iii pulmonary syphilis - sti.bmj.com · koch, orbythefindingoflesions orphysicalsigns, which are...
TRANSCRIPT
III
PULMONARY SYPHILISBy E. T. BURKE, D.S.O., M.B., Ch.B.
OF the diseases affecting the human race, pulmonarytuberculosis is regarded, not only as one of the most grave,but also as one of the most common. It is generallyhailed as " The Captain of the Men of Death." That thisis so is evident from the far-reaching, carefully organised,and costly Public Health measures that have beeninstituted to combat it.That tuberculosis is a common disease has been amply
demonstrated. Osler instances the investigations ofNaegeli in this respect. In a series of cases studied,97 per cent. of adult bodies showed tuberculosis lesions.In every body over the age of forty years, a focus oftuberculosis was found. The same author also quotesBulmer and Lartigan as finding healed lesions of pul-monary tuberculosis in 30 per cent. of 500 bodies in-vestigated in the post-mortem room.Not only records such as these, but general experience
also, make it very clear that this disease is one in whichspontaneous cure occurs with great frequency. Clinicalevidence of this is to be found in the multitude of patientswho, having for a time coughed up tubercle bacilli, have,under general hygienic treatment-and often in itsabsence-ceased to do so, and have completely recovered.Anatomical proof is furnished by the post-mortem findingof tuberculosis lesions undergoing resolution and repair.The treatment of pulmonary tuberculosis is at the
present day not specific. Success does not involve adirect attack upon the tubercle bacillus, but rests simplyupon the principle of raising the defensive mechanism ofthe host. Recovery from the disease appears to be depen-dent upon how far the internal economy of the patientcan be stimulated and built up. The aim is so to raisethe bodily condition that a stage will be attained in whichthe bacillus tuberculosis will find the environment so
99
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

BRITISH JOURNAL OF VENEREAL DISEASES
unsuited to its existence that it will succumb. That iswhat Sanatorium treatment accomplishes. Experienceshows how very little of it may, at times, be necessary toobtain good results. It is really a regimen which issuitable for, and which is indicated in, disease of anykind. It is applicable in equal degree to fractured femur,neurasthenia, and chicken-pox. Recovery is always morerapid and more certain in the pine groves of Hygeia thanin the workshops of Vulcan.There are several reasons why this so-called " sanatorium
treatment" is more successful in pulmonary tuberculosisthan in any other specific disease. The causal organismis comparatively vulnerable. Tuberculosis only attacks,and survives in, an unhealthy person. It can only thrivein a suitably debilitated soil. It cannot exist in a healthybody. Furthermore, there exists in the vast majority ofcivilised individuals a variable degree of immunity to it.The essence of treatment consists in placing the infectedperson in the optimum hygienic surroundings, so givinghis body freedom to work out its own salvation.The general trend would appear to be towards re-
covery, and there would seem to be but little tendencyfor the consumptive to remain in statu quo. He eitherrecovers to break his neck in the hunting field, or coughshis way into the Valley where " finis " is written byAsthenia, Syncope, or Haemorrhage.
Strictly speaking, the diagnosis of any specific diseasecan only be clinched by the discovery of the specificorganism, by the occurrence of a somatic or local tissue-reaction characteristic of the specific organism, or by somespecific serum-or other test. The identification of theorganism is, of course, conclusive.A diagnosis of tuberculosis of the lungs cannot be made
on physical signs alone. By such means one may con-clude that there is fibrosis, a cavity, inflammation, andsuch-like; but the identification of the cause of theseconditions is dependent upon the microscope and thelaboratory. Pulmonary tuberculosis can only be defi-nitely diagnosed by the demonstration of the bacillus ofKoch, or by the finding of lesions or physical signs, whichare capable of being produced by that organism alone.Of course in practice a lung condition is often diagnosedas being tubercular on the history and the physicalsigns. It must inevitably be so; and no doubt the
IOO
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from
PULMONARY SYPHILIS
majority of such diagnoses are correct; but they aremerely guesses nevertheless. The correctness of the guessdepends upon the clinical experience and acumen of thephysician. Nay more, the accuracy of the diagnosis willvary directly with the amount of knowledge that theclinician possesses of the morbid conditions, other thantuberculosis, which may affect the lungs.The frequency with which the pulmonary tissues are
attacked by the tubercle bacillus has made the possibilityof pulmonary syphilis seem to the clinician a very remoteone. This is due in great part to the usual teaching thata luetic condition of the lungs is an extremely infrequentoccurrence. It will be well to consider upon what groundsthe rarity of pulmonary syphilis has been asserted.Without seeking to obtain the title of " Bolshevik,"
one would venture to say that in medical science, respectfor authority has very narrow limits of desirability orusefulness. The prestige of John Hunter and the mis-interpretation of his ill-fated personal experiment estab-lished for too long the error of the identity of syphilis andgonorrhoea. This dictum was handed down from teacherto pupil in much the same way as is, at the present day,the myth of the osteogenetic function of the periosteum.
Osler is generally quoted as the firmest authority forthe statement that pulmonary syphilis is very rare. Oslerand Gibson say that in 2,500 autopsies performed at theJohns Hopkins Hospital in Baltimore, in only twelve caseswas lung syphilis demonstrated. Fowler's study of all thespecimens available in the London hospitals revealedonly ten undoubted cases of syphilis pulmonalis. Down-ing investigated 3,ooo autopsies at the MassachusettsGeneral Hospital for lung syphilis with totally negativeresults. Hazen states that in 6,ooo cases of syphilis takenfrom the records of the Copenhagen Hospital, there werebut two cases of pulmonary lues. Jonathan Hutchinsonremarks upon the rarity of the condition. It is upon thesefoundations that the teaching of the rarity of pulmonarysyphilis is based.
In order to obtain a proper perspective of the syphiliticlandscape, it is well, at first, not to focus attention tooclosely upon the lungs. By taking a more general pre-liminary survey there may be found a more favourablestance from which to view syphilis in its purely pulmonaryaspect.
IOI
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

BRITISH JOURNAL OF VENEREAL DISEASES
Symmers analysed the results of 4,880 post-mortemexaminations which were performed in ten years at theBelle Vue Hospital in New York. Evidence of syphilisin some organ was demonstrated in only 3I4 cases, or6-5 per cent. Warthin, on the other hand, made 750autopsies in the rural district of Ann Arbor in Michigan,and found syphilis to be present in 300 instances, or in40 per cent. of cases.
Bearing in mind the respective venues in which thesestudies were made-the former in a great city among thepoorer classes; the latter in a country district amongmore well-to-do people-the results are very striking intheir wide divergence. Either of the two explanations,(i) that in the United States syphilis is more common inthe country than in the city, or (2) that all the syphiliticsin the North American continent go to Ann Arbor to die,is untenable. It is only mental inertia which wouldsuggest that the truth must lie somewhere between thetwo. The true explanation is only to be arrived at afteran examination of the standards of diagnosis applied ineither case. In every analysis or statement that is madeconcerning the diagnosis of syphilis or its incidence inany organ, the criteria upon which the diagnosis is basedmust be critically considered.
Medical evidence is often-and when there is no needfor it to be so-of a very lax character; and this bothin its positive and negative aspects. Such evidence is fre-quently submitted, and accepted, when it is of such anature as to be quite valueless in a court of law. Thepresence of an indurated penile ulcer or an apparentlytypical rash on the chest is by no means proof of syphilis,although it would, in the consulting room, be a sufficientindication for the institution of antisyphilitic treatmentpending the arrival of the laboratory report. While it isbut right and proper in the living to give the patient thebenefit of the doubt by commencing treatment, in thecadaver, the presence or absence of syphilis must only beconcluded after a most rigid and searching examination.The evidence, in order to carry conviction, must not onlybe consistent with the presence of syphilis, but must atthe same time be inconsistent with its absence. Theconverse, of course, is equally true.The criteria for the diagnosis of syphilis in the dead are
the demonstration of the treponema pallidum, and of theI02
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from
PULMONARY SYPHILIS
histological changes which are alone typical of its activi-ties. The work of Graves showed that post-mortemWassermann tests confirmed the ante-mortem reports in97 per cent. of cases. The post-mortem Wassermannshould, therefore, not be omitted. The presence ofsyphilis may be inferred-and often with some assurance-from gross evidences alone; but its absence can only beaccepted after negative bacteriological, histological, andserological investigation. Its presence can only bedefinitely proved after a similar series of examinationshave yielded positive results.Now, Symmers's diagnoses were made upon gross
pathological appearances-aortitis, aneurism, gummata.The latter has long been enthroned as the symbol parexcellence of post-mortem syphilis. This has been pro-claimed by book after book, and is still, no doubt, beingbroadcast into the more or less receptive ears of themedical student. The general view is that the fre-quency with which gummata are found in an organ afterdeath is an index of the incidence of syphilis of thatorgan during life. The truth is that the gumma is animpostor. If it be taken as the criterion of post-mortemsyphilis, then syphilis is not only a rare disease of thelungs, but is an infrequent disease of any part of thehuman body.The essence of the syphilitic reaction-that is, the
response of the tissues to the activities of the treponemapallidum-is that it is of the nature of a granulomaoriginating in the perivascular lymph spaces as an in-filtrat on of lymphocytes and plasma cells. The chancre,the cutaneous syphilides, the gumma, the fibrosis, areall simply different stages and degrees of this reaction.The type depends upon the organ or tissue affected, theage of the disease, and the time that the reaction hasbeen in progress. There is no essential histologicaldifference between the primary and the tertiary or otherlesion. The matter of the incidence and diagnosis ofsyphilis in the dead body resolves itself into a decisionas to what is the type-lesion and how it is to be identified.This is especially so when the disease is in its late orso-called " latent " stages.The latter term is a misnomer. The disease can never
be latent. It can only be present or absent. If it ispresent it is invariably active, although it may not, at
I03
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

BRITISH JOURNAL OF VENEREAL DISEASES
the moment, be . giving rise to well-defined clinicalsigns. Whenever syphilis is present, whenever a positiveresult is obtained in a Wassermann test, active patho-logical processes are taking place in some organ or tissueof the body. Such a condition is most properly termed" endosyphilis," which means syphilis without clinicalsigns. In such cases, the presence of the disease is indi-cated by a distinct histological picture in the organaffected.The gross signs of syphilis which have been mentioned-
those lesions which are appreciable by the naked eye-areto be regarded merely as the ultimate response of thetissues, principally reparative in nature, to the activitiesof the treponema pallidum. Warthin showed, as a resultof his investigations, that the gumma is not the typicallesion of late or of endosyphilis. The viscera are involvedin all such cases, and the type-lesion consists, not ofgummatous, but of specific inflammatory processes.This condition eventually proceeds to fibrosis, and per-haps further. The typical inflammatory reaction is mildin character, but is of profound pathological importancebecause of its steady progressive nature.
In his 750 autopsies, of which 40 per cent. were foundto be syphilitic, Warthin adopted the histological andmodern method of investigation. His standard of diag-nosis was most rigid ; and indeed it is the only one capableof carrying positive or negative conviction. His firstendeavour was to demonstrate the treponema pallidumin the tissues. By the Levaditi method this was a com-paratively easy matter in congenital cases, and especiallyin the heart-muscle. In all cases of congenital syphiliticmyocarditis there was seen a typical microscopic pictureof cedema of the interstitial tissues with a lymphocyte andplasma cell infiltration. It has been fairly generallyaccepted that luetic myocarditis is secondary to a peri-arteritis of the coronary vessels, but Warthin has shownthat it may be a primary condition. In congenital myo-carditis the treponema pallidum was constantly found,and fibroblastic and angioblastic proliferations were alsopresent. Although the presence of treponemata isnecessary to cause the typical histological appearances,yet the organisms may be in the congenitally syphilitictissues without producing any of these changes.
In cases of acquired syphilis, the treponema pallidumI04
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

PULMONARY SYPHILIS
majority of such diagnoses are correct; but they aremerely guesses nevertheless. The correctness of the guessdepends upon the clinical experience and acumen of thephysician. Nay more, the accuracy of the diagnosis willvary directly with the amount of knowledge that theclinician possesses of the morbid conditions, other thantuberculosis, which may affect the lungs.The frequency with which the pulmonary tissues are
attacked by the tubercle bacillus has made the possibilityof pulmonary syphilis seem to the clinician a very remoteone. This is due in great part to the usual teaching thata luetic condition of the lungs is an extremely infrequentoccurrence. It will be well to consider upon what groundsthe rarity of pulmonary syphilis has been asserted.Without seeking to obtain the title of " Bolshevik,"
one would venture to say that in medical science, respectfor authority has very narrow limits of desirability orusefulness. The prestige of John Hunter and the mis-interpretation of his ill-fated personal experiment estab-lished for too long the error of the identity of syphilis andgonorrhoea. This dictum was handed down from teacherto pupil in much the same way as is, at the present day,the myth of the osteogenetic function of the periosteum.
Osler is generally quoted as the firmest authority forthe statement that pulmonary syphilis is very rare. Oslerand Gibson say that in 2,500 autopsies performed at theJohns Hopkins Hospital in Baltimore, in only twelve caseswas lung syphilis demonstrated. Fowler's study of all thespecimens available in the London hospitals revealedonly ten undoubted cases of syphilis pulmonalis. Down-ing investigated 3,ooo autopsies at the MassachusettsGeneral Hospital for lung syphilis with totally negativeresults. Hazen states that in 6,ooo cases of syphilis takenfrom the records of the Copenhagen Hospital, there werebut two cases of pulmonary lues. Jonathan Hutchinsonremarks upon the rarity of the condition. It is upon thesefoundations that the teaching of the rarity of pulmonarysyphilis is based.
In order to obtain a proper perspective of the syphiliticlandscape, it is well, at first, not to focus attention tooclosely upon the lungs. By taking a more general pre-liminary survey there may be found a more favourablestance from which to view syphilis in its purely pulmonaryaspect.
IOI
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

BRITISH JOURNAL OF VENEREAL DISEASES
A new and more accurate pathology of syphilis hasarisen, and by virtue of it fewer cases are missed. Thepractical point is that under the old concept it was onlypossible to diagnose syphilis in the dead body when verygross evidences were apparent.From a consideration of the foregoing it would appear
that the hitherto accepted teaching as to the rarity oflung syphilis requires revision. Recent post-mortemexaminations show, when modem criteria of diagnosis areadopted, that the general incidence of syphilis is muchhigher than was at one time believed or suspected. Aninvestigation along modern lines, with special reference tothe lungs, is a field that is worthy of the very closestattention by the histo-pathologist. Only after it has beenfully traversed will the picture of pulmonary syphilisappear in true perspective.A very thorough study of this kind was carried out by
Carrera upon the lungs of I50 cases of undoubted syphi-litics. These lungs were examined histologically, butnaturally, considering the size of the organs, the amountof tissue actually passed under the microscope wasrelatively small. A negative result is not, therefore,absolutely indicative of the absence of syphilis; a smallluetic area might easily have been missed. A certainunknown proportion of the negative results it is justifiableto attribute to inadequate search. Positive diagnoseswere made only upon modem histological criteria. Outof the I52 cases examined, twelve were found to havepulmonary syphilis, or roughly, 8 per cent.
Contrary to what is found in miliary tuberculosis of the'lung, gummata do not fuse, but remain discrete. Wherecaseous areas are present, fibrin threads are absent. This-is again in contrast to what is found in tuberculosis. Inall cases the gumma is found to be essentially a vascularlesion consisting of " angioblastic proliferations infil-trated with plasma cells and histogenetic lymphocytes."In the affected areas, elastic tissue is generally seen to bemore abundant than is the case in tuberculosis. Thegummatous area fades gradually into the neighbouringtissue, while the tubercle is sharply demarcated from itssurroundings. The healed scars of lung syphilis arecharacteristic, being of irregular form, and showingbranchings as well as vascularisation.Although out of the I52 cases only twelve were posi-
io6
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

PULMONARY SYPHILIS
tively diagnosed as pulmonary syphilis, yet at the sametime, a condition of fibrosis associated with brown indura-tion was present in the lungs of I24 bodies, or 82 per cent.In these cases it is not too easy to decide whether thisfibrosis is due to the local action of the treponema pallidumon the pulmonary tissues, or whether all or part of it isdue to cardiac damage-chronic passive venous conges-tion. Syphilitic fibrosis is simply the further developmentof the specific inflammatory process, and it proceeds alongthe vessels and bronchi. At present one cannot dogmatiseon the matter, but it is noteworthy that while 82 per cent.of syphilitic post-mortems showed chronic passive venouscongestion of the lungs, only 5 per cent. of non-syphiliticsshowed the same condition. It would appear from thisthat syphilis has a very profound effect upon the heart,with consequent secondary effects upon the lungs. Thisbut strengthens the view that syphilis is the most potentweapon in inflicting cardiac damage. In any cadavershowing well-marked brown induration of the lungs it isvery long odds in favour of the cause being syphilis.The chief points by which primary syphilitic fibrosis
may be distinguished from secondary chronic venouscongestion are, the presence in the former of connectivetissue bundles outside the vessels, their vascularisation,and the presence of plasma-cell infiltration. The syphiliticfibrosis shows distinct stellate radiations. On account ofthe fact that practically all lungs showing syphiliticfibrosis also suffer from chronic passive venous congestion,a painstakinig histological study is necessary to determinewhich is the primary condition.The differential diagnosis of the pulmonary connective
tissue formation in syphilis and in tuberculosis may betabulated thus:
Gumma. Tubercle.
Loosely packed with cells. Closely packed.Not sharply circumscribed. Sharply circumscribed.Few epithelioid and giant Many epithelioid and giant
cells. cells.Discrete. Confluent.Preponderance of lympho- Not so.
cytes and plasma cells.Granular. Hyaline.
I07 1 2
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
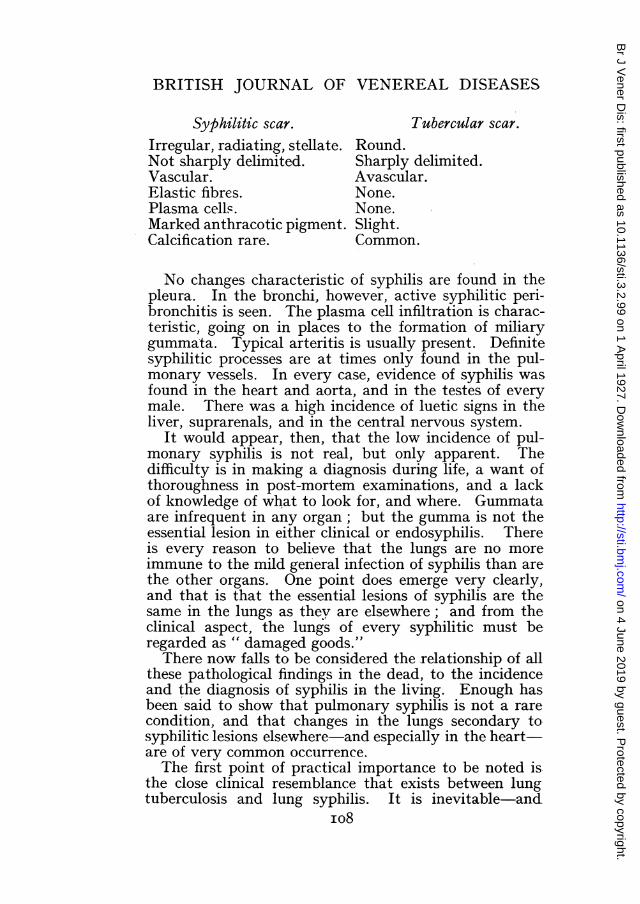
Syphilitic scar. Tubercular scar.Irregular, radiating, stellate. Round.Not sharply delimited. Sharply delimited.Vascular. Avascular.Elastic fibres. None.Plasma cells. None.Marked anthracotic pigment. Slight.Calcification rare. Common.
No changes characteristic of syphilis are found in thepleura. In the bronchi, however, active syphilitic peri-bronchitis is seen. The plasma cell infiltration is charac-teristic, going on in places to the formation of miliarygummata. Typical arteritis is usually present. Definitesyphilitic processes are at times only found in the pul-monary vessels. In every case, evidence of syphilis wasfound in the heart and aorta, and in the testes of everymale. There was a high incidence of luetic signs in theliver, suprarenals, and in the central nervous system.
It would appear, then, that the low incidence of pul-monary syphilis is not real, but only apparent. Thedifficulty is in making a diagnosis during life, a want ofthoroughness in post-mortem examinations, and a lackof knowledge of what to look for, and where. Gummataare infrequent in any organ; but the gumma is not theessential lesion in either cllnical or endosyphilis. Thereis every reason to believe that the lungs are no moreimmune to the mild general infection of syphilis than arethe other organs. One point does emerge very clearly,and that is that the essential lesions of syphilis are thesame in the lungs as they are elsewhere; and from theclinical aspect, the lungs of every syphilitic must beregarded as " damaged goods."There now falls to be considered the relationship of all
these pathological findings in the dead, to the incidenceand the diagnosis of syphilis in the living. Enough hasbeen said to show that pulmonary syphilis is not a rare-condition, and that changes in the lungs secondary tosyphilitic lesions elsewhere and especially in the heart-are of very common occurrence.The first point of practical importance to be noted is
the close clinical resemblance that exists between lungtuberculosis and lung syphilis. It is inevitable-and
io8
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from
PULMONARY SYPHILIS
the attitude is a perfectly correct one-that pulmonarytuberculosis should be thought of in any given casebefore pulmonary syphilis. But even so, the latter shouldalways be carefully eliminated before, in the absence oftubercle bacilli in the sputum, instituting sanatoriumtreatment to the exclusion of all antisyphilitic measures.
Histological post-mortem investigation provides verysure ground for the belief that the lungs share with allthe other organs in the general syphilitic infection. Itis therefore incumbent upon the clinician, when investi-gating the viscera of his syphilitic patient, to give as closeattention to the organs of respiration as to the cutaneous,circulatory, and central nervous systems.The differential diagnosis between pulmonary syphilis
and pulmonary tuberculosis is not really a very difficultmatter. The approximate truth may be expressedaphoristically by saying that every case of pulmonarytuberculosis which has a persistently negative sputumand which remains in a stationary condition is pulmonarysyphilis.
Accurately to diagnose pulmonary syphilis in the livingentails a careful consideration of the history, the physicalsigns in the chest-, the X-ray appearances, the sputum,the Wassermann report, and the effect of antisyphilitictherapy. The two most important aids in diagnosis arethe X-rays and the therapeutic test.The fundamental pathological fact to lay hold of in
considering the radiological diagnosis of syphilis of thelung is that insisted upon by Virchow, that it occurs as aninterstitial pulmonitis. Three very distinct conditionscan be demonstrated by the X-rays
(i) Syphilitic consolidation.(2) Early diffuse sclerosis.(3) Dense sclerosis.In syphilitic consolidation the radiogram shows a
massive shadow either occupying a whole lobe or thatportion of a lobe adjoining the hilum. The shadow isdensest at the hilum, and gradually becomes lighter asthe periphery is approached. In early diffuse sclerosisthe picture shows radiating linear shadows proceedingoutwards from the hilum. This is often accompanied by adiffuse mottling throughout the lung. When the con-dition is one of dense sclerosis, the lung is contracted andthe pleura thickened. Characteristically there is seen a,
IO9
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

BRITISH JOURNAL OF VENEREAL DISEASES
wedge-shaped shadow with its base at the hilum and withprocesses projecting into the surrounding pulmonarytissue. Syphilis appears to neglect almost entirely theupper lobes and to confine itself to the middle and lowerones. This is a diagnostic point of some value, since thereverse is the case in tuberculosis.Watkins points out that in order to differentiate be-
tween tuberculosis and syphilis of the lung in a radio-gram, there must be a clear conception of the pathologyof the two infections and the pathways by which theyattack the organ. The first distinguishing point is thatwhile in syphilis there is a perivascular infiltration, intuberculosis this infiltration spreads along the lymphchannels. The bronchioles within the lobule are accom-panied by branches of the pulmonary and bronchialarteries, but not by veins. The main lymphatic channelsare outside the lobule and accompany the veins. At theentrance to the lobule, the vein lies close to the bronchus,but it immediately separates from it and courses roundthe outside.
Tuberculosis proceeds along the main lymph channelsand proliferation occurs in the lymph tissue surroundingthe lobules. The shadow of tuberculosis is thus perilobularand is usually in the upper lobes and in relation to theapical and subpleural lobules. Syphilis, on the otherhand, attacks the hilum first, and, proceeding along thearteries, reaches the interior of the lobule. Its shadowis characteristically dense, irregular, and intra-lobular.Tubercular shadows have a distinct relationship to somebranch of the bronchial tree, while those of syphilis havenot. The latter shadows may have an irregular edge, thelung may show a mottled appearance, or there may bedense spike-like radiations.
Clinically it is found that the patient who is sufferingfrom pulmonary syphilis does not present a " tubercularappearance." He exhibits no progressive loss of weight,there is no marked anaemia, and he may even look ple-thoric. There are however many cases in which bothpulmonary syphilis and pulmonary tuberculosis are pre-sent together; and in such persons, the general health iswell maintained in spite of slight cavitation. They do not" go downhill " in the same manner as the pure " con-sumptive." Furthermore, the physical signs are usuallyunilateral and are more pronounced at the base of the lung.
IIO
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from

PULMONARY SYPHILIS
There is much sound sense in the institution of theroutine Wassermann by those who are dealing withpulmonary tuberculosis. It is well to keep in mind thepossibility of syphilis in every pulmonary conditionclinically resembling tuberculosis in general, but differingfrom it in certain particulars such as have been mentioned.The X-ray examination should be conducted, and theradiogram interpreted, in the light of the anatomicalpathways taken by the two diseases; not as is frequentlydone with the diagnosis of tuberculosis already made, asa means merely of accurately locating the seat of thedisease or of observing its progress. With experience, thedifferential diagnosis between the two conditions can bemade by the X-rays alone.One has found, from the frequency with which the
two diseases co-exist, that treatment is better carried outby bismuth than by the arsenicals. This is especially sowhen fever is present. It has seemed in several instancesthat arsenobenzol has had a stimulating effect upon thetuberculosis. Where the condition is one of fibrosis, thetubercular syphilitic does well under large doses ofiodides, and moderate doses of arsenobenzol with bismuthin alternate courses. In carrying out the therapeutic testone would rely upon bismuth alone.
REFERENCESCARRERA. Amer. Journ. of Syphilis, 1920, iv., I. (This paper is
provided with an excellent bibliography of I97 items.)The following are some of the chief contributions to the subject either
omitted by Carrera or published since the beginning of I920BAUCH. Med. Record, May, I9I6.BERIsso and ADELARDI. Rev. Stud-Amer. de Endocrin. Immunol. y
Quimioterap., I92I, iV., I.BoISLINIERE. Amer. Journ. of Syphilis, I9I9, iii., 472.CALLENDER. Interstate Med. Journ., June, I915.CANELLI. La Pediat., I919, xxvii., II.CARMAN. Amer. Journ. of Syphilis, I9I8, ii., 297.
Deut. Fortsch. a.d. Gebiete der Roentg., xxiv., I9I8-I9I9.DUNHAM. Stereo-Clinic, Sect. 38.EDELMANN. Wien. klin. Woch., No. 49, I9I9.HAWES. Boston M. and S. Journ., I924, cxc., 92.LEREDDE. Ann. des. Malad. Vener., I9I8, xiii., 760.MINTON. N.Y. Med. Journ., I92I, CXiii., 8I3.MOORE and CARMAN. Amer. Journ. Roentg., March, I9I6.MORRIS. Amer. Journ. of Syphilis, I9I8, ii., 23I.MUNRO. Lancet, December 30th, I922.OLIVER. Practitioner, I923, CXi., 249.
III
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
PLIQUE. Journ. de Mdi. et de Chirurg. prat., I9I8, lxxxix., 32I.POTTINGER. Amer. Journ. of Syphilis, I9I7, i., 7I8.RENTON. Lancet, March I7th, I923.SPENGLER. Arbeit. Tuberkulose und Syphilis,STIMSON. Amer. Journ. Med. Sc., I921, clxi., 740.STOKES. Modern Clinical Syphilology. Saunders & Co., London,
I926.TIECHE. Schweuzer. med. zevoch., I920, xxx., 65I.WARTHIN. Amer. Journ. of Syphilis, I9I7, i., 693.WARTHIN. Amer. Journ. of Svphilis, I9I8, H., 444.WATKINS. Amer. Journ. of Syphilis, I9I7, i., 760.WILE and MARSHALL. Arch. Dermat. and Syph., I92I, iv., 37.
II2
on 4 June 2019 by guest. Protected by copyright.
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.3.2.99 on 1 April 1927. D
ownloaded from