induced lung injury (vili) - · pdf fileคือวืธิีการีการช...
TRANSCRIPT
1
ผศ. นพ. สนต ปณณะหตานนทหนวยทารกแรกเกด ภาควชากมารเวชศาสตรคณะแพทยศาสตร จฬาลงกรณมหาวทยาลย
Ventilator induced lung injury (VILI)Type of injury:
BarotraumaVolutraumaAtelectotraumaBiotrauma
Various clinical manifestations

2
lungs after mechanical ventilation at 45 cm H2O peak airway pressure
normal lungs 5 min 20 min
Am. J. Respir. Crit. Care Med. 157: 294-323
Non invasive ventilationAvoiding intubationShorten duration of intubationMinimize compl ications of intubation and mechanical
til tiventilation
CPAP คออะไร?คอวธการคอวธการชวยหายใจแบบหนงทมลกษณะสาคญดงน ::--
11.. ใหแรงดนบวก ใหแรงดนบวก (Positive pressure) (Positive pressure) กบทางเดน กบทางเดน หายใจหายใจ22. . ผปวยมการหายใจดวยตวเอง ผปวยมการหายใจดวยตวเอง (Spontaneous Spontaneous
breathing) breathing) 33. . ใชแรงดนบวกตลอดชวงการหายใจเขาและออกใชแรงดนบวกตลอดชวงการหายใจเขาและออก
ผลทางสรรวทยาของ CPAP ชวยใหปอดขยายตวไดตลอดระยะการหายใจ ปองกนปอดแฟบ
ใ ใ ( i i t )ลดแรงตานทานในทางเดนหายใจ (airway resistance)ชวยใหผปวยหายใจไดสมาเสมอชวยเกยวกบ surfactant metabolismทาใหทรวงอกและทางเดนหายใจคงรปได
ผลทางสรรวทยาของการใชCPAPทาใหถงลมปอดสวนทแฟบขยายตวขนการแลกเปลยนกาซดขนชวยใหสารลดแรงตงผวทางานดขนลด Intrapulmonary shunting

3
CPAP ชวยผปวยอยางไร ?ลดอตราการหายใจลดการใช O2
ลดอาการหายใจลาบาก : grunting, sternal &ลดอาการหายใจลาบาก : grunting, sternal & intercostal recessionทาใหผปวยหายใจสบายขน (Reduces work of breathing)
ขอดของ Nasal CPAPมประสทธภาพNon-invasiveNon invasiveประกอบงาย วธการใชไมยงยากการดแลงายไมซบซอนประหยดกวาการชวยหายใจแบบอน
ประโยชนทางคลนกของ ประโยชนทางคลนกของ NCPAPNCPAP1. ใชชวยหายใจในทารกกอนกาหนดทหายใจลาบากจากโรค
RDS (Early NCPAP) (Lundstrom KE. Eur J Pediatr 1996;155:S22-29 ; Ho et al. Cochrane Database
Systemic Reviews 2000)Systemic Reviews 2000) 2. ใชชวยหายใจหลงจากการถอดทอหายใจ(postextubation)
(Davis & Henderson :Cochrane Database Syst Rev. 2000)
3. ใชรกษาการหยดหายใจในทารกกอนกาหนด (apnea of prematurity)
ขอบงชของการใช ขอบงชของการใช nasal CPAPnasal CPAPEarly support for infants with mild to moderate RDSPost extubation supportApnea of prematurityPhrenic nerve palsyPhrenic nerve palsyAtelectasisTracheomalacia or other airway abnormalities
ขอบงหามของ CPAPภาวะหายใจวายอยางรนแรงความพการผดปกตของทางเดนหายใจ: cleft palate, TE-fistula, diaphragmatic herniap , , p gระบบหวใจไหลเวยนเลอดไมปกตทองอดมาก หรอทารกปวยดวยโรค NECทารกมอาการไมคงท : frequent apneas or bradycardia
สวนประกอบของ CPAP Gas source: warm humidified and blended gases Pressure generatorPatient interface: To connect the CPAP circuit to the i f t iinfants airway

4
สวนใหกาเนดแรงดนบวกสวนใหกาเนดแรงดนบวกContinuous flow devicesVariable flow devices
Flow characteristicsUnderwater bubble CPAP 5-6 L/minConventional ventilators for NCPAP : 6 L/minCPAP generatorCPAP generator Infant flow driver system : > 8 L/min
Bubble nasal CPAPBubble nasal CPAP
Non-Invasive Ventilation Neonatal – Device – Arabella CPAP & Vapotherm
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
5
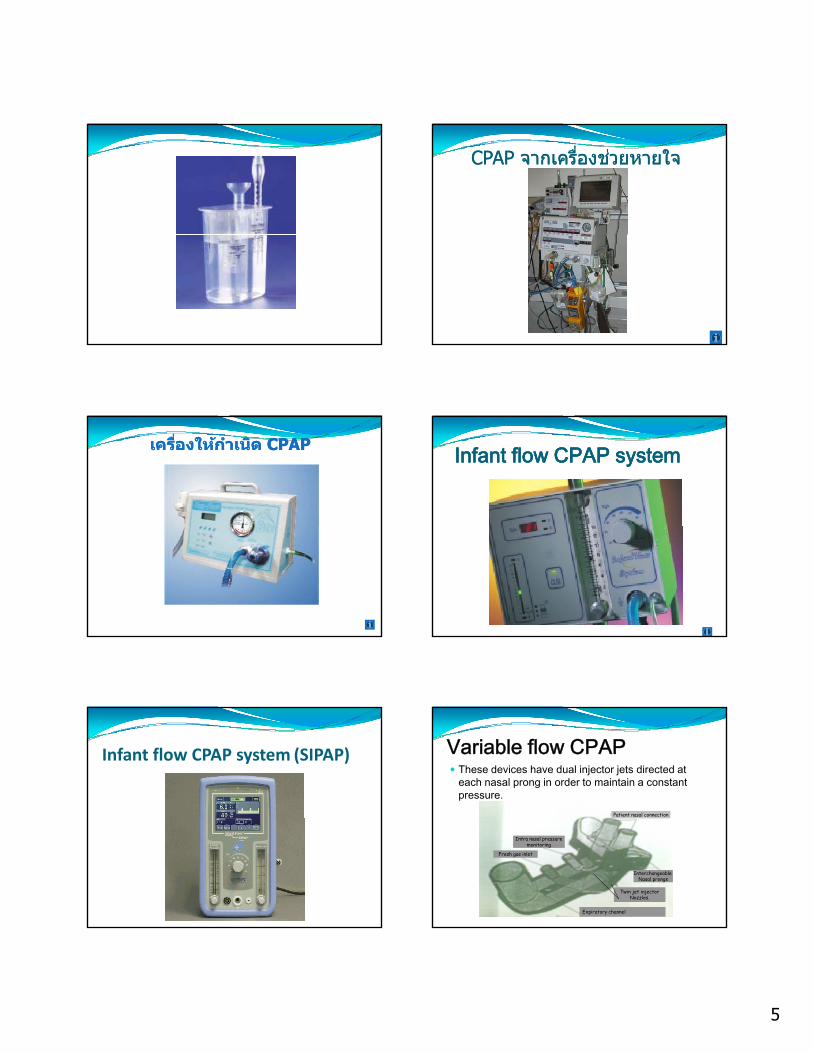
CPAP CPAP จากเครองชวยหายใจจากเครองชวยหายใจ
เครองใหกาเนด เครองใหกาเนด CPAP CPAP Infant flow CPAP systemInfant flow CPAP system
Infant flow CPAP system (SIPAP) Variable flow CPAPThese devices have dual injector jets directed at each nasal prong in order to maintain a constant pressure.
Patient nasal connection
Interchangeable Nasal prongs
Twin jet injectorNozzles.
Expiratory channel
Fresh gas inlet
Intra nasal pressuremonitoring

6
Infant flow CPAP system
The major advantage of variable flow CPAP is reducing the work breathing.The fluidic flip of variable flow devices assists exhalation.
Infant flow CPAP system
Patient interfacePatient interface
Hudson
Argyle
Types of prongsTypes of prongs
Inca
Fisher & Paykel
EME Nasopharyngeal
Argyle nasal cannula
Short binasal prongs
Silicone nasal prongs
Hudson binasal prongs

7
Hudson prongNon-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Hudson binasal prongsHudson binasal prongs
Silicone nasal prongsSilicone nasal prongs Silicone nasal prongSilicone nasal prong

8
Nasal mask Silicone nasal maskSilicone nasal mask
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Nasopharyngeal CPAPNasopharyngeal CPAP
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care

9
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Case report Oral continuous positive airway pressure (CPAP) following nasal injury in a preterm infant, H R Carlisle, C O F Kamlin, L S Owen, P G Davis, C J Morley; Arch Dis Child Fetal Neonatal Ed 2010;95:F142F143 doi:10.1136/adc.2009.170084
CPAP Devices : patient interfaceEndotracheal tubeFace mask Si l lSingle nasal prongs Nasopharyngeal prongsShort binasal prongsNasal maskNasal cannula
ควรเลอกใชอปกรณ ควรเลอกใชอปกรณ nasal CPAP nasal CPAP แบบแบบไหนไหน??
Single nasal prongDouble nasal prongp g
Argyle nasal cannula Hudson prongsInfant flow driver prongs
Nasal mask
ขอดขอเสยของ ขอดขอเสยของ NCPAP NCPAP แบบตางๆแบบตางๆMethods Advantages Disadvantages
ET Tube Stable ++/ good control & ventilator access
Invasive / Airway resistance ++
Nasal Prongs Easy / low resistance /easy feeding / non‐invasive
Septal erosion /nasal obstruction /abd. di idistension
Nasopharyng. tube
Non‐invasive / easy feeding Leaks /pressure necrosis/abd. distension
MaskCPAP mask
Easiest application Oral care difficult /leak / aspiration
Head box Easy application Leak /high flow 02 / access difficult
ปจจยทตองพจารณากอนใช NCPAP
อายครรภ : too immature ?อายหลงคลอดนาหนกตว : too small ?นาหนกตว : too small ?โรคของทารก : moderate RDSการควบคมการหายใจของทารก (Respiratory drive) : spontaneous breathing?, frequent apneas?ภาวะผดปกตอนๆของระบบหวใจและหลอดเลอด: PDA?, inotropes?ยาททารกไดรบ: sedation?
การต งระดบความดนและออกซเจนของ การต งระดบความดนและออกซเจนของ CPAPCPAPพจารณาจาก :
ขนาดทารกความรนแรงของโรคความรนแรงของโรคความตองการออกซเจนChest x-ray

10
การต งระดบความดนและออกซเจนของ การต งระดบความดนและออกซเจนของ CPAPCPAP
โดยทวไป เรมทแรงดน 4-6 cmH2OFiO2 เรมจาก 0.3-0.4 แลวปรบตามความตองการของทารกตองการของทารก
CPAP RangesCPAP RangesRangesRanges CommentComment
LowLow 44——55 CPAP< 3 not usefulCPAP< 3 not useful
MediumMedium 66——88 Good rangeGood range
HighHigh 99‐‐‐‐1010 Adverse effects commonAdverse effects common
ระดบ ระดบ CPAP CPAP ทด ท ด ฟงไดยนเสยงลมทชายปอดชดเจน
สามารถปรบลด FiO2 ลงได จากภาพถายรงสปอดเหนปอดขยายตวไดถง 7‐8 ชองระหวางซโครงคา blood gas อยในเกณฑยอมรบได
Chest x ray
กอนใส กอนใส CPAPCPAP หลงใส หลงใส CPAPCPAP CPAP สงเกนไป
pharyngeal pressure in passive and closed mouth positions :De Paoli, Lau, Davis, et al. Arch Dis Child Fetal Neonatal Ed 2005;90:F79–F81
Pharyngeal pressure during NCPAPDe Paoli, Lau, Davis, et al. Arch Dis Child Fetal Neonatal Ed 2005;90:F79–F81

11
การปรบลด การปรบลด CPAPCPAPเมอทารกอาการดขน ไมมอาการแสดงของ respiratory distressnormal blood gasnormal blood gasimproving CXR
การปรบลด การปรบลด CPAPCPAPเรมจากลด FiO2 ชาๆ โดยรกษาระดบ SpO2 ท 90-95%เรมลดแรงดนบวกหลงจากลด FiO2 ไดตากวา 0.3 2 หรอปอดขยายตวมากเกนไปจาก X-rayลดแรงดนบวกครงละ 1 cm H2O ชาๆ (ทก6-12 ชวโมง) จนถง 3 – 4 cm H2O
การพจารณาหยดการชวยหายใจดวย การพจารณาหยดการชวยหายใจดวย NCPAPNCPAPทารกหายใจไดสบายไมมอาการเหนอยขณะไดรบการชวยจากเครองในขนาดตา
ถาความดนลดลงไดจนถง 3 – 4 ซม.นา
และ FiO2 ตากวา 0.25
CPAP failure หมายถงถาตองใช FiO2 > 0.7 หรอ CPAP pressure > 8 cmH2O เพอรกษาความอมตวของออกซเจนในเลอดใหสงกวา 90% หรอ PCO2 ใหตากวา 50 มม. ปรอท
ในขณะททารกไดรบการรกษาดวย nasal CPAP ใน setting ทเหมาะสมแลวเกดปญหาดงน
ทารกหยดหายใจนานกวา 20 วนาท เกน 2 ครง ใน 1 ชวโมง
Bradycardia ( ชพจรชากวา 100 ครง/นาท)
ตองใหการชวยเหลอดวย positive pressure ventilation บอยทารกมอาการเขยวบอย (oxygen saturation < 85 %) มากกวา 3 ครงในเวลา 1 ชวโมง
CPAP failure ????Persistent serious apneic episodesPaCO2 > 60 mmHgFiO2 > 0.6 to keep SaO2
ปญหาทางเทคนคทแกไขไดปญหาทางเทคนคทแกไขไดแรงดนบวกไมพอ (Insufficient pressure)อตราการไหลของกาซไมพอ (Insufficient flow)เลอกขนาดของ prong ไมเหมาะสมNasal prong อยตาแหนงไมถกตองSecretion obstructionทารกอาปาก
การดแลทารกระหวางการใช NCPAPรบกวนทารกใหนอยทสด หลกเลยงการใหยา Sedationดแล Nasal prongs ใหอยในจมกตลอดเวลา (FIXATION)Orogastric tubeOrogastric tubeดดเสมหะในปากและจมก
ดแลผวหนงบรเวณจมก
เปลยนทานอนทารกตามความเหมาะสม
ตดตาม Vital signs และ pulse oximetryLab เทาทจาเปน Blood gas, hematological, X‐ray
12
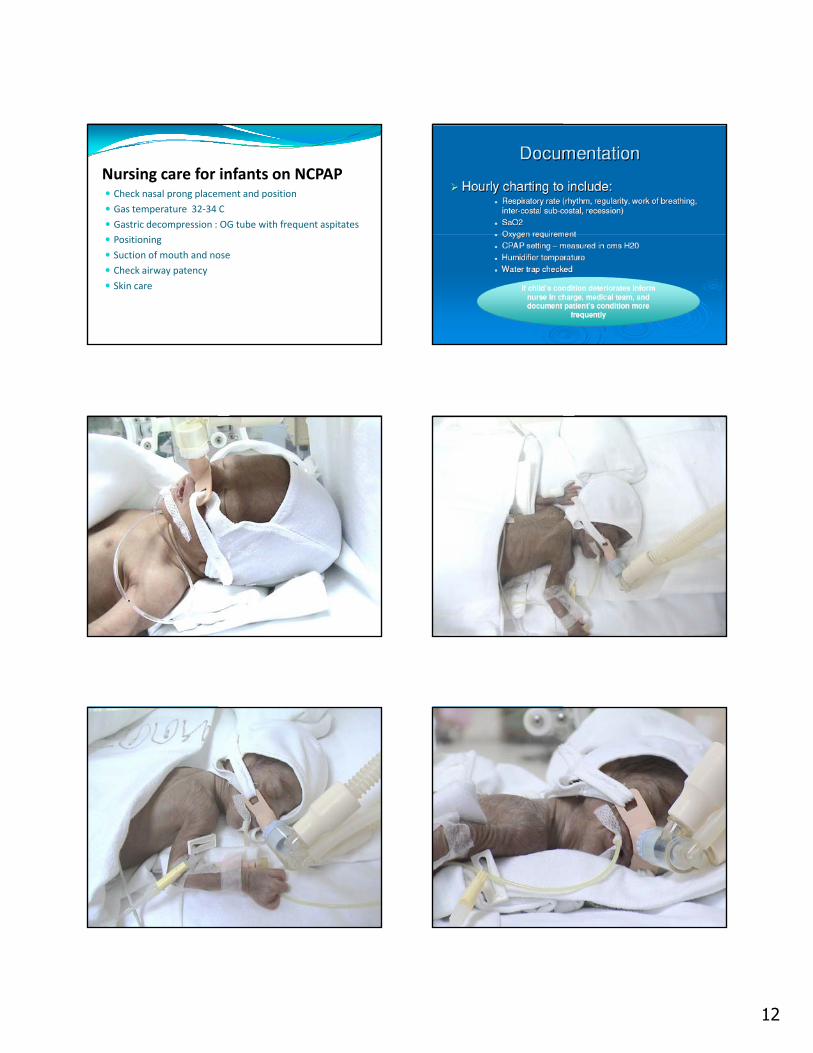
Nursing care for infants on NCPAPCheck nasal prong placement and positionGas temperature 32‐34 CGastric decompression : OG tube with frequent aspitatesPositioningSuction of mouth and noseCheck airway patencySkin care
13
I am sleeping
อนตรายและภาวะแทรกซอนจาก NCPAP1. จมกตน, prong อดตนจากเสมหะ,เมอก
2. ปอดขยายมากเกนไป:CO2 retention, air leak3. Impaired cardiac output, pulmonary blood3. Impaired cardiac output, pulmonary blood
flow4. ทองอดจากลมในกระเพาะอาหาร
5. อนตรายตอผวหนงและเยอบจมก
6. Prong เลอนหลด
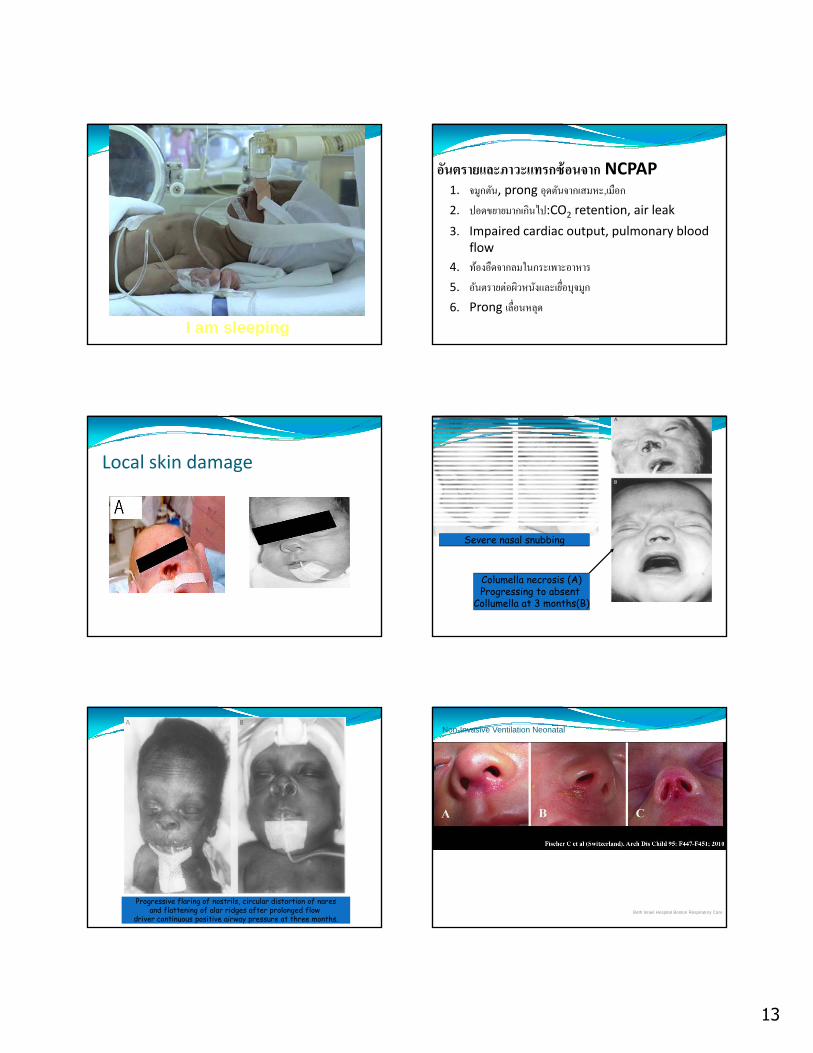
Local skin damage
Severe nasal snubbing
Columella necrosis (A)Progressing to absent
Collumella at 3 months(B)
Progressive flaring of nostrils, circular distortion of naresand flattening of alar ridges after prolonged flow
driver continuous positive airway pressure at three months.
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care

14
CPAP bellyCPAP bellyCPAP belly
15
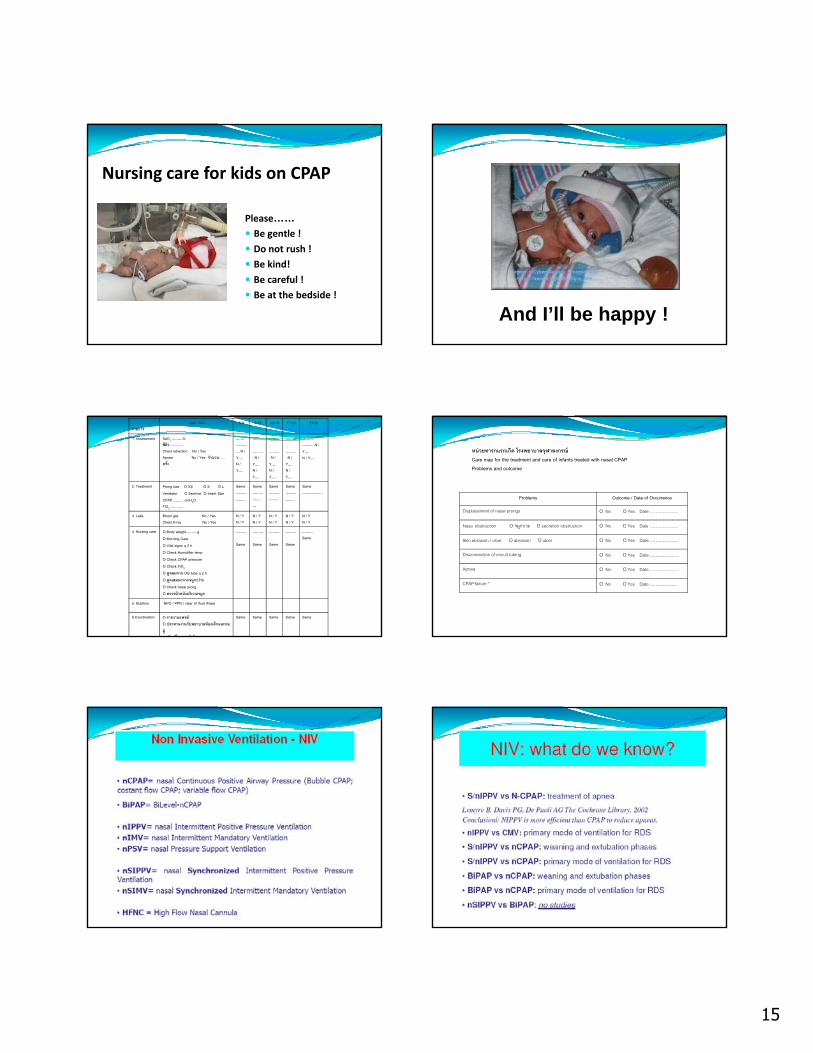
Nursing care for kids on CPAP
Please……Be gentle !Be gentle !Do not rush !Be kind!Be careful !Be at the bedside !
And I’ll be happy !
รายการhour : 0-4 5-8 9-12 13-16 17-20 21-24
1. Assessment SaO2 ………%สผว …………Chest retraction No / YesApnea No / Yes จานวน...... ครง
….…………….N / Y….N / Y….
………..………..N / Y….N / Y….
………..………..N / Y….N / Y….
………..………..N / Y….N / Y….
………..………..N / Y….N / Y….
2. Treatment Prong size O XS O S O LVentilator O Sechrist O Infant StarCPAP………..cmH2OFiO2………….
Same ……………...
Same…………….…
Same……………....
Same……………...
Same……………...
3. Labs Blood gas No / YesChest X-ray No / Yes
N / YN / Y
N / YN / Y
N / YN / Y
N / YN / Y
N / YN / Y
4. Nursing care O Body weight……….gO Morning CareO Vital signs q 2 hO Check Humidifier tempO Check CPAP pressureO Check FiO2
O ดดลมจาก OG tube q 2 hO ดดเสมหะจากจมก/ปากO Check nasal prong O ตรวจผวหนงบรเวณจมก
……….Same
……….Same
……….Same
……….Same
……….Same
5. Nutrition NPO / PPN / clear IV fluid /Feed
6.Coordination O รายงานแพทยO ประสานงานกบพยาบาลหองเดกและหอผ ปวยทมารดาพกรกษา
Same Same Same Same Same
หนวยทารกแรกเกด โรงพยาบาลจฬาลงกรณCare map for the treatment and care of infants treated with nasal CPAPProblems and outcome
Problems Outcome / Date of Occurrence
Displacement of nasal prongs O No O Yes Date………………..
Nasal obstruction O จมกบวม O secretion obstruction O No O Yes DateNasal obstruction O จมกบวม O secretion obstruction O No O Yes Date………………..
Skin abrasion / ulcer O abrasion O ulcer O No O Yes Date………………..
Disconnection of circuit tubing O No O Yes Date………………..
Apnea O No O Yes Date………………..
CPAP failure * O No O Yes Date………………..

16
NIPPVNeonatal nasal intermittent positive pressure ventilation (NIPPV) provides non‐invasive respiratory support to premature infants who may otherwise require endotracheal intubation and ventilationendotracheal intubation and ventilation.
NIPPV is the augmentation of continuous positive airway pressure (CPAP) with superimposed inflations, to a set peak pressure
HOW DOES NIPPV WORKincreasing pharyngeal dilation
improving the respiratory drive
inducing Head’s paradoxical reflexinducing Head s paradoxical reflex
increasing mean airway pressure allowing recruitment of alveoli
increasing functional residual capacity;
increasing tidal and minute volume.
Arch. Dis. Child. Fetal Neonatal Ed., Sep 2007; 92: F414 ‐ F418.
SNIPPVSynchronisation, defined as mechanical inflation commencing within 100 ms of the onset of inspiration, uses a capsule to detect abdominal movement at the start of inspirationstart of inspiration.
WHAT VENTILATOR SETTINGS SHOULD WE USE
DURING NIPPV?
PEEP 3‐6 cm H2OPIP 8‐21 cm H2oR 10‐30 /miT 0.4‐0.6 sFlow 8‐10 l/m up to 15 l/m
Setup of NIPPVNon-Invasive Ventilation Neonatal CLD Working Group
rate Ti PIP PEEP rise time flow LPM Pressure MAX
Ramanathan
40 max 500.5to1
PEEP plus
10-155-8 0.1-0.2 10-15 PIP 30
PIPvent Not MAP
* V Bhandari JOP 2010 30, 505-512•O2 to optimize saturation per policy, •Caffeine •Hct. > 35
Beth Israel Hospital Boston Respiratory Care
V Bhandari *
~40 ~0.45 plus4
4-6 Notspecified 8-10 14 < 1000g
16 > 1000 g
Chronic LungDisease NIPPV
Overview
15-200.3to
0.5
PIPvent plus2-4
5 Notspecified
Notspecified
Notspecified
*

17
Transition of Support• Remove
NIPPV– Rate 15-25– PIP < 17
• Intubate– pH < 7.25 PaCO2 > 60– Apnea requiring bagging– Frequent As & Bs– Frequent desaturations
Non-Invasive Ventilation Neonatal
PIP < 17– PEEP <6– FiO2 <35
V Bhandari JOP 2010 30, 505-512Beth Israel Hospital Boston Respiratory Care
“…can use blood gases to help wean, but not typically needed—can wean or increase settings based on clinical appearance” CLD Working Group
NN‐‐SIPPV SIPPV vsvs NN‐‐CPAP: weaning and CPAP: weaning and extubationextubation phasesphasesConclusion:N‐SIPPV resulted in lower extubation failure rates and better respiratory evolution thanrates and better respiratory evolution, than N‐CPAP.
BiPAPBiPAP vsvs NN‐‐CPAP: weaning and CPAP: weaning and extubationextubation phasesphasesConclusion: Oxygen saturation and tcO2 increased, and tcCO2 and respiratory rate decreased during the bilevel CPAP periods after MVperiods, after MV.
NN‐‐SIPPV SIPPV vsvs NN‐‐CPAP:CPAP:primary mode of ventilation for RDSprimary mode of ventilation for RDS
BiPAPBiPAP vsvs NN‐‐CPAP: primary mode of ventilation CPAP: primary mode of ventilation for RDSfor RDS

18
Thank you. Thank you.
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory CareINSURE (intubatio-surfactant-extubation)
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care

19
Non-Invasive Ventilation Neonatal – Indications & Incentives
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
20
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal – High Flow Cannula
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal – High Flow Cannula
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal – High Flow Cannula
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care
Non-Invasive Ventilation Neonatal
Beth Israel Hospital Boston Respiratory Care

21