iacp 2015 eoin s (eoin-hp's conflicted copy 2015-10-16)
TRANSCRIPT
Conference 2015“Improving Therapeutic Relationships”
******
“The Therapeutic Relationship in the
Cognitive-Behavioural Therapies:
Past, Present & Future”
Eoin Stephens
Aim
To provide attendees with perspectives
which can enable them to incorporate
CBT approaches
into a Relational therapeutic framework.
Outline• Background
• Concerns, myths?
• Past: Main distinctive focus not Therapeutic Relat
BUT… Core Conditions…
• Present: Collaboration, Guided Discovery –“2 experts”
Triangular Model
• Future: Integration
Integrative CBT?
Background
• Many CBTs - Boundaries/definitions unclear
• Constantly Developinghttp://www.madinamerica.com/2015/03/cognitive-behavioural-therapy-
not-exist/
• CBT necessary but insufficient.
• Evidence Base v Face Value (client is still the expert).
• Evidence Base: Therapist also expert.
• Both Science and Art (like medicine)
• Good CBT v Bad CBT…
Cognitive Behavioural Therapies
• Cognitive Therapy – Aaron Beck
• Rational Emotive Behavioural Therapy –
Albert Ellis
• Reality Therapy – William Glasser
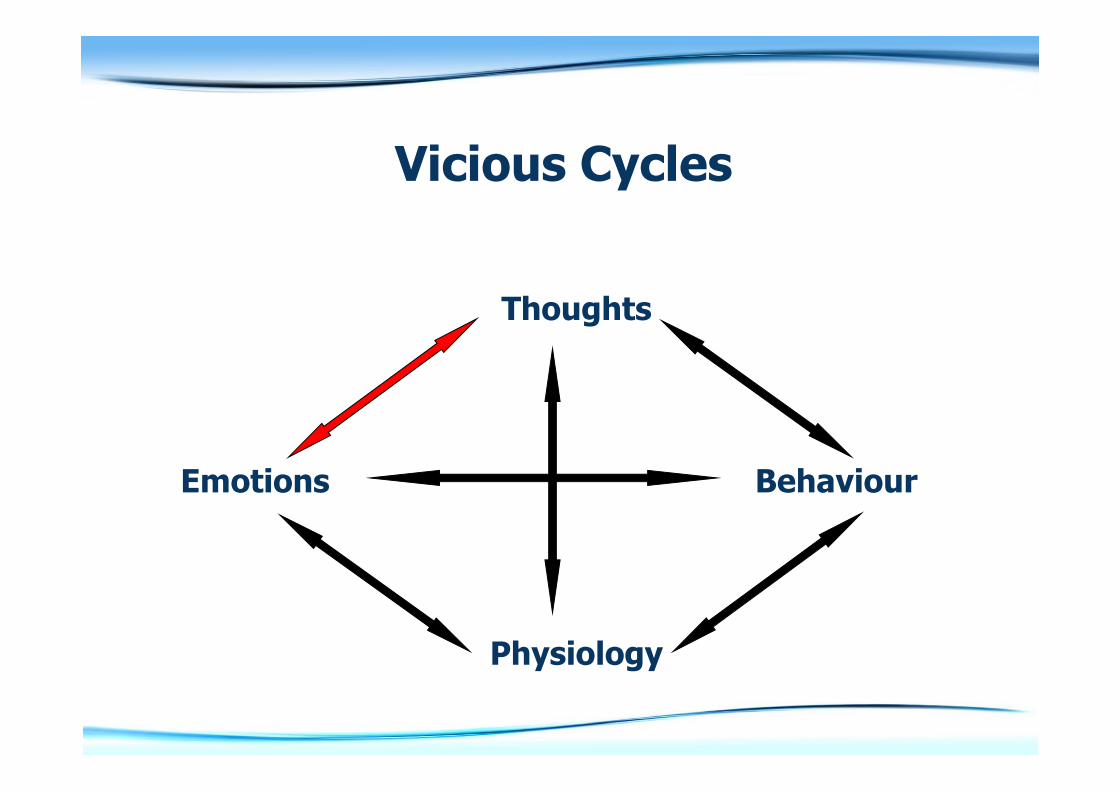
• CBT is based on the idea that how we think, how we act, how we feel and what goes on in our bodies all interact together.
• In particular, our thoughts strongly influence our feelings and behaviours, therefore any unhelpful, unrealistic or negative thoughts can be a major source of distress.
Why is the Therapeutic Relationship an issue?
Concerns/myths
re therapeutic relationship in CBT?
• Barely adequate, functional?
• Inadequate?
• Non-existent?
• Harsh, damaging?
Concerns/myths?
BACP Therapy Today articles, May 2015:
http://www.therapytoday.net/article/sho
w/4797/when-cbt-doesnt-help/
http://www.therapytoday.net/article/sho
w/4798/empathy-key-to-cbt/
PAST
• Main distinctive focus not Therapeutic Relationship
• But Beck: Core Conditions…
• Beck & Ellis – Collaboration & Disputation
• “Patient” v “Client”
• The various meanings of “expert”, and the issue of professional authority
• “Directive”, “Direct” & “Directional” – meanings and connotations
• Guided Discovery…
Beck - Cognitive Therapy
• Collaborative
• Guided Discovery
• Specific issues, diagnoses
• Specific (cognitive) models
• Case Formulation approach
• Including relevance of the past
• Core Conditions
• Integrative perspective
Principles of Cognitive Therapy (J. Beck, 1995)
• Cognitive therapy is based on an ever-evolving formulation of the client and their problems in cognitive terms.
• Cognitive therapy requires a sound therapeutic alliance.
• Cognitive therapy emphasises collaboration and active participation.
• Cognitive therapy is goal oriented and problem focused.
• Cognitive therapy initially emphasises the present.
• Cognitive therapy is educative, aims to teach the client to be his or her own therapist, and emphasises relapse prevention.
• Cognitive therapy aims to be time limited.
• Cognitive therapy sessions are structured.
• Cognitive therapy teaches clients to identify, evaluate and respond to their dysfunctional thoughts and beliefs.
• Cognitive therapy uses a variety of techniques to change thinking, mood and behaviour.
Some well-established
Cognitive Interventions
• Distraction
• Identification of relevant cognitions
(NATs, assumptions, core beliefs, cognitive distortions)
• Socratic Questioning
• Double Standard method
• Coping self talk
• …
Some well-established
Behavioural Interventions
• Activity Monitoring
• Increasing pleasurable activities.
• Behavioural Experiments - test predictions.
• Graded exposure
• …
PRESENT
• Protocols for specific Mental Health issues + Individualised Case Formulation
• Psychoeducation, Self-Help
• Structured & Facilitated Self-Help, Stepped Care
• Collaborative, Guided Discovery – “2 experts”
• The closeness of Cognition & Emotion – “Hot Cognition”
• Socratic Questioning & Cognitive-Emotional Empathy
• “3rd Generation” Approaches
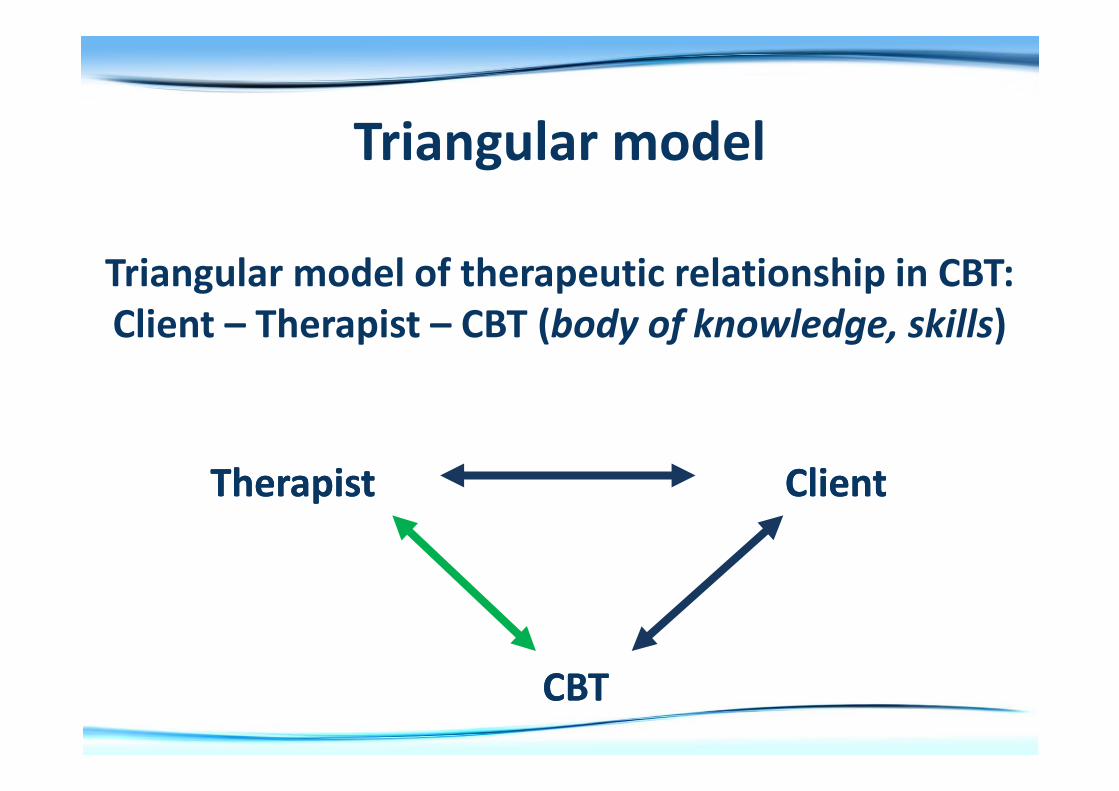
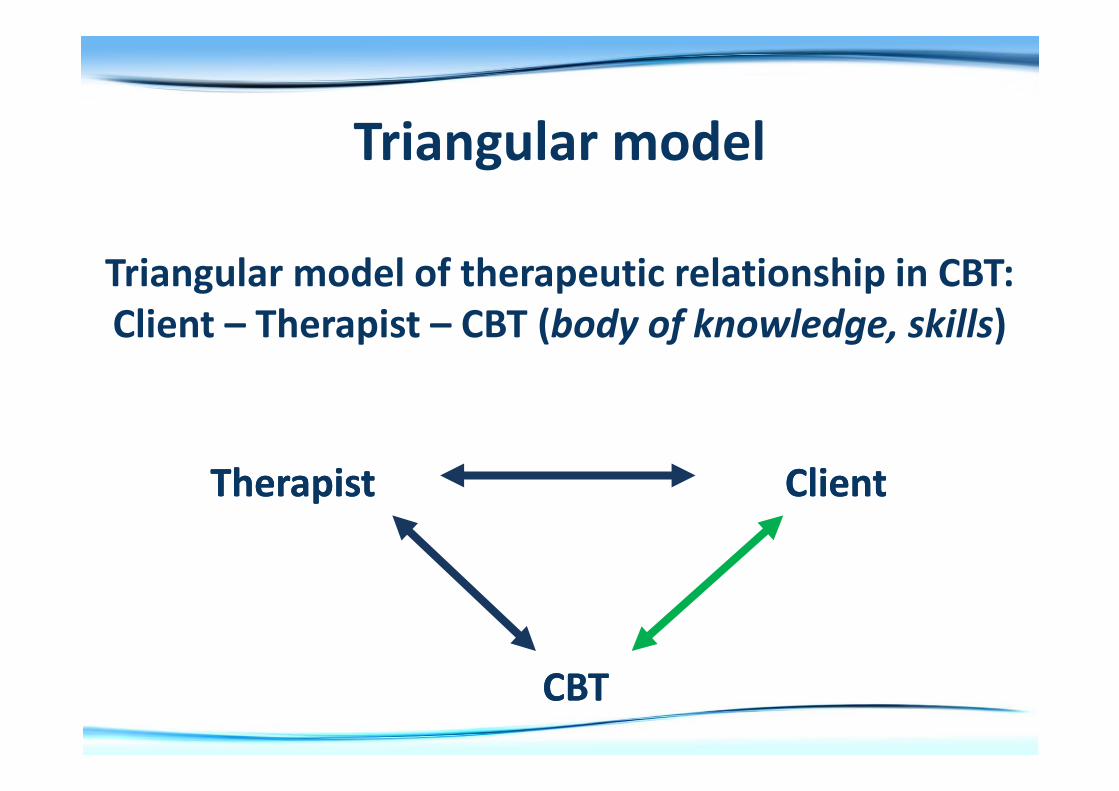
• CBT as the “third member” of the therapeutic relationship
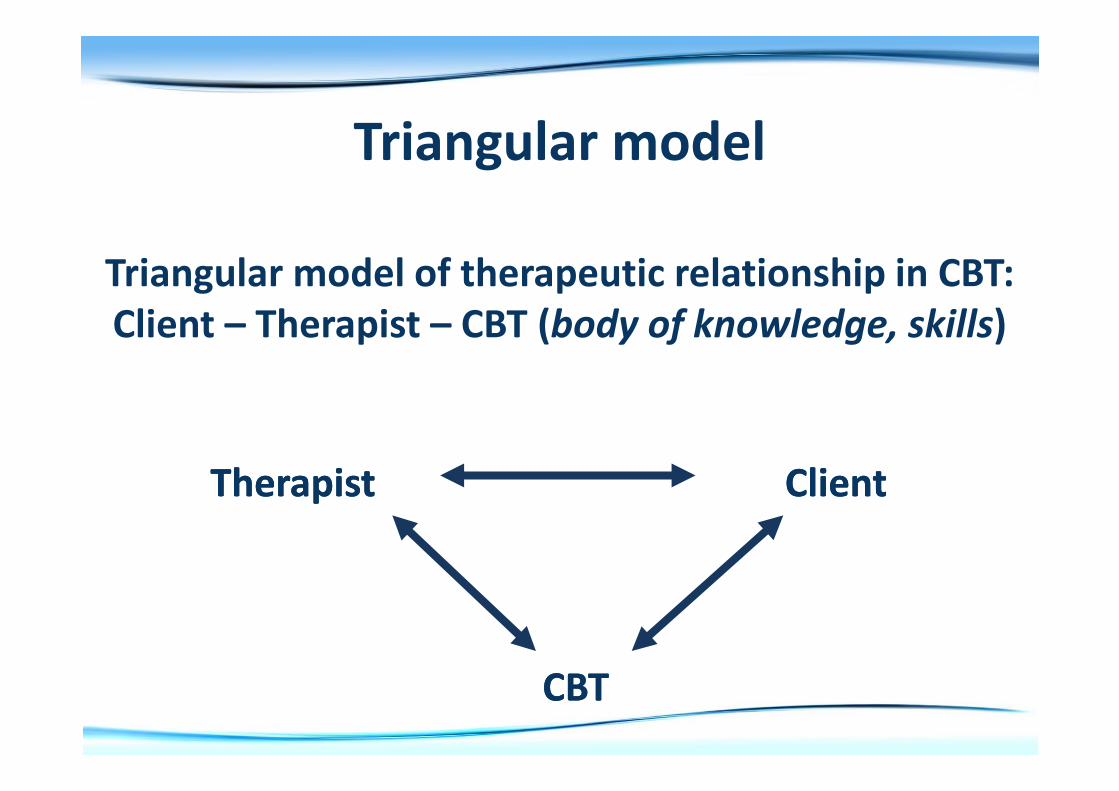
Triangular model
Triangular model of therapeutic relationship in CBT:
Client – Therapist – CBT (body of knowledge, skills)
Therapist Client
CBT
Therapist Client
CBT
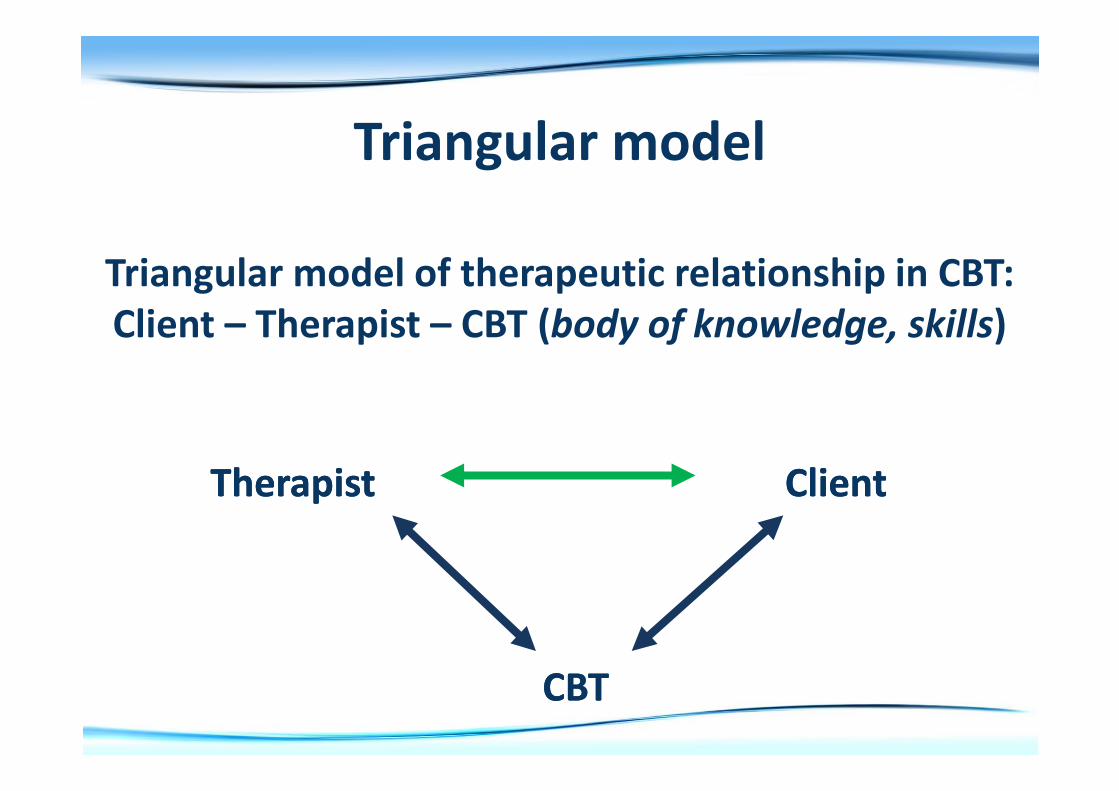
Triangular model
Triangular model of therapeutic relationship in CBT:
Client – Therapist – CBT (body of knowledge, skills)
Therapist Client
CBT
Therapist Client
CBT
Triangular model
Triangular model of therapeutic relationship in CBT:
Client – Therapist – CBT (body of knowledge, skills)
Therapist Client
CBT
Therapist Client
CBT
Triangular model
Triangular model of therapeutic relationship in CBT:
Client – Therapist – CBT (body of knowledge, skills)
Therapist Client
CBT
Therapist Client
CBT
Thoughts
Emotions Behaviour
Physiology
Vicious Cycles
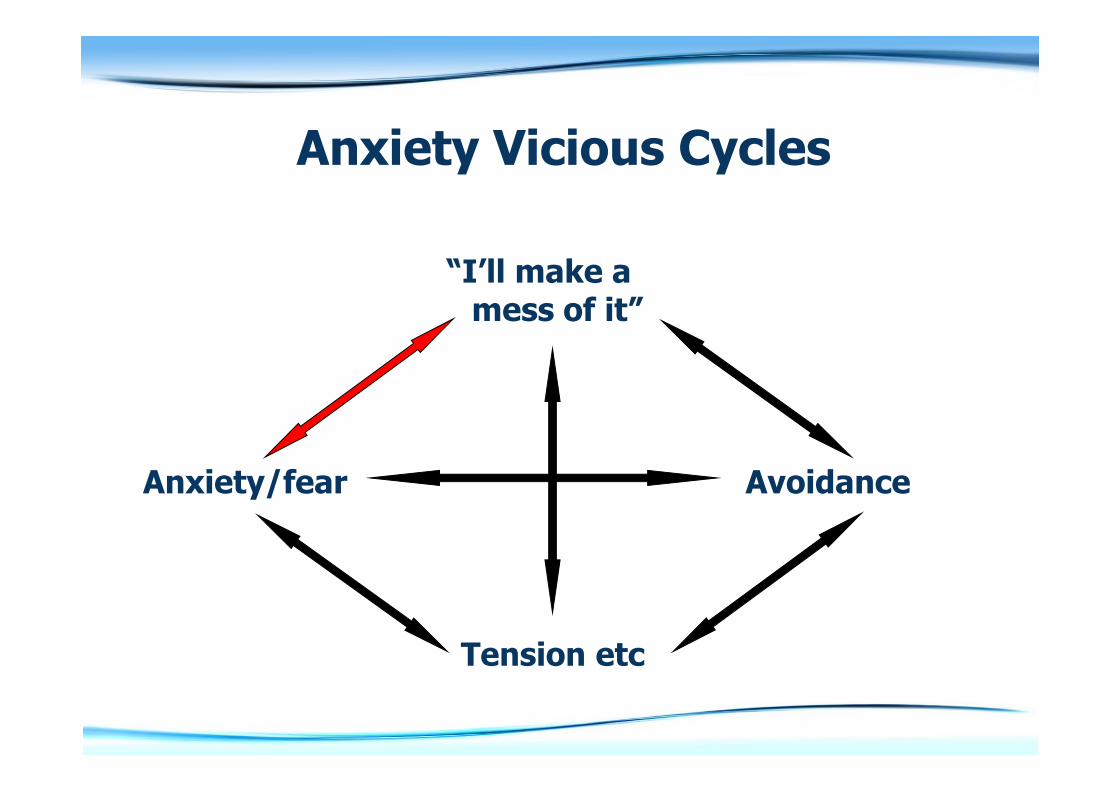
“I’ll make amess of it”
Anxiety/fear Avoidance
Tension etc
Anxiety Vicious Cycles
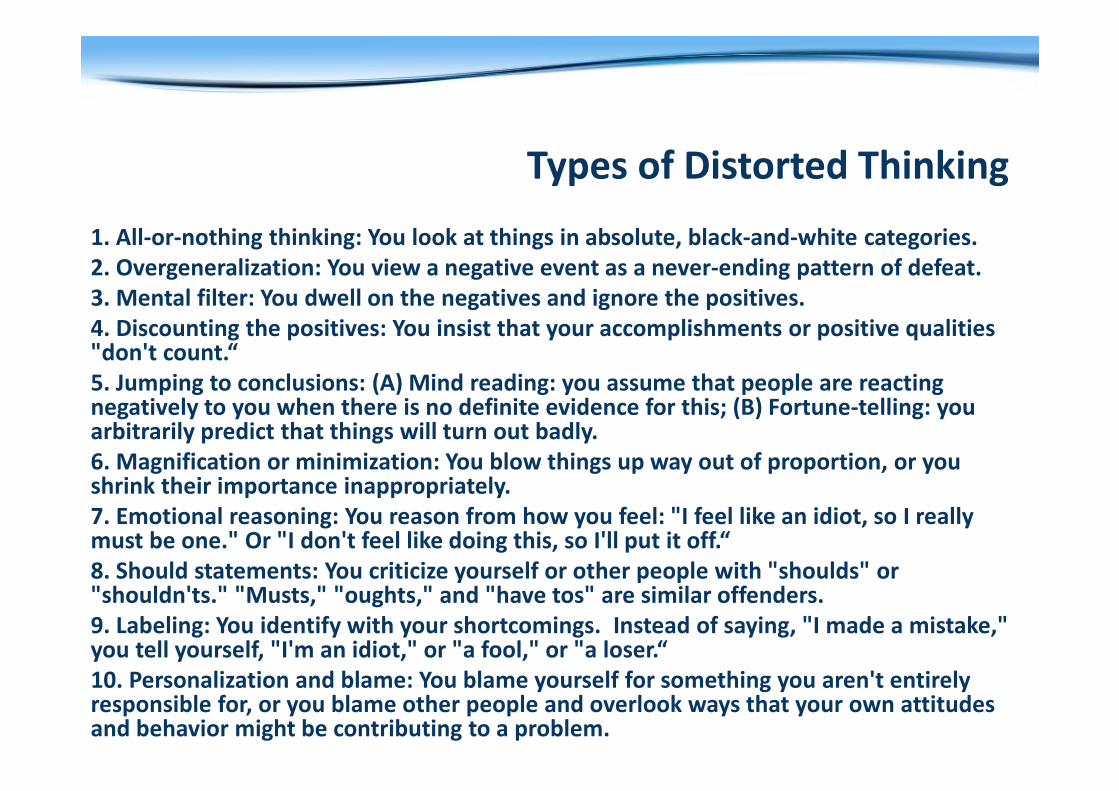
Types of Distorted Thinking
1. All-or-nothing thinking: You look at things in absolute, black-and-white categories.
2. Overgeneralization: You view a negative event as a never-ending pattern of defeat.
3. Mental filter: You dwell on the negatives and ignore the positives.
4. Discounting the positives: You insist that your accomplishments or positive qualities "don't count.“
5. Jumping to conclusions: (A) Mind reading: you assume that people are reacting negatively to you when there is no definite evidence for this; (B) Fortune-telling: you arbitrarily predict that things will turn out badly.
6. Magnification or minimization: You blow things up way out of proportion, or you shrink their importance inappropriately.
7. Emotional reasoning: You reason from how you feel: "I feel like an idiot, so I really must be one." Or "I don't feel like doing this, so I'll put it off.“
8. Should statements: You criticize yourself or other people with "shoulds" or "shouldn'ts." "Musts," "oughts," and "have tos" are similar offenders.
9. Labeling: You identify with your shortcomings. Instead of saying, "I made a mistake," you tell yourself, "I'm an idiot," or "a fool," or "a loser.“
10. Personalization and blame: You blame yourself for something you aren't entirely responsible for, or you blame other people and overlook ways that your own attitudes and behavior might be contributing to a problem.
An overanxious/depressed personno longer learns from experience,
because the Cycle of Experiential Learning
has become blocked.
CBT tries to unblock the vicious cycles= Experiential Relearning.
This can take place with a therapist,but this is not always necessary,
self-help may be sufficient.
FUTURE?
• Learning theory + Relational theory
• Experiential learning as a core framework
• 3rd Generation Approaches
• Integration – e.g. Integrative CBT
“3rd Generation” of CBT approaches
Dialectical Behaviour Therapy (Linehan)
Mindfulness-Based Cognitive Therapy (Williams et al)
Acceptance & Commitment Therapy (Hayes)
Compassion Focused Therapy (Gilbert)
Schema Therapy (Young)
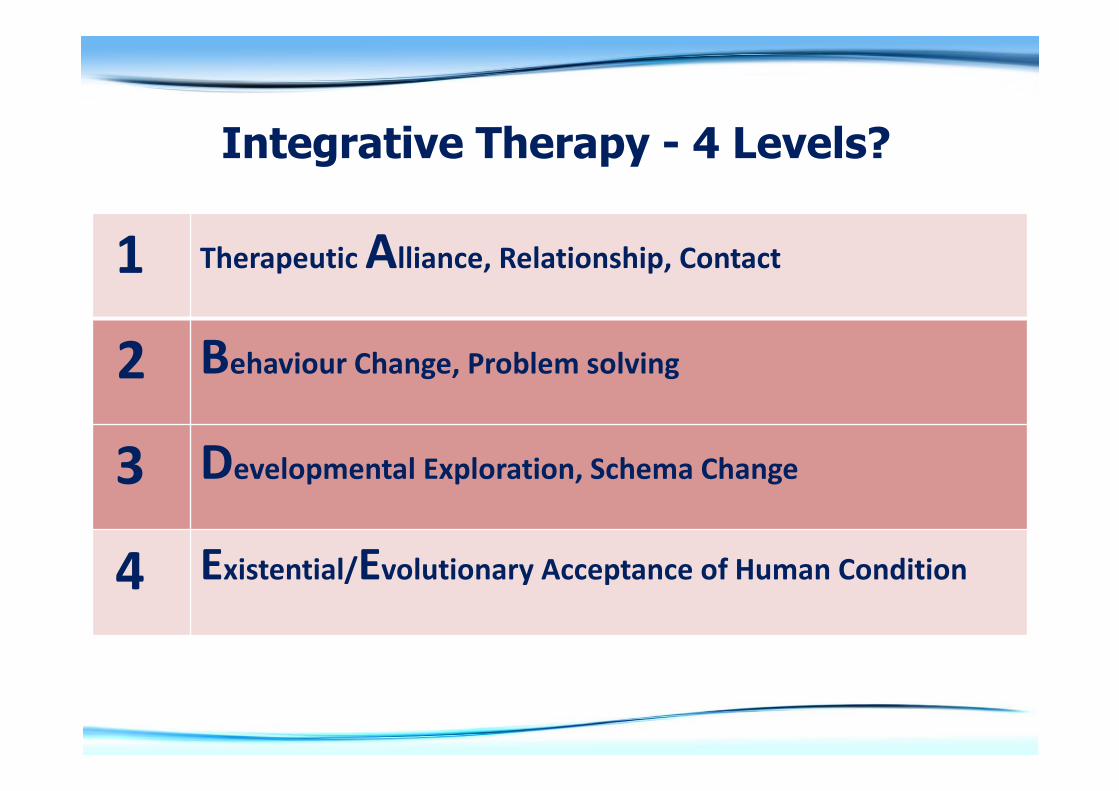
Integrative Therapy - 4 Levels?
1 Therapeutic Alliance, Relationship, Contact
2 Behaviour Change, Problem solving
3 Developmental Exploration, Schema Change
4 Existential/Evolutionary Acceptance of Human Condition
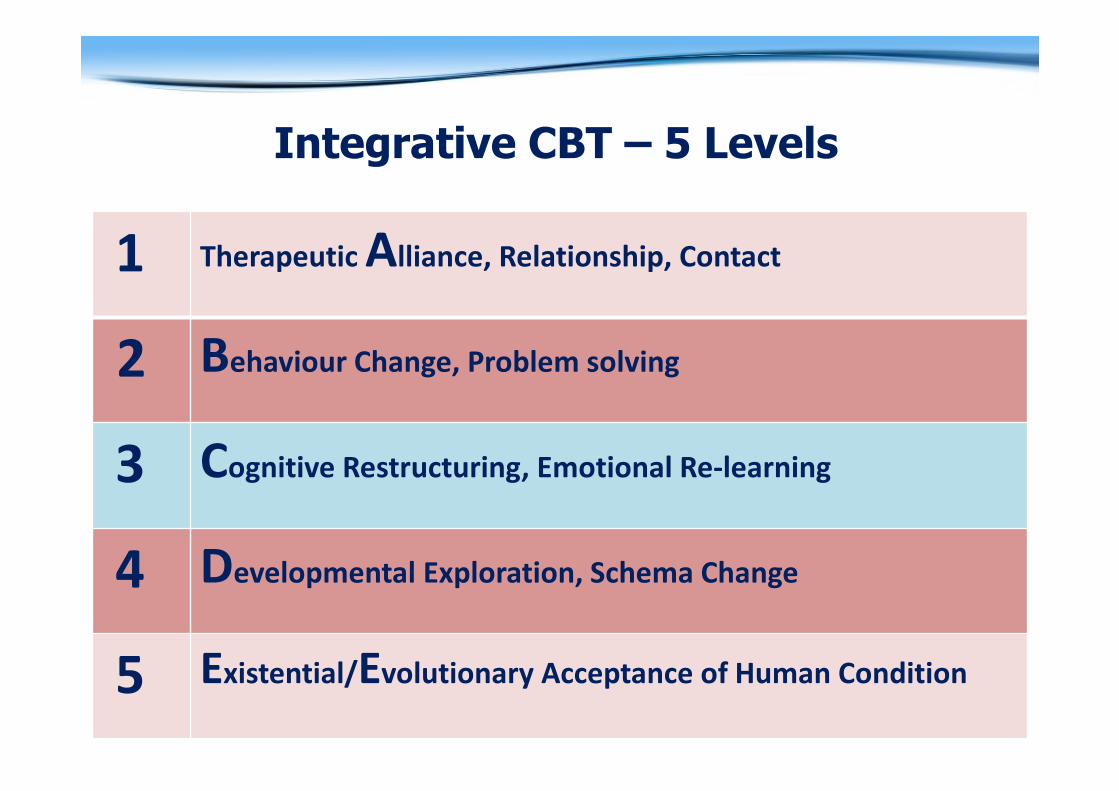
Integrative CBT – 5 Levels
1 Therapeutic Alliance, Relationship, Contact
2 Behaviour Change, Problem solving
3 Cognitive Restructuring, Emotional Re-learning
4 Developmental Exploration, Schema Change
5 Existential/Evolutionary Acceptance of Human Condition
1 Therapeutic Alliance,
Therapeutic Relating
Integrative CBT needs to be first of all grounded in a
therapeutic relationship,
where skills such as Active Listening, Advanced Empathy
etc are used to enable the client to experience the
therapeutic benefits of a helping human encounter.
Sometimes this is all a client needs: containing, holding,
support, validation, a safe space to explore their world
and their concerns. For other clients, this working alliance
serves as the basis for work at the other levels below.
At this level, much can be learned from Humanistic
approaches such as
Person-Centred Therapy and Gestalt Therapy.
2 Behavioural Intervention,
Practical Problem-Solving
The next level many clients need, to create change in their
lives, is problem-clarification & practical action, where they
can be helped to engage effectively with their environment
by decreasing negative behaviours (e.g. social avoidance,
passive/aggressive behaviours) & increasing positive
behaviours (using social supports, asserting oneself). This can
be achieved both by introducing them to general principles
of change such as goal-setting, planning, reviewing, as well
as by introducing specific life-skills training in areas like stress
management, assertiveness, decision-making.
Useful approaches which can be incorporated here are
Egan’s Skilled Helper Model, Glasser’s Choice
Theory, and Motivational Interviewing.
3 Cognitive Restructuring,
Cognitive-Emotional Re-learning
The next level of intervention which may be needed
(especially for those with specific mental health issues such as
Addiction, Depression, etc) is collaborative, educative
Cognitive/Emotional re-learning. Here we help the client
untangle self-perpetuating vicious cycles between their
Environment, Cognition, Emotion, Behaviour and Physiology,
so that they can unlearn what is dysfunctional and learn new,
more functional, approaches. Guided Discovery processes
such as Socratic Questioning and Behavioural
Experimentation are used at this level, and many techniques
from other approaches can also be usefully integrated;
Mindfulness is a well-known example.
Cognitive Therapy & REBT are relevant here.
4 Developmental Exploration,
Schema Change
Integrative CBT sees detailed exploration of the client’s past,
and especially their early development, as essential -
though it may or may not need to be the immediate or
central focus of therapy, depending on the client’s issues
and goals. Longer-term developmental work, involving
more detailed life-history exploration and deeper
Cognitive/Emotional restructuring at the level of Core
Beliefs, can help clients to gain a broader understanding of
the sources of their difficulties, as well as increasing
resistance to relapse through lessening the influence of
maladaptive Core Beliefs/Schemas.
Freudian/Jungian approaches, Attachment
Theory, Schema Therapy, can be useful here.
5 Existential/Evolutionary Acceptance,
Embracing the Human Condition
As not all difficulties can be resolved via therapy, clients may
need help to process the remaining realities of the human
condition. These may be specific to circumstances or particular
mental health issues (long-term health issues, separation, wasted
career potential, partially-healed trauma), or may arise from evolved
species vulnerabilities (taste for sugar, anxiety about status/meaning),
or from the nature of life (rejection, loss, age, death).
The therapist helps the client toward greater understanding of
themselves as a human being, incorporating whatever philosophical,
cultural, scientific, existential, spiritual perspectives are relevant.
Focusing on what it means to be human can help clients to more
deeply understand not just why they are individually vulnerable to
depression or addiction, but why humans in general are vulnerable.
This can help de-stigmatise problems, developing self-compassion.
Existential Approaches, Evolutionary Theory, etc, etc can be relevant here.

More info at
integrativecbt.com
Bibliography
Alford, B.A. & Beck, A.T. (1998) The Integrative Power of Cognitive Therapy. New York: Guilford Press.
Beck, J. (1995). Cognitive Therapy: Basics and beyond. New York: Guilford Press.
Gilbert, P. & Leahy, R.L. (2009) The Therapeutic Relationship in the Cognitive Behavioural Psychotherapies. London: Routledge
Thagard, P. (2008) Hot Thought: Mechanisms and Applications of Emotional Cognition. Cambridge MA: Bradford Books.
Wills, F. & Sanders, D. (2012). Cognitive Behaviour Therapy: Foundations for practice. London: Sage.
Weishaar, M. E. (1993). Aaron T. Beck. London: Sage.
Video clips
Beck (on Case Formulation)https://www.youtube.com/watch?v=SJ2J9um-nMA
Ellis (Gloria)https://www.youtube.com/watch?v=odnoF8V3g6g
