pitts, N. B. (2007) Dental caries. Lancet 369, 51-9.
Seymour, G. J. and Gemmell, E. (2001) Cytokines in periodontal disease: where to from
here? Acta Odontol Scand 59, 167-73.
Shapira, L., Wilensky, A. and Kinane, D. F. (2005) Effect of genetic variability on the
inflammatory response to periodontal infection. J Clin Periodontol 32 (Suppl 6),
72-86.
Simonsson, T., Rönström, A., Rundegren, J. and Birkhed, D. (1987) Rate of plaque
formation- some clinical and biochemical characteristics of “heavy” and “light”
plaque formers. Scand J Dent Res 95, 97-103.

60
Sjögren, G., Lantto, R. and Tillberg, A. (1999) Clinical evaluations of all-ceramic crowns
(Dicor) in general practice. J Prosthet Dent 81, 277-84.
Socransky, S. S. and Haffajee, A. D. (2002) Dental biofilms: difficult therapeutic targets.
Periodontol 2000 28, 12-55.
Socransky, S. S. and Haffajee, A. D. (2005) Periodontal microbial ecology. Periodontol
2000 38, 135-87.
Steinberg, D., Eyal, S. (2002) Early formation of Streptococcus sobrinus biofilm on
various dental restorative materials. J Dent 30, 47-51.
Stenberg, R. and Matsson, L. (1993) Clinical evaluation of glass ceramic inlays (Dicor).
Acta Odontol Scand 51, 91-7.
Stoller, N. H., Karras, D. C. and Johnson, L. R. (1990) Reliability of crevicular fluid
measurements taken in presence of supragingival plaque. J Periodontol 61,
660-73.
Suljak, J. P., Reid, G., Wood, S. M., McConell, R. J., van der Mei, H. C., Busscher, H. J.
(1995) Bacterial adhesion to dental amalgam and three resin composites. J
Dent 23, 171-6.
Sunnegårdh-Grönberg, K. Calcium aluminate cement as dental restorative. Mechanical
properties and clinical durability. Umeå university odontological dissertations,
No 84, Umeå, Sweden, 2004.
Sunnegårdh-Grönberg, K. and Dijken, J. W. V. van. (2003) Surface roughness of a novel
“ceramic restorative cement” after treatment with different polishing
techniques in vitro. Clin Oral Invest 7, 27-31.
Sutherland, I. W. (2001) Biofilm exopolysaccharides: a strong and sticky framework.
Microbiology 147, 3-9.
Söder, B., Johansen, A. and Lagerlöf, F. (2003) Percent of plaque on individual tooth
surfaces and differences in plaque area between adjacent teeth in healthy
adults. Int J Dent Hyg 1, 23-28.
Tanner, J., Robinson, C., Söderling, E. and Vallittu, P. (2005) Early plaque formation on
fibre-reinforced composites in vivo. Clin Oral Invest 9, 154-160.
ten Cate, J. M. (2006) Biofilms, a new approach to the microbiology of dental plaque.
Odontology 94, 1-9.
Teughels, W., Assche, N. van., Sliepen, I. and Quirynen, M. (2006) Effect of material
characteristics and/or surface topography on biofilm development. Clin Oral
Imp Res 17, Suppl 29, 68-81.

61
Theilade, E., Wrigth, H., Jensen, S. B. and Löe, H. (1966) Experimental gingivitis in man.
II. A longitudinal clinical and bacteriological investigation. J Periodontal Res 1,
1-13.
Tidehag, P. and Gunne, J. (1995) A 2-year clinical follow-up study of IPS Empress
ceramic inlays. Int J Prosthodont 8, 456-60.
Trombelli, L., Tatakis, D. N., Scapoli, C., Bottega, S., Orlandini, E. and Tosi, M. (2004)
Modulation of clinical expression of plaque-induced gingivitis. II. Identification
of “high-responder” and “low-responder” subjects. J Clin Periodontol 31, 239-
52.
Turesky, S., Gilmore, N., Glickman, I. (1970) Reduced plaque formation by the
chloromethyl analogue of victamin C. Ann Periodontol 41, 41-3.
Uitto, V-J. (2003) Gingival crevice fluid-an introduction. Periodontol 2000 31, 9-11.
Waschul, B., Herforth, A., Stiller-Winkler, R., Idel, H., Granrath, N. and Deinzer, R.
(2003). Effects plaque, physiological stress and gender on crevicular IL-1β and
IL-1ra secretion. J Clin Periodontol 30, 238-48.
Wataha, J. C., Hanks, C.T., Strawn, S.E. and Fat, J. C. (1994) Cytotoxicity of components
of resins and other dental restorative materials. J Oral Rehabil 21, 453-62.
Weber, R. L. and Iacono, V. J. (1997) Basic science update for the clinician. The
cytokines: A review of interleukins. Periodont Clin Investig 19, 17-22.
Wilton, J. M., Bampton, J. L., Griffiths, G. S., Curtis, M. A., Life, J. S., Johnson, N. W.,
Powell, J. R., Harrap, G. P. and Critchley, P. (1992) Interleukin-1beta (Il-1 beta)
levels in GCF from adults with previous evidence of destructive periodontitis. A
cross sectional study. J Clin Periodontol 19, 53-7.
Wrangsjö, K., Swartling, C. and Meding, B. (2001) Occupational dermatitis in dental
personnel: contact dermatitis with special reference to (meth)acrylates in 174
patients. Contact Dermatitis 45, 158-63.
Yoshimura, A., Hara., Y., Kaneko, T. and Kato, I. (1997) Secretion of IL-1β, TNF-α, IL-8
and IL-1ra by human polymorphonuclear leukocytes in response to
lipopolysaccharides from periodontopathic bacteria. J Periodont Res 32, 279-
86.
Zappa, U. (1995) Histology of the periodontal lesion: implications for diagnosis.
Periodontol 2000 7, 22-38.
Zhang, J., Kashket, S. and Lingström, P. (2002) Evidence for the early onset of gingival
inflammation following short-term plaque accumulation. J Clin Periodontol 29,
1082-5.