i i iiii 9 i ii i ii pityriasis rubra pilaris: a review of diagnosis and...
TRANSCRIPT

Clinica l r e v i e w
I I IIII �9 I II I I I
Pityriasis rubra pilaris: A review treatment
of diagnosis and
Philip R. Cohen, MD, and Janet H. Prystowsky, MD, PhD New York, New York
The diagnosis of pityriasis rubra pilaris is based essentially on characteristic clinical features. Although the histologic features are not pathognomonic, a lesional skin biopsy for evaluation is important to rule out other papulosquamous and erythematous disorders. The presence of prominent seborrheic keratoses occurring in two cases of pityriasis rubra pilaris is presented. Our understanding of the relationship between vitamin A metabolism and pityriasis rubra pilaris is discussed. Currently available systemic therapeutic modalities for pityriasis rubra pilaris are reviewed. Although pityriasis rubra pilaris does not represent a vitamin A deficiency state, it is responsive to isotretinoin, etretinate, and vitamin A. Antimetabolites remain an alternative therapy. (J AM AcAD DERM^TOL 1989;20:801-7.)
The five clinical types of pityriasis rubra pilaris, as categorized by Griffiths, are based on age of onset, cutaneous features, disease course, and prog- nosis (Table I)? "6 We report two cases of classic adult (type I) pityriasis rubra pilaris with promi- nent seborrheic keratoses. We review its clinical and histologic features and the prior and current systemic therapeutic modalities for this condition. In addition, we discuss our current understanding of vitamin A metabolism in patients with pityriasis rubra pilaris.
CASE REPORTS Case 1
An 85-year-old white woman had pruritus, progres- sive erythroderma, and multiple accentuated seborrheic keratoses. Examination revealed an extensive erythro- derma with randomly distributed patches of normal skin ("islands of sparing"). The palmar and plantar surfaces were hyperkeratotic and fissured with large areas of peeling. Other findings included bilateral ectropions, subungual hyperkeratosis, nail plate thickening with a distal yellow-brown discoloration, sprinter hemorrhages, and prominent seborrheic keratoses. Physical, neurolog- ic, and gastrointestinal evaluation showed negative find-
From the Department of Dermatology, Col/ege of Physicians and Surgeons of Columbia University.
Reprint requests: Philip R. Cohen, MD, Department of Dermatology, College of Physicians and Surgeons of Columbia University, 630 W. t6gth St., New York, NY 10032.
ings for underlying disease. Histologic evaluation of multiple skin biopsy specimens showed orthokeratosis, mild acanthosis, and a confluent granular layer in the epidermis. A perivascular mononuclear cell infiltrate was observed in the papillary dermis. Neither a 3-week course of oral prednisone nor the daffy oral administra- tion of vitamin A, 200,000 IU, improved her condition. Although modified Goeckerman therapy relieved the pruritus, the erythroderma persisted. Oral isotretinoin (0.4 mg/kg/day) was initiated. After 2 weeks the hyperkeratosis of the palms and soles had resolved and the daffy dose was doubled. Within 2 more weeks the erythroderma began to dissipate. The patient was main- rained on a regimen of isotretinoin, 0.8 mg/kg/day, and continues to improve.
Case 2
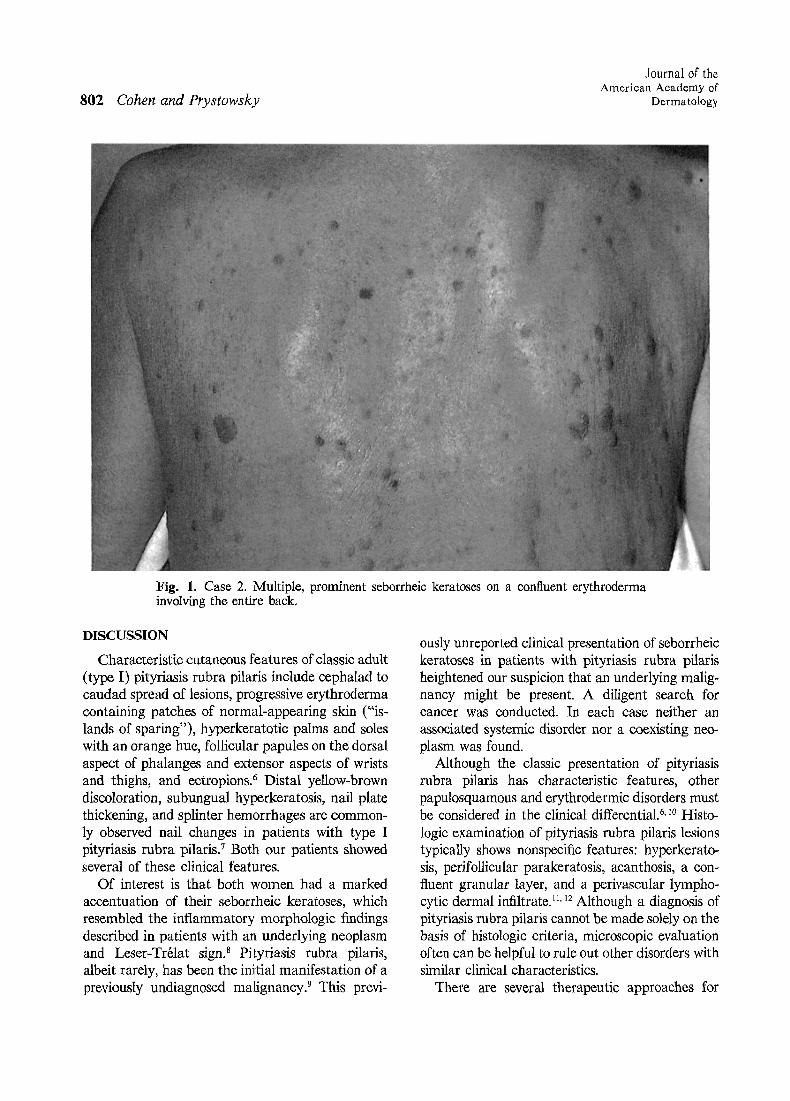
A 72-year-old white woman had an exfoliative eryth- roderma and numerous seborrheic keratoses. Significant findings on examination included an orange-hued exfo- liative erythroderma involving nearly the entire body, with rare areas of normal-appearing skin, palmar and plantar hyperkeratosis, distal ortycholysis, and bilateral ectropions. Multiple prominent seborrheic keratoses were present on her chest, abdomen, and back (Fig. 1). Neither cancer nor an associated systemic disease was found on complete physical and laboratory evaluation. Microscopic evaluation of her lesional skin biopsy spec- imens showed changes consistent with pityriasis rubra pilaris. Isotretinoin therapy was initiated at 1.0 rag/ kg/day. Within 7 to 10 days clinical improvement began. Subsequently, the patient was maintained on isotretinoin therapy.
801
802 Cohen and Prystowsky
Journal of the American Academy of
Dermatology
Fig. 1. Case 2. Multiple, prominent seborrheic keratoses on a confluent erythroderma involving the entire back.
DISCUSSION
Characteristic cutaneous features of classic adult (type I) pityriasis rubra pilaris include cephalad to caudad spread of lesions, progressive erythroderma containing patches of normal-appearing skin ("is- lands of sparing"), hyperkeratotic palms and soles with an orange hue, follicular papules on the dorsal aspect of phalanges and extensor aspects of wrists and thighs, and ectropions. ~ Distal yellow-brown discoloration, subungual hyperkeratosis, nail plate thickening, and splinter hemorrhages are common- ly observed nail changes in patients with type I pityriasis rubra pilaris. 7 Both our patients showed several of these clinical features.
Of interest is that both women had a marked accentuation of their seborrheic keratoses, which resembled the inflammatory morphologic findings described in patients with an underlying neoplasm and Leser-Tr61at sign3 Pityriasis rubra pilaris, albeit rarely, has been the initial manifestation of a previously undiagnosed malignancy? This previ-
ously unreported clinical presentation of seborrheic keratoses in patients with pityriasis rubra pilaris heightened our suspicion that an underlying malig- nancy might be present. A diligent search for cancer was conducted. In each case neither an associated systemic disorder nor a coexisting neo- plasm was found.
Although the classic presentation of pityriasis rubra pilaris has characteristic features, other papulosquamous and erythrodermic disorders must be considered in the clinical differential. 6, z0 Histo- logic examination of pityriasis rubra pilaris lesions typically shows nonspecific features: hyperkerato- sis, perifollicular parakeratosis, acanthosis, a con- fluent granular tayer, and a perivascular lympho- cytic dermal infiltrate. 1I, 12 Although a diagnosis of pityriasis rubra pilaris cannot be made solely on the basis of histologic criteria, microscopic evaluation often can be helpful to rule out other disorders with similar clinical characteristics.
There are several therapeutic approaches for

Volume 20 Number 5, Part 1 May 1989 Pityriasis rubra pilaris 803
Table I. Clinical characteristics of pityriasis rubra pilaris
I Incidence I Clear in 3 yr Type (%) (%)
Adult Classic (I) 50 81
Atypical (II) 5 20
Juvenile Classic (III) 10 16
Circumscribed (IV) 25 32
Atypical (V) 5 0
Characteristics
Acute onset; no precipitating factors; occasional pruritus; "classic" features
Long duration; alopecia; iehthyosiform scaling; eczematous areas
Onset before age of 2 yr; similar features to type [
Focal areas of erythema and hyperkeratosis; rarely progresses
Early Onset and chronic course; predominantly hyperkeratosis; infrequent erythema; seleroderrna-like changes on the palms and soles
Modified from Griffiths WAD. Br J Dermatol 1977;97(suppl 15):18 and from Griffiths WAD. Clin Exp Dermatol 1980;5:105-12.
patients with pityriasis rubra pilaris (Table II). 6,12-42 Clinical improvement and resolution of pityriasis rubra pilaris have been reported within 3 years in 81% of classic adult (type I) cases. Other types have a poorer prognosis for remission (Table I). 6 Currently, retinoids 12"23 and antimetabolites 6,~8"32 are the most successful therapies.
Vitamin A therapy has been successful but may be associated with toxicity because high doses are necessary.~5' 24-26 Patients with pityriasis rubra pilar- is responded favorably when vitamin A was admin- istered either topically (250,000 to 500,000 IU/ ounce of Lubriderm lotion) 27 or systemically.tS. 2,26 Although clinical improvement within 2 months of initiation of topical vitamin A therapy Was observed in a preliminary study involving two patients, z7 the evaluation of additional patients treated with topical vitamin A would be necessary to confirm the potential efficacy of this treatment modality. Many patients with pityriasis rubra pilaris have been treated with high dosages (150,000 to 300,000 IU/day) of oral vitam{n A. ~5 When treated at this dosage, approximately one third of patients improved, t5 Initial therapy usually is tolerated well and rarely causes an adverse effect; however, clinical data regarding long-term treatment andthe incidence of vitamin A toxicity have not been reported. It is worth noting that the recommended dietary allowance of vitamin A is 5000 IU. 43 Hypervitaminosis A has been reported in adults receiving prolonged daily administration
Table II. Therapeutic approaches for pityriasis rubra pilaris
Therapy Reference No.
Retinoids Isotretinoin 13-16 Etretinate 12,17-23 Vitamin A 15,24-27
Antimetabolites Methotrexate 6,28-31 Azathioprine 6,32
Other agents Vitamins (C and E) 33,34 Stanozolol 35,36 Antituberculous 37 Antibiotics 37,38 Antimalarials 37 Arsenic 27 Pilocarpine 27 Pituitary and foreign 27
proteins 6-Aminonicotinamide 39,40
Phototherapy PUVA 6,12,14,15,19,21,41,42 Ultraviolet B 15,24,42
of 50,000 IU of vitamin A. 44,45 Thus the potential for hypervitaminosis clearly is present when high doses of vitamin A are used. Follow-up to monitor for signs of vitamin A toxicity is imperative. Megadose oral vitamin A therapy (usually 1 million IU/day for 10 to 14 days) also has been used effectively but with a higher incidence of side
804 Cohen and Prystowsky
Journal of the Amer ican Academy of
Dermatology
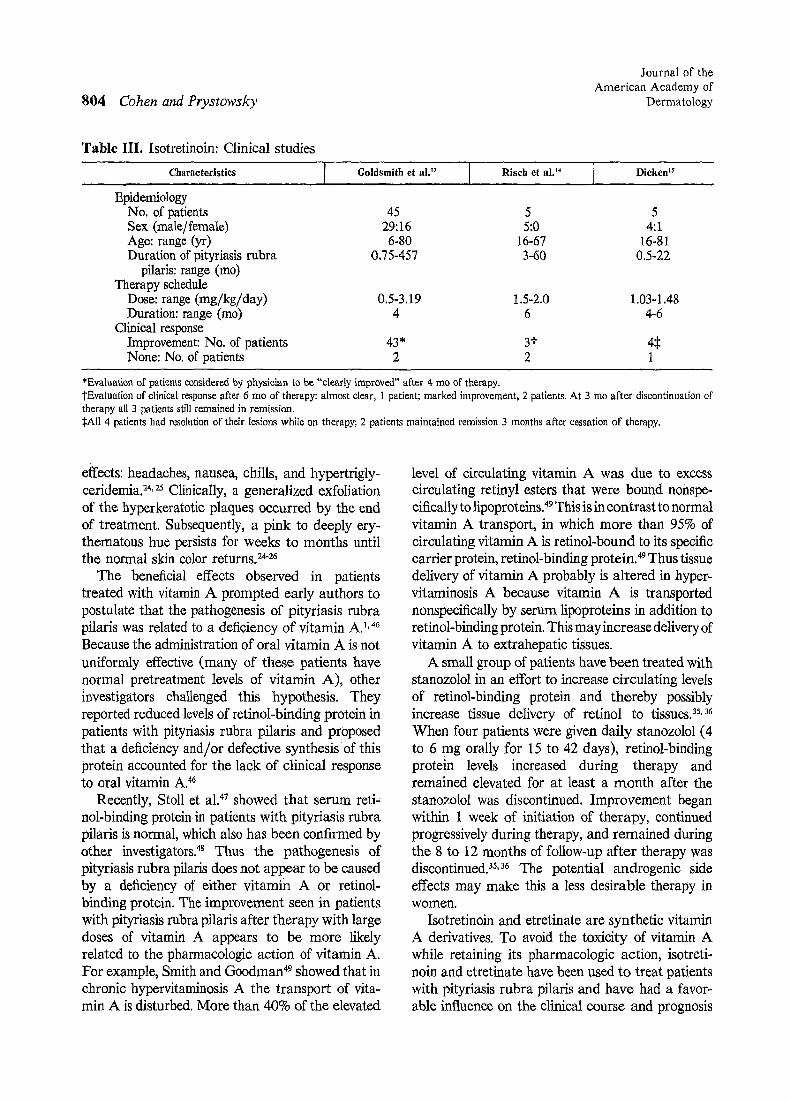
Table III. Isotretinoin: Clinical studies
Characteristics [ Goldsmith et al. t~ ] Risch et a12 4 . Dieken 15
Epidemiology No. of patients 45 5 5 Sex (male/female) 29:16 5:0 4:1 Age: range (yr) 6-80 16-67 16-81 Duration of pityriasis rubra 0.75-457 3-60 0.5-22
pilaris: range (too) Therapy schedule
Dose: range (mg/kg/day) 0.5-3.19 1.5-2.0 1.03-1.48 Duration: range (mo) 4 6 4-6
Clinical response Improvement: No. of patients 43* 31- 4:~ None: No. of patients 2 2 1
*Evaluation of patients considered by physician to be "clearly improved" after 4 mo of therapy. revaluation of clinical response after 6 mo of therapy: almost dear, 1 patient; marked improvement, 2 patients. At 3 mo after discontinuation of therapy all 3 patients still remained in remission. :gAll 4 patients had resolution of their lesions while on therapy; 2 patients maintained remission 3 months after cessation of therapy.
effects: headaches, nausea, chills, and hypertrigly- ceridemia? 4,25 Clinically, a generalized exfoliation of the hyperkeratotic plaques occurred by the end of treatment. Subsequently, a pink to deeply ery- thematous hue persists for weeks to months until the normal skin color returns. 24-26
The beneficial effects observed in patients treated with vitamin A prompted early authors to postulate that the pathogenesis of pityriasis rubra pilaris was related to a deficiency of vitamin A. TM
Because the administration of oral vitamin A is not uniformly effective (many of these patients have normal pretreatment levels of vitamin A), other investigators challenged this hypothesis. They reported reduced levels of retinoi-binding protein in patients with pityriasis rubra pilaris and proposed that a deficiency and/or defective synthesis of this protein accounted for the lack of clinical response to oral vitamin A. 46
Recently, Stoll et al. 47 showed that serum reti, nol-binding protein in patients with pityriasis rubra pilaris is normal, which also has been confirmed by other investigators. 48 Thus the pathogenesis of pityriasis rubra pilaris does not appear to be caused by a deficiency of either vitamin A or retinol- binding protein. The improvement seen in patients with pityriasis rubra pilaris after therapy with large doses of vitamin A appears to be more likely related to the pharmacologic action of vitamin A. For example, Smith and Goodman 49 showed that in chronic hypervitaminosis A the transport of vita- min A is disturbed. More than 40% of the elevated
level of circulating vitamin A was due to excess circulating retinyl esters that were bound nonspe- cifically to lipoproteins. 49 This is in contrast to normal vitamin A transport, in which more than 95% of circulating vitamin A is retinol-bound to its specific carrier protein, retinol-binding protein. 49 Thus tissue delivery of vitamin A probably is altered in hyper- vitaminosis A because vitamin A is transported nonspecifically by serum lipoproteins in addition to retinol-binding protein. This may increase delivery of vitamin A to extrahepatic tissues.
A small group of patients have been treated with stanozolol in an effort to increase circulating levels of retinol-binding protein and thereby possibly increase tissue delivery of retinol to tissues? s,36 When four patients were given daily stanozolol (4 to 6 mg orally for 15 to 42 days), retinol-binding protein levels increased during therapy and remained elevated for at least a month after the stanozolol was discontinued. Improvement began within 1 week of initiation of therapy, continued progressively during therapy, and remained during the 8 to 12 months of follow-up after therapy was discontinued? TM The potential androgenic side effects may make this a less desirable therapy in women.
Isotretinoin and etretinate are synthetic vitamin A derivatives. To avoid the toxicity of vitamin A while retaining its pharmacologic action, isotreti- noin and etretinate have been used to treat patients with pityriasis rubra pilaris and have had a favor- able influence on the clinical course and prognosis
Volume 20 Number 5, Part 1 May 1989 Pityriasis rubra pilaris 805
for many patients. 12-2~ Clinical characteristics of three representative isotretinoin studies are sum- marized in Table III. 13-~5 Isotretinoin has been effective in both men and women with either juvenile or adult type pityriasis rubra pilaris. Between 60.0% to 95.5% of patients had clinical improvement within 4 to 6 months after starting isotretinoin therapy. The clinical response was independent of the duration of pityriasis rubra pilaris before initiation of isotretinoin therapy. 13 Although the daily dosage varied from 0.5 to 3.19 mg/kg/day, later studies demonstrated clinical improvement at lower dosages of 1.0 to 1.5 mg/ kg/day.t4, ms
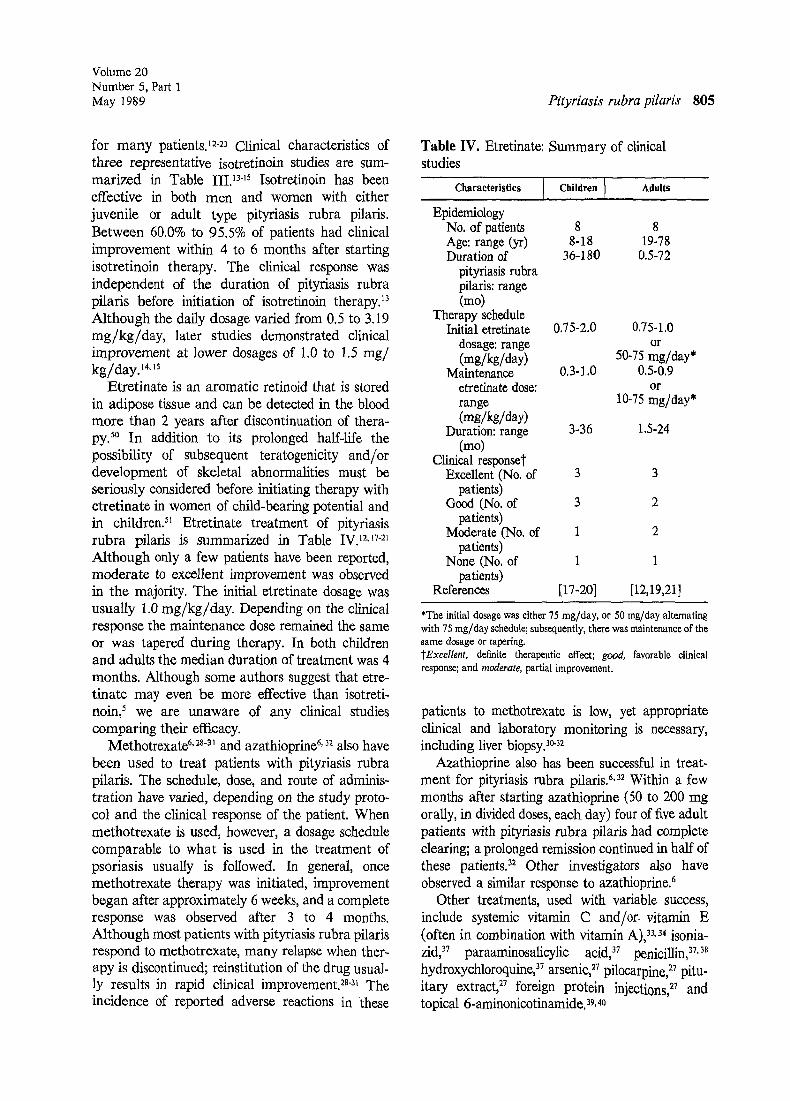
Etretinate is an aromatic retinoid that is stored in adipose tissue and can be detected in the blood more than 2 years after discontinuation of thera- py.5O In addition to its prolonged half-life the possibility of subsequent teratogenicity and/or development of skeletal abnormalities must be seriously considered before initiating therapy with etretinate in women of child-bearing potential and in children? 1 Etretinate treatment of pityriasis rubra pilaris is summarized in Table IV. ~2,17a~ Although only a few patients have been reported, moderate to excellent improvement was observed in the majority. The initial etretinate dosage was usually 1.0 mg/kg/day. Depending on the clinical response the maintenance dose remained the same or was tapered during therapy. In both children and adults the median duration of treatment was 4 months. Although some authors suggest that etre- tinate may even be more effective than isotreti- noin, 5 we are unaware of any clinical studies comparing their efficacy.
Methotrexate 6. :8-3~ and azathioprine 6, 3~ also have been used to treat patients with pityriasis rubra pilaris. The schedule, dose, and route of adminis- tration have varied, depending on the study proto- col and the clinical response of the patient. When methotrexate is used, however, a dosage schedule comparable to what is used in the treatment of psoriasis usually is followed. In general, once methotrexate therapy was initiated, improvement began after approximately 6 weeks, and a complete response was observed after 3 to 4 months. Although most patients with pityriasis rubra pilaris respond to methotrexate, many relapse when ther- apy is discontinued; reinstitution of the drug usual- ly results in rapid clinical improvement, w3t The incidence of reported adverse reactions in these
Table IV. Etretinate: Summary of clinical studies
Characteristics [., Children,, Adults
Epidemiology No. of patients 8 8 Age: range (yr) 8-18 19-78 Duration of 36-180 0.5-72
pityriasis rubra pilaris: range (mo)
Therapy schedule Initial etretinate 0 .75-2 .0 0.75-1.0
dosage: range or (mg/kg/day) 50-75 rag/day*
Maintenance 0.3-1.0 0.5-0.9 etretinate dose: or range 10-75 rag/day* (mg/kg/day)
Duration: range 3-36 1.5-24 (mo)
Clinical responset Excellent (No. of 3 3
patients) Good (No. of 3 2
patients) Moderate (No. of 1 2
patients) None (No. of 1 1
patients) References [17-20] [12,19,21]
*The initial dosage was either 75 mg/day, or 50 rag/day alternating with 75 mg/day schedule; subsequently, there was maintenance of the same dosage or tapering. ~fExcellent, definite therapeutic effect; good, favorable clinical response; and moderate, partial improvement.
patients to methotrexate is low, yet appropriate clinical and laboratory monitoring is necessary, including liver biopsy? c-3~
Azathioprine also has been successful in treat- ment for pityriasis rubra pilaris. 6,a2 Within a few months after starting azathioprine (50 to 200 mg orally, in divided doses, each day) four of five adult patients with pityriasis rubra pilaris had complete clearing; a prolonged remission continued in half of these patients. 32 Other investigators also have observed a similar response to azathioprine. 6
Other treatments, used with variable success, include systemic vitamin C and/or, vitamin E (often in combination with vitamin A), 33, 34 isonia- zid, 37 paraaminosalicylic acid, 37 penicillin, 37,38
37 hydroxychloroquine, arsenic, 27 pilocarpine, ~7 pitu- itary extract) 7 foreign protein injections, 27 and topical 6-aminonicotinamide.39, 40
806 Cohen and Prystowsky
Phototherapy, as a primary and/or adjuvant treatment modality, generaUy has been unsuccess- ful in the management of pityriasis rubra pilaris. Only one patient is reported to have demonstrated clinical improvement when systemic psoralens and ultraviolet A (PUVA treatment), either alone or in concert with etretinate (Re-PUVA), was initi- ated, 41 No benefit 15 or exacerbation 6,12, ~4.19. 21. 42 was described in several other cases of PUVA-treated pityriasis rubra pilaris. In a small number of patients the onset or worsening of pityriasis rubra pilaris may have been related to a preceding sunburn 29 or to sunlight. 2,42,5~ In more recent reports the use of ultraviolet B, alone or with topical crude coal tar, did not result in significant clinical improvement; yet an averse effect was not observed, zs. 24.42 The poor response to phototherapy is, in fact, supportive of the diagnosis of pityriasis rubra pilaris.
In summary, the. diagnosis of pityriasis rubra pilaris is based primarily on the clinical presenta- tion. A histologic evaluation is helpful to rule out other papulosquamous and erythrodermic disor- ders. Seborrheic keratoses may become more prominent if erythroderma develops and may raise the suspicion of internal malignancy, which should be appropriately evaluated. Although no defect in vitamin A metabolism has been conclusively dem- onstrated, vitamin A and the newer synthetic derivatives play a significant role in therapy for many patients with pityriasis rubra pilaris. Thus a pathogenetic linkage between pityriasis rubra pilar- is and vitamin A metabolism remains an intriguing possibility. We believe that isotretinoin should be the first choice of systemic therapy for most patients with pityriasis rubra pilaris because of its therapeutic efficacy and safety. There is less toxic- ity, relative to the observed clinical response, with isotretinoin than with oral vitamin A. In compari- son with etretinate the shorter hal_f-life of isotreti- noin is favorable. The slow elimination of etretinate from the body---even after discontinuation of the drug--produces a prolonged risk of teratogenicity. However, long-term follow-up of isotretinoin- treated cases of pityriasis rubra pilaris, with respect to maintenance of remission, has not been reported. Premature closure of epiphyses in children treated with retinoids for other skin disorders is of concern in younger patients with pityriasis rubra pilaris. When retinoids are not successful, we favor the use of methotrexate or azathioprine.
Journal of the American Academy of
Dermatology
REFERENCES 1. Griffiths WAD. Pityriasis rubra pilaris--an historical
approach. Trans St Johns Hosp Dermatol Soc 1975; 61:58-69.
2. Griffiths WAD. Pityriasis rubra pilaris---an historical approach. II. Clinical features. Clin Exp Dermatol 1976;1:37-50.
3. Gross DA, Landau JW, Newcomer VD. Pityriasis rubra pflaris. Report of a case and analysis of the fiterature. Arch Dermatol 1969;99:710-6.
4. Griffiths A. Pityriasis rubra pilaris. Etiologic considera- tions. J AM AcAo DERMATOL 1984;10:1086-8.
5. Griffiths WAD. Pityriasis rubra pilaris: clinical features and natural history in a study of 93 patients (summaries of papers). Br J Dermatol 1977;97(suppl 15):18.
6. Griffiths WAD. Pityriasis rubra pilaris. Clin Exp Derma- tol 1980;5:105-12.
7. Sonnex TS, Dawber RPR, Zachary CB, Millard PR, Griffiths AD. The nails in adult type 1 pityriasis rubra pilaris. A comparison with Srzary syndrome and psoriasis. J AM A c ~ DEI~2ClATOL 1986;15:956-60.
8. Holdiness MR. The sign of Leser-Trrlat: a review. Int J Dermatol 1986;25:564-72.
9. Reinhardt LA, Rosen T. Pityriasls rubra pilaris as the initial manifestation of leukemia. Cutis 1983;31: 100-2.
10. King LE Jr, Dufresne RG Jr, Lovett GL, Rosin MA. Erythroderma: review of 82 cases. South Med J 1986; 79:1210-5.
11. Niemi K-M, Kousa M, Sorgards K, Karvonen J. Pityria- sis rubra pilaris. A clinico-pathological study with a special reference to autoradiography and histocompatibil- ity antigens. Dermatologica 1976;152:109-18.
12. Braun-Falco O, Ryckmanns F, Schmoeckel C, Landthal- er M. Pityriasis rubra pilaris: a clinico-pathological and therapeutic study with special reference to histochemistry, autoradiography, and electron microscopy. Arch Derma- tol Res 1983;275:287-95.
13. Goldsmith LA, Weinrich AE, Shupack J. Pityriasis rubra pilaris response to 13-cis-retinoic acid (isotretinoin). J AM ACAD D~RMATOL 1982;6:710-5.
14. Risch J, Ashton RE, Lowe N J, Chalet M. 13-cis-retinoic acid for dyskeratinizing disease---clinicopathological responses. Clin Exp Dermatol 1984;9:472-83.
15. Dicken CH. Isotretinoin treatment of pityriasis rubra pilaris. J AM ACAD DERMATOL 1987;16:297-301.
16. Windhorst DB. The use of isotretinoin in disorders of keratinization. An introduction. J AM ACAD DERMATOL 1982;6:708-9.
17. Fleissner J, Happle R: Etretinate in the treatment of juvenile pityriasis rubra pilaris. Arch Dermatol 1981; 117:749-50.
18. Gelmetti C, Schiuma AA, Cerri D, Gianotti F. Pityriasis rubra pilaris in childhood: a long-term study of 29 cases. Pediatr Dermatol 1986;3:446-51.
19. Kanerva L, Lauharanta J, Niemi K-M, Lassus A. Ultrastructure of pityriasis rubra pilaris with observations during retinoid (etretinate) treatment. Br J Dermatol 1983;108:653-63.
20. Traupe H, Happle R. Etretinate therapy in children with severe keratinization defects. Eur J Pediatr 1985;143: 166-9.
21. Lauharanta J, Lassus A. Treatment of pityriasis rubra pilaris with an oral aromatic retinoid (RO 10-9359). Acta Derm Venereol (Stockh) 1980;60:460-2.
22. Marks R, Finlay AY, Holt PJA. Severe disorders of
Volume 20 Number 5, Part I May 1989 Pityriasis rubra pilaris 807
keratinization: effects of treatment with Tigason (etreti- nate). Br J Dermatol 1981;104:667-73.
23. Viglioglia PA. Therapeutic evaluation of the oral retinoid Ro 10-9359 in several non-psoriatic dermatoses. Br J Dermatol 1980;103:483-7.
24. Randle HW, Diaz-Perez JL, Winkelmann RK. Toxic doses of vitamin A for pityriasis rubra pilaris. Arch Dermatol 1980;116:888-92.
25. Murray JC, Gilgor RS, Lazarus GS. Serum triglyceride elevation following high-dose vitamin A therapy for pityriasis rubra pilaris. Arch Dermatol 1983;119:675-6.
26. Winkelmann RK, Thomas JR III, Randle HW. Further experience with toxic vitamin A therapy in pityriasis rubra pilaris. Cutis 1983;31:621-9.
27. Lamar LM, Gaethe G. Pityriasis rubra pilaris. Arch Dermatol 1964;89:515-22.
28. Hanke CW, Steck WD. Childhood-onset pityriasis rubra pilaris treated with methotrexate administered intrave- nously. Cleve Clin Q 1983;50:201-3.
29. Knowles WR, Chernosky ME. Pityriasis rubra pilaris. Prolonged treatment with methotrexate, Arch Dermatol 1970;102:603-12.
30. Parish LC, Woo TH. Pityriasis rubra pilaris in Korea. Treatment with methotrexate. Dermatologica 1969; 139:399-403.
31. Brown J, Perry HO. Pityriasis rubra pilaris. Treatment with folio acid antagonists. Arch Dermatol 1966;94: 636-8.
32. Hunter GA, Forbes IJ. Treatment of pityriasis rubra pilaris with azathioprine. Br J Dermatol 1972;87:42-5.
33. Irgang S. Pityriasis rubra pilaris responsive to ascorhic acid. Aust J Dermatol 1968;9:211-7.
34. Ayres S Jr. Pityriasis rubra pilaris controlled by synergism of vitamins A and E. J AM AcAo DERMATOL 1981;5: 350-1.
35. Bergamaschini L, Tucci A, Colombo A, et al. Effect of stanozolol in patients with pityriasis rubra pilaris and retinol-binding protein deficiency [Letter]. N Engl J Med 1982;306:546-7.
36. Pavlidakey GP, Hashimoto K, Savoy LB, Heller GL, Iacobelli D, Barfield L. Stanozolol in the treatment of pityriasis rubra pilaris. Arch Dermatol 1985;121:546-8.
37. Watt TL, Jillson OF. Pityriasis rubra pilaris. Penicillin
and antitubereulous drugs as possibel therapeutic agents. Arch Dermatol 1965;92:428-30.
38. Stanoeva L, Konstantinov D, Ristov R. Clinical aspect of pityriasis rubra pilaris in childhood. Dermatotogica 1971;142:1-6.
39. Binniek SA. Pityriasis rubra pilaris responding to aminon- icotinamide. Arch Dermatol 1978;114:1348-9.
40. Zackheim HS. Topical 6-aminonicotinamide plus oral niacinamide therapy for psoriasis. Arch Dermatol 1978; 114:1632-8.
41. Brenner W, Gsehnait F, Honigsmann H, Fritsch P. Eprobung yon PUVA bei verschiedenen Dermatosen. Hautarzt 1978;29:541-4.
42. Hanny MG. Two cases of ? pityriasis rubra pilaris. Prec R Soc Med 1921;14:70-1.
43. Food and Nutrition Board: Recommended dietary allow- ances. 9th ext. Washington, DC: National Academy of Sciences. National Research Council, 1980.
44. Korner WF, Vollm J. New aspects of the tolerance of retinol in humans. Int J Vitam Nutr Res 1975;45:363- 72.
45. Silverman AK, Ellis CN, Voorhees JJ. Hypervitaminosis A syndrome: a paradigm of retinoid side effects. J AM AcAB DERMATOL 1987;16:1027-39.
46. Finzi AF, Altomare G, Bergamasehini L, Tucei A. Pityriasis rubra pilaris and retinol-binding protein. Br J Dermatol 1981;104:253-6.
47. Stoll DM, King LE Jr, Chytil F. Serum levels of retinol binding protein in patients with pityriasis rubra pilaris. Br J Dermatol 1983;108:375-8.
48. Vahlquist A. Retinol binding protein and pityriasis rubra pilaris [Letter]. Br J Dermatol 1982;107:125-71
49. Smith FR, Goodman DeWS. Vitamin A transport in human vitamin A toxicity. N Engl J Med 1976;294: 805-8.
50. Ellis CN, Voorhees JJ. Etretinate therapy. J AM ACAD DBR~ATOL 1987;16:267-91.
51. Peck GL, DiGiovanna JJ. Retinoids. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen KF, eds. Dermatology in general medicine. 3rd ed. New York: McGraw-Hill, 1987;2582-609.
52. Beamer JE, Newman SB, Reed WB, Cram D. Pityriasis rubra pilaris. Cutis 1972;10:419-23.
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具